
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Health Serv. , 09 March 2023
Sec. Mental Health Services
Volume 3 - 2023 | https://doi.org/10.3389/frhs.2023.1032317
This article is part of the Research Topic World Mental Health Day 2022: Key Drivers of Risk to Mental Health Services and Innovative Solutions View all 16 articles
 Elijah W. Hale1*
Elijah W. Hale1* Rachel A. Davis1,2
Rachel A. Davis1,2
Background: Mental health issues are common among United States medical students, and the AAMC has established recommendations for student mental health services provided by medical schools. Few studies directly compare mental health services at medical schools across the United States and, to our knowledge, none analyze how well schools adhere to the established AAMC recommendations.
Objective: To determine whether mental health services at United States medical schools adhere to established guidelines.
Methods: From October 2021 to March 2022, we obtained student handbooks and policy manuals from 77% of the accredited LCME United States medical schools. The AAMC guidelines were operationalized and placed into a rubric format. Each set of handbooks was independently scored against this rubric. A total of 120 handbooks were scored and the results were compiled.
Results: Rates of comprehensive adherence were very low, with only 13.3% of schools displaying adherence to the full set of AAMC guidelines. Partial adherence was higher, with 46.7% of schools meeting at least one of three guidelines. Portions of guidelines whose requirements reflected a standard for LCME accreditation displayed a higher rate of adherence.
Conclusion: The low rates of adherence across medical schools, as measured by handbooks and Policies & Procedures manuals, represents an opportunity to improve the mental health services within United States allopathic schools. An increase in adherence could be a step towards improving the mental health of United States medical students.
In recent years, medical schools have sought to foster wellness with encouragement of activities such as mindfulness, exercise, peer connections, healthy diet, and self-care (1). However, mental health is an often overlooked aspect of wellness, despite the higher rates of depression, burnout, and suicidal ideation present in medical students compared to the general population (2, 3). Therefore, it is necessary to ensure students are receiving adequate support and mental health services to best support their patients and themselves. However, there is little research available on the information provided to medical students regarding the availability of mental health services.
Both the Association of American Medical Colleges (AAMC) and the Liaison Committee on Medical Education recognize medical student mental health as a vital aspect of education and suggest the availability of counseling, and the AAMC has a publicly available set of guidelines regarding mental health services for students at United States allopathic schools (Table 1) (4, 5). Despite widespread recognition of the existing barriers to mental health care, the AAMC guidelines remain the only publicly available document guiding the structure of mental health services offered to medical students in the United States. Additionally, the authors are not aware of any research directly comparing the availability of mental health services across United States medical schools. However, the availability of substance use treatment for medical students has been assessed by examination of school handbooks and policy manuals (6). Using similar methodology to evaluate the accessibility of mental health services in medical schools, we reviewed medical school student handbooks and Policies & Procedures (P & P) manuals to assess adherence to the established AAMC guidelines.
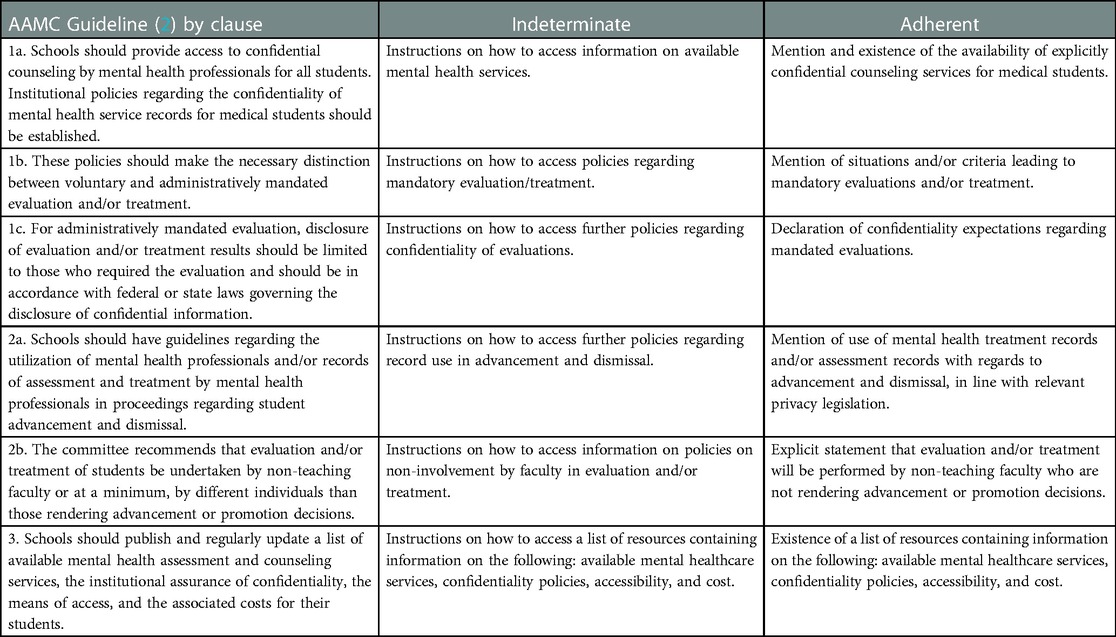
Table 1. Operationalized rubric of AAMC mental health guidelines for medical schools.
