 Moréniké Oluwátóyìn Foláyan1,2*
Moréniké Oluwátóyìn Foláyan1,2* Francisco Ramos-Gomez3
Francisco Ramos-Gomez3 Olawunmi Adedoyin Fatusi4
Olawunmi Adedoyin Fatusi4 Nouran Nabil5
Nouran Nabil5 Germana V. Lyimo6
Germana V. Lyimo6 Irene Kida Minja7
Irene Kida Minja7 Ray M. Masumo8
Ray M. Masumo8 Nadia Mohamed9
Nadia Mohamed9 Nicoline Potgieter9
Nicoline Potgieter9 Cleopatra Matanhire10Pamela Maposa11Chiedza Runyararo Akino10Abiola Adeniyi12
Cleopatra Matanhire10Pamela Maposa11Chiedza Runyararo Akino10Abiola Adeniyi12 Simin Z. Mohebbi13
Simin Z. Mohebbi13 Passent Ellakany14
Passent Ellakany14 Jieyi Chen15
Jieyi Chen15 Rosa Amalia16
Rosa Amalia16 Alfredo Iandolo17
Alfredo Iandolo17 Faizal C. Peedikayil18Athira Aravind18
Faizal C. Peedikayil18Athira Aravind18 Ola B. Al-Batayneh19,20
Ola B. Al-Batayneh19,20 Yousef S. Khader21
Yousef S. Khader21 Sadeq Ali Al-Maweri22
Sadeq Ali Al-Maweri22 Wael Sabbah23
Wael Sabbah23 Roberto Ariel Abeldaño Zuñiga24,25
Roberto Ariel Abeldaño Zuñiga24,25 Ana Vukovic26Julijana Jovanovic26
Ana Vukovic26Julijana Jovanovic26 Ro’aa Mohammed Jafar27
Ro’aa Mohammed Jafar27 Ilze Maldupa28
Ilze Maldupa28 Arheiam Arheiam29
Arheiam Arheiam29 Fausto M. Mendes29Sergio E. Uribe28,30,31
Fausto M. Mendes29Sergio E. Uribe28,30,31 María del Carmen López Jordi32
María del Carmen López Jordi32 Rita S. Villena33Duangporn Duangthip34
Rita S. Villena33Duangporn Duangthip34 Nadia A. Sam-Agudu35,36,37
Nadia A. Sam-Agudu35,36,37 Maha El Tantawi2,38
Maha El Tantawi2,38
- 1Department of Child Dental Health, Obafemi Awolowo University, Ile-Ife, Nigeria
- 2Oral Health Initiative, Nigerian Institute of Medical Research, Yaba, Nigeria
- 3Division of Preventive and Restorative Oral Health Sciences, UCLA School of Dentistry, Los Angeles, CA, United States
- 4Department of Oral and Maxillofacial Surgery, Obafemi Awolowo University, Ile-Ife, Nigeria
- 5Department of Pediatric Dentistry and Dental Public Health, Faculty of Dentistry, Alexandria University, Alexandria, Egypt
- 6Department of Dentistry, Muhimbili National Hospital, Dar es Salaam, Tanzania
- 7Department of Restorative Dentistry, Muhimbili University of Health and Allied Sciences, Dar es Salaam, Tanzania
- 8Department of Community Health and Nutrition, Tanzania Food and Nutrition Centre, Dar es Salaam, Tanzania
- 9Department of Paediatric Dentistry, Faculty of Dentistry, University of the Western Cape, Cape Town, South Africa
- 10Department of Oral Health, University of Zimbabwe, Harare, Zimbabwe
- 11Department of Paediatrics, University of Zimbabwe, Harare, Zimbabwe
- 12School of Policy and Global Affairs, Fairleigh Dickinson University, Vancouver, BC, Canada
- 13Department of Community Oral Health, School of Dentistry, Tehran University of Medical Sciences, Tehran, Iran
- 14Department of Substitutive Dental Sciences, College of Dentistry, Imam Abdurrahman Bin Faisal University, Dammam, Saudi Arabia
- 15Guanghua School of Stomatology, Hospital of Stomatology, Sun Yat-sen University, Guangzhou, China
- 16Department of Preventive and Community Dentistry, Faculty of Dentistry, Universitas Gadjah Mada, Yogyakarta, Indonesia
- 17Department of Endodontics, Faculty of Dentistry, University of Salerno, Salerno, Italy
- 18Department of Pediatric and Preventive Dentistry, Kannur Dental College, Anjarakandy, India
- 19Department of Orthodontics, Pediatric and Community Dentistry, College of Dental Medicine, University of Sharjah, Sharjah, United Arab Emirates
- 20Department of Preventive Dentistry, Faculty of Dentistry, Jordan University of Science and Technology, Irbid, Jordan
- 21Department of Public Health and Community Medicine, Jordan University of Science and Technology, Irbid, Jordan
- 22College of Dental Medicine, QU Health, Qatar University, Doha, Qatar
- 23Faculty of Dentistry, Oral & Craniofacial Sciences, King’s College London, London, United Kingdom
- 24Postgraduate Department, University of Sierra Sur, Oaxaca, Mexico
- 25Centre for Social Data Science, Faculty of Social Sciences, University of Helsinki, Helsinki, Finland
- 26Clinic for Pediatric and Preventive Dentistry, School of Dental Medicine, University of Belgrade, Belgrade, Serbia
- 27Department of Pediatric Dentistry, University of Khartoum, Khartoum, Sudan
- 28Department of Conservative Dentistry and Oral Health, Riga Stradins University, Riga, Latvia
- 29Department of Dental Public Health and Preventive Dentistry, Faculty of Dentistry, University of Benghazi, Benghazi, Libya
- 30School of Dentistry, Universidad Austral de Chile, Valdivia, Chile
- 31Baltic Biomaterials Centre of Excellence, Headquarters at Riga Technical University, Riga, Latvia
- 32School of Dentistry, University of la Republica, Montevideo, Uruguay
- 33Department of Pediatric Dentistry, School of Dentistry, University San Martin de Porres, Lima, Perú
- 34Faculty of Dentistry, The University of Hong Kong, Hong Kong, Hong Kong SAR China
- 35International Research Center of Excellence, Institute of Human Virology Nigeria, Abuja, Nigeria
- 36Institute of Human Virology, University of Maryland School of Medicine, Baltimore, MD, United States
- 37Department of Paediatrics and Child Health, University of Cape Coast School of Medical Sciences, Cape Coast, Ghana
- 38Department of Pediatric Dentistry and Dental Public Health, Faculty of Dentistry, Alexandria University, Alexandria, Egypt
Background: Child neglect is a public health, human rights, and social problem, with potentially devastating and costly consequences. The aim of this study was to: (1) summarize the oral health profile of children across the globe; (2) provide a brief overview of legal instruments that can offer children protection from dental neglect; and (3) discuss the effectiveness of these legal instruments.
Methods: We summarized and highlighted the caries profile and status of implementation of legislation on child dental neglect for 26 countries representing the World Health Organization regions: five countries in Africa (Nigeria, South Africa, Sudan, Tanzania, Zimbabwe), eight in the Americas (Argentina, Brazil, Canada, Chile, Mexico, Peru, Unites States of America, Uruguay), six in the Eastern Mediterranean (Egypt, Iran, Libya, Jordan, Qatar, Saudi Arabia), four in Europe (Italy, Latvia, Serbia, United Kingdom), two in South-East Asia (India and Indonesia) and one country (China) with its special administrative region (Hong Kong) in the Western Pacific.
Results: Twenty-five of the 26 countries have legal instruments to address child neglect. Only two (8.0%) of these 25 countries had specific legal instruments on child dental neglect. Although child neglect laws can be interpreted to establish a case of child dental neglect, the latter may be difficult to establish in countries where governments have not addressed barriers that limit children's access to oral healthcare. Where there are specific legal instruments to address child dental neglect, a supportive social ecosystem has also been built to facilitate children's access to oral healthcare. A supportive legal environment, however, does not seem to confer extra protection against risks for untreated dental caries.
Conclusions: The institution of specific country-level legislation on child dental neglect may not significantly reduce the national prevalence of untreated caries in children. It, however, increases the prospect for building a social ecosystem that may reduce the risk of untreated caries at the individual level. Social ecosystems to mitigate child dental neglect can be built when there is specific legislation against child dental neglect. It may be more effective to combine public health and human rights-based approaches, inclusive of an efficient criminal justice system to deal with child dental neglect.
Introduction
Child neglect is a public health, human rights, and social problem, with potentially devastating and costly consequences (1). Globally, it is estimated that up to one billion children aged 2–17 years have experienced physical, sexual, or emotional violence or neglect in the previous 12 months (2). The actions or inactions of parents, caregivers and other authority figures resulting in the neglect of children and adolescents are classified as maltreatment (3). Child maltreatment or neglect result in neurological and biological events that have a negative impact on physical and behavioral health and have academic and economic consequences (4).
One such physical health consequence of child maltreatment or neglect is poor oral health. Oral health is vital for the overall health and well-being of children (5), and it is recommended that they have annual dental visits to receive oral screening and risk assessment with timely and comprehensive preventive dental care planned according to assessed risk (6). Children with oral diseases also need dental clinic visits for disease management to ensure freedom from pain and infection (7). Caries is an important oral disease; untreated caries in primary teeth and permanent teeth affect 621 million children and 2.4 billion people, respectively, worldwide (8). Untreated caries negatively impacts quality of life for children, affecting their ability to learn, play, eat and sleep. Severe caries can contribute to failure to thrive and limits children's ability to live a fulfilling and productive life (9–15). Parents and other caregivers are guilty of dental neglect when they fail to pursue the dental care required to maintain their child's oral health (7).
Dental health professionals in countries like the United Kingdom are required to ensure that all children and adolescents have access to preventive dental care and treatment for oral disease and injury, to mitigate the risk of dental neglect (16). This is important, because a case of dental neglect can be made if a parent persistently fails to obtain treatment for their child's dental caries when such dental services are available (17). While there is no evidence to suggest a specific threshold of oral disease to diagnose dental neglect, a case of dental neglect can be made when there are features of a lack of basic oral care, including oral hygiene, failure to seek treatment for oral pain, and leaving infections untreated (17).
Neglect is often dictated by culture [ways of thinking, feeling and behavior that are socially and not biologically transmitted from one generation to the next (18)], tradition, religion and familial norms that influence home life, parenting practices, and upbringing. This makes what is considered neglect highly context-specific and often controversial, with socio-economic status adding another layer of complexity. While the influence of culture on child-rearing practices has been well studied (19, 20), there is little known about how cultural nuances may influence perceptions of child neglect and its impact on child oral health. Irrespective of cultural nuances, official recognition of dental neglect as a form of child neglect raises the profile of child oral health in the public health agenda (16), potentially resulting in the institution of legal instruments to reduce the risk of child dental neglect.
The aim of this study was to: (1) summarize the oral health profile of children in different countries across the globe; (2) provide a brief overview of existing legal instruments that can offer (or have offered) protection for children from dental neglect; (3) examine limitations on implementation of these legal instruments, which criminalize child dental neglect; and (4) discuss facilitating actions to reduce the risk of children's exposure to dental neglect.
Methods
This narrative review presents country-level status quos regarding child dental neglect, using series of case studies with varying contextual backgrounds. For this study, we broadly define policy as government actions in response to societal issues, specifically focusing on child dental neglect and poor oral health in children. These policies may take the form of regulations, rules, or administrative codes with the force of law, and may be based on statutory interpretations (21, 22). We also recognize that policies pertaining to child neglect serve as social (protective) regulatory guidelines that establish boundaries for permissible behavior within their jurisdictions (23). We centered our attention on the policy analysis stage of the policy-making process, as outlined by Dunn (24) and Howlett and Ramlesh (25). The objective was to assess policies, identifying any potential issues, to provide further guidance (26).
To achieve this, we have compiled a summary of legislations on child dental neglect from 26 countries representing the World Health Organization (WHO) regions: five countries in Africa (Nigeria, South Africa, Sudan, Tanzania, Zimbabwe), eight in the Americas (Argentina, Brazil, Canada, Chile, Mexico, Peru, Unites States of America, Uruguay), six in the Eastern Mediterranean (Egypt, Iran, Libya, Jordan, Qatar, Saudi Arabia), four in Europe (Italy, Latvia, Serbia, United Kingdom), two in South-East Asia (India and Indonesia) and one country and its special administrative region in the Western Pacific (China and Hong Kong). We adopted a case-study method of policy analysis (27), which allows the contextualization of problem definition and sheds light on issues relevant to policy-setting based on real life conditions. By presenting case studies from countries with different cultural, economic, social, and healthcare backgrounds, we highlight contrasting approaches to address the same problem: child dental neglect. Although the available literature about the extent of dental neglect and relevant policies is too sparse for hypothesis generation, we theorize that countries with developed health and social care systems have well-defined policies to address child dental neglect. This theory guides the selection of case studies from countries in all WHO regions since it is the global authority on healthcare policy recommendations.
The summary of legislations on child dental neglect for each country was compiled by conveniently selected country experts who understood both the legal context of child dental abuse and the magnitude of oral health problems in their respective countries. The primary consideration for selecting each country expert was a history of publication on country-specific oral health problems. Each country expert was required to conduct a search of databases (PubMed, Scopus, PsycINFO, and CINAHL) for studies and documents on the prevalence of oral diseases (caries, periodontal diseases) and caries risk behaviors (oral hygiene status and history of dental service utilization), and on child neglect and child dental neglect. A search of grey literature was also conducted. The findings were synthesized and summarized into a table. The summary for each country was organized into their respective WHO regions (the Americas, Eastern Mediterranean, African, European, South East Asian, and the Western Pacific regions).
The commonalities and differences within and between regions were reported. The links between the presence (or absence) of policies and the prevalence of oral diseases (specifically dental caries) was addressed. Dental caries was selected because it is the only childhood oral disease with globally available data that allows for standardized between inter-country comparison. The dental caries analysis was based on the Global Burden of Disease studies used in the 2022 WHO Global Oral Health Status Report. Findings were discussed, and proposals were made for policy changes to effectively address child dental neglect.
Results
African region
Nigeria
In Nigeria, the burden of untreated caries in children is a cause for concern, as the prevalence of untreated caries is high (28). The prevalence of poor oral hygiene ranges from 0.2% in 1–5-year-olds to 4.4% in 6–12-year-olds (29); and for gingivitis ranges from 63.3% in 6–11-year-olds (30) to 57.2% in 10–19-year-olds (31). Untreated caries in children is over 80% and results from poor uptake of oral health services for several reasons, ranging from high out-of-pocket expenditure and poor insurance coverage for oral healthcare (32), low socioeconomic status (33), low level of maternal education (34), perceiving hospital visits as synonymous with need for curative care (35), poor perception of the need for oral health care (36), to rurality and a complex oral health system that is difficult to navigate (37).
The 2003 Child's Right Act guarantees the rights of children in Nigeria (38), and the National Human Rights Commission undertakes actions to promote and protect the rights of children from fetus to 17-years of age (39). Section 2 (1 and 2), and Section 13 (1 and 2) of the Act recognize the right of children to health. Section 13 (5a and 5b) place the liability of child oral health care on caregivers, punishable with a fine for the first offence and a one-month imprisonment for a second offence. The Act does not explicitly mention child dental neglect as a criminal offence.
