 Chee Weng Yong
Chee Weng Yong Andrew Robinson
Andrew Robinson Catherine Hong
Catherine Hong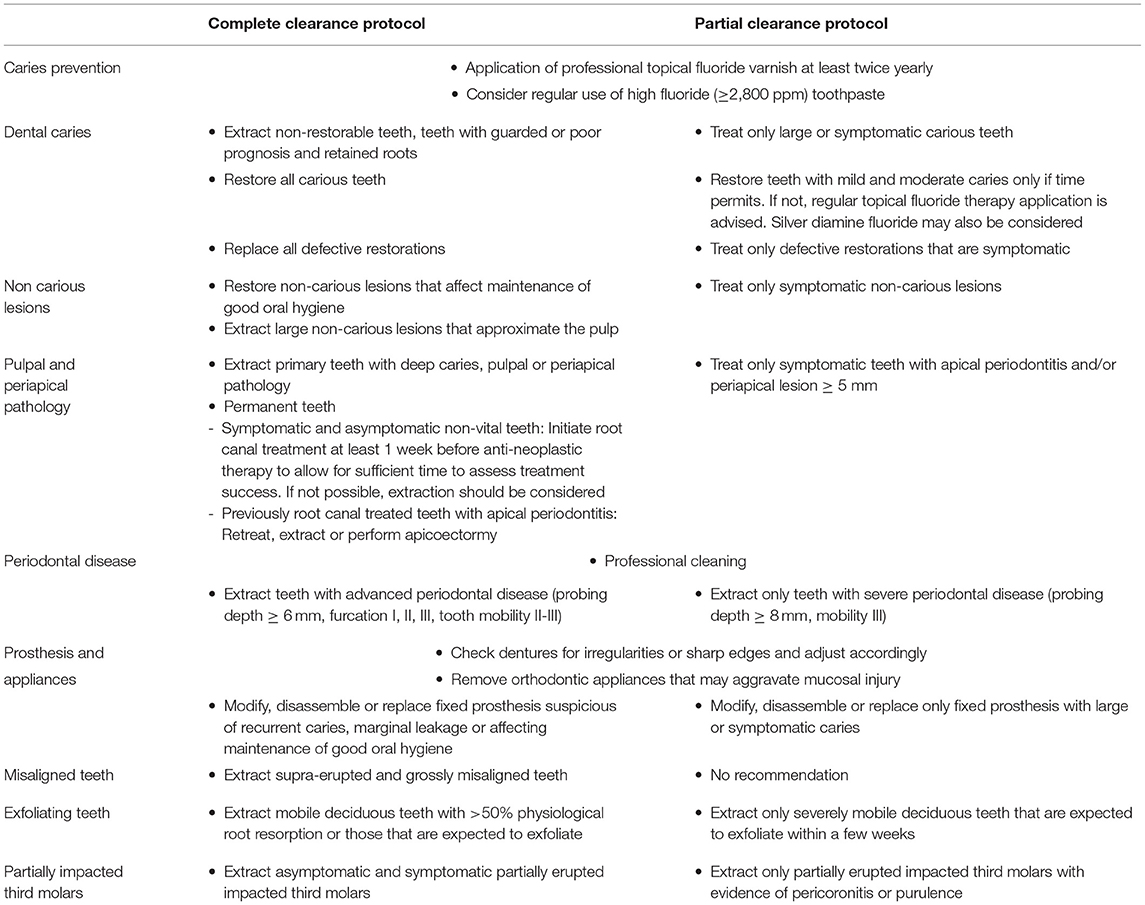

94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Oral. Health, 18 April 2022
Sec. Oral Cancers
Volume 3 - 2022 | https://doi.org/10.3389/froh.2022.876941
This article is part of the Research TopicOral Complications in Cancer PatientsView all 19 articles
A comprehensive oral examination and dental care prior to the start of cancer therapy is the standard of care in many cancer centers. This is because good oral health will likely minimize the undesirable complications such as opportunistic infections during cancer therapy. As the considerations differ between anti-neoplastic regimens, this chapter discusses the indications and rationale when planning and executing a treatment plan for patients undergoing various cancer therapies.
Many cancer centers routinely recommend that patients undergo a comprehensive oral examination and if necessary, receive dental treatment prior to the commencement of anti-neoplastic therapy [1, 2]. This concept is commonly referred to as “dental clearance” and the rationale for this is based on the assumption that good oral health can likely minimize the undesirable oral sequelae from anti-neoplastic therapy [3, 4]. For instance, basic oral care strategies to improve oral health modifies the oral microbial load, which is proposed to decrease oral mucositis severity via modulation of the host inflammatory response [5]. As there are ethical issues with the conduct of clinical trials evaluating the benefit of dental clearance, the evidence regarding the effectiveness of dental clearance protocols and the extent of clearance needed to prevent or minimize oral complications arising during anti-neoplastic therapy is limited [2]. Thus, dental clearance protocols often vary between cancer centers; especially with regard to the aggressiveness of dental therapy needed (e.g., need for removal of asymptomatic partially impacted third molars). Despite these differences, the majority of dental clearance protocols generally follow these principles: [1] to stabilize and/or remove existing and potential sources of infection and irritation in the oral cavity and [2] to educate patient regarding the acute and chronic oral manifestations associated with anti-neoplastic therapy as well as oral care recommendations throughout their anti-neoplastic therapy [1, 4].
This aim of this chapter is to review the indications, rationale and guiding principles when planning and executing a dental treatment plan for patients undergoing anti-neoplastic therapy.
As the considerations differ between anti-neoplastic regimens, dental practitioners should be cognizant of the rationale and objectives for dental clearance for the various anti-neoplastic therapies.
The main mechanism of anti-neoplastic chemotherapeutics is the inhibition of cell proliferation and growth [6]. The majority of these agents do not differentiate between the cancer and healthy tissues; thus rapidly dividing non-cancerous tissues such as the hair follicles, skin or the bone marrow are also affected by anti-neoplastic chemotherapeutics [7]. Of significance to dentistry is the suppression of the bone marrow resulting in immunosuppression, which predisposes the patient to increased risk of opportunistic viral and fungal infections [8, 9]. Exacerbation of pre-existing oral or dental infections can also occur and may be complicated by superinfection and necrosis [10–13]. Oral mucositis, which is associated with the use of certain chemotherapy agents (e.g., methotrexate, doxorubicin, 5-fluorouracil, busulfan, bleomycin, and platinum co-ordination complexes) further increases the risk of a systemic infection from a local site due to the loss of an intact oral mucosal barrier [13–17].