From October 2021 to March 2022, we sought to obtain medical student handbooks and Policies & Procedures (P & P) manuals from the 155 LCME accredited US allopathic medical schools. Most documents were easily accessible via the schools' main websites. When a document was not readily available online, we contacted the medical school's office of student affairs or equivalent office via email and phone a maximum of three times. Schools replying to contact after the month of March 2022 were not included in the analysis. Documents were examined when they were identified as either a “student handbook” or “policy & procedure manual” through title or by confirmation via school representatives.
The AAMC guidelines for mental health services were separated into clauses, and then operationalized into a rubric (Table 1). Each set of documents was scored according to the ternary categorical rubric, with the three categories being “adherent,” “indeterminate,” and “nonadherent.” Guidelines were considered “adherent” when all the rubric criteria were met. The term “indeterminate” was applied to criteria when documents contained instructions on where to obtain the corresponding information, but did not provide the information within the text. This term was chosen as the completeness of the information provided was unclear, and the multiple steps required to access the information presented a potential boundary to care. For example, a document with the statement “Inquire at the Office of Student Affairs for information on mental health services” would be labelled “indeterminate” for criteria 1a, as it does not provide any information on the availability of confidential counseling but does provide an avenue for further inquiry. Documents were considered “nonadherent” to a criteria when the information was not present in the text, and no further information on where to locate the information was presented.
The scoring of documents was performed by EWH, and frequency of criteria adherence was added into a spreadsheet. In order to ensure consistency, results were intermittently spot checked. When all documents had been scored, we generated descriptive statistics based on the frequency count of adherence for each criterion. This structure and publication of this study followed the most recent Standards for Quality Improvement Reporting Excellence (SQUIRE) guidelines (7). The Colorado Multiple Institutional Review Board (COMIRB) designated this study as non-human research and not in need of review.
Out of 155 schools, we were successful in obtaining documents from 120 (77.4%). Of the outstanding 35, six schools denied access to the documents, and the remaining 29 did not respond to repeated requests. A final 120 (77.4%) sets of school documents were inspected. Document length ranged from 14 to 454 pages.
Of the 120 sets of documents analyzed, sixteen (13.3%) adhered to all AAMC guidelines for mental health services. Thirty-three schools (27.5%) fulfilled the criteria for only one AAMC guideline, and sixty-four schools (53.3%) did not fulfill the criteria for any AAMC guideline. Guideline 2 had the highest frequency of adherence, with 39 schools (32.5%) fulfilling criteria. Individual criteria had higher rates of adherence. Criterion 2b, which details non-involvement of psychiatric providers in evaluation of patient-students, was adhered to by 95 schools (79.2%). The second highest criterion, with 88 sets of documents (73.3%) adhering, was 1a, detailing the availability of confidential counseling for students (Table 2). These results are graphically represented in Figure 1.
