 Abdelrahman M. Alhilou
Abdelrahman M. Alhilou Essam Ahmed Al-Moraissi
Essam Ahmed Al-Moraissi Abdulaziz Bakhsh
Abdulaziz Bakhsh Nikolaos Christidis
Nikolaos Christidis Peggy Näsman4
Peggy Näsman4

94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Oral. Health, 18 October 2023
Sec. Oral and Maxillofacial Surgery
Volume 4 - 2023 | https://doi.org/10.3389/froh.2023.1147884
This article is part of the Research TopicReviews in the Neuroscience of Orofacial FunctionsView all 5 articles
Background: Symptomatic irreversible pulpitis (SIP) or symptomatic apical periodontitis (SAP) are two painful conditions often warranting emergency treatment. The most common emergency treatments supported by evidence are pulpotomy and pulpectomy and are normally performed under time-constrained circumstances. However, there is no strong evidence of which treatment suggested in literature a clinician can use to reduce endodontic pain effectively. Therefore, the aim of this systematic review is to investigate the present knowledge on postoperative pain related to the two types of emergency treatments available for treating SIP and SAP.
Methods: Randomized controlled trials investigating postoperative pain after emergency treatments (pulpotomy and/or pulpectomy) on permanent dentition with signs and symptoms of SIP and/or SAP were searched in three major databases from 1978 until 2022. Risk of bias was assessed with Cochrane's tool.
Results: Only five studies fulfilled the inclusion criteria. The included studies indicated that pulpotomy and pulpectomy are both suitable treatment options for SAP and SIP, as they provide sufficient alleviation of pain in permanent dentition. However, inconsistent results were found between the included trials on which emergency treatment is more effective in reducing pain. Cochrane's tool revealed that the studies had a low risk of bias. Limitations found in the design of the included randomized control trials decreased the level of evidence. None of the included studies accounted for essential confounding variables, such as factors affecting pain (including the psychological aspects). Moreover, possible non-odontogenic pain was not assessed, and therefore, it was not excluded; hence, affecting the internal validity of the studies.
Conclusion: There are controversies within the available randomized control trials on which treatment is most effective in reducing emergency pain. This could be due to some weaknesses in the design of the clinical trials. Thus, further well-designed studies are warranted to draw conclusions on which emergency treatment is more effective in reducing pain.
Systematic Review Registration: PROSPERO (CRD42023422282).
Oro-facial pain, is a pain related to the mouth and/or face (1). The prevalence of orofacial pain varies between countries, i.e., 5%–57% (2); specifically, toothache or dental pain prevalence range globally between 7% and 32%, which has a psychological, social and economic negative impact on the person affected as well as on the society (3). Most of the dental pain is due to periapical or pulpal disease, requiring emergency intervention, such as endodontic treatment or extraction (4). The prevalence of pain requiring endodontic procedures is 81% (5). Endodontic emergency treatment is generally a procedure needed to soothe patients' acute symptoms and is completed in limited time, as the treatment is normally booked in emergency slots. The primary goal of the treatment is to eliminate the patient's symptoms during this short period of time. However, the goal is not always easy to achieve, especially that several factors can contribute to such pain, including the emotional experiences of the person affected and the ability of the dentist to diagnose and choose the effective treatment modality.
Pain is defined by the International Association for the Study of Pain (IASP) as “an unpleasant sensory and emotional experience associated with or resembling that associated with, actual or potential tissue damage” (6). This unpleasant subjective sensation is also related to emotional experiences. Highly anxious patients have expectations of higher pain during the treatment compared to those with a lower level of anxiety (7). Therefore, the emotional state is as important as the patients' physical symptoms and must be considered during treatment. However, it is unknown if the literature related to dental pain emergency treatments considers such aspects when evaluating pre-/post-operative pain.