Section 13 subsections 3b and 3g, however, create a leeway to exonerate caregivers from an offence of child (dental) neglect by indicating that the government has the responsibility to provide medical assistance and health care services to all children through the development of primary health care services. However, the government only provides dental care through 27 (0.08%) of the 33,156 primary health care centers in Nigeria (40, 41), which indicates severely limited access to dental care in the country. In addition, dental care is expensive (42), health insurance coverage is low and extremely limited for oral health care-almost to the exclusion of preventive oral health care services (37)- and human resources for oral health care are scarce (42, 43). These gaps make it difficult to establish a charge of child dental neglect in Nigeria. In addition, most dentists in Nigeria do not screen for dental neglect (44), only 51.3% recognize neglect as a form of child abuse (45), and only 14.1% of those who suspect child abuse and neglect file reports to social services (44). To date, there has been no legal prosecution of a case of child dental neglect in Nigeria.
South Africa
Early Childhood Caries (ECC) is a significant public health problem in South Africa, with prevalence reaching 60% in 2004, which is the most recent estimate (46). The prevalence of ECC had increased to 71.6% in 2018 for children resident in low socioeconomic communities, of whom 70% need dental treatment (47). Parents are responsible for their child's basic needs, including diet, personal hygiene, and access to health care, and therefore play an important role in preventing dental disease in their children. The high rates of untreated caries and extractions may be pointers to child neglect, though this needs to be contextualized.
South Africa has a population of approximately 60 million people, of whom 9.4% are 5 years and younger, and 28% are 15 years and younger (48). The South African population is diverse in socioeconomic status, living conditions, access to health care and quality education, and therefore, diverse in caries risk (49). Although 71.9% of households access public clinics, only 16.1% have medical aid (50). Limited access to oral health care results in high prevalence of untreated caries with many children requiring multiple extractions under dental general anesthesia (51).
Dental practitioners are trained to be sensitive towards inequalities and to differentiate between ignorance, lack of education, limited access to oral health care and dental neglect. Section 110 (1) of the Children's Act (No 38 of 2005) (52) states that if there is a reasonable suspicion (on the part of treating professionals) that a child is being abused in a way that causes physical injury, sexual abuse or neglect, this must be reported. A range of professions including legal practitioners, medical and dental practitioners, traditional and religious leaders, psychologists, social workers, teachers and persons working in care facilities, are empowered to report neglect to a social worker, a designated child protection unit or organization or to the police [Section 110 (2)]. The Children's Amendment Act (2007) (53) is more detailed and provides psychosocial, rehabilitation and therapeutic services for neglected children. The South African law is, however, not specific on child dental neglect.
Sudan
There are 17 states in Sudan. However, data about the prevalence of dental caries, and decayed, missing, and filled teeth (DMFT) values are available only in the three states of Khartoum, Kassala and Gazeerah. The prevalence of caries in children and adolescents is very high, and ranges from 70.9% (54) to 91.1% (55).
The Sudanese's Child Act (2010) (56) is housed by the Ministry of Justice and addresses the rights of children with respect to nutrition and breastfeeding, immunization, physical and mental health, and protection of children from infectious diseases and physical and sexual exploitation. There are also chapters on the right of children to education, and the rights of vulnerable children. However, to date, there is no legislation to protect the Sudanese child from dental neglect. There are currently no studies investigating the prevalence, knowledge, causes and types of dental neglect in Sudan.
Tanzania
In Tanzania, more than 3 in 10 children have experienced dental caries (57), and 5-year-old children have higher dental caries experience than 12 and 15-year-olds, with the decay component accounting for 99% of the total caries experience (57). Also, 57.4% of 12 and 15-year-olds have gingivitis and 4.4% have experienced dental trauma, with more children affected in rural than urban areas (65.2% vs. 52.0% and 5.7% vs. 2.7% respectively) (57).
Tanzania is a signatory to the 1989 Convention on the Rights of the Child and the 1990 African Charter on the Rights and Welfare of the Child. In 2009, Tanzania enacted the Law of the Child Act to accommodate the requirements of International Legal Frameworks on the protection of children (58). Section 4 (2) of the Act insists that the best interest of a child should be the primary consideration in all actions taken with respect to children. Section 9 (1) provides that parents, guardians and relatives are responsible for ensuring children's right to life, dignity, respect, leisure, liberty and health. Section 13 (1) prohibits degrading treatment to children, and institutions like local government authorities and police are vested with the legal duty to ensure children's safety. Despite the enactment of the Law of the Child Act, child neglect is still a serious problem in Tanzania (57). The 2020 UNICEF report noted that many children in Tanzania experience violence, neglect, and exploitation (59). There is no enforcement mechanism to monitor children's protection.
Efforts to strengthen the 2009 Child Act have not been sufficient to address dental neglect in children. Strategies to improve the knowledge and awareness of caregivers toward children's daily oral health practices and correct feeding habits are essential in addressing dental neglect in Tanzania (60). Furthermore, tailored public education programs addressing dental neglect and building the competency of oral health personnel to detect and manage dental neglect are needed.
Zimbabwe
The caries prevalence of 12-year-olds has increased from 27.6% in urban areas and 20.9% in rural areas in 1989 (61), to 59.5% among urban and 40.8% among rural children in 2013 (62). Furthermore, 65.2% of carious teeth are untreated and 34.8% are missing (63). The instituted school-based oral health programs responsible for tackling oral health problems in children attending primary and secondary schools (64) have limited effectiveness (65). Many children present with untreated carious lesions that their parents have the responsibility to manage.
Zimbabwe adopted the Children's Act (Chapter 5:06) in 2001 to domesticate several international treaties on childcare and protection it was a signatory to. The Act states that a parent or guardian of a child or young person shall be deemed to have abandoned or neglected that child or young person if (s)he …(b) failed to provide or pay for dental, medical, or surgical aid or other effective remedial care necessary for his/her health or well-being. The Act is enforced by the Victim Friendly Unit of the Zimbabwe Republic Police which works closely with hospital police posts or police stations to handle reported cases of child abuse. Currently, there is no stand-alone legislation on child dental neglect.
The effectiveness of the Children's Act to deal with child dental neglect is currently limited, as there are no defined parameters to identify cases of child dental neglect in the country. No parameters that define child dental neglect and abuse have been declared to the public and health service providers, and cases remain undetected and unassisted. In addition, the curriculum of undergraduate and postgraduate dental students does not cover this aspect of childcare.
Region of the Americas
Argentina
In 1985, 40% of children aged 7% and 68% of children aged 13 years had caries in permanent teeth (66). By 2010, caries was reported in 49% of 4-year-old children, of which only 10% had treatment (67). In 2019, 70% of children had caries (68, 69).
Argentina ratified the International Convention on the Rights of the Child in 1990. The International Convention on the Rights of the Child led to the incorporation of Article 75 into the new Constitution of the Argentine Nation, and the 2005 National Law 26,061 on Comprehensive Protection of the Rights of Girls, Boys and Adolescents. The 2005 National Law establishes that “Girls, boys and adolescents have the right to comprehensive health care, to receive the necessary medical assistance and to have equal access to opportunities for services and actions for prevention, promotion, information, protection, early diagnosis, timely treatment and recovery of health” (70). In 2017, the Oral Prevention and Primary Assistance Program was created, through Resolution 440-E/2017 of the Ministry of Health, but it does not have the force of Law.
Greater emphasis is placed on addressing the increasing violence in schools, societal fragmentation, and inequalities than on addressing oral health problems. This leads to the neglect of oral health (71), which, if addressed, should reduce the burden of oral diseases in children. However, children's oral health continues to be a public health problem despite the presence of relevant legislation, and epidemiologic indicators reflect this.
Brazil
Preliminary results obtained from 25% of the required sample of the ongoing Brazilian Oral Health Epidemiological Survey indicates that prevalence of caries in the permanent dentition is 49.2% and 50.7% in the primary dentition (72). Also, the mean number of teeth with untreated caries was 1.82 for 5-year-olds and 1.04 for 12-year-olds (72). The prevalence of caries in the permanent dentition has decreased over the years. However, this same trend has not been observed for primary dentition.
Child neglect is addressed through the Child and Adolescent Statute (ECA—Estatuto da Criança e do Adolescente), a federal law created in 1990 to establish the right and protections of Brazilian children and adolescents (73). The ECA states that the Brazilian public health system (SUS—Sistema Único de Saúde) must promote general and oral health care programs focusing on the most prevalent diseases affecting children (73). The ECA also notes that the family, community, and government should ensure that children have access to oral health care. Oral health care should be promoted for pregnant women and children through education and prevention before the child's birth, and when the children are 6 and 12 years of age. Furthermore, the cost of treatment for children with dental treatment needs should be covered by the SUS.
In 2004, the Brazilian Policy of Oral Health was created and promoted the reorganization of primary health care by expanding oral health teams, the family health strategy and creating dental specialty centers (74). However, the program has been criticized due to the poor coverage of children with oral health needs, emphasis on operative treatment, and lack of trained professionals, mainly for children requiring complex dental treatments. These problems can be ascribed to the low utilization of dental services: only 25% of preschool children make use of these services (75). Dental caries indicators for primary teeth have not improved in the last decade (72, 76, 77).
Canada
Untreated dental caries and untreated dental trauma are two examples of reportable dental neglect among children in Canada (78). The 2007–2009 National Oral Health Survey indicated that 56.8% of 6–11-year-old Canadian children had dental caries, with untreated carious lesions accounting for 14.7% of all reported cases (79). Low-income (17.6%) and uninsured families (19.1%), those who had not visited a dentist in the previous 12 months (30.9%), and families with low levels of education (18.9%) had more untreated caries than better-off subgroups with various socio-demographic characteristics (79). Among adolescents, caries prevalence was 59.8%, the proportion of untreated caries was very low, with higher prevalence among those from lower, than higher income groups by more than threefold (80). Among children of Indigenous descent, nearly half of the caries lesions in preschool children were untreated (80). The reasons caregivers delay dental treatment are mainly because of their inability to pay for dental care and the perception that primary teeth will eventually be lost (81).
When a parent fails to act after being properly informed about the nature of their child's oral health problem and the specific treatment required, this is considered negligence and requires intervention. There are laws at the federal and provincial levels in Canada that provide the legal framework to address child dental neglect. The law requires that dentists report dental neglect only after questioning the child and the parent separately about the clinical presentation, with a staff member present to act as a witness (82).
There are several agencies in Canada that can receive and investigate reports of dental neglect. These include the local Royal Canadian Mounted Police, municipal police station, and the government ministry in charge of child and family welfare. Provincial and territorial legislations have been helpful in early detection and intervention for child neglect in Canada (83). However, there is little evidence to assess their effectiveness in addressing child dental neglect.
Chile
Chile has a favorable children's rights environment, scoring 9.22 out of 10 and receiving a “green” classification (84). The estimated prevalence of untreated caries in the primary dentition among Chilean children aged 1–9 years is 46.6% (85), with a higher prevalence in rural areas (86). Also, the prevalence of dental trauma [37.95% (87)] and malocclusions [38%–53% (88),] are high.
Chile's does not have a specific law focusing on comprehensive child rights protection. Instead, it relies on the Intersectoral System of Social Protection (Chile Solidario), which includes the Chile Grows with You (CGY, Chile Crece Contigo) program (89). Established in 2006, CGY is a comprehensive program that supports early childhood education, child health and nutrition services, family support, and social protection through coordination between various ministries and institutions, such as the Ministry of Social Development and Family, the Ministry of Health, the Ministry of Education, and the National Board of Kindergartens (89). It incorporates an oral health component called “Oral Health in Your Life” (Salud Oral en tu Vida), promoting good oral health habits among pregnant women, infants, and children up to four years old through education and preventive services (90). The creation of the Children's Ombudsman Office (Defensoría de la Niñez) in 2018 strengthened Chile's commitment to safeguarding children's rights (90).
In addition, Chile has implemented several policies using a common risk approach to address sugar consumption, which contributes to dental neglect. These policies include a tax on sugary drinks containing more than 6.25 g of sugar per 100 ml (91). The allowable amount of sugar in foods without warning labels has also been reduced from 22.5 g per 100 g to 10 g per 100 g. In 2016, the Law of Food Labeling and Advertising was enacted. This requires front-of-package warning labels, restricts child-directed marketing, and bans sales in schools of all foods and beverages containing added sugars, sodium, or saturated fats that exceed set nutrient or calorie thresholds (91). The government also covers the cost for essential curative (but not preventive) oral health care for six-year-old children through the Explicit Health Guarantees. This is, however, a counterproductive program as children already have dental caries at a much younger age and need care much earlier: 80% of two-year-olds have dental caries, and the provision of oral health care at a later age does not align with the strategies of the Oral Health Department of the Chilean Health Ministry which aims to have at least, 80% are children been caries-free (92). These actions are all together complex and make it difficult to establish cases of child dental neglect in Chile.
Mexico
Caries has been a growing problem over the last 30 years in Mexico, with the current prevalence of caries estimated to range between 80% and 90%, and at least 10 million children between 2 and 5 years of age having caries (93, 94).
The Convention on the Rights of the Child (95), the American Convention on Human Rights (96) and the General Law on Human Rights of Girls, Boys and Adolescents (97) establishes the obligation of the Mexican State to guarantee the right to health of people younger than 18 years of age. This broad legal framework recognizes three guiding principles that the Mexican state must consider in relevant actions: non-discrimination, superior interest, and recognition of evolutionary capacities, in accordance with their interests and needs. Likewise, the General Health Law establishes the right to protect the health of the population, through actions to promote health, disease prevention and control, among others (98). Neglect is criminalized through the Comprehensive Care Clinic for Abused Children of the National Institute of Paediatrics that defines child abuse as “any aggression or intentional omission, whether physical, sexual, psychological, or negligent, within or outside the home, against a minor, before or after birth, that affects their biopsychosocial integrity, regularly or occasionally carried out by a person, institution or society, based on their physical, intellectual or economic superiority” (99). Parents and children's guardians are responsible for ensuring the health of their children or wards. However, Mexico is a country of profound social inequalities, with 28.6% of children never having contact with a dentist. This poor dental service utilization is associated with indicators of socioeconomic status and reflects inequality in dental service access (100, 101). The challenges that government face in addressing inequality in dental service access makes the case of child dental neglect difficult to establish in Mexico.
Peru
Peru is promoting a reform process that supports achieving universal health coverage. Since 2015, health insurance enables pregnant women and children up to five years of age to access free health care. When there is no health insurance, the newborn is automatically affiliated with the Comprehensive Health Insurance (SIS) regardless of their socioeconomic status.
The last national study (2001–2002) of the Ministry of Health that was carried out in children 3 to 15 years old showed a prevalence of dental caries ranging from 57.6% to 63.5% with a mean of 60.5% in the primary dentition, and from 56.2 to 65.1% with an mean of 60.6% in the permanent dentition. 10 years later, an unpublished 2012–2014 national study conducted by the National Epidemiology Center of the Ministry of Health found very similar values without significant differences in both dentitions. The data is similar to that reported for the Americas by the WHO in 2022 (102, 103).
In 2017, a Ministerial Decree modified the Technical Health Standard for the Control of Growth and Development of children under 5 years of age. The modification included a provision that the health professional (nurse, pediatrician, or general practitioner), would review the child's mouth by age one year, and all children should be checked by a dentist before one year of age. However, there is no national dental program with well-defined guidelines for monitoring child oral health. Also, although Peruvian law 30364 (104) promotes protection against violence affecting women and children, there is no specific rule that recognizes poor child oral health as an act of neglect. There is also low uptake of dental health services in the population under 12 years of age (105), and a lack of training and integration of child oral care into multidisciplinary practices. There are however good intentions to address these gaps in order to achieve established universal health goals.
United States of America
Although completely preventable, ECC is currently the most common chronic disease in children from the United States of America, and its prevalence continues to be high in poor and near-poor children of preschool age (106, 107). Furthermore, socially disadvantaged children are less likely to have access to oral health care, instead seeking care for oral infections from emergency departments and hospitals (108).