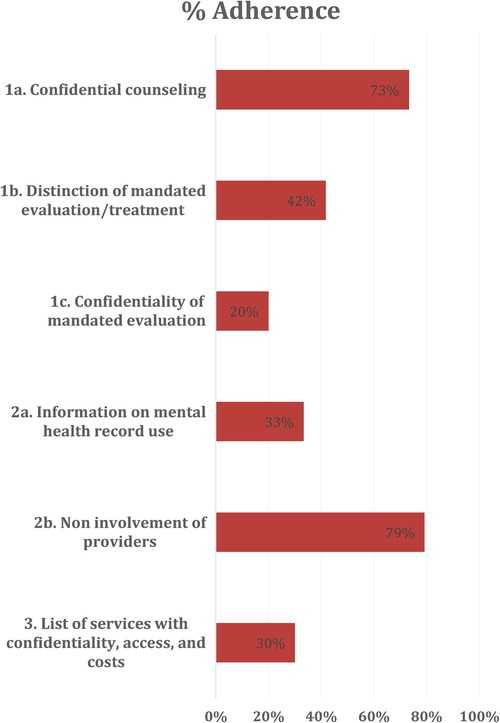
Figure 1. School document adherence to criteria, in percentage of total schools analyzed.
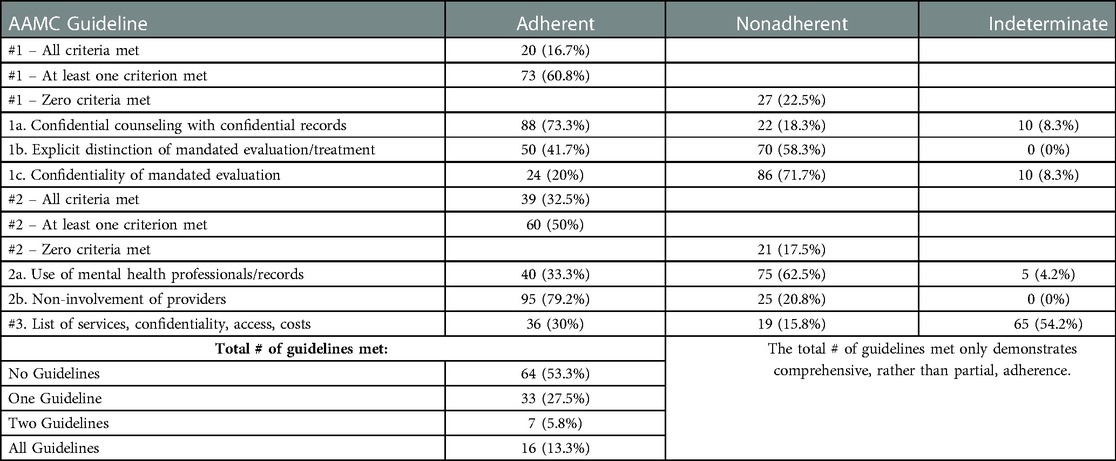
Table 2. Adherence, nonadherence, and indeterminate adherence by AAMC guideline.
Our findings demonstrate the need for increased focus on provision of mental health treatment. Fewer than 14% of schools fully adhere to all of the established AAMC guidelines. Even one of the most commonly fulfilled criteria, availability of confidential counseling services, was present in fewer than 75% of the published documents. In fact, our data show that most medical school documents did not adhere to any of the AAMC guidelines. The highest degree of adherence was to criterion 2b, which is directly related to the LCME standard of accreditation which requires that health professionals involved in psychiatric or psychological care of a medical student not be involved in that student's assessment or promotion (5). This LCME standard also recommends availability of student counseling, but the recommendation is not compulsory (5). This LCME standard relating to criterion 2b and 1a may contribute to their high rate of adherence. The other criteria are not reflected in LCME standards, and there is a drop in adherence of 29% between criterion 2b and the third most fulfilled criterion, 1b, which details the importance of separating mandatory evaluation and elective treatment. One possibility for the difference could be that medical schools' abidance to the AAMC guidelines is driven by accreditation standards. This presents the possibility that adherence to these guidelines could be improved by adapting the LCME standards to include specific requirements regarding student mental health services. If accreditation standards mandated the availability of student mental health services, it is likely that more schools would offer these services and provide information in their handbooks and official P & P manuals.
