
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oral. Health , 07 May 2021
Sec. Preventive Dentistry
Volume 2 - 2021 | https://doi.org/10.3389/froh.2021.682139
This article is part of the Research Topic Women in Preventive Dentistry: 2021/2022 View all 4 articles
 Sophie Schaper1Sinja Meyer-Rötz1Claudia Bartels1
Sophie Schaper1Sinja Meyer-Rötz1Claudia Bartels1 Jens Wiltfang1,2,3Tina Rödig4
Jens Wiltfang1,2,3Tina Rödig4 Björn H. Schott1,2,5
Björn H. Schott1,2,5 Michael Belz1*
Michael Belz1*For patients with dementia, dental care can pose a considerable challenge due to cognitive impairment, behavioral, and psychological symptoms, and (often subsequently) limited autonomous oral care. In this study, we aimed to assess the proficiency of dentists in general practice in the outpatient dental care of these patients. A total of 119 dentists from private practices in Lower Saxony, Germany, participated in this study. Concerning treatment of patients with dementia, they provided details about (1) practice equipment/consultation, (2) training/expertise, and (3) special circumstances of dental treatment. Participating dentists predominantly reported to use medical aids (e.g., positioning cushions) to improve the treatment situation for patients with dementia. Over two thirds (68.6%) offered consultations in nursing homes, and at the patients' homes (47.0%). The training rate was remarkably low in the field of gerodontology for dentists and their practice staff (<10%), however, 54.5% expressed interest in such training. The majority of dentists reportedly adapted their treatment strategy to the needs of patients with dementia (e.g., communication, inclusion of caregivers, time management). Furthermore, most participants adapted dental treatment adequately (e.g., strict indication for tooth extraction, simple design of dental prostheses). In summary, even though training in the field of gerodontology must be considered insufficient, most dentists in this study showed an adequate adaptation of their treatment strategy as well as consideration of dental characteristics in patients with dementia, along with interest in trainings. We conclude that dementia-specific training should be expanded in the field of dentistry, preferably already at university level.
Dental treatment can pose a considerable challenge in the growing population of older people (≥65 years), as age-related factors like multimorbidity and polypharmacy complicate professional dental treatment [1]. These circumstances are further aggravated in individuals diagnosed with dementia, the risk of which increases steadily with older age—especially from 65 years and above [2, 3]. The resulting cognitive impairment accompanied by psychological and behavioral symptoms usually prompts the need for long-term dental care. However, patients with dementia are often no longer able to adequately care for their personal health and hygiene, including dental health. Several studies have confirmed a close and possibly reciprocal relationship between dental health and cognitive functioning in older adults [4–6]. Patients with dementia commonly fail to attend necessary dental appointments and subsequently suffer from a pronounced decline in oral health, including the loss of teeth [7, 8]. In addition, poor oral health in patients with dementia is potentially aggravated by pharmacological treatment with neuroleptics or antidepressants, which commonly have adverse side effects like xerostomia or orofacial dyskinesia resulting in bruxism, which in turn increase the need for adequate dental treatment [9].
In addition to lack of dental self-care, patients with dementia also experience increased difficulties with respect to dental interventions. On the one hand, access to dentists may be limited, as most work in private practices, which may be difficult to access for severely cognitively impaired individuals [7]. Often, the need for dental intervention is not even detected in patients with dementia. For example, when the affected individuals are unable to express themselves adequately and develop agitation symptoms or aggressive behavior due to intraoral pain, the behavioral problems are frequently treated with psychotropic drugs, but the correct detection and/or elimination of the pain's cause often remains absent [10]. On the other hand, dental procedures themselves can prove challenging in older people with dementia. Dementia is often accompanied by pronounced affective and behavioral disturbances, including depressed mood and aggressive behavior, both of which can complicate medical, including dental, treatment [11]. In more advanced stages of dementia, patients may no longer be cognitively capable of understanding the need for medical or dental visits. In such cases, a relative, health care proxy or legal guardian must be involved, which increases the effort required for treatment and requires the scheduling of longer session times [12]. Adapting communication to the needs of individuals with reduced cognitive ability (e.g., by speaking in simple, short sentences, keeping eye contact, or communicating via third parties), as well as involving familiar caregivers, can prove challenging in everyday dental practice. At the organizational level, practitioners also face an increased burden, requiring, for example, adequate recall structures to avoid missed appointments and to better monitor oral health. Finally, yet importantly, dental treatment itself may also need to be adapted, owing to both impaired understanding of the required procedures and possible difficulties with day-to-day handling of dentures. One example would be the early switch to a robust, easy-to-care-for and easy-to-handle denture [13] in order to preserve the functional ability of the masticatory organ as long as possible.
