
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Health Serv. , 05 July 2024
Sec. Implementation Science
Volume 4 - 2024 | https://doi.org/10.3389/frhs.2024.1326777
 Robert E. Brady1,2*
Robert E. Brady1,2* Kathleen D. Lyons3Courtney J. Stevens1,2Cassandra M. Godzik1,2Andrew J. Smith1,2,4Pamela J. Bagley5
Kathleen D. Lyons3Courtney J. Stevens1,2Cassandra M. Godzik1,2Andrew J. Smith1,2,4Pamela J. Bagley5 Elaina J. Vitale5Steven L. Bernstein2,6
Elaina J. Vitale5Steven L. Bernstein2,6
Background: Rural healthcare has unique characteristics that affect the dissemination and implementation of evidence-based interventions. Numerous theories, models, and frameworks have been developed to guide implementation of healthcare interventions, though not specific to rural healthcare. The present scoping review sought to identify the theories, models, and frameworks most frequently applied to rural health and propose an approach to rural health research that harnesses selected constructs from these theories, models, and frameworks. This resulting synthesis can serve as a guide to researchers, policy makers, and clinicians seeking to employ commonly used theories, models, and frameworks to rural health.
Methods: We used the Scopus abstract indexing service to identify peer-reviewed literature citing one or more of theories, models, or frameworks used in dissemination and implementation research and including the word “rural” in the Title, Abstract, or Keywords. We screened the remaining titles and abstracts to ensure articles met additional inclusion criteria. We conducted a full review of the resulting 172 articles to ensure they identified one or more discrete theory, model, or framework applied to research or quality improvement projects. We extracted the theories, models, and frameworks and categorized these as process models, determinant frameworks, classic theories, or evaluation frameworks.
Results: We retained 61 articles of which 28 used RE-AIM, 11 used Community-Based Participatory Research (CBPR) framework, eight used the Consolidated Framework for Implementation Research (CFIR), and six used the integrated-Promoting Action on Research Implementation in Health Services (iPARIHS). Additional theories, models, and frameworks were cited in three or fewer reports in the literature. The 14 theories, models, and frameworks cited in the literature were categorized as seven process models, four determinant frameworks, one evaluation framework, and one classic theory.
Conclusions: The RE-AIM framework was the most frequently cited framework in the rural health literature, followed by CBPR, CFIR, and iPARIHS. A notable advantage of RE-AIM in rural healthcare settings is the focus on reach as a specified outcome, given the challenges of engaging a geographically diffuse and often isolated population. We present a rationale for combining the strengths of these theories, models, and frameworks to guide a research agenda specific to rural healthcare research.
Systematic Review Registration: https://osf.io/fn2cd/.
Rural settings are characterized by features such as low population density and geographic isolation (1). The population of people living in rural settings in the United States experience worsened health outcomes compared to densely populated urban settings (2). The causes of these disparities are numerous and complexly intertwined, leading to what has been termed the “rural mortality penalty.” (3) For example, many rural settings have less access to primary and specialty medical care, increased travel time for urgent and emergency care, and more workforce shortages than urban settings (4–6). As such, disseminating and implementing evidence-based healthcare practices and policies into rural settings includes unique challenges across a range of contextual variables (7).
Implementation science has the potential to address the challenges of healthcare delivery in rural settings (8). Among the most significant developments from this young but rapidly maturing field is the development and refinement of dissemination (i.e., spreading knowledge of an innovation or intervention) and implementation (i.e., getting the innovation or intervention into routine practice) theories, models, and frameworks used to guide the design, implementation, and evaluation of evidence-based interventions. The definitions of theories, models, and frameworks and their distinctions within dissemination and implementation research was most effectively provided by Nilsen (9). In brief, theories seek to explain observed phenomena, models seek to simplify otherwise complex observed or predicted phenomena, and frameworks seek to establish a structure for the relation between components of those phenomena. There are currently at least 110 published theories, models, and frameworks (10), expanded from the seminal paper by Tabak and colleagues that identified 61 such theories, models, and frameworks (11). Together, these compilations provide a convenient source for identifying and selecting theories, models, and frameworks that can guide implementation, determination of factors that can influence implementation, or evaluation and interpretation of implementation outcomes (9).
Our overarching research goal is to improve understanding of implementation methods and approaches in rural healthcare to support the development of a strategic and cohesive approach to conducting evidence-based healthcare throughout rural-based healthcare delivery systems. Our first step in this process was to conduct a scoping review of healthcare dissemination and implementation studies occurring in rural settings. Scoping reviews are appropriate for providing an overview of a topic (e.g., what do we know about implementing evidence-based practices in rural settings?), as opposed to answering a tightly worded clinical question (e.g., is palliative care effective for rural-dwelling patients recently diagnosed with advanced cancer?) (12). The results of this scoping review will inform model development for the integration of research and practice within rural academic medical systems.
The specific aim of this scoping review is to characterize the theories, models, and frameworks used in rural healthcare research and quality improvement including the frequency and type of theory, model, or framework that have been applied in rural settings to support the development of a strategic and cohesive approach to conducting evidence-based healthcare throughout rural-based healthcare delivery systems. We limited this review to research that examines evidence-based medical interventions implemented and delivered within rural settings, including in the context of quality improvement initiatives. Thus, the review does not include those studies that would examine themes and constructs considered preparatory for research, such as formative evaluations, case studies of interventions, and observational studies examining a clinical phenomenon (e.g., survey designs and secondary data analyses).
We used the steps recommended by Arksey and O'Malley for conducting scoping reviews. We pilot tested the search strategy and operationalization of the eligibility criteria prior to conducting the full search (13). The steps of the scoping review were as follows: (1) specify the research question(s), (2) identify the relevant studies, (3) select studies using predetermined inclusion/exclusion criteria, (4) extract data, and (5) synthesize and report the results. Our protocol was registered in the Open Science Forum prior to extracting data (https://osf.io/fn2cd). We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews Checklist to ensure best practices in this review (See Supplementary File S1).
Given the overarching goal of improving understanding of implementation methods and approaches in rural healthcare, we focused on this broad question for the present scoping review: What dissemination and implementation theories, models, and frameworks are used in rural healthcare research?
We partnered with librarians at our institution to create a rigorous search strategy. The librarians first identified the primary citations for each of the 110 theories, models, and frameworks catalogued on the Dissemination and Implementation Models in Health website (www.dissemination-implementation.org) (10). The librarians constructed a search string within the Scopus (Elsevier) database for all sources citing these articles using the REFTITLE field. To focus on rural settings, they searched Scopus, a large interdisciplinary database that includes records from Medline and EMBASE, for the term “rural” in the TITLE, ABSTRACT, or KEYWORD fields and combine these results with the sources citing dissemination and implementation theories, models, and frameworks. This created a citation list consisting of all articles published between 2022 and 1998, the latter being a proposed initial date of formal implementation science research coinciding with the formation of Quality Enhancement Research Initiative (QUERI). This search strategy yielded 1,677 publications. The search was conducted on February 2, 2022. The complete search strategy is available in Supplementary File S2. The publications were loaded into the Covidence software program to manage the screening and extraction process (14).
