
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oral. Health, 31 May 2023
Sec. Oral and Maxillofacial Surgery
Volume 4 - 2023 | https://doi.org/10.3389/froh.2023.1196813
This article is part of the Research TopicTechnological Innovations for Improved Prevention and Diagnosis of Oral DiseaseView all 5 articles
 Rosanna Guarnieri*†
Rosanna Guarnieri*† Camilla Grenga†
Camilla Grenga† Federica Altieri†Federica RocchettiErsilia Barbato†Michele Cassetta†
Federica Altieri†Federica RocchettiErsilia Barbato†Michele Cassetta†
Orthodontics has considerably increased the use of technology combined with surgery as a tool to improve dental movements in terms of predictability, acceleration of movement, and fewer side effects. To achieve these goals miniscrews and corticotomy were introduced. The digital workflow permits an increase in the accuracy of surgical and orthodontic setups. The tool that transfers the information is the CAD/CAM (Computer-Aided Design/ Computer-Aided Manufacturing) template. The aim of this review is to illustrate the use of computer-guided surgery in orthodontics regarding miniscrews and piezocision. The search strategy was a combination of Medical Subject Headings (Mesh) and free text words for PubMed. A total of 27 articles were included in this review: 16 concerned miniscrews and 11 concerned corticotomy. The current need for faster treatments, the improved systems of anchorage, and the evolution of imaging technologies require operators to be knowledgeable of the digital workflow. CAD/CAM templates allow greater precision and predictability of miniscrew insertion even if in the hands of less experienced clinicians and permit a better orientation and depth of the cortical incision. In conclusion, digital planning makes surgery faster and easier and allows for the identification and correction of any potential problem before the procedure.
Throughout history orthodontics has faced several periods and, recently, has considerably increased the use of technology combined with surgery to support the improvement in dental movements in terms of predictability, acceleration of movement, and fewer side effects (1).
To achieve these goals, TADs (Temporary Anchorage Devices) were introduced to move the teeth in a more specific way, minimizing side effects, such as the loss of anchorage when not planned. In addition, corticotomy interventions began being used to speed up tooth displacement, thus allowing a much shorter treatment time (1, 2).
Moreover, radiographic techniques have evolved from conventional two-dimensional (2-D) radiographs to computerized tomography (CT) and cone-beam state of the computerized tomography (CBCT), allowing the skeletal and dental structures to be reconstructed in a detailed and three-dimensional way (3).
The successive advent of intraoral scanners introduced a three-dimensional (3-D) vision of the dental arches in STL format (an acronym for “Standard Triangulation Language”); these data in STL format can be matched or overlapped with the three-dimensional information of the CBCT using dedicated software (4, 5). The integration of all these digital information results in a digital workflow that permits more details and accuracy of surgical and orthodontic setups. Finally, the tool that allows clinicians to transfer the information of the digital workflow is the template designed and manufactured with the help of computer support (CAD/CAM, Computer Aided Design / Computer Aided Manufacturing) (6). The digital manufacturing technology related to 3-D printing allows customization of the surgical guide and concomitantly greater precision and predictability of the surgical procedure selected, as in the case of insertion of miniscrews or in corticotomy cuts (7-10).
Orthodontic miniscrews provide skeletal anchorage, bypassing the patient's need for cooperation. For these reasons, their use has increased, as reported in several studies (11, 12). The boost in the use of miniscrews went hand in hand with the study of methods that would provide better stability during insertion, leading to greater success rates (3).
Surgical guides help clinicians to position dental implants with more accuracy and predictability. This also applies to mini-implants such as miniscrews or TADs in orthodontics (6).
Corticotomy-accelerated orthodontics (CAO), based on the principle of regional acceleratory phenomenon (RAP), allows for a faster movement of the teeth. Dibart et al. introduced an innovative surgical technique to achieve rapid tooth movements while preserving periodontal support without extensive surgical trauma: the piezocision. Piezocision is a flapless procedure characterized by multiple small mucoperiosteal vertical incisions and ultrasonic corticotomies done with piezoelectric inserts (2).
The piezocision procedure, as well as the insertion of miniscrews, is greatly enhanced using a 3-D CAD/CAM surgical guide that minimizes the potential risks, such as incidental contact of tooth roots or any critical structure.
This is the first narrative review to illustrate the state-of-the-art use and the evolution in the use of computer-guided surgery in orthodontics relating to miniscrews and corticotomies. We aim to provide an overview and general indications of 3-D CAD/CAM technology both regarding the insertion of miniscrews and the surgical procedure for the acceleration of tooth movements. It is important to highlight how the 3-D CAD/CAM technological advance should not substitute but improve the diagnosis in orthodontics.
The need for this review is to illustrate the benefits of computer-guided surgery, a safe and affordable tool, in an era where digitization has become essential for everyday clinical practice.
The literature search and study inclusion were carried out in duplicate by two review authors (R.G and C.G.). Any discrepancy was discussed with a third reviewer for consensus (M.C.).
The bibliographic research was carried out on Pubmed, MEDLINE (via Pubmed), EMBASE (via Ovid), Cochrane Reviews, and Cochrane Register of Controlled Trials (CENTRAL) from August 2022 until April 2023. The search strategy was a combination of Medical Subject Headings (Mesh) and free text words for PubMed and was optimized for each database. The details of the search strategy are summarized in Table 1. In addition, relevant journals and reference sections of retrieved studies were manually searched.
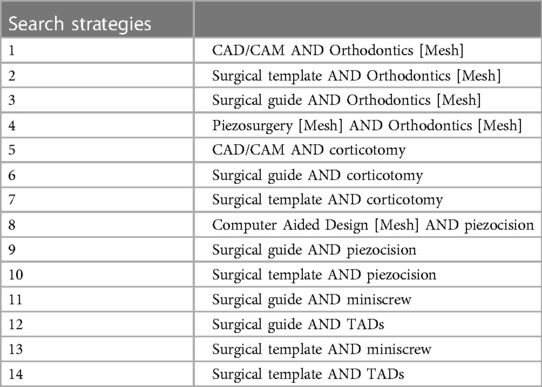
Table 1. Search strategies.
