 Ranam Moreira Reis1
Ranam Moreira Reis1 Hugo Lemes Carlo1
Hugo Lemes Carlo1 Rogério Lacerda dos Santos1
Rogério Lacerda dos Santos1 Fernanda Maria Sabella2
Fernanda Maria Sabella2 Thaís Manzano Parisotto2
Thaís Manzano Parisotto2 Fabíola Galbiatti de Carvalho1*
Fabíola Galbiatti de Carvalho1*- 1Department of Dentistry, Federal University of Juiz de Fora, Governador Valadares, Brazil
- 2Laboratory of Clinical and Molecular Microbiology, São Francisco University, Bragança Paulista, Brazil
The COVID-19 pandemic has brought health damage and socioeconomic disruptions, together with lifestyle disorders around the world. Children are one of the most commonly affected, mainly due to social isolation and changes in eating habits and physical activities. This way, the risk of weight gain and obesity is possibly enhanced, as well as poor oral hygiene conditions and early childhood caries (ECC) development during the lockdown. In children under 6 years of age, ECC is defined as carious lesions in one or more primary teeth, with or without cavitation. Importantly, alterations in the oral microbiome caused by changes in children lifestyles have much more than a local impact on oral tissues, interplaying with the gut microbiome and influencing systemic environments. Recent studies have been exploring the oral health conditions, eating habits, and weight gain in the childhood population during the COVID-19 pandemic; however, there is a lack of information concerning the association among oral and gut microbiome, dental caries, and obesity in the COVID-19 era. In this context, this review aimed at analyzing a possible relationship between the oral and gut microbiome, caries, and obesity in children during the COVID-19 pandemic.
Introduction
The advent of COVID-19 and its widespread brought losses and changes not only linked to health but also habits and personal interrelationships of billions of people altogether [1]. The WHO declared a pandemic in March 2020, which sought to protect the integrity and health of the world population through measures of social isolation [2], which in turn brought disruptions in lifestyle affecting the population's physical and mental health [3].
Children are strongly affected in this context, mainly due to social distance and absence from school [4]. With the revolution in routine, physical and other daily activities were seriously prejudiced, favoring sedentarism and worsening the quality of life and health, especially for children who lived in compact urban environments and who were used to spending most of their time at school, socializing, playing with friends, and being active in general [5]. In that same context, children's consumption of unhealthy food increased during the pandemic and confinement [6, 7].
A cariogenic diet and poor oral hygiene could lead to dysbiotic microbiota and the development of biofilm-mediated oral diseases, for example, caries and gingivitis [8, 9]. Interestingly, systemic pathologies such as obesity, diabetes, and cardiovascular problems have been also influenced by dental plaque-associated oral disturbs [10]. Thus, dental caries and obesity are both diet-related diseases and can share common risk factors. Oral bacteria are frequently swallowed with food and beverages during the digestion process and can reach the gastrointestinal tract [11]. Consequently, the dysbiotic state described in the caries development can interplay with the gut microbiome, influencing the gut dysbiosis, and weight gain [11–13].
Some studies have demonstrated the increased risk of obesity, poor toothbrushing, and sweets consumption in children during the COVID-19 pandemic [1, 3, 6, 7, 14–18]. However, there is a lack of information concerning the association among the oral microbiome, dental caries, and obesity during the COVID-19 pandemic, caused by lifestyle changes in the childhood population. Therefore, this mini-review aimed to review the available literature regarding a possible relationship between the oral and gut microbiome, caries, and obesity in children during the COVID-19 pandemic era.
Subsection and Discussion
Methodology
We conducted a literature search of articles at the PubMed database concerning oral and gut microbiome, caries, obesity, and COVID-19. No time period limits were placed, and key search terms included are described in the Appendix 1. Narrative and systematic reviews, experimental and observational studies in the English language were appraised and used as basis for conclusions. Manual search in the reference list of the main papers were also used to detect other relevant manuscripts. Full-text included articles were selected based on their title and abstract.
Obesity in Children and COVID-19 Pandemic
The COVID-19 social isolation and closing of schools and other extracurricular activities limited or completely compromised the learning of children, their social interactions, and performance of activities, which are essential for the good development and maintenance of children's physical and mental health [4, 7, 19]. The reduction in hours of physical exercise, the practices involving low energy expenditure, and sedentarism predispose to weight gain and consequent obesity [7, 19]. This is worrisome given the fact that childhood obesity can be strongly associated with weight gain in adults and subsequent comorbidities [5, 20].
Systematic reviews conducted during the COVID-19 pandemic explored the impact of lockdown on the diet, lifestyle changes, body weight, and body mass index (BMI) in children [19, 21, 22]. The COVID-19 control measures showed a negative impact on feeding practices and lifestyles, with an increase in central fat accumulation and body weight [21]. The meta-analysis of Chang et al. [19] also pointed to a significant BMI and weight gain during lockdown among school-age children and adolescents. The prevalence of obesity and overweight also enlarged [19]. By systematically reviewing the literature, Chaabane et al. [22] concluded that the longer the duration of school closure and the reduction of daily physical activity, the higher predicted increase of BMI and prevalence of childhood obesity.