We used the following inclusion criteria:
1) Presents data (qualitative or quantitative) from a trial of an intervention or quality improvement effort to improve delivery of an intervention within the physical medicine, mental health, or pharmacy literature. Rationale: For study protocol publications that meet this criterion, we searched for available outcomes papers for inclusion. We determined this a priori based on the observation that many protocol papers specify a theory, model, or framework to be used in the study, but do not necessarily report this in the outcomes paper. Protocol papers that did not have a corresponding outcomes paper were removed prior to data extraction. Additionally, we used a broad definition of healthcare settings for this review to reflect the variability of settings in which healthcare is delivered in rural communities. We included studies or projects in which an intervention was delivered for the explicit purpose of modifying a health outcome regardless of the regular use physical location (e.g., community resource centers, churches, schools) within the physical medicine, mental health, or pharmacy domains. This also included traditional healthcare settings such as community health centers and rural hospitals.
2) Reports the use of a discrete theory, model, or framework included in the Dissemination and Implementation Models in Health registry. Rationale: Because our goal is to develop or tailor a model that will guide our research and practice, we sought articles that explicitly locate themselves within implementation science and use a theory, model, or framework to guide their study or quality improvement design.
3) Includes the word “rural” in the title or abstract or author keywords. Rationale: There are many operational definitions of rurality and many studies inconsistently report their definition of rurality. We chose to be inclusive, and included any study where the authors identify their setting or population as rural within the title, abstract, or keywords.
4) Reports on data collected within the United States and published in English. Rationale: We recognize that many high-quality studies occur outside the United States, but also that the U.S. population represents a broad range of cultural, healthcare, and demographic variables that make it unique relative to much of the world. Additionally, studies situated in low- and middle-income countries have infrastructure and cultural expectations that result in conclusions less germane to the approaches used in this system.
5) Published after 1998, coinciding with the initiation of the QUERI. Rationale: Although dissemination and implementation theories, models, and frameworks existed before this date, the initiation of QUERI was selected as an early point of formal research on the dissemination and implementation of interventions in healthcare specifically (15).
The study team conducted an initial pilot test of the review method using a sample of 50 randomly selected citations prior to the full review. The pilot search verified that the search terms applied to the specified databases were yielding the expected articles, namely those identifying research citing dissemination and implementation theories, models, or frameworks applied to rural health research. This also provided a training set for the study abstract screening process. A team of four reviewers (RB, CS, CG, AS) screened each citation to eliminate articles that did not meet the inclusion criteria. The first stage of screening utilized the title and abstract and the second stage of screening utilized the full text of each article. In both stages, each citation was screened by two independent screeners unaware of the other screener's vote for inclusion or exclusion of the citation. A third screener (RB or KL) provided a tie-breaking vote reviewed for citations with conflicting votes for inclusion or exclusion. For articles where it was unclear whether the authors applied a theory, model, or framework to the design or execution of the study, the first author (RB) contacted the corresponding author for confirmation. A full report of these data is presented in Figure 1.
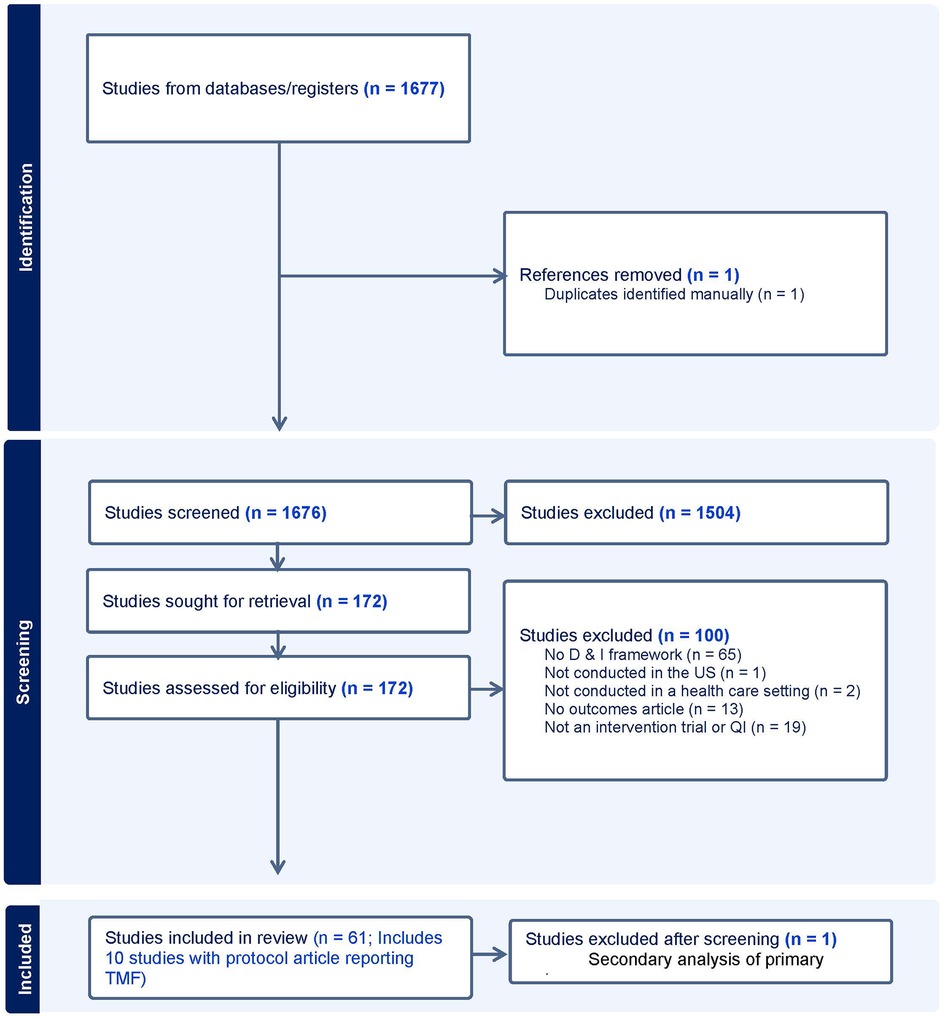
Figure 1 Flow diagram of search strategy and article selection.
We constructed a data extraction matrix in Covidence to chart and sort the data (14). The matrix included basic information about each study (author, year, title, and publication date) and the theory, model, or framework used in the study. Extraction was completed by two team members per study. Pairs met after initial extraction to resolve disagreements in a consensus process moderated by the first author (RB).
We calculated the frequencies of each theory, model, or framework and categorized the year of publication by decade. Using the definitions posed by Nilsen, we then categorized each as a (a) classic theory (i.e., theories that originate outside of implementation science specifically, but are used to understand implementation processes), (b) process model (i.e., that guide or describe the how evidence is translated into practice) (c) determinants framework or theory (i.e., explain factors that influence implementation) or (d) evaluation framework (i.e., guide the measurement of implementation outcomes) (9).
