 Georgia Vasiliki Gkountana1,2
Georgia Vasiliki Gkountana1,2 Lezhou Wang3,4,†Martina Giacomini1,†
Lezhou Wang3,4,†Martina Giacomini1,† Aini Hyytiäinen1,2
Aini Hyytiäinen1,2 Krista Juurikka3,4,5
Krista Juurikka3,4,5 Tuula Salo1,2,3,4
Tuula Salo1,2,3,4 Ahmed Al-Samadi1,2,6*
Ahmed Al-Samadi1,2,6*
- 1Department of Oral and Maxillofacial Diseases, Clinicum, Faculty of Medicine, University of Helsinki, Helsinki, Finland
- 2Translational Immunology Research Program (TRIMM), Faculty of Medicine, University of Helsinki, Helsinki, Finland
- 3Research Unit of Population Health, Faculty of Medicine, University of Oulu, Oulu, Finland
- 4Medical Research Center Oulu, Oulu University Hospital, University of Oulu, Oulu, Finland
- 5Faculty of Biochemistry and Molecular Medicine, University of Oulu, Oulu, Finland
- 6Institute of Dentistry, School of Medicine, Faculty of Health Sciences, University of Eastern Finland, Kuopio, Finland
Background: Head and neck squamous cell carcinoma (HNSCCs) is a common cancer type with a high mortality rate and poor prognosis. Recent studies have focused on the role of immune checkpoints in HNSCC progression and in their potential use as prognostic markers and immunotherapeutic candidates. Some immune checkpoints, such as PD-1 and PD-L1, have been studied thoroughly in HNSCC. Other molecules, such as indoleamine 2,3-dioxygenase 1 (IDO1), have been investigated minimally.
Methods: IDO1 expression, prognostic potential, and association with the immune profile of HNSCC were explored using online databases, including GEPIA, UALCAN, TIMER2.0, cBioPortal, and LinkedOmics, which utilize TCGA datasets and are freely available for use. For validation purposes, seven pairs of primary and metastatic HNSCC were immunostained for IDO1.
Results: Our analysis revealed significantly higher expression of IDO1 in HNSCC, especially in HPV+ SCCs compared with healthy control tissue. However, IDO1 expression showed weak to no prognostic potential for overall and disease-free survival in HNSCC. IDO1 expression in HNSCC was positively correlated with several immune-related molecules, including most of the immune checkpoints. Additionally, GO enrichment analysis revealed that several immune-related pathways are positively correlated with IDO1 expression in HNSCC, such as response to type I interferon and lymphocyte-mediated immunity pathways. Finally, IDO1 expression positively correlated with infiltration of most of the immune cells in HNSCC, such as CD4+ T cells, CD8+ T cells, M1 and M2 macrophages, dendritic cells, and B cells.
Conclusion: IDO1 expression is closely correlated with the immune profile of the HNSCC. This observation should be explored further to elucidate the potential of targeting IDO1 as a novel immunotherapeutic approach for HNSCC.
1 Introduction
Head and neck squamous cell carcinoma (HNSCC) is the eighth most common cancer type worldwide (1). HNSCC affects the mucosal surfaces of the oral cavity, nasal cavity, pharynx, and larynx and is associated with several risk factors, including alcohol consumption, tobacco use, and some viral infections, such as human papillomavirus (HPV) and Epstein-Barr virus (2, 3). HNSCC is currently treated with surgery with or without radiotherapy, chemotherapy, or targeted therapy (4). Additionally, nivolumab and pembrolizumab (anti-PD-1 antibodies) have recently been approved for treatment of recurrent or metastatic HNSCC (5).
As in all cancer types, HNSCC uses a variety of mechanisms to evade the immune system and to promote tumor growth and metastasis (6). One of these mechanisms is promoting immunosuppression, for example by stimulating the differentiation of suppressive immune cells (7). In fact, HNSCC patients have increased levels of T regulatory cells (Tregs) within the tumor-infiltrating lymphocyte (TIL) fraction, and immune responses of effector T cells are often defective (7, 8). Moreover, overexpression of immune checkpoints on the surface of T cells is another mechanism of immune evasion in HNSCC (9). The main immune checkpoint pathways in HNSCC include PD-1/PD-L1, cytotoxic T lymphocyte antigen 4 (CTLA-4), T-cell immunoglobulin mucin 3 (TIM-3), lymphocyte activation gene 3 (LAG-3), T-cell immunoglobulin and immunoreceptor tyrosine-based inhibitory motif (TIGIT), and indoleamine 2,3-dioxygenase 1 (IDO1) (9, 10).
IDO1 is a catabolic enzyme that converts tryptophan (Trp) into kynurenine in peripheral tissues (11) and is an immune-checkpoint molecule that is highly expressed in many cancers. IDO1 overexpression is usually associated with poor prognosis (12). In the tumor microenvironment (TME), IDO1 is expressed by cancer and stromal cells (such as tumor-associated macrophages and fibroblasts), endothelial cells, and some immune cells [such as dendritic cells and other antigen presenting cells (APC)] (11–13). IDO1 overexpression leads to Trp depletion, which in turn leads to inhibition of the mammalian target of rapamycin complex (mTORC) pathway and activation of the stress-response general control over nonderepressible (GCN2) kinase in tumor-infiltrating T cells, which both lead to immunosuppression (11). In addition, aryl hydrocarbon receptor (AhR) on several immune cell types is also activated, further promoting a suppressive TME (11). Furthermore, IDO1 is positively correlated to levels of TILs in HNSCC. Some reports identified IDO1 as a potential prognostic marker for HNSCC (14).
The role of IDO1 in HNSCC metabolism and immunosuppression is not fully understood. More data are needed to understand the clinical relevance of IDO1 in immunotherapeutic approaches for HNSCC and its potential as a biomarker. Moreover, knowledge on IDO1 in HNSCC may reveal new pathways that could be targeted therapeutically or used for prognostication. Further elucidating the crosstalk between the immune system, cancer cells, and TME-related molecules may lead to a better understanding of disease development and progression. Several databases, such as TIMER, UALCAN, and cBioPortal contain an abundance of multi-omics patient data for different types of cancers. Here, we sought to analyze data acquired from different databases to investigate IDO1 expression in HNSCC tumors and its correlation with patient survival, drug response, and tumor immune profile. Our analysis revealed that IDO1 is correlated with the immune landscape of HNSCC patients through a positive correlation with immune-related genes and immune-cell infiltration.
2 Methods
2.1 IDO1 gene expression analysis in normal tissues and HNSCC samples and its correlation with patient survival
Gene expression analysis of IDO1 in 520 HNSCC tumor samples from The Cancer Genomic Atlas (TCGA) and 44 adjacent normal tissue samples was performed using the TIMER2.0 database (15). TIMER2.0 provides gene-expression level data represented in a log2 transcripts per million (TPM) scale. The UALCAN platform (http://ualcan.path.uab.edu) was used to assess the correlation between IDO1 gene expression, illustrated as TPM, and patients' clinical and pathological characteristics, such as tumor stage and grade and patient age and gender (16, 17).
Single-cell RNA-seq data for eight distinct cell types (fibroblasts, macrophages, B, T, dendritic, cancer, endothelial, and mast cells) in HNSCC were retrieved from Gene Expression Omnibus database with the accession code GSE103322 (https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE103322). IDO1 expression levels in different cell populations in both primary tumor and lymph node metastasis (LNM) were analyzed and visualized using R (version 4.2.2) with dplyr, reshape2, data.table, tidyverse, ggplot2, ggpubr, hrbrthemes, viridis, and scales packages. Statistical significance in IDO1 expression in different cell types between primary tumor and LNM was assessed with Student's t-test. p-value < 0.05 was considered statistically significant.
Overall survival (OS) and disease-free survival (DFS) of HNSCC patients were evaluated in correlation to tumoral IDO1 expression using GEPIA (http://gepia.cancer-pku.cn) webtools and data obtained from TCGA Program project consisting of 518 HNSCC samples. The median of IDO1 expression levels was used as a group cutoff to determine high- and low-IDO1 expressing groups.
2.2 Immunostaining
Seven pairs of primary and metastatic HNSCC samples were collected at the Oulu University Hospital. The data inquiry was approved by the Finnish Medicines Agency (FIMEA). The use of patient material for this study was approved by the Northern Ostrobothnia Hospital District Ethics Committee (statement 101/2020). Detailed patient data are presented in Table 1.