Randomized controlled trials (RCTs), quasi-RCT (Q-RCTs), controlled clinical trials (CCTs), unclear non-randomized studies (uNRS), prospective and retrospective studies, systematic reviews with and without meta-analysis, reviews, and case reports were included in this study. We decided to include case reports considering the small number of other kinds of studies relevant to the research topic. Eligibility criteria comprised articles published in English after 1990, and those that included a description of computer-guided surgery in orthodontics and a description of the digital workflow of computer-guided surgery in orthodontics. Exclusion criteria were: non-English language studies and FEM/laboratory/animal studies. Thus, studies dealing with the surgical template in the context of mini-screws and piezocision were analyzed.
A total of 1,795 studies were identified through the database search. Out of these, 863 were excluded as duplicates. Abstracts were read and 859 articles were excluded because they were not related (irrelevant) to the research that was being carried out.
The full texts of the remaining 73 articles were examined and 45 were excluded because they did not match the eligibility criteria: 5 of them were excluded because the full text was not in English, 40 studies were inconsistent with respect to the purpose of the study and 1 was based on animal tests. Finally, 27 articles were included in this review and qualitative synthesis. The selection procedure is represented in Figure 1.
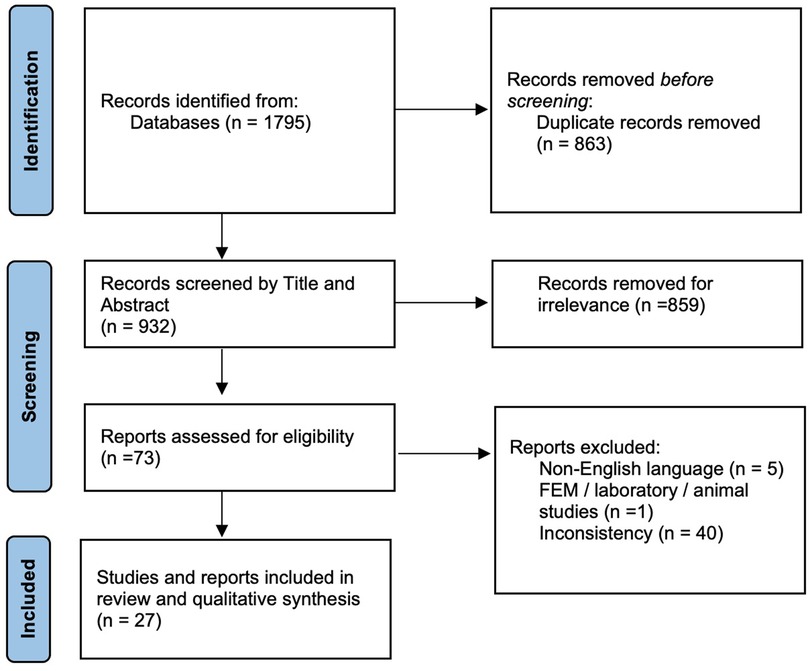
Figure 1. Flowchart of the study selection.
Of the 27 studies analyzed on computer-guided surgery, 16 concerned miniscrews and 11 concerned piezocision. Of these 27 studies, one was an RCT, four were CCTs, five were prospective studies, two were retrospective studies, one was a review, three were systematic reviews, and one was a systematic review with meta-analysis. Finally, there were 10 case reports. The data are summarized in Table 2. The qualitative synthesis then envisaged the structuring of two major paragraphs or relevant sections.
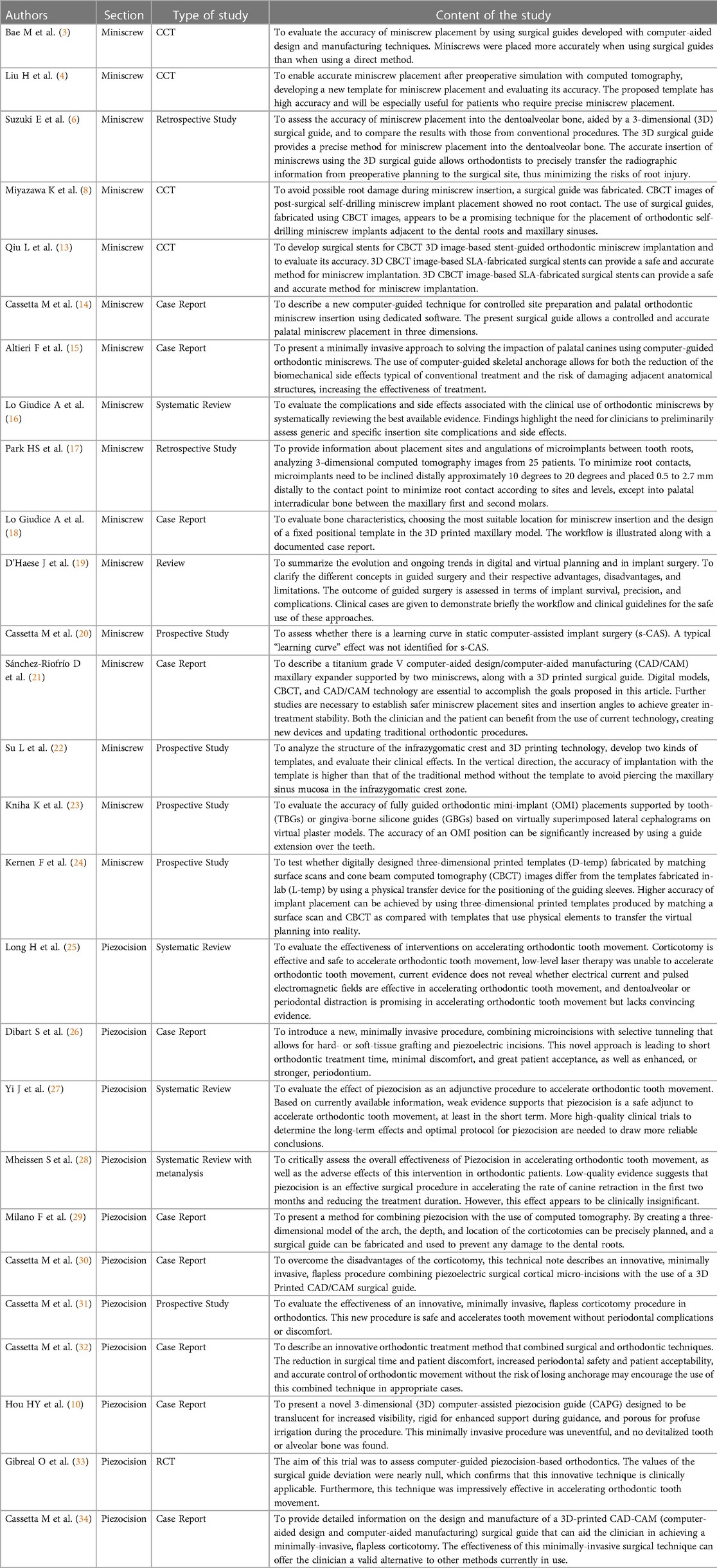
Table 2. Study types.