A total of 1,683 candidate publications were identified from the search strategy. The study team completed a title and abstract screening process that resulted in the exclusion of 1,508 publications that failed to meet inclusion criteria. Data collected outside of the United States was the most frequent reason for exclusion. The full text review excluded an additional 100 articles that did not meet eligibility criteria, including four in which the corresponding author confirmed that a cited theory, model, or framework was not actually applied to the design or conduct of the trial. Of the remaining 72 articles, 10 were protocol articles for which there was an outcomes article signifying that the study had be conducted. For review and charting purposes, these studies were combined with the outcomes article such that if the protocol paper described the theory, model, or framework used, but the outcomes article did not, it was still identified as used for the purpose of the study reported in the outcomes article. One article by Zoellner and colleagues provided an additional analysis of a single trial, which was subsequently removed to reduce inflation of the corresponding framework's use, leaving a final sample of 61 articles. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram depicts our study selection process in Figure 1 (16). All citations for the included articles are provided in Table 1.
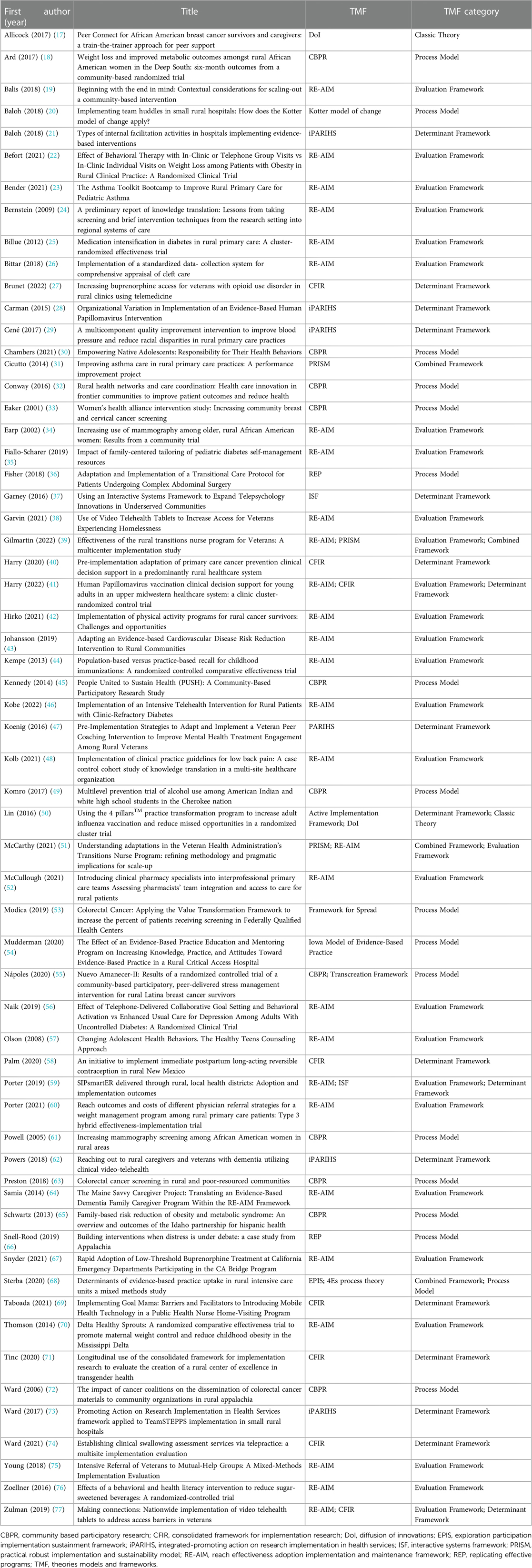
Table 1 Characteristics of included studies.
The 61 publications that were ultimately included in this scoping review depict a wide range of designs, including randomized and quasi-experimental clinical trials and quality improvement projects. All studies depicted efforts to implement or disseminate a healthcare intervention targeting physical health (n = 52) or mental health (including substance use) (n = 9). Publication dates ranged from 1998 to 2022, consistent with our use of the creation of QUERI as a start date for formal implementation research. We were unable to identify any publications from 1998 to 1999. Six studies were published in the 2000s, with the first study published in 2001. Thirty-three studies were published between 2010 and 2019, with the remaining 22 published since 2020.
Because our search strategy began with identifying articles that cited at least one validated and published implementation or dissemination theory, model, or framework, all publications included at least one theory, model, or framework. Some publications not included in the final review cited a theory, model, or framework, but did not indicate its use in the design, execution, or evaluation of outcomes. For example, several studies referenced a theory, model, or framework in the discussion section when describing a future direction of study. Those articles that did not indicate that the theory, model, or framework was used in the design or execution of the research or quality improvement or evaluation of its outcomes were excluded. Although RE-AIM and the Practical, Robust Implementation and Sustainability Model (78) (PRISM) are derived from the same underlying theory and are frequently used in tandem as partner frameworks where PRISM uses the outcomes outlined by RE-AIM, we examined the use of these frameworks separately in the literature to understand better how they are applied to the rural healthcare setting.
The most commonly used theories, models, and frameworks in the scope of this review were RE-AIM (79) (n = 28) and Community-Based Participatory Research framework (CBPR) (80) (n = 11). Less frequently cited were the integrated-Promoting Action on Research Implementation in Health Services (iPARIHS) (81) (n = 6) and Consolidated Framework for Implementation Research (CFIR) (82) (n = 8). PRISM was cited three times, either independently or in concert with RE-AIM. The Interactive Systems Framework (83), Replicating Effective Programs framework (84), and Diffusion of Innovations (85) were each cited two times. The remaining cited theories, models, and frameworks appeared once in the reviewed literature, including the Iowa Model of Evidence-Based Practice (86), Active Implementation Framework (87), Framework for Spread (88), 4Es Process Theory (89), and Exploration, Preparation, Implementation, Sustainment (EPIS) framework (90). The Kotter Model of Change (91) was not included in the larger collection of theories, models, and frameworks, but is relevant to rural health implementation and was included for its single citation. The use of each theory, model, or framework is presented in Table 1.
We categorized the 14 theories, models, and frameworks identified in this review according to the conventions outlined by Nilsen (9). This resulted in categorization of seven process models (CBPR, Iowa Model of Evidence-Based Practice, Replicating Effective Programs, Transcreation Framework, 4Es process theory, Framework for Spread, and Kotter Model of Change), four determinant frameworks (CFIR, iPARIHS, Interactive Systems Framework, and Active Implementation Framework), one classic theory (Diffusion of Innovations), and one evaluation framework (RE-AIM). Because the PRISM model is informed by elements from the IHI Model for Improvement, iPARIHS framework, and RE-AIM framework (78) and the EPIS framework includes elements of process and determinant frameworks (92) and do not clearly fit within a single category, we denoted an additional category of “combined” occurring four times. Category labels are included per citation in Table 1. The total frequency and citations per theory, model, or framework category are summarized in Table 2.
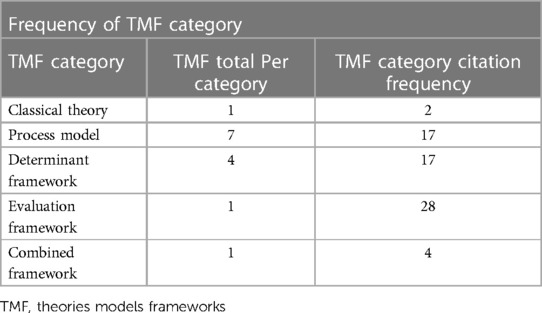
Table 2 Frequency of theories, models, and frameworks by nilsen categories.
