
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Health Serv. , 15 April 2022
Sec. Health Policy and Management
Volume 2 - 2022 | https://doi.org/10.3389/frhs.2022.847753
This article is part of the Research Topic Women in Health Services: Health Policy and Management 2021 View all 6 articles
 Mili Roopchand Sahay
Mili Roopchand Sahay Shubhankar Dubey
Shubhankar Dubey Rakesh Kumar SahooSrikanta Kanungo
Rakesh Kumar SahooSrikanta Kanungo Krushna Chandra Sahoo*
Krushna Chandra Sahoo* Sanghamitra Pati*
Sanghamitra Pati*Equality and empowerment for women are among the 17 Sustainable Development Goals (SDGs 5). Although women were confronted with more challenges in various ways during pandemics; however, there is hardly any systematic synthesis of evidence on women's health-related challenges during pandemics. We reviewed the health challenges faced by women during the pandemic. We searched MEDLINE, PsycINFO, and CINAHL following PRISMA guidelines. We identified 2,831 studies, of which we included 17. Reproductive health, psychosocial health, and gender-based violence emerged as significant challenges. Many studies reported challenges in provisions for routine services and increased anxiety, fear, and stress among women. The findings highlighted that pandemic have a significant impact on women's health. Women must have equal rights and opportunities without discrimination, which requires urgent action to enhance women's rights and to achieve SDGs. Women engagement/involvement in pandemic-related services needs to be explored, which will aid in developing strategies to alleviate vulnerabilities.
Several pandemics have occurred throughout human history, most recently those caused by smallpox, cholera, plague, influenza, Ebola, severe acute respiratory syndrome (SARS), West Nile disease, and COVID-19 (1, 2). Pandemics have infected millions of people, resulting in widespread illness and thousands of deaths (3, 4). Apart from the debilitating and sometimes fatal effects on those directly affected, pandemics have a slew of negative social, economic, and political consequences (5, 6). Pandemics have enormous ramifications, particularly for women (7–9).
The pandemics have a systemic problem of human development that exacerbates challenges to gender equality (10, 11). The crisis disproportionately impacts women and girls on various social, economic, and political levels. Women lost jobs more rapidly than men, owing to the high percentage of women employed in hard-hit businesses such as restaurants and hotels. Women working in the informal economy have suffered from a lack of health care, unemployment benefits, and other protections (12). Pandemics are having an effect on gender disparity in health and education and the burden of unpaid care work and gender-based violence. While the pandemics affects everyone, women and girls suffer particular and frequently disproportionate economic, health, and social risks due to ingrained inequities, social norms, and unequal power relations (13). Understanding the gender-disaggregated effects of the pandemics crisis through sex-disaggregated data is crucial for developing policy solutions that minimize vulnerable conditions and improve women's agency while prioritizing gender equality (14). It employs impact evaluation research to identify policy alternatives to increase women's economic resilience and reduce any negative repercussions during the pandemics.
SDGs (Sustainable Development Goals) prioritize gender equality and empowerment and the elimination of all forms of discrimination against women (15). Despite progress toward gender equality, disparities persist in the form of sexual or intimate partner violence and social underrepresentation (16, 17). The difference becomes even more pronounced during unprecedented pandemics when women face adversity in the form of illnesses, economic burden, workplace or household stress, and more (18–20). Additionally, if a woman works, she must balance domestic responsibilities with professional responsibilities (21). Usually, women provided 70% of all health and social services staff globally (17). Moreover, the isolation and confinement may increase gender-based violence (22). Discord between women's personal and professional lives during a pandemic may have long-term consequences (23, 24).
Women generally have more experience using health facilities, whereas men may regard healthcare venues as “feminized” and frequently have low health literacy. This study provides an evidence-based overview of critical analysis of masculinities and pandemics in a gendered lens. It examines the impact of pandemics on men and women in various social groupings. It makes suggestions and recommendations to politicians and other decision-makers on addressing masculinity concerns during times of crisis. Pandemics exacerbate inequalities in women's health (12). Women faced additional obstacles in various ways during pandemics; however, there is less evidence focusing exclusively on women's health-related barriers. This study narrated the health challenges and coping women faced during pandemics.