The extent of bone marrow suppression is dependent on the chemotherapeutic regimen. Non-myeloablative regimens are reduced in intensity and do not completely suppress the bone marrow. They are usually used as adjuvant treatment for a variety of solid organ malignancies. High-dose myeloablative chemotherapy regimens are typically indicated for patients with hematological malignancies and are associated with a significant decline in hemoglobin, platelet and neutrophil levels. This occurs about 7 days after the drug administration, with the nadir occurring between 10 and 14 days and recovery in 3–4 weeks. The recovery to functional blood count levels is prolonged in some patients for various reasons such as advanced age, decreased clearance of chemotherapeutic drugs due to renal or liver dysfunction or concurrent radiotherapy to the bone marrow [18–20]. For allogeneic hematopoietic stem cell transplantation recipients, a certain degree of immunosuppression is deliberately maintained for 6–12 months after myeloablative chemotherapy for prophylaxis against graft-vs.-host-disease [21]. For the reasons mentioned above, the primary aim for dental evaluation in patients undergoing anti-neoplastic chemotherapy and hematopoietic stem cell transplantation is to prevent and minimize the occurrence of opportunistic infections and the potential systemic spread of a local infection [22, 23].
Radiation therapy is the use of ionizing radiation to diminish or kill cancer cells. Unlike anti-neoplastic chemotherapy where only rapidly proliferating cells are targeted, radiation therapy affects all structures in the exposed field. The main dental concern with head and neck radiation therapy (HNRT) is the life-long risk of Osteoradionecrosis of the Jaw (ORNJ) development with radiation doses ≥ 60 Gy [24–32]. ORNJ is defined as a slow-healing radiation-induced ischemic necrosis of bone with or without associated soft tissue necrosis of variable extent, occurring in the absence of local primary tumor necrosis, recurrence, or metastatic disease [33]. The reported prevalence of ORNJ is ~3–7% [34, 35]. The mandible, radiation doses ≥ 65–70 Gy [25, 26], co-morbidities (e.g., diabetes mellitus, excessive alcohol consumption), poor oral health, invasive dental treatment and ill-fitting prosthesis have been associated with higher risk of ORNJ development [24, 27–32, 36]. The treatment of ORNJ is based on the severity and remains challenging. Current treatment modalities range from antibiotic therapy, combination therapy with pentoxifylline, tocopherol and/or clodronate, hyperbaric oxygen therapy and surgical intervention [37–39]. Other significant oral manifestations arising from HNRT include permanent salivary gland hypofunction and trismus which can occur at radiation doses as low as 20 and 50 Gy, respectively [40–43]. Both conditions exponentially increase the patient's caries risk resulting in rapidly progressing dental decay. In view of the life-long risk of ORNJ and its associated treatment challenges, the main objective of dental evaluation for HNRT patients is to eradicate local risk factors to minimize ORNJ risk. A secondary objective is to provide anticipatory guidance regarding preventive oral care strategies because of the high risk of rapidly progressing dental caries in post-HNRT patients.
The first reports of osteonecrosis of the jaw associated with bisphosphonates emerged in the early 2000s and was termed Bisphosphonates-Related Osteonecrosis of the Jaw [44]. This term was changed in 2014 to Medication Related Osteonecrosis of the Jaw (MRONJ) when reports of osteonecrosis of the jaw associated with the use of other anti-resorptive agents (ARAs) and anti-angiogenic agents (AAAs) were published [45]. ARAs are used in cancer therapy to prevent skeletal related events (e.g., pathological fractures, hypercalcemia of malignancy), while AAAs disrupt (neo) angiogenesis which hampers tumor growth and development. MRONJ is defined clinically by 3 criteria: (1) current or previous treatment with ARAs or AAAs; (2) exposed bone or bone that can be probed through an intra-oral or extra-oral fistula(s) in the maxillofacial region that has persisted for more than 8 weeks; and (3) no history of radiation therapy or obvious metastatic disease to the jaws [45]. The prevalence of MRONJ in cancer patients on ARAs or AAAs ranges widely between 0 and 18% [45, 46]. Longer duration of therapy, pre-existing inflammatory dental disease (e.g., periodontal disease), ill-fitting dentures, invasive dental procedures, uncontrolled diabetes mellitus, immunocompromised states and tobacco use are associated with higher risk [45–48]. Currently, there is no universally accepted treatment for MRONJ [46, 49, 50]. Treatment options include conservative symptomatic management, pharmacological interventions with pentoxifylline and tocopherol, hyperbaric oxygen therapy or surgical management [46, 49–51]. With the increasing use of ARAs and AAAs for cancer treatment, dental evaluation prior to the initiation of AAA or ARA therapies to address and mitigate modifiable risk factors associated with MRONJ development is considered routine in many cancer centers [45, 49].
Thorough medical, dental and social histories as well as patient's dental complaints should be elicited as part of the clinical assessment prior to initiating anti-neoplastic therapy.
A comprehensive clinical examination begins with a thorough assessment of the extra-oral structures to evaluate for any sources of pain or infection. Next, the intraoral examination should include a systematic assessment of the oral mucosal tissues for soft tissue pathologies, opportunistic infections or other abnormalities. This should be followed by the assessment of the teeth for caries and quality of existing restorations. Teeth with large restorations or suspicious for pulpal or periapical pathologies should be further evaluated using adjunctive aids (e.g., pulp sensibility tests) to rule out acute and/or chronic infections. If present, oral prosthesis should be checked and adjusted for any areas that could cause mucosal trauma. A periodontal examination to identify the presence of deep or suppurative periodontal pockets, inflamed gingiva, clinical attachment loss and furcal exposure should be performed [4, 45, 52–58].
For radiographic examination, acquiring a dental panoramic pantogram (DPT) provides an overview of the general oral health status and is useful for identifying pathology (e.g., impacted teeth, cysts) [59, 60]. A baseline DPT should be taken if one is not available within the year, or if there is a clinical suspicion of an intra-bony pathology. Bitewing radiographs should be taken to assess for caries and to check the quality of existing restorations (i.e., recurrent caries) [59, 60]. For patients with bitewings that were done within a year, a new set of bitewing radiographs may not be needed if the suspicion for new caries is low. Periapical radiographs should be captured for both asymptomatic and symptomatic teeth with large cavities and restorations to rule out pulpal or periapical pathologies as well as to assess the periodontal health [59, 60].