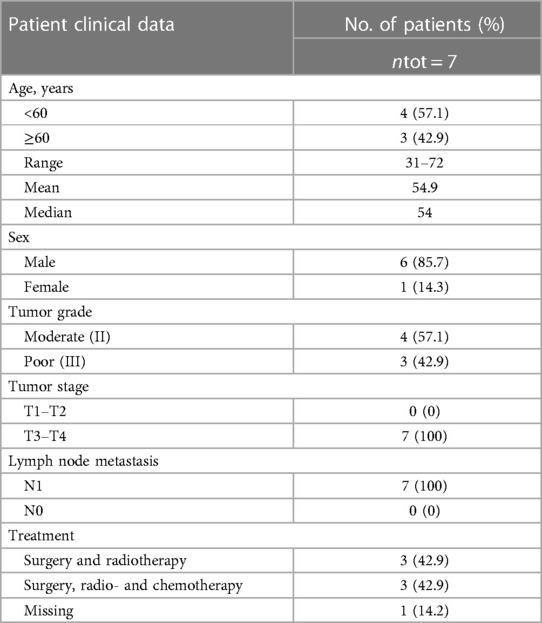
Table 1. Baseline characteristics of patients with HNSCC.
Samples were cut into 4 µm thick sections and deparaffinized. Antigen retrieval was carried out in citrate buffer using a microwave oven (MicroMED T⁄T Mega Histoprocessing Labstation; Milestone Srl, Sorisole, Italy). Afterwards, the slides were subjected to immunohistochemical (IHC) staining. The slides were incubated in Dako Peroxidase blocking agent (Agilent DAKO, Santa Clara, USA) for 15 min. After washes in PBS 3 × 5 min, the slides were incubated in 10% normal goat serum (Vector Laboratories, Burlingame, CA, USA) for 1h at room temperature (RT). Normal serum was blotted away, and the slides were incubated with 1:50 monoclonal Alexa Fluor-488 rabbit anti-human IDO1 primary antibody (Abcam, Cambridge, UK) overnight at +4°C. After washes, the slides were incubated with 1:300 biotinylated goat anti-rabbit secondary antibody (Vector Laboratories) in 2% BSA-PBS and 1% normal goat serum for 1 h at RT. After washes, the slides were incubated with avidin–biotin–peroxidase complex (Vectastain Elite ABC kit; Vector Laboratories) for 1 h at RT. After washes, the slides were incubated in 3,3′-diaminobenzidine tetrahydrochloride (DAB) chromogen (Agilent DAKO) for 10 min at RT. After washes in PBS 1 × 5 min and dH2O 2 × 5 min, the slides were incubated with Mayer's hematoxylin (Sigma-Aldrich, St. Louis, MI, USA) for 2 min at RT. After washing under running water for 10 min, the slides were dehydrated and cleared in xylene, mounted with J.T.Baker UltraKitt (Avantor, Radnor, PA, USA) and imaged.
Another batch of deparaffinized and antigen retrieved slides was used to perform double immunofluorescence (IF) staining. The slides were incubated with Intercept PBS Blocking Buffer (LI-COR, Lincoln, NE, USA) for 30 min at RT. The blocking buffer was blotted away, and the slides were incubated in 1:200 monoclonal mouse anti-human CD163 primary antibody (Leica, Deer Park, IL, USA) and 1:10,000 Hoechst (Thermo Scientific, Waltham, MA, USA) overnight at +4°C. After washes in PBS 3 × 5 min, the slides were incubated in 1:200 polyclonal Alexa Fluor-568 donkey anti-mouse secondary antibody (Invitrogen, Waltham, MA, USA) for 1h at RT. After washes in PBS 3 × 5 min, the slides were incubated in 1:50 monoclonal Alexa Fluor-488 rabbit anti-human IDO1 primary antibody (Abcam, Cambridge, UK) in PBS overnight at +4°C. After washes in PBS 3 × 5 min the slides were mounted using SlowFade diamond antifade (Invitrogen) and imaged.
Stained tissues were analysed and photographed using Leica DM6000 B/M light microscope connected to a digital camera (DFC420 and DFC365FX; Leica Microsystems, Wetzlar, Germany).
2.3 Analysis of IDO1 genetic alteration and DNA methylation
We used cBioPortal (https://www.cbioportal.org/) to investigate IDO1 genetic alterations and their possible effect on HNSCC patient survival (18, 19). For this purpose, the TCGA Firehose Legacy dataset was used and 504 HNSCC tumor samples were screened for mutations and copy number alterations (CNAs). Correlation between IDO1 alteration and patient survival was also explored.
The UALCAN database was employed to evaluate IDO1 promoter methylation levels in HNSCC and its association with patient clinical and pathological characteristics, such as tumor stage and grade and patient age and gender, in 528 TCGA HNSCC tumor samples and 50 normal tissue samples.
2.4 Correlation analysis of IDO1 expression and drug sensitivity on HNSCC cell lines
The association between IDO1 expression and drug sensitivity in HNSCC cell lines was assessed using the “Genomics of Drug Sensitivity in Cancer (GDSC) gene expression—drug sensitivity correlations” online tool provided by Tableau Public (https://public.tableau.com/profile/jason.roszik#!/vizhome/CCLE_GDSC_correlations/CCLE_GDSC). This dataset contains gene-expression and drug-screening data for 40 HNSCC cancer cell lines originating from the GDSC project (20).
2.5 IDO1 co-expression genes and gene set enrichment analysis
The LinkedOmics (http://www.linkedomics.org/) database was used to identify genes that are co-expressed with IDO1 in 520 TCGA HNSCC tumor samples, based on TCGA RNA sequencing data (21). IDO1 co-expressed genes are presented in a volcano plot produced using Spearman's correlation test. Moreover, Gene Ontology (GO) analysis for biological process, cellular component, molecular function, and KEGG pathway analysis were performed using the gene set enrichment analysis (GSEA) tool of LinkInterpreter. For the GSEA, the following parameters were chosen: false discovery rate (FDR) < 0.05 as rank criteria; minimum number of genes 3; and 1,000 simulations.
Additionally, the “Cancer Exploration” tool of TIMER2.0 was utilized to define the association between IDO1 and several immune checkpoints expression, including ADORA2A, B7-H1 (PD-L1), CD276, CTLA4, C10ORF54, KIR2DL1, KIR2DL3, KIR2DS4, KIR3DL1, KIR3DL2, KIR3DL3, KIR3DP1, KIR3DX1, LAG3, PD-1, and VTCN1 in 520 TCGA HNSCC tumor samples.
2.6 Correlation analysis of IDO1 expression and immune cell infiltration
Lastly, the “Immune Association” tool of TIMER2.0 was used to assess the correlation between IDO1 expression and immune infiltrates in 520 TCGA HNSCC tumor samples (15). The xCELL (https://xcell.ucsf.edu/) estimation tool was used as it contains gene-expression data for a large number of immune cells (22). Tumor purity adjustment was applied for the analysis.
3 Results
3.1 IDO1 expression is higher in HNSCC tumors compared to normal tissue and high expression predicts better overall survival for HNSCC patients
Gene expression analysis using TIMER2.0 revealed significantly higher (p < 0.001) IDO1 expression in HNSCC tumor samples (n = 520) than in the adjacent normal tissues (n = 44, Figure 1A). In addition, when HNSCC samples were stratified according to HPV− (n = 421) and HPV+ (n = 97) status, a significantly higher (p < 0.001) expression of IDO1 was observed in HPV+ compared to HPV− tumors (Figure 1A).