While the problem of dental care in patients with dementia is nowadays widely recognized, less is known about the preparedness among practitioners to adapt their treatments to older people with dementia, and about both, existing approaches and unmet needs in dementia-sensitive dentistry. In the present study, we aimed to assess the status of dental care for patients with dementia by dentists in private practice in southern Lower Saxony, Germany. The region investigated covered a predominantly rural area surrounding the city of Göttingen, encompassing the counties of Göttingen, Goslar, Holzminden, and Northeim (Figure 1). The survey reported here is specifically directed at dental care for patients with dementia.
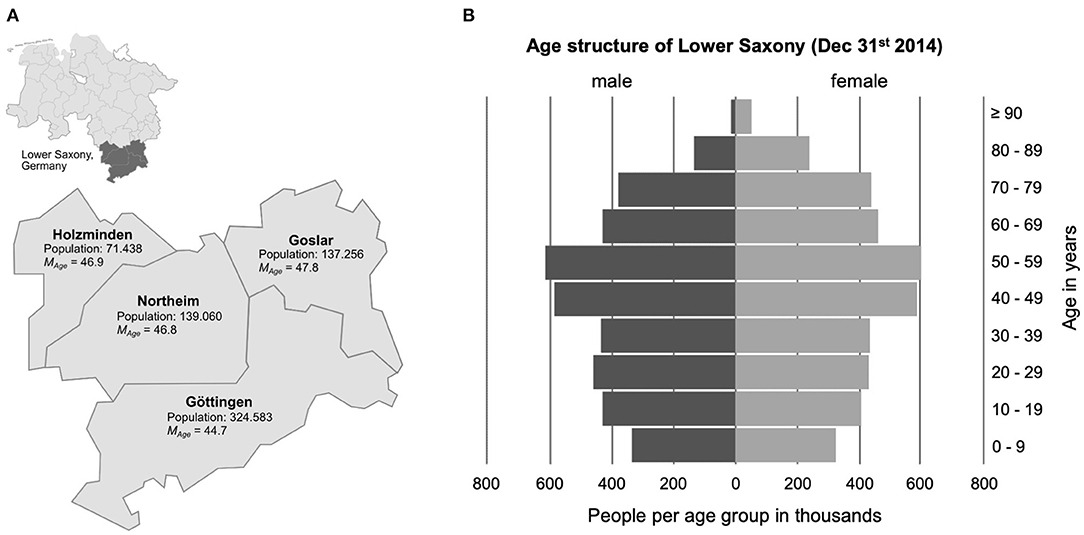
Figure 1. (A) Display of the region in Lower Saxony, Germany, investigated in this study. The data on the number of inhabitants and mean age of each county are predictions for the year 2014, based on the German population survey “Zensus” from 2011. (B) Age structure of the State of Lower Saxony in 2014, as provided by the Landesamt für Statistik Niedersachsen (2016). The source materials for generating the map and the age pyramid were obtained from publicly available materials on https://www.niedersachsen.de.
We carried out a mail-based survey, and obtained questionnaire data from 119 dentists in private practice, which were empirically analyzed to address the following three research questions:
(1) Are there practice equipment and consultation procedures adequately adapted to treat patients with dementia?
(2) Are dentists trained in dementia-specific aspects of gerodontology, and can they rely on existing expertise?
(3) What are the special circumstances of dental treatment of patients with dementia, and how are they addressed in practice?
With a response rate of almost 30%, we received a sufficiently large number of completed questionnaires to obtain representative information on dentists' experience and proficiency in providing dental care to older individuals affected by dementia.
A questionnaire was developed for the present study (see section Measurement for details). A total of 406 dentists in private practice enlisted with the Lower Saxony Chamber of Dentists (Zahnärztekammer Niedersachsen, ZKN) were identified in the counties of Göttingen, Holzminden, Goslar, and Northeim, as defined by zip code, and the survey was provided to all dentists by mail in this cross-sectional study. The response rate during the survey period from February 1st 2017 to March 15th 2017 was 29.3% (N = 119). Approximately two thirds of the responding participants were male (68.9%, n = 82), and the mean age of respondents was M = 52.95 years (SD = 10.55). The state exam was taken between 1990 and 1991 (M = 1,990.75, SD = 10.42 years), and the mean interval between exam and interview time was 26.25 years (SD = 10.42). Female dentists had taken the state exam on average in the year 1996.46 (SD = 8.85) compared to male dentists [year: 1,988.14, SD = 10.07, t(116) = 4.32, p < 0.001]. They were significantly younger (M = 46.89, SD = 9.18) compared to their male colleagues [M = 55.71, SD = 10.01, t(113) = 4.49, p < 0.001]. The majority of dentists surveyed worked in solo practices (58.8%, n = 70), and the remaining respondents worked in group practices (41.2%, n = 49). On average, participants reported treating ~10 individuals with dementia (M = 9.51, SD = 13.96) per quarter in their practice1. All data processing was performed in accordance with European, national, and state regulations on data protection, and the local ethics committee of the University Medical Center Göttingen approved the study.