Treatment planning is directed by the nature and urgency of the dental problem, the time available to complete the treatment, the patient's medical fitness and considerations unique to the type of anti-neoplastic therapy [2].
The dental practitioner should consider the potential for a dental finding to develop into an infection or become a problem in the future, and the consequences of treatment versus no treatment. The considerations differ based on the type of anti-neoplastic therapy planned which has been discussed in the earlier section.
Another consideration is to prioritize and sequence dental procedures to ensure sufficient time for healing. For example, dental extractions should be performed earlier to allow time for wound mucosalization. Typically, the minimum healing durations prior to initiation of chemotherapy and HNRT/ARA/AAA therapies are ~7–10 days and 10–14 days, respectively [45, 56, 61, 62].
For cancer patients who are immunosuppressed from their underlying illness or as a consequence of their anti-neoplastic therapy, a baseline complete blood count may be necessary to assess the need for antibiotic prophylaxis or blood transfusions prior to invasive dental procedures [63]. Although recommendations may vary across different centers, the common thresholds to determine the need for antibiotic prophylaxis and platelet transfusions are absolute neutrophil count 1 × 109/L (<1000/mm3) and platelet count of 60 × 109/L (<60,000/mm3), respectively [35, 64]. Another consideration for necessitating antibiotic prophylaxis is the presence of a central indwelling catheter because of the potential for a distant site infection after an invasive dental procedure. However, evidence supporting this practice is limited [65].
For patients undergoing high dose HNRT, the advent of Intensity Modulated Radiation Therapy (IMRT) has allowed for continued high dose delivery to the tumor bed while reducing the radiation to the adjacent tissues [66–68]. This has resulted in some reduction of the oral toxicities induced by HNRT [28, 69]. Polce et al. had further explored using the IMRT radiation plans to estimate the radiation dose to each tooth or selected area of interest so that decision making during treatment planning can be more precise [66]. Other local measures include fabrication of intra-oral stents to be worn during HNRT treatment sessions to decrease radiation scatter in patients with heavily restored dentition, to displace the tongue or to position the oral structures away from the epicenter where the radiation dose is at the highest [70, 71]. While potentially effective in reducing the oral side effects of HNRT, intra-oral stents are not widely used due to the lack of standardized protocols and limited high-quality evidence [71, 72]. Patients also often find the intra-oral stents bulky and uncomfortable, especially for those experiencing oral pain and trismus [72].
Lastly, while it is ideal to eliminate all dental disease, the clinician must consider the intent of the anti-neoplastic therapy during the treatment planning process. The benefit of total dental disease eradication in patients undergoing palliative treatment should be balanced against the discomfort and post-operative sequelae of extensive dental procedures.
Conventionally, the objective of dental clearance has been to eliminate all dental pathology prior to anti-neoplastic therapy. However, the complete clearance approach may carry some risk of complications arising from the dental treatment itself [2, 73–75]. Tai et al. reported that 40% of patients who had third molar extractions prior to their anti-neoplastic therapy developed post-operative complications (e.g., alveolar osteitis) [76]. Another consideration is when there is inadequate time to complete all planned treatment, and for treatment to be completed and adequate healing to occur, anti-neoplastic therapy would have to be delayed. This is not ideal because of the well-documented association between delay in anti-neoplastic therapy initiation and poorer survival rates [77].
In recent years, the concept of partial or minimal dental clearance protocols have emerged in the literature [2]. A partial clearance protocol allows for a less aggressive dental clearance and does not require for all dental pathologies to be eliminated prior to the anti-neoplastic therapy. A minimal protocol involves the treatment of only symptomatic oral disease. In a systematic review evaluating the adequacy of the partial and minimal dental clearance protocols prior to chemotherapy and HSCT, the authors recommended that a partial dental clearance protocol may be appropriate when there is insufficient time for complete dental clearance [2]. However, whenever possible, complete treatment clearance protocol is preferred [2]. Table 1 provides an overview of the typical procedures performed in complete and partial clearance protocol [52, 58, 73, 78–85].
Dental evaluation and treatment should be ideally performed prior to the initiation of anti-neoplastic therapy. If extractions are required after HNRT, some authors have suggested that atraumatic extractions are best performed within 6 months after HNRT to mitigate the risks of ORNJ [86–88]. This recommendation is based on a landmark histology study by Marx et al. whereby serial biopsies from 64 patients at varying times (unspecified) during and after receiving 72 Gy of HNRT demonstrated hyperemia and endarteritis in the first 6 months post-HNRT [74]. After which, the tissues demonstrated hypovascularity and fibrosis that progressively worsened with time [74]. In a recent systematic review evaluating the incidence of ORNJ in patients who had dental extractions before or after HNRT, authors found no difference in ORNJ incidence between the 2 groups [89]. However, authors cautioned that these results were based on vastly heterogeneous studies that lacked detail regarding the timing of dental procedures in relation to HNRT and recommended the need for larger longitudinal studies [89].
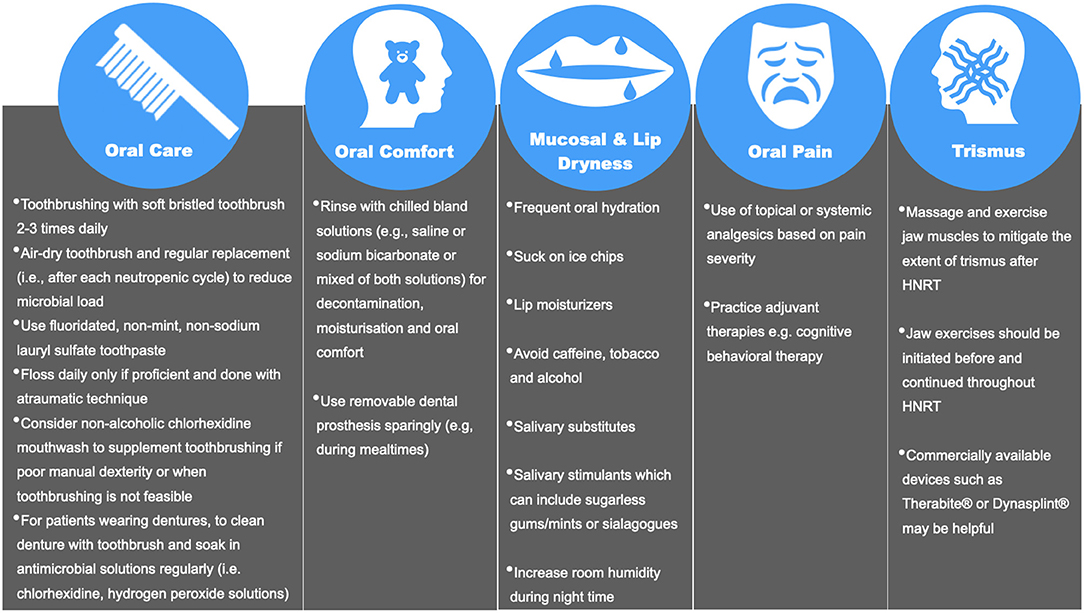
Patient education is an essential element of the dental clearance protocol. The dental professional should communicate with the patient about the rationale for dental evaluation, the potential acute and chronic oral complications and the recommended oral care during anti-neoplastic therapy (Figure 1) [54, 63, 90–101]. The recommendations should be customized to the patient's needs, which is dependent on the type of anti-neoplastic therapy as well as their underlying medical and dental conditions.