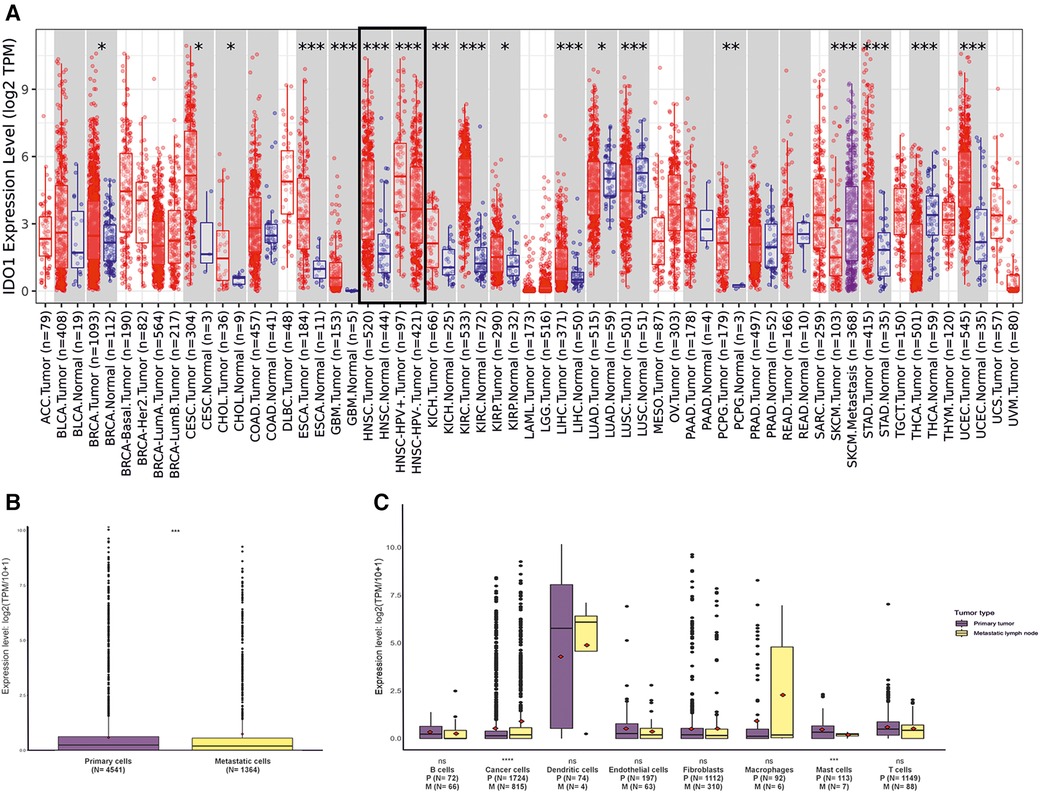
Figure 1. IDO1 expression levels in different tumors, matched normal tissues, and in various cell populations in HNSCC primary tumors and metastatic lymph nodes. (A) IDO1 expression in different tumors and their matched normal tissues. Statistical significance computed by the Wilcoxon test is provided by TIMER2.0. (B) IDO1 expression in primary and metastatic lymph node tumors. (C) Comparison of IDO1 expression levels in different cell types between primary tumors and metastatic lymph node sites. Statistical significance was assessed with Student's t-test. *indicates p-value < 0.05; **p-value < 0.01; ***p-value < 0.001; ****p-value < 0.0001. HNSCC, head and neck squamous cell carcinoma; HPV, human papilloma virus; TPM, transcripts per million; P, primary tumor; M, metastatic lymph node.
To investigate the cellular sources of IDO1 expression in HNSCC tumors, we analyzed a single-cell RNA-seq dataset taken from the study of Puram et al. (23). IDO1 expression in the metastatic lymph node tumors was slightly but significantly (p < 0.001) higher than in the primary tumors (Figure 1B). Interestingly, cancer cells in metastatic lymph nodes express significantly (p < 0.0001) higher levels of IDO1 than cancer cells in the primary tumor (Figure 1C). On the other hand, mast cells in metastatic lymph nodes express lower levels (p < 0.001) of IDO1 than the mast cells in the primary tumor. However, there were only seven mast cells analyzed in the metastatic lymph nodes compared with 113 cells in the primary tumor (Figure 1C). No other statistically significant difference was observed for the remaining cell types (i.e., B cells, dendritic cells, endothelial cells, fibroblasts, macrophages, and T cells), (Figure 1C). Macrophages and dendritic cells showed the highest level of IDO1 expression compared with other cells (Figure 1C).
In order to validate the single-cell RNA-seq dataset, we did IHC staining of IDO1 on seven pairs of primary and metastatic HNSCC samples (Figures 2A,B). Primary and metastatic cancer cells showed similar levels of IDO1 expression (Figure 2C). Interestingly, we found a moderate correlation (r = 0.07) of IDO1 expression between the primary and metastatic cancer cells (Figure 2D). Additionally, we conducted double IF staining of IDO1 and macrophage marker (CD163, Figures 2E–H). Similar to the single-cell RNA-seq dataset, several macrophages were positive for IDO1 indicating that macrophages are one source of IDO1 in HNSCC (Figures 2E–H).
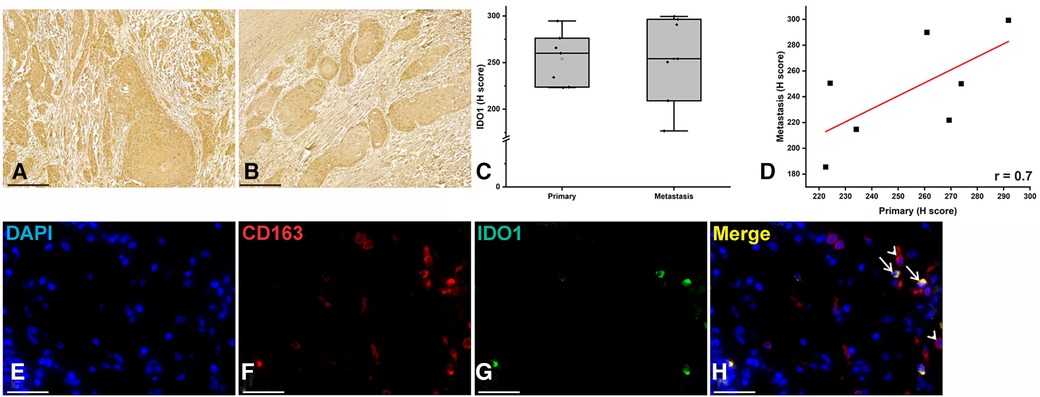
Figure 2. IDO1 immunostaining in HNSCC samples. (A–C) Immunohistochemical staining revealed similar staining intensity of IDO1 between primary and metastatic HNSCC cells. (D) Pearson correlation showed a moderate correlation of IDO1 expression between the primary and metastatic HNSCC cells. (E–H) Double immunofluorescence staining showed double positive cells for IDO1 (green) and macrophage marker CD163 (red).
Investigating IDO1 expression against clinicopathological characteristics of HNSCC patients using the UACLAN database revealed a significant decrease in IDO1 expression with increasing tumor stage (Figure 3A). On the other hand, IDO1 did not have a significant correlation with the other clinical and pathological characteristics of HNSCC patients, such as tumor grade (Figure 3B), patient age (Figure 3C), and patient gender (Figure 3D). However, we observed a trend (p = ns) for increased IDO1 expression with increasing tumor grade (Figure 3B).