Children's observational studies revealed that breakfast, sweets, and total snacks consumption, enlarged significantly during the lockdown, together with the fruits/fresh fruit juices, and vegetable intake [6, 7]. On the other hand, sports practices decreased, whereas sleep hours and screen time exposure were enhanced [6, 7]. Notably, weight gain was closely linked to the changes described above [7] as well, and depending on the duration period, these unhealthy habits may cause a residual impact on adiposity level in further stages of life, such as adolescence and adulthood [6].
The findings discussed above point to the need for public policy approaches to prevent future severe obesity and its associated comorbidities, to improve eating habits and the unhealthy lifestyle behaviors acquired during the unresolved COVID-19 era [21].
Furthermore, childhood obesity and weight gain may be associated with high levels of parental stress, due to job loss or changes in the routine and workplace, jointly with reduced income and social isolation. Altogether, these factors can consequently impair children's mental health and potentially raise their stress level [23]. Outstandingly, irrepressible stress changes feeding practices, stimulating the intake of high-fat/high sugar foods, referred to as hyper-palatable. Over time, this seems to trigger neurobiological adjustments connected to addictive patterns, and changes in hormones linked to appetite (i.e., sensitivity to insulin) and metabolism of glucose. Chronic stress might impact the brain's mesolimbic dopaminergic system and areas associated with rewards behavior and food preferences, favoring metabolic changes that promote weight and body fat/weight gain [24].
Thus, alterations in the lifestyle and routine of the child population due to the stressor COVID-19 pandemic can impact their systemic health and weight maintenance. Good and healthy relationships and family/community care during this hard and challenging phase are essential for physical and mental health and consequently better quality in later life [19, 23].
Despite the lack of studies exploring the interplay among microbiome, COVID-19, caries, and obesity, SARS-CoV-2 infection has already shown changes in the oral and gut microbiome [25, 26]. Oral and fecal microbial diversity was significantly decreased in patients with COVID-19 compared to healthy ones [25]. Interestingly, butyric acid-producing bacteria were decreased and lipopolysaccharide-producing bacteria were increased in the oral cavity of COVID-19 patients [25]. The SARS-CoV-2 infection showed elevated numbers of Granulicatella and Rothia mucilaginosa in both oral and gut microbiome [26].
Dental Caries in Children and COVID-19 Pandemic
At the beginning of the pandemic dental offices were closed due to the high risk of contamination by coronavirus during the contact with body fluids, especially saliva. With vaccination and the gradual reestablishment of routine, appointments also returned following strict biosecurity measures [27].
In the peak of the pandemic, only urgent care was provided to patients [28–30]. A cohort retrospective study in Germany revealed that during the pandemic period, emergency care increased by 45%, with the most common complaint being plaque-induced gingivitis, followed by dental caries. Most interventions in this epoch were less invasive and include pharmacological treatments [30].
As the prevention and the oral health care promotion for children is regulated by the frequency of follow-ups and dental appointments, there was an important lag in this face-to-face treatment during the lockdown [31]. In this context, teledentistry was able to provide remote diagnosis and oral care of children during pandemics [32, 33]. On the other hand, the lifestyle changes caused by social isolation, the socioeconomic status of the patients, and the temporary closure of dental clinics may have influenced the risk for caries lesions development.
There is not much information in the scientific literature about caries prevalence in children before and during the COVID-19 era, as well as regarding caries experience in children and socioeconomic status during social isolation. Cross-sectional studies investigated oral care, toothbrushing, and eating habits during the COVID-19 pandemic by self-report of parents or children [3, 16, 18]. While an increase in the consumption of sugary-rich food during the pandemic was noticed, children's reports of brushing habits varied among studies, i.e., brushing habits did not change or worsened [3, 16, 18].
The eating habits, lifestyle, and home oral hygiene during the COVID-19 pandemic were assessed in the Italian pediatric population, regarding caries risk [3]. During social isolation, children were moderately or vigorously less active, watching more television programs. Despite the fact that the consumption of sweets and the number of meals increased, children did not change their brushing habits. However, dental pain and abscesses were declared in some cases [3]. In Wuhan city, during the lockdown, the preschool children related being more active in brushing their teeth; nevertheless, 60.8, 35.5, and 18.3% of children had, respectively, self-reported dental caries, toothache, and halitosis [16]. Similarly, in Brazil and Portugal, parents/caregivers reported changes in the child's routine during COVID-19 social isolation, and sleep disorders were associated with poor oral hygiene [18].
Also, children were forced to spend most of their time at home during home confinement, and the acquisition of incorrect alimentary habits was favored [3, 16, 31], as well as increased stress levels [18, 31]. These factors might have influenced their risk of carious lesions development. It was shown that stress, sleep disturbances, and other changes in routine during social isolation encouraged parents to apply different sleep schedules in their young children, and baby bottles containing sugary and fermentable liquids were given to calm them down. This change of behavior may have increased the risk of ECC during the COVID-19 pandemic [31]. Interestingly, high exposure to fermentable carbohydrates and sugar is also linked to an enlarged incidence of childhood obesity [34]. Conversely, unlike obesity, caries can interpolate periods of activity and inactivity, making the early diagnosis in the initial stages of the disease challenging [35]. The exact incidence of carious lesions during the COVID-19 pandemic may be underreported due to its subclinical stage (not cavitated lesions), together with the closure of dental clinics [35]. In this scenario, the attention of pediatric dentists during the clinical examinations should be doubled.