Parents must be informed by a health care provider about the necessity of oral health care for their child, their child's oral health status, the treatment required, and how to access that treatment (109). Since some caregivers may, however, be unaware of their children's need for dental care, it is important to differentiate between a lack of oral health literacy and willful failure to seek care when determining whether a situation qualifies as dental neglect (110). Also, there are several barriers that may interfere with parents seeking appropriate oral health care for their child (110–112). If a provider has ascertained that the parent understands what dental care their child needs and how to obtain it, and the above factors still indicate a case of dental neglect, the provider should report the case to the appropriate child protection services agency (109).
It is important that health care providers from all disciplines are aware of signs that indicate child abuse and/or neglect (109). The American Association of Pediatric Dentistry states that all health care providers, including dental providers. are expected according to local or state requirements to report injuries that cause concern for abuse or neglect to child protective services (108). Additionally, they are encouraged to collaborate with interprofessional colleagues to provide support for affected families (109).
Uruguay
The prevalence of dental caries is high, and worse among those with low socioeconomic status: in the poorest populations the rate of caries disease is five to eight times higher. The DMFT among 12-year-olds is 4.2–4.7 in the most deprived areas, and 2.5 among those with high socioeconomic status (113). Among adolescents, 60% of those with high socioeconomic status are caries-free, while only 11% of those with low socio-economic status are (114). A study conducted in 2017 (115) indicated that most children have active untreated cavitated lesions, possibly due to poor access to timely care, and that if the approximately 25% of 5-year-old children with non-cavitated lesions could have access to early treatment, cavitation, and complex and expensive treatments could be avoided.
The 2004 law 17.823 on children and adolescents (116) is applied through the National Integrated Health (SNIS) law 18.121 of December 2007, and implemented by the Ministry of Public Health ((117). The law articulates that public and private providers of comprehensive health care should ensure access to comprehensive health services for all residents in the country. Uruguay has a National School Oral Health Plan under the State Health Services Administration (ASSE-MSP) that serves around 75,000 children per year and develops a program for the prevention and minimal intervention with 430 dentists and two mobile clinics that operate throughout the country. However, the integration of dentistry into the general health system could be better, as that may facilitate detecting and addressing child dental neglect.
Eastern Mediterranean
Egypt
A 2014 nationwide survey indicated that nearly 70% of Egyptian children had untreated caries and about 80% had periodontal disease (118). In 2009, Egypt developed a national strategy to combat abuse, including activating laws, raising awareness, and establishing agencies to help victims of neglect (119). This was in response to articles 80 and 96 of the Egyptian constitution, which stipulate that the state shall care for children and protect them from all forms of neglect threatening their wellbeing (120). Alhough the Egyptian Law penalizes child neglect after receiving a warning notice (120, 121), the law does not criminalize the parental negligence of children.
The National Council for Childhood and Motherhood has a helpline for child complaints, and it provides counseling and referral services to victims of violence, abuse, and neglect. The Ministries of Health, Social Services and Interior, and non-governmental organizations are responsible for child protection (122). However, reports of neglect is low, due to poor public awareness of reporting mechanisms (123). In 2022, only 13.6% of citizens were aware of the presence of agencies supporting abuse victims, and 7.7% were aware of a hotline to report instances of neglect (124). Though dentists can play a role in diagnosing and managing child dental neglect, only 40% of dentists indicated ever suspecting abuse in their patients, despite learning about social indicators of child maltreatment in dental school (123, 125).
There is no law that mandates reporting of child maltreatment, and there is no penalty for non-reporting. Currently, only schoolchildren 6 to 18 years old have access to regular care covered by health insurance, and it is expected that this coverage will extend to preschool children when the Universal Health Insurance Law is fully applied at a national level (126). The persistence of untreated oral diseases in children with health insurance coverage and access to regular care should indicate dental neglect. However, limited parental literacy and poor oral health values (60) reduce the possibility that parents would be charged for dental neglect of children. In addition, no laws or guidelines specifically identify cases of dental neglect, and there is a paucity of information about the prevalence of child dental neglect.
Iran
The prevalence of dental caries in primary teeth among children in Iran has been on the increase in the last 28 years (127). The dmft index for 5–6-year-old children is 5.16, and 86.9% of it is related to the decay component. The DMFT index in 12-year-old children is 2.1, and 81.8% of this index is related to decayed teeth (127, 128). In Iran, child neglect is considered a social emergency (129). The Iranian welfare organization has specifically targeted children living on the streets, children who are working, and children who are abused and neglected, for priority interventions. The public is expected to place a call to the Social Emergency Department of Welfare (Behzisty) organization if anyone identifies a case of child abuse or neglect.
Article 4 of the Law on Protection of Children and Adolescents was approved in 2003. It states that any physical and mental harm or torture of children and neglect deliberately affecting their mental and physical health or preventing them from studying, is prohibited and punishable by imprisonment or a monetary fine. Also, Article 1173 of the Civil Law (amended 1998) can be invoked in case of non-observance of the child's physical health by parents (130). The Article states that when the physical health of the child is in danger due to a lack of care or moral degeneration of the father or mother under whose custody the child is, the court can take any decision deemed appropriate for the custody of the child upon the request of the child's relatives, guardian or the head of the jurisdiction.
Despite the law, only advanced and life-threatening mental or physical health problems are reported, with very low public sensitivity to dental neglect. The absence of local guidelines on child dental neglect has also complicated matters (131). The faculties in the School of Dentistry, Isfahan University of Medical Sciences and the Ministry of Health are developing evidence-based guidelines for the reporting of child abuse and neglect, including the reporting of child dental neglect by dentists. These guidelines will take a lot of resource investment to implement throughout the country. It is, however, a welcome development to complement the existing law for legally addressing child dental neglect in Iran.
Libya
The oral health care system is hybrid, composed of both public and private sectors. Although health care policy in Libya implies that free care should be provided to all, only few emergency services are provided in the public sector, and most of dental services are provided as fee-per-service in the private sector. Several studies have demonstrated highly unmet treatment needs among school children: 70% of 6-year-olds and 42% of 12-year-olds have untreated caries (132, 133). There is also a high level of unmet treatment needs related to dental trauma (134), dental fluorosis (135) and molar incisor hypo-mineralization (136).
Although professionalism and ethics are key subjects in the dental curricula in Libya, anecdotal evidence indicates that dental neglect does not receive much attention compared to other medicolegal topics. The Libyan law has clear legislation and guidance on how to deal with professional neglect that causes morbidity and mortality. However, there is no clear legislation that describes what should be done to protect children from domestic child neglect. There is also no national guidance on protecting the rights of children with dental neglect or other forms of health neglect. This calls for advocacy for these issues in Libya, in addition to strengthening dental curricula to build competency on the identification and management of dental neglect.
Jordan
Research on child dental neglect in Jordan is scarce. Parents have poor knowledge about their children's oral health, and parental opinion of their children's oral health status s overrated (137). There are currently no country-level legal instruments that specifically address child dental neglect in Jordan. However, children in Jordan have specific rights under the United Nations Convention on the Rights of the Child, to which Jordan is a signatory (138). In addition, the Jordanian constitution guarantees the right of the child to protection and the Draft Jordanian Child Rights Law provides comprehensive protection for the rights and well-being of all children residing in the country (139).
In addition, the government provides health insurance, which covers dental treatment for children under age six years (140). In 1991, Jordan ratified the Convention on the Rights of the Child (141). In 2011, the country added two new paragraphs to Article 6 of its Constitution, which state that “the law shall protect motherhood, childhood and the old-aged; and shall avail care for the youngsters and those with disabilities and protect them against abuse and exploitation” (142). Despite the existence of such legal instruments, there are limitations with their implementation, such as poor awareness of parental legal obligations to provide adequate dental care for children, limited access to dental care particularly in rural areas, lack of law enforcement systems to hold parents responsible for dental neglect, poor parental prioritization of dental care, and financial barriers. Therefore, it is necessary to increase awareness and legal obligations of parents to provide dental care through public education campaigns and by working with healthcare providers to promote oral health.
Qatar
The State of Qatar has a population of 2.7 million and has the six-highest GDP per capita in the world at the end of 2022 (https://www.visualcapitalist.com/cp/ranked-countries-gdp-per-capita-2023/). A significant shift in lifestyle and dietary habits due to rapid socioeconomic development has led to a marked increase in the prevalence of dental diseases, mainly dental caries, among children. The prevention, oral health promotion, early detection and treatment of dental diseases had been largely driven by the Primary Health Care Corporation that target high-risk groups, including pregnant women, infants, and school children. Oral health screening is provided to kindergarten and schoolchildren through the “Asnani School Oral Health Program”. Despite these efforts, the prevalence of dental caries among children is still high: 85% of 12–14-year-olds have caries, with the mean number of decayed teeth being 4.62 (143); 71.4% of 6-year-olds have caries with a mean dmft of 4.2 (144); and 89.2% of 4–5-year-olds have caries with dmft of 7.6 and dt of 7.1 (145). These findings suggest the presence of dental neglect and unsatisfactory oral health status.
Qatar adopted legislation to ensure child protection and to prevent abuse (146). The Qatari constitution states that: “The State shall provide care for the young and protect them from corruption, exploitation, and the evils of physical, mental and spiritual neglect” (147). The first child abuse protection program, the Sidra Child Advocacy Program (S-CAP), was established by Sidra Medicine to provide child abuse services by well-trained pediatricians and supporting staff. S-CAP includes safe, discreet facilities for conducting interviews, medical examinations, and creating medico-legal reports. Additionally, S-CAP established a child hotline for the public to report any suspected child abuse (148).
There are, however, no specific legal provisions related to child dental neglect. The extension of the current laws on child protection and the inclusion of child dental neglect in the mandate of S-CAP may further promote oral health among children, reduce the burden of dental disease and positively impact the wellbeing and quality of life of children in Qatar. The identification and reporting of dental neglect may, however, be difficult, due to challenges with identifying children who are dentally neglected (149), gaps in the knowledge of dentists regarding dental neglect, and the absence of a system for reporting child dental neglect.
The Kingdom of Saudi Arabia
The prevalence of dental caries in children has increased significantly, to almost 70% in the permanent dentition and 80% in the primary dentition (150, 151). The prevalence of complicated untreated dental caries among children is high, with up to 4 in 10 children visiting the dental clinic due to tooth ache resulting from caries (151, 152). Although dental care services are free, the prevalence of child dental neglect is high. Hospital-based reports of child abuse rose from 65 cases in 2008 to 73 cases in 2009, 80 cases in 2010 and 616 in 2011 (153). The reasons for this include low levels of parental education (154), poor perception of the need for oral health care, fear of dental treatment, lack of public transportation (155) and inability to obtain a dental appointment because of the long waiting lists (156). Also, working mothers may not have free time to visit the dental hospitals except for emergency care (157).
In Saudi Arabia, child neglect is an offense that must be reported. In August 2013, the law of protection from child abuse and neglect was enacted (158). The Ministry of Education also launched an awareness campaign online to provide information on early childhood care (159). As a part of this campaign, the Child Protection System, the policy of child protection against abuse or neglect and the ways of managing reports submitted to authorities were explained in detail (160). Dentists are responsible for identifying and reporting suspected cases of dental neglect to authorities (161). The police station is the certified agency for handling reports of child abuse and neglect. Police then refer certified cases to child protection teams to manage (158).
Despite the law, the reporting of child dental neglect by dentists is low, due to a lack of training (162). The lack of awareness about the referral process and responsible legal authorities reduces the number of reported cases (163). The competency of dentists to identify cases can be addressed by building additional training elements into the dental curricula to train students on identifying the following: signs and symptoms of neglect, documentation and reporting, the Saudi child protection policy, and the consequences of failure to report abuse and neglect for the child's oral and physical health, and behavioral and psychological development. Training has increased the reporting of child abuse and neglect cases by dentists in Saudi Arabia (164).
European region
Italy
Caries prevalence among 4-year-olds is 21.6% and 43.1% for 12-year-old children in Italy (165). In 2006, approximately 75% of 4-year-olds and 50% of 12-year-olds were reported to have more than one carious lesion, thus, requiring dental care (166).
Italy adopted a legislation to ensure child protection and abuse prevention. Article 572–591 of the Italian penal code states that: “Anyone who abandons and mistreats a person under the age of fourteen, or a person who is incapable, due to mental or physical illness, of providing for himself, and for whom he has custody or has to take care of, is punished with imprisonment from six months to 24 years.” The Office of the Guarantor Authority for Childhood and Adolescence oversees child projects and reported in its 2018–2020 investigation of 250 out of the 6,080 municipalities in Italy that out of every 1,000 resident minors, 45 were in the care of Social Services. Of the 401,766 children and young people in the care of Social Services, 77,493 (19.3%) had experienced some form of abuse. Twenty percent of these reported cases of abuse came from the hospital, the dentist, and the pediatrician (167).
There is no specific legislation or guideline on child dental neglect, nor are there screenings, reporting or management of child dental neglect in Italy. The 2018–2020 survey highlighted the need for instituting periodic monitoring systems to support the implementation of policies on prevention, protection, and treatment of abused minors (167). However, the current policy supporting children who survive child abuse seems not to have effectively addressed child dental neglect as a distinct form of child abuse despite evidence that child dental neglect is an indicator of child abuse.
Latvia
The estimated prevalence of untreated caries in primary teeth is 47.5%, and the prevalence of caries in the enamel level reaches 98.5% in 12-year-olds at the enamel level (168). In addition, the number of cases of dental treatments for children under general anesthesia has increased by 350% over the past 16 years (169). However, despite legislation mandating public dental care for children under 18 years of age, access to dental care is limited due to funding shortages and the need for dentists, particularly in regions outside the capital city.
Latvian laws emphasize the importance of ensuring children's access to healthcare, including dental care, and hold parents or guardians responsible for their child's health and well-being. Neglect is defined as the failure or negligent performance of duties of care and supervision or prolonged neglect that harms the child's development or causes physical or psycho-emotional suffering, as stated in Article 13 of the Law on the Protection of the Rights of the Child (170). Liability for failure to fulfil childcare obligations can result in a warning or a fine, as described in Article 51 (170). Parental custody may also be suspended in cases where the parent endangers the child's health or life, abuses their rights, or fails to ensure the care and supervision of the child, as per Article 200 of the Civil Code (171). However, it is challenging to implement legal instruments to address child dental neglect in Latvia. This is because of limited access to public service, which has resulted in delays in adequate care, a lack of timely interventions and no prevention programs.
To effectively address the oral health needs of children in Latvia, it is imperative to shift towards evidence-based interventions supported by reforms in the payment systems. The adoption of value-based healthcare models (172), which prioritize health outcomes rather than paying for manipulations, could raise public awareness about parents' responsibilities. By implementing these reforms, Latvia can strengthen the application of legal instruments, ultimately leading to improved oral health outcomes for children and reducing the prevalence of caries.
Serbia
One third (36.7%) of children aged 12 to 71 months in Serbia had ECC, and a mean dmft of 0.9, with 94.1% of the lesions untreated (173). About 44.3% of parents are actively involved with daily toothbrushing for their children. Children living in poor regions of the country have a higher likelihood of ECC and untreated lesions (173).
Although there is universal dental health care coverage for children and adolescents until age 18 years and for undergraduate students until age 26 years, there is poor uptake of the free public dental services: 23% of infants received oral health examination and advice before their first birthday, 18% of parents of infants received free individual oral health education, 20% of toddlers received oral health examination, 17% of parents of toddlers received free individual oral health education and 20% of 3-year-olds received oral health examination (174).