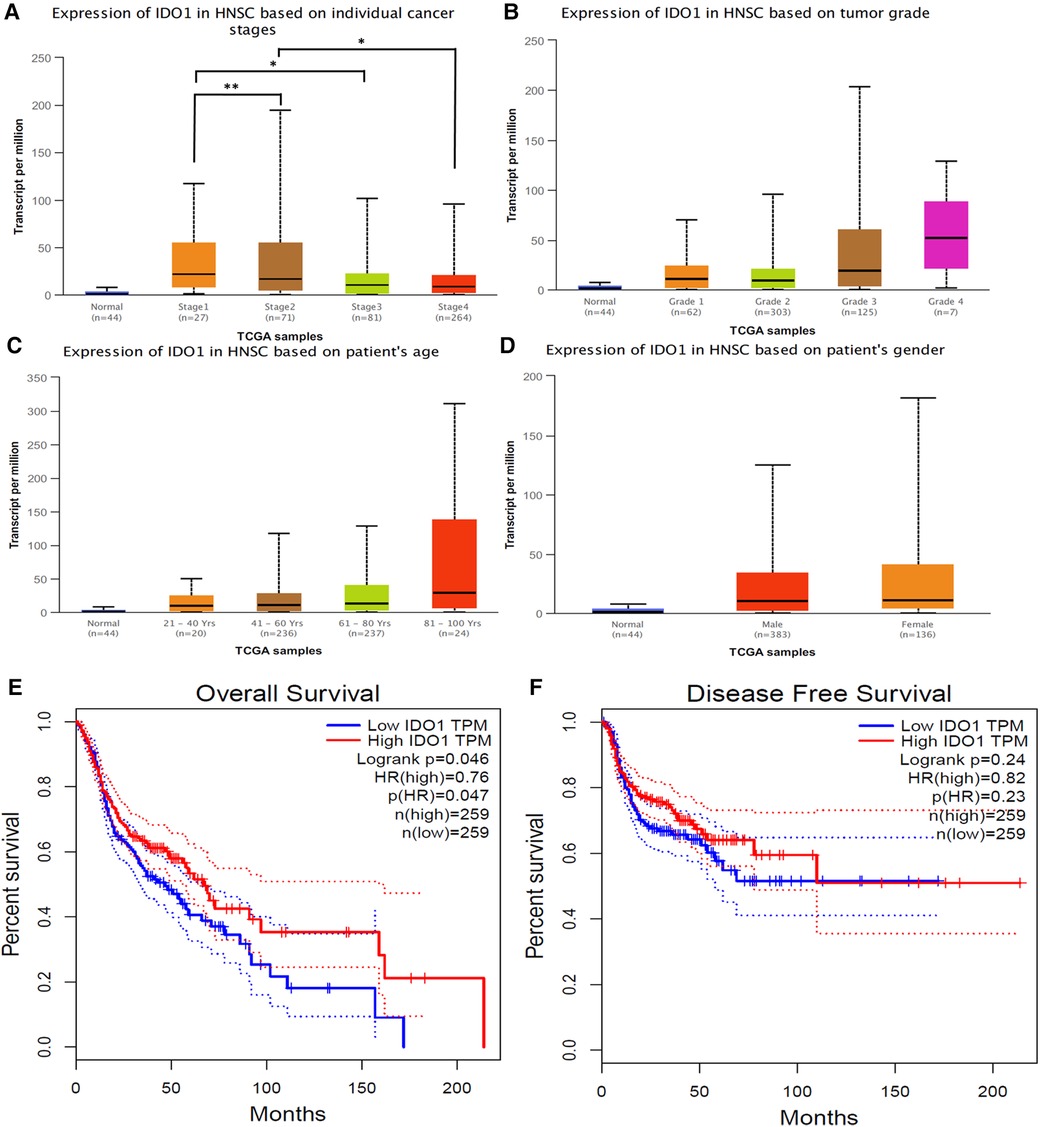
Figure 3. Correlation between IDO1 expression and clinicopathological characteristics of HNSCC patients. (A) tumor stage, (B) tumor grade, (C) patient age, (D) patient gender. Statistical significance is provided by UALCAN and is represented by the number of stars; *p-value < 0.05; **p-value < 0.01. Normal samples were not included in the statistical analysis. (E) Analysis of IDO1 expression in correlation to HNSCC patient overall survival and (F) disease-free survival. HNSCC, head and neck squamous cell carcinoma; HR, hazard ratio; TPM, transcripts per million.
We examined the association between IDO1 expression and OS and DFS of HNSCC patients using GEPIA. Univariate analysis revealed a significant correlation between IDO1 expression and patient OS (p = 0.047, Figure 3E); HNSCC patients with higher IDO1 expression had a better OS than patients with lower IDO1 expression. However, no significant correlation was observed between IDO1 expression and patient DFS (Figure 3F). Multivariate analysis was not performed on this data.
3.2 IDO1 genetic alteration and DNA methylation in HNSCC
Next, we examined genetic alterations in the IDO1 gene in HNSCC tumors using cBioPortal, which revealed that IDO1 was altered in 33 out of 504 HNSCC tumor samples (6.5% of the samples, Figure 4A). The most common alteration was amplification in 22 samples (4.37%), followed by mutation in 6 samples (1.19%), and deep deletion in 5 samples (0.99%; Figure 4A). None of the IDO1 copy-number alterations (CNA) seemed to affect IDO1 expression in HNSCC tumors, as we observed similar IDO1 expression in each type of CNA compared to the diploid samples (Figure 4B).

Figure 4. IDO1 genetic alterations in HNSCC and their effect on patient survival. (A) Frequency and types of IDO1 genetic alterations in HNSCC tumors. (B) Correlation between IDO1 mRNA expression and copy-number alteration in HNSCC tumors. (C) Overall survival comparison between IDO1-altered and IDO1-unaltered patient groups. (D) Disease-free survival comparison between IDO1-altered and IDO1-unaltered patient groups. HNSCC, head and neck squamous cell carcinoma.
The 504 HNSCC patients from the cBioPortal database were then clustered into the following two groups: altered group, consisting of patients with IDO1 genetic alterations and unaltered group, consisting of patients without IDO1 genetic alteration. The two groups were then compared in terms of OS and DFS. Alterations in IDO1 appeared to have no significant effect on either OS (Figure 4C) or DFS (Figure 4D). However, there appeared to be a trend (p = ns) for better patient OS and DFS in the altered patient group, which was difficult to verify statistically due to the low number of cases with altered IDO1.
Analysis of IDO1 DNA methylation in UALCAN showed a significant (p < 0.0001) decrease in promoter methylation in HNSCC tumor samples (n = 528) compared to the adjacent normal tissues (n = 50; Figure 5A). Correlation analysis between promoter methylation and tumor stage and grade and patient age and gender did not reveal significant results (Figures 5B–E).
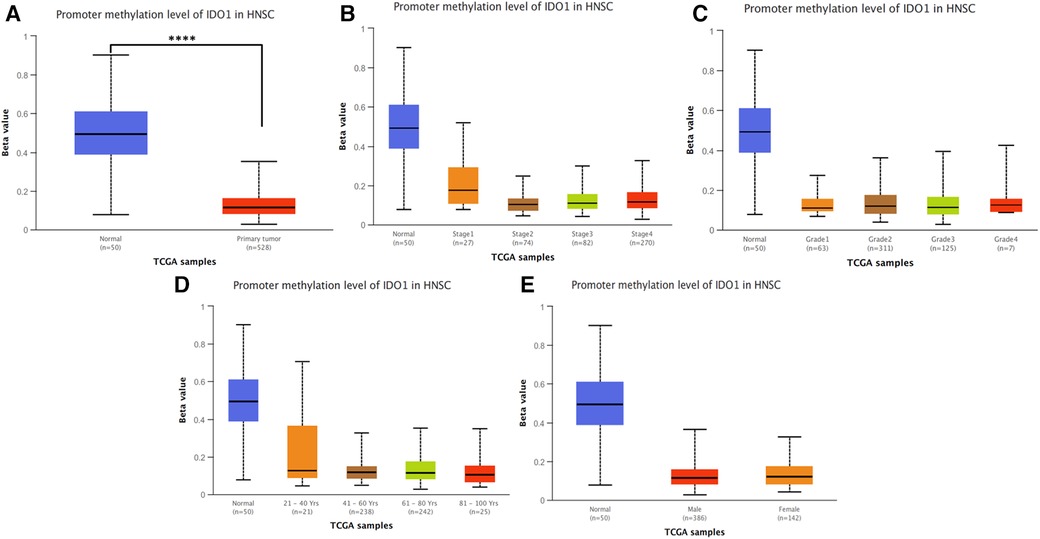
Figure 5. IDO1 DNA promoter methylation analysis. (A) Promoter methylation levels of normal tissues and HNSCC tumor samples. Correlation between promoter methylation levels and (B) tumor stage, (C) tumor grade, (D) patient age, and (E) patient gender. Statistical significance is provided by UALCAN and is represented by the number of stars; **** p-value < 0.0001. (B–E) Normal samples were not included in the statistical analysis. HNSCC, head and neck squamous cell carcinoma.
3.3 IDO1 expression correlate with the potency of several drugs on HNSCC cell lines
Using the “GDSC gene expression—drug sensitivity correlations” tool of Tableau Public, 15 drugs tested in 40 HNSCC cell lines were significantly correlated with IDO1 expression (Table 2). Drug sensitivity of 2 out of 15 drugs (MG-132 and Z-LLNIe-CHO) was positively correlated with IDO1 expression, while sensitivity of 13 out of 15 drugs (AZD6482, UNC1215, BX-912, OSI-930, CAL-101, XMD13-2, PLX4720, GW-2580, DMOG, BX-795, Genentech Cpd 10, GSK-650394, and QS11) was negatively correlated with IDO1 expression (Table 2).