The use of minimally invasive therapies for the management of carious lesions in primary teeth is well accepted among the childhood population and was broadly used during pandemics [28, 36]. Of interest, children are mainly asymptomatic for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), which can contribute to the uncertainty of their infectious status; and they can cough, sneeze, and cry during dental treatment, which can generate more natural aerosols when compared to treatment in adults [28]. Thus, the use of minimally invasive therapies with reduced Aerosol Generating Procedures (AGP), such as selective carious tissue removal, sealants, resin infiltration, and silver diamine fluoride application, atraumatic restorative, and Hall technique diminished the risk of viral cross-infection, favoring a safer clinical environment [28, 36]. Probably, specific recommendations for dental management in pediatric patients during the COVID-19 pandemic will be kept in the post-COVID-19 era, such as AGP procedures replacement, and personalization of non-invasive or minimally invasive methods [37].
It is relevant to keep parents informed about the protective and cariogenic properties of different kinds of diet plenty of fruit and vegetables can help to protect from the onset of caries, by vigorous mastication, mechanically stimulating salivary production and rate. Additionally, fruits and vegetables are connected to weight gain and obesity prevention and control. Therefore, there is a substantial need for a common risk approach concerning caries and obesity in young children, especially in periods of confinement [31]. The role played by effective campaigns of hygiene education, dental care improvement, and stimuli of a healthy lifestyle [3, 31] should be highlighted, since they can reduce the risk for both diseases.
Early Childhood Caries, Obesity, Oral, and Gut Microbiome
Dental caries or tooth decay is one of the most common diseases in childhood and its global prevalence approaches 600 million children [38, 39]. Early childhood caries (ECC) is defined as a carious lesion in one or more primary teeth, with or without cavitation, in children under 6 years of age. It is related to the frequent consumption of carbohydrates, especially sugars, and inadequate or lack of oral hygiene in small children, which can make the enamel prone to demineralization [40–42]. Pain, discomfort, poor nutrition, sleep impairment, damage to normal physical development, and even a possible increase in the risk of hospitalization, are some of the negative consequences of dental caries in children [41–44]. As ECC is a multifactorial disease, it is also determined by biological, environmental, social, economic, cultural, behavioral, and psychological factors [31, 45].
Obesity is also a chronic and multifactorial disease, resulting from energy imbalance, where more energy is consumed than is expended. It can be characterized by excessive accumulation of fat in body tissues [46]. Childhood weight can be determined by the body mass index (BMI), and in ones under the age of 5, overweight is considered when percentiles are >97 ≤ 99,9 and obesity when percentiles are higher than 99,9. In 2020, nearly 40 million children 5 years or younger, are expected to be overweight or obese around the world [47]. As a risk factor for adulthood obesity, childhood overweight and obesity can lead to other chronic diseases such as diabetes, cardiovascular and metabolic dysfunctions, sleep apnea, even depression, and certain types of cancer [48–50].
In terms of oral health, overweight and obese children are twice as likely to have ECC compared to the ones with adequate weight [34]. The association between caries and obesity is also found in adolescents [51, 52]. However, diet is not the only common causal factor related to dental caries and obesity, and the microbiota dysbiosis play also important roles in this context [9, 12]. The human microbiome is composed of microorganisms, about 100 trillion, that colonize the human body dynamically and can be altered by environmental factors such as drug use, disease response, hygiene, and diet; constantly interacting with the host in health and disease situations [53–55].
The oral cavity is colonized by a variety of microbial communities, including viruses, protozoa, fungi, and bacteria, making the oral microbiome one of the most complex, with over 1,000 species of bacteria alone [56, 57]. Among the bacteria, the presence of Streptococcus mutans, Lactobacillus spp., Porphyromonas gingivalis, and Aggregatibacter actinomycetemcomitans should be highlighted, as they are relevant pathogens for dental caries and periodontal diseases [58, 59].
With the development of the deciduous dentition in children, tooth tissues appear and an enamel structure is introduced into the oral cavity favoring microbial colonization and leading to changes in the oral microbiome [60]. Dental caries is an oral biofilm-mediated disease caused mainly by the initial colonization of Streptococcus mutans that metabolize fermentable carbohydrates, especially sucrose. The combination of a sugar-rich diet with poor oral hygiene potentialize the cariogenic biofilm formation on the teeth surfaces, with increased production of acid. This way, the pH of the oral environment is altered, and the demineralization of dental tissues takes place, leading to early carious lesions or white chalky spots, that further progresses into cavities [22, 61, 62]. As the cavitation stage progresses, Lactobacillus spp. [63, 64], together with other microorganisms could be identified in dentine caries lesions: Bifidobacterium spp., species of Veillonella, Actinomyces, Prevotella, and Porphyromonas, as well as C. albicans [65, 66].
Although carious lesions involve a variety of microorganisms, as stated above, acidogenic and aciduric bacteria are predominant, and it is possible to perceive an initial dysbiosis [67–69]. Intriguingly, in children with severe ECC a less complex microbiome, with low biofilm microbial variety has been reported, because unfilled cavities can act as an ecological niche for cariogenic bacteria that, by competition, dominate and force down the proliferation of other microorganisms [70].