In addition to the collection of basic demographic data, we administered a self-developed questionnaire. It contained a total of 24 items formulated as statements with the dichotomous response options “Yes” and “No' (e.g., “Is your practice barrier-free?”), grouped according to the three research questions. The participating dentists were informed in an accompanying letter that participation in the survey was voluntary and without financial compensation. The survey was part of an empirical study focused specifically on the dental care of patients with dementia. The questionnaires were returned using a stamped envelope provided along with the questionnaire, and data collection was performed in a fully anonymized way. It has therefore at no time been possible to identify any of the participating dentists or their patients. Table 1 shows the allocation of the individual items to each research question: (1) practice equipment and consultation (items 1a to 1h), (2) training and expertise (items 2a to 2i), (3) dementia-related special circumstances of dental treatment (items 3a to 3i). Two open questions were included [item 1e, question (1): use of aids; item 2i, question (2): special features of consultation; see Table 1 for details]. Assigned to research question (3), a total of nine ratings on the most frequent intraoral diseases were additionally asked using a 5-point Likert scale (item 3j): “Do you notice intraoral abnormalities and diseases more frequently in patients with dementia?” (e.g., “caries”; response: 1 = “does not apply,” to 5 = “fully applies”).
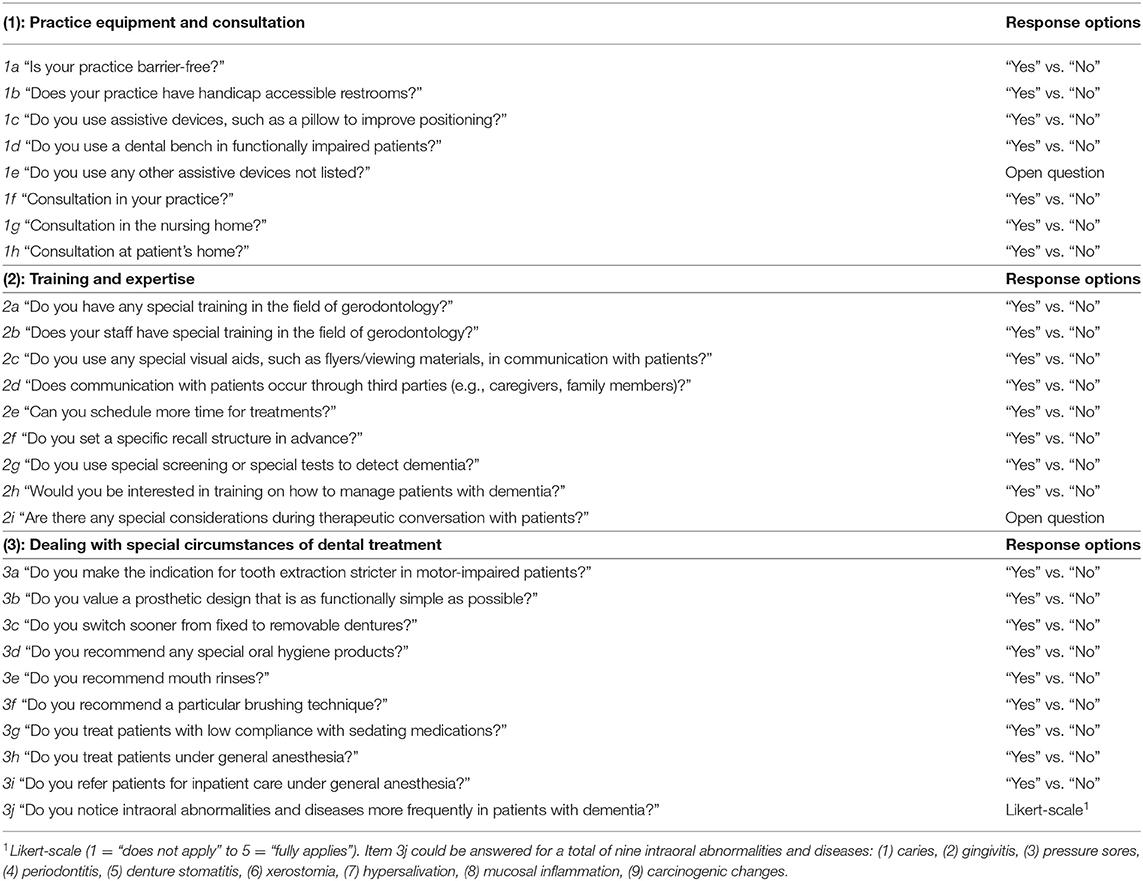
Table 1. Questionnaire-items about patients with dementia.