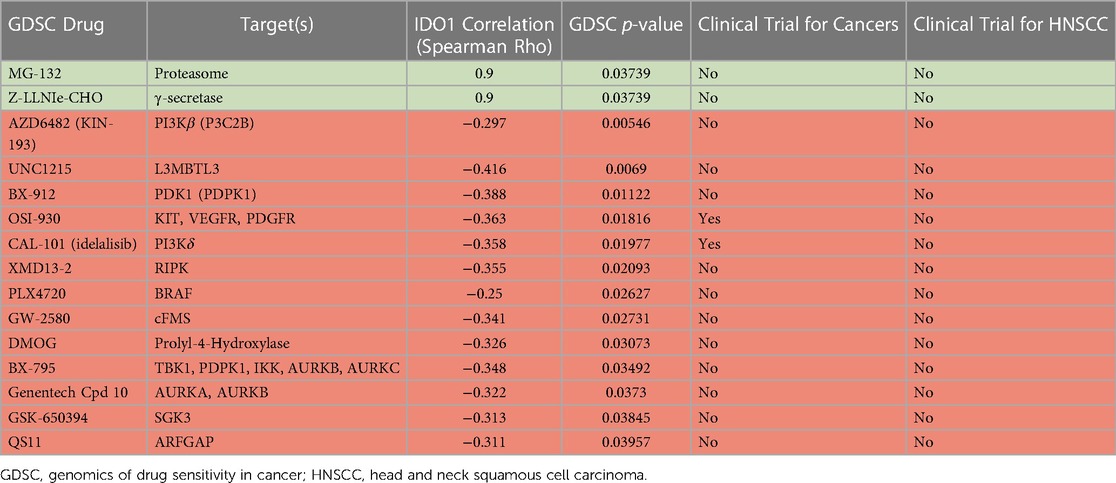
Table 2. Correlation analysis between IDO1 expression levels and drug sensitivity on HNSCC cell lines. Green lines represent positive and red lines negative correlated drugs.
Furthermore, the “clinical trials” tool provided by the U.S. National Library of Medicine (https://clinicaltrials.gov/) was used to explore whether these drugs have been or are currently in clinical trials for different cancers, including HNSCC. Two of these drugs, OSI-930 and idelalisib (CAL-101), have been in clinical trials for other types of cancers. None of the drugs has been in a clinical trial for HNSCC (Table 2).
3.4 IDO1 expression is positively correlated with immune-related genes and immune checkpoints in HNSCC
Correlation between IDO1 expression and 20,164 other genes in HNSCC was analyzed in LinkedOmics and revealed that IDO1 is significantly correlated with 10,322 genes expressed in HNSCC (Figure 6A). Of these, 4,715 genes were positively correlated with IDO1 expression, while 5,607 genes were negatively correlated with IDO1 expression. For further analysis, we plotted the top 50 genes positively or negatively correlated with IDO1 expression in HNSCC (Figures 6B,C). Of note, 41 out of the 50 genes that were positively correlated with IDO1 expression (Figure 6B) were immune-related genes, while only 3 out of 50 genes that were negatively correlated with IDO1 expression (Figure 6C) had immune-related roles. Furthermore, GO analysis of these genes revealed that IDO1-correlated genes are mainly involved in immune-related processes, as seen in the analysis of biological processes (Figure 6D), cellular components (Figure 6E), molecular functions (Figure 6F), and KEGG pathways (Figure 6G).
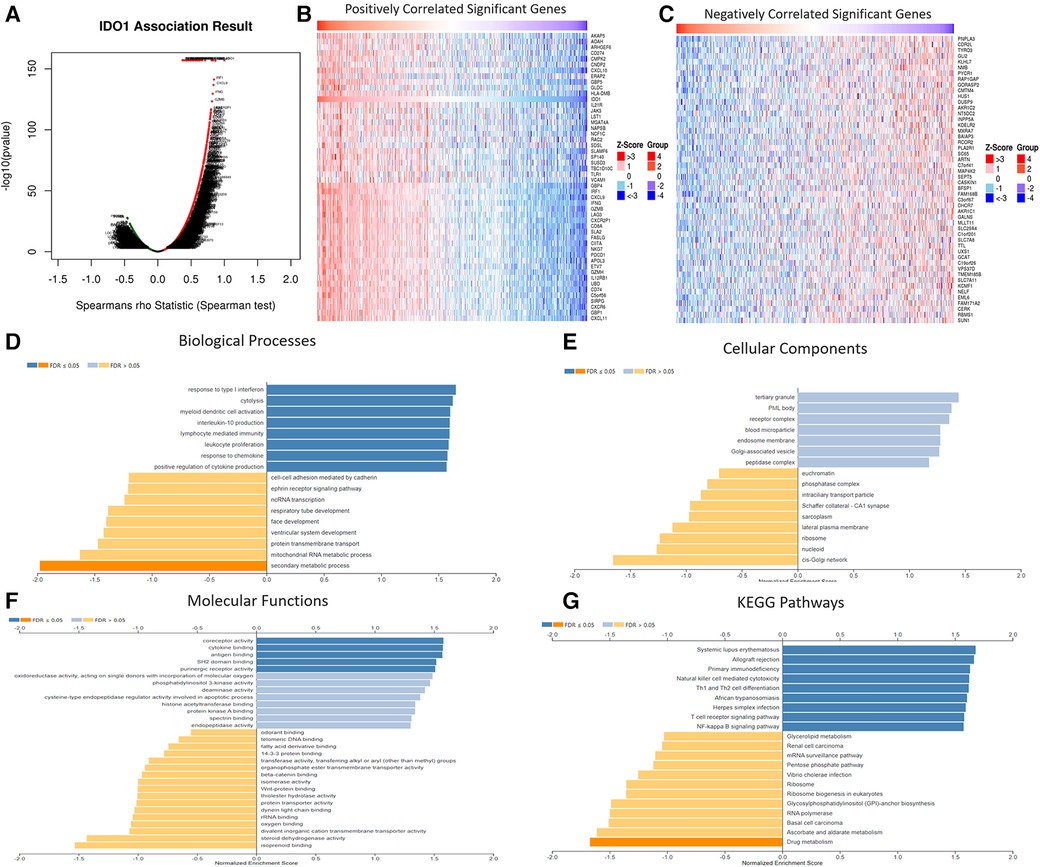
Figure 6. Correlation between IDO1 expression and its co-expressed genes in HNSCC. (A) Volcano plot of IDO1-correlated genes in HNSCC. (B) Top 50 IDO1 positively correlated genes in HNSCC. (C) Top 50 IDO1 negatively correlated genes in HNSCC. (D) GO analysis for biological processes of IDO1-correlated genes in HNSCC. (E) GO analysis for cellular components of IDO1-correlated genes in HNSCC. (F) GO analysis for molecular functions of IDO1-correlated genes in HNSCC. (G) GO analysis for the KEGG pathways of IDO1-correlated genes in HNSCC. GO, gene ontology; FDR, false discovery rate; KEGG, kyoto encyclopedia of genes and genomes.
Expression of several immune checkpoints in correlation to IDO1 expression in HNSCC was analyzed with TIMER2.0. IDO1 expression was positively and significantly (at least p < 0.01) correlated with most (14 out of 17) of the immune checkpoints tested (Figure 7). Interestingly, when HNSCC cases were stratified by HPV− and HPV+ status, both groups showed similar results (Figures 7A,B).