The dysbiotic state described in the caries development can interplay with the gut microbiome and with the gut dysbiosis, influencing the production of gastrointestinal peptides associated with satiety. This dysfunction can lead to an increase in food consumption, and consequent weight gain [10]. Considering that the bacteria in the oral cavity can spread through the epithelial surfaces of the body and reach several areas [11], the connection between ECC, obesity, and microbial dysbiosis becomes more evident [71, 72]. When dental caries progresses until a severe stage, the pulp (an organ full of nerves and capillaries) is exposed, favoring a bacteremia via the bloodstream, in a way that microbes get access to other organs, such as the heart [10]. Some groups of bacteria could overlap in oral and stool samples [9, 10, 72], due to oral bacteria often being swallowed together with saliva and food during the digestion process. Furthermore, two of the main caries pathogens, Streptococcus mutans, and Lactobacillus spp., belong to Firmicutes phylum, which is more abundant in the gut microbiota of obese children [12, 13, 73]. Other bacteria are also related to weight gain, for example, Eubacterium halllii and Clostridium leptum, the last one being considered important in the fermentation of carbohydrates and the production of short-chain fatty acids [12, 74].
A recent cross-sectional study investigated the relationship between Firmicutes and Bacteroidetes oral and gut levels, with respect to obesity and ECC, suggesting that oral Firmicutes can reflect the gut condition in preschool-aged obese children, modulated by ECC [72]. A systematic review and meta-analyses investigated whether children aged 6 years and younger with overweight and/or obesity could have higher dental caries experience compared with children with normal weight. Children with overweight and obesity were more vulnerable to dental caries, and the low levels of parental income and education were the main associated factors. The diet alone cannot explain the experience of caries, as this complex disease could be affected by lots of other factors [34].
In the scenario described above, changes in lifestyle and wellbeing habits can impact the oral and systemic health in the childhood population, mediated by an imbalance in their oral and gut microbiome [8–13, 69, 71, 73, 74] (Figure 1). The central role of oral bacteria that ectopically colonize the gut remains unknown [8–12], but it is notorious that ECC and obesity continue to affect millions of children, even though being preventable diseases [10]. Thus, the interplay between oral and gut microbiome needs to be further explored, bringing valuable information to better understand the course of both diseases, mainly in periods of lifestyle changes, favoring the establishment of effective prevention and control strategies.
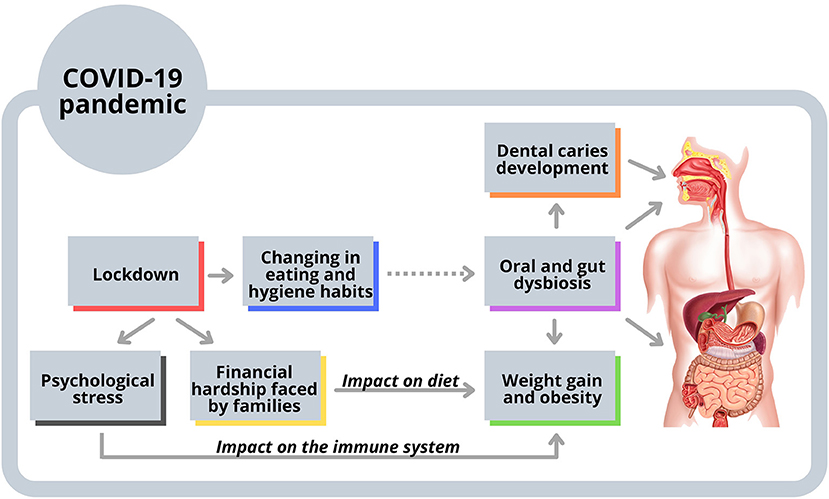
Figure 1. Possible interplay among oral and gut microbiome, dental caries, and obesity. The consumption of unhealthy food for children increased during the confinement of COVID-19 pandemic. Eating and hygiene habits were also changed and could affect the oral microbiome. As oral bacteria are frequently swallowed with food and beverages during the digestion process, they can reach the gastrointestinal tract influencing the gut dysbiosis and weight gain. Also, factors linked to the lockdown, such as psychological stress and financial hardship faced by families, could have impacted the immune system, eating habits, and obesity.
Final Considerations
It is known that the COVID-19 pandemic and its restrictions were not homogeneous around the world, and due to the variations in the way on how the pandemic was treated or experienced in each country, prospective studies are scarce. Although there is a gap in the scientific literature concerning the interplay among oral and gut microbiome, dental caries, and obesity in the COVID-19 era, the present mini-review showed that during the stressor pandemic period the carious lesions development in primary teeth and weight gain were probably favored. Changes in hygiene habits and increased exposure to hyper-palatable foods during pandemic could characterize a caries dysbiotic environment. High-fat/high sugar meals could be also allied to gut dysbiosis in obesity pathogenesis. Considering that other factors linked to the lockdown, such as anxiety, tension, and sleep disorders could impact on the immune system and also exacerbate caries and obesity, a relationship between these diseases could have been reinforced in the pandemic. In addition, the pandemic has brought financial hardship faced by families, especially those in developing countries, which also had a direct impact on diet and obesity.