Statistical analysis was performed using SPSS version 26 (IBM Corp. Armonk, NY). For descriptive presentation of the questionnaire data, frequencies and percentages were calculated for dichotomous items. Only valid percentages are reported in figures and text, excluding missing values. For dichotomous items, exploratory inferential statistics were performed using multiple chi-square tests (χ2). Furthermore, ratings on intraoral disease in patients with dementia are presented as means and standard deviations (M ± SD), along with the respective 95% confidence intervals (CIs). Differences between these nine intra-individual ratings were tested using a general linear model for multiple measures (GLM). All p-values were adjusted for the number of statistical tests within the GLM using the Bonferroni method (initial significance level was set at p < 0.05, two-tailed). Responses to open-ended questions were categorized and then analyzed descriptively (i.e., frequencies).
The valid percentages for the dichotomous items are summarized in Figure 2A. While the majority of respondents affirmed the presence of barrier-free access to their practice (63.0%, n = 75), handicap accessible restrooms were available in only 31.9% of cases (n = 38). The use of assistive devices for positioning (e.g., pillows) was affirmed by a sizable majority (83.9%, n = 99), while only 39.1% (n = 45) of respondents reported using dental benches for cognitively impaired patients. In response to the open-ended question about other assistive devices (item 1e), n = 4 participants responded (“bite wedges,” “patience,” “holding and supporting by staff,” “metal finger guards”). Toilets accessible to the disabled were significantly more common in group practices than in individual practices [ = 4.57, p = 0.045].
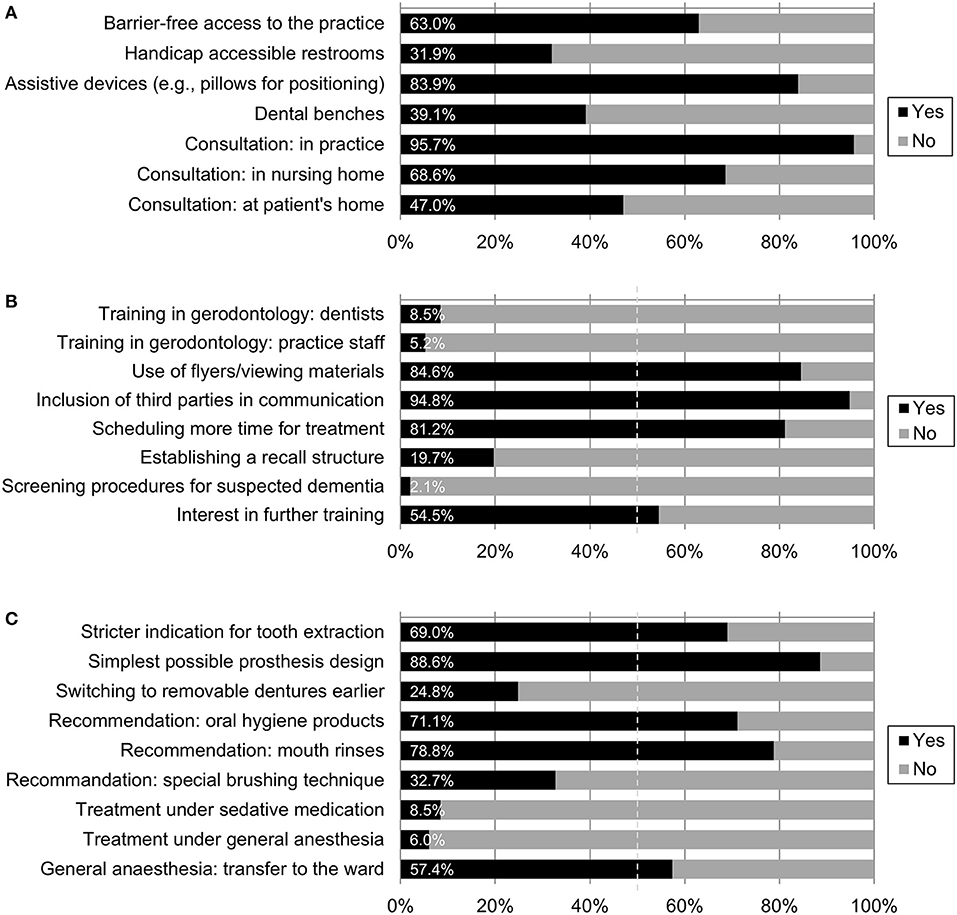
Figure 2. (A) Practice equipment and consultation. Valid percentages for seven dichotomous items (see Table 1 for formulations), n = 100–119. (B) Training and expertise. Valid percentages for eight dichotomous items (see Table 1 for formulations), n = 94 to 117. (C) Dealing with special circumstances of dental treatment. Valid percentages for nine dichotomous items (see Table 1 for formulations), n = 104–117.
Almost all respondents reported consulting patients with dementia in their practice (95.7%, n = 110), followed by consultation in nursing homes (68.6%, n = 72). Slightly less than half of the dentists reported also seeing patients with dementia at home (47.0%, n = 47). No further differences were found between the two types of practice.