Symptomatic pain that requires endodontic intervention is due to pulpal damage caused by carious lesions, cracks, trauma and/or crown preparation. When such damage occurs, the pulp starts a normal defensive mechanism and develops pulpitis (pulp inflammation) (8). Based on the clinical signs and symptoms, as well as the degree to which the pulp can heal itself, diagnosis of pulpal inflammation can be either reversible or irreversible pulpitis (9). However, irreversible pulpitis as a diagnosis is being questioned due to new evidence showing that this clinical diagnosis does not necessarily match the histologic condition of the pulp. A histological study showed that in some cases diagnosed with irreversible pulpitis, only the upper part of the pulp, which is close to caries, had bacterial invasion, while the rest of the pulp remained free of inflammation (10). Hence, if the inflamed coronal part of the pulp is removed (partial pulpotomy or pulpotomy), it will have the ability to regenerate and return to its normal state (11). However, if bacteria succeed to invade the whole pulp; as a result, the pulp becomes partially or fully necrotic (infected), which could create either symptomatic or asymptomatic apical periodontitis (8, 12, 13). Symptomatic apical periodontitis was defined as “inflammation usually of the apical periodontium, producing clinical symptoms including a painful response to biting and/or percussion or palpation. It might or might not be associated with an apical radiolucent area” (9).
Pulpotomy and pulpectomy as emergency treatments have been suggested to reduce endodontic pain (14, 15). The procedure where the infected/inflamed/necrotic pulp tissue is removed from the root canals where the pulp tissue is replaced with a root filling material is called pulpectomy. This procedure is considered a time-consuming and invasive procedure (16); however, it has a success rate of almost 90% (17). On the other hand, a pulpotomy is a procedure that can be completed in a limited time where diseased pulp tissue is excised from the pulp chamber, leaving healthy tissue intact (18). Historically, emergency pulpotomy treatment aims were first to relieve pain and second to allow the development of uncompleted root apices followed by pulpectomy after complete root formation (19). Moreover, the success rate of the treatment was considered relatively low, i.e., from 13 to 37% (20, 21). The concept of vital pulp therapy, including pulpotomy have recently changed especially with the relatively high success rates reported (11, 22). However, no firm evidence, such as a systematic review, proves the superiority of one treatment over another in reducing emergency endodontic pain. Therefore, this systematic review aims first to investigate pulpotomy as an emergency treatment of symptomatic apical periodontitis (SAP) and symptomatic irreversible pulpitis (SIP) compared to pulpectomy on postoperative pain. Second, to investigate if the psychological aspects of the patients are considered in investigated randomized control trials (RCT). Current study hypothesized that pulpotomy as an emergency treatment has less postoperative pain than pulpectomy. Moreover, no studies have investigated the psychological aspects of the patients before assessing pain.
This review was done based on Preferred Reporting Items for Systematic reviews and Meta Analyses (PRISMA) statement for reporting systematic reviews (23) (Figure 1). The review was registered in PROSPERO (CRD42023422282).

Figure 1. The process of identifying studies through databases and registers.
The electronic databases “Medline (Ovid)”, “Embase (embase.com)” and “Web of science (Clarivate Analytics)” were used to conduct a search of clinical controlled trials published from 1978 until 2022, which investigated the use of emergency pulpotomy and/or pulpectomy to alleviate pain (toothache). The search terms and the search strategy are presented in Supplementary Material (Table 1).
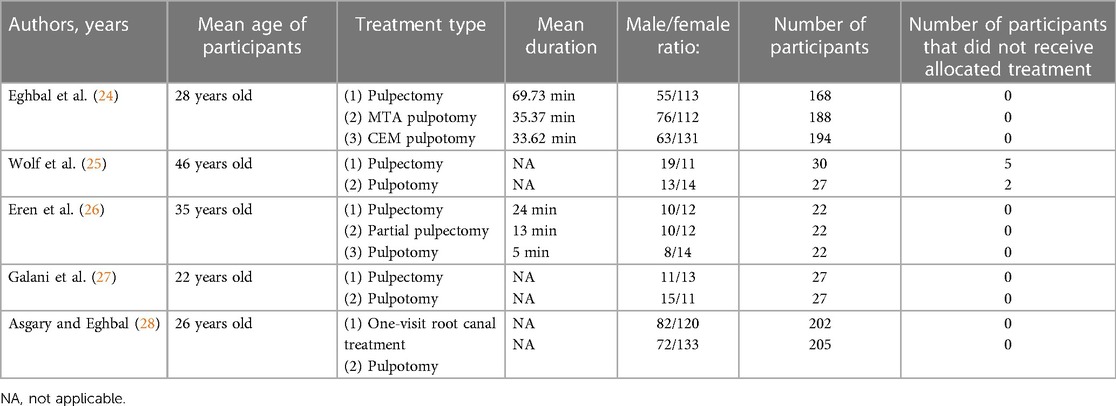
Table 1. The table presents the population characteristics, treatment types and mean duration of treatment for the five studies included in the systematic review.