A systematic review of the existing literature was conducted, emphasizing health-related challenges and coping strategies among women during pandemics. We registered the protocol in PROSPERO (CRD42020187826), and the findings were reported following PRISMA guidelines (25). We conducted a thorough search of the MEDLINE (PubMed), PsycINFO (ProQuest), and CINAHL (EBSCO) databases to identify studies published between January 2000 and September 30, 2020.
We identified qualitative studies that documented the difficulties faced by women during pandemics. The titles and abstracts of the articles retrieved from the database were screened. The full text of the studies was independently screened by the authors (MRS and SD), and KCS resolved any disagreements. We included studies involving women of any age group. We excluded commentary, reviews and studies that did not meet the objective.
The authors (MRS, SD) independently extracted data from the included studies, with disagreements resolved by consulting a third reviewer (KCS). The Consolidated Criteria for Reporting Qualitative Research (COREQ) was used to assess the quality of studies (26) by two authors (MRS, SD) independently (Supplementary Material 1). We used thematic analysis (27) to synthesize the data and identify recurrent themes. The authors read and reread each article to identify potential codes, categories, and themes, as well as coded data, using MAXQDA Analytics Pro 2020 (VERBI GmbH Berlin).
After screening 2,831 abstracts, 141 were considered relevant for full-text review, and finally, 17 were included (Figure 1). Included articles were on influenza (n = 3), COVID-19 (n = 5), Zika (n = 5), Ebola (n = 2) and SARS (n = 2). Eight studies reported reproductive health, while the remaining seven explored primarily psychosocial health (Table 1). The major themes were (1) Reproductive health, (2) Psychosocial health, and (3) Coping strategies and support systems (Table 2).
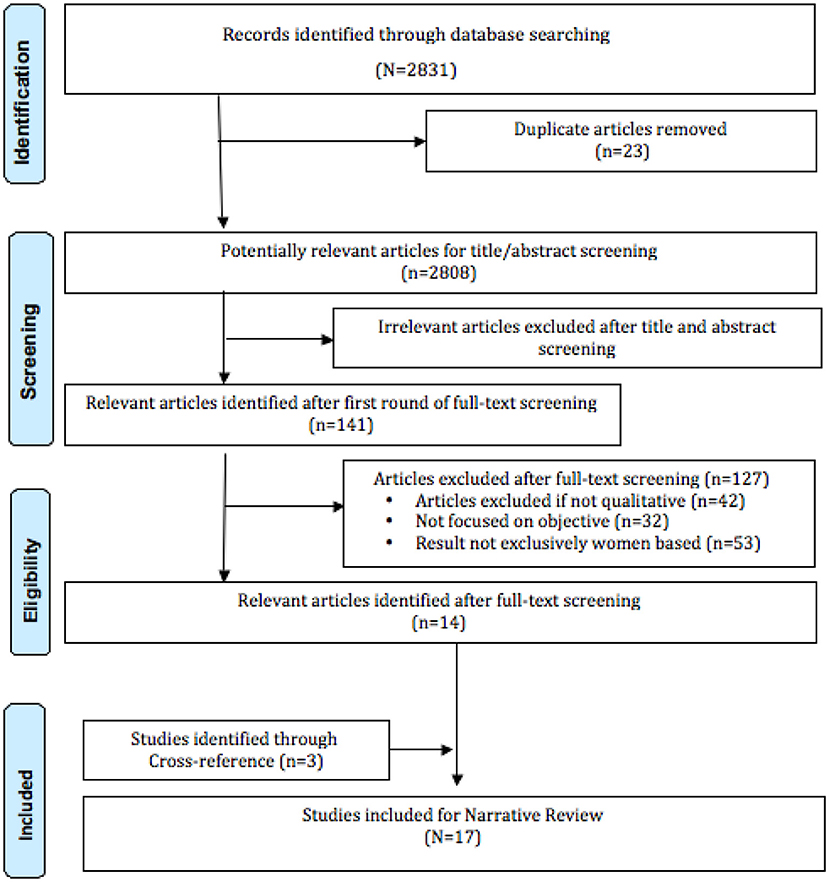
Figure 1. PRISMA flow diagram.