Medical students have unique mental health needs. They face intense and increasing competition in nearly all aspects of their training, from the rising standards of admission to the increasingly competitive residency match (8, 9). As a result, medical students are under immense academic and emotional stress and regularly report perceiving limited support from their medical schools, which may be one of many factors that contribute to their high rates of depression and anxiety (10). In spite of medical training in psychiatric illness, students largely report not seeking treatment for their own mental health needs, even when they recognize those needs as unmet (11). Untreated mental illness puts medical students at risk across a variety of domains. In their personal health, medical students may experience increased substance use or severe infectious illness COVID-19, both of which have demonstrated increased prevalence in individuals with untreated mental illness (12, 13). Within school, medical students with underlying mental illness may experience higher rates of sleep issues and poorer academic performance (14). Even after graduating, they may experience higher rates of burnout and even suicidality (15). It is incumbent upon medical schools to teach students how to mitigate this stress by instilling curriculum supporting the development help-seeking and self-care skills into their professionalism curriculum, as well as offering ample mental health resources for students.
While overall wellness includes mental health, many medical schools provide resources that primarily focus on other aspects such as meditation, exercise, and an increase in coaching relationships (1). While these aspects are important, a focus on wellness in the absence of a similar focus on and normalization of mental health treatment may lead to feelings of inadequacy, shame, or imposter syndrome when students are unable to independently “be well.” (16) Furthermore, it can also increase stigma around trainees who may be considered “unwell,” including those with disabilities (17). In an AAMC report, learners with disabilities described many barriers within their medical education, including lack of clear policies/procedures and lack of access to health care and wellness supports (18). Centralizing information in readily available school documents could help remove lack of resource awareness as a potential barrier to mental health treatment. Additionally, the handbooks offer an opportunity to reduce feelings of imposter syndrome for struggling learners by providing an institutional acknowledgment that the use of resources is encouraged (19).
There are both strengths and limitations inherent to the use of school documents as proxies for availability of mental health services. While it is possible that handbooks and official P & P manuals may not represent all information presented to students, and therefore underestimate rates of adherence, the handbook is often a central resource for students seeking information. More than 80% of document sets had statements indicating medical students were required to read and understand the information within, which indicates they should be a reliable reflection of school resources. Nonetheless, schools may provide information regarding mental health services through other avenues, such as email, websites, lectures, or campus announcements. Conversely, it is also possible that student handbooks provide a more robust description of services than what is realistically available to students, due to factors such as psychiatric provider shortages. For example, a school may report availability of confidential counseling, but the waitlist for an appointment may exceed several months, greatly hindering student access.
Our investigation provides an examination into the availability of mental health services at United States allopathic medical schools. Our data suggests a lack of adherence to AAMC guidelines, despite the prevalence of mental health issues among medical students and the established importance of mental health treatment. Improving the information contained within student handbooks and P & P manuals, as well as offering services recommended by the AAMC, could help reduce barriers to mental health treatment. As the awareness of barriers to psychiatric care increases, it becomes even more important that medical students are aware of resources available to support their mental health. Regardless of their chosen specialty, medical students and future physicians will ultimately be relied upon to support patients' mental and emotional health at different points in their training. Adequate mental health services must be provided to ensure students' behavioral health is maintained and supported throughout their medical education.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The Colorado Multiple Institutional Review Board (COMIRB) designated this study as non-human research and not in need of review.
EWH had full access to all the data in the study and takes full responsibility for the integrity of the data and the accuracy of the data analysis. Concept, design and drafting: RAD and EWH. Critical revision, administrative support, supervision: RAD. All authors contributed to the article and approved the submitted version.
RAD served as Medical Director of Student and Resident Mental Health at the University of Colorado Anschutz Medical Campus until June 2022.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Young C, Caceres J, Jackson A, Lee WW, Philips A, Rea M, et al. UME Wellness Programming and Strategies for Evaluating Wellness Programs: A National Review. https://www.aamc.org/media/56246/download?attachment (Accessed August 1, 2022).
2. Rotenstein LS, Ramos MA, Torre M, Segal JB, Peluso MJ, Guille C, et al. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: a systematic review and meta-analysis. JAMA. (2016) 316(21):2214–36. doi: 10.1001/JAMA.2016.17324
3. Dyrbye LN, West CP, Satele D, Boone S, Tan L, Sloan J, et al. Burnout among U.S. Medical students, residents, and early career physicians relative to the general U.S. Population. Acad Med. (2014) 89(3):443–51. doi: 10.1097/ACM.0000000000000134
4. Association of American Medical Colleges. Recommendations Regarding Health Services for Medical Students (1992). https://www.aamc.org/professional-development/affinity-groups/gsa/health-services-recommendations (Accessed November 1, 2021).