The PICOTS process was used to adopt the following inclusion criteria: (a) Randomized clinical trials (b) patients suffered from SIP or SAP (c) treatment performed on permanent teeth (d) complete pulpotomy or partial pulpotomy as an emergency treatment using pulpectomy as a comparative control (d) all reported follow-up times, especially for postoperative pain after emergency treatment and finally (e) pain relief. The articles were excluded if: (a) Treatment was performed on anything other than acute symptomatic tooth (b) treatment other than pulpectomy or pulpotomy (c) treatment performed on primary teeth (d) studies other than randomized control trials. The assessment for the eligibility for inclusion was done independently by 2 of the authors (AB and AA). Then, the authors conducted two rounds of meetings together and solved the heterogeneity by consensus. Therefore, the kappa statistics agreement was deemed not necessary.
The modern version of Cochranes tool was used to evaluate risk of bias by assessing randomization, blinding of participants, blinding of assessors, drop out, reporting bias and judgement (29). Several systems can be used to classify evidence. The grading system GRADE, which stands for Grading of Recommendations Assessment, Development and Evaluation, to assess the treatment studies from strong (number 4) to weak (number 1) was first planned to use (30). However, the studies included in this review were insufficient for a meta-analysis; hence this grading system was not applicable.
The outcome of the search from the three electronic databases gave us a result of 6,603 articles; however, 2,025 duplicate records were removed. Based on the articles' title and abstract, only six randomized control trials met the inclusion criteria (24–28, 31). However, one of these papers was excluded after reassessing the eligibility by reading the papers thoroughly (31). The reason behind the exclusion of this paper is that a pulpectomy was performed on necrotic canals for the teeth assigned for the group of pulpotomy procedure. i.e., only vital or partially vital canals received a pulpotomy procedure. Therefore, 4,573 articles were excluded (Figure 1).
The population characteristics for the studies included are presented in Table 1. Moreover, studies characteristics are presented in Table 2. Well-designed RCT is considered the most reliable evidence as it reduces the effect of confounding factors (32). Limitations are found in the design of all the included studies, i.e., Some essential factors that could affect pain evaluation were not considered (patient's psychological state, patient history of pain, the type of tooth treated, age of participants and sex); moreover, possible non-odontogenic pain was not assessed, minimizing the reliability of all included randomized control trials. None of the studies considered the psychological aspect when evaluating pre-or postoperative pain. Only one study evaluated tooth survival and the follow-up was 18 months. The study found no significant differences in tooth survival between pulpotomy and pulpectomy. The reported success rate was 85% for pulpotomy and 87% for pulpectomy (27). Only five articles were found, which was not sufficient for a meta-analysis. The longest follow up period was 5 years (28); however, no pain evaluation with numerical rating scale (NRS) was performed after seven days of treatment. Five years follow up on that study was for clinical and radiographic evaluation only. Pain follow up in the other four studies ranged from 5 to 7 days.