The objectives of oral care during and immediately after anti-neoplastic therapy are to prevent infections, control pain, maintain function and manage acute and chronic oral complications [4].
During active anti-neoplastic therapy, elective dental treatment should be avoided. In the event of an acute dental infection, pharmacological intervention with antibiotic therapy and analgesics are the preferred management modality [83]. If an emergency dental procedure is required (e.g., severe odontogenic abscess with potential airway embarrassment), the dental practitioner should plan for dental treatment in liaison with the patient's oncologist or medical physician. Specific pre-procedure considerations include the need for antibiotic prophylaxis, replacement of blood products and in some situations, disruption of anti-neoplastic therapy.
After active anti-neoplastic therapy or in patients with a history of cancer, 3–6 monthly routine reviews are recommended, and the interval is based on patient's dental needs. Other than addressing patient's complaints and performing a comprehensive clinical examination at these reviews, the dental professional should carefully evaluate the oral cavity for signs or symptoms of chronic oral manifestations from anti-neoplastic therapies as well as recurrence and occurrence of secondary malignancies. At the review, the importance of maintaining a good oral hygiene homecare program should also be reiterated.
Dental clearance prior to anti-neoplastic therapy is routine in many cancer centers. To be able to deliver the best care for the patient, it is essential for the dental practitioner to be aware of the rationale and objectives for dental evaluation as well as the specific considerations unique to the various anti-neoplastic treatment modalities.
CWY contributed to majority of the writing. AR contributed to the framework of the manuscript, provided expertise in the area, and checked the manuscript for accuracy. CH developed the framework for the manuscript and contributed to the writing. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. National National Institutes of Health consensus development conference statement: oral complications of cancer therapies: diagnosis prevention and treatment. J Am Dent Assoc. (1989) 119:179–83. doi: 10.14219/jada.archive.1989.0130
2. Hong CHL, Hu S, Haverman T, Stokman M, Napeñas JJ, Braber JB, et al. A systematic review of dental disease management in cancer patients. Support Care Cancer. (2018) 26:155–74. doi: 10.1007/s00520-017-3829-y
3. Schuurhuis JM, Stokman MA, Witjes MJ, Dijkstra PU, Vissink A, Spijkervet FK. Evidence supporting pre-radiation elimination of oral foci of infection in head and neck cancer patients to prevent oral sequelae. A systematic review. Oral Oncol. (2015) 51:212–20. doi: 10.1016/j.oraloncology.2014.11.017
4. Elad S, Raber-Durlacher JE, Brennan MT, Saunders DP, Mank AP, Zadik Y, et al. Basic oral care for hematology-oncology patients and hematopoietic stem cell transplantation recipients: a position paper from the joint task force of the Multinational Association of Supportive Care in Cancer/International Society of Oral Oncology (MASCC/ISOO) and the European Society for Blood and Marrow Transplantation (EBMT). Support Care Cancer. (2015) 23:223–36. doi: 10.1007/s00520-014-2378-x
5. Stringer AM, Logan RM. The role of oral flora in the development of chemotherapy-induced oral mucositis. J Oral Pathol Med. (2015) 44:81–7. doi: 10.1111/jop.12152
6. Falzone L, Salomone S, Libra M. Evolution of cancer pharmacological treatments at the turn of the third millennium. Front Pharmacol. (2018) 9:1300. doi: 10.3389/fphar.2018.01300
7. Rasmussen L, Arvin A. Chemotherapy-induced immunosuppression. Environ Health Perspect. (1982) 43:21–5. doi: 10.1289/ehp.824321
8. Lalla RV, Latortue MC, Hong CH, Ariyawardana A, D'Amato-Palumbo S, Fischer DJ, et al. A systematic review of oral fungal infections in patients receiving cancer therapy. Support Care Cancer. (2010) 18:985–92. doi: 10.1007/s00520-010-0892-z
9. Elad S, Zadik Y, Hewson I, Hovan A, Correa ME, Logan R, et al. A systematic review of viral infections associated with oral involvement in cancer patients: a spotlight on Herpesviridea. Support Care Cancer. (2010) 18:993–1006. doi: 10.1007/s00520-010-0900-3
10. Overholser CD, Peterson DE, Williams LT, Schimpff SC. Periodontal infection in patients with acute nonlymphocyte leukemia. Prevalence of acute exacerbations. Arch Intern Med. (1982) 142:551–4. doi: 10.1001/archinte.142.3.551
11. Sonis S, Kunz A. Impact of improved dental services on the frequency of oral complications of cancer therapy for patients with non-head-and-neck malignancies. Oral Surg Oral Med Oral Pathol. (1988) 65:19–22. doi: 10.1016/0030-4220(88)90184-3
12. Arsati F, Montalli VA, Florio FM, Ramacciato JC, da Cunha FL, Cecanho R, et al. Brazilian dentists' attitudes about medical emergencies during dental treatment. J Dent Educ. (2010) 74:661–6. doi: 10.1002/j.0022-0337.2010.74.6.tb04912.x
13. Epstein JB. Mucositis in the cancer patient and immunosuppressed host. Infect Dis Clin North Am. (2007) 21:503–22, vii. doi: 10.1016/j.idc.2007.03.003
14. Ruescher TJ, Sodeifi A, Scrivani SJ, Kaban LB, Sonis ST. The impact of mucositis on alpha-hemolytic streptococcal infection in patients undergoing autologous bone marrow transplantation for hematologic malignancies. Cancer. (1998) 82:2275–81. doi: 10.1002/(SICI)1097-0142(19980601)82:11<2275::AID-CNCR25>3.0.CO;2-Q
15. Vidal AM, Sarria JC, Kimbrough RC 3rd, Keung YK. Anaerobic bacteremia in a neutropenic patient with oral mucositis. Am J Med Sci. (2000) 319:189–90. doi: 10.1016/S0002-9629(15)40718-9
16. Wardill HR, Sonis ST, Blijlevens NMA, Van Sebille YZA, Ciorba MA, Loeffen EAH, et al. Prediction of mucositis risk secondary to cancer therapy: a systematic review of current evidence and call to action. Support Care Cancer. (2020) 28:5059–73. doi: 10.1007/s00520-020-05579-7
17. de Farias Gabriel A, Silveira FM, Curra M, Schuch LF, Wagner VP, Martins MAT, et al. Risk factors associated with the development of oral mucositis in pediatric oncology patients: systematic review and meta-analysis. Oral Dis. (2021). doi: 10.1111/odi.13863 [Epub ahead of print].