Figure 2B displays responses to questions assessing training and expertise. Only a small minority of the participating dentists (8.5%; n = 10) stated that they had received further training in the field of gerodontology, and among the practice staff, this number was even lower (5.2%; n = 6). Despite the lack of specific training, the majority of respondents affirmed the use of flyers/viewing materials in communication with patients with dementia (84.6%, n = 99), the inclusion of third parties such as relatives in therapeutic conversation (94.8%, n = 110), and scheduling more time for treatment (81.2%, n = 95). A recall structure in advance of treatment was established by 19.7% of the participating dentists (n = 23). Only two respondents (2.1%) used screening procedures for suspected dementia. More than half of the respondents expressed interest in further training in dealing with patients with dementia (54.5%, n = 61). Analyses did not reveal significant differences between the types of practice (single practice vs. group practice) for any of these items.
A total of n = 26 participants answered the free-text question on special considerations during therapeutic conversation with patients with dementia (item 2i), but in some cases repeated information from the previous items in their own words. Beyond this, the majority of comments referred to the way of speaking with patients (n = 11: language/word choice “clear, calm, friendly, loud, slow”). Single participants reported paying attention to keeping the course of treatment as consistent as possible to avoid confusing patients (n = 3). A total of n = 7 participants made reference to conducting the conversation via third parties, describing ideally only “involving” accompanying persons, and conducting the conversation with the patients themselves as far as possible.
See Figure 2C for a listing of the valid percentages for the dichotomous items. The majority of participating dentists gave a stricter indication for tooth extraction in patients with dementia and concomitant motor impairment (69.0%, n = 80) and paid attention to using the simplest possible denture design (88.6%, n = 101). At the same time, only a minority of practitioners switched to removable dentures earlier in the course of treatment (24.8%, n = 28). The majority of participating dentists recommended specific oral hygiene products (71.1%, n = 81) as well as mouth rinses (78.8%, n = 82), and 32.7% (n = 37) also recommended a special brushing technique. While practitioners in group practices were significantly more likely to recommend special brushing techniques [ = 5.21, p = 0.027], practitioners in individual practices were significantly more likely to pay attention to simple prosthesis design [ = 4.43 p = 0.042]. No further differences between the two types of practices were found.
Treatment of patients with low compliance under sedative medication was performed by a small number of respondents (8.5%, n = 10), as was treatment under general anesthesia (6.0%, n = 7). A majority reported to refer patients with dementia to inpatient dental treatment, if general anesthesia was needed (57.4%, n = 62).
Overall, participants estimated the queried intraoral diseases in patients with dementia as being differently frequent [GLM: F(8, 776) = 103.40, p < 0.001, partial η2 = 0.69, see Figure 3 for all assessments]. They reported the lowest frequency for carcinogenic changes (M = 2.04, SD = 0.84) and hypersalivation (M = 2.59, SD = 0.82): both were significantly lower than all remaining diseases (pairwise comparisons: p < 0.001). The value of 3 = “undecided” was exceeded for all other diseases (M from 3.21 to 4.29). The intraoral conditions significantly rated as most common in patients with dementia (value ≥ 4, “somewhat agree”) were caries (M = 4.06, SD = 0.85), periodontitis (M = 4.08, SD = 0.83), and gingivitis (M = 4.29, SD = 0.70). In sum, participating dentists assessed the probability of intraoral diseases to occur more frequently in patients with dementia between 3 = “undecided” and 4 = “more likely true” (overall M = 3.44).
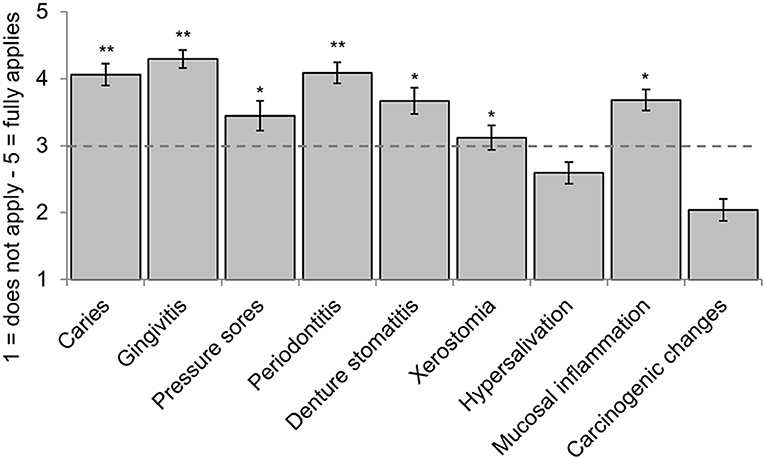
Figure 3. Estimated intraoral diseases in patients with dementia (means, 95%-CIs). Caries, gingivitis, pressure sores, periodontitis, denture stomatitis, xerostomia, hypersalivation, oral mucosal inflammation, carcinogenic changes; *exceeds expression 3 = “undecided”; **exceeds expression 4 = “somewhat agree,” n = 101–106.