Even though multiple attempts have been made for caries and obesity prevention in childhood these disturbances are extremely difficult to manage, particularly under stressful situations. So, it is imperative to deeply improve the understanding of the complex interrelationship between the mouth and other body systems, as well as oral and systemic diseases, which cannot be studied separately. A holistic and multidisciplinary model of care for young patients is necessary for a humanized clinical practice based on scientific evidence, focused on the integrality of the child human being, stimulating the development of effective prevention and treatment measures. It is also a priority to develop public policies based on health care for children and parents in the COVID-19 era, especially focusing on diet, oral hygiene, mental health, physical activities, and a healthy lifestyle.
Author Contributions
FC, RR, and TP: conceptualization and writing-review and editing. FC, RR, HC, RS, and FS: writing-original draft preparation. TP and FC: supervision. All authors significantly contributed to the manuscript preparation and approved the final version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/froh.2022.887765/full#supplementary-material
References
1. Valenzise M, D'Amico F, Cucinotta U, Lugarà C, Zirilli G, Zema A, et al. The lockdown effects on a pediatric obese population in the COVID-19 era. Ital J Pediatr. (2021) 47:209. doi: 10.1186/s13052-021-01142-0
2. Cucinotta D, Vanelli M. WHO Declares COVID-19 a Pandemic. Acta Biomed. (2020) 91:157–60. doi: 10.23750/abm.v91i1.9397
3. Docimo R, Costacurta M, Gualtieri P, Pujia A, Leggeri C, Attinà A, et al. Cariogenic risk and COVID-19 lockdown in a paediatric population. Int J Environ Res Public Health. (2021) 18:7558. doi: 10.3390/ijerph18147558
4. Sama BK, Kaur P, Thind PS, Verma MK, Kaur M, Singh DD. Implications of COVID-19-induced nationwide lockdown on children's behaviour in Punjab, India. Child Care Health Dev. (2021) 47:128–35. doi: 10.1111/cch.12816
5. Rundle AG, Park Y, Herbstman JB, Kinsey EW, Wang YC. COVID-19-related school closings and risk of weight gain among children. Obesity. (2020) 28:1008–09. doi: 10.1002/oby.22813
6. Pietrobelli A, Pecoraro L, Ferruzzi A, Heo M, Faith M, Zoller T, et al. Effects of COVID-19 lockdown on lifestyle behaviors in children with obesity living in Verona, Italy: a longitudinal study. Obesity. (2020) 28:1382–5. doi: 10.1002/oby.22861
7. Androutsos O, Perperidi M, Georgiou C, Chouliaras G. Lifestyle changes and determinants of children's and adolescents' body weight increase during the first COVID-19 lockdown in Greece: The COV-EAT Study. Nutrients. (2021) 13:930. doi: 10.3390/nu13030930
8. Gomez A, Nelson KE. The oral microbiome of children: development, disease, and implications beyond oral health. Microb Ecol. (2017) 73:492–503. doi: 10.1007/s00248-016-0854-1
9. Indiani C, Rizzardi KF, Crescente CL, Steiner-Oliveira C, Nobre-Dos-Santos M, Parisotto TM. Relationship between mutans streptococci and lactobacilli in the oral cavity and intestine of obese and eutrophic children with early childhood caries-preliminary findings of a cross-sectional study. Front Pediatr. (2020) 8:588965. doi: 10.3389/fped.2020.588965
10. Sabella FM, Feiria SNB, Ribeiro AA, Theodoro LH, Höfling JF, Parisotto TM, et al. Exploring the interplay between oral diseases, microbiome, and chronic diseases driven by metabolic dysfunction in childhood. Front Dent Med. (2021) 2:718441. doi: 10.3389/fdmed.2021.718441
11. Olsen I, Yamazaki K. Can oral bacteria affect the microbiome of the gut? J Oral Microbiol. (2019) 11:1586422. doi: 10.1080/20002297.2019.1586422
12. Indiani C, Rizzardi KF, Castelo PM, Ferraz L, Darrieux M, Parisotto TM. Childhood obesity and Firmicutes/Bacteroidetes ratio in the gut microbiota: a systematic review. Chil Obes. (2018) 14:501–9. doi: 10.1089/chi.2018.0040
13. Gallardo-Becerra L, Cornejo-Granados F, García-López R, Valdez-Lara A, Canizales-Quinteros BS, et al. Metatranscriptomic analysis to define the Secrebiome, and 16S rRNA profiling of the gut microbiome in obesity and metabolic syndrome of Mexican children. Microb Cell Fact. (2020) 19:61. doi: 10.1186/s12934-020-01319-y
14. Campagnaro R, Collet GO, Andrade MP, Salles J, Calvo Fracasso ML, Scheffel D, et al. COVID-19 pandemic and pediatric dentistry: fear, eating habits and parent's oral health perceptions. Child Youth Serv Rev. (2020) 118:105469. doi: 10.1016/j.childyouth.2020.105469
15. Gotler M, Oren L, Spierer S, Yarom N, Ashkenazi M. The impact of COVID-19 lockdown on maintenance of children's dental health: a questionnaire-based survey. J Am Dent Assoc. (2021) 153:440-9. doi: 10.1016/j.adaj.2021.10.004
16. Liu C, Zhang S, Zhang C, Tai B, Jiang H, Du M. The impact of coronavirus lockdown on oral healthcare and its associated issues of pre-schoolers in China: an online cross-sectional survey. BMC Oral Health. (2021) 21:54. doi: 10.1186/s12903-021-01410-9