18. Rossi A, Cortelazzo S, Bellavita P, Viero P, Bassan R, Comotti B, et al. Long-term haematological reconstitution following BEAM and autologous transplantation of circulating progenitor cells in non-Hodgkin's lymphoma. Br J Haematol. (1997) 96:620–6. doi: 10.1046/j.1365-2141.1997.d01-2060.x
19. Olivieri A, Offidani M, Montanari M, Ciniero L, Cantori I, Ombrosi L, et al. Factors affecting hemopoietic recovery after high-dose therapy and autologous peripheral blood progenitor cell transplantation: a single center experience. Haematologica. (1998) 83:329–37.
20. Domenech J, Linassier C, Gihana E, Dayan A, Truglio D, Bout M, et al. Prolonged impairment of hematopoiesis after high-dose therapy followed by autologous bone marrow transplantation. Blood. (1995) 85:3320–7. doi: 10.1182/blood.V85.11.3320.bloodjournal85113320
21. Park H, Byun JM, Koh Y, Yoon SS, Park H, Lee J, et al. Comparison of different conditioning regimens in allogeneic hematopoietic stem-cell transplantation shows superiority of total body irradiation-based regimen for younger patients with acute leukemia: a nationwide study. Clin Lymphoma Myeloma Leuk. (2019) 19:e605–e15. doi: 10.1016/j.clml.2019.08.005
22. Bergmann OJ. Oral infections and fever in immunocompromised patients with haematologic malignancies. Eur J Clin Microbiol Infect Dis. (1989) 8:207–13. doi: 10.1007/BF01965262
23. Greenberg MS, Cohen SG, McKitrick JC, Cassileth PA. The oral flor as a source of septicemia in patients with acute leukemia. Oral Surg Oral Med Oral Pathol. (1982) 53:32–6. doi: 10.1016/0030-4220(82)90483-2
24. Chen JA, Wang CC, Wong YK, Wang CP, Jiang RS, Lin JC, et al. Osteoradionecrosis of mandible bone in patients with oral cancer–associated factors and treatment outcomes. Head Neck. (2016) 38:762–8. doi: 10.1002/hed.23949
25. Gomez DR, Estilo CL, Wolden SL, Zelefsky MJ, Kraus DH, Wong RJ, et al. Correlation of osteoradionecrosis and dental events with dosimetric parameters in intensity-modulated radiation therapy for head-and-neck cancer. Int J Radiat Oncol Biol Phys. (2011) 81:e207–13. doi: 10.1016/j.ijrobp.2011.02.003
26. Owosho AA, Tsai CJ, Lee RS, Freymiller H, Kadempour A, Varthis S, et al. The prevalence and risk factors associated with osteoradionecrosis of the jaw in oral and oropharyngeal cancer patients treated with intensity-modulated radiation therapy (IMRT): The Memorial Sloan Kettering Cancer Center experience. Oral Oncol. (2017) 64:44–51. doi: 10.1016/j.oraloncology.2016.11.015
27. Tsai CJ, Hofstede TM, Sturgis EM, Garden AS, Lindberg ME, Wei Q, et al. Osteoradionecrosis and radiation dose to the mandible in patients with oropharyngeal cancer. Int J Radiat Oncol Biol Phys. (2013) 85:415–20. doi: 10.1016/j.ijrobp.2012.05.032
28. Caparrotti F, Huang SH, Lu L, Bratman SV, Ringash J, Bayley A, et al. Osteoradionecrosis of the mandible in patients with oropharyngeal carcinoma treated with intensity-modulated radiotherapy. Cancer. (2017) 123:3691–700. doi: 10.1002/cncr.30803
29. Kubota H, Miyawaki D, Mukumoto N, Ishihara T, Matsumura M, Hasegawa T, et al. Risk factors for osteoradionecrosis of the jaw in patients with head and neck squamous cell carcinoma. Radiat Oncol. (2021) 16:1. doi: 10.1186/s13014-020-01701-5
30. Moon DH, Moon SH, Wang K, Weissler MC, Hackman TG, Zanation AM, et al. Incidence of, and risk factors for, mandibular osteoradionecrosis in patients with oral cavity and oropharynx cancers. Oral Oncol. (2017) 72:98–103. doi: 10.1016/j.oraloncology.2017.07.014
31. Nabil S, Samman N. Incidence and prevention of osteoradionecrosis after dental extraction in irradiated patients: a systematic review. Int J Oral Maxillofac Surg. (2011) 40:229–43. doi: 10.1016/j.ijom.2010.10.005
32. Katsura K, Sasai K, Sato K, Saito M, Hoshina H, Hayashi T. Relationship between oral health status and development of osteoradionecrosis of the mandible: a retrospective longitudinal study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. (2008) 105:731–8. doi: 10.1016/j.tripleo.2007.10.011
33. Wong JK, Wood RE, McLean M. Conservative management of osteoradionecrosis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. (1997) 84:16–21. doi: 10.1016/S1079-2104(97)90287-0
34. Peterson DE, Doerr W, Hovan A, Pinto A, Saunders D, Elting LS, et al. Osteoradionecrosis in cancer patients: the evidence base for treatment-dependent frequency, current management strategies, and future studies. Support Care Cancer. (2010) 18:1089–98. doi: 10.1007/s00520-010-0898-6
35. PDQ® Supportive Palliative Care Editorial Board. PDQ Oral Complications of Chemotherapy and Head/Neck Radiation. Bethesda, MD: National Cancer Institute (2021). Available online at: https://www.cancer.gov/about-cancer/treatment/side-effects/mouth-throat/oral-complications-hp-pdq (accessed November 13, 2021).