Anchorage is one of the essential elements for the success of orthodontic treatment. Traditionally, the teeth themselves or appliances have been used as intra and extraoral anchors, often relying on the patient's compliance for the success of the treatment (35). TADs are compliance-free and provide absolute anchorage during orthodontic treatment both directly and indirectly (13).
Currently, among the TADs, the most used anchoring devices are the miniscrews, which are positioned in the midsagittal area of the palate, in the retromolar area of the mandible, and also in the dentoalveolar area thanks to the reduced size of the diameter that allows the insertion between the roots of adjacent teeth (4). Miniscrews are relatively inexpensive, easy to insert and remove, versatile (they can be positioned in different areas of the maxilla and mandible), and, above all, they are predictable enough to be used routinely in clinical practice (14). The insertion areas can be interradicular and extra-radicular. Among the extra-radicular sites, the tuberosity of the maxilla, the zygomatic process, the chin region, the buccal shelf, and more frequently the anterior palate can be identified as areas of interest. The third palatine ruga is a reliable clinical reference point for assessing bone availability and thickness for the placement of miniscrews in the anterior palate (36-38).
Nowadays, miniscrews are widely used to improve the efficiency of dental movements (mesialization-distalization, intrusion-extrusion, retraction, and uprighting) decreasing the possible side effects of conventional treatments (15). Nevertheless, the clinical use of miniscrews is not free from potential unwanted effects and complications that may occur during insertion, use, and removal.
A complication that can occur during the insertion and removal of miniscrews, especially in the posterior region and in areas of very dense bone, is fracture or breakage of the miniscrew. The tendency to change the insertion angle by moving the handpiece or increasing torsional stress can lead to a fracture of the neck of the miniscrew (16). However, the most frequent complication reported in the literature is root damage during the interradicular insertion of the miniscrew. This complication can also occur during the insertion of the miniscrews in the anterior area of the palate. The most frequent side effects are pain, inflammation of soft and hard tissues, and hypertrophy of the peri-implant gingival tissue (3, 16). The miniscrew-tooth contact, and the lesion of the root, which can be of varying degrees of severity up to the loss of vitality of the dental element, can contribute to the early loss of the miniscrew. For these reasons, the insertion of miniscrews requires appropriate anatomical knowledge and radiographic evaluation to guide the clinician in determining the safest area for insertion. Regarding interradicular miniscrews, some authors recommend a positioning from 4 to 6 mm under the alveolar ridge with an angle from 30° to 45 ° with miniscrews that have a diameter between 1.2 and 1.6 and a length of 6-8 mm (3, 17). A good compromise in the use of interradicular miniscrews may be to consider an average miniscrew diameter of 1.5 mm and a minimum interradicular distance of 3 mm (39). Different methods have been proposed in order to achieve a precise and safe positioning for interradicular miniscrews. For example, the use of a radiopaque reference in an endoral 2D x-ray has been proposed in order to assess the mesiodistal distance of the roots (40). These methods based on two-dimensional image evaluation, however, cannot guarantee predictable and precise positioning due to the absence of three-dimensional programming and control in the miniscrew positioning (3).
A controllable, reliable, and reproducible method for miniscrew positioning is important for orthodontists and, nowadays, a CAD/CAM surgical guide can be a viable solution (2). CAD/CAM technology has been used in implantology to determine accurate positioning and to manufacture surgical guides for dental implant insertion. Computed tomography or Cone Beam Computer Tomography (CT or CBCT) is performed to assess bone quality and quantity, and implant position is determined based on 3D digital images that are reconstructed from CT or CBCT data (18).
It should be noted that the reconstruction of digital 3D images from computer tomography images alone is associated with image distortion of computed tomography or artifacts caused by metal in the mouth. To overcome these problems, it has been proposed and suggested to combine images of the dental arch, including both scanned images of plaster models and intraoral scanning data, with images of computed tomography (19).
The surgical guide is built starting from the STL files of the arches and the digital model images are fused with CT or CBCT images of the jaws using 3D software. On the STL 3D model file the ideal points for miniscrew insertion are identified and a software application is used for the design of the surgical guide. Then the 3D STL model of the surgical guide is printed using a 3D printer through stereolithography apparatus (SLA). SLA is the process of using laser-cured photosensitive resins layer by layer (2). A diagram of the digital workflow is summarized in Figure 2.