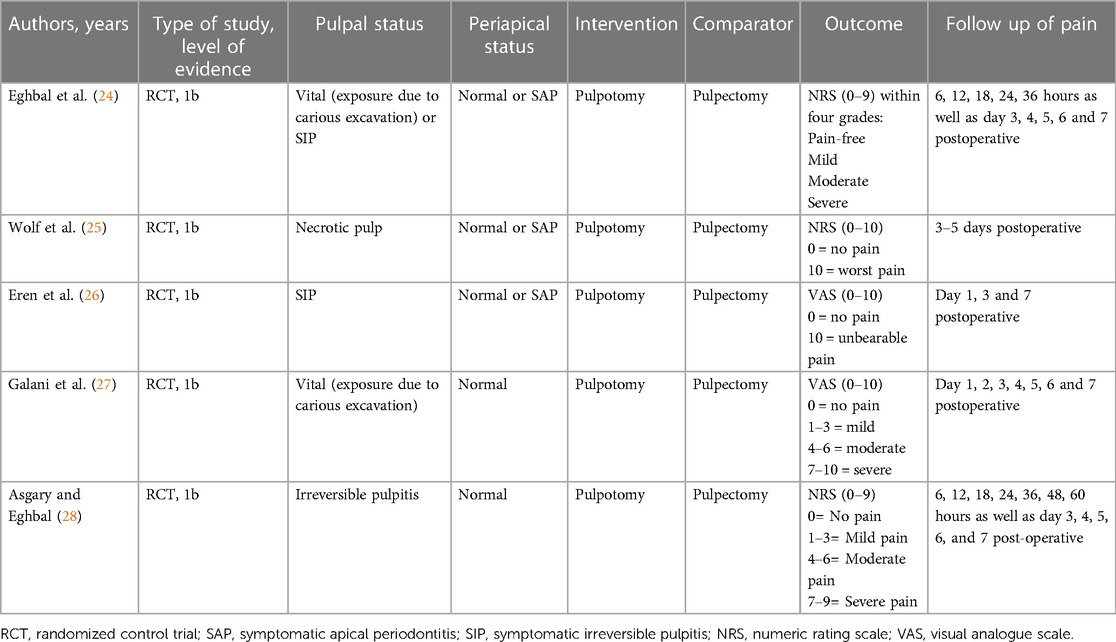
Table 2. The table present studies characteristics and selection criteria using PICOTS.
The five clinical trials which satisfied the inclusion criteria showed that pulpotomy and pulpectomy are both suitable treatment options for SIP and SAP, as they provide sufficient pain relief in permanent dentition. Studies have used different methods to evaluate postoperative pain. Two studies used the numeric rating scale for pain assessment (24, 25) found no differences between pulpotomy and pulpectomy in reducing pain up to seven days postoperatively (24, 25). Another study which used NRS for pain evaluation described pulpotomy as less painful over the assessment period (28). In addition, two studies have used the visual analogue scale (VAS) to evaluate postoperative pain (26, 27). Galani et al. reported that emergency treatment using pulpotomy was less painful than pulpectomy, in contrast, Eren et al. found the opposite, i.e., pulpectomy reduced postoperative pain more than pulpotomy.
Only one study was single-blinded (26). Application of blinding was difficult due to the nature of the research. All included studies reported risk of bias except one (25). The evidence had a low risk of bias in all included articles (Table 3).

Table 3. Table representing cochranes “Risk of bias”.
The findings of the current review revealed that both pulpotomy and pulpectomy are effective emergency treatments to reduce endodontic related pain. The limitation found in the design of all the included studies reduced the quality of evidence from strong (randomized control trials), to moderate evidence.
Studies varied in tools used for pain assessment. Aforementioned, some studies that considered NRS to evaluate pain reported no differences between pulpotomy and pulpectomy in reducing endodontic pain (24, 25), while others using the same tool found a difference (28). Moreover, studies which assessed the post-operative pain through the VAS reported differences between treatments (26, 27). Although the reliability and validity of both VAS and NRS to measure pain intensity are previously supported by evidence (33, 34), studies showed a slight preference toward NRS over VAS scales. For example, it has been reported that VAS is not always normally distributed (35). Moreover, one study had shown the superiority of NRS on responsivity to pain compared to VAS (36). Nevertheless, both VAS and NRS scales are only tools to record subjective symptoms that can be affected by several factors. The patient's psychological state is one of the most important factors that affect pain (37). Highly anxious patients have higher pain expectations during endodontic treatment than those with a lower level of anxiety (7). Furthermore, pain past experiences have an impact on the threshold of individuals and can be a valuable tool for good diagnosis (7, 8). Other factors could include the type of tooth treated (multi-rooted or single-rooted teeth), age of participants and sex (38). According to epidemiological studies, females have a higher prevalence of chronic pain than males (39). Evidence shows that females are more prone to temporomandibular disorder (a chronic pain affecting orofacial region) than males (40, 41). Unfortunately, none of the five randomized control trials included in the current review considered the psychosocial state of participants when comparing treatments. Only one study had a past history of pain in their inclusion criteria for diagnosis of irreversible pulpitis; however, it was not considered when pain intensity was analysed between treatments (24). All the studies used a single type of tooth (standard methodology), except for one study. In that study, the pre-/post-operative pain was reported for each treatment on each tooth type. However, the pain intensity reported for each tooth type was not compared between treatments (25). In all of the studies, age and sex data were reported but was not used for further analysis when pain intensity was compared between treatments. All previously mentioned factors could be considered confounding factors; and most probably this is why results differ between these clinical trials. These confounding factors are limitations in the design of the studies, hence reducing their quality.