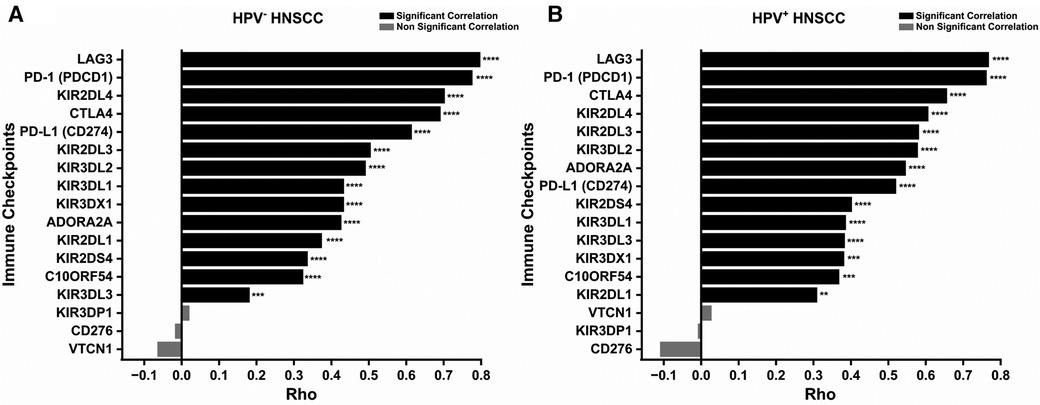
Figure 7. Correlation between IDO1 expression and immune checkpoints in HNSCC. (A) Correlation between IDO1 expression and immune checkpoints in HPV− HNSCC. (B) Correlation between IDO1 expression and immune checkpoints in HPV+ HNSCC. **p-value < 0.01; ***p-value < 0.001; ****p-value < 0.0001. HNSCC, head and neck squamous cell carcinoma; HPV, Human papillomavirus.
3.5 IDO1 expression positively correlates with immune-cell infiltration in HNSCC
Correlation analysis between immune-cell infiltrates and IDO1 expression using TIMER2.0 showed that IDO1 has a significant positive correlation with most of the immune cells in HPV− and HPV+ HNSCC (Figures 8, 9). Interestingly, both groups shared large similarities.
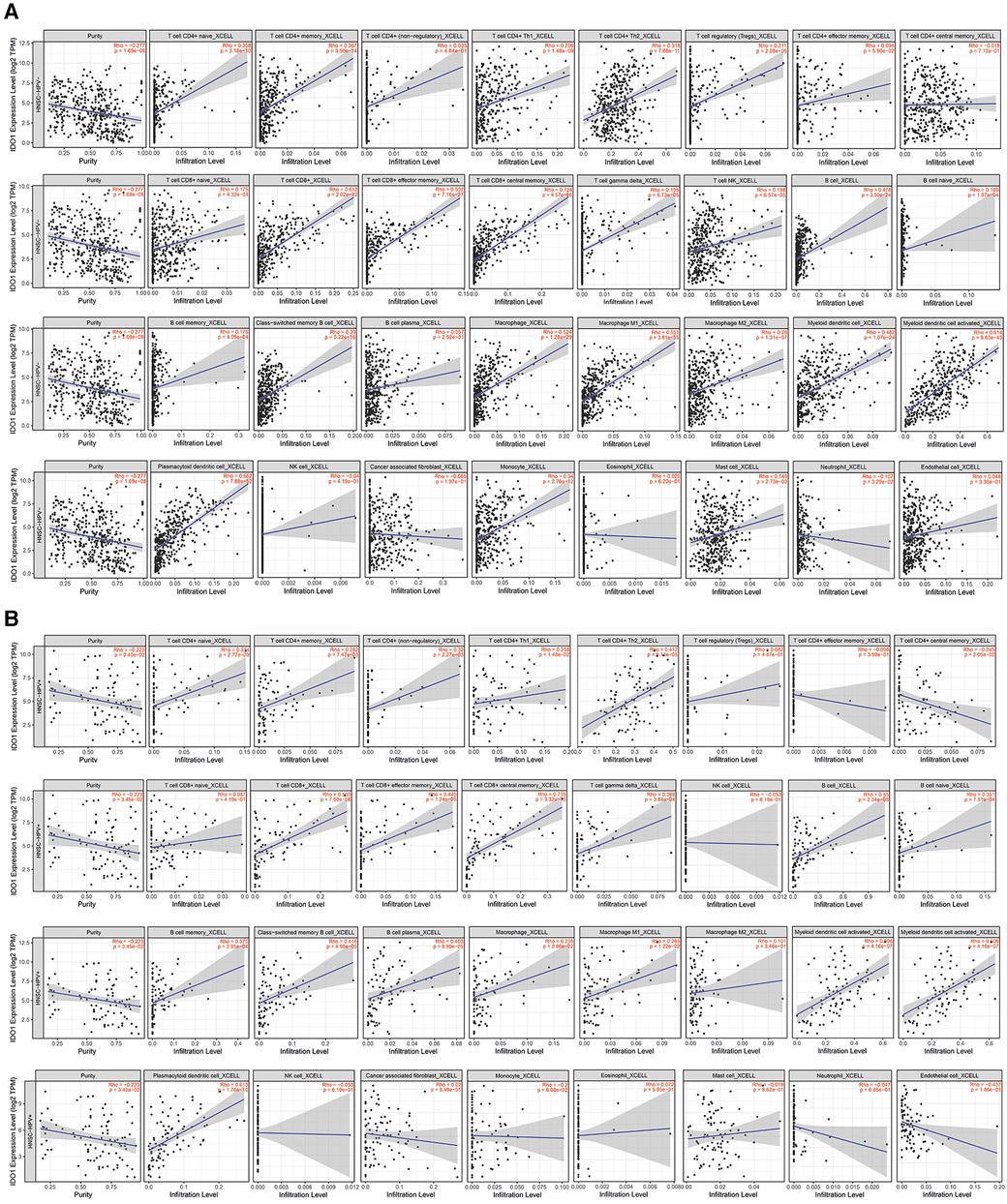
Figure 8. Correlation between IDO1 expression levels and immune infiltration. (A) HPV− HNSCC, (B) HPV+ HNSCC. Tumor purity for each category (HPV- and HPV+) is depicted in the first place of each line.
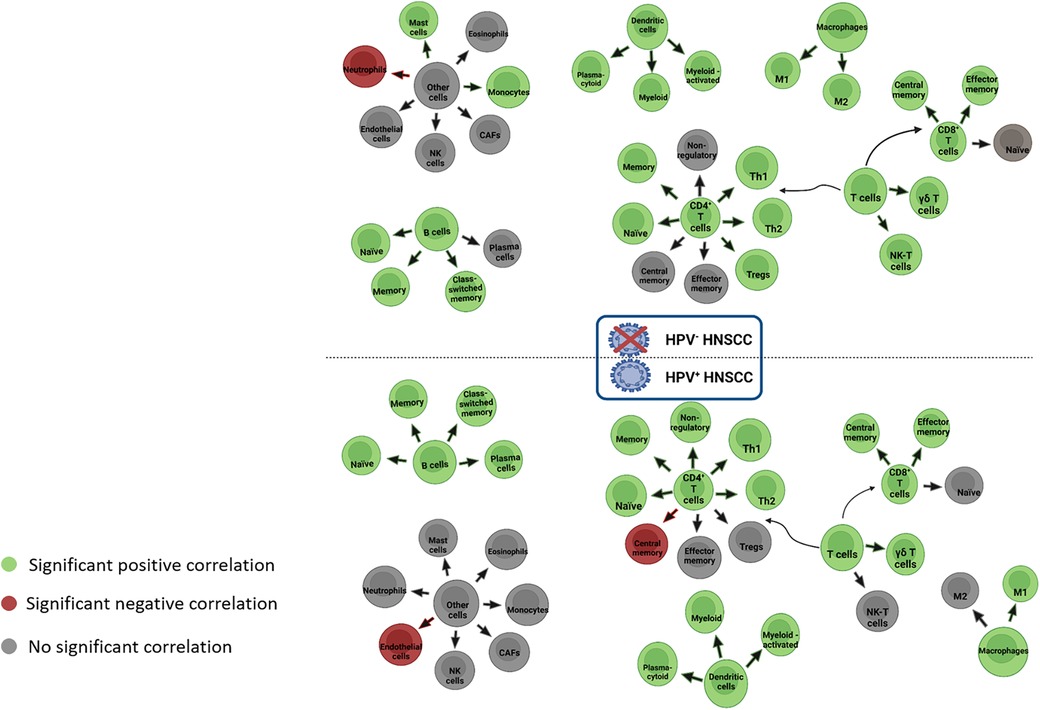
Figure 9. Correlation between IDO1 expression and immune infiltration in HPV− and HPV+ HNSCC. CAFs, cancer-associated fibroblasts; HNSCC, head and neck squamous cell carcinoma; HPV, human papillomavirus; M1/M2, macrophage 1 or macrophage 2; NK, natural killer cells; Th, T helper cells.