The General Protocol for Child Protection from Abuse and Neglect was adopted for implementation by the Government of the Republic of Serbia in 2005 and was developed in collaboration with the WHO and International Society for Prevention of Child Abuse and Neglect (175, 176). The document notes that neglect includes neglecting health care needs of children, such as not providing necessary dental care. However, child dental neglect is not officially reported as an independent diagnostic entity in any legal act or document concerning child neglect or abuse in the country. To date, there has only been one case of dental neglect reported (177). Also, no pediatric dentist serves as an expert on the working group that developed the National Strategy on Abuse Prevention and Child Protection in the Republic of Serbia (178). This oversight may have created a gap in the use of specific terminology, although dental neglect is an officially reportable entity. Having a specialist in dentistry as a member in the multidisciplinary team handling child neglect will improve the attention paid to dental neglect in Serbia.
United Kingdom
Despite the availability of free dental care to children through the National Health Service (NHS), inequality in dental caries is a persistent problem in England. Dental caries affects children whose families are subjected to socioeconomic adversities, live in deprived areas and are ethnic minorities (179). Furthermore, apparent socioeconomic inequalities in regular dental visits were also observed among children in the UK (180). This is particularly important, as it hinders early identification of those at high disease risk for prevention and timely intervention. Difficulties such as availability of dental appointments, inability to take time off work and cost of transportation have been recognized as potential contributors to inadequate regular dental visits and have led to delayed caries detection and treatment; however, others have highlighted the possibility of child dental neglect as a reason for delayed treatment of caries (181).
The National Institute for Health and Care Excellence (NICE) recognizes unexplained oral injuries and persistent failure to seek dental care for dental problems when services are available as child dental neglect (182). The NICE guidelines enumerate considerations for child dental neglect and place the responsibility of child dental neglect on parents (183). Others have criticized this approach and argued that there should be a role for dentists to communicate with other healthcare professionals and social services to tackle child dental neglect (184). In 2022, there was an apparent improvement in the training of undergraduate and postgraduate dental students to identify child neglect, communicate with different agencies and refer suspected cases of maltreatment and neglect (185).
The government has however also recognized the role of socioeconomic and environmental factors in child dental neglect and has developed guidance aimed at preventing dental caries and making healthy choices the easier choices. This included providing parental advice on breastfeeding, healthy eating and reduction of sugar consumption, increased taxation on soft drinks, targeted supervised tooth brushing, provision of toothbrushes and toothpaste by post, and targeted community fluoride varnish and water fluoridation (186). The government also has legislation and recommendations to prevent child maltreatment and neglect, which include the Children's Act 1989 (187) and the Working Together to Safeguard Children program.
South-East Asia region
India
India is home to the largest child population in the world, with almost 41% of its 1.4 billion people under 18 years of age. For children below 6 years, the prevalence of ECC is about 49.6%, ranging from 41.9% to 69% in different regions (188); the prevalence of dental trauma is about 15% (189). Dental neglect is a significant problem, and causes include parental deferment of the child's treatment needs despite being aware, or the child's fear of dental treatment preventing the treatment from being done (190). Neglect is worse amongst female children, children from joint families and children of parents with low socioeconomic status (191).
Article 21 of the constitution of India (192) guarantees the right to health as a fundamental right of all citizens. The scope of Article 21 was further widened, as the Supreme Court held that it is the responsibility of the Government to provide adequate medical aid to every person and to strive for the welfare of the public at large. India is also a signatory to the United Nations Convention on the Rights of the Child and has the Children Act, 1960 (193), which provides for the care, protection, maintenance, welfare, training, education, and rehabilitation of neglected or delinquent children. There are, however, no studies that quantify the magnitude of established cases of child dental neglect. The constitutional right of the child to health has not been reflected in the oral health of children in India. Awareness of oral diseases is a key for preventing dental neglect. A specific law on the right of every child in India to oral health may change this paradigm.
Indonesia
Many children in Indonesia have poor oral health, and this problem continues into teenage and adult years (194). Over 90% of Indonesian children aged 5–6 years have caries (195) and the oral health of street children is very poor (196). It is estimated that approximately 22.2% of children in Indonesia experience neglect (196) driven by variables at the individual (gender, age of the child, and child's disability status) and household level (housing condition, education level and age of the head of household, household economic status, number of minor household members, parents' working status, one or both parents dead, existence of other neglected children in the household, and living arrangements).
The Law of the Republic of Indonesia Number 23 of 2002 and Number 35 of 2014 make up the primary legal framework that governs the protection of children in Indonesia (197, 198). These laws recognize the fundamental right of children to protection from violence, abuse, neglect, and exploitation, as well as the right to education, healthcare, and social welfare. The laws also recognize the importance of providing children (anyone below the age of 18 years) with access to quality health care services, nutrition, clean water and sanitation; and ensuring that children's physical, mental, and emotional well-being is protected (197, 198). The laws also prohibit any form of violence, abuse, or neglect that may harm children's physical or mental health, and imposes penalties on perpetrators (197, 198). The law, however, requires that the government provide free health care services to children in need, particularly those from low-income families, marginalized communities, and remote areas. When the government has met its obligation, a case can be established of willful failure of a parent or guardian to seek and receive treatment necessary to ensure a level of oral health essential for adequate function and freedom from pain and infection of the child. However, there is no specific data on the neglect of children, nor is there any on child dental neglect. This highlights an area that needs further research and policy attention in the country.
Western pacific region
Mainland China
Dental caries among children is a major public health problem in Mainland China. Over 70% of 5-year-olds and about 40% of 12-year-old children experienced dental caries in 2015 (199, 200). Most of the decayed teeth were not restored. The mean DMFT score was 0.83 and the mean DT score accounted for 83.4% of dental caries experience among 12-year-old children. For the 5-year-old children, the mean caries experience score was 4.24 and the mean dt score accounted for 95.9% of dental caries experience (200). Dental neglect resulting from poor awareness of oral healthcare and poor oral health-related knowledge contributes to the high level of untreated decayed teeth (77, 201).
The 2016 Healthy China 2030 blueprint and associated action plans proposed promotion of oral health, integration of oral examination into regular physical examinations and provision of topical fluoride, pit and fissure sealing and other oral health-care measures for children (202). Also, China enacted the Law on Protection of Minors (203), which requires that stakeholders, including parents/legal guardians, schoolteachers, and healthcare workers, be responsible for the protection of the physical and mental health of minors, safeguard their lawful rights and interests, and promote their all-around development. This law implies that poor uptake of accessible oral healthcare services by caretakers of children in need of oral health care is illegal. There is, however, no country level legal instrument that directly addresses child dental neglect in China.
The establishment of cases of child dental neglect may be challenging in the short run. China has a large population of children with dental caries experience, many of whom do not routinely visit the dental clinic: about 40% of 12-year-old school children have never visited a dentist (204). This makes it difficult to establish a case of dental neglect for most affected children. When a child has no dental home, dental professionals have poor knowledge and awareness of dental neglect (201), and the general public's prioritization of oral health needs is low (199). These individual, household, and structural barriers may limit the possibility of establishing a case of dental neglect against caregivers.
Hong Kong
The prevalence of dental caries in preschool children in Hong Kong has remained persistently high at 55% for many years (205). Unfortunately, dental services have not kept up with this burden (206), and a staggering 95% of caries in primary dentition remains untreated (205). In contrast, the caries prevalence in 12-year-old children is lower at 23% with a DMFT index of 0.4 (207). The success of the free dental care services provided by the School Dental Care Service is believed to contribute to this lower caries prevalence in older children while low socioeconomic status has been linked to a higher prevalence of dental caries in young children (208).
The Hong Kong government adopted the United Nations Convention on the Rights of the Child in 1997, with a commitment to providing children with the highest attainable standard of health (209). Policies related to child protection and child abuse are formulated by the Child Protection Policy Unit (210), and services for children in need of protection from maltreatment are provided by the Family and Child Protective Services (211). The law holds individuals over the age of 16 years responsible for willfully neglecting a child, with potential prison sentences of ten years on indictment or three years on summary conviction (212).
Despite these regulations and efforts, the number of new child abuse cases in Hong Kong has alarmingly increased from 940 in 2020 to 1367 in 2021, with child neglect accounting for about 20% of all reported cases of abuse/maltreatment (211). Dental neglect, which can be prosecuted as child neglect, often goes unnoticed or unreported due to poor awareness and knowledge about the signs of dental neglect. It is particularly prevalent among those with low socioeconomic status (213).
Summary of findings
As mentioned in the Methods section, we theorized that countries with developed health and social care systems [including for child dental health and child (dental) neglect] had well-defined policies to address child dental neglect. Table 1 provides a summary of the prevalence of caries, and alongside, summarizes the legal status on child dental neglect in the 26 countries and the one special administrative region studied. The side-by-side presentation of this data allows for an at-a-glance review of the data relevant to our theory. Twenty-five of the 26 countries and administrative regions have legal instruments to address child neglect. However, only two (8.0%) of these 25 countries and administrative regions had specific legal instruments on child dental neglect.
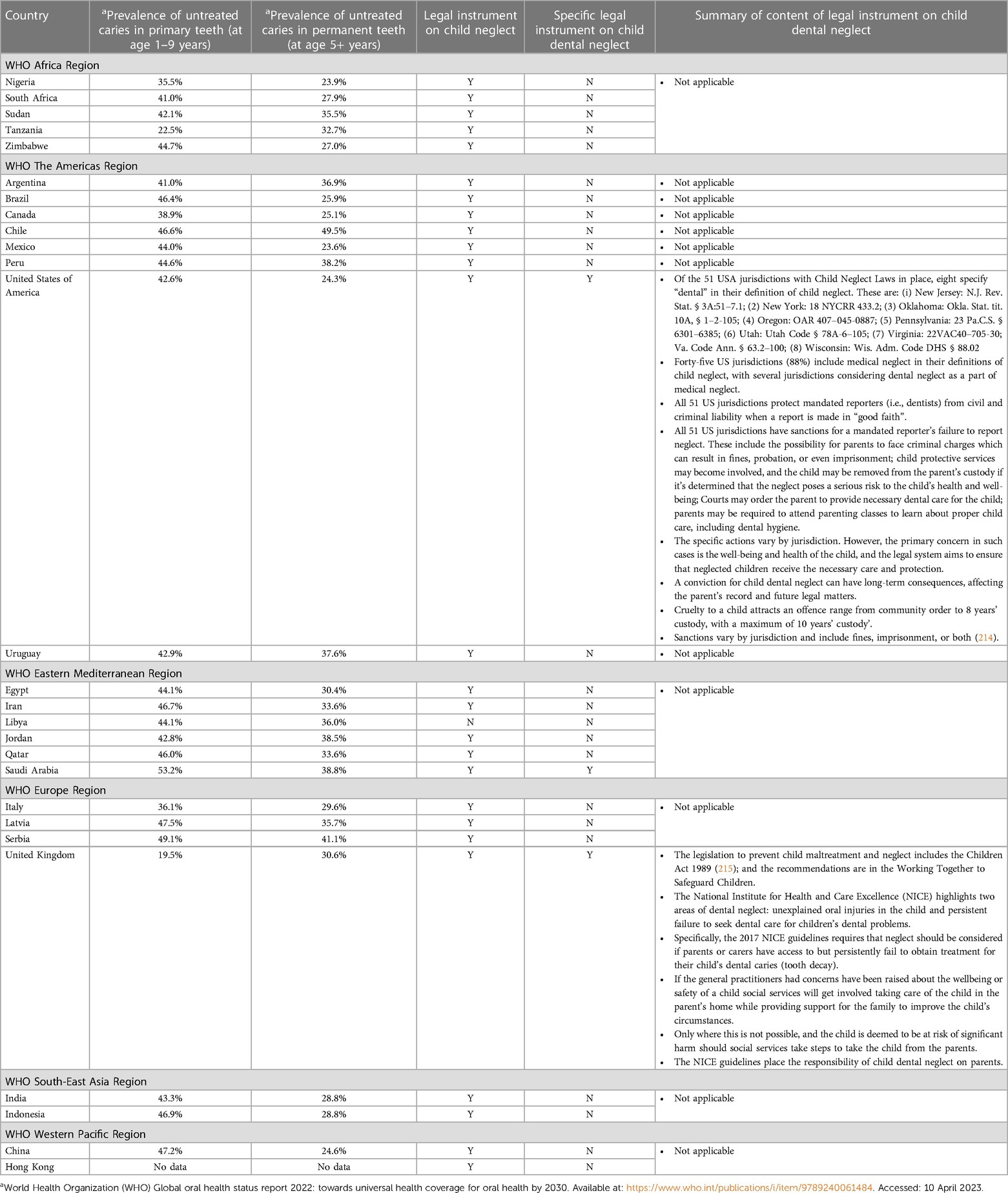
Table 1. Prevalence of caries and legal status on child (dental) neglect in 26 countries and a special administrative unit of China.
The data does not reveal any discernible correlation between the prevalence of untreated ECC and the presence of specific legal measures addressing child dental neglect. Nevertheless, in the two countries where legal provisions for child dental neglect exist, these measures outline the responsibilities of general practitioners in identifying instances of dental neglect and involve social protective agents to enhance the well-being of affected children. In both countries, the social workers are involved in managing the child before prosecution, and sanctions for child dental neglect can be as severe as been held in custody. The involvement of social protective agents consistently aims to address the needs of the affected child.
Discussion
This policy analysis indicates that while many countries may have laws pertaining to child neglect, specific laws addressing the failure of caregivers to seek and provide adequate oral care and treatment for children as child neglect are uncommon. However, child neglect laws can be interpreted to encompass cases of child dental neglect, provided other corroborating conditions are met. In countries where the government has not adequately addressed barriers that limit children's access to oral healthcare, establishing a case of child dental neglect may prove challenging. These barriers include the unavailability of dental care, limited affordability of dental services, dentists' lack of awareness and competency to identify, manage, and report cases of child dental neglect, and a general lack of public awareness regarding the significance of oral health, the dental care system for children, and the legal implications of failing to provide oral healthcare. In high-income countries where legal instruments exist, the supporting environment does not appear to offer additional protection against the risk of untreated dental caries in children.
We hypothesize that having specific laws on child dental neglect may not provide significant protection for children against the risk of untreated caries. However, in countries where such laws exist, it is more likely that the government will establish supportive systems and structures to enhance children's access to dental care. These legal mandates for oral health care may encourage regular dental visits for checkups and diagnostic tests, thereby reducing the risk of caries at the individual level. Moreover, the existence of specific laws on child dental neglect may lead to public education on the legal responsibilities of parents and caregivers to ensure children's access to oral health care, the training of dentists in diagnosing and reporting cases of neglect, and the training of the judiciary to handle cases related to child dental neglect. This comprehensive approach can be referred to as a “social ecosystem” that promotes preventive dental care for children. Furthermore, in situations where specific laws on dental neglect are in place, but the government is not fulfilling its responsibilities, advocates can actively campaign for the establishment of systems and structures to protect the oral health of children and minimize neglect. This proactive stance can lead to improved access to dental care for children and better oral health outcomes.
Creating social ecosystems to prevent child dental neglect fits well within a human rights framework. The right to health is a fundamental human right protected and guaranteed by laws, as identified by this study. Oral health is an integral component of general health; without it, there can be no sound state of overall health. However, whether the right to health includes the right to oral health remains unresolved (216), we the authors believe that the right to health includes oral health. Where the right to oral health for children is guaranteed by legislation, the evidence highlighted in Table 1 seems to suggest that this is not enough. A social ecosystem for the prevention of child dental neglect, inclusive of the law, is needed. However, parents need to be educated about their responsibility to seek dental care for their children, particularly where free dental services are available. The competency of dental practitioners to identify, report and manage child dental neglect needs to be built. Public health authorities need to support and maintain an environment that promotes health and develop preventive dental programs for those who are overwhelmed by adverse socioeconomic conditions. Laws ensure that rights are protected and laws against dental neglect ensure that children's rights to oral health care is considered important enough for systems to be established and processes to be instituted.