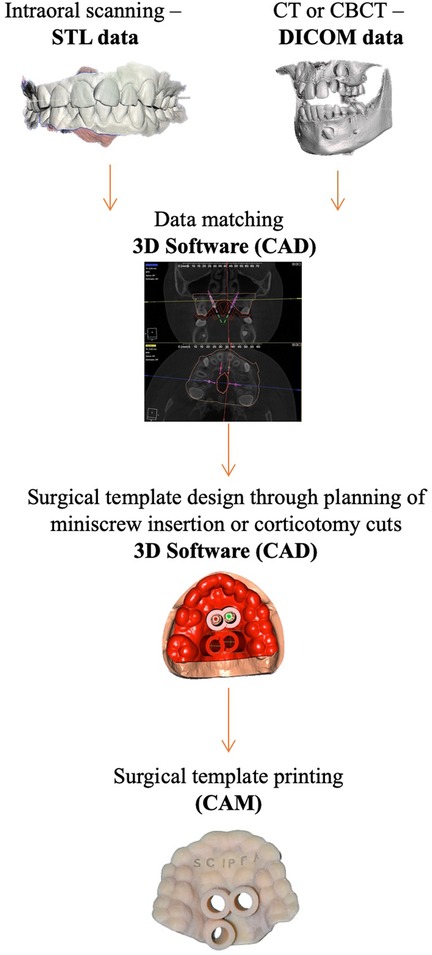
Figure 2. The workflow of computer-guided surgery in miniscrews insertion and corticotomies.
The CAD/CAM technology allows the clinician to design and plan everything in a single visit, while the 3D printed surgical guide allows the positioning of the miniscrews or the miniscrews together with the device on the same day, confirming their precise position according to the digital planning. The accuracy of this technique is discussed by Cassetta et al. and Sánchez-Riofrío et al. who highlighted that it lacks a “learning curve” effect, thus making it a simple procedure with a very low risk of failure (20, 21). CAD/CAM technology can therefore help less experienced clinically-surgical operators in safely positioning the miniscrews. Several studies show how the use of surgical templates allows bicortical anchorage during TADs insertion, improves primary stability, and reduces the risk of injury to contiguous anatomical structures (16, 18).
Qiu et al. compared the precision of insertion of miniscrews between a study group where insertion was computer guided and a control group where insertion was freehand; the results showed that no root had been touched with computer-guided insertion while in the freehand group, some miniscrews had come into contact with the root. The same study also demonstrated how the programmed insertion accuracy was highly more reliable in the study group than in the control group (13). Another study by Su et al. confirmed that the use of CAD/CAM templates can increase the accuracy of inserting miniscrews, thus reducing the risk of damaging adjacent structures (22). Similar results were reported by Suzuki et al. (4). In addition, Bae et al. observed that in the study group with guide placement of miniscrews, no miniscrews came into contact with the roots of the adjacent teeth (3); Miyazawa et al. found that the success rate of miniscrew placement was 90.9% when surgical guides were used (6).
The interradicular area of the maxilla is often too small for the placement of miniscrews, leading to the infrazygomatic crest being proposed as an alternative. The infrazygomatic crest has a double cortical layer and is close to the center of resistance of the maxilla, providing greater anchorage. However, it is adjacent to the maxillary sinus and the apical portion of the roots and the risk of injury is present. Therefore, the template is also very useful in cases of insertion into the infrazygomatic crest (22).
Surgical guides for TADs insertion can be manufactured in acrylic resin or in PMMA (Polymethyl methacrylate) and are anchored to the teeth mechanically or chemically. Depending on the characteristics (stiffness) of the template material, the retention tooth cover can be complete or partial with the addition of any retention hooks. The guide must be firmly anchored in order to avoid unwanted movement during the insertion of the miniscrews. In fact, many parameters potentially contribute to the accuracy of the insertion of the computer-guided miniscrews: radiographic inaccuracies, intraoral scanning, the production of the plasters, and surgical guide 3D printing (23, 24).
The insertion accuracy also depends on the transfer accuracy: generally, surgical guides can be supported by teeth, mucosa, bone, and implants, but for TADs insertion, dental support is preferable (16). Movements of the surgical guide might cause differences in the deviation during implant site preparation, for this reason, it is preferable to use sleeves (metal or polymeric material) inserted in the surgical template in order to direct the drill more precisely and without the risk of potential deviations during perforation (23).
In the placement of palatal miniscrews in deep and narrow palatine vaults, one difficulty that must be overcome is the convergence of the insertion axes of the miniscrews. In these cases, in order to achieve good insertion accuracy, two surgical templates are required to prevent the insertion handpiece from coming into contact with the template itself.
The use of surgical guides built with CAD/CAM technology is an important tool in the hands of a less experienced clinician and serves as an encouragement for the initial use of the miniscrews. In the hands of more experienced clinicians, surgical guides built with CAD/CAM technology increase the predictability of insertion (18).
The growing demand from adult patients for orthodontic treatment determined the development and the consequent evolution of methods and alternatives able to shorten the duration of the treatment. The absence of growth in adult patients also involves different therapeutic approaches: the phenomena of hyalinization and reduced cell mobilization during treatment are more frequent in subjects at the end of growth, and a lower conversion rate of the collagen fibers and an increased probability to develop periodontal complications are usual (41).
In a systematic review by Long et al. several novel modalities were reported to accelerate orthodontic tooth movement, including low-level laser therapy, pulsed electromagnetic fields, electrical currents, mechanical vibration, distraction osteogenesis, and corticotomy (42). The review showed that corticotomy is only effective and safe in accelerating orthodontic tooth movement (25). Other more recent reviews confirmed the effectiveness of corticotomy in accelerating orthodontic movement (43–45).
In the first decade of this century, Wilcko et al. proposed the corticotomy approach to accelerate orthodontic tooth movement. They called this method Accelerated Osteogenic Orthodontics (AOO) technique or, more precisely, Periodontally Accelerated Osteogenic Orthodontics (PAOO) technique (46). The technique consists of full-thickness flaps labially and lingually inserted in the zone in which the teeth will be moved. Then circumferential corticotomy cuts and intramarrow penetrations are made with rotating burs. Finally, the “activated” bone is covered with a particulate bone grafting mixture and the flaps are sutured to completely cover the surgical area. This procedure is based on the concept of regional acceleratory phenomenon (RAP) defined by Frost: immediately after corticotomy, during the healing process, there is transitory osteopenia responsible for the rapid tooth movement (47).