36. Treister NS, Brennan MT, Sollecito TP, Schmidt BL, Patton LL, Mitchell R, et al. Exposed bone in patients with head and neck cancer treated with radiation therapy: an analysis of the observational study of dental outcomes in head and neck cancer patients (OraRad). Cancer. (2022) 128:487–96. doi: 10.1002/cncr.33948
37. Kolokythas A, Rasmussen JT, Reardon J, Feng C. Management of osteoradionecrosis of the jaws with pentoxifylline-tocopherol: a systematic review of the literature and meta-analysis. Int J Oral Maxillofac Surg. (2019) 48:173–80. doi: 10.1016/j.ijom.2018.08.007
38. Rice N, Polyzois I, Ekanayake K, Omer O, Stassen LF. The management of osteoradionecrosis of the jaws–a review. Surgeon. (2015) 13:101–9. doi: 10.1016/j.surge.2014.07.003
39. El-Rabbany M, Duchnay M, Raziee HR, Zych M, Tenenbaum H, Shah PS, et al. Interventions for preventing osteoradionecrosis of the jaws in adults receiving head and neck radiotherapy. Cochrane Database Syst Rev. (2019) 2019. doi: 10.1002/14651858.CD011559.pub2
40. Rao SD, Saleh ZH, Setton J, Tam M, McBride SM, Riaz N, et al. Dose-volume factors correlating with trismus following chemoradiation for head and neck cancer. Acta Oncol. (2016) 55:99–104. doi: 10.3109/0284186X.2015.1037864
41. Marks JE, Davis CC, Gottsman VL, Purdy JE, Lee F. The effects of radiation of parotid salivary function. Int J Radiat Oncol Biol Phys. (1981) 7:1013–9. doi: 10.1016/0360-3016(81)90152-8
42. Gupta N, Pal M, Rawat S, Grewal MS, Garg H, Chauhan D, et al. Radiation-induced dental caries, prevention and treatment - a systematic review. Natl J Maxillofac Surg. (2015) 6:160–6. doi: 10.4103/0975-5950.183870
43. Brennan MT, Treister NS, Sollecito TP, Schmidt BL, Patton LL, Lin A, et al. Tooth failure post-radiotherapy in head and neck cancer: primary report of the clinical registry of dental outcomes in head and neck cancer patients (OraRad) study. Int J Radiat Oncol Biol Phys. (2021) S0360-3016(21)03219-3. doi: 10.1016/j.ijrobp.2021.11.021
44. Marx RE. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic. J Oral Maxillofac Surg. (2003) 61:1115–7. doi: 10.1016/S0278-2391(03)00720-1
45. Ruggiero SL, Dodson TB, Aghaloo T, Carlson ER, Ward BB, Kademani D. American association of oral and maxillofacial surgeons' position paper on medication-related osteonecrosis of the jaw – 2022 update. J Oral Maxillofac Surg. (2022) S0278-2391(22)00148-3. doi: 10.1016/j.joms.2022.02.008
46. Yarom N, Shapiro CL, Peterson DE, Van Poznak CH, Bohlke K, Ruggiero SL, et al. Medication-related osteonecrosis of the jaw: MASCC/ISOO/ASCO clinical practice guideline. J Clin Oncol. (2019) 37:2270–90. doi: 10.1200/JCO.19.01186
47. Tsao C, Darby I, Ebeling PR, Walsh K, O'Brien-Simpson N, Reynolds E, et al. Oral health risk factors for bisphosphonate-associated jaw osteonecrosis. J Oral Maxillofac Surg. (2013) 71:1360–6. doi: 10.1016/j.joms.2013.02.016
48. Vahtsevanos K, Kyrgidis A, Verrou E, Katodritou E, Triaridis S, Andreadis CG, et al. Longitudinal cohort study of risk factors in cancer patients of bisphosphonate-related osteonecrosis of the jaw. J Clin Oncol. (2009) 27:5356–62. doi: 10.1200/JCO.2009.21.9584
49. Khan AA, Morrison A, Hanley DA, Felsenberg D, McCauley LK, O'Ryan F, et al. Diagnosis and management of osteonecrosis of the jaw: a systematic review and international consensus. J Bone Miner Res. (2015) 30:3–23. doi: 10.1002/jbmr.2405
50. Beth-Tasdogan NH, Mayer B, Hussein H, Zolk O. Interventions for managing medication-related osteonecrosis of the jaw. Cochrane Database Syst Rev. (2017) 10:Cd012432. doi: 10.1002/14651858.CD012432.pub2
51. Yoneda T, Hagino H, Sugimoto T, Ohta H, Takahashi S, Soen S, et al. Bisphosphonate-related osteonecrosis of the jaw: position paper from the Allied Task Force Committee of Japanese Society for Bone and Mineral Research, Japan Osteoporosis Society, Japanese Society of Periodontology, Japanese Society for Oral and Maxillofacial Radiology, and Japanese Society of Oral and Maxillofacial Surgeons. J Bone Miner Metab. (2010) 28:365–83. doi: 10.1007/s00774-010-0162-7
52. Tomblyn M, Chiller T, Einsele H, Gress R, Sepkowitz K, Storek J, et al. Guidelines for preventing infectious complications among hematopoietic cell transplantation recipients: a global perspective. Biol Blood Marrow Transplant. (2009) 15:1143–238. doi: 10.1016/j.bbmt.2009.06.019
53. Guideline Guideline on dental management of pediatric patients receiving chemotherapy hematopoietic cell transplantation and/or radiation. Pediatr Dent. (2013) 35:E185–93.
54. PDQ® Supportive Palliative Care Editorial Board. PDQ Oral Complications of Chemotherapy and Head/Neck Radiation. Bethesda, MD: National Cancer Institute (2021). Available online at: https://www.cancer.gov/about-cancer/treatment/side-effects/mouth-throat/oral-complications-hp-pdq (accessed January 24, 2022).