Finally, we assessed the number of theories, models, and frameworks used in each report. No citation reported using more than two and the majority (87%) cited a single theory, model, or framework. Among the theories, models, and frameworks used alongside another, RE-AIM was cited most, occurring in five of eight instances, alongside CFIR (2), PRISM (2), and ISF (1). The other reports used CBPR and the Transcreation Framework, EPIS and the 4Es process theory, or the Active Implementation Framework and Diffusion of Innovations.
The specific aim of this scoping review was to identify the leading dissemination and implementation theories, models, and frameworks used to assess the impact of medical, psychosocial, and pharmacologic interventions in rural healthcare in the U.S, with the larger goal of advancing a research agenda that harnesses the leading implementation theories, models, and frameworks to guide efforts to improve the health and well-being of rural populations, where disparities in health outcomes and research remain present despite the growth of rural health as a focus of public policy (93).
The overwhelming majority of studies identified in this review specified use of RE-AIM (79) as the chosen framework to guide selection of outcomes. This is consistent with its overall prominence as a guiding framework for implementation and dissemination outcomes in healthcare research and delivery. Its frequent appearance in the reviewed literature likely reflects the premium placed on the identification of implementation outcomes in the larger dissemination and implementation research domain. Within the rural healthcare research domain, like other healthcare areas, RE-AIM has a particularly robust role in evaluating whether an intervention supported by implementation strategies achieves greater reach and adoption among rural healthcare facilities.
PRISM (78) was used in tandem with RE-AIM to aid in the determination of strategies to improve key implementation outcomes such as sustainment, but in relatively few studies, suggesting greater emphasis on the use of RE-AIM for defining outcomes. The specification of outcomes may also drive overall implementation, as attention to outcomes necessitates use of approaches and strategies focused on achieving those same outcomes. Given that reach among rural people is a specific challenge of rural health implementation, prioritizing the reach outcome from RE-AIM may be an optimal use of that framework. This does not suggest that the other domains within RE-AIM are irrelevant to rural health, but rather that emphasizing reach given the recognized difficulties getting into these populations has particular importance for advancing rural health.
The frequent appearance of CBPR (80) in the studies included in this review is expected given that research teams developing and evaluating interventions for deployment in rural settings are often not co-located in these communities. As a process model useful in rural health, CBPR has relevance in increasing engagement in the innovation and evaluation in a research context. Indeed, many clinical trials are at least initially launched by academic institutions that are not deeply engaged with the rural community structure, which then may hesitate to make substantive changes to settings (e.g., modifying clinical infrastructure) with their own culture and way of delivering care. Prioritizing the use of CBPR as a guiding framework for rural health research may lead to greater frequency of academic-community partnerships and facilitate these potentially meaningful changes in rural healthcare delivery. Thus, our approach will emphasize engagement with the community to increase the salience and fit of the research performed in these settings.
The CFIR (82) and iPARIHS (81) frameworks were less frequently cited, but were used effectively in the studies that employed them as determinant frameworks. The primary use of CFIR was determination of the facilitators and barriers to implementation as an initial step in the development and evaluation of the intervention to be tested. iPARIHS was used more diversely, including as an evaluation framework of outcomes or process, and as a guiding framework for the steps of implementation, with an emphasis on how the intervention could be best facilitated. PRISM has been identified as a determinant framework in prior work as well, where its emphasis on context as a means of identifying contextual influences on implementation success and approach (94). The uses of these frameworks in the reviewed literature is largely consistent with their use in research beyond the rural scope.
The synthesis of the research included in this review suggests that a research agenda that integrates the contributions of the RE-AIM framework couched within a CBPR approach to engagement and implementation process and informed by elements of the CFIR and i-PARIHS frameworks is ideal for development, evaluation, implementation, and dissemination of interventions targeting rural health. Specifically, our review pointed to the (1) need to begin with a CFIR-based analysis of facilitators and barriers, (2) identify implementation outcomes aligned with RE-AIM, and (3) develop and evaluate facilitation efforts consistent with the iPARIHS framework. All of these research practices are determined in consultation with rural community stakeholders to ensure contextual fit in line with the CBPR approach. We also prioritized the external environment and implementation and sustainability infrastructure domains of the PRISM framework to ensure sustainability from the financial, regulatory, and practical infrastructure perspectives. This is an intentional integration of selected components of these leading frameworks to form a research agenda rather than an explicit adherence to any one framework and is open to improvements and modification at later points in the research process.
Although the approach described here could also be applied to urban healthcare settings, it may have specific utility for the rural setting. Several examples from the reviewed literature highlight the importance of identifying barriers to effective implementation such as geographic isolation and distance from healthcare centers and meeting those challenges with telehealth and other forms of remote care. Others noted the importance of engaging communities using a CBPR approach given the outsider status of large healthcare systems that are not inherently within the rural community. Finally, as previously mentioned, the emphasis on reach within the underserved rural setting contributed to utilization of lay providers and other nontraditional care providers to enhance engagement with the target populations. Thus, these frameworks and their selected domains may help to identify lines of investigation specific to the rural health setting.
An additional notable observation from this scoping review was the tendency for some studies to reference a theory, model, or framework at some point in the article, but to never specify its use in the design, execution, or evaluation of the research. This occurred most often in the context of describing future directions for the research program or when situating the research within a larger body of literature focused on one or more theories, models, and frameworks. The importance of clearly specifying a theory, model, or framework is analogous to the recommendation of Proctor et al. to name, define, and operationalize implementation strategies used in dissemination and implementation research (95). As noted by those authors, the absence of specification of implementation strategies contributes to the “Tower of Babel” phenomenon in implementation science, meaning that inconsistent use and operationalization of terminology leads to confusion in the field. That confusion functions as a barrier to progress in implementation science including in understanding of the application of its own theories, models, and frameworks (96).
A failure to adequately specify theories, models, and frameworks similarly hampers efforts to improve understanding of what works in implementation science. Research teams would do well to similarly specify the theory, model, or framework used in the research process by naming it, ideally with primary source citation, and describing how it was used, particularly at the phase of research where it was applied (e.g., designing, executing, or evaluating). Such reporting could also clearly articulate which elements of a given theory, models, or framework were most emphasized, or alternatively, which elements were excluded from the work. As described in the method used for this review, we included several studies where a given theory, model, or framework was not specified in the final outcomes report, but was included in the protocol paper. This likely reflects the study teams’ tendency to apply a theory, model, or framework in the initial planning phases of the research, but not to subsequently specify and describe its use in the later work.
This scoping review relied on authors’ reporting of dissemination and implementation theories, models, and frameworks for inclusion in the reviewed literature. A well-known deficit in the clinical trials and quality improvement literature is the inconsistent specification and reporting of theories, models, and frameworks (7). Therefore, this review likely does not include many studies that used one or more theory, model, or framework but did not specifically acknowledge or cite it. As previously noted, a recommendation based on this limitation is that implementation scientists more clearly specify their use of theories, models, and frameworks in methods sections, as well as how they are used and operationalized, similar to prior recommendations to specify implementation strategies (95).