Pain caused by a physical issue can be explained and treated easily: however, pain that is unusual or has no apparent cause can be more confusing and frustrating. Referred pain and psychosomatic pain are other significant problems. Psychosomatic pain is when psyche issues such as depression, anxiety, or stress induce pain that spreads to other body parts (42). On the other hand, referred pain is when the patient feels symptoms in a different location from where the cause of the pain is. Referred pain and psychosomatic pain leads to difficulty in identifying the source of patients' symptoms. The origin of intradental pain could be odontogenic, non-odontogenic or even systematic. Referred pain from the masticatory muscles, suboccipital muscles or the temporomandibular joints are examples of non-odontogenic pain often misdiagnosed with odontogenic pain. However, referred pain from the central nervous system (systematic) such as trigeminal neuralgia or atypical facial neuralgia can also lead to a missed diagnosis (8). No studies included diagnostic tests rather than clinical dental diagnosis, including pulp sensitivity tests that have limitations (43), i.e., studies show a poor correlation between pulp sensitivity tests and the histological state of the pulp (44, 45). Hence, the internal validity of the trials is mostly affected. Therefore, one can suggest the diagnostic criteria of temporomandibular joint disorder (TMD) (DC/TMD) (46) as an additive value for future research concerning the current topic to minimise the possibilities of misdiagnosis (comorbidity). DC/TMD Axis I is a valid diagnostic tool for detecting and differentiating TMD related pain (sensitivity ≥0.86, specificity ≥0.98). This will help researchers to exclude non-odontogenic pain before conducting trials. Moreover, the DC/TMD Axis II questionnaire will help assess the participants' behavioural and psychosocial status and correlate it with pre-/post-operative pain intensity. Hence, it will reduce the possibility of having psychosocial confounding factor (previously mentioned in the first paragraph) on future study designs.
Each emergency treatment has its pros and cons. Pulpotomy is a treatment in which the pulp tissue of the pulp chamber is removed. The dentist does not penetrate the canal(s) of the tooth, and the patient is recommended to return for a complete root canal treatment. Some studies suggested that pulpotomy does not require the use of rubber dam, nor the change of instrumentation to sterile ones, as the canals are not penetrated (14, 47). This saves time during emergency treatment, and time is critical in an emergency visit. Nonetheless, recent studies are emphasizing the importance of using rubber dam during pulpotomy which will improve the success rate of the treatment, especially in cases diagnosed with reversible or irreversible pulpitis (11, 22). Pulpectomy starts the same way as a pulpotomy; however, it is continued by chemo-mechanical treatment of the root canal system by application of rubber dam to prevent any contamination of the area. Pulpectomy is a more time-consuming treatment than pulpotomy, but the success rate reported in the literature is higher than pulpotomy (16). The most probable reasons for pain relief in both emergency treatments are intra-pulpal reduction of tissue pressure and the concentration of inflammatory mediators. Moreover, excision of the inflamed coronal part of the pulp or the whole pulp will reduce or eliminate the number of nociceptive sensory free nerve endings (48). However, there is still a significant gap in the literature that has to be filled related to which emergency treatment is most effective in reducing pain.