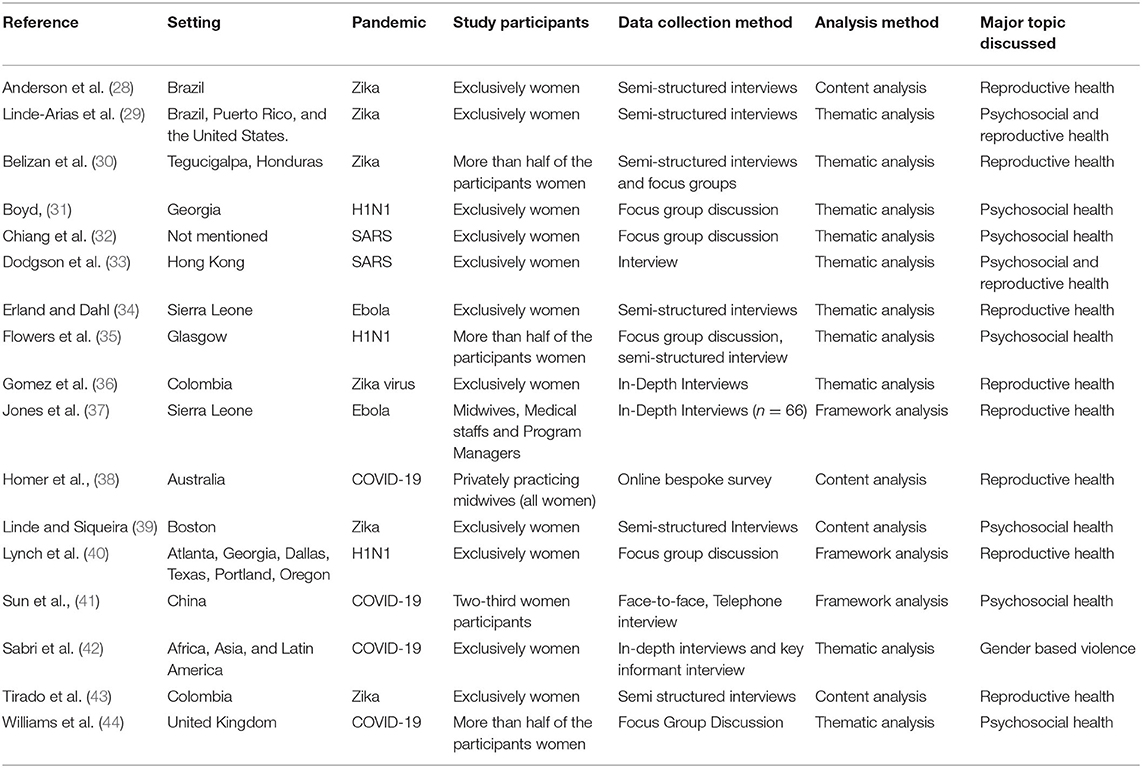
Table 1. Characteristics of the selected studies.

Table 2. Summary of key findings.
The studies were conducted in Africa, Asia, Australia, Brazil, China, Colombia, Georgia, Honduras, Hong Kong, Latin America, Puerto Rico, Scotland, Sierra Leone, the United Kingdom, and the United States. In 11 studies, the participants were exclusively women; in the remaining studies, more than half of the participants were women. The study participants were female community members and female healthcare professionals. All the studies were qualitative and collected semi-structured interviews or focus group discussions.