Additionally, our review focused only on trials and practical implementation studies (e.g., quality improvement projects) of healthcare interventions, seeking to understand the use of theories, models, and frameworks specific to research evaluating and implementing healthcare interventions. Thus, we did not include in our review the many studies aimed at better understanding the barriers that might exist to implementing an intervention. Much of this research consists of formative evaluation that may effectively use theories, models, and frameworks to guide identification of various barriers and facilitators and subsequent modifications to the intervention. Those studies do not depict the actual deployment and evaluation of the intervention approach itself, which was the focus of this review. A subsequent review may effectively scope and summarize the formative research that is critical to advancing healthcare.
The proliferation of theories, models, and frameworks in implementation science presents numerous choices for consideration when designing research trials and quality improvement initiatives aimed at improving rural health outcomes. This review sought to examine the scope of these options and determine which theories, models, and frameworks were most prominent for developing a research agenda specific to dissemination and implementation research and practice in rural health.
From this scoping review, we specifically identified RE-AIM as the primary framework for evaluating outcomes in rural healthcare implementation research, which is consistent with the broader field. CBPR represented a particularly applicable framework for conducting healthcare implementation research in rural settings. Given its explicit focus on effectively engaging communities as partners in the research process, CBPR would likely increase the buy-in of participants and thus the generalizability of findings and overcome the tendency for research teams to “parachute in” to communities with which they are usually disconnected. CFIR and iPARIHS were recognized as the leading frameworks for the identification of determinants of implementation and opportunities to improve facilitation of implementation, respectively.
Accordingly, we concluded that a combination of the strengths drawn from RE-AIM (79), CBPR (80), iPARIHS (81), CFIR (82) has the potential to inform an approach for structuring implementation research in rural communities based on the available evidence for their utility in a variety of relevant dissemination and implementation work performed over nearly four decades of research.
The original contributions presented in the study are included in the article/Supplementary Materials, further inquiries can be directed to the corresponding author.
RB: Conceptualization, Formal Analysis, Investigation, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing. KL: Conceptualization, Formal Analysis, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. CS: Data curation, Formal Analysis, Investigation, Writing – review & editing. CG: Formal Analysis, Investigation, Writing – review & editing. AS: Formal Analysis, Investigation, Writing – review & editing. PB: Data curation, Writing – review & editing. EV: Data curation, Writing – review & editing. SB: Conceptualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This work was supported by the National Institute of Mental Health [K23MH116367 to RB], National Cancer Institute [K08CA259632 to CS and R01CA225792 to KL] and Health Resources and Services Administration [HRSA T32HP32520 for CG and U3M45388 for AS].
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frhs.2024.1326777/full#supplementary-material
1. Economic Research Service. What is rural? U.S. Department of Agriculture. Updated October 23, 2019. Available online at: https://www.ers.usda.gov/topics/rural-economy-population/rural-classifications/what-is-rural/
2. Garcia MC, Rossen LM, Bastian B, Faul M, Dowling NF, Thomas CC, et al. Potentially excess deaths from the five leading causes of death in metropolitan and nonmetropolitan counties—United States, 2010–2017. MMWR Surveill Summ. (2019) 68(10):1–11. doi: 10.15585/mmwr.ss6810a1
3. James WL. All rural places are not created equal: revisiting the rural mortality penalty in the United States. Am J Public Health. (2014) 104(11):2122–9. doi: 10.2105/ajph.2014.301989
4. Kozhimannil KB, Henning-Smith C. Improving health among rural residents in the US. JAMA. (2021) 325(11):1033–4. doi: 10.1001/JAMA.2020.26372
5. Chan L, Hart LG, Goodman DC. Geographic access to health care for rural medicare beneficiaries. J Rural Health. (2006) 22(2):140–6. doi: 10.1111/j.1748-0361.2006.00022.x
6. Litaker D, Koroukian SM, Love TE. Context and healthcare access: looking beyond the individual. Med Care. (2005) 43(6):531–40. doi: 10.1097/01.mlr.0000163642.88413.58
7. Wong Shee A, Quilliam C, Corboy D, Glenister K, McKinstry C, Beauchamp A, et al. What shapes research and research capacity building in rural health services? Context matters. Aust J Rural Health. (2022) 30(3):410–21. doi: 10.1111/ajr.12852
8. Afifi RA, Parker EA, Dino G, Hall DM, Ulin B. Reimagining rural: shifting paradigms about health and well-being in the rural United States. Annu Rev Public Health. (2022) 43:135–54. doi: 10.1146/annurev-publhealth-052020-123413
9. Nilsen P. Making sense of implementation theories, models and frameworks. Implement Sci. (2015) 10:53. doi: 10.1186/s13012-015-0242-0
10. Dissemination and Implementation Models in Health: An Interactive Webtool to Help You Use D&I Models. Available online at: https://dissemination-implementation.org/ (accessed June 21, 2021).
11. Tabak RG, Khoong EC, Chambers DA, Brownson RC. Bridging research and practice: models for dissemination and implementation research. Am J Prev Med. (2012) 43(3):337–50. doi: 10.1016/J.AMEPRE.2012.05.024
12. Munn Z, Peters MDJ, Stern C, Tufanaru C, McArthur A, Aromataris E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. (2018) 18(1):143. doi: 10.1186/s12874-018-0611-x
13. Arksey H, O'Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8(1):19–32. doi: 10.1080/1364557032000119616
14. Covidence systematic review software. Veritas Health Innovation. (2021). Available online at: www.covidence.org
15. Demakis JG, McQueen L, Kizer KW, Feussner JR. Quality enhancement research initiative (QUERI): a collaboration between research and clinical practice. Med Care. (2000) 38(6 Suppl 1):I17–25. doi: 10.1097/00005650-200006001-00003
16. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