55. Levi LE, Lalla RV. Dental treatment planning for the patient with oral cancer. Dent Clin North Am. (2018) 62:121–30. doi: 10.1016/j.cden.2017.08.009
56. Butterworth C, McCaul L, Barclay C. Restorative dentistry and oral rehabilitation: United Kingdom National Multidisciplinary Guidelines. J Laryngol Otol. (2016) 130:S41–4. doi: 10.1017/S0022215116000414
57. Epstein JB, Güneri P, Barasch A. Appropriate and necessary oral care for people with cancer: guidance to obtain the right oral and dental care at the right time. Support Care Cancer. (2014) 22:1981–8. doi: 10.1007/s00520-014-2228-x
58. Epstein JB, Stevenson-Moore P. Periodontal disease and periodontal management in patients with cancer. Oral Oncol. (2001) 37:613–9. doi: 10.1016/S1368-8375(01)00025-2
59. American Dental Association Council on Scientific Affairs U,.S. Food Drug Administration. Dental Radiographic Examinations: Recommendations for Patient Selection Limiting Radiation Exposure (2012). Available online at: https://www.fda.gov/media/84818/download
60. Prescribing dental radiographs for infants children adolescents and individuals with special health care needs. Pediatr Dent. (2017) 39:205–7.
61. Elad S, Garfunkel AA, Or R, Michaeli E, Shapira MY, Galili D. Time limitations and the challenge of providing infection-preventing dental care to hematopoietic stem-cell transplantation patients. Support Care Cancer. (2003) 11:674–7. doi: 10.1007/s00520-003-0499-8
62. Clayman L. Clinical controversies in oral and maxillofacial surgery: Part two. Management of dental extractions in irradiated jaws: a protocol without hyperbaric oxygen therapy. J Oral Maxillofac Surg. (1997) 55:275–81. doi: 10.1016/S0278-2391(97)90542-5
63. Hong CHL, Gueiros LA, Fulton JS, Cheng KKF, Kandwal A, Galiti D, et al. Systematic review of basic oral care for the management of oral mucositis in cancer patients and clinical practice guidelines. Support Care Cancer. (2019) 27:3949–67. doi: 10.1007/s00520-019-04848-4
64. Zimmermann C, Meurer MI, Grando LJ, Gonzaga Del Moral J, da Silva Rath IB, Schaefer Tavares S. Dental treatment in patients with leukemia. J Oncol. (2015) 2015:571739. doi: 10.1155/2015/571739
65. Hong CH, Allred R, Napenas JJ, Brennan MT, Baddour LM, Lockhart PB. Antibiotic prophylaxis for dental procedures to prevent indwelling venous catheter-related infections. Am J Med. (2010) 123:1128–33.
66. Polce S, Gogineni E, Antone J, Ghaly M, Keith Frank D, Segal JD, et al. Dental radiation dosimetric maps from intensity-modulated radiation therapy planning for head and neck cancers. Head Neck. (2021) 43:1428–39. doi: 10.1002/hed.26611
67. Fregnani ER, Parahyba CJ, Morais-Faria K, Fonseca FP, Ramos PAM, de Moraes FY, et al. IMRT delivers lower radiation doses to dental structures than 3DRT in head and neck cancer patients. Radiat Oncol. (2016) 11:116. doi: 10.1186/s13014-016-0694-7
68. Bak SY, Qi XS, Kelly JA, Alexander S, Chung Y, Gyurdzhyan S, et al. Dosimetric distribution to tooth-bearing areas in intensity-modulated radiation therapy for head and neck cancer: a pilot study. Oral Surg Oral Med Oral Pathol Oral Radiol. (2016) 121:43–8. doi: 10.1016/j.oooo.2015.10.007
69. De Sanctis V, Merlotti A, De Felice F, Trignani M, Dell'Oca I, Lastrucci L, et al. Intensity modulated radiation therapy and oral mucosa sparing in head and neck cancer patients: a systematic review on behalf of Italian Association of Radiation Oncology - Head and neck working group. Crit Rev Oncol Hematol. (2019) 139:24–30. doi: 10.1016/j.critrevonc.2019.04.022
70. Verrone JR, Alves FA, Prado JD, Marcicano A, de Assis Pellizzon AC, Damascena AS, et al. Benefits of an intraoral stent in decreasing the irradiation dose to oral healthy tissue: dosimetric and clinical features. Oral Surg Oral Med Oral Pathol Oral Radiol. (2014) 118:573–8. doi: 10.1016/j.oooo.2014.08.008
71. Singh A, Rosen EB, Randazzo JD, Estilo CL, Gelblum DY, Huryn JM. Intraoral radiation stents-Primer for clinical use in head and neck cancer therapy. Head Neck. (2021) 43:4010–7. doi: 10.1002/hed.26848
72. Alves LDB, Menezes ACS, Pereira DL, Santos MTC, Antunes HS. Benefits of intraoral stents in patients with head and neck cancer undergoing radiotherapy: Systematic review. Head Neck. (2021) 43:1652–63. doi: 10.1002/hed.26620
73. Raut A, Huryn JM, Hwang FR, Zlotolow IM. Sequelae and complications related to dental extractions in patients with hematologic malignancies and the impact on medical outcome. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. (2001) 92:49–55. doi: 10.1067/moe.2001.113588
74. Marx RE, Johnson RP. Studies in the radiobiology of osteoradionecrosis and their clinical significance. Oral Surg Oral Med Oral Pathol. (1987) 64:379–90. doi: 10.1016/0030-4220(87)90136-8
75. Lajolo C, Gioco G, Rupe C, Troiano G, Cordaro M, Lucchese A, et al. Tooth extraction before radiotherapy is a risk factor for developing osteoradionecrosis of the jaws: a systematic review. Oral Dis. (2021) 27:1595–605. doi: 10.1111/odi.13485
76. Tai CC, Precious DS, Wood RE. Prophylactic extraction of third molars in cancer patients. Oral Surg Oral Med Oral Pathol. (1994) 78:151–5. doi: 10.1016/0030-4220(94)90138-4
77. Graboyes EM, Kompelli AR, Neskey DM, Brennan E, Nguyen S, Sterba KR, et al. Association of treatment delays with survival for patients with head and neck cancer: a systematic review. JAMA Otolaryngol Head Neck Surg. (2019) 145:166–77. doi: 10.1001/jamaoto.2018.2716
78. Sheller B, Williams B. Orthodontic management of patients with hematologic malignancies. Am J Orthod Dentofacial Orthop. (1996) 109:575–80. doi: 10.1016/S0889-5406(96)70068-9
79. Schiødt M, Hermund NU. Management of oral disease prior to radiation therapy. Support Care Cancer. (2002) 10:40–3. doi: 10.1007/s005200100284
80. Gürgan CA, Özcan M, Karakuş Ö, Zincircioglu G, Arat M, Soydan E, et al. Periodontal status and post-transplantation complications following intensive periodontal treatment in patients underwent allogenic hematopoietic stem cell transplantation conditioned with myeloablative regimen. Int J Dent Hyg. (2013) 11:84–90. doi: 10.1111/j.1601-5037.2012.00550.x
81. Haytac MC, Dogan MC, Antmen B. The results of a preventive dental program for pediatric patients with hematologic malignancies. Oral Health Prev Dent. (2004) 2:59–65.