Many studies, also on experimental animals, have successively illustrated the effectiveness of the corticotomy technique in terms of shortening treatment time (48–51). The acceleration of the orthodontic tooth movements immediately after corticotomy seems to be attributed to increased bone turnover due to a greater number of osteoclasts in the stimulated area. In 2019, a review of the literature stated that alveolar corticotomies as an adjunct to orthodontic treatment can decrease total treatment time for the orthodontic patient (52).
In 2007, Vercellotti et al. and, in 2011, Bertossi et al. proposed a new surgical approach to the corticotomy: the use of a piezosurgical device to minimize the side effects of the traditional burs, so reducing the traumatism at the bone and ensuring better cutting precision, more predictable bone regeneration, and faster healing with minimal morbidity (53, 54). Dibart further perfected this technique, making it easier and less traumatic by removing the elevation flap. The technique was called Piezocision, which means a corticotomy performed with a piezosurgical device with or without bone graft and without flap elevation. Sutures are not required if a bone graft is not performed (26).
In a study conducted on rats in 2016, Han and He stated that the use of piezosurgery for the corticotomy used in accelerating the movement of the teeth during orthodontic treatment is associated with an increase of the bone morphogenetic protein-2 (BMP-2) (55). BMP-2 is a multifunctional growth factor that promotes the proliferation, differentiation, and apoptosis of many cells and is involved in the regeneration and repair of tissues, particularly bone tissues.
A systematic review, conducted in 2017, concerning the efficacy of piezocision on accelerating orthodontic tooth movement, stated that weak evidence supports that piezocision is a safe adjunct to accelerate orthodontic tooth movement and that more high-quality clinical trials are needed to draw more reliable conclusions (27). Furthermore, a systematic review with meta-analysis published in 2020 suggested that piezocision is an effective surgical procedure in accelerating tooth movement and in reducing the treatment duration even if further studies are needed (28).
The surgical cut of the bone is performed in an area of close root proximity and this is a potential risk for root damage. Moreover, corticotomy during piezocision is carried out flapless making it even more difficult to correctly identify the dental roots and their root tips.
During these last years, the introduction of more refined diagnostic techniques, such as the CBCT, has allowed a 3D reconstruction of the maxilla and the mandible, permitting very precise planning of the depth and location of the decortications. It is possible to transfer the CBCT data to a 3D printer in order to create a surgical guide that assures a more predictable flapless cut without potential risks to the dental root, which also reduces surgical treatment time. In 2014, Milano et al. published a case report illustrating a method for combining piezocision and CBCT to construct a surgical guide to make high-precision bone cuts. By creating a three-dimensional (3D) model of the arch, the depth and location of the corticotomies were planned and transferred to a resin surgical guide using a numerically controlled milling machine (29). Cassetta et al. successively illustrated in 2015, 2016, and 2017, as well as Hou et al. in 2019, the procedures to perform a 3D computer-assisted surgical guide (30–33). Finally, in a randomized controlled clinical trial, Gibreal et al. confirmed that computer-guided surgical templates are effective and clinically applicable tools (33).
First of all, the impressions must be taken with extreme precision trying to go as far as the reading of the fornix in order to then obtain adequate templates for the length of the corticotomy lines. The presence of orthodontic brackets during the impression could create inaccuracies for the subsequent construction of the template, but today this problem is solved by the intraoral scanner and the development of a digital model (5). During the impression phase, attention must be paid to the relief of the frenulum which could then complicate the correct insertion of the surgical guide (7). Furthermore, the use of transparent material to construct the surgical guide can facilitate a direct view of the operating field (8). To avoid damage to the mucosal tissue and alveolar bone, due to overheating during the computer-guided procedure, multiple pores and drain tubes can be performed on the surgical guide to allow copious saline irrigation to have greater access to the surgical guide (31, 34).
In addition, it is important to highlight how the use of CBCT in the planning phase of the intervention is an important tool in the identification of vascular-nervous structures, thus decreasing the risk of damage to these structures through the CAD/Cam template (56).
A limitation of corticotomy and piezocision is the additional surgery the orthodontic patient has to undergo; furthermore, this technique cannot predictably move ankylosed teeth or be performed in devitalized bone, a frequent situation in patients being treated with bisphosphonates or corticosteroids (57).
In conclusion, the use of a surgical guide during corticotomy and the piezocision technique can permit a better and more precise orientation and depth of the cortical incision. With the aid of a CBCT, it is also possible to perform cuts in areas where the cortical bone is thick, avoiding damage to the root of the teeth and limiting postoperative discomfort and complications.
Computer-guided surgery is not without its criticalities. It is always necessary to consider both the additional biological cost in the prescription of a second-level investigation such as CBCT and the possibility of complications that would not otherwise occur, such as the breakage of the surgical guide itself during its use (16). Considering the use of miniscrews in pediatric patients we refer to the DIMITRA project for indication-oriented and patient-specific recommendations regarding the main cone-beam CT applications in the pediatric field (58). Last but not least, a careful examination of the patient's condition is always necessary: a reduced mouth opening is a contraindication to the use of surgical templates due to the increased size of the mounting device with regard to the height of the surgical guide tube.
This is the first narrative review that offers an overview of computer-guided surgery for miniscrews and corticotomy in orthodontics using a standardized methodology and reporting on its practical applications and advantages. However, this review does not allow for analytical data. To date, there are few RCT, CCT, and very heterogeneous studies, which do not allow for a systematic review. It would be interesting to conduct studies with a standardized methodology and then conduct meta-analyses on the collected data and offer the reader an objective report of the results, for example with regard to the operator's comfort or not in using the computer-guided surgical template in orthodontics.
In addition, not having included studies in another language may have marred the quality of the work.
The current need for faster treatments, the improved systems of anchorage, and the evolution of imaging technologies for accurate diagnosis and treatment simulation require orthodontists to be knowledgeable of the digital workflow. The use of CAD/CAM templates allows greater precision and predictability of the surgical technique selected for the purpose of personalized orthodontic treatment. In this way it is possible to reduce the risk of injury to contiguous anatomical structures and to reduce surgical treatment time, allowing better comfort to the patient. This planning makes surgery faster and easier and allows any potential problems to be identified and corrected before the procedure.