The aim of the present study was to obtain more information on the hitherto insufficiently researched current state of outpatient dental care in patients with dementia. To this end, we evaluated the results of a cross-sectional survey of 119 dentists in private practice, focusing on: (1) practice equipment and consultation, (2) training and expertise, (3) dealing with special circumstances of dental treatment.
In the majority of practices, aids were used to improve the treatment situation in order to render dental treatment in patients with dementia as stress-free as possible. Deficits in equipment were evident in the use of dental benches and the low availability of toilet facilities suitable for individuals with special needs. Despite the considerable associated time burden, more than two-thirds of the participating dentists reportedly performed consultations in nursing homes, and almost half of the respondents even performed consultations at individual patients' homes. Although this does not per se indicate a high level of continuity of care, it does at least indicate a good quality of care based on studies to date [14, 15].
The reported sensitivity for the specific issues related to dental care in patients with dementia was in sharp contrast to the rate of specific training in gerodontology: it was extremely low among both dental and practice staff, with only a small minority of respondents reporting a corresponding qualification at the time of the survey. Topics related to senior dentistry are yet underrepresented in undergraduate study programs [16], and considering the increasing proportion of older people in the population, improvement is strongly warranted [17]. Encouragingly, a majority of respondents expressed interest in specific training in dementia-sensitive dental care. The respondents also stated that they had already themselves undertaken comprehensive efforts to adapt their treatment strategies to the needs of patients affected by dementia (e.g., adapted communication, inclusion of relatives, scheduling of more time) [12]. This highlights that dental practitioners are indeed sensitive to the topic and raises the question whether the low rate of specific training may rather result from insufficient availability of adequate training opportunities. While time constraints often limit the implementation of further training at the post-graduate level (i.e., in parallel to the daily practice), it seems promising to offer specific gerodontological courses already at the undergraduate level, which would also sensitize aspiring dentists to this important issue.
Regarding dental treatment itself, the majority of dentists reportedly considered the special circumstances in treating patients with dementia. For example, they stated that indication for tooth extractions was generally stricter, and that dentures were designed as simply as possible, indicating that they paid attention to preservation of functionality and ease of use [13]. Early conversion to removable dentures was performed by only a quarter of the respondents. While we did not explicitly ask about the possible reasons for this, we suggest that they could include increased wearing comfort, better acceptance of fixed dentures by the patients, and protection against loss of removable dentures. Overall, respondents rated the incidence of intraoral disease in patients with dementia as significantly increased. This is in agreement with numerous studies [18–20]. Treatment under sedative medication or even general anesthesia in patients with dementia was performed by only a small proportion of the dentists surveyed. Instead, the majority of patients requiring sedation or general anesthesia were referred to full inpatient treatment, which allows closer monitoring. In our view, this was likely adequate, as the dentists surveyed carefully weighed the associated risks and benefits. As individuals with dementia are particularly prone to suffering from delirium as an acute complication or postoperative cognitive dysfunction (POCD) as a possible long-term consequence of general anesthesia [21], any form of deeper sedation must be carefully considered in this vulnerable population, and most dental practices are not equipped to adequately cope with such situations.
At 29.3%, the response rate in the present study can be considered good for a postal survey [22]. Nevertheless, we cannot completely exclude potential biases. Most importantly, since the questionnaire had a large number of items and a detailed cover letter, it can be assumed that the majority of respondents who provided information also showed above-average interest in the topic. Thus, some statements (e.g., interest in gerodontological training, adaptation of treatment strategy) are very likely to be positively biased—also due to the mean age of the sample (~53 years). In our sample, the majority of respondents were male (68.9%), but, on the other hand, this is in line with a nationwide survey for the year 2019 (Lower Saxony: 64.5% male dentists in private practice) [23]. While we cannot exclude that age and gender distribution of the respondents might have influenced the data reported here, it should be noted that no significant differences between male compared to female dentists were found regarding the main outcomes in this study. Future use of online questionnaires could encourage more, including younger, practitioners to participate, and thus further increase the representativeness of the sample beyond the regional sample reported here. A larger number of participants would also further validate the questionnaire employed. As of now, the cross-sectional study reported here essentially represents a snapshot and allows for a primarily descriptive analysis of the data. A longitudinal version of our survey may, for example, prove useful when applied before and after specific gerodontological training, as it could help to assess the efficacy of such an intervention.
