
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Health Serv. , 13 March 2024
Sec. Health Policy and Management
Volume 4 - 2024 | https://doi.org/10.3389/frhs.2024.1372522
This article is part of the Research Topic Digital Health Applications: Acceptance, Benefit Assessment, and Costs from the Perspective of Patients and Medical Professionals View all 12 articles
 G. D. Giebel1*
G. D. Giebel1* C. Abels1K. Börchers2B. Kampka2S. Neusser1H. R. Cissarek1F. Plescher1J. Wasem1N. Blase1
C. Abels1K. Börchers2B. Kampka2S. Neusser1H. R. Cissarek1F. Plescher1J. Wasem1N. Blase1
Introduction: Since 2019 people who have insured in the German statutory health insurance are entitled to use certified apps called the Digitale Gesundheitsanwendungen [Digital Health Applications (DiGAs)]. The prerequisite for this is that an app certified as DiGA and suitable for their diagnosis exists. The DiGA can then either be prescribed by a physician or psychotherapist or requested by the patient from the statutory health insurance fund. Given the novelty of this type of healthcare, the implementation of a DiGA should be closely monitored to identify potential weaknesses and achieve quality improvements. To enable an analysis of the supply of DiGAs step-by-step, we aimed to create the DiGA-Care Path.
Methods: We conducted three steps to create the DiGA-Care Path. First, a knowledge base was created based on a structured literature research matched with knowledge gathered from the superordinate research project “QuaSiApps” funded by the German Federal Joint Committee. Second, we aimed to create an “ideal-typical” DiGA-Care Path using a flowchart. Third, based on the first path, a final path was developed using the graphical modeling language “Event-Driven Process Chain.”
Results: The DiGA-Care Path was developed to depict the supply of DiGAs in Germany. The final path is constituted by a “main path” as well as a corresponding “sub-path”. While the “main path” focuses more on the supply environment in which a DiGA is used, the “sub-path” depicts the supply delivered by the DiGA itself. Besides the process itself, the paths include relevant actors to indicate responsibilities for individual process steps.
Discussion: The DiGA-Care Path helps to analyze the current supply of DiGAs step-by-step. Thereby, each step can be investigated in detail to identify problems and to detect further steps where quality improvements can be enabled. Depending on the perspective, focused either on the supply environment, or the supply delivered by the DiGA itself, the “main path” or the “sub-path” can be used, respectively. Besides the potential of the DiGA-Care Path to improve the current supply of DiGAs, it can help as an orientation for international policymakers or further stakeholders either to develop their own integration of apps into healthcare systems or for international manufacturers to consider entering the German market.
Since the introduction of the Apple iPhone in 2007, mHealth apps are on the rise and permit multiple patient benefits. These benefits can be achieved in five domains: educational health applications, applications to contact healthcare professionals, applications to check the personal health records, personal care applications, and social networking applications (1).
To help patients benefit from opportunities through mHealth apps, the German Bundestag passed the Digital Care Act (DVG) in 2019. This act established specific mobile as well as web apps also known as Digitale Gesundheitsanwendungen [Digital Health Applications (DiGAs)] as an integral part of the German healthcare system (2). Other European countries such as France and Austria are also considering establishing similar concepts (3). In addition, efforts are being made at the European level to establish a harmonized authorization (4).
DiGAs are not limited to mobile apps; they can also exist in the form of web applications or include other devices [such as virtual reality (VR) glasses]. To become a DiGA, an app has to go through a testing procedure, the “Fast-Track Process for Digital Health Applications (DiGA) according to Section 139e SGB V” (5, 6). The basic requirements for a DiGA tested in this process are as follows: (1) The app must be a European conformity (CE)-certified medical product (risk class I or IIa); (2) the main function of the app is based on digital technologies; (3) the app supports the recognition, monitoring, treatment, or alleviation of diseases or the recognition, treatment, alleviation, or compensation of injuries or disabilities [§33a Social Code Book V (SGB V)]. An approval for apps focused on primary prevention is not provided. After passing the Fast-Track Process, the app will be registered in the DiGA directory managed by the Federal Institute for Drugs and Medical Devices (BfArM) and is reimbursable by the German statutory health insurance.
In general, there are two categories of listing in the directory: (1) DiGA with a provisional listing or (2) DiGA with a final listing. The decision depends on the availability of a comparative study that is suitable to prove a positive healthcare effect. If such a proof exists, a DiGA can directly be final listed in the directory. If manufacturers cannot present a suitable study, they can apply for provisional listing. Nevertheless, all listed DiGA must fulfill requirements such as security, functional capability, quality, data protection, and information security, regardless of their listing status (provisional or final). A corresponding study to prove the positive healthcare effect can be carried out retrospectively as part of a trial phase lasting up to 1 year. If there is a prospect of evidence, a decision may be made at the request of the manufacturer to grant a maximum of a further 12 months for the proof (5, 6).
There are two valid types of positive healthcare effects: Either in the form of a medical benefit or in the form of a patient-relevant improvement of structure and processes (§139e Abs. 2 SGB V). Prior to the approval study, a target patient group has to be determined according to the International Classification of Diseases (ICD-10). Reimbursement for a DiGA is only provided for this designated patient group (5, 6).
The DiGA prices are regulated within §134 SGB V. They differ between the first year and subsequent years. In the first year, the manufacturer is free to determine a price. However, fixed reference price groups must be taken into account depending on the indication and the category of positive healthcare effect. From the 13th month, prices apply that are negotiated between the manufacturer and the National Association of Statutory Health Insurance Funds (GKV-Spitzenverband). If no agreement is reached, an independent arbitration board decides on the price.