More specifically, in HPV− tumors (Figure 8A), IDO1 seems to be positively correlated with naïve, memory, and class-switched memory B cells; naïve, memory, helper 1, helper 2, and regulatory CD4+ T cells; central memory and effector memory CD8+ T cells; γδ T cells and NK-T cells; plasmacytoid, myeloid, and activated myeloid dendritic cells (DCs); M1 and M2 macrophages; monocytes; and mast cells. IDO1 seems to be negatively correlated with neutrophils in HPV− tumors. In HPV + tumors (Figure 8B), IDO1 appears to be positively correlated with naïve, memory, class-switched memory B cells and plasma cells; naïve, memory, helper 1, helper 2, and non-regulatory CD4+ T cells; central memory and effector memory CD8+ T cells; γδ T cells; plasmacytoid, myeloid, and activated myeloid DCs; and M1 macrophages. In the same cases, IDO1 appears to be negatively correlated with central memory CD4+ T cells and endothelial cells.
4 Discussion
IDO1 is highly expressed in a variety of cancers (24). Our analysis revealed that IDO1 expression is higher in HNSCC tumors compared to that in normal tissues. Interestingly, IDO1 is highly expressed especially in HPV+ HNSCC tumors compared with HPV− tumors. The high expression of IDO1 in HPV+ tumors can be explained in the context of high inflammation usually seen in this type of tumor in comparison with HPV− cases (25). We also conducted a comparison analysis of IDO1 expression levels in different cells between the primary tumor and metastatic lymph nodes. This analysis revealed that cancer cells in metastatic lymph nodes express higher levels of IDO1 than cancer cells in the primary tumor. However, based on our IHC staining, this was not validated which could be due to the small sample size and the small difference that was found at the mRNA level. Furthermore, we also observed significantly higher expression of IDO1 in primary tumor mast cells (N = 113) than in mast cells located in the metastatic lymph nodes (N = 7). However, this difference needs further validation due to the large difference in the number of cells between the two groups.
High IDO1 expression positively correlates with advanced stage in oral squamous cell carcinoma (26). In this study, we investigated the correlation between IDO1 expression and clinicopathological characteristics of HNSCC patients. Our results contrast with those of Struckmeier et al. (26), as higher IDO1 expression is positively associated with lower HNSCC stage. This suggests that IDO1 can be used as a biomarker for new treatment approaches for late-stage HNSCC.
The correlation between IDO1 expression and patient survival is controversial. For example, higher IDO1 expression correlated with better survival in melanoma patients, whereas high IDO1 expression predicted poorer survival in patients with glioblastoma when compared with patients with low IDO1 expression (24). Based on our data, IDO1 expression showed weak to no potential to predict patient survival in HNSCC. Our observation is consistent with previous studies. One study reported that high IDO1 expression has prognostic potential (14), while another study indicated that IDO1 could be used as a prognostic marker only in the early stages of oral cancer (27). In that study, patients with higher IDO1 expression levels had significantly better OS than patients with lower IDO1 levels. However, here the correlation between IDO1 expression and OS was observed only in a univariate analysis, with borderline significance (p = 0.047). Additionally, IDO1 expression had no correlation with DFS. Altogether, current data suggest that IDO1 is not a suitable prognostic marker for HNSCC patient survival or for cancer recurrence. Furthermore, we investigated IDO1 genetic alterations and their association with HNSCC patient survival. We found that IDO1 is rarely altered in HNSCC and none of the alterations had any significant effect on IDO1 expression. Moreover, patient survival was similar between patients with (altered group) or without (unaltered group) IDO1 genetic alterations, suggesting that IDO1 genetic changes should not be used as a prognostic marker.
We explored IDO1 DNA promoter methylation in HNSCC and its correlation with patient clinicopathological characteristics. Although no significant correlation was observed between IDO1 DNA promoter methylation and patient characteristics, we found that HNSCC samples have significantly lower IDO1 promoter methylation levels than normal tissues. IDO1 promoter methylation is negatively correlated with IDO1 expression in HNSCC, and HNSCC tumors, especially HPV+, have lower IDO1 promoter methylation (28), consistent with the data presented in this study. In addition, Sailer et al. (27) also showed that IDO1 promoter flank methylation correlates with tumor immunity of HNSCC tissues, as promoter flank methylation is associated with TILs and other immune cells (28). This suggests that IDO1 promoter methylation could be used as a biomarker for immune hot or cold tumors and therefore could be applied for decisions on patient treatment.
An assessment of drug sensitivity in relation to IDO1 expression in 40 HNSCC cell lines revealed two compounds, MG-132 and Z-LLNIe-CHO, that were positively correlated to IDO1 expression. Our analysis showed that 13 compounds had a negative association in terms of drug sensitivity to IDO1 expression. Of these, only two [OSI-930 and CAL-101 (idelalisib)] have been in clinical trials for cancers, but none for HNSCC. Idelalisib has been studied mainly in hematological and B-cell malignancies, while OSI-930 has been studied for advanced solid tumors (NCT02739360, NCT01796470, NCT00513851). These results may be a useful tool for future clinical trials or treatment decisions for patients with high or low IDO1 expression and could open possibilities for more personalized treatment combinations depending on IDO1 expression levels.
IDO1 is significantly positively correlated to genes with immune-related functions, further strengthening the role and relation of IDO1 to tumor immunity. Additionally, we found that IDO1 expression is positively correlated with 14 out of 17 tested immune checkpoints. It is worth mentioning that three of these immune markers belong to the main immune checkpoint pathways in HNSCC, namely PD-1, CTLA-4, and LAG3, which suggests that combination treatment with IDO1 inhibitors may be beneficial for some patients.
We observed that IDO1 expression is positively correlated to most of the immune infiltrates in HNSCC in both HPV+ and HPV− tumors. This correlation is mainly returned to the fact that IDO1 is positively correlated with the presence of cancer-associated inflammation. Additionally, due to M1 and M2 plasticity, it is expected to see a positive correlation between IDO1 and both M1 and M2 at the same time. Thus far, there are not many studies on the association between IDO1 expression and immune infiltration in HNSCC. One of the existing, webtool-based studies conducted by Li et al. showed that IDO1 expression was positively correlated with infiltration of CD4+ T cells, CD8+ T cells, neutrophils, macrophages, and myeloid dendritic cells (14). While our results are slightly different from the study, we stratified HNSCC tumors into HPV− and HPV+ status, which may result in slightly different but more accurate results. Moreover, online databases are constantly updated with new patient samples and data, which can also lead to inconsistent results between different studies.
There are some limitations to the present study. Firstly, most of the acquired data and analyses were based on online databases and web tools. The patient sample number in some of the analyses was small, especially when subcategorizing patients into smaller groups, for example in the analysis of genetic alterations of IDO1 in comparison to HNSCC patient survival. Furthermore, the treatment approach of HNSCC patients was not reported and was not considered for any of the analyses.
In conclusion, IDO1 appears to be highly associated with the immune landscape in HNSCC patients and is therefore a promising target for new treatment approaches. Further elucidating the association between IDO1, TME, and immune profile of HNSCC may be essential for identifying predictive biomarkers that could be useful in personalized immunotherapeutic approaches. Further in vitro and in vivo experiments are needed for a more in-depth knowledge on the biology of IDO1 in HNSCC.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary Material.