5. Liaison Committee on Medical Education. Functions and Structure of a Medical School: Standards for Accreditation of Medical Education Programs Leading to the MD Degree 2021-22. (2017). https://lcme.org/publications/#Standards (Accessed November 10, 2021).
6. Mannes PZ, Wang TL, Ma W, Selzer J, Blanco C. Student substance use policies in US allopathic medical schools: a national study. JAMA Psychiatry. (2021) 78(12):1393–5. doi: 10.1001/jamapsychiatry.2021.2666
7. Ogrinc G, Davies L, Goodman D, Batalden P, Davidoff F, Stevens D. SQUIRE 2.0 (standards for QUality improvement reporting excellence): revised publication guidelines from a detailed consensus process. BMJ Qual Saf. (2016) 25(12):986–92. doi: 10.1136/bmjqs-2015-004411
8. Advance Data Tables 2022 Main Residency Match®. www.nrmp.org (Accessed August 12, 2022).
9. Heller CA, Rúa SH, Mazumdar M, Moon JE, Bardes C, Gotto AM Jr. Diversity efforts, admissions, and national rankings: can We align priorities? Teach Learn Med. (2014) 26(3):304–11. doi: 10.1080/10401334.2014.910465
10. Lefebvre C, Hartman N, Tooze J, Manthey D. Determinants of medical specialty competitiveness. Postgrad Med J. (2020) 96(1139):511–4. doi: 10.1136/postgradmedj-2019-137160
11. Matheson KM, Barrett T, Landine J, McLuckie A, Soh NLW, Walter G. Experiences of psychological distress and sources of stress and support during medical training: a survey of medical students. Acad Psychiatry. (2016) 40(1):63–8. doi: 10.1007/s40596-015-0395-9
12. Gold JA, Johnson B, Leydon G, Rohrbaugh RM, Wilkins KM. Mental health self-care in medical students: a comprehensive look at help-seeking. Acad Psychiatry. (2015) 39(1):37–46. doi: 10.1007/s40596-014-0202-z
13. CDC. People with Certain Medical Conditions. https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html (Accessed January 10, 2022)
14. Ahrberg K, Dresler M, Niedermaier S, Steiger A, Genzel L. The interaction between sleep quality and academic performance. J Psychiatr Res. (2012) 46(12):1618–22. doi: 10.1016/J.JPSYCHIRES.2012.09.008
15. Harvey SB, Epstein RM, Glozier N, Petrie K, Strudwick J, Gayed A, et al. Mental illness and suicide among physicians. Lancet. (2021) 398(10303):920–30. doi: 10.1016/S0140-6736(21)01596-8
16. Rivera N, Feldman EA, Augustin DA, Caceres W, Gans HA, Blankenburg R. Do I belong here? Confronting imposter syndrome at an individual, peer, and institutional level in health professionals. MedEdPORTAL. (2021) 17:11166. doi: 10.15766/MEP_2374-8265.11166
17. Stergiopoulos E, Hodges B, Martimianakis MA. Should Wellness Be a core competency for physicians? Acad Med. (2020) 95(9):1350–3. doi: 10.1097/ACM.0000000000003280
18. Meeks LM, Jain NR. Accessibility, Inclusion, and Action in Medical Education: Lived Experiences of Learners and Physicians With Disabilities. (2018). AAMC. https://sds.ucsf.edu/sites/g/files/tkssra2986/f/aamc-ucsf-disability-special-report-accessible.pdf (Accessed August 1, 2022).
Keywords: student mental health and wellness, policy, handbook evaluation, student services, mental health support
Citation: Hale EW and Davis RA (2023) Supporting the future of medicine: Student mental health services in medical school. Front. Health Serv. 3:1032317. doi: 10.3389/frhs.2023.1032317
Received: 30 August 2022; Accepted: 20 February 2023;
Published: 9 March 2023.
Edited by:
Jennifer M. Hensel, University of Manitoba, CanadaReviewed by:
Erene Stergiopoulos, University of Toronto, Canada© 2023 Hale and Davis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elijah W. Hale ZWxpamFoLmhhbGVAY3VhbnNjaHV0ei5lZHU=
Specialty Section: This article was submitted to Mental Health Services, a section of the journal Frontiers in Health Services
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.