We acknowledge that the right to oral health is a complex concept that has normative, philosophical, and practical dimensions, and its implementation is dictated by available resources and local priorities based on contextual factors (217). Also, the neurological, biological, and behavioral sequelae of neglect are driven by the chronicity, severity, and timing of neglect experiences (4). This complexity suggests that the determination of child neglect should be on a case-by-case basis, taking into consideration all the nuances that influence the establishments of such a case. These nuances may create a gap between the existence of laws and policies that protect children from dental neglect, and their implementation. For example, where dentists are mandated to establish the case of dental neglect, care reporting will be very low when the number of children who utilize oral health facilities is low. Children experiencing dental neglect will be less likely to be detected in the dental clinic, as they will likely only visit when there is an extreme need for dental care services. Also, in countries where the judiciary system is weak and corrupt, police reporting of child dental neglect will be low, and prosecuting cases may be compromised. Yet, deliberate actions need to be taken to safeguard the health, wellbeing, and welfare of every child by maintaining their oral health. These country specific nuances may imply that the operationalization of child dental neglect may differ from country to country.
The influence of culture on child management adds another layer of complexity to diagnosing child dental neglect and impacts how communities perceive such cases. Parenting behaviors are culturally shaped, and definitions of neglect vary across different cultures and societies (218). In some societies where poverty and limited access to dental care prevail, the lack of provisions for oral health care affects the entire community, making what may be otherwise defined as child dental neglect more of a community-level issue rather than solely the responsibility of neglectful parents as would be the case in a well-provisioned community (218). These cultural and societal nuances can impact how dental neglect is perceived, potentially leading to it being seen as a societal problem with health impact rather than a criminal act. Unfortunately, there is no consensus in the literature on the contextual definition of child dental neglect, making it challenging to analyze the factors that may influence the criminalization of such cases.
In addition, although child dental neglect may exist in isolation, untreated oral diseases can be a sign of broader child neglect and exposure to adverse experiences (77). Family isolation, lack of financial support, transportation difficulties, parental ignorance, parental psychopathology, poverty, or a lack of perceived value of oral health may all contribute to a failure to seek or obtain proper dental care (109, 119). Child dental neglect may be an indicator of child maltreatment (220), with children who are maltreated likely to have 2–8 more teeth with caries experience than children who are not maltreated (221, 222).
Ironically, although laws should protect the interests of children, their use may jeopardize public health efforts to meet children's oral health needs. Laws that criminalize child dental neglect assign blame and may not be strong enough to prevent harm (223), as the parent may be living in a social context that is disempowering, or they lack the tools to act on behalf of the child's oral health wellness and wellbeing (224). Children then experience deleterious chronic stress and adverse childhood events that further reduce their quality of life in addition to the impact on oral diseases they are suffering from (224). This collateral damage may result from the criminalization of dental neglect in countries where the experience of adverse childhood events is already high, as criminalization may have a more negative than positive impact on the child's long-term wellbeing. A viable alternative is creating or strengthening public health systems to meet the child's oral healthcare needs. Children who experience dental neglect most likely come from disadvantaged and vulnerable communities (225), which may do better with access to support rather than criminalization.
The intricate interplay of various factors complicates the establishment of a criminal case for child dental neglect, making it challenging to assess the effectiveness of legal measures in curbing untreated dental caries, a primary objective of this study. To begin with, there seems to be very few countries with explicit legal provisions addressing child dental neglect, thereby restricting the collection and analysis of pertinent data concerning child dental neglect. In cases where legal instruments do exist, the availability of analyzable data is exceedingly scarce, posing considerable difficulties in evaluating the effectiveness of such laws on a broader scale. While it's conceivable that these laws might be effective at the household level, there is minimal accessible literature providing evidence in this regard. Consequently, there is a substantial need for further research to address these gaps resulting from limited evidence, which is essential for advocating the implementation of specific laws pertaining to child dental neglect.
In the interim, combining a public health approach with a human rights-based approach, inclusive of an efficient criminal justice system to deal with dental neglect, may be more effective to control children dental neglect. The public health focus brings an analytic approach to identifying risk factors that then become the focus of preventive interventions. This may be more effective for the primary prevention of crimes than the use of punitive criminal laws (226). Such public health approach includes the use of outreach dental clinics to provide oral health services for disadvantaged and vulnerable communities (227). Unlike the criminal justice system that is reactive and punitive, the public health response is proactive and preventive. Also, the criminal justice system in many countries is ineffective in criminal behavior control, as the system is tainted from the point of arrest to investigation, arraignment in court, case hearing, verdict, and execution of court verdict (228).
In summary, the neglect of a child's oral health when caregivers or parents fail to seek and provide appropriate oral care and treatment is a matter that requires attention. However, addressing child dental neglect and considering whether it should be a criminal offense is a multifaceted issue with normative, philosophical, and practical aspects. It necessitates a careful examination of country-specific circumstances to establish the conditions under which a criminal case can be established. Both public health initiatives and the criminal justice system should, at the very least, prioritize the prevention of untreated dental caries due to its severe consequences, which include stunted physical growth and development, impaired psychological and cognitive development, adverse neurodevelopmental outcomes, and diminished quality of life (229, 230). When public health systems are sufficiently equipped to facilitate children's access to oral healthcare, then criminal penalties may be imposed on caregivers who neglect to seek oral health treatment, whether for preventive or curative purposes, for children with dental caries or other oral health needs. The extent of punitive measures should be tailored to the specific context.
This study has several limitations that should be acknowledged. Firstly, this was a narrative literature review, which may not offer a fully exhaustive and detailed understanding of the issues concerning child dental neglect and oral health problems (231). However, the review effectively fulfills its objective of providing an overview of a topic that has not been extensively explored before. The overview was, however, limited to 26 (12.7%) of the 204 countries in the world, and these countries were conveniently selected, with the number of countries not being proportionately distributed across regions. Despite these limitations in the sampling procedure, the information provided by the study sample still offers an insightful overview of a social and public health issue that may be interplaying to exacerbate societal problems.
Conclusion
This policy review indicates that different countries have varying legislative approaches to addressing child dental neglect, and that legislative efforts alone may not be sufficient to solve this problem. A more comprehensive approach that uses a mix of public health and human rights approaches may be more successful. However, it seems that laws and legislation that prohibit child dental neglect increase the prospect of building a social ecosystem that may reduce children's risk to caries at the individual level. Where there are laws that prohibit child neglect without explicit focus on child dental neglect, it is unlikely that there will be a social ecosystem that prevents child dental neglect. Also, the social context may inform how child dental neglect is defined and operationalized. Therefore, we recommend that countries set their own nuanced definition of child dental neglect and develop a social ecosystem and legal instruments specific to country context without undermining the right of the child to oral health.
Author contributions
MF conceptualized the study, was involved with data management, wrote the first draft of the manuscript and consents to the final version of the manuscript for submission. NN extracted the data on caries for the Table. MF, FR-G, OF, NN, GL, IM RM, NM, NP, CM, PM, CA, AA, SM, PE, JC, RA, AI, FP, AA, OA-B, YK, SA-M, WB, RAZ, AV, JJ, RJ, IM, AA, FM, SU, MC, DD, and MET wrote the brief for specific countries, read multiple versions of the manuscript for intellectual inputs and consent to the final version of the manuscript for submission. FR-G, MET and NASA conducted extensive review of multiple versions of the manuscript for intellectual input and consent to the final version of the manuscript for submission. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization, United Nations. Global Status report on violence prevention 2014. Geneva, Switzerland: WHO Press (2014).
2. Hillis S, Mercy J, Amobi A, Kress H. Global prevalence of past-year violence against children: a systematic review and minimum estimates. Pediatrics. (2016) 137(3):e20154079. doi: 10.1542/peds.2015-4079
3. World Health Organization. Violence Against Children. Available at: https://www.who.int/health-topics/violence-against-children (Accessed: 9th April 2023).
4. Committee on Child Maltreatment Research, Policy, and Practice for the Next Decade: Phase II; Board on Children, Youth, and Families; Committee on Law and Justice; Institute of Medicine; National Research Council. Consequences of child abuse and neglect. In: Petersen AC, Joseph J, Feit M, editors. New directions in child abuse and neglect research. Washington (DC): National Academies Press (US) (2014). Available from: https://www.ncbi.nlm.nih.gov/books/NBK195987/
5. Sabbah W, Folayan MO, El Tantawi M. The link between oral and general health. Int J Dent. (2019) 2019:7862923. doi: 10.1155/2019/7862923
6. Onyejaka NK, Folayan MO, Folaranmi N. Barriers and facilitators of dental service utilization by children aged 8 to 11 years in enugu state, Nigeria. BMC Health Serv Res. (2016) 16:93. doi: 10.1186/s12913-016-1341-6
7. Clinical Affairs Committee, American Academy of Pediatric Dentistry. Guideline on adolescent oral health care. Pediatr Dent. (2015) 37(5):49–56.26531076
8. Kassebaum NJ, Bernabé E, Dahiya M, Bhandari B, Murray CJ, Marcenes W. Global burden of untreated caries: a systematic review and metaregression. J Dent Res. (2015) 94(5):650–8. doi: 10.1177/0022034515573272
9. Fox J. The epidemic of the children’s dental disease: putting teeth into law. Yale journal of health policy. Law Ethics. (2011) 11(2):231.
10. Elice CE, Fields HW. Failure to thrive: a review of the literature, case report and implications for dental treatment. Pediatr Dent. (1990) 12:185–9.2150222
11. Acs G, Lodolini G, Kaminski S, Cisneros GJ. Effect of nursing caries on body weight in pediatric population. Pediatr Dent. (1992) 14:302–5.1303533
12. Palermo TM. Impact of recurrent and chronic pain on child and family daily function: a critical review of the literature. J Dev Behav Pediatrics. (2000) 21(1):58–69. doi: 10.1097/00004703-200002000-00011
13. Oral health, dental disease is a chronic problem among low-income populations. (2000). 4 United States General Accounting Office, report to congressional requesters.
14. Clarke M, Locker D, Berall G, Pencharz P, Kenny DJ, Judd P. Malnutrition in a population of young children with severe early childhood caries. Paediatric Dentistry. (2006) 28:254. 16805358
15. National Maternal and child oral health resource centre, oral health and learning: when children’s health suffers so does their ability to learn. (2003) 2.
16. Department of Health. Child protection and the dental team. (2005). Available at: http://www.cpdt.org.uk/f_info/dload/Childprotectionandthedentalteam_v1_4_Nov09.pdf (Accessed March 26, 2012).
17. Noble F, Dickie J, Conway DI. Systematic review highlights difficulty in clearly identifying dental neglect in children. Evid Based Dent. (2014) 15(1):3–4. doi: 10.1038/sj.ebd.6400978.
19. Ferrari AM. The impact of culture upon child rearing practices and definitions of maltreatment. Child Abuse Negl. (2002) 26(8):793–813. doi: 10.1016/s0145-2134(02)00345-9
20. He H, Usami S, Rikimaru Y, Jiang L. Cultural roots of parenting: mothers’ parental social cognitions and practices from western US and Shanghai/China. Front Psychol. (2021) 12:565040. doi: 10.3389/fpsyg.2021.565040
21. Kitschelt H. Four theories of public policy making and fast breeder reactor development. Int Organ. (1986) 40(1): 65–104. Available at: http://www.jstor.org/stable/2706743 doi: 10.1017/S0020818300004483
22. Sheldon MR. Policy-Making theory as an analytical framework in policy analysis: implications for research design and professional advocacy. Phys Ther. (2016) 96(1):101–10. doi: 10.2522/ptj.20150032
23. Sabatier PA, Weible CM, editors. Theories of the policy process. 3rd ed. Boulder, CO: Westview Press (2014). p. 3–20.
25. Howlett M, Ramesh M. Studying public policy: policy cycles and policy subsystems. Oxford, UK: Oxford University Press (2003).
26. Parsons T. Full citizenship for the Negro American? A sociological problem. Daedalus. (1965) 94(4):1009–54. doi: 10.1080/13621020802586776
27. Pal LA. Case study method and policy analysis. In: Geva-May I, editors. Thinking like a policy analyst. New York. Palgrave Macmillan. (2005). p. 227–57. doi: 10.1057/9781403980939_12
28. Folayan MO, Chukwumah NM, Onyejaka N, Adeniyi AA, Olatosi OO. Appraisal of the national response to the caries epidemic in children in Nigeria. BMC Oral Health. (2014) 14:76. doi: 10.1186/1472-6831-14-76
29. Agbaje HO, Kolawole KA, Folayan MO, Onyejaka NK, Oziegbe EO, Oyedele TA, et al. Digit sucking, age, sex, and socioeconomic Status as determinants of oral hygiene Status and gingival health of children in suburban Nigeria. J Periodontol. (2016) 87(9):1047–56. doi: 10.1902/jop.2016.150681
30. Folayan MO, Adeniyi AA, Arowolo O, Maureen CN, Alade MA, Tantawi ME. Risk indicators for dental caries, and gingivitis among 6-11-year-old children in Nigeria: a household-based survey. BMC Oral Health. (2022) 22(1):465. doi: 10.1186/s12903-022-02470-1
31. Folayan MO, El Tantawi M, Chukwumah NM, Alade M, Oginni O, Mapayi B, et al. Individual and familial factors associated with caries and gingivitis among adolescents resident in a semi-urban community in south-western Nigeria. BMC Oral Health. (2021) 21(1):166. doi: 10.1186/s12903-021-01527-x
32. Uguru N, Onwujekwe O, Uguru CC, Ogu UU. Achieving universal health coverage in Nigeria: the dilemma of accessing dental care in enugu state, Nigeria, a mixed methods study. Heliyon. (2021) 7(1):e05977. doi: 10.1016/j.heliyon.2021.e05977
33. Ola DO, Gambôa ABO, Folayan MO, Marcene W. Family structure, socio-economic position and oral health services utilisation in Nigerian senior secondary school pupils. J Public Health Dent. (2013) 73(2):158–65. doi: 10.1111/j.1752-7325.2012.00362.x
34. Abiola Adeniyi A, Eyitope Ogunbodede O, Sonny Jeboda O, Morenike Folayan O. Do maternal factors influence the dental health status of Nigerian pre-school children? Int J Paediatr Dent. (2009) 19(6):448–54. doi: 10.1111/j.1365-263X.2009.01019.x
35. Ayanda JO. Utilization of health care services in rural and urban areas: a determinant factor in planning and managing health care delivery systems. Afr Health Sci. (2014) 14(2):322–33. doi: 10.4314/ahs.v14i2.6
36. Folayan MO, Ozeigbe E, Oyedele T, Ola D. Factors limiting dental service utilization by pupils in ile-ife, Nigeria. Nigeria J Health Sci. (2013) 13(2):18–23.
37. Uguru N, Onwujekwe O, Ogu UU, Uguru C. Access to oral health care: a focus on dental caries treatment provision in enugu Nigeria. BMC Oral Health. (2020) 20(1):145. doi: 10.1186/s12903-020-01135-1
38. Federal Government of Nigeria. Child Right Act 2003 No 26. A451-A605. Available at: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.refworld.org/pdfid/5568201f4.pdf (Accessed April, 9 2023).