Conceptualization, MC and EB; methodology, RG and CG; validation, RG; formal analysis, RG and FR; data curation, CG and FA; writing—original draft preparation, CG and RG; writing—review and editing, RG; visualization, MC and EB; supervision, MC All authors have read and agreed to the published version of the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ghafari JG. Centennial inventory: the changing face of orthodontics. Am J Orthod Dentofacial Orthop. (2015) 148(5):732–9. doi: 10.1016/j.ajodo.2015.08.011
2. Dibart S. Piezocision™: accelerating orthodontic tooth movement while correcting hard and soft tissue deficiencies; Front Oral Biol. (2016) 18:102–8. doi: 10.1159/000351903
3. Bae MJ, Kim JY, Park JT, Cha JY, Kim HJ, Yu HS, Hwang CJ. Accuracy of miniscrew surgical guides assessed from cone-beam computed tomography and digital models. Am J Orthod Dentofacial Orthop. (2013) 143(6):893–901. doi: 10.1016/j.ajodo.2013.02.018
4. Liu H, Liu DX, Wang G, Wang CL, Zhao Z. Accuracy of surgical positioning of orthodontic miniscrews with a computer-aided design and manufacturing template. Am J Orthod Dentofacial Orthop. (2010) 137(6):728.e1–728.e10. doi: 10.1016/j.ajodo.2009.12.025
5. Cassetta M, Altieri F, Guarnieri R, Padalino G, Mezio M, Barbato E. L’inserimento di miniviti palatali con dima chirurgica CAD/CAM: un caso clinico. Dent Cadmos. (2020) 88(10):691. doi: 10.19256/d.cadmos.10.2020.08
6. Suzuki EY, Suzuki B. Accuracy of miniscrew implant placement with a 3-dimensional surgical guide. J Oral Maxillofac Surg. (2008) 66(6):1245–52. doi: 10.1016/j.joms.2007.08.047
7. Cassetta M, Guarnieri R, Altieri F. The combined use of clear aligners and computer-guided piezocision: a case report with a 2-year follow-up. Int J Comput Dent. (2020) 23(1):57–71. PMID: 3220746232207462
8. Miyazawa K, Kawaguchi M, Tabuchi M, Goto S. Accurate Pre-surgical determination for self-drilling miniscrew implant placement using surgical guides and cone-beam computed tomography. Eur J Orthod. (2010) 32(6):735–40. doi: 10.1093/ejo/cjq012
9. Cassetta M, Ivani M. The accuracy of computer-guided piezocision: a prospective clinical pilot study. Int J Oral Maxillofac Surg. (2017) 46(6):756–65. doi: 10.1016/j.ijom.2017.02.1273
10. Hou H-Y, Li C-H, Chen M-C, Lin P-Y, Liu W-C, Cathy Tsai Y-W, Huang R-Y. A novel 3D-printed computer-assisted piezocision guide for surgically facilitated orthodontics. Am J Orthod Dentofacial Orthop. (2019) 155(4):584–91. doi: 10.1016/j.ajodo.2018.11.010
11. Brettin BT, Grosland NM, Qian F, Southard KA, Stuntz TD, Morgan TA, Marshall SD, Southard TE. Bicortical vs monocortical orthodontic skeletal anchorage. Am J Orthod Dentofacial Orthop. (2008) 134(5):625–35. doi: 10.1016/j.ajodo.2007.01.031
12. Mohammed H, Wafaie K, Rizk MZ, Almuzian M, Sosly R, Bearn DR. Role of anatomical sites and correlated risk factors on the survival of orthodontic miniscrew implants: a systematic review and meta-analysis. Prog Orthod. (2018) 19(1):36. doi: 10.1186/s40510-018-0225-1
13. Qiu L, Haruyama N, Suzuki S, Yamada D, Obayashi N, Kurabayashi T, Moriyama K. Accuracy of orthodontic miniscrew implantation guided by stereolithographic surgical stent based on cone-beam CT-derived 3D images. Angle Orthod. (2012) 82(2):284–93. doi: 10.2319/033111-231.1
14. Cassetta M, Altieri F, di Giorgio R, Barbato E. Palatal orthodontic miniscrew insertion using a CAD-CAM surgical guide: description of a technique. Int J Oral Maxillofac Surg. (2018) 47(9):1195–8. doi: 10.1016/j.ijom.2018.03.018
15. Altieri F, Padalino G, Guarnieri R, Barbato E, Cassetta M. Computer-Guided palatal canine disimpaction: a technical note. Int J Comput Dent. (2020) 23(3):219–24. PMID: 3278930932789309
16. Lo Giudice A, Rustico L, Longo M, Oteri G, Papadopoulos MA, Nucera R. Complications reported with the use of orthodontic miniscrews: a systematic review. Korean J Orthod. (2021) 51(3):199–216. doi: 10.4041/kjod.2021.51.3.199
17. Park H-S, HwangBo E-S, Kwon T-G. Proper mesiodistal angles for microimplant placement assessed with 3-dimensional computed tomography images. Am J Orthod Dentofacial Orthop. (2010) 137(2):200–6. doi: 10.1016/j.ajodo.2008.04.028
18. Lo Giudice A, Quinzi V, Ronsivalle V, Martina S, Bennici O, Isola G. Description of a digital work-flow for CBCT-guided construction of micro-implant supported maxillary skeletal expander. Materials (Basel). (2020) 13(8):1815. doi: 10.3390/ma13081815
19. D’haese J, Ackhurst J, Wismeijer D, de Bruyn H, Tahmaseb A. Current state of the art of computer-guided implant surgery. Periodontol 2000. (2017) 73(1):121–33. doi: 10.1111/prd.12175
20. Cassetta M, Altieri F, Giansanti M, Bellardini M, Brandetti G, Piccoli L. Is there a learning curve in static computer-assisted implant surgery? A prospective clinical study. Int J Oral Maxillofac Surg. (2020) 49(10):1335–42. doi: 10.1016/j.ijom.2020.03.007