Once listed, the manufacturer still has some obligations. In case of significant changes to the DiGA, the BfArM has to be informed. Furthermore, the manufacturer must ensure that information in the DiGA directory, in the distribution platform, or on the application website, is up-to-date and complete. With regard to further requirements, continuous maintenance, reassessment, and further development of the technical and organizational data protection and information security measures must be ensured. This also includes penetration tests. Further requirements are listed within the guide for manufacturers, service providers, and users provided by the BfArM (5, 6) or the Digital Health Applications Ordinance (DiGAV) (7).
Currently, the DiGA directory includes 56 DiGAs. Thereof, 24 DiGAs are provisionally listed and 32 DiGAs are final listed. Six DiGAs could not prove their positive healthcare effect and were subsequently delisted. DiGAs are approved for a broad range of diseases, such as mental illnesses, cardiovascular diseases, cancer, diseases of the muscles, bones, and joints, or hormonal or metabolic diseases (8). Overall, the demand for DiGAs is increasing. While the health insurance funds reimbursed just under 40,000 DiGAs in the first year (October 202 –September 2021), the number rose to over 200,000 reimbursements last year (October 2022–September 2023) (3).
Although safety and clinical performance are tested in the context of the medical device approval process [Medical Device Regulation (MDR), Annex I Chapter 1] and further test criteria such as data protection, information security, interoperability, and further quality requirements are part of the Fast-Track test procedure (5, 6), several problems can emerge within the use of a DiGA. These were found in 10 different categories: (1) validity, (2) usability, (3) technology, (4) use and adherence, (5) data privacy and security, (6) patient–physician relationship, (7) knowledge and skills, (8) individuality, (9) implementation, and (10) costs. On a more abstract level, these are problems concerned either with the DiGAs themselves or their integration into the healthcare system (9).
To address these existing problems and to ensure a high quality of DiGAs, we established the QuaSiApps project with the aim to develop a comprehensive, continuous quality assurance system for DiGAs (10, 11). The project is funded by the German Federal Joint Committee (12).
According to the International Organization for Standardization (ISO) 9000 standard, quality is “the degree to which a set of inherent characteristics fulfills requirements” (13). Thus, a fundamental need to determine the quality of a DiGA and its supply is to know the requirements and gain clarity about the exact procedures and the respective tasks of the concerned parties. One way to guarantee such clarity is the visualization in the form of a care path as the ideal-typical path for the defined patient groups with its decisive diagnostic services in chronological order (14).
Care paths are a methodological basis for the development of quality assurance procedures. Despite some indifferent results, it is now well documented that care paths—or their implementation as a control and standardization instrument for processes—are effective and useful in the context of quality management and quality assurance (15, 16). However, the requirements for the creation of care paths are complex, especially because the fundamental question of care paths: “Who does what with whom at what time” (17) is complex and challenging with regard to the various interfaces (including service providers, payers, and patients). We searched for a clear definition, and a precise depiction, of the ideal-typical care path in the context of DiGAs to build on our quality assurance system. Since our research on guidelines or care paths for DiGA did not result in any eligible results, we determined to create the actual DiGA-Care Path by ourselves. In addition to the benefits that the DiGA-Care Path brings to our project, it can also help national and international stakeholders and interested parties to understand the German DiGA-Care System and look at it in detail.
Hence, the aim of this research was twofold. First, we collected available evidence on the supply of DiGAs in Germany to create a clear understanding of the process, and second, we developed the DiGA-Care Path upon this base.
We pursued a three-stage process to develop the DiGA-Care Path. First, we conducted a structured literature research to identify relevant articles and legal standards describing the supply of DiGAs. Therefore, we searched in scientific databases such as MEDLINE via PubMed and Embase for websites of DiGA-relevant stakeholders in the German healthcare system as well as relevant laws and acts in the context of healthcare supply and especially DiGAs. Hereby, the aim was not to conduct an exhaustive research identifying all the relevant literature in the context of these apps but to gain a broad and reliable knowledge base on which the DiGA-Care Path can be developed further.
Second, a first version of the DiGA-Care Path (see Supplementary Figure S1) was developed. It summarizes the ideal-typical path of DiGA patient groups with decisive services in the chronological sequence. In addition, the actors involved and the DiGA interventions (e.g., the performance of a DiGA application anamnesis) are depicted.
This first care path is based on various sources of knowledge that were generated both within the QuaSiApps project and with the help of external literature. A flowchart was modeled based on: (1) statements of patients (18) and experts from a qualitative survey within the project; (2) a case-based problem outline of medical ethical implications in the use of a DiGA (19); (3) the four medical ethical principles of autonomy, care, non-harm, and justice (20); and (4) the model professional code for doctors working in Germany (21).
Based on this draft, we discussed and decided that the model would benefit from a modeling language that enables a more complex branching than “yes/no-decisions.” We also wanted to add the relevant application software (in our context, the DiGA) and the relevant organizational unit (e.g., patient, DiGA manufacturer, or service provider) to the respective process steps in the path. Since the Event-Driven Process Chain (EPC) modeling language developed at the Institute for Information Systems (IWi) at the University of Saarland, Germany (22), offers these possibilities, we used it.
To depict the processes, the EPC uses alternating events and functions that are connected through arrows, showing what is called the “Control Flow.” In case a function can be followed by different “Events,” “Connectors” are used to branch the “Control Flow.” In our case we used “XOR (Either-or)” and “OR (And-or) Connectors.”
To clarify which executing body is responsible for a function, we modeled the respective “Organizational Unit” to each function. Where indicated, we added the DiGA as an “Application Software.” To indicate the conjunction between a main- and a sub-path, an interface was implemented by a “Sub-process” (cf. Figure 1).
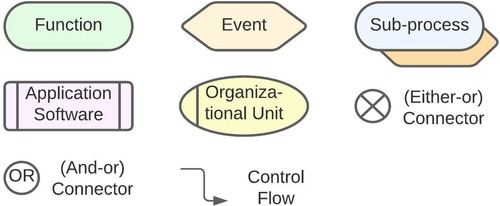
Figure 1. Basic components of the event-driven process chain.