Despite the comprehensive questionnaire used in this study, the inclusion of additional items might, retrospectively, have been helpful to assess to what extend dementia-specific training of dentists can be considered (in)-sufficient. First, dentists' level of knowledge regarding the relationship between dental health and risk of dementia was not assessed—an important question that should be urgently surveyed in future studies, as the level of knowledge may be a moderator or mediator of other variables assessed here. Additional items may also cover fields in dentistry that require specific training, such as root canal treatment in older patients with multiple systemic conditions [24]. Second, questions concerning the usage of specialized practice equipment for safe treatment of older patients (e.g., bite blocks) should be added in a future survey, along with questions assessing the knowledge on a broader spectrum of dental diseases especially in older patients.
A further limitation arises from the fact that the questionnaire study was conducted before the onset of the ongoing SARS-CoV2 pandemic: older people, and particularly those with dementia and/or residing in care homes, are particularly vulnerable to a severe or even fatal disease course of COVID-19 [25]. Dental care is associated with considerable risk of SARS-CoV2 transmission [26], and specific precautions are required in vulnerable patients. Follow-up studies should thus assess how dentists have adapted their treatments of older people and particularly those with dementia as a result of the pandemic.
According to our survey results, dentists already use specific aids and treatment strategies as well as adapted therapeutic conversation when treating patients with dementia. Importantly, they are sensitive to an increased incidence of intraoral diseases in this population and show interest in additional specific training. However, the availability of such training for outpatient dentists is limited. An improvement and expansion of both undergraduate and continuing education opportunities is therefore recommendable, particularly since gerodontology will have a significantly higher relevance due to demographic change. Future studies should systematically assess the effects of gerodontological trainings on outpatient dental care in longitudinal studies, and the questionnaire presented here may constitute a helpful tool in the evaluation of such training interventions.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Ethics Comittee of the University of Göttingen, Faculty of Medicine. The patients/participants provided their written informed consent to participate in this study.
JW, SS, and TR: design and conception. SS, SM-R, and MB: data acquisition and analysis. MB: formal analysis. SS, CB, BS, and MB: writing. All authors approved the final version of the manuscript.
BS was supported by the Ministry of Social Affairs, Health, and Equal Opportunities of Lower Saxony (project call “Dementia in Hospitals”), and holds a grant from the European Union and the State of Saxony-Anhalt (Research Alliance “Autonomy in Old Age”). We acknowledge support by the Open Access Publication Funds of the Göttingen University.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to thank all respondents for taking the time and effort to participate in our survey.
1. ^No other significant differences were found between the demographic variables recorded. Additional exploratory subgroup analyses, based on the demographic information, were performed for the target variables collected in the questionnaire; however, no significant differences were found between the subgroups.
1. Petersen PE, Yamamoto T. Improving the oral health of older people: the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol. (2005) 33:81–92. doi: 10.1111/j.1600-0528.2004.00219x
2. Lee H, Kim D, Lee W, Kim HY, Kim Y. Preventive approach for overcoming dementia. Arch Pharm Res. (2019) 42:647–57. doi: 10.1007/s12272-019-01168-3
3. Rosa G, Giannotti C, Martella L, Massa F, Serafini G, Pardini M, et al. Brain aging, cardiovascular diseases, mixed dementia, and frailty in the oldest old: from brain phenotype to clinical expression. J Alzheimers Dis. (2020) 75:1083–03. doi: 10.3233/JAD-191075
4. Hatipoglu MG, Kabay SC, Güven G. The clinical evaluation of the oral status in Alzheimer-type dementia patients. Gerodontology. (2011) 28:302–6. doi: 10.1111/j.1741-2358.2010.00401x
5. Chen X, D'souza V, Yu L. The oral health status of residents with different cognitive and dental-related functions in three North Carolina assisted living facilities. Gerodontology. (2019) 36:142–8. doi: 10.1111/ger12391
6. Lauritano D, Moreo G, Della Vella F, Di Stasio D, Carinci F, Lucchese A, et al. Oral health status and need for oral care in an aging population: a systematic review. Int J Environ Res Public Health. (2019) 16:4558. doi: 10.3390/ijerph16224558