21. Sánchez-Riofrío D, Viñas MJ, Ustrell-Torrent JM. CBCT And CAD-CAM technology to design a minimally invasive maxillary expander. BMC Oral Health. (2020) 20(1):303. doi: 10.1186/s12903-020-01292-3
22. Su L, Song H, Huang X. Accuracy of two orthodontic Mini-implant templates in the infrazygomatic crest zone: a prospective cohort study. BMC Oral Health. (2022) 22(1):252. doi: 10.1186/s12903-022-02285-0
23. Kniha K, Brandt M, Bock A, Modabber A, Prescher A, Hölzle F, Danesh G, Möhlhenrich SC. Accuracy of fully guided orthodontic mini-implant placement evaluated by cone-beam computed tomography: a study involving human cadaver heads. Clin Oral Investig. (2021) 25(3):1299–306. doi: 10.1007/s00784-020-03436-9
24. Kernen F, Benic GI, Payer M, Schär A, Müller-Gerbl M, Filippi A, Kühl S. Accuracy of three-dimensional printed templates for guided implant placement based on matching a surface scan with CBCT. Clin Implant Dent Relat Res. (2016) 18(4):762–8. doi: 10.1111/cid.12348
25. Long H, Pyakurel U, Wang Y, Liao L, Zhou Y, Lai W. Interventions for accelerating orthodontic tooth movement: a systematic review. Angle Orthod. (2013) 83(1):164–71. doi: 10.2319/031512-224.1
26. Dibart S, Sebaoun JD, Surmenian J. Piezocision: a minimally invasive, periodontally accelerated orthodontic tooth movement procedure. Compend Contin Educ Dent. (2009) 30(6):342–4, 346, 348–350. PMID: 1971501119715011
27. Yi J, Xiao J, Li Y, Li X, Zhao Z. Efficacy of piezocision on accelerating orthodontic tooth movement: a systematic review. Angle Orthod. (2017) 87(4):491–8. doi: 10.2319/01191-751.1
28. Mheissen S, Khan H, Samawi S. Is piezocision effective in accelerating orthodontic tooth movement: a systematic review and meta-analysis. PLoS One. (2020) 15(4):e0231492. doi: 10.1371/journal.pone.0231492
29. Milano F, Dibart S, Montesani L, Guerra L. Computer-Guided surgery using the piezocision technique. Int J Periodontics Restor Dent. (2014) 34(4):523–9. doi: 10.11607/prd.1741
30. Cassetta M, Pandolfi S, Giansanti M. Minimally invasive corticotomy in orthodontics: a new technique using a CAD/CAM surgical template. Int J Oral Maxillofac Surg. (2015) 44(7):830–3. doi: 10.1016/j.ijom.2015.02.020
31. Cassetta M, Giansanti M, di Mambro A, Calasso S, Barbato E. Minimally invasive corticotomy in orthodontics using a three-dimensional printed CAD/CAM surgical guide. Int J Oral Maxillofac Surg. (2016) 45(9):1059–64. doi: 10.1016/j.ijom.2016.04.017
32. Cassetta M, Altieri F, Pandolfi S, Giansanti M. The combined use of computer-guided, minimally invasive, flapless corticotomy and clear aligners as a novel approach to moderate crowding: a case report. Korean J Orthod. (2017) 47(2):130–41. doi: 10.4041/kjod.2017.47.2.130
33. Gibreal O, Al-Modallal Y, Mahmoud G, Gibreal A. The efficacy and accuracy of 3D-guided orthodontic piezocision: a randomized controlled trial. BMC Oral Health. 2023;23(1):181. doi: 10.1186/s12903-023-02902-6
34. Cassetta M, Giansanti M. Accelerating orthodontic tooth movement: a new, minimally-invasive corticotomy technique using a 3D-printed surgical template. Med Oral Patol Oral Cir Bucal. (2016) 21(4):e483–7. doi: 10.4317/medoral.21082
35. Bucur SM, Vaida LL, Olteanu CD, Checchi V. A brief review on micro-implants and their use in orthodontics and dentofacial orthopaedics. Appl. Sci. (2021) 11:10719–00. doi: 10.3390/app112210719
36. Ludwig B, Glasl B, Bowman SJ, Wilmes B, Kinzinger GSM, Lisson JA. Anatomical guidelines for miniscrew insertion: palatal sites. J Clin Orthod. (2011) 45(8):433–41; quiz 467. PMID: 2209472422094724
37. Hourfar J, Ludwig B, Bister D, Braun A, Kanavakis G. The most distal palatal Ruga for placement of orthodontic Mini-implants. Eur J Orthod. (2015) 37(4):373–8. doi: 10.1093/ejo/cju056
38. Hourfar J, Kanavakis G, Bister D, Schätzle M, Awad L, Nienkemper M, Goldbecher C, Ludwig B. Three dimensional anatomical exploration of the anterior hard palate at the level of the third Ruga for the placement of Mini-implants—a cone-beam CT study. Eur J Orthod. (2015) 37(6):589–95. doi: 10.1093/ejo/cju093
39. Ludwig B, Glasl B, Kinzinger GS, Lietz T, Lisson JA. Anatomical guidelines for miniscrew insertion: vestibular interradicular sites. J Clin Orthod. 2011;45(3):165–73. PMID: 2178520121785201
40. Kyung HM, Park HS, Bae SM, Sung JH, Kim IB. Development of orthodontic micro-implants for intraoral anchorage. J Clin Orthod. (2003) 37(6):321–8; quiz 314. PMID: 12866214.12866214
41. Chiapasco M, Casentini P, Tommasato G, Dellavia C, del Fabbro M. Customized CAD/CAM Titanium meshes for the guided bone regeneration of severe alveolar ridge defects: preliminary results of a retrospective clinical study in humans. Clin Oral Implants Res. (2021) 32(4):498–510. doi: 10.1111/clr.13720