To implement the DiGA-Care Path, we used Lucidchart (23), a web-based diagramming application from Lucid Software Inc. that allows visualization of charts and diagrams, organizational structures, and especially processes.
Finally, after developing the DiGA-Care Path, we sent it out to independent DiGA-experts without conflicts of interest with the research project and asked them after 1 week within an online meeting to evaluate whether the path is correct and intuitive to understand.
To develop the DiGA-Care Path, we started with the structured literature search yielding four legal standards (cf. Table 1), six articles (9, 19, 24–27), the QuaSiApps project accompanying working paper (10), a book about DiGAs (28, 29) as well as the Fast-Track Process for DiGA (5, 6) (cf. Table 2).
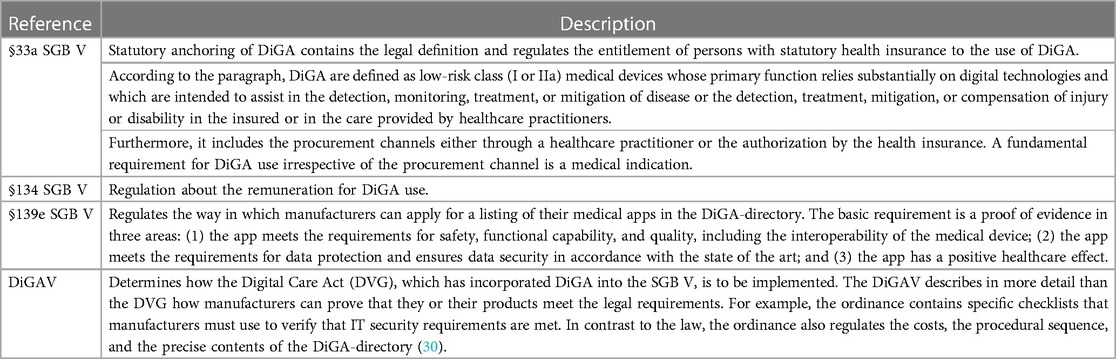
Table 1. Legal standards relevant in the context of DiGA.
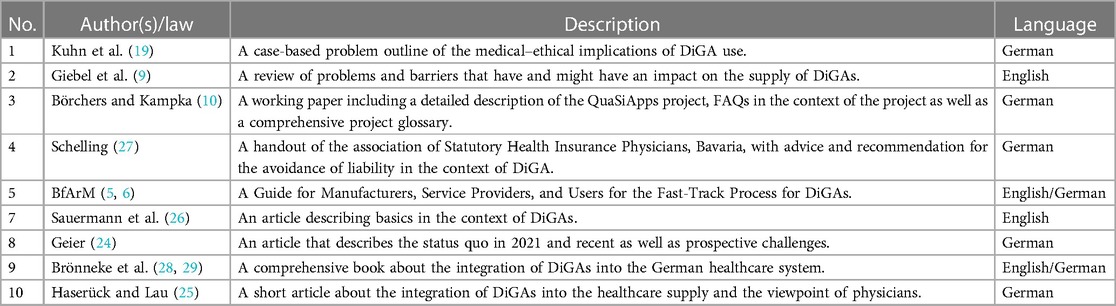
Table 2. Sources included from the structured research that were used to build the DiGA-Care Path.
Based on the included articles and the knowledge generated within the QuaSiApps project, authors KB and BK developed a first DiGA-Care Path (September 2022) as a basis for discussion. After a project meeting that served for a discussion on the consortium of gathered ideas, corrections and improvements were highlighted and we consented to rework the path and implement it in more detail.
Mainly the need for an either–or branching after an activity or function led to the decision to choose another more comprehensive modeling language. Thus, we chose the EPC allowing this modeling.