Within the few articles found, the results of this systematic review show that both pulpectomy and pulpotomy as emergency treatments can reduce pain in permanent dentition with signs and symptoms of SIP and/or SAP. However, there are still controversies within these moderate-quality papers on which treatment is most effective in reducing pain. The controversy could be due to cofounding factors not considered during pain evaluation in any of the investigated randomized control trials. Hence, there is still a big need for better designed randomized control trials assessing the best possible emergency treatment option in minimizing the pain.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
NC, PN, and EA-M contributed to conceptualization, methodology, reviewing and writing. AA and AB contributed to screening, evaluating articles and writing the original draft. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/froh.2023.1147884/full#supplementary-material
1. Khawaja N, Renton T. Pain part 3: acute orofacial pain. Dent Update. (2015) 42(5):442–4. 7–50, 53–7 passim. doi: 10.12968/denu.2015.42.5.442
2. Horst OV, Cunha-Cruz J, Zhou L, Manning W, Mancl L, DeRouen TA. Prevalence of pain in the orofacial regions in patients visiting general dentists in the northwest practice-based REsearch collaborative in evidence-based DENTistry research network. J Am Dent Assoc. (2015) 146(10):721–8.e3. doi: 10.1016/j.adaj.2015.04.001
3. Pau AK, Croucher R, Marcenes W. Prevalence estimates and associated factors for dental pain: a review. Oral Health Prev Dent. (2003) 1(3):209–20. doi: 10.3290/j.ohpd.a8529
4. Hasler J, Mitchell D. Analysis of 1628 cases of odontalgia: a corroborative study. J Indianapolis Dent Soc. (1963) 17:23–5.
5. Pak JG, White SN. Pain prevalence and severity before, during, and after root canal treatment: a systematic review. J Endod. (2011) 37(4):429–38. doi: 10.1016/j.joen.2010.12.016
6. Raja SN, Carr DB, Cohen M, Finnerup NB, Flor H, Gibson S, et al. The revised international association for the study of pain definition of pain: concepts, challenges, and compromises. Pain. (2020). doi: 10.1097/j.pain.0000000000001939
7. van Wijk AJ, Hoogstraten J. Reducing fear of pain associated with endodontic therapy. Int Endod J. (2006) 39(5):384–8. doi: 10.1111/j.1365-2591.2006.01090.x
8. Bender IB. Pulpal pain diagnosis–a review. J Endod. (2000) 26(3):175–9. doi: 10.1097/00004770-200003000-00012
9. Glickman G. AAE Consensus conference recommended diagnostic terminology. J Endod. (2009) 35(12):1634. doi: 10.1016/j.joen.2009.09.035
10. Ricucci D, Loghin S, Siqueira JF Jr. Correlation between clinical and histologic pulp diagnoses. J Endod. (2014) 40(12):1932–9. doi: 10.1016/j.joen.2014.08.010
11. Ricucci D, Siqueira JF Jr, Li Y, Tay FR. Vital pulp therapy: histopathology and histobacteriology-based guidelines to treat teeth with deep caries and pulp exposure. J Dent. (2019) 86:41–52. doi: 10.1016/j.jdent.2019.05.022
12. Kakehashi S, Stanley HR, Fitzgerald RJ. The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surg Oral Med Oral Pathol. (1965) 20:340–9. doi: 10.1016/0030-4220(65)90166-0
13. Möller AJ, Fabricius L, Dahlén G, Ohman AE, Heyden G. Influence on periapical tissues of indigenous oral bacteria and necrotic pulp tissue in monkeys. Scand J Dent Res. (1981) 89(6):475–84. doi: 10.1111/j.1600-0722.1981.tb01711.x
14. Hasselgren G, Reit C. Emergency pulpotomy: pain relieving effect with and without the use of sedative dressings. J Endod. (1989) 15(6):254–6. doi: 10.1016/S0099-2399(89)80219-5