17. Goswami M, Grewal M, Garg A. Attitude and practices of parents toward their children's oral health care during COVID-19 pandemic. J Indian Soc Pedod Prev Dent. (2021) 39:22–8. doi: 10.4103/jisppd.jisppd_478_20
18. Baptista AS, Prado IM, Perazzo MF, Pinho T, Paiva SM, Pordeus IA, et al. Can children's oral hygiene and sleep routines be compromised during the COVID-19 pandemic? Int J Paediatr Dent. (2021) 3:12–9. doi: 10.1111/ipd.12732
19. Chang TH, Chen YC, Chen WY, Chen CY, Hsu WY, Chou Y, et al. Weight gain associated with COVID-19 lockdown in children and adolescents: a systematic review and meta-analysis. Nutrients. (2021) 13:3668. doi: 10.3390/nu13103668
20. Rundle AG, Factor-Litvak P, Suglia SF, Susser ES, Kezios KL, Lovasi GS, et al. Tracking of obesity in childhood into adulthood: effects on body mass index and fat mass index at age 50. Child Obes. (2020) 16:226–33. doi: 10.1089/chi.2019.0185
21. Karatzi K, Poulia KA, Papakonstantinou E, Zampelas A. The impact of nutritional and lifestyle changes on body weight, body composition and cardiometabolic risk factors in children and adolescents during the pandemic of COVID-19: a systematic review. Children. (2021) 8:1130. doi: 10.3390/children8121130
22. Chaabane S, Doraiswamy S, Chaabna K, Mamtani R, Cheema S. The impact of COVID-19 school closure on child and adolescent health: a rapid systematic review. Children. (2021) 8:415. doi: 10.3390/children8050415
23. Browne NT, Snethen JA, Greenberg CS, Frenn M, Kilanowski JF, Gance-Cleveland B, et al. When pandemics collide: the impact of COVID-19 on childhood obesity. J Pediatr Nurs. (2021) 56:90–8. doi: 10.1016/j.pedn.2020.11.004
25. Ren Z, Wang H, Cui G, Lu H, Wang L, Luo H, et al. Alterations in the human oral and gut microbiomes and lipidomics in COVID-19. Gut. (2021) 70:1253–65. doi: 10.1136/gutjnl-2020-323826
26. Wu Y, Cheng X, Jiang G, Tang H, Ming S, Tang L, et al. Altered oral and gut microbiota and its association with SARS-CoV-2 viral load in COVID-19 patients during hospitalization. NPJ Biofilms Microbiomes. (2021) 7:61. doi: 10.1038/s41522-021-00232-5
27. Sharma A, Jain MB. Dentistry during Coronavirus Disease-2019 pandemic: a paradigm shift in treatment options. Int J Clin Ped Dent. (2020) 13:412–15. doi: 10.5005/jp-journals-10005-1809
28. BaniHani A, Gardener C, Raggio DP, Santamaría RM, Albadri S. Could COVID-19 change the way we manage caries in primary teeth? Current implications on Paediatric Dentistry. Int J Paediatr Dent. (2020) 30:523–25. doi: 10.1111/ipd.12690
29. Alzahrani SB, Alrusayes AA, Alfraih YK, Aldossary MS. Characteristics of paediatric dental emergencies during the COVID-19 pandemic in Riyadh City, Saudi Arabia. Eur J Paediatr Dent. (2021) 22:95–7. doi: 10.1007/s40368-021-00618-1
30. Al Masri A, Abudrya M, Splieth CH, Schmoeckel J, Mourad MS, Santamaría RM. How did the COVID-19 pandemic lockdown affect dental emergency care in children? retrospective study in a specialized pedodontic center. Quintessence Int. (2021) 52:788–96. doi: 10.3290/j.qi.b1763637
31. Luzzi V, Ierardo G, Bossù M, Polimeni A. Paediatric oral health during and after the COVID-19 pandemic. Int J Paed Dent. (2021) 31:20–6. doi: 10.1111/ipd.12737
32. Rahman N, Nathwani S, Kandiah T. Teledentistry from a patient perspective during the coronavirus pandemic. Br Dent J. (2020) 14:1–4. doi: 10.1038/s41415-020-1919-6
33. Sharma H, Suprabha BS, Rao A. Teledentistry and its applications in paediatric dentistry: a literature review. Pediatr Dent J. (2021) 31:203–15. doi: 10.1016/j.pdj.2021.08.003
34. Manohar N, Hayen A, Fahey P, Arora A. Obesity and dental caries in early childhood: a systematic review and meta-analyses. Obes Rev. (2020) 21:e12960. doi: 10.1111/obr.12960
35. Jayam C, Babu TA. Dental caries in children during COVID-19 pandemic - are we doing enough? Indian Pediatr. (2021) 58:999. doi: 10.1007/s13312-021-2344-x
36. Cianetti S, Pagano S, Nardone M, Lombardo G. Model for taking care of patients with early childhood caries during the SARS-Cov-2 Pandemic. Int J Environ Res Public Health. (2020) 17:3751. doi: 10.3390/ijerph17113751
37. Al-Halabi M, Salami A, Alnuaimi E, Kowash M, Hussein I. Assessment of paediatric dental guidelines and caries management alternatives in the post COVID-19 period. a critical review and clinical recommendations. Eur Arch Paediatr Dent. (2020) 21:543–56. doi: 10.1007/s40368-020-00547-5
38. Kassebaum NJ, Bernabé E, Dahiya M, Bhandari B, Murray CJ, Marcenes W. Global burden of untreated caries: a systematic review and metaregression. J Dent Res. (2015) 94:650–8. doi: 10.1177/0022034515573272
39. World Health Organization. Oral Health. (2020). Available online at: https://www.who.int/news-room/fact-sheets/detail/oral-health (accessed January 20, 2022).