Author contributions
GG: Conceptualization, Data curation, Formal Analysis, Methodology, Writing – original draft. LW: Data curation, Methodology, Writing – review & editing. MG: Data curation, Methodology, Writing – review & editing, Formal Analysis. AH: Data curation, Methodology, Writing – review & editing. KJ: Data curation, Formal Analysis, Writing – review & editing, Methodology, Supervision. TS: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Writing – review & editing. AA-S: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This work was supported by Research Council of Finland, Minerva Foundation, Cancer Society of Finland, the Sigrid Juselius Foundation, the Finnish Dental Society Apollonia, the Jane and Aatos Erkko Foundation, and Helsinki University Central hospital research funds.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
2. Gormley M, Creaney G, Schache A, Ingarfield K, Conway DI. Reviewing the epidemiology of head and neck cancer: definitions, trends and risk factors. Br Dent J. (2022) 233:780–6. doi: 10.1038/s41415-022-5166-x
3. Mody MD, Rocco JW, Yom SS, Haddad RI, Saba NF. Head and neck cancer. Lancet. (2021) 398:2289–99. doi: 10.1016/S0140-6736(21)01550-6
4. Sacco AG, Cohen EE. Current treatment options for recurrent or metastatic head and neck squamous cell carcinoma. J Clin Oncol. (2015) 33:3305–13. doi: 10.1200/JCO.2015.62.0963
5. Hsieh RW, Borson S, Tsagianni A, Zandberg DP. Immunotherapy in recurrent/metastatic squamous cell carcinoma of the head and neck. Front Oncol. (2021) 11:705614. doi: 10.3389/fonc.2021.705614
6. Elmusrati A, Wang J, Wang CY. Tumor microenvironment and immune evasion in head and neck squamous cell carcinoma. Int J Oral Sci. (2021) 13:24. doi: 10.1038/s41368-021-00131-7
7. Damasio MPS, Nascimento CS, Andrade LM, de Oliveira VL, Calzavara-Silva CE. The role of T-cells in head and neck squamous cell carcinoma: from immunity to immunotherapy. Front Oncol. (2022) 12:1021609. doi: 10.3389/fonc.2022.1021609
8. Duray A, Demoulin S, Hubert P, Delvenne P, Saussez S. Immune suppression in head and neck cancers: a review. Clin Dev Immunol. (2010) 2010:701657. doi: 10.1155/2010/701657
9. Veigas F, Mahmoud YD, Merlo J, Rinflerch A, Rabinovich GA, Girotti MR. Immune checkpoints pathways in head and neck squamous cell carcinoma. Cancers (Basel). (2021) 13:1018. doi: 10.3390/cancers13051018
10. Lin DJ, Ng JCK, Huang L, Robinson M, O'Hara J, Wilson JA, et al. The immunotherapeutic role of indoleamine 2,3-dioxygenase in head and neck squamous cell carcinoma: a systematic review. Clin Otolaryngol. (2021) 46:919–34. doi: 10.1111/coa.13794
11. Peyraud F, Guegan JP, Bodet D, Cousin S, Bessede A, Italiano A. Targeting tryptophan catabolism in cancer immunotherapy era: challenges and perspectives. Front Immunol. (2022) 13:807271. doi: 10.3389/fimmu.2022.807271
12. Tang K, Wu YH, Song Y, Yu B. Indoleamine 2,3-dioxygenase 1 (IDO1) inhibitors in clinical trials for cancer immunotherapy. J Hematol Oncol. (2021) 14:68. doi: 10.1186/s13045-021-01080-8
13. Liu M, Wang X, Wang L, Ma X, Gong Z, Zhang S, et al. Targeting the IDO1 pathway in cancer: from bench to bedside. J Hematol Oncol. (2018) 11:100. doi: 10.1186/s13045-018-0644-y
14. Li C, Chen S, Jia W, Li W, Wei D, Cao S, et al. Identify metabolism-related genes IDO1, ALDH2, NCOA2, SLC7A5, SLC3A2, LDHB, and HPRT1 as potential prognostic markers and correlate with immune infiltrates in head and neck squamous cell carcinoma. Front Immunol. (2022) 13:955614. doi: 10.3389/fimmu.2022.955614
15. Li T, Fu J, Zeng Z, Cohen D, Li J, Chen Q, et al. TIMER2.0 for analysis of tumor-infiltrating immune cells. Nucleic Acids Res. (2020) 48:509–14. doi: 10.1093/nar/gkaa407
16. Chandrashekar DS, Bashel B, Balasubramanya AKH, Creighton CJ, Ponce-Rodriguez I, Chakravarthi BVSK, et al. UALCAN: a portal for facilitating tumor subgroup gene expression and survival analyses. Neoplasia. (2017) 19:649–58. doi: 10.1016/j.neo.2017.05.002
17. Chandrashekar DS, Karthikeyan SK, Korla PK, Patel H, Shovon AR, Athar M, et al. UALCAN: an update to the integrated cancer data analysis platform. Neoplasia. (2022) 25:18–27. doi: 10.1016/j.neo.2022.01.001
18. Cerami E, Gao J, Dogrusoz U, Gross BE, Sumer SO, Aksoy BA, et al. The cBio cancer genomics portal: an open platform for exploring multidimensional cancer genomics data. Cancer Discov. (2012) 2:401–4. doi: 10.1158/2159-8290.CD-12-0095
19. Gao J, Aksoy BA, Dogrusoz U, Dresdner G, Gross B, Sumer SO, et al. Integrative analysis of complex cancer genomics and clinical profiles using the cBioPortal. Sci Signal. (2013) 6:l1. doi: 10.1126/scisignal.2004088
20. Qin Y, Conley AP, Grimm EA, Roszik J. A tool for discovering drug sensitivity and gene expression associations in cancer cells. PLoS One. (2017) 12(4):e0176763. doi: 10.1371/journal.pone.0176763
21. Vasaikar SV, Straub P, Wang J, Zhang B. Linkedomics: analyzing multi-omics data within and across 32 cancer types. Nucleic Acids Res. (2018) 46:956–63. doi: 10.1093/nar/gkx1090
22. Aran D, Hu Z, Butte AJ. Xcell: digitally portraying the tissue cellular heterogeneity landscape. Genome Biol. (2017) 18:220. doi: 10.1186/s13059-017-1349-1
23. Puram SV, Tirosh I, Parikh AS, Patel AP, Yizhak K, Gillespie S, et al. Single-cell transcriptomic analysis of primary and metastatic tumor ecosystems in head and neck cancer. Cell. (2017) 171:1611–1624.e24. doi: 10.1016/j.cell.2017.10.044
24. Zhai L, Ladomersky E, Lenzen A, Nguyen B, Patel R, Lauing KL, et al. IDO1 in cancer: a gemini of immune checkpoints. Cell Mol Immunol. (2018) 15:447–57. doi: 10.1038/cmi.2017.143
25. Conarty JP, Wieland A. The tumor-specific immune landscape in HPV+ head and neck cancer. Viruses. (2023) 15:1296. doi: 10.3390/v15061296
26. Struckmeier AK, Radermacher A, Fehrenz M, Bellin T, Alansary D, Wartenberg P, et al. IDO1 is highly expressed in macrophages of patients in advanced tumour stages of oral squamous cell carcinoma. J Cancer Res Clin Oncol. (2023) 149:3623–35. doi: 10.1007/s00432-022-04277-7
27. Seppälä M, Halme E, Tiilikainen L, Luukkainen A, Laranne J, Rautiainen M, et al. The expression and prognostic relevance of indoleamine 2,3-dioxygenase in tongue squamous cell carcinoma. Acta Otolaryngol. (2016) 136:729–35. doi: 10.3109/00016489.2016.1152631
28. Sailer V, Sailer U, Bawden EG, Zarbl R, Wiek C, Vogt TJ, et al. DNA methylation of indoleamine 2,3-dioxygenase 1 (IDO1) in head and neck squamous cell carcinomas correlates with IDO1 expression, HPV status, patients’ survival, immune cell infiltrates, mutational load, and interferon γ signature. EBioMedicine. (2019) 48:341–52. doi: 10.1016/j.ebiom.2019.09.038
Keywords: head and neck squamous cell carcinoma, IDO1, immune cells, prognostic marker, immune checkpoint
Citation: Gkountana GV, Wang L, Giacomini M, Hyytiäinen A, Juurikka K, Salo T and Al-Samadi A (2024) IDO1 correlates with the immune landscape of head and neck squamous cell carcinoma: a study based on bioinformatics analyses. Front. Oral. Health 5:1335648. doi: 10.3389/froh.2024.1335648
Received: 9 November 2023; Accepted: 12 April 2024;
Published: 26 April 2024.
Edited by:
Daniel Lambert, The University of Sheffield, United KingdomReviewed by:
Vui King Vincent-Chong, University at Buffalo, United States Samapika Routray, All India Institute of Medical Sciences Bhubaneswar, India© 2024 Gkountana, Wang, Giacomini, Hyytiäinen, Juurikka, Salo and Al-Samadi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ahmed Al-Samadi YWhtZWQuYWwtc2FtYWRpQGhlbHNpbmtpLmZp
†These authors have contributed equally to this work