82. Melkos AB, Massenkeil G, Arnold R, Reichart PA. Dental treatment prior to stem cell transplantation and its influence on the posttransplantation outcome. Clin Oral Investig. (2003) 7:113–5. doi: 10.1007/s00784-003-0209-4
83. Tsuji K, Shibuya Y, Akashi M, Furudoi S, Yakushijin K, Kawamoto S, et al. Prospective study of dental intervention for hematopoietic malignancy. J Dent Res. (2015) 94:289–96. doi: 10.1177/0022034514561768
84. Yamagata K, Onizawa K, Yanagawa T, Takeuchi Y, Hasegawa Y, Chiba S, et al. Prospective study establishing a management plan for impacted third molar in patients undergoing hematopoietic stem cell transplantation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. (2011) 111:146–52. doi: 10.1016/j.tripleo.2010.09.006
85. Yamagata K, Onizawa K, Yanagawa T, Hasegawa Y, Kojima H, Nagasawa T, et al. A prospective study to evaluate a new dental management protocol before hematopoietic stem cell transplantation. Bone Marrow Transplant. (2006) 38:237–42. doi: 10.1038/sj.bmt.1705429
86. Chrcanovic BR, Reher P, Sousa AA, Harris M. Osteoradionecrosis of the jaws–a current overview–Part 2: dental management and therapeutic options for treatment. Oral Maxillofac Surg. (2010) 14:81–95. doi: 10.1007/s10006-010-0205-1
87. Kuo TJ, Leung CM, Chang HS, Wu CN, Chen WL, Chen GJ, et al. Jaw osteoradionecrosis and dental extraction after head and neck radiotherapy: a nationwide population-based retrospective study in Taiwan. Oral Oncol. (2016) 56:71–7. doi: 10.1016/j.oraloncology.2016.03.005
88. Liao PH, Chu CH, Hung YM, Tang PL, Kuo TJ. Tumor subsites and risk of osteoradionecrosis of the jaw in patients with oral cavity cancer: a national-based cohort study. Eur Arch Otorhinolaryngol. (2021) 278:3425–33. doi: 10.1007/s00405-020-06529-z
89. Beaumont S, Bhatia N, McDowell L, Fua T, McCullough M, Celentano A, et al. Timing of dental extractions in patients undergoing radiotherapy and the incidence of osteoradionecrosis: a systematic review and meta-analysis. Br J Oral Maxillofac Surg. (2021) 59:511–23. doi: 10.1016/j.bjoms.2020.10.006
90. Haverman TM, Raber-Durlacher JE, Rademacher WM, Vokurka S, Epstein JB, Huisman C, et al. Oral complications in hematopoietic stem cell recipients: the role of inflammation. Mediators Inflamm. (2014) 2014:378281. doi: 10.1155/2014/378281
91. Jaffe N, Toth BB, Hoar RE, Ried HL, Sullivan MP, McNeese MD. Dental and maxillofacial abnormalities in long-term survivors of childhood cancer: effects of treatment with chemotherapy and radiation to the head and neck. Pediatrics. (1984) 73:816–23. doi: 10.1542/peds.73.6.816
92. Featherstone JD. Prevention and reversal of dental caries: role of low level fluoride. Community Dent Oral Epidemiol. (1999) 27:31–40. doi: 10.1111/j.1600-0528.1999.tb01989.x
93. Qutob AF, Allen G, Gue S, Revesz T, Logan RM, Keefe D. Implementation of a hospital oral care protocol and recording of oral mucositis in children receiving cancer treatment : a retrospective and a prospective study. Support Care Cancer. (2013) 21:1113–20. doi: 10.1007/s00520-012-1633-2
94. Newbrun E. Topical fluorides in caries prevention and management: a North American perspective. J Dent Educ. (2001) 65:1078–83. doi: 10.1002/j.0022-0337.2001.65.10.tb03452.x
95. Rankin KV, Epstein J, Huber MA, Peterson DE, Plemons JM, Redding SS, et al. Oral health in cancer therapy. Tex Dent J. (2009) 126:389-97:406–19,22–37.
96. Santos PS, Tinôco-Araújo JE, Souza LM, Ferreira R, Ikoma MR, Razera AP, et al. Efficacy of HPA Lanolin® in treatment of lip alterations related to chemotherapy. J Appl Oral Sci. (2013) 21:163–6. doi: 10.1590/1678-7757201302308
97. Scherpenhuizen A, van Waes AM, Janssen LM, Van Cann EM, Stegeman I. The effect of exercise therapy in head and neck cancer patients in the treatment of radiotherapy-induced trismus: A systematic review. Oral Oncol. (2015) 51:745–50. doi: 10.1016/j.oraloncology.2015.05.001
98. Epstein JB, Miaskowski C. Oral pain in the cancer patient. J Natl Cancer Inst Monogr. (2019) 2019:lgz003. doi: 10.1093/jncimonographs/lgz003
99. Epstein JB, Hong C, Logan RM, Barasch A, Gordon SM, Oberle-Edwards L, et al. A systematic review of orofacial pain in patients receiving cancer therapy. Support Care Cancer. (2010) 18:1023–31. doi: 10.1007/s00520-010-0897-7
100. Saunders DP, Rouleau T, Cheng K, Yarom N, Kandwal A, Joy J, et al. Systematic review of antimicrobials, mucosal coating agents, anesthetics, and analgesics for the management of oral mucositis in cancer patients and clinical practice guidelines. Support Care Cancer. (2020) 28:2473–84. doi: 10.1007/s00520-019-05181-6
Keywords: radiotherapy, antineoplastic agents, bone density conservation agents, dental care, dental service, hospital
Citation: Yong CW, Robinson A and Hong C (2022) Dental Evaluation Prior to Cancer Therapy. Front. Oral. Health 3:876941. doi: 10.3389/froh.2022.876941
Received: 16 February 2022; Accepted: 14 March 2022;
Published: 18 April 2022.
Edited by:
Nathaniel Simon Treister, Brigham and Women's Hospital and Harvard Medical School, United StatesReviewed by:
Markéta Janovská, Charles University, CzechiaCopyright © 2022 Yong, Robinson and Hong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Catherine Hong, ZGVuY2hobEBudXMuZWR1LnNn
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.