17. Allicock M, Haynes-Maslow L, Johnson LS, Carpenter WR, Vines AI, Belle DG, et al. Peer connect for African American breast cancer survivors and caregivers: a train-the-trainer approach for peer support. Transl Behav Med. (2017) 7(3):495–505. doi: 10.1007/s13142-017-0490-4
18. Ard JD, Carson TL, Shikany JM, Li Y, Hardy CM, Robinson JC, et al. Weight loss and improved metabolic outcomes amongst rural African American women in the deep south: six-month outcomes from a community-based randomized trial. J Intern Med. (2017) 282(1):102–13. doi: 10.1111/joim.12622
19. Balis LE, Strayer TE III, Ramalingam N, Harden SM. Beginning with the end in mind: contextual considerations for scaling-out a community-based intervention. Front Public Health. (2018) 6(December). doi: 10.3389/fpubh.2018.00357
20. Baloh J, Zhu X, Ward MM. Implementing team huddles in small rural hospitals: how does the kotter model of change apply? J Nurs Manage. (2018) 26(5):571–8. doi: 10.1111/jonm.12584
21. Baloh J, Zhu X, Ward MM. Types of internal facilitation activities in hospitals implementing evidence-based interventions. Health Care Manage Rev. (2018) 43(3):229–37. doi: 10.1097/HMR.0000000000000145
22. Befort CA, Vanwormer JJ, Desouza C, Ellerbeck EF, Gajewski B, Kimminau KS, et al. Effect of behavioral therapy with in-clinic or telephone group visits vs in-clinic individual visits on weight loss among patients with obesity in rural clinical practice: a randomized clinical trial. JAMA. (2021) 325(4):363–72. doi: 10.1001/jama.2020.25855
23. Bender BG, Simmons B, Konkoly N, Liu AH. The asthma toolkit bootcamp to improve rural primary care for pediatric asthma. J Allergy Clin Immunol Pract. (2021) 9(8):3091–3097.e1. doi: 10.1016/j.jaip.2021.03.058
24. Bernstein E, Topp D, Shaw E, Girard C, Pressman K, Woolcock E, et al. A preliminary report of knowledge translation: lessons from taking screening and brief intervention techniques from the research setting into regional systems of care. Acad Emerg Med. (2009) 16(11):1225–33. doi: 10.1111/j.1553-2712.2009.00516.x
25. Billue KL, Safford MM, Salanitro AH, Houston TK, Curry W, Kim Y, et al. Medication intensification in diabetes in rural primary care: a cluster-randomised effectiveness trial. BMJ Open. (2012) 2(5):e000959. doi: 10.1136/bmjopen-2012-000959
26. Bittar PG, Carlson AR, Mabie-DeRuyter A, Marcus JR, Allori AC. Implementation of a standardized data- collection system for comprehensive appraisal of cleft care. Cleft Palate-Craniofac J. (2018) 55(10):1382–90. doi: 10.1177/1055665618764952
27. Brunet N, Moore DT, Lendvai Wischik D, Mattocks KM, Rosen MI. Increasing buprenorphine access for veterans with opioid use disorder in rural clinics using telemedicine. Subst Abuse. (2022) 43(1):39–46. doi: 10.1080/08897077.2020.1728466
28. Carman AL, McGladrey ML, Goodman Hoover A, Crosby RA. Organizational variation in implementation of an evidence-based human papillomavirus intervention. Am J Prev Med. (2015) 49(2):301–8. doi: 10.1016/j.amepre.2015.03.011
29. Cené CW, Halladay JR, Gizlice Z, Donahue KE, Cummings DM, Hinderliter A, et al. A multicomponent quality improvement intervention to improve blood pressure and reduce racial disparities in rural primary care practices. J Clin Hypertens. (2017) 19(4):351–60. doi: 10.1111/jch.12944
30. Chambers RA, Hautala D, Kenney A, Rosenstock S, Begay M, Neault N, et al. Empowering native adolescents: responsibility for their health behaviors. Am J Health Behav. (2021) 45(1):3–16. doi: 10.5993/AJHB.45.1.1
31. Cicutto L, Dingae MB, Langmack EL. Improving asthma care in rural primary care practices: a performance improvement project. J Cont Educ Health Prof. (2014) 34(4):205–14. doi: 10.1002/chp.21254
32. Conway P, Favet H, Hall L, Uhrich J, Palcher J, Olimb S, et al. Rural health networks and care coordination: health care innovation in frontier communities to improve patient outcomes and reduce health. J Health Care Poor Underserved. (2016) 27(4):91–115. doi: 10.1353/hpu.2016.0181
33. Eaker ED, Jaros L, Vierkant RA, Lantz P, Remington PL. Women’s health alliance intervention study: increasing community breast and cervical cancer screening. J Public Health Manage Pract. (2001) 7(5):20–30. doi: 10.1097/00124784-200107050-00004
34. Earp JA, Eng E, O'Malley MS, Altpeter M, Rauscher G, Mayne L, et al. Increasing use of mammography among older, rural African American women: results from a community trial. Am J Public Health. (2002) 92(4):646–54. doi: 10.2105/AJPH.92.4.646
35. Fiallo-Scharer R, Palta M, Chewning BA, Rajamanickam V, Wysocki T, Wetterneck TB, et al. Impact of family-centered tailoring of pediatric diabetes self-management resources. Pediatr Diabetes. (2019) 20(7):1016–24. doi: 10.1111/pedi.12899
36. Fisher AV, Campbell-Flohr SA, Sell L, Osterhaus E, Acher AW, Leahy-Gross K, et al. Adaptation and implementation of a transitional care protocol for patients undergoing complex abdominal surgery. Jt Comm J Qual Patient Saf. (2018) 44(12):741–50. doi: 10.1016/j.jcjq.2018.05.001
37. Garney WR, McCord CE, Walsh MV, Alaniz AB. Using an interactive systems framework to expand telepsychology innovations in underserved communities. Scientifica (Cairo). (2016):2016. doi: 10.1155/2016/4818053
38. Garvin LA, Hu J, Slightam C, McInnes DK, Zulman DM. Use of video telehealth tablets to increase access for veterans experiencing homelessness. J Gen Intern Med. (2021) 36(8):2274–82. doi: 10.1007/s11606-021-06900-8
39. Gilmartin HM, Warsavage T, Hines A, Leonard C, Kelley L, Wills A, et al. Effectiveness of the rural transitions nurse program for veterans: a multicenter implementation study. J Hosp Med. (2022) 17(3):149–57. doi: 10.1002/jhm.12802
40. Harry ML, Saman DM, Truitt AR, Allen CI, Walton KM, O'Connor PJ, et al. Pre-implementation adaptation of primary care cancer prevention clinical decision support in a predominantly rural healthcare system. BMC Med Informatics Decis Mak. (2020) 20(1). doi: 10.1186/s12911-020-01136-8
41. Harry ML, Asche SE, Freitag LA, Sperl-Hillen JM, Saman DM, Ekstrom HL, et al. Human papillomavirus vaccination clinical decision support for young adults in an upper midwestern healthcare system: a clinic cluster-randomized control trial. Hum Vaccin Immunother. (2022) 18(1):2040933. doi: 10.1080/21645515.2022.2040933
42. Hirko KA, Dorn JM, Dearing JW, Alfano CM, Wigton A, Schmitz KH. Implementation of physical activity programs for rural cancer survivors: challenges and opportunities. Int J Environ Res Public Health. (2021) 18(24):12909. doi: 10.3390/ijerph182412909
43. Johansson P, Schober D, Tutsch SF, Brueggeman G, Leon M, Lyden E, et al. Adapting an evidence-based cardiovascular disease risk reduction intervention to rural communities. J Rural Health. (2019) 35(1):87–96. doi: 10.1111/jrh.12306