To reduce the complexity, we decided to separate the DiGA-Care Path into a main path as well as a sub-path contained therein. The main path represents the supply environment in which the DiGA is used (cf. Figure 2). The sub-path includes the supply by the DiGA itself (cf. Figure 3). According to the consensus, the final paths were iteratively modeled with feedback loops including the whole consortium.
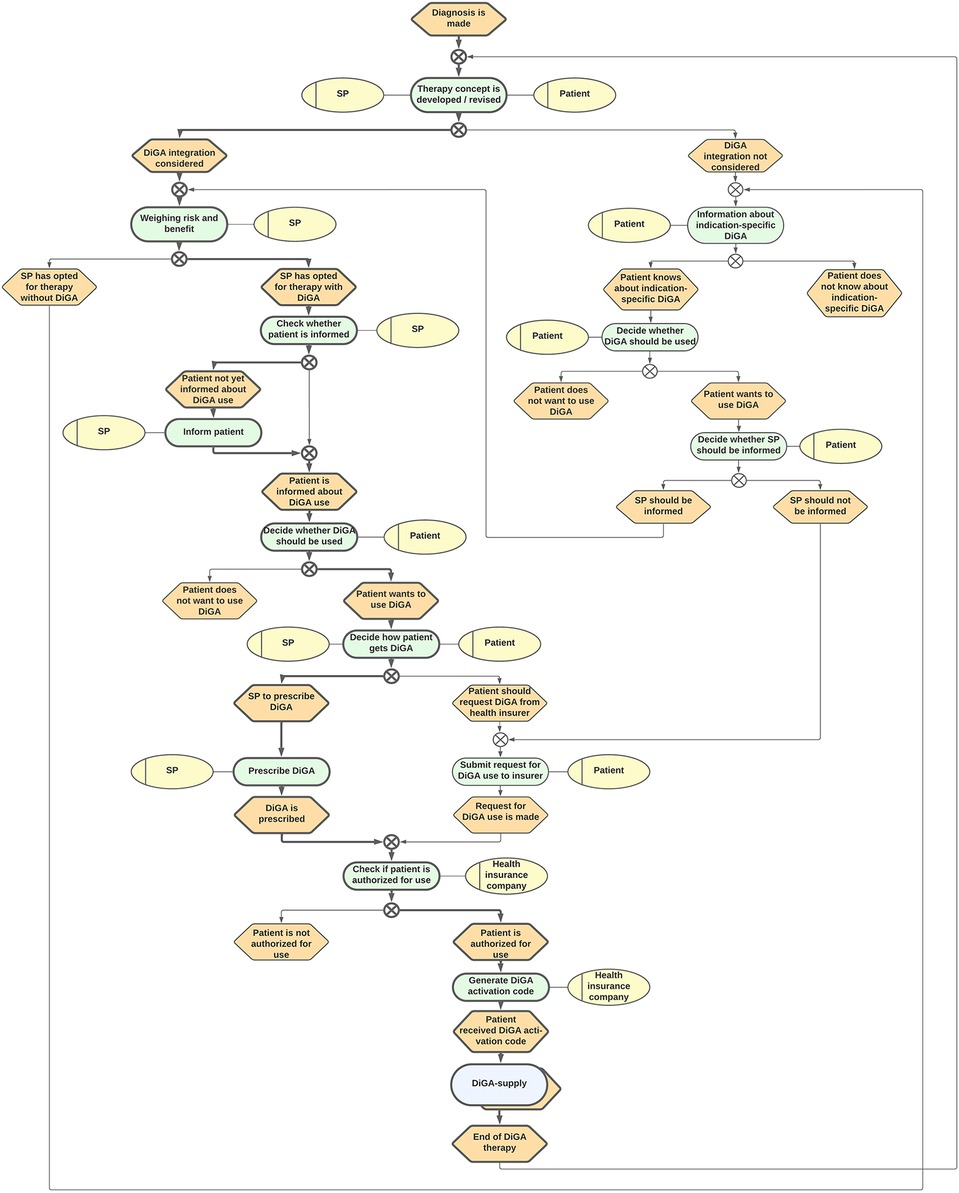
Figure 2. DiGA-Care Path 1: supply environment in which DiGAs are used. SP, Service provider (either physician or psychotherapist); DiGA, Digitale Gesundheitsanwendung (Digital Health Application).
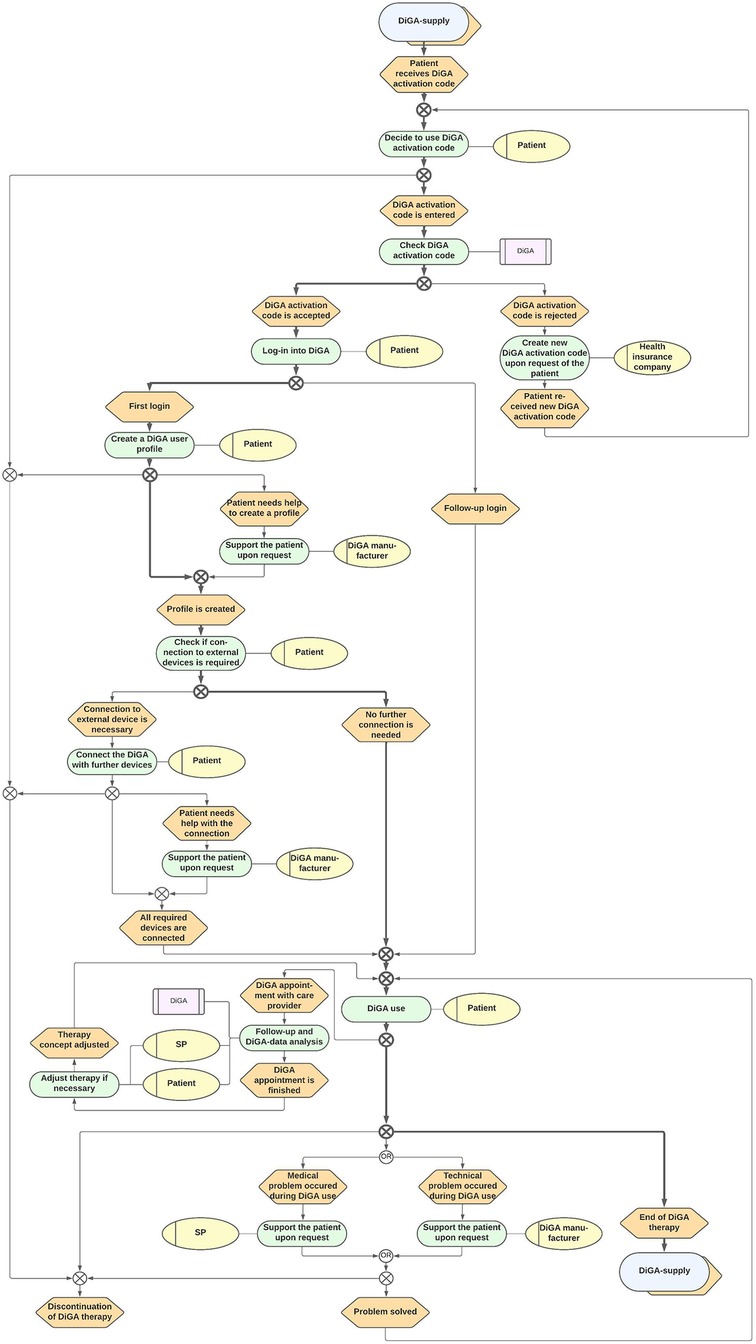
Figure 3. DiGA-Care Path 2: supply by the DiGA itself. SP, Service provider (either physician or psychotherapist); DiGA, Digitale Gesundheitsanwendung (Digital Health Application).
Once the paths were developed, we sent them to four independent experts for review. We then held an online meeting together with the experts to discuss the accuracy and comprehensibility of the DiGA-Care Paths. Both paths were judged to be easily understandable as well as correct in content. Nevertheless, it was suggested to emphasize the most frequently followed path within the DiGA-Care Path. To find this, we used the DiGA-Report 2022 from Germany's largest health insurance company. According to the report, 85% of users receive their DiGA via a prescription and 15% receive it via a direct request to their health insurance company (31).