39. National Human Rights Commission. Child Rights. Available at: https://www.nigeriarights.gov.ng/focus-areas/child-rights.html#:∼:text=Child’s%20Right%20Act%20(2003)%20is,36%20states%20of%20the%20federation (Accessed April 9, 2023).
41. Federal Ministry of health. Nigeria Health Facility Registry. Available at: https://hfr.health.gov.ng/statistics/tables (Accessed April 9, 2023).
42. Olusile A. Improving low awareness and inadequate access to oral health care in Nigeria: the role of dentists, the government & non-governmental agencies. Nigerian Med J. 2010;51(3):134. Available at: https://www.ajol.info/index.php/nmj/article/view/59905 (Accessed January 23, 2023).
43. Ajikobi D. Africa check: sorting fact from fiction 2017. (2018). Available at: https://africacheck.org/reports/do-fewer-than-20-of-nigerians-have-access-to-oral-health-care-services/ (Accessed January 23, 2022).
44. Olatosi OO, Ogordi PU, Oredugba FA, Sote EO. Experience and knowledge of child abuse and neglect: a survey among a group of resident doctors in Nigeria. Niger Postgrad Med J. (2018) 25(4):225–33. doi: 10.4103/npmj.npmj_92_18
45. Bankole OO, Denloye OO, Adeyemi AT. Child abuse and dentistry: a study of knowledge and attitudes among Nigerian dentists. Afr J Med Med Sci. (2008) 37(2):125–34. 18939395
46. van Wyk PJ, van Wyk C. Oral health in South Africa. Int Dent J. (2004) 54(6 Suppl 1):373–7. doi: 10.1111/j.1875-595x.2004.tb00014.x
47. Mohamed N, Barnes J. Early childhood caries and dental treatment need in low socio-economic communities in Cape Town, South Africa. Health SA. (2018) 23:1039. doi: 10.4102/hsag.v23i0.1039
48. STATSSA. Mid-Year Population Estimates. STATSSA Mid Year Population. (2022). Available at: https://www.statssa.gov.za/publications/P0302/P03022022.pdf (Accessed April 12, 2023).
49. Simón-Soro A, Mira A. Solving the etiology of dental caries. Trends Microbiol. (2015) 23(2):76–82. doi: 10.1016/j.tim.2014.10.010
50. STATSSA. General Household Survey 2021. STATSSA: General Household Survey. (2021). Available at: http://www.statssa.gov.za/publications/P0318/P03182018.pdf (Accessed April 12, 2023).
51. Peerbhay F, Barrie RB. The burden of early childhood caries in the western cape public service in relation to dental general anaesthesia: implications for prevention. SADJ. (2012) 67(1):14–6. 18. 23189901
52. Children’s Act No 38 of 2005. Available at: https://www.justice.gov.za/legislation/acts/2005-038%20childrensact.pdf (Accessed April 12, 2023).
53. Children’s Amendment Act No 41 of 2007. Available at: https://www.gov.za/sites/default/files/gcis_document/201409/a41-070.pdf (Accessed April 12, 2023).
54. Ibrahim REHM, Helaly MO, Ahmed EMA. Assessment of brushing techniques in school children and its association with dental caries, omdurman, 2019. Int J Dent. (2021) 2021:4383418. doi: 10.1155/2021/4383418
55. Omara H, Elamin A. Oral health status and related risk factors among adolescents attending high schools in Khartoum, Sudan: a cross-sectional study. Clin Epidemiol Glob Health. (2022) 16:101080. doi: 10.1016/j.cegh.2022.101080
56. Ministry of Justice. Sudanese Child Act Arabic version. (2010). Available at: https://www.arabccd.org/files/0000/516/ (Accessed April 15, 2023).
57. The Ministry of Health, Community Development, Gender, Elderly and Children. The Fifth Tanzania National Oral Health Survey Report (2020). Available at: https://hssrc.tamisemi.go.tz/storage/app/uploads/public/61e/962/c04/61e962c047b75470406472.pdf (Accessed April 15, 2023).
58. The Law of Child Act. (2009). Available at: https://www.ilo.org/wcmsp5/groups/public/—ed_protect/—protrav/—ilo_aids/documents/legaldocument/wcms_151287.pdf (Accessed April 9, 2023).
59. The United Nations Children’s Fund (UNICEF). Child protection report of 2020. Available at: https://www.unicef.org/tanzania/what-we-do/child-protection (Accessed April 9, 2023).
60. Ramazani N. Child dental neglect: a short review. Int J High Risk Behav Addict. (2014) 3:e21861. doi: 10.5812/ijhrba.21861
61. Frencken JE, Sithole WD, Mwaenga R, Htoon HM, Simon E. National oral health survey Zimbabwe 1995: dental caries situation. Int Dent J. (1999) 49:3–9. doi: 10.1111/j.1875-595X.1999.tb00501.x
62. Mafuvadze BS, Mahachi L, Mafuvadze B. Dental caries and oral health practice among 12 year old school children from low socioeconomic status background in Zimbabwe. Pan Afr Med J. (2013) 14(164):164. doi: 10.11604/pamj.2013.14.164.2399
64. Matanhire C, Masiiwa A, Sibanda M. The dental caries experience of preschool children in Harare. Int J Res Rep Dent. (2020) 3(1):27–36.
65. Akino C, Matanhire C, Mucheto P. Assessing oral health promotion activities within primary schools in Harare. Zimbabwe: University Of Zimbabwe, College Of Health Sciences, Department Of Dentistry (2021).
66. Munniz BR. Epidemiologic oral health survey of argentine children. Commun Dent Oral Epidemiol. (1985) 13:328–33. doi: 10.1111/j.1600-0528.1985.tb00466.x
67. Bardauil G. Abordaje de la negligencia infantil: una función de los Pediatras. Not. la Soc. Argentina Pediatría. (2010). 47. Available at: https://www.sap.org.ar/docs/noticias_metr_49.pdf (Accessed April 20, 2024).
68. Ministerio de Salud de la Nacion Argentina. (2022). Caries [WWW Document]. Available at: https://www.argentina.gob.ar/cuidados-de-la-salud-hospital-posadas/caries (Accessed April 11, 2023).
69. Confederación Odontológica de la República Argentina. (2019). Perfil epidemiológico de caries en niños de Misiones. Available at: https://www.cora.org.ar/noticias/459 (Accessed April 11, 2023).
70. Congreso de la Nación Argentina. (2005). Ley de Protección Integral de los Derechos de las Niñas, niños y adolescentes. Available at: http://servicios.infoleg.gob.ar/infolegInternet/anexos/110000-114999/110778/norma.htm (Accessed April 11, 2023).
71. Pabayo R, Janosz M, Bisset S, Kawachi I. School social fragmentation, economic deprivation and social cohesion and adolescent physical inactivity: a longitudinal study. PLoS One. (2014) 9:e99154. doi: 10.1371/journal.pone.0099154
72. Brasil. Estatuto da Criança e do Adolescente (Child and adolescent statute). Lei 8.069/90. São Paulo: Atlas (1991) (in portuguese).
73. Jr PG, Lucena EH, Cawahisa PT. Financing national policy on oral health in Brazil in the context of the unified health system. Braz Oral Res. (2010) 24(Suppl 1):26–32. doi: 10.1590/s1806-83242010000500005
74. Agostini BA, Emmanuelli B, Piovesan C, Mendes FM, Ardenghi TM. Trends in use of dental services by Brazilian preschool children considering age-period- cohort effect. Int J Paediatr Dent. (2019) 29(4):413–21. doi: 10.1111/ipd.12481
75. Brasil SB 2010: Pesquisa Nacional de Saúde Bucal: resultados principais. Brasília: Ministério da Saúde (2012). (in Portuguese). Available at: http://bvsms.saude.gov.br/bvs/publicacoes/pesquisa_nacional_saude_bucal.pdf (Accessed April 20, 2023.
76. Gimenez T, Bispo BA, Souza DP, Viganó ME, Wanderley MT, Mendes FM, et al. Does the decline in caries prevalence of latin American and Caribbean children continue in the new century? Evidence from systematic review with meta-analysis. PLoS One. (2016) 11(10):e0164903. doi: 10.1371/journal.pone.0164903
77. Spiller L, Lukefahr J, Kellogg N. Dental neglect. J Child Adolesc Trauma. (2020) 13:299–303. doi: 10.1007/s40653-019-0247-y
78. Health Canada. Summary report on the findings of the oral health component of the Canadian Health Measures Survey, 2007-2009. Ottawa (ON): Health Canada. (2010). Available at: http://publications.gc.ca/site/eng/369653/publication.html (Accessed April 20, 2023).
79. Health Canada, Nunavut Tunngavik Incorporated, Nunatsiavut Government, Inuvialuit Regional Corporation, Inuit Tapiriit Kanatami. Inuit Oral Health Survey Report 2008–2009. Ottawa: Health Canada. (2011). Available at: http://www.hc-sc.gc.ca/fniah-spnia/alt_formats/pdf/pubs/promotion/_oral-bucco/oral-inuit-buccal-eng.pdf
80. Tsang A, Sweet D. Detecting child abuse and neglect–are dentists doing enough? J Can Dent Assoc. 1999;65(7):387–91. 10465918 (Accessed April 3, 2023).10465918
81. Child and Family Services Act, RSO 1990, c C.11. Available at: https://canlii.ca/t/532gf (Accessed April 3, 2023).
82. Public Health Agency of Canada. Provincial and Territorial Child Protection Legislation and Policy 2018.
83. Brasil SB 2020. Pesquisa Nacional de Saúde Bucal: resultados preliminares. Brasília: Ministério da Saúde (2022). (in Portuguese). Available at: http://egestorab.saude.gov.br/image/?file=20221216_I_mod2resultadospreliminaresBrasiliamonsitecompressed_288277690346345359.pdf
84. Humanium. (n.d.). Chile. Available at: https://www.humanium.org/en/chile/ (Accessed April 16, 2023).
85. World Health Organization. Oral Health Country Profile, World Health Organization. (2022). Available at: https://www.who.int/publications/m/item/oral-health-chl-2022-country-profile (Accessed April 19, 2023).
86. Uribe SE, Innes N, Maldupa I. The global prevalence of early childhood caries: a systematic review with meta-analysis using the WHO diagnostic criteria. Int J Paediatr Dent. (2021) 31(6):817–30. doi: 10.1111/ipd.12783
87. Díaz JA, Bustos L, Brandt AC, Fernández BE. Dental injuries among children and adolescents aged 1-15 years attending to public hospital in temuco, Chile. Dent Traumatol. (2010) 26:254–61. doi: 10.1111/j.1600-9657.2010.00878.x
88. MINSAL. Diagnóstico de situación de salud bucal. (2010). Available at: https://www.minsal.cl/portal/url/item/7dc33df0bb34ec58e04001011e011c36.pdf (Accessed April 16, 2023).
89. UNESCO. Chile. SITEAL—Sistema de Información de Tendencias Educativas en América Latina. (2021). Available at: Https://siteal.iiep.unesco.org/pais/chile (Accessed April 16, 2023).
90. Ministerio de Desarrollo Social y Familia. Salud Bucal [Chile Crece Contigo program]. Gobierno de Chile. (2022). Available at: https://www.crececontigo.gob.cl/tema/salud-bucal/ (Accessed April 16, 2023).
91. Taillie LS, Reyes M, Colchero MA, Popkin B, Corvalán C. An evaluation of Chile’s law of food labeling and advertising on sugar-sweetened beverage purchases from 2015 to 2017: a before-and-after study. PLoS Med. (2020) 17(2):e1003015. doi: 10.1371/journal.pmed.1003015
92. Ministerio de Salud. Salud Bucal. Gobierno de Chile. (2022). Available at: https://www.minsal.cl/salud-bucal/ (Accessed April 16, 2023).
93. Universidad Nacional Autónoma de México. En México, 10 millones de niños con caries. Boletín UNAM-DGCS-538 Ciudad Univ. 2019. Available at: https://www.dgcs.unam.mx/boletin/bdboletin/2019_538.html (Accessed April 13, 2023).
94. Portal Odontólogos. En México, 9 de cada 10 niños tienen caries: Asociación Dental Mexicana. (2019). Available at: https://www.portalodontologos.mx/pacientes/noticias/3078/en-mexico-9-de-cada-10-ninos-tienen-caries-asociacion-dental-mexicana (Accessed April 13, 2023).
95. UNICEF. Convención Sobre Los Derechos Del Niño. (2022). Available at: https://www.unicef.es/publicacion/convencion-sobre-los-derechos-del-nino (Accessed April 13, 2023).
96. Convención Interamericana de los Derechos Humanos. Documentos Básicos En Materia de Derechos Humanos. (2001). Available at: http://www.cidh.org/Basicos/Básicos-indice.htm (Accessed April 13, 2023).
97. Gobierno de México. Ley General de Los Derechos de Niñas, Niños y Adolescentes (Reformada 23 Marzo 2022). (2022). Available at: https://www.gob.mx/sipinna/documentos/ley-general-de-los-derechos-de-ninas-ninos-y-adolescente (Accessed April 13, 2023).
98. Diario Oficial de la Federación, NORMA Oficial Mexicana NOM-047-SSA2-2015, Para la atención a la salud del Grupo Etario de 10 a 19 años de edad. (2015). Available at: https://www.dof.gob.mx/nota_detalle.php?codigo=5403545&fecha=12/08/2015#gsc.tab=0 (Accessed April 13, 2023).
99. Tiol-Carrillo A. Caries en niños. ¿maltrato infantil o ignorancia parental? Rev La Asoc Dent Mex. (2012) 78:205–8. doi: 10.35366/101074
100. Jiménez-Gayosso SI, Medina-Solís CE, Lara-Carrillo E, Scougal-Vilchis RJ, De La Rosa-Santillana R, Márquez-Rodríguez S, Mendoza-Rodríguez M, Navarrete-Hernández JJ. Desigualdades socioeconómicas en la utilización de servicios de salud bucal (USSB) alguna vez en la vida por escolares mexicanos de 6-12 años de edad. Gac Med Mex. (2015) 151:27–33. Available at: https://www.anmm.org.mx/GMM/2015/n1/GMM_151_2015_1_027-033.pdf (Accessed April 20, 2023).
101. Medina-Solís CE, Maupomé G, Pelcastre-Villafuerte B, Avila-Burgos L, Vallejos-Sánchez AA, Casanova-Rosado AJ. Desigualdades socioeconómicas en salud bucal: caries dental en niños de seis a 12 años de edad. Rev Investig Clin. (2006) 58:296–304. Available at: https://www.scielo.org.mx/scielo.php?script=sci_arttext&pid=S0034-83762006000400005 (Accessed April 20, 2023).
102. Ministerio de Salud. Prevalencia nacional de caries dental, fluorosis del esmalte y urgencia de tratamiento en escolares de 6 a 8, 10, 12 y 15 años, Lima:Oficina General de epidemiología, miNSA; 2005. (Accessed April 20, 2023).
103. Ley para prevenir, sancionar y erradicar la violencia contra las mujeres y los integrantes del grupo familiar. https://www.mimp.gob.pe/webs/mimp/ley30364/sobre-ley-30364.php (Accessed April 20, 2023).
104. Ministerio de Salud. Perfil epidemiológico de salud bucal en el Perú. Lima: miNSA. (2013). Available at: https://goo.gl/descbW (Accessed April 20, 2023).