44. Kempe A, Saville A, Dickinson LM, Eisert S, Reynolds J, Herrero D, et al. Population-based versus practice-based recall for childhood immunizations: a randomized controlled comparative effectiveness trial. Am J Public Health. (2013) 103(6):1116–23. doi: 10.2105/AJPH.2012.301035
45. Kennedy BM, Katzmarzyk PT, Johnson WD, Johnson GS, McGee BB, Champagne CM, et al. People united to sustain health (PUSH): a community-based participatory research study. Clin Transl Sci. (2014) 7(2):108–14. doi: 10.1111/cts.12133
46. Kobe EA, Lewinski AA, Jeffreys AS, Smith VA, Coffman CJ, Danus SM, et al. Implementation of an intensive telehealth intervention for rural patients with clinic-refractory diabetes. J Gen Intern Med. (2022) 37(12):3080–8. doi: 10.1007/s11606-021-07281-8
47. Koenig CJ, Abraham T, Zamora KA, Hill C, Kelly PA, Uddo M, et al. Pre-implementation strategies to adapt and implement a veteran peer coaching intervention to improve mental health treatment engagement among rural veterans. J Rural Health. (2016) 32(4):418–28. doi: 10.1111/jrh.12201
48. Kolb WH, Bade MJ, Bradberry C. Implementation of clinical practice guidelines for low back pain: a case control cohort study of knowledge translation in a multi-site healthcare organization. J Eval Clin Pract. (2021) 28(2):288–302. doi: 10.1111/jep.13633
49. Komro KA, Livingston MD, Wagenaar AC, Kominsky TK, Pettigrew DW, Garrett BA, et al. Multilevel prevention trial of alcohol use among American Indian and white high school students in the cherokee nation. Am J Public Health. (2017) 107(3):453–9. doi: 10.2105/AJPH.2016.303603
50. Lin CJ, Nowalk MP, Pavlik VN, Brown AE, Zhang S, Raviotta JM, et al. Using the 4 pillars™ practice transformation program to increase adult influenza vaccination and reduce missed opportunities in a randomized cluster trial. BMC Infect Dis. (2016) 16(1). doi: 10.1186/s12879-016-1940-1
51. McCarthy MS, Ujano-De Motta LL, Nunnery MA, Gilmartin H, Kelley L, Wills A, et al. Understanding adaptations in the veteran health administration’s transitions nurse program: refining methodology and pragmatic implications for scale-up. Implement Sci. (2021) 16(1). doi: 10.1186/s13012-021-01126-y
52. McCullough MB, Zogas A, Gillespie C, Kleinberg F, Reisman JI, Ndiwane N, et al. Introducing clinical pharmacy specialists into interprofessional primary care teams: assessing pharmacists’ team integration and access to care for rural patients. Medicine (Baltimore). (2021) 100(38):e26689. doi: 10.1097/MD.0000000000026689
53. Modica C, Lewis JH, Bay C. Colorectal cancer: applying the value transformation framework to increase the percent of patients receiving screening in federally qualified health centers. Prev Med Rep. (2019) 15:15. doi: 10.1016/j.pmedr.2019.100894
54. Mudderman J, Nelson-Brantley HV, Wilson-Sands CL, Brahn P, Graves KL. The effect of an evidence-based practice education and mentoring program on increasing knowledge, practice, and attitudes toward evidence-based practice in a rural critical access hospital. J Nurs Adm. (2020) 50(5):281–6. doi: 10.1097/NNA.0000000000000884
55. Nápoles AM, Santoyo-Olsson J, Stewart AL, Ortiz C, Samayoa C, Torres-Nguyen A, et al. Nuevo amanecer-II: results of a randomized controlled trial of a community-based participatory, peer-delivered stress management intervention for rural Latina breast cancer survivors. Psychooncology. (2020) 29(11):1802–14. doi: 10.1002/pon.5481
56. Naik AD, Hundt NE, Vaughan EM, Petersen NJ, Zeno D, Kunik ME, et al. Effect of telephone-delivered collaborative goal setting and behavioral activation vs enhanced usual care for depression among adults with uncontrolled diabetes: a randomized clinical trial. JAMA Network Open. (2019) 2(8):e198634–e198634. doi: 10.1001/jamanetworkopen.2019.8634
57. Olson AL, Gaffney CA, Lee PW, Starr P. Changing adolescent health behaviors. The healthy teens counseling approach. Am J Prev Med. (2008) 35(5 SUPPL.):S359–64. doi: 10.1016/j.amepre.2008.08.014
58. Palm HC, Degnan JH, Biefeld SD, Reese AL, Espey E, Hofler LG. An initiative to implement immediate postpartum long-acting reversible contraception in rural New Mexico. Am J Obstet Gynecol. (2020) 222(4):S911.e1–.e7. doi: 10.1016/j.ajog.2020.01.027
59. Porter KJ, Brock DJ, Estabrooks PA, Perzynski KM, Hecht ER, Ray P, et al. SIPsmartER delivered through rural, local health districts: adoption and implementation outcomes. BMC Public Health. (2019) 19(1):1273. doi: 10.1186/s12889-019-7567-6
60. Porter G, Michaud TL, Schwab RJ, Hill JL, Estabrooks PA. Reach outcomes and costs of different physician referral strategies for a weight management program among rural primary care patients: type 3 hybrid effectiveness-implementation trial. JMIR Form Res. (2021) 5(10):e28622. doi: 10.2196/28622
61. Powell ME, Carter V, Bonsi E, Johnson G, Williams L, Taylor-Smith L, et al. Increasing mammography screening among African American women in rural areas. J Health Care Poor Underserved. (2005) 16(4 SUPPL. A):11–21. doi: 10.1353/hpu.2005.0071
62. Powers JS, Buckner J. Reaching out to rural caregivers and veterans with dementia utilizing clinical video-telehealth. Geriatrics. (2018) 3(2):29. doi: 10.3390/geriatrics3020029
63. Preston MA, Glover-Collins K, Ross L, Porter A, Bursac Z, Woods D, et al. Colorectal cancer screening in rural and poor-resourced communities. Am J Surg. (2018) 216(2):245–50. doi: 10.1016/j.amjsurg.2017.08.004
64. Samia LW, Aboueissa AEM, Halloran J, Hepburn K. The Maine savvy caregiver project: translating an evidence-based dementia family caregiver program within the RE-AIM framework. J Gerontol Soc Work. (2014) 57(6-7):640–61. doi: 10.1080/01634372.2013.859201
65. Schwartz R, Powell L, Keifer M. Family-based risk reduction of obesity and metabolic syndrome: an overview and outcomes of the Idaho partnership for hispanic health. J Health Care Poor Underserved. (2013) 24(SUPPL.2):129–44. doi: 10.1353/hpu.2013.0106
66. Snell-Rood C, Jenkins R, Hudson K, Frazier C, Noble W, Feltner F. Building interventions when distress is under debate: a case study from appalachia. Transcult Psychiatry. (2019) 56(5):918–46. doi: 10.1177/1363461519833580
67. Snyder H, Kalmin MM, Moulin A, Campbell A, Goodman-Meza D, Padwa H, et al. Rapid adoption of low-threshold buprenorphine treatment at California emergency departments participating in the CA bridge program. Ann Emerg Med. (2021) 78(6):759–72. doi: 10.1016/j.annemergmed.2021.05.024
68. Sterba KR, Johnson EE, Nadig N, Simpson AN, Simpson KN, Goodwin AJ, et al. Determinants of evidence-based practice uptake in rural intensive care units a mixed methods study. Ann Am Thorac Soc. (2020) 17(9):1104–16. doi: 10.1513/AnnalsATS.202002-170OC