15. McDougal RA, Delano EO, Caplan D, Sigurdsson A, Trope M. Success of an alternative for interim management of irreversible pulpitis. J Am Dent Assoc. (2004) 135(12):1707–12. doi: 10.14219/jada.archive.2004.0123
16. Gesi A, Bergenholtz G. Pulpectomy–studies on outcome. Endod Top. (2003) 5(1):57–70. doi: 10.1111/j.1601-1546.2003.00020.x
17. Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature—part 1. Effects of study characteristics on probability of success. Int Endod J. (2007) 40(12):921–39. doi: 10.1111/j.1365-2591.2007.01322.x
18. Armstrong RL, Patterson SS, Kafrawy AH, Feltman EM. Comparison of dycal and formocresol pulpotomies in young permanent teeth in monkeys. Oral Surg Oral Med Oral Pathol. (1979) 48(2):160–8. doi: 10.1016/0030-4220(79)90055-0
19. Langeland K, Dowden WE, Tronstad L, Langeland LK. Human pulp changes of iatrogenic origin. Oral Surg Oral Med Oral Pathol. (1971) 32(6):943–80. doi: 10.1016/0030-4220(71)90183-6
20. Bjørndal L, Reit C, Bruun G, Markvart M, Kjaeldgaard M, Näsman P, et al. Treatment of deep caries lesions in adults: randomized clinical trials comparing stepwise vs. direct complete excavation, and direct pulp capping vs. partial pulpotomy. Eur J Oral Sci. (2010) 118(3):290–7. doi: 10.1111/j.1600-0722.2010.00731.x
21. Barthel CR, Rosenkranz B, Leuenberg A, Roulet JF. Pulp capping of carious exposures: treatment outcome after 5 and 10 years: a retrospective study. J Endod. (2000) 26(9):525–8. doi: 10.1097/00004770-200009000-00010
22. Aguilar P, Linsuwanont P. Vital pulp therapy in vital permanent teeth with cariously exposed pulp: a systematic review. J Endod. (2011) 37(5):581–7. doi: 10.1016/j.joen.2010.12.004
23. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. (2021) 372:n71. doi: 10.1136/bmj.n71
24. Eghbal MJ, Haeri A, Shahravan A, Kazemi A, Moazami F, Mozayeni MA, et al. Postendodontic pain after pulpotomy or root canal treatment in mature teeth with carious pulp exposure: a multicenter randomized controlled trial. Pain Res Manag. (2020) 2020. doi: 10.1155/2020/5853412
25. Wolf E, Dragicevic M, Fuhrmann M. Alleviation of acute dental pain from localised apical periodontitis: a prospective randomised study comparing two emergency treatment procedures. J Oral Rehabil. (2019) 46(2):120–6. doi: 10.1111/joor.12730
26. Eren B, Onay EO, Ungor M. Assessment of alternative emergency treatments for symptomatic irreversible pulpitis: a randomized clinical trial. Int Endod J. (2018) 51(Suppl 3):e227–e37. doi: 10.1111/iej.12851
27. Galani M, Tewari S, Sangwan P, Mittal S, Kumar V, Duhan J. Comparative evaluation of postoperative pain and success rate after pulpotomy and root canal treatment in cariously exposed mature permanent molars: a randomized controlled trial. J Endod. (2017) 43(12):1953–62. doi: 10.1016/j.joen.2017.08.007
28. Asgary S, Eghbal MJ. The effect of pulpotomy using a calcium-enriched mixture cement versus one-visit root canal therapy on postoperative pain relief in irreversible pulpitis: a randomized clinical trial. Odontology. (2010) 98(2):126–33. doi: 10.1007/s10266-010-0127-2
29. Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions. John Wiley & Sons (2019).
30. Handbook G, Schünemann H, Brożek J, Guyatt G, Oxman A. Handbook for grading the quality of evidence and the strength of recommendations using the GRADE approach (updated October 2013). GRADE Working Group. (2013).