40. Pitts NB, Zero DT, Marsh PD, Ekstrand K, Weintraub JA, Ramos-Gomez F, et al. Dental caries. Nat Rev Dis Primers. (2017) 3:17030. doi: 10.1038/nrdp.2017.30
41. Leong PM, Gussy MG, Barrow S-YL, de Silva-Sanigorski A, Waters E. A systematic review of risk factors during first year of life for early childhood caries. Int J Paediatr Dent. (2013) 23:235–50. doi: 10.1111/j.1365-263X.2012.01260.x
42. Machiulskiene V, Campus G, Carvalho JC, Dige I, Ekstrand KR, Jablonski-Momeni A, et al. Terminology of dental caries and dental caries management: consensus report of a workshop organized by ORCA and cariology research group of IADR. Caries Res. (2020) 54:7–14. doi: 10.1159/000503309
43. Martins-Júnior PA, Vieira-Andrade RG, Corrêa-Faria P, Oliveira- Ferreira F, Marques LS, Ramos-Jorge ML. Impact of early childhood caries on the oral health-related quality of life of preschool children and their parents. Caries Res. (2013) 47:211–18. doi: 10.1159/000345534
44. Acharya A, Khan S, Hoang H, Bettiol S, Goldberg L, Crocombe L. Dental conditions associated with preventable hospital admissions in Australia: a systematic literature review. BMC Health Serv Res. (2018) 18:921. doi: 10.1186/s12913-018-3733-2
45. Costacurta M, Epis M, Docimo R. Evaluation of DMFT in paediatric patients with social vulnerability conditions. Eur J Paediatr Dent. (2020) 21:70–3. doi: 10.23804/ejpd.2020.21.01.14
46. Lin X, Li H. Obesity: epidemiology, pathophysiology, and therapeutics. Front Endocrinol. (2021) 12:706978. doi: 10.3389/fendo.2021.706978
47. World Health Organization (2021). About Child & Teen BMI. Healthy Weight, Nutrition, and Physical Activity. Division of Nutrition, Physical Activity, and Obesity, National Center for Chronic Disease Prevention and Health Promotion. Available online at: https://www.cdc.gov/healthyweight/assessing/bmi/childrensbmi/aboutchildrensbmi.html (accessed January 20, 2022).
48. Swinburn BA, Sacks G, Hall KD, McPherson K, Finegood DT, Moodie ML, et al. The global obesity pandemic: shaped by global drivers and local environments. Lancet. (2011) 378:804–14. doi: 10.1016/S0140-6736(11)60813-1
49. Sanders RH, Han A, Baker JS, Cobley S. Childhood obesity and its physical and psychological co-morbidities: a systematic review of Australian children and adolescents. Eur J Pediatr. (2015) 174:715–46. doi: 10.1007/s00431-015-2551-3
50. Anderson AS, Key TJ, Norat T, Scoccianti C, Cecchini M, Berrino F, et al. European code against cancer 4th edition: obesity, body fatness, and cancer. Cancer Epidemiol. (2015) 39:S34–45. doi: 10.1016/j.canep.2015.01.017
51. Li LW, Wong HM, McGrath CP. Longitudinal association between obesity and dental caries in adolescents. J Pediatr. (2017) 189:149–54. doi: 10.1016/j.jpeds.2017.06.050
52. Al-Ansari A, Nazir M. Relationship between obesity and dental caries in Saudi male adolescents. Int J Dent. (2020) 2020:8811974. doi: 10.1155/2020/8811974
53. Lozupone CA, Stombaugh JI, Gordon JI, Jansson JK, Knight R. Diversity, stability and resilience of the human gut microbiota. Nature. (2012) 489:220–30. doi: 10.1038/nature11550
54. Amon P, Sanderson I. What is the microbiome? Arch Dis Child Educ Practice Ed. (2017) 102:257–60. doi: 10.1136/archdischild-2016-311643
55. Toor D, Wsson MK, Kumar P, Karthikeyan G, Kaushik NK, Goel C, et al. Dysbiosis disrupts gut immune homeostasis and promotes gastric diseases. Int J Mol Sci. (2019) 20:2432. doi: 10.3390/ijms20102432
56. Wade WG. The oral microbiome in health and disease. Pharmacol Res. (2013) 69:137–43. doi: 10.1016/j.phrs.2012.11.006
57. Dewhirst FE, Chen T, Izard J, Paster BJ, Tanner AC, Yu WH, et al. The human oral microbiome. J Bacteriol. (2010) 192:5002–17. doi: 10.1128/JB.00542-10
58. Holt SC, Ebersole JL. Porphyromonas Gingivalis, Treponema Denticola, and Tannerella Forsythia: the “red complex”, a prototype polybacterial pathogenic consortium in periodontitis. Periodontol 2000. (2005) 38:72–122. doi: 10.1111/j.1600-0757.2005.00113.x