69. Taboada A, Ly E, Ramo D, Dillon F, Chang YJ, Hooper C, et al. Implementing goal mama: barriers and facilitators to introducing mobile health technology in a public health nurse home-visiting program. Glob Qual Nurs Res. (2021) 8:1–13. doi: 10.1177/23333936211014497
70. Thomson JL, Tussing-Humphreys LM, Goodman MH. Delta healthy sprouts: a randomized comparative effectiveness trial to promote maternal weight control and reduce childhood obesity in the Mississippi Delta. Contemp Clin Trials. (2014) 38(1):82–91. doi: 10.1016/j.cct.2014.03.004
71. Tinc PJ, Wolf-Gould C, Gadomski A. Longitudinal use of the consolidated framework for implementation research to evaluate the creation of a rural center of excellence in transgender health. Int J Environ Res Public Health. (2020) 17(23):1–18. doi: 10.3390/ijerph17239047
72. Ward AJ, Kluhsman BC, Lengerich EJ, Piccinin AM. The impact of cancer coalitions on the dissemination of colorectal cancer materials to community organizations in rural appalachia. Prev Chronic Dis. (2006) 3(2):1–13. http://www.cdc.gov/pcd/issues/2006/apr/05_0087.htm
73. Ward MM, Baloh J, Zhu X, Stewart GL. Promoting action on research implementation in health services framework applied to TeamSTEPPS implementation in small rural hospitals. Health Care Manage Rev. (2017) 42(1):2–13. doi: 10.1097/HMR.0000000000000086
74. Ward EC, Burns CL, Gray A, Baker L, Cowie B, Winter N, et al. Establishing clinical swallowing assessment services via telepractice: a multisite implementation evaluation. Am J Speech-Lang Pathol. (2021) 30(6):2456–64. doi: 10.1044/2021_AJSLP-21-00109
75. Young LB, Grant KM, Pulido RD, Simpson JL, Tyler KA, Timko C. Intensive referral of veterans to mutual-help groups: a mixed-methods implementation evaluation. Alcohol Treat Q. (2018) 36(2):179–201. doi: 10.1080/07347324.2017.1407224
76. Zoellner JM, Hedrick VE, You W, Chen Y, Davy BM, Porter KJ, et al. Effects of a behavioral and health literacy intervention to reduce sugar-sweetened beverages: a randomized-controlled trial. Int J Behav Nutr Phys Act. (2016) 13(1):38. doi: 10.1186/s12966-016-0362-1
77. Zulman DM, Wong EP, Slightam C, Gregory A, Jacobs JC, Kimerling R, et al. Making connections: nationwide implementation of video telehealth tablets to address access barriers in veterans. JAMIA Open. (2019) 2(3):323–9. doi: 10.1093/jamiaopen/ooz024
78. Feldstein AC, Glasgow RE. A practical, robust implementation and sustainability model (PRISM) for integrating research findings into practice. Jt Comm J Qual Patient Saf. (2008) 34(4):228–43. doi: 10.1016/s1553-7250(08)34030-6
79. Glasgow RE, Vogt TM, Boles SM. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. Am J Public Health. (1999) 89(9):1322–7. doi: 10.2105/ajph.89.9.1322
80. Israel BA, Schulz AJ, Parker EA, Becker AB. Review of community-based research: assessing partnership approaches to improve public health. Annu Rev Public Health. (1998) 19:173–202. doi: 10.1146/annurev.publhealth.19.1.173
81. Rycroft-Malone J. The PARIHS framework–a framework for guiding the implementation of evidence-based practice. J Nurs Care Qual. (2004) 19(4):297–304. doi: 10.1097/00001786-200410000-00002
82. Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. (2009) 4(1). doi: 10.1186/1748-5908-4-50
83. Wandersman A, Duffy J, Flaspohler P, Noonan R, Lubell K, Stillman L, et al. Bridging the gap between prevention research and practice: the interactive systems framework for dissemination and implementation. Am J Community Psychol. (2008) 41:171–81. doi: 10.1007/s10464-008-9174-z
84. Kilbourne AM, Neumann MS, Pincus HA, Bauer MS, Stall R. Implementing evidence-based interventions in health care: application of the replicating effective programs framework. Implement Sci. (2007) 2(1):42. doi: 10.1186/1748-5908-2-42
86. Titler MG, Kleiber C, Steelman VJ, Rakel BA, Budreau G, Everett LQ, et al. The Iowa model of evidence-based practice to promote quality care. Crit Care Nurs Clin North Am. (2001) 13(4):497–509. doi: 10.1016/S0899-5885(18)30017-0
87. Fixsen DL, Naoom SF, Blase KA, Friedman RM, Wallace F. Implementation Research: A Synthesis of the Literature. University of South Florida, Louis de la Parte Florida Mental Health Institute, The National Implementation Research Network. (2005)).
88. Langley GJ, Moen RD, Nolan KM, Nolan TW, Norman CL, Provost LP. The Model for Improvement. the Improvement Guide: A Practical Approach to Enhancing Organizational Performance. San Francisco, CA: Jossey-Bass Publishers (2009).
89. Pronovost PJ, Berenholtz SM, Needham DM. Translating evidence into practice: a model for large scale knowledge translation. Br Med J. (2008) 337:a1714. doi: 10.1136/bmj.a1714
90. Aarons GA, Hurlburt M, Horwitz SM. Advancing a conceptual model of evidence-based practice implementation in public service sectors. Adm Policy Ment Health. (2011) 38(1):4–23. doi: 10.1007/s10488-010-0327-7
92. Moullin JC, Dickson KS, Stadnick NA, Albers B, Nilsen P, Broder-Fingert S, et al. Ten recommendations for using implementation frameworks in research and practice. Implement Sci Commun. (2020) 1:42. doi: 10.1186/s43058-020-00023-7
93. Harris JK, Beatty K, Leider JP, Knudson A, Anderson BL, Meit M. The double disparity facing rural local health departments. Annu Rev Public Health. (2016) 37:167–84. doi: 10.1146/annurev-publhealth-031914-122755
94. Nilsen P, Bernhardsson S. Context matters in implementation science: a scoping review of determinant frameworks that describe contextual determinants for implementation outcomes. BMC Health Serv Res. (2019) 19(1):189. doi: 10.1186/s12913-019-4015-3
95. Proctor EK, Powell BJ, McMillen JC. Implementation strategies: recommendations for specifying and reporting. Implement Sci. (2013) 8:139. doi: 10.1186/1748-5908-8-139
Keywords: scoping review, implementation frameworks, re-aim, CFIR, CBPR, iPARIHS
Citation: Brady RE, Lyons KD, Stevens CJ, Godzik CM, Smith AJ, Bagley PJ, Vitale EJ and Bernstein SL (2024) Implementing evidence-based practices in rural settings: a scoping review of theories, models, and frameworks. Front. Health Serv. 4:1326777. doi: 10.3389/frhs.2024.1326777
Received: 8 November 2023; Accepted: 10 June 2024;
Published: 5 July 2024.
Edited by:
Ekaterina Noyes, University at Buffalo, United StatesReviewed by:
Christina Crabtree-Ide, Roswell Park Comprehensive Cancer Center, United States© 2024 Brady, Lyons, Stevens, Godzik, Smith, Bagley, Vitale and Bernstein. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Robert E. Brady, Um9iZXJ0LkUuQnJhZHlAaGl0Y2hjb2NrLm9yZw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.