105. Hernàndez-Vasquez A, Azañedo D, Dìaz-Seijas D, Bendezù-Quispe G, Arroyo-Hernàndez H, Vilcarromero S, et al. Access to oral health services in children under twelve years of age in Peru, 2014. Salad Colectiva. (2016) 12(3):429–41. doi: 10.18294/sc.2016.912
106. Fleming E, Afful J. Prevalence of total and untreated dental caries among youth: united States, 2015-2016. NCHS Data Brief. (2018) (307):1–8. 29717975
107. Dye BA, Thornton-Evans G, Li X, Iafolla TJ. Dental caries and sealant prevalence in children and adolescents in the United States, 2011–2012. NCHS Data Brief. (2015) (191):1–8. 25932891
108. Jackson SL, Vann WF Jr, Kotch JB, Pahel BT, Lee JY. Impact of poor oral health on children’s school attendance and performance. Am J Public Health. (2011) 101(10):1900–6. doi: 10.2105/AJPH.2010.200915
109. Fisher-Owens SA, Lukefahr JL, Tate AR. American Academy of pediatric dentistry, council on clinical affairs, council on scientific affairs, ad hoc work group on child abuse and neglect, American academy of pediatrics, section on oral health committee on child abuse and neglect. Oral and dental aspects of child abuse and neglect. Pediatr Dent. (2017) 39(4):278–83. doi: 10.1542/peds.2017-1487
110. Berger S. California Society of pediatric dentistry dental neglect—when to report. California Pediatrician. (1989) 1:31–2.
111. Krug EG, Dahlberg LL, Mercy JA, Zwi AB, Lozano R. World report on violence and health. Geneva: World Health Organization (2002). Available at: http://www.who.int/violence_injury_prevention/violence/world_report/ en/ (Accessed May 23, 2016).
112. Bhatia SK, Maguire SA, Chadwick BL, Hunter ML, Harris JC, Tempest V, et al. Characteristics of child dental neglect: a systematic review. J Dent. (2014) 42(3):229–39. doi: 10.1016/j.jdent.2013.10.010.
113. Angulo M, Pivel L, Zinemanas E, Jorysz E, Krasse B. Dental caries and microbial and salivary conditions in Uruguayan children from two different socioeconomic areas. Acta OdontoIScan. (1994) 52:377–83. doi: 10.3109/00016359409029035
114. Lorenzo S, Álvarez-Vaz R. Prevalence of caries in schoolchildren aged 12 years of different socioeconomic status Montevideo, Uruguay, 2003. Odontoestomatología. (2009) 11(13):27–36. Available at: http://hdl.handle.net/20.500.12008/2624
115. García Righetti G, Caviglia Acosta y Lara I, Lorenzo S, Massa F, Álvarez L. Caries dental en preescolares: estudio transversal de base poblacional en Montevideo, Uruguay. Odontoestomatología. (2023) 25(41):e228. doi: 10.22592/ode2023n41e228
116. El Tantawi M, Nabil N. 116. Law 17.823 on children and adolescents, República Oriental del Uruguay 2004. Available at: http://sip.parlamento.gub.uy/leyes/AccesoTextoLey.asp?Ley=17823 (Accessed April 21, 2023).
117. Law 18. 211. Uruguay 2007. Creation of the National Health System. Available at: https://www.impo.com.uy/bases/leyes/18211-2007/61 (Accessed April 21, 2023).
118. WHO EMRO | Egypt releases results of epidemiological study on oral health status | Egypt-events | Egypt. (2014). Available at: https://www.emro.who.int/egy/egypt-events/results-of-epidemiological-study-on-oral-health-status-released.html (Accessed March 10, 2023).
119. The National Strategy for Combating Violence against Women Title of Book: The National Strategy for Combating Violence against Women. (2015). Available at: www.ncwegypt.com (Accessed March 1, 2023).
120. Child Law of Egypt (document, English) | Women’s Learning Partnership. (2008). Available at: https://learningpartnership.org/resource/child-law-egypt-document-english (Accessed March 9, 2023).
121. The Cabinet The National Council For Childhood And Motherhood Law No. 12 Of 1996 Promulgating The Child Law Amended By Law No. 126 Of 2008. Available at: http://www.nccm-egypt.org/e7/e2498/e2691/infoboxContent2692/ChildLawno126english_eng.pdf (Accessed March 1, 2023).
122. Child Helpline 16000. (2005). Available at: http://www.nccm-egypt.org/e11/e3189/index_eng.html (Accessed March 1, 2023).
123. United Nations Study on Violence against Children Response to the questionnaire received from the Government of the Arab Republic of EGYPT. (2007). Available at: https://www.ohchr.org/sites/default/files/Documents/HRBodies/CRC/StudyViolenceChildren/Responses/Egypt.pdf (Accessed March 1, 2023).
124. El Tantawi M, Nabil N, Mahmoud SH, Elhendawy F. Capability, opportunity, motivation, and behaviour (COM-B) model association with Egyptian dentists’ reporting of suspected abuse. BMC Oral Health. (2022) 22(1):55. doi: 10.1186/s12903-022-02094-5
125. Khattab A, Beltagy T. Dentists’ knowledge of and attitudes toward recognizing and reporting child abuse and neglect in Egypt. Egypt Dent J. (2011) 57:3524. I.S.S.N 0070-9484.
126. The Universal Health Insurance Project. Available at: https://www.presidency.eg/en/ (Cited April 21, 2023).
127. Shoaee S, Saeedi Moghaddam S, Masinaei M, Sofi-Mahmudi A, Hessari H, Heydari MH, et al. Trends in dental caries of deciduous teeth in Iran: a systematic analysis of the national and sub-national data from 1990 to 2017. BMC Oral Health. (2022) 22:634. doi: 10.1186/s12903-022-02634-z
128. Khoshnevisan M.H, Ghasemianpour M, Samadzadeh H, and Baez RJ. Oral health status and healthcare system in I.R. Iran. J Contemp Med Sci. (2018) 4:107–18. https://www.jocms.org/index.php/jcms/article/view/460
129. Iran welfare organization. Available at: https://www.behzisti.ir (Accessed March 13, 2023).
130. The constitution of the Islamic Republic of Iran (in Persian). Available at: https://www.shora-gc.ir/files/fa/news/1398/9/21/4354_236.pdf (Accessed March 12, 2023).
131. Iranian Association for Pediatric Dentistry (IAPD). Available at: http://iapd.ir (Accessed March 13, 2023).
132. Arheiam AA, Harris RV, Baker SR. Changes in dental caries and sugar intake before and during the conflict in Libya: a natural experiment. Community Dent Oral Epidemiol. (2020) 48(3):201–7. doi: 10.1111/cdoe.12526
133. Ballo L, Arheiam A, Marhazlinda J. Determinants of caries experience and the impact on the OHRQOL of 6-year-old Libyan children: a cross-sectional survey. BMC Oral Health. (2021) 21(1):320. doi: 10.1186/s12903-021-01681-2
134. Arheiam AA, Elareibi I, Elatrash A, Baker SR. Prevalence and factors associated with traumatic dental injuries among schoolchildren in war-torn Libya. Dent Traumatol. (2020) 36(2):185–91. doi: 10.1111/edt.12529
135. Arheiam A, Aloshiby A, Gaber A, Fakron S. Dental fluorosis and its associated factors amongst Libyan schoolchildren. Int Dent J. (2022) 72(6):853–8. doi: 10.1016/j.identj.2022.04.010
136. Arheiam A, Abbas S, Ballo L, Borowis E, Rashwan S, El Tantawi M. Prevalence, distribution, characteristics and associated factors of molar-incisor hypo-mineralisation among Libyan schoolchildren: a cross-sectional survey. Eur Arch Paediatr Dent. (2021) 22(4):595–601. doi: 10.1007/s40368-020-00594-y
137. Al-Batayneh OB, Al-Khateeb HO, Ibrahim WM, Khader YS. Parental knowledge and acceptance of different treatment options for primary teeth provided by dental practitioners. Front Public Health. (2019) 7:322. doi: 10.3389/fpubh.2019.00322
138. Save the Children Fund. UN Convention for the right of the child. Available at: https://www.savethechildren.org.uk/what-we-do/childrens-rights/united-nations-convention-of-the-rights-of-the-child (Accessed April 14, 2023).
139. Children of Jordan. Why do we need a child rights law in Jordan? Available at: https://www.childrenofjordan.org/en/why-do-we-need-a-child-rights-law-in-jordan/ (Accessed April 14, 2023).
140. Children of Jordan. An Overview. Available at: https://www.childrenofjordan.org/en/children-of-jordan/ (Accessed April 14, 2023).
141. Pledge by Jordan, Convention on the Rights of the Child (CRC). Available at: https://www.ohchr.org/en/treaty-bodies/crc/celebrating-30-years-convention-rights-child/pledge-jordan (Accessed April 9, 2023)
142. Nasrawin L. Protection against domestic violence in Jordanian law and international conventions. Arab Law Quarterly. (2017) 31(4):363–87. Available at: https://www.jstor.org/stable/26567164 doi: 10.1163/15730255-12314047
143. Al-Darwish M, El Ansari W, Bener A. Prevalence of dental caries among 12-14 year old children in Qatar. Saudi Dent J. (2014) 26(3):115–25. doi: 10.1016/j.sdentj.2014.03.006
144. Al-Thani MH, Al-Thani AA, Al-Emadi AA, Al-Chetachi WF, Akram H, Poovelil BV. Oral health status of six-year-old children in Qatar: findings from the national oral health survey. Int J Dent Hyg. (2018) 16(2):225–32. doi: 10.1111/idh.12258
145. Alkhtib A, Ghanim A, Temple-Smith M, Messer LB, Pirotta M, Morgan M. Prevalence of early childhood caries and enamel defects in four and five-year old qatari preschool children. BMC Oral Health. (2016) 16(1):73. doi: 10.1186/s12903-016-0267-z
146. Almeezan. Law No. 11 of 2004 Issuing the Penal Code. Exposing children to danger, 269 Article. Ministry of Justice, Qatar. (2004).
147. Ministry of Justice. The Permanent Constitution of the State of Qatar. Available at: https://www.almeezan.qa/LawArticles.aspx?LawArticleID=25775&LawId=2284&language=en (Accessed April 9, 2023).
148. Sidra Medicine. Sidra Child Advocacy Program(S-CAP): Qatar Child Abuse Protection Services. Available at: https://www.sidra.org/clinics-services/childrens-and-young-people/child-safety-and-advocacy/sidra-child-advocacy-program (Accessed April 9, 2023).
149. Loochtan RM, Bross DC, Domoto PK. Dental neglect in children: definition, legal aspects, and challenges. Pediatr Dent. (1986) 8(1 Spec No):113–6. 3460034
150. AlDosari AM, Akpata ES, Khan N. Associations among dental caries experience, fluorosis, and fluoride exposure from drinking water sources in Saudi Arabia. J Public Health Dent. (2010) 70(3):220–6. doi: 10.1111/j.1752-7325.2010.00169.x
151. Al Agili DE. A systematic review of population-based dental caries studies among children in Saudi Arabia. Saudi Dent J. (2013) 25:3–11. doi: 10.1016/j.sdentj.2012.10.002
152. Al Agili DE, Farsi NJ. Need for dental care drives utilisation of dental services among children in Saudi Arabia. Int Dent J. (2020) 70:183–92. doi: 10.1111/idj.12539
153. Child Maltreatment Prevention Readiness Assessment Country Report: Saudi Arabia. Available at: https://www.who.int/violence_injury_prevention/violence/child/saudi_arabia_rap_cm.pdf.pdf (Accessed March 28, 2023).
154. Sabbagh HJ, Aljehani SA, Abdulaziz BM, Alshehri NZ, Bajkhaif MO, Alrosini SK, et al. Oral health needs and barriers among children in Saudi Arabia. Int J Environ Res Public Health. (2022) 19(20):13584. doi: 10.3390/ijerph192013584
155. Hamasha AA-H, Aldosari MN, Alturki AM, Aljohani SA, Aljabali IF, Alotibi RF. Barrier to access and dental care utilization behavior with related independent variables in the elderly population of Saudi Arabia. J Int Soc Prev Commun Dent. (2019) 9:349–55. doi: 10.4103/jispcd.JISPCD_21_19
156. Shubayr MA, Kruger E, Tennant M. Access to dental-care services in jazan, Saudi Arabia: a scoping review. Saudi J Health Syst Res. (2022) 2:9–19. doi: 10.1159/000517661
157. Taormina M, Montal S, Maitre Y, Tramini P, Moulis E. Perception of dental caries and parental difficulties in implementing oral hygiene for children aged less than 6 years: a qualitative study. Dent J. (2020) 8:62. doi: 10.3390/dj8030062
158. Ministry of Social Affairs. Law of Protection from Abuse. Bureau of Experts at the Council of Ministers; Riyadh, Saudi Arabia: 2013. Available at: https://www.nfsp.org.sa/ar/awareness/DocLib/english_law.pdf (Accessed March 12, 2023).
159. Awareness platform in Ministry of Health, Saudi Arabia. Child’s health. Child dental care. Available at: https://www.moh.gov.sa/en/awarenessplateform/ChildsHealth/Pages/ChildrenDentalCare.aspx (Accessed March 12, 2023).
160. Ministry of Human resources and social development, Saudi Arabia, 2022. Regulations for the Child Protection System. Available at: https://www.hrsd.gov.sa/en/knowledge-centre/decisions-and-regulations/regulation-and-procedures/70775 (Accessed March 12, 2023).
161. Almuneef M, Al-Eissa M. Preventing child abuse and neglect in Saudi Arabia: are we ready? Ann Saudi Med. (2011) 31(6):635–40. doi: 10.4103/0256-4947.87102
162. Mogaddam M, Kamal I, Merdad L, Alamoudi N. Knowledge, attitudes, and behaviors of dentists regarding child physical abuse in jeddah, Saudi Arabia. Child Abus Negl. (2016) 54:43–56. doi: 10.1016/j.chiabu.2016.02.004
163. Al-Dabaan R, Newton JT, Asimakopoulou K. Knowledge, attitudes, and experience of dentists living in Saudi Arabia toward child abuse and neglect. Saudi Dent J. (2014) 26(3):79–87. doi: 10.1016/j.sdentj.2014.03.008
164. Al-Dabaan R, Asimakopoulou K, Newton JT. Effectiveness of a web-based child protection training programme designed for dental practitioners in Saudi Arabia: a pre- and post-test study. Eur J Dent Educ. (2015) 20:45–54. doi: 10.1111/eje.12141
165. Campus G, Solinas G, Cagetti MG, Senna A, Minelli L, Majori S, et al. National pathfinder survey of 12-year-old children’s oral health in Italy. Caries Res. (2007) 41(6):512–7. doi: 10.1159/000110884
166. Campus G, Solinas G, Strohmenger L, Cagetti MG, Senna A, Minelli L, Majori S, Montagna MT, Reali D, Castiglia P; Collaborating Study Group. National pathfinder survey on children’s oral health in Italy: pattern and severity of caries disease in 4-year-olds. Caries Res. (2009) 43(2):155–62. doi: 10.1159/000211719
167. © Guarantor Authority for Childhood and Adolescence—CISMAI—Terre des Hommes Foundation Italy, 2021.
168. Maldupa I, Sopule A, Uribe SE, Brinkmane A, Senakola E. Caries prevalence and severity for 12-year-old children in Latvia. Int Dent J. (2021) 71(3):214–23. doi: 10.1111/idj.12627
169. Maldupa I, Uribe S. Trends in dental treatment under general anaesthesia for children in Latvia 2005-2020—Dataset. Epub ahead of print 2023. doi: 10.48510/FK2/LUUOMS
170. LIKUMI.LV. https://likumi.lv/ta/id/49096-bernu-tiesibu-aizsardzibas-likums (Accessed April 13, 2023).
171. LIKUMI.LV. https://likumi.lv/ta/id/90223-civillikums-pirma-dala-gimenes-tiesibas (Accessed April 14, 2023).
172. Behmane D, Dudele A. The Concept Of Value-Based Healthcare In Latvia. © The American Chamber of Commerce in Latvia © Riga Stradins University. (2022).