The final paths are represented in Figures 2, 3. Since they were judged to be self-explanatory, only a short, written description of the process is given here.
The “Supply environment in which DiGAs are used” is depicted in care path 1 (cf. Figure 2). Care path 1 is the higher-level process that includes the “Supply by the DiGA itself” (cf. Figure 3) as a sub-process.
The starting point of DiGA supply is always the diagnosis of a disease made by a healthcare practitioner for which a DiGA exists. After the diagnosis, the healthcare practitioner and patient together develop a concept of therapy that can either include a DiGA or not. If the healthcare practitioner estimates the risk–benefit assessment positive, he offers to inform the patient about the use of the DiGA. If the patient is already experienced with the appropriate DiGA, he can waive the medical information. If the patient declines the use of the DiGA at any point, the app does not become part of the healthcare supply.
If the patient and healthcare practitioner both decide to integrate DiGA into the therapy, the usual path will continue with a prescription made by the healthcare practitioner. Subsequently, the health insurance company of the patient will check if the patient is entitled to use the DiGA or not. If their review results in a positive assessment, the patient receives an activation code to use the DiGA.
Otherwise, if either the healthcare practitioner is not aware of the DiGA or declines its usage within the concept of therapy, the patient himself can request for the DiGA when given the suitable diagnosis (and no relevant contraindications) directly from his healthcare insurance company.
Irrespective of the way of procurement, the patient always has the option to ask or inform the healthcare practitioner about the DiGA use.
The supply provided by the DiGA itself is shown in care path 2 (Figure 3). This path is a sub-process of the supply environment process. After the patient receives his activation code, he decides whether to use it or not. If he does not use it, the DiGA therapy is canceled. Otherwise, the code is checked by the DiGA automatically. Once the code is accepted and the user creates a profile and connects any additional devices, the patient can use the DiGA. In case of any appointments due to the use, the healthcare practitioner and patient analyze the DiGA data and possibly adjust the DiGA therapy concept. If there are any medical or technical problems during use, the patient should get support from his healthcare practitioner or the manufacturer, respectively. If the problem is solved, the patient can continue the use. At the end of the “DiGA utilization period,” the patient is redirected to the care path 1 and should evaluate (alone or together with the healthcare practitioner) whether a further use is indicated or not.
The DiGA-Care Path was developed to depict the supply of DiGAs in the German healthcare system. It enables researchers, policymakers, and further stakeholders to analyze the supply of a DiGA step-by-step, to identify the parties involved in each case and to locate potential weaknesses, problems, and quality indicators at individual points.
In principle, it can be assumed that the German healthcare system improves through the integration of DiGAs. This assumption is mainly based on two reasons: (1) A DiGA must prove either a medical benefit or a patient-relevant improvement of structure and processes (§139e Abs. 2 SGB V), and (2) the positive attitude of outpatient-care general practitioners, physicians, and psychotherapists (32) as well as physical therapists, occupational therapists, and speech-language pathologists (33) toward DiGAs. Nevertheless, there are several problems and barriers that might impede the prescription and use of a DiGA (9, 32). To face those challenges as well as to optimize the integration and maximize the subsequent positive effects of DiGAs, different approaches should be pursued. One is the implementation of quality assurance. The starting point for quality assurance should be a clear understanding of the care process. Therefore, we gathered and analyzed laws, literature, and project knowledge to build on the DiGA-Care Path.
Even if the high quality of the DiGA itself and its optimal integration into existing care are factors that affect patient benefit, other factors such as the actual use of the app must be taken into account. To verify the actual patient benefit, a new law provides the implementation of application-related performance measurements. This law, the “Act to accelerate the digitalization of the healthcare system” [Digital-Gesetz (DigiG), not yet in force] (34) will also bring further changes such as a closer integration of DiGAs into existing processes and the extension of the risk class of DiGAs to class IIb according to the MDR.
Even if the developed path correctly represents the theoretical requirements for the supply, at some points in the supply reality, the supply of DiGAs could deviate from the path. Such an example we know from focus groups with patients (18) within the QuaSiApps project: In some cases, younger, tech-savvy family members take on the role of DiGA manufacturers and support users with technical questions.
Especially, the closer integration into existing processes is welcomed by many stakeholders because concerns were raised that DiGAs should not be used without integration into the standard care provided by physicians and psychotherapists [e.g., the German Psychotherapists Association (35), the German Diabetes Society (36), the Professional Association for Orthopaedics and Trauma Surgery e.V (37), or Heidel et al. (38)]. Nevertheless, insufficient reimbursement of medical services in the context of DiGAs might be a problem or barrier toward the prescription of DiGAs by physicians or psychotherapists (9, 32, 38). Such changes should always be kept in mind when using the DiGA-Care Path. From time to time, it should be reflected if the DiGA-care is changing and if subsequent changes should be implemented in the DiGA-Care Path.
Furthermore, even if not regulated yet, other stakeholders such as physical therapists, occupational therapists, and speech-language pathologists might play a role in the supply of DiGAs. Thus, for example, a survey with 150 therapists found that 87.3% indicated a positive intention to use a DiGA. In addition, it was to be expected that patients would use DiGAs incorrectly and that errors could therefore occur during training with an app. Therefore, it is necessary to examine to what extent a DiGA can replace an in-person therapy, or whether supplementary or partial replacement use is preferable (33).
Even if apps are becoming more ubiquitous in healthcare systems all over the world, most countries, however, did not or only rudimentarily regulate their integration and use. Also, the European Union only dictates that apps must fulfill the criteria of the MDR to become medical products and to receive admission to healthcare systems and in the secondary healthcare market. Further regulations about how apps should be integrated into care do not exist on this level. Germany took it one step further and created a legal basis for the integration of distinct apps (DiGAs).