31. Koli B, Chawla A, Logani A, Kumar V, Sharma S. Combination of nonsurgical endodontic and vital pulp therapy for management of mature permanent mandibular molar teeth with symptomatic irreversible pulpitis and apical periodontitis. J Endod. (2021) 47(3):374–81. doi: 10.1016/j.joen.2020.10.010
32. Evans D. Hierarchy of evidence: a framework for ranking evidence evaluating healthcare interventions. J Clin Nurs. (2003) 12(1):77–84. doi: 10.1046/j.1365-2702.2003.00662.x
33. Jensen M, Chen C, Brugger A. The relative validity of three pain treatment outcome measures in post-surgical pain. Pain. (2003) 99:101–9. doi: 10.1016/S0304-3959(02)00063-5
34. Jensen MP, Miller L, Fisher LD. Assessment of pain during medical procedures: a comparison of three scales. Clin J Pain. (1998) 14(4):343–9. doi: 10.1097/00002508-199812000-00012
35. Williamson A, Hoggart B. Pain: a review of three commonly used pain rating scales. J Clin Nurs. (2005) 14(7):798–804. doi: 10.1111/j.1365-2702.2005.01121.x
36. Ferreira-Valente MA, Pais-Ribeiro JL, Jensen MP. Validity of four pain intensity rating scales. Pain®. (2011) 152(10):2399–404. doi: 10.1016/j.pain.2011.07.005
37. Rugh JD. Psychological components of pain. Dent Clin North Am. (1987) 31(4):579–94. doi: 10.1016/S0011-8532(22)00375-5
38. Arias A, de la Macorra JC, Hidalgo JJ, Azabal M. Predictive models of pain following root canal treatment: a prospective clinical study. Int Endod J. (2013) 46(8):784–93. doi: 10.1111/iej.12059
39. Unruh AM. Gender variations in clinical pain experience. Pain. (1996) 65(2–3):123–67. doi: 10.1016/0304-3959(95)00214-6
40. Dworkin SF, Huggins KH, LeResche L, Von Korff M, Howard J, Truelove E, et al. Epidemiology of signs and symptoms in temporomandibular disorders: clinical signs in cases and controls. J Am Dent Assoc. (1990) 120(3):273–81. doi: 10.14219/jada.archive.1990.0043
41. LeResche L. Epidemiology of temporomandibular disorders: implications for the investigation of etiologic factors. Crit Rev Oral Biol Med. (1997) 8(3):291–305. doi: 10.1177/10454411970080030401
42. Rubin JJ. Psychosomatic pain: new insights and management strategies. S Med J. (2005) 98(11):1099–111. doi: 10.1097/01.smj.0000191268.48828.3a
43. Zanini M, Meyer E, Simon S. Pulp inflammation diagnosis from clinical to inflammatory mediators: a systematic review. J Endod. (2017) 43(7):1033–51. doi: 10.1016/j.joen.2017.02.009
44. Seltzer S, Bender I, Ziontz M. The dynamics of pulp inflammation: correlations between diagnostic data and actual histologic findings in the pulp. Oral Surg Oral Med Oral Pathol. (1963) 16(7):846–71. doi: 10.1016/0030-4220(63)90323-2
45. Dummer P, Hicks R, Huws D. Clinical signs and symptoms in pulp disease. Int Endod J. (1980) 13(1):27–35. doi: 10.1111/j.1365-2591.1980.tb00834.x
46. Schiffman E, Ohrbach R, Truelove E, Look J, Anderson G, Goulet JP, et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: recommendations of the international RDC/TMD consortium network* and orofacial pain special interest groupdagger. J Oral Facial Pain Headache. (2014) 28(1):6–27. doi: 10.11607/jop.1151
47. Nyerere JW, Matee MI, Simon EN. Emergency pulpotomy in relieving acute dental pain among Tanzanian patients. BMC oral Health. (2006) 6(1). doi: 10.1186/1472-6831-6-1
Keywords: symptomatic, irreversible pulpitis, apical periodontitis, pulpectomy, pulpotomy, pain, emergency treatment
Citation: Alhilou AM, Al-Moraissi EA, Bakhsh A, Christidis N and Näsman P (2023) Pain after emergency treatments of symptomatic irreversible pulpitis and symptomatic apical periodontitis in the permanent dentition: a systematic review of randomized clinical trials. Front. Oral. Health 4:1147884. doi: 10.3389/froh.2023.1147884
Received: 19 January 2023; Accepted: 26 September 2023;
Published: 18 October 2023.
Edited by:
Paolo Boffano, Azienda Sanitaria Locale Vercelli, ItalyReviewed by:
Iffat Nasim, Saveetha Dental College And Hospitals, India© 2023 Alhilou, Al-Moraissi, Bakhsh, Christidis and Näsman. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abdelrahman M. Alhilou YW1oaWxvdUB1cXUuZWR1LnNh
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.