59. Takahashi N. Oral Microbiome metabolism: from “who are they?” To “what are they doing?” J Dent Res. (2015) 94:1628–37. doi: 10.1177/0022034515606045
60. Mason MR, Chambers S, Dabdoub SM, Thikkurissy S, Kumar PS. Characterizing oral microbial communities across dentition states and colonization niches. Microbiome. (2018) 6:1–10. doi: 10.1186/s40168-018-0443-2
61. Aas JA, Griffen AL, Dardis SR, Lee AM, Olsen I, Dewhirst FE, et al. Bacteria of dental caries in primary and permanent teeth in children and young adults. J Clin Microbiol. (2008) 46:1407–17. doi: 10.1128/JCM.01410-07
62. Mulu W, Demilie T, Yimer M, Meshesha K, Abera B. Dental caries and associated factors among primary school children in Bahir Dar city: a cross-sectional study. BMC Res Notes. (2014) 7:949. doi: 10.1186/1756-0500-7-949
63. Parisotto TM, Steiner-Oliveira C, Duque C, Peres RCR, Rodrigues LKA, Nobre-dos-Santos M. Relationship among microbiological composition and presence of dental plaque, sugar exposure, social factors and different stages of early childhood caries. Arch Oral Biol. (2010) 55:365. doi: 10.1016/j.archoralbio.2010.03.005
64. Ledder RG, Kampoo K, Teanpaisan R, McBain AJ. Oral microbiota in severe early childhood caries in thai children and their families: a pilot study. Front Microbiol. (2018) 9:2420. doi: 10.3389/fmicb.2018.02420
65. Tanner ACR, Kent RL, Holgerson PL, Hughes CV, Chalmers NI, Johansson I. Microbiota of severe early childhood caries before and after therapy. J Dent Res. (2011) 90:1298–305. doi: 10.1177/0022034511421201
66. Xiao J, Grier A, Faustoferri RC, Alzoubi S, Gill AL, Feng C, et al. Association between oral candida and bacteriome in children with severe ECC. J Dent Res. (2018) 97:1468–76. doi: 10.1177/0022034518790941
67. Selwitz RH, Ismail AI, Pitts NB. Dental caries. Lancet. (2007) 369:51–9. doi: 10.1016/S0140-6736(07)60031-2
68. Seow WK. Early childhood caries. Pediatr Clin North Am. (2018) 65:941–54. doi: 10.1016/j.pcl.2018.05.004
69. Tanner ACR, Kressirer CA, Rothmiller S, Johansson I, Chalmers NI. The caries microbiome: implications for reversing dysbiosis. Adv Dent Res. (2018) 29:78–85. doi: 10.1177/0022034517736496
70. Li Y, Ge Y, Saxena D, Caufield PW. Genetic profiling of the oral microbiota associated with severe early-childhood caries. J Clin Microbiol. (2007) 45:81–7. doi: 10.1128/JCM.01622-06
71. Zhan L. Rebalancing the caries microbiome dysbiosis: targeted treatment and sugar alcohols. Adv Dent Res. (2018) 29:110–6. doi: 10.1177/0022034517736498
72. Rizzardi KF, Indiani CMSP, Mattos-Graner RO, de Sousa ET, Nobre-dos-Santos M, et al. Firmicutes levels in the mouth reflect the gut condition with respect to obesity and early childhood caries. Front Cell Infect Microbiol. (2021) 11:593734. doi: 10.3389/fcimb.2021.593734
73. Da Silva CC, Monteil MA, Davis EM. Overweight and obesity in children are associated with an abundance of firmicutes and reduction of bifidobacterium in their gastrointestinal microbiota. Child Obes. (2020) 16:204–10. doi: 10.1089/chi.2019.0280
Keywords: child, obesity, dental caries, gastrointestinal microbiome, COVID-19 pandemic
Citation: Reis RM, Carlo HL, Santos RLd, Sabella FM, Parisotto TM and Carvalho FGd (2022) Possible Relationship Between the Oral and Gut Microbiome, Caries Development, and Obesity in Children During the COVID-19 Pandemic. Front. Oral. Health 3:887765. doi: 10.3389/froh.2022.887765
Received: 02 March 2022; Accepted: 28 April 2022;
Published: 30 May 2022.
Edited by:
Naile Dame-Teixeira, University of Brazilia, BrazilReviewed by:
Beatriz Gonçalves Neves, Federal University of Ceará Campus Sobral, BrazilPatricia Daniela Melchiors Angst, Federal University of Rio Grande do Sul, Brazil
Copyright © 2022 Reis, Carlo, Santos, Sabella, Parisotto and Carvalho. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fabíola Galbiatti de Carvalho, ZmFiaWdhbGJpQHlhaG9vLmNvbS5icg==