But even if there is a legal basis, the integration of DiGAs into care paths is uncertain. Therefore, the National Association of the Statutory Health Insurance Funds emphasized: “DiGA must be integrated into the care paths. To this end, the potential for digitalization in treatment and networking across service sectors must be exploited” (39). While we depicted the general DiGA-Care Path that is independent of indication, the integration of DiGAs should also be considered in the context of disease-specific care paths, especially by medical professional societies.
DiGA-care in Germany is a very complex system. Nevertheless, we aimed to illustrate it as clearly organized as possible. Therefore, we had to neglect some aspects. Such an aspect is especially the contact between the patient and the healthcare practitioner. Even if we depicted this contact at some points of our path, it should be emphasized that the patient should always have the option to contact the respective healthcare practitioner at any time during the DiGA-Care Path.
We decided to use the EPC to represent the German DiGA supply. Even if the EPC was originally developed to model business processes (22), it proved to be the right modeling language for our purpose. This was mainly because it provides the possibility to use Either–Or Connectors, which were necessary to detail the complex system, and because of the easy readability. Since there is a variety of other modeling languages (e.g., the BPMN), translating the DiGA-Care Path into other forms of representation could also be considered.
The DiGA-Care Path was reviewed by four independent DiGA-experts. It can therefore be assumed that in principle it correctly maps the supply of DiGAs. Nevertheless, the review did not include a broad range of different stakeholders. Further stakeholders, such as patients, physicians, manufacturers, or policymakers, should also be asked about their assessment of the appropriateness of the path. Hence, the path should be subject to further discussion and could therefore be subject to change in the future.
A further limitation was the non-systematic evidence collection we used to develop the DiGA-Care Path. We did not conduct a systematic literature review or a systematic survey of experts. Therefore, there is a risk that the evidence is incomplete. Nevertheless, we are convinced that based on the knowledge gathered during the project, together with the literature and the review by the four experts, our DiGA-Care Path adequately represents the DiGA-care.
We analyzed and subsequently visualized the DiGA-Care Path using the graphical modeling language EPC. Thereby, the DiGA-care process becomes transparent and can be further investigated in detail. The developed DiGA-Care Path serves as a solid foundation to examine the weaknesses of the current situation as well as to indicate areas where one can start to improve care. Furthermore, it provides an overview of the German DiGA supply. Thus, the DiGA-Care Path can either be used as an inspiration for policymakers or further stakeholders to develop their own integration of mHealth apps into healthcare systems, or for international manufacturers to consider entering the German market.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants in accordance with the national legislation and the institutional requirements.
GG: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. CA: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Validation, Visualization, Writing – review & editing. KB: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Validation, Visualization, Writing – review & editing. BK: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Validation, Visualization, Writing – review & editing. SN: Conceptualization, Funding acquisition, Validation, Writing – review & editing. HC: Data curation, Formal Analysis, Validation, Writing – review & editing. FP: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Validation, Visualization, Writing – review & editing. JW: Funding acquisition, Project administration, Supervision, Validation, Writing – review & editing. NB: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – review & editing.
The authors declare that financial support was received for the research, authorship, and/or publication of this article.
The research project [“Continuous quality assurance of Digital Health Applications”, respectively “Fortlaufende Qualitätssicherung von in der GKV-Regelversorgung eingesetzten Gesundheits-Apps” (“QuaSiApps”)] is funded by the German Federal Joint Committee (01VSF20007—QuaSiApps). The authors acknowledge the support from the Open Access Publication Fund of the University of Duisburg-Essen. The funders had no influence in the study design, conduct of the study, or the decision to publish or prepare the manuscript.
The authors thank Tonio Schönfelder, Sina Busse, Ulrich Paschen, and Susanne Rode for their professional support within the QuaSiApps project.
KB and BK were employed by QM BÖRCHERS CONSULTING+.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frhs.2024.1372522/full#supplementary-material
1. Pires IM, Marques G, Garcia NM, Flórez-Revuelta F, Ponciano V, Oniani S. A research on the classification and applicability of the Mobile health applications. J Pers Med. (2020) 10(1):11. doi: 10.3390/jpm10010011
2. Bundesgesundheitsministerium [Federal Ministry of Health]. Driving the Digital Transformation of Germany’s Healthcare System for the Good of Patients (2020). Available online at: https://www.bundesgesundheitsministerium.de/en/digital-healthcare-act.html (accessed January 9, 2024).
3. Meskendahl D, Bachmann T. Marktentwicklung Digitaler Gesundheitsanwendungen (DiGA-report). Berlin: Spitzenverband Digitale Gesundheitsversorgung e.V. (2024). Available online at: https://digitalversorgt.de/wp-content/uploads/2024/01/DiGA-Report-2023.pdf (accessed January 12, 2024).
4. European Institute for Innovation and Technology—Health. European Taskforce for Harmonised Evaluations of Digital Medical Devices (DMDs). (n.d.). Available online at: https://eithealth.eu/european-taskforce-for-harmonised-evaluations-of-digital-medical-devices-dmds/ (accessed January 12, 2024).
5. Bundesinstitut für Arzneimittel und Medizinprodukte [Federal Institute for Drugs and Medical Devices]. The Fast-Track Process for Digital Health Applications (DiGA) According to Section 139e SGB V. A Guide for Manufacturers, Service Providers and Users. Bonn: BfArM (2020). Available online at: https://www.bfarm.de/SharedDocs/Downloads/EN/MedicalDevices/DiGA_Guide.html (accessed January 9, 2024).
6. Bundesinstitut für Arzneimittel und Medizinprodukte [Federal Institute for Drugs and Medical Devices]. Das Fast-Track-Verfahren für digitale Gesundheitsanwendungen (DiGA) nach § 139e SGB V. Bonn: BfArM (2023). Dez. Available online at: https://www.bfarm.de/SharedDocs/Downloads/DE/Medizinprodukte/diga_leitfaden.html (accessed January 9, 2024).