173. Markovic D, Soldatovic I, Vukovic R, Peric T, Campus GG, Vukovic A. How much country economy influences ECC profile in serbian children-A macro-level factor analysis. Front Public Health. (2019) 7:285. doi: 10.3389/fpubh.2019.00285
174. Batut MJ. Analysis of planned and used primary health care coverage in 2017, 2018. Institute of Public Health of Serbia).
175. International Society for Prevention of Child Abuse and Neglect. Intersectoral Approach to Child Maltreatment, draft. ISPCAN. (2003).
176. World Health Organization. Report on Consultation on Child Abuse Prevention. Geneva, World Health Organization, document WHO/HSC/PVI/99.1. (1999).
177. Filipovic Simic V, Stevanovic M, Hamzagic N, Lekovic E. Dental neglect—case report (abstract in serbian). Spring symposium of pediatric dentistry, Belgrade, Serbia, (abstract book). Belgrade, Serbia: Association of Paediatric and Preventive Dentists of Serbia (2019). p. 38.
178. National Strategy on Abuse Prevention and Child Protection in the Republic of Serbia. The Official Gazette. (2020);80.
179. PHE. Inequality in Oral Health. 2021. Public Health England. Available at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/970380/Inequalities_in_oral_health_in_England.pdf (Accessed April 14, 2023).
180. Shaban R, Kassim S, Sabbah W. Socioeconomic inequality in the provision of specific preventive dental interventions among children in the UK: children’s dental health survey 2003. BDJ. (2017) 222(11):865–9. doi: 10.1038/sj.bdj.2017.499
181. Sarri G, Marcenes W. Child dental neglect: is it a neglected area in the UK? BDJ. (2012) 213:103–4. doi: 10.1038/sj.bdj.2012.668
183. NICE. Child abuse and neglect. (2017). NICE guidelines. Available at: https://www.nice.org.uk/guidance/ng76 (Accessed April 14, 2023).
184. Harris J C, Elcock C, Sidebotham P D, Welbury R R. Safeguarding children in dentistry: 2. Do paediatric dentists neglect child dental neglect? Br Dent J. (2009) 206:465–70. doi: 10.1038/sj.bdj.2009.356
185. Harris JC, Baker SR, Elcock C. Paediatric dentists’ role in child protection practice: progress over time? Int J Paediatr Dent. (2022) 32(5):714–23. doi: 10.1111/ipd.12950
186. PHE. Health matters: child dental health. (2017). Public Health England. Available at: https://www.gov.uk/government/publications/health-matters-child-dental-health/health-matters-child-dental-health (Accessed April 14, 2023).
187. UK Public general Acts. Children Act 1989. UK Legislation. (2023). Available at: https://www.legislation.gov.uk/ukpga/1989/41/contents (Accessed April 14, 2023).
188. Ganesh A, Muthu MS, Mohan A, Kirubakaran R. Prevalence of early childhood caries in India—a systematic review. Indian J Pediatr. (2019) 86(3):276–86. doi: 10.1007/s12098-018-2793-y
189. Tewari N, Mathur VP, Siddiqui I, Morankar R, Verma AR, Pandey RM. Prevalence of traumatic dental injuries in India: a systematic review and meta-analysis. Indian J Dent Res. (2020) 31(4):601–14. doi: 10.4103/ijdr.IJDR_953_19
190. Mathur A, Mathur A, Aggarwal VP. Dental neglect affecting oral health Status in India. Int J Pediatr Res. (2016) 2:016. doi: 10.23937/2469-5769/1510016
191. Mohanan TV S, Sankeshwari RM, Ankola AV. Perspectives towards child abuse and neglect among dental practitioners in belagavi city: a cross-sectional study. J Educ Health Promot. (2020) 9:295. doi: 10.4103/jehp.jehp_244_20
192. Jani N. Article 21 of constitution of India and right to livelihood. Voice Res. (2013) 2(2):61–6. ISSN: 2277-7733.
193. Dasgupta S. Child welfare legislation in India: will Indian children benefit from the united nations convention on the rights of the child. Mich J Intl L. (1989) 11:1301. Available at: https://repository.law.umich.edu/mjil/vol11/iss4/9 (Accessed April 24 2023).
194. Ministry of Health Republic Indonesia. Basic Health Survey. (2019). Available at: https://www.litbang.kemkes.go.id/laporan-riset-kesehatan-dasar-riskesdas/ (Accessed November 6, 2021).
195. Gildasya G, Riyanti E, Hidayat S. Prevalence of oral habits in homeless children under care of yayasan bahtera bandung. Dent J. (2006) 39(4):165–7. doi: 10.20473/j.djmkg.v39.i4.p165-167
196. Berliana SM, Augustia AW, Rachmawati PD, Retnayu Pradanie R, Efendi F, Aurizki GE. Factors associated with child neglect in Indonesia: findings from national socio-economic survey. Child Youth Serv Rev. (2019) 106:10448. doi: 10.1016/j.childyouth.2019.104487
197. Law of the Republic Indonesia No. 23 of 2002 concerning child protection. Available at: https://peraturan.bpk.go.id/Home/Details/44473/uu-no-23-tahun-2002 (Accessed March 10, 2023, In Bahasa).
198. Law of the Republic Indonesia No. 35 of 2014 concerning Amendments to Law Number 23 of 2002 Concerning Child Protection. Available at: https://peraturan.bpk.go.id/Home/Details/38723/uu-no-35-tahun-2014 (Accessed March 10, 2023, In Bahasa).
199. Li F, Wu SC, Zhang ZY, Lo ECM, Gu WJ, Tao DY. Trend on dental caries status and its risk indicators in children aged 12 years in China: a multilevel analysis based on the repeated national cross-sectional surveys in 2005 and 2015. BMC Public Health. (2021) 21(1):2285. doi: 10.1186/s12889-021-12262-x
200. Du MQ, Li Z, Jiang H, Wang X, Feng XP, Hu Y. Dental caries Status and its associated factors among 3- to 5-year-old children in China: a national survey. Chin J Dent Res. (2018) 21(3):167–79. doi: 10.3290/j.cjdr.a41076
201. Chen L, Hong J, Xiong D, Zhang L, Li Y, Huang S. Are parents’ education levels associated with either their oral health knowledge or their children’s oral health behaviors? A survey of 8446 families in Wuhan. BMC Oral Health. (2020) 20(1):203. doi: 10.1186/s12903-020-01186-4
202. He J, Liang H, Kang J, Yuan C. Subgroup detection-based dental caries status and inequalities trend exploration: a nationwide, 10-year-repeated cross-sectional study. Front Public Health. (2022) 10:916878. doi: 10.3389/fpubh.2022.916878
203. Tan X, Liu X, Shao H. Healthy China 2030: a vision for health care. Value Health Reg Issues. (2017) 12:112–4. doi: 10.1016/j.vhri.2017.04.001
204. Order of the President of the People’s Republic of China No. 57. Law of the People’s Republic of China on Protection of Minors. (2020). Available at: http://www.npc.gov.cn/englishnpc/c23934/202109/39cab704f98246afbed02aed50df517a.shtml (Cited March 13, 2023).
205. Duangthip D, Chen KJ, Gao SS, Lo ECM, Chu CH. Early childhood caries among 3- to 5-year-old children in Hong Kong. Int Dent J. (2019) 69(3):230–6. doi: 10.1111/idj.12455
206. Zheng FM, Yan IG, Duangthip D, Gao SS, Lo ECM, Chu CH. Prevalence of untreated early childhood caries of 5-year-old children in Hong Kong: a cross-sectional study. Int J Environ Res Public Health. (2021) 18(22):11934. doi: 10.3390/ijerph182211934
207. Department of Health, The Government of the Hong Kong Special Administrative Region. Oral Health Survey 2011 Hong Kong. Available at: https://www.toothclub.gov.hk/en/en_pdf/Oral_Health_Survey_2011/Oral_Health_Survey_2011_WCAG_20141112_(EN_Full).pdf
208. Gao SS, Duangthip D, Lo ECM, Chu CH. Risk factors of early childhood caries among young children in Hong Kong: a cross-sectional study. J Clin Pediatr Dent. (2018) 42(5):367–72. doi: 10.17796/1053-4625-42.5.8
209. Constitutional and Mainland Affairs Bureau, The Goverment of the Hong Kong Special Administrative Region. Convention on the Rights of the Child. Hong Kong. (2009). Available at: https://www.cmab.gov.hk/doc/en/documents/policy_responsibilities/CRC_comic.pdf
210. Hong Kong Police Force, The Government of the Hong Kong Special Administrative Region. Child Protection Policy Unit (CPPU) 2023. Available at: https://www.police.gov.hk/ppp_en/04_crime_matters/child/cppu.html
211. Social Welfare Department, The Government of the Hong Kong Special Administrative Region. Family and Child Protective Services 2023. Available at: https://www.swd.gov.hk/en/index/site_pubsvc/page_family/sub_listofserv/id_familyandc/#:∼:text=FCPSUs%20provide%20services%20to%20children,casework%20and%20group%20work%20services
212. Hong Kong Legal Information Institute, The Government of the Hong Kong Special Administrative Region. Cap 212 offences against the person ordinance Section 27 Ill-treatment or neglect by those in charge of child or young person 2023. Available at: https://www.hklii.hk/eng/hk/legis/ord/212/s27.html
213. McGrath C, Sham AS, Ho DK, Wong JH. The impact of dental neglect on oral health: a population based study in Hong Kong. Int Dent J. (2007) 57(1):3–8. doi: 10.1111/j.1875-595X.2007.tb00111.x
214. Burgette JM, Safdari-Sadaloo SM, Van Nostrand E. Child dental neglect laws: specifications and repercussions for dentists in 51 jurisdictions. J Am Dent Assoc. (2020) 151(2):98–107.e5. doi: 10.1016/j.adaj.2019.09.010
215. UK Public general Acts. Children Act 1989. UK Legislation. (2023). https://www.legislation.gov.uk/ukpga/1989/41/contents
216. Jean G, Kruger E, Lok V. Oral health as a human right: support for a rights-based approach to oral health system design. Int Dent J. (2021) 71(5):353–7. doi: 10.1016/j.identj.2020.12.021
217. Hunt P. Interpreting the international right to health in a human rights-based approach to health. Health Hum Rights. (2016) 18(2):109–30. 28559680; PMCID: PMC539499628559680
218. Lansford JE, Godwin J, Uribe Tirado LM, Zelli A, Al-Hassan SM, Bacchini D, et al. Individual, family, and culture level contributions to child physical abuse and neglect: a longitudinal study in nine countries. Dev Psychopathol. (2015) 27(4 Pt 2):1417–28. doi: 10.1017/S095457941500084X
219. McCurdy K. The influence of support and stress on maternal attitudes. Child Abuse Negl. (2005) 29(3):251–68. doi: 10.1016/j.chiabu.2004.12.007
220. Bradbury-Jones C, Innes N, Evans D, Ballantyne F, Taylor J. Dental neglect as a marker of broader neglect: a qualitative investigation of public health nurses’ assessments of oral health in preschool children. BMC Public Health. (2013) 13:370. doi: 10.1186/1471-2458-13-370
221. Valencia-Rojas N, Lawrence HP. Goodman D: prevalence of early childhood caries in a population of children with history of maltreatment. J Public Health Dent. (2008) 68(2):94–101. doi: 10.1111/j.1752-7325.2007.00077.x
222. Greene P, Chisick M. Aaron G: a comparison of oral health status and need for dental care between abused/neglected children and nonabused/non-neglected children. Pediatr Dent. (1994) 16(1):41–5. 8015941
223. Moore MH. Public health and criminal justice approaches to prevention. In: Crime and justice, vol. 19. Chicago: University of Chicago Press, University of Chicago (1995). p. 237–62.
224. Condry R, Minson S. Conceptualizing the effects of imprisonment on families: collateral consequences, secondary punishment, or symbiotic harms? Theor Criminol. (2021) 25(4):540–58. doi: 10.1177/1362480619897078
225. Long T, Lockwood K, Loucks N, Nugent B, Raikes B, Sharratt K, et al. Improving outcomes for children affected by parental involvement with the criminal justice system in Scotland. Appl Res Qual Life. (2022) 17:1883–908. doi: 10.1007/s11482-021-10012-0
226. Prothrow-Stith D. Strengthening the collaboration between public health and criminal justice to prevent violence. J Law Med Ethics. (2004) 32:82–8. doi: 10.1111/j.1748-720x.2004.tb00451.x
227. Simons D, Pearson N, Evans P. A pilot of a school-based dental treatment programme for vulnerable children with possible dental neglect: the Back2School programme. Br Dent J. (2013) 215:E15. doi: 10.1038/sj.bdj.2013.998
228. Olonisakin TT, Ogunleye AJ, Adebayo SO. The Nigeria criminal justice system and its effectiveness in criminal behaviour control: a social-psychological analysis. IOSR J Hum Soc Sci. (2017) 22(2):33–48. doi: 10.12816/0052295
229. Sheiham A. Dental caries affects body weight, growth and quality of life in pre-school children. Br Dent J. (2006 Nov 25) 201(10):625–6. doi: 10.1038/sj.bdj.4814259
230. Liu YCG, Shieh TY, Teng AY. Is caries an independent risk factor for the child’s psychomotor development? A new insight to potentially shed the underlying mechanisms. J Dent Sci. (2018) 13:179–81. doi: 10.1016/j.jds.2018.07.001
Keywords: child abuse, oral health, human rights, legislation, public health
Citation: Foláyan MO, Ramos-Gomez F, Fatusi OA, Nabil N, Lyimo GV, Minja IK, Masumo RM, Mohamed N, Potgieter N, Matanhire C, Maposa P, Akino CR, Adeniyi A, Mohebbi SZ, Ellakany P, Chen J, Amalia R, Iandolo A, Peedikayil FC, Aravind A, Al-Batayneh OB, Khader YS, Al-Maweri SA, Sabbah W, Abeldaño Zuñiga RA, Vukovic A, Jovanovic J, Jafar RM, Maldupa I, Arheiam A, Mendes FM, Uribe SE, López Jordi MC, Villena RS, Duangthip D, Sam-Agudu NA and El Tantawi M (2023) Child dental neglect and legal protections: a compendium of briefs from policy reviews in 26 countries and a special administrative region of China. Front. Oral. Health 4:1211242. doi: 10.3389/froh.2023.1211242
Received: 24 April 2023; Accepted: 26 September 2023;
Published: 20 October 2023.
Edited by:
Gillian Lee, The University of Hong Kong, Hong Kong, SAR ChinaReviewed by:
Chloe Meng Jiang, The University of Hong Kong, Hong Kong, SAR ChinaPrathip Phantumvanit, Thammasat University, Thailand
© 2023 Foláyan, Ramos-Gomez, Fatusi, Nabil, Lyimo, Minja, Masumo, Mohamed, Potgieter, Matanhire, Maposa, Akino, Adeniyi, Mohebbi, Ellakany, Chen, Amalia, Iandolo, Peedikayil, Aravind, Al-Batayneh, Khader, Al-Maweri, Sabbah, Abeldaño Zuñiga, Vukovic, Jovanovic, Jafar, Maldupa, Arheiam, Mendes, Uribe, López Jordi, Villena, Sam-Agudu and El Tantawi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Moréniké Oluwátóyìn Foláyan dG95aW51a3BvbmdAb2F1aWZlLmVkdS5uZw==