42. Savoldi F, Tsoi JKH, Paganelli C, Matinlinna JP. The biomechanical properties of human craniofacial sutures and relevant variables in sutural distraction osteogenesis: a critical review. Tissue Eng Part B Rev. (2018) 24(1):25–36. doi: 10.1089/ten.teb.2017.0116
43. Alsino HI, Hajeer MY, Burhan AS, Alkhouri I, Darwich K. The effectiveness of periodontally accelerated osteogenic orthodontics (PAOO) in accelerating tooth movement and supporting alveolar bone thickness during orthodontic treatment: a systematic review. Cureus. (2022) 14(5):e24985. doi: 10.7759/cureus.24985
44. Vannala V, Katta A, Reddy MS, Shetty SR, Shetty RM, Khazi SS. Periodontal accelerated osteogenic orthodontics technique for rapid orthodontic tooth movement: a systematic review. J Pharm Bioallied Sci. (2019) 11(Suppl 2):S97–S106. doi: 10.4103/JPBS.JPBS_298_18
45. Apalimova A, Roselló À, Jané-Salas E, Arranz-Obispo C, Marí-Roig A, López-López J. Corticotomy in orthodontic treatment: systematic review. Heliyon. (2020) 6(5):e04013. doi: 10.1016/j.heliyon.2020.e04013
46. Wilcko MT, Wilcko WM, Bissada NF. An evidence-based analysis of periodontally accelerated orthodontic and osteogenic techniques: a synthesis of scientific perspectives. Semin Orthod. (2008) 14(4):305–16. doi: 10.1053/j.sodo.2008.07.007
47. Frost HM. The regional acceleratory phenomenon: a review. Henry Ford Hosp Med J. (1983) 31(1):3–9. PMID: 63454756345475
48. Mostafa YA.; Mohamed Salah Fayed M, Mehanni S, ElBokle NN, Heider AM. Comparison of corticotomy-facilitated vs standard tooth-movement techniques in dogs with miniscrews as anchor units. Am J Orthod Dentofacial Orthop. (2009) 136(4):570–7. doi: 10.1016/j.ajodo.2007.10.052
49. Chung KR, Oh MY, Ko SJ. Corticotomy-Assisted orthodontics. J Clin Orthod. (2001) 35(5):331–9. PMID: 1147554411475544
50. Zou M, Li C, Zheng Z. Remote corticotomy accelerates orthodontic tooth movement in a rat model. Biomed Res Int. (2019) 2019:1–9. doi: 10.1155/2019/4934128
51. Lee W. Corticotomy for orthodontic tooth movement. J Korean Assoc Oral Maxillofac Surg. (2018) 44(6):251. doi: 10.5125/jkaoms.2018.44.6.251
52. Mota-Rodriguez A, Olmedo-Hernandez O, Argueta-Figueroa L. A systematic analysis of evidence for surgically accelerated orthodontics. J Clin Exp Dent. (2019) 11(9):e829–e838. doi: 10.4317/jced.56048
53. Vercellotti T, Podesta A. Orthodontic microsurgery: a new surgically guided technique for dental movement. Int J Periodontics Restorative Dent. (2007) 27(4):325–31. PMID: 1772698817726988
54. Bertossi D, Vercellotti T, Podesta A, Nocini PF. Orthodontic microsurgery for rapid dental repositioning in dental malpositions. J Oral Maxillofac Surg. (2011) 69(3):747–53. doi: 10.1016/j.joms.2009.07.112
55. Han J, He H. Effects of piezosurgery in accelerating the movement of orthodontic alveolar bone tooth of rats and the expression mechanism of BMP-2. Exp Ther Med. (2016) 12(5):3009–13. doi: 10.3892/etm.2016.3704
56. Savoldi F, Yon MJ, Kwok VM, Yeung AW, Tanaka R, Tsoi JK, Matinlinna JP, Bornstein MM. Accuracy of CBCT in the identification of mental, lingual, and retromolar foramina: a comparison with visual inspection of human dry mandibles. Int J Periodontics Restorative Dent. (2021) 41(6):e277–86. doi: 10.11607/prd.4770
57. Apalimova A, Roselló À, Jané-Salas E, Arranz-Obispo C, Marí-Roig A, López-López J. Corticotomy in orthodontic treatment: systematic review. Heliyon. (2020) 6(5):e04013. doi: 10.1016/j.heliyon.2020.e04013
58. Oenning AC, Jacobs R, Pauwels R, Stratis A, Hedesiu M, Salmon B; DIMITRA Research group. Cone-beam CT in paediatric dentistry: dIMITRA project position statement. Pediatr Radiol. (2018) 48(3):308–16. http://www.dimitra.be. doi: 10.1007/s00247-017-4012-9
Keywords: CAD-CAM, digital orthodontics, surgical template, corticotomy, piezocision, miniscrew, TAD
Citation: Guarnieri R, Grenga C, Altieri F, Rocchetti F, Barbato E and Cassetta M (2023) Can computer-guided surgery help orthodontics in miniscrew insertion and corticotomies? A narrative review. Front. Oral. Health 4:1196813. doi: 10.3389/froh.2023.1196813
Received: 30 March 2023; Accepted: 8 May 2023;
Published: 31 May 2023.
Edited by:
Vahid Rakhshan, Institute for Cognitive Science Studies (ICSS), IranReviewed by:
Xin Xiong, Sichuan University, China© 2023 Guarnieri, Grenga, Altieri, Rocchetti, Barbato and Cassetta. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rosanna Guarnieri cm9zYW5uYS5ndWFybmllcmlAdW5pcm9tYTEuaXQ=
†ORCID Rosanna Guarnieri orcid.org/0000-0003-0497-5991 Camilla Grenga orcid.org/0000-0001-7822-5953 Federica Altieri orcid.org/0000-0002-3618-5970 Ersilia Barbato orcid.org/0000-0002-5328-3580 Michele Cassetta orcid.org/0000-0003-2633-5514
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.