7. Bundesgesundheitsministerium [Federal Ministry of Health]. Digitale-Gesundheitsanwendungen-Verordnung (DiGAV) (2021). Available online at: https://www.bundesgesundheitsministerium.de/service/gesetze-und-verordnungen/detail/digitale-gesundheitsanwendungen-verordnung-digav.html#chr-261 (accessed February 19, 2024).
8. Bundesinstitut für Arzneimittel und Medizinprodukte (Federal Institute for Drugs and Medical Devices). DiGA-Verzeichnis (2024). Available online at: https://diga.bfarm.de/de/verzeichnis?sort=publicationDate-desc&type=%5B%5D (accessed February 19, 2024).
9. Giebel GD, Speckemeier C, Abels C, Plescher F, Börchers K, Wasem J, et al. Problems and barriers related to the use of digital health applications: scoping review. J Med Internet Res. (2023) 25:e43808. doi: 10.2196/43808
10. Börchers K, Kampka B. Entwicklung einer fortlaufenden Qualitätssicherung digitaler Gesundheitsanwendungen (DiGA): Das Innovationsfonds-Projekt QuaSiApps—(Der Weg zu einem) Qualitätsverständnis, FAQs mit Erläuterungen und Glossar. IBES Diskussionsbeitrag, No. 236. Essen: Universität Duisburg-Essen, Institut für Betriebswirtschaft und Volkswirtschaft (IBES) (2023). Available online at: http://hdl.handle.net/10419/273091 (accessed January 9, 2024).
11. Universität Duisburg-Essen [University Duisburg-Essen]. Fortlaufende Qualitätssicherung von in der GKV-Regelversorgung eingesetzten Gesundheits-Apps (2023). Available online at: https://www.uni-due.de/quasiapps/startseite.php (accessed January 9, 2024).
12. Gemeinsamer Bundesauschuss [Federal Joint Committee]. QuaSiApps—Fortlaufende Qualitätssicherung von in der GKV-Regelversorgung eingesetzten Gesundheits-Apps. (n.d.). Available online at: https://innovationsfonds.g-ba.de/projekte/versorgungsforschung/quasiapps-fortlaufende-qualitaetssicherung-von-in-der-gkv-regelversorgung-eingesetzten-gesundheits-apps.387 (accessed January 9, 2024).
13. Deutsches Institut für Normung e.V. [German Institute für Standardization]. DIN EN ISO 9000: Quality Management Systems - Fundamentals and Vocabulary. Berlin: DIN e.V. (2015).
14. aQua—Institut für angewandte Qualitätsförderung und Forschung im Gesundheitswesen GmbH [Institute for Applied Quality Improvement and Research in Health Care]. Entwicklung eines QS-Verfahrens Mitralklappeneingriffe. Göttingen: aQua (2016). Availabe online at: https://iqtig.org/downloads/berichte/2016/AQUA_Mitralklappeneingriffe_Abschlussbericht_2016-05-19.pdf (accessed January 9, 2024).
15. Koitka C, Roeder N, Hensen P. Ergebnismessung von klinischen behandlungspfaden in internationalen studien: eine systematische literaturanalyse. Gesundheitsökonomie Qualitätsmanagement. (2012) 17(1):33–40. doi: 10.1055/s-0031-1273452
16. Mad P, Johanson T, Guba B, Wild C. Klinische Pfade: Systematischer Review zur Ergebnismessung der Wirksamkeit. HTA-Projektbericht Nr. 16. Wien: Ludwig Boltzmann Institut für Health Technology Assessment (2008). Available online at: https://eprints.aihta.at/801/1/HTA-Projektbericht_016.pdf (accessed January 9, 2024).
17. Lelgemann M, Ollenschläger G. Evidenzbasierte leitlinien und behandlungspfade. Ergänzung oder widerspruch? Internist. (2006) 47(7):690–692-697. doi: 10.1007/s00108-006-1652-5
18. Giebel GD, Abels C, Plescher F, Speckemeier C, Schrader N, Börchers K, et al. Problems and barriers related to the use of mHealth apps from the perspective of patients: a focus group and interview study. J Med Internet Res. (2024). doi: 10.2196/49982
19. Kuhn E, Rogge A, Schreyer KF, Buyx A. Apps auf rezept in der arztpraxis, aber wie? Fallbasierter problemaufriss medizinethischer implikationen bei der nutzung von DiGA. Gesundheitswesen. (2022) 84(8/9):696–700. doi: 10.1055/a-1473-5655
20. Beauchamp TL, Childress JF. Principles of Biomedical Ethics. Eighth ed. New York: Oxford University Press (2019). ISBN: 978-0-19-064087-3.
21. Bundesärztekammer [German Medical Association]. (Muster-)Berufsordnung für die in Deutschland tätigen Ärztinnen und Ärzte—MBO-Ä 1997—* in der Fassung des Beschlusses des 124. Deutschen Ärztetages vom 5. Berlin: BÄK (2021). Available online at: https://www.bundesaerztekammer.de/fileadmin/user_upload/_old-files/downloads/pdf-Ordner/Recht/_Bek_BAEK_MBO-AE_Online_final.pdf (accessed January 9, 2024).
22. Scheer AW, Thomas O, Adam O. Process modeling using event-driven process chains. In: Dumas M, van der Aalst WMP, ter Hofstede AHM, editors. Process-Aware Information Systems: Bridging People and Software through Process Technology. Hoboken, New Jersey: John Wiley & Sons, Inc (2005). p. 119–45. doi: 10.1002/0471741442
23. Lucid Software Inc. LucidChart. (n.d.). Available online at: https://www.lucidchart.com (accessed February 14, 2014).