7. Fereshtehnejad SM, Garcia-Ptacek S, Religa D, Holmer J, Buhlin K, Eriksdotter M, et al. Dental care utilization in patients with different types of dementia: A longitudinal nationwide study of 58,037 individuals. Alzheimers Dement. (2018) 14:10–9. doi: 10.1016/j.jalz.2017.05004
8. Lopez-Jornet P, Zamora Lavella C, Pons-Fuster Lopez E, Tvarijonaviciute A. Oral health status in older people with dementia: a case-control study. J Clin Med. (2021) 10:477. doi: 10.3390/jcm10030477
9. Fratto G, Manzon L. Use of psychotropic drugs and associated dental diseases. Int J Psychiatry Med. (2014) 48:185–97. doi: 10.2190/PM.48.3d
10. Cohen-Mansfield J, Lipson S. The underdetection of pain of dental etiology in persons with dementia. Am J Alzheimers Dis Other Demen. (2002) 17:249–53. doi: 10.1177/153331750201700404
11. Chalmers JM. Behavior management and communication strategies for dental professionals when caring for patients with dementia. Spec Care Dentist. (2000) 20:147–54. doi: 10.1111/j.1754-4505.2000.tb01152x
12. Niessen LC, Jones JA. Professional dental care for patients with dementia. Gerodontology. (1987) 6:67–71. doi: 10.1111/j.1741-2358.1987.tb00391x
13. Nitschke I, Wendland A, Weber S, Jockusch J, Lethaus B, Hahnel S. Considerations for the prosthetic dental treatment of geriatric patients in Germany. J Clin Med. (2021) 10:304. doi: 10.3390/jcm10020304
14. Knabe C, Kram P. Dental care for institutionalized geriatric patients in Germany. J Oral Rehabil. (1997) 24:909–12. doi: 10.1046/j.1365-2842.1997.00196x
15. Miremadi SR, Cosyn J, Janssens B, De Bruyn H, Vanobbergen J, De Visschere L. A pilot assessment tool of the need for oral health care and cost prediction in institutionalized elderly people. Int J Dent Hyg. (2017) 15:306–12. doi: 10.1111/idh12222
16. Nitschke I, Neitzel M, Sobotta B.a.J. Development of undergraduate gerodontology courses in Austria, Germany and Switzerland 2004-2014. Eur J Dent Educ. (2018) 22:e303–e11. doi: 10.1111/eje12294
17. Stuck AK, Schimmel M. A model for a geriatric teaching program and its impact on self-rated and tested competencies of undergraduate dental students. Eur J Dent Educ. (2021) doi: 10.1111/eje12668. [Epub ahead of print].
18. Gao SS, Chen KJ, Duangthip D, Lo ECM, Chu CH. The oral health status of Chinese elderly people with and without dementia: a cross-sectional study. Int J Environ Res Public Health. (2020) 17:1913. doi: 10.3390/ijerph17061913
19. Yamaguchi S, Horigome Y, Endo K, Komagata M, Komai S, Komaki K, et al. Caregiver-reported dementia as a predictor of oral health among patients receiving home-visit dental treatment: a retrospective cohort study. Clin Exp Dent Res. (2021) 7:49–55. doi: 10.1002/cre2333
20. Zeng LN, Zong QQ, Xu SW, An FR, Ungvari GS, Bressington DT, et al. Oral health in patients with dementia: a meta-analysis of comparative and observational studies. Int J Geriatr Psychiatry. (2021) 36:467–78. doi: 10.1002/gps5453
21. Fong TG, Davis D, Growdon ME, Albuquerque A, Inouye SK. The interface between delirium and dementia in elderly adults. Lancet Neurol. (2015) 14:823–32. doi: 10.1016/S1474-4422(15)00101-5
22. Sinclair M, O'toole J, Malawaraarachchi M, Leder K. Comparison of response rates and cost-effectiveness for a community-based survey: postal, internet and telephone modes with generic or personalised recruitment approaches. BMC Med Res Methodol. (2012) 12:132. doi: 10.1186/1471-2288-12-132
23. Bundeszahnärztekammer. Berufliche Stellung (2019). Available online at: https://www.bzaek.de/ueber-uns/daten-und-zahlen/mitgliederstatistik/berufliche-stellung/ (accessed April 6, 2021).
24. AlRahabi MK. Root canal treatment in elderly patients: a review and clinical considerations. Saudi Med J. (2019) 40:217–223. doi: 10.15537/smj.2019.323769
25. Panagiotou OA, Kosar CM, White EM, Bantis LE, Yang X, Santostefano CM, et al. Risk factors associated with All-cause 30-day mortality in nursing home residents with COVID-19. JAMA Intern Med. (2021) 34:181–6. doi: 10.1001/jamainternmed.20207968
Keywords: dementia, gerodontology, outpatient dental care, treatment strategy, aging
Citation: Schaper S, Meyer-Rötz S, Bartels C, Wiltfang J, Rödig T, Schott BH and Belz M (2021) Dental Care of Patients With Dementia: A Survey on Practice Equipment, Training, and Dental Treatment. Front. Oral. Health 2:682139. doi: 10.3389/froh.2021.682139
Received: 17 March 2021; Accepted: 12 April 2021;
Published: 07 May 2021.
Edited by:
Katherine C. M. Leung, The University of Hong Kong, Hong KongReviewed by:
Fabricio Ferreira de Oliveira, Elysian Clinic, BrazilCopyright © 2021 Schaper, Meyer-Rötz, Bartels, Wiltfang, Rödig, Schott and Belz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michael Belz, bWljaGFlbC5iZWx6QG1lZC51bmktZ29ldHRpbmdlbi5kZQ==; orcid.org/0000-0001-9250-6049
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.