24. Geier AS. Digital health applications (DiGA) on the road to success-the perspective of the German digital healthcare association. Bundesgesundheitsblatt. (2021) 64(10):1228–31. doi: 10.1007/s00103-021-03419-5
25. Haserück A, Lau T. Digitalisierung: medizinische apps in die versorgung integrieren. Deutsches Ärzteblatt. (2023) 120(23):A-1014/B-873. Available online at: https://www.aerzteblatt.de/pdf.asp?id=231932 (accessed March 07, 2024).
26. Sauermann S, Herzberg J, Burkert S, Habetha S. DiGA—a chance for the German healthcare system. J Eur CME. (2022) 11(1):1–4. doi: 10.1080/21614083.2021.2014047
27. Schelling P. Digitale Gesundheitsanwendungen: Hinweise und Empfehlungen zur Haftungsvermeidung für Ärzte und Psychotherapeuten. München: Kassenärztliche Vereinigung Bayern (2021). Available online at: https://www.kvb.de/fileadmin/kvb/Mitglieder/Praxisfuehrung/Praxis-IT/KVB-Infoblatt-DIGAs-Haftungshinweise.pdf (accessed January 9, 2024).
28. Brönneke JB, Debatin JF, Hagen J, Kircher P, Matthies H. DiGA VADEMECUM. Was man zu Digitalen Gesundheitsanwendungen wissen muss. Berlin: Medizinisch Wissenschaftliche Verlagsgesellschaft (2020). ISBN: 978-3-95466-569-3.
29. Brönneke JB, Debatin JF, Hagen J, Kircher P, Matthies H. DiGA VADEMECUM. How to Launch Digital Health Apps in the German Healthcare System. Berlin: Medizinisch Wissenschaftliche Verlagsgesellschaft (2020). ISBN: 978-3-95466-614-0.
30. Schulze A. Digitale Gesundheitsanwendungen-Verordnung (DiGAV): Was Hersteller wissen sollten (2022). Available online at: https://www.johner-institut.de/blog/gesundheitswesen/digitale-gesundheitsanwendungen-verordnung-digav/ (accessed January 9, 2024).
31. Techniker Krankenkasse. DiGA-Report 2022. Hamburg: Techniker Krankenkasse (2022). Available online at: https://www.tk.de/resource/blob/2125136/dd3d3dbafcfaef0984dcf8576b1d7713/tk-diga-report-2022-data.pdf (accessed January 9, 2024).
32. Dahlhausen F, Zinner M, Bieske L, Ehlers JP, Boehme P, Fehring L. Physicians’ attitudes toward prescribable mHealth apps and implications for adoption in Germany: mixed methods study. JMIR Mhealth Uhealth. (2021) 9(11):e33012. doi: 10.2196/33012
33. Frey S, Kerkemeyer L. Acceptance of digital health applications in non-pharmacological therapies in German statutory healthcare system: results of an online survey. Digital Health. (2022) 8:1–10. doi: 10.1177/20552076221131142
34. Bundesgesundheitsministerium [Federal Ministry of Health]. Digital-Gesetz (DigiG). (2024). Available online at: https://www.bundesgesundheitsministerium.de/service/gesetze-und-verordnungen/detail/digital-gesetz.html (accessed February 19, 2024).
35. Deutsche Psychotherapeuten Vereinigung [German Psychotherapists Association]. Noch offene Fragen zu Wirksamkeit. Berlin: Datenschutz, Verordnung von DiGA (2020). Available online at: https://www.dptv.de/aktuelles/meldung/noch-offene-fragen-zu-wirksamkeit-datenschutz-verordnung-von-diga/ (accessed March 07, 2024).
36. Deutsche Diabetes Gesellschaft e.V. [German Diabetes Society]. Digital Health und Diabetologie 2022: DDG legt ein Update ihres Code of Conduct vor. (2022). Available online at: https://www.ddg.info/diabetes-zeitung/ddg-05/2022/digital-health-und-diabetologie-2022 (accessed January 9, 2024).
37. Berufsverband für Orthopädie und Unfallchirurgie. DiGA [Professional Association for Orthopedics and Trauma Surgery]: Digitalisierung ja—aber für alle (2021). Available online at: https://www.bvou.net/digitalisierung-ja-aber-fuer-alle/ (accessed January 9, 2024).
38. Heidel A, Hagist C, Spinler S, Schoeneberger M. Removing dust from the German health care system by introducing health apps into standard care: semistructured interview study. JMIR Hum Factors. (2023) 10:e42186. doi: 10.2196/42186
39. Spitzenverband Bund der Krankenkassen [National Association of Statutory Health Insurance Funds]. Fokus: digitale gesundheitsanwendungen (DiGA) (2023). Available online at: https://www.gkv-spitzenverband.de/gkv_spitzenverband/presse/fokus/fokus_diga.jsp (accessed January 9, 2024).
Keywords: digital health application, DHA, Digitale Gesundheitsanwendungen, DiGA, care path, mHealth, mobile app
Citation: Giebel GD, Abels C, Börchers K, Kampka B, Neusser S, Cissarek HR, Plescher F, Wasem J and Blase N (2024) Integration of digital health applications into the German healthcare system: development of “The DiGA-Care Path”. Front. Health Serv. 4:1372522. doi: 10.3389/frhs.2024.1372522
Received: 18 January 2024; Accepted: 27 February 2024;
Published: 13 March 2024.
Edited by:
Tom Schaal, West Saxon University of Applied Sciences of Zwickau, GermanyReviewed by:
Hajo Zeeb, Leibniz Institute for Prevention Research and Epidemiology (LG), Germany© 2024 Giebel, Abels, Börchers, Kampka, Neusser, Cissarek, Plescher, Wasem and Blase. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: G. D. Giebel Z29kd2luLmdpZWJlbEBtZWRtYW4udW5pLWR1ZS5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.