Inadequate information and knowledge about pandemics, limited access to routine care, shift work for regular service providers, a shortage of medical facilities, and increased out-of-pocket expenses were all identified as common challenges during all types of pandemics (28, 33, 34, 37, 40, 41, 44). Many women and their family members believed hospitals were a source of infection during various pandemics and avoided hospital visits to avoid infection (34, 37). Women abstained from conception during pandemics out of fear or concern for inadequate prenatal care (28, 36, 39, 43). Additionally, many women were dissatisfied with institutional deliveries and preferred home delivery (28, 38). Some women opted for private facilities, increasing their out-of-pocket expenses (30, 33, 36, 37). Similarly, female healthcare providers stated that they felt helpless to treat patients due to insufficient infrastructure and supply, including essential equipment (41). Most of the time, medicines were out of stock, referral services were inadequate due to the absence of ambulances assigned to pandemic duties, and health care providers struggled to promote facility-based deliveries (28, 30, 37). During pandemics, new hospital policies limited interaction between intra-natal women and their families during their hospitalization (30, 33, 38). Additionally, women viewed public transportation as risky, preferring to travel in their vehicle or a hired taxi (33).
Concerns about infection containment prompted restrictive practices such as limiting antenatal appointments, modifying consultation practices (telephonic consultation), and restricting consultation time in health facilities during COVID-19 (38). During the SARS (severe acute respiratory syndrome) epidemic, women's reproductive health was harmed by inadequate counseling services and isolation from healthcare providers (33).
Many pregnant women were concerned about abnormal deliveries, fearful that their children would be born with disabilities. They chose private facilities due to the lengthy wait for a doctor's appointment in public hospitals resulted in out-of-pocket expenses (28, 36). Additionally, due to the lack of family planning services, condom use was reported to be the only method of contraception available (28).
The women faced difficulties such as disrupted counseling services, a lack of basic healthcare facilities, a drug shortage, and referral services (37). During the Ebola outbreak, there was a staff shortage due to relocation, trained infection control personnel, and personal protective equipment. Additionally, it was reported that authorities lacked adequate scientific information and accountability (34, 37).
The primary impediment to vaccine uptake was the lack of scientific information about vaccines (31). They believed that seasonal flu vaccination was a more secure option than the H1N1 vaccine (40). Women were encouraged to get vaccinated out of concern for their children's health (31, 35, 40).
The majority of studies have revealed that pandemics have a detrimental effect on women's psychological health. The most frequently reported psychological effects were fear, stress, anxiety, uneasiness, helplessness, and sadness. These effects had a detrimental impact on women's emotional wellbeing, exacerbating their concern for their families' safety, particularly the elderly and children (29, 31, 32, 34, 37–39, 41, 43, 44). Numerous studies have discovered that female health care providers face emotional stress daily while performing their duties (29, 32). Inadequate information about the new pandemic, a lack of effective pandemic management strategies, and work overload caused them to feel uneasy and stressed (28, 29, 31, 33–37, 40, 44).
The reluctance to visit the hospital was attributed to a persistent fear of contracting an infection (38). They felt claustrophobic due to the lockdown because they were forced to stay inside their homes (44). This increased abusive relationships, as well as an increase in the frequency and severity of intimate partner violence and family conflicts (42). Fear of joblessness or losing a job, as well as financial hardships as a result of the prolonged lockdown, resulted in depression, anxiety, and gender-based violence (42, 44). Working women felt overwhelmed as they were forced to restructure their routine to strike a balance between work and home chores while remaining at home (44). During SARS, despite their willingness to deliver normally in a public facility, they preferred Cesarean section in a private facility due to the risk of contracting SARS (33).
Most participants expressed concern and fear that their baby would have complications during diagnostic procedures and if born with same would require special care with compromised acceptance (43). Even though healthcare providers performed their duties with dedication, they were also subjected to physical and emotional stress (29, 41). Female health workers explained that their workload was doubled due to a staff shortage, leaving them frustrated (30, 36, 37).
Women were afraid to visit health facilities because they believed the Ebola virus was being injected by healthcare providers, causing fear of cross-infection (34, 37). Inadequate preparation due to a lack of knowledge resulted in mistrust in midwives, motivating women to avoid health facilities (37).
According to the study, extensive media broadcasting exacerbated hyper-awareness, anxiety, and fear of contracting the infection, as well as unwarranted panic (31). Participants in the higher risk zone expressed more significant concern than those in other containment zones, owing to the increasing number of illnesses and deaths (40).
Women used a variety of coping strategies to protect themselves from the pandemic and its repercussions. They triggered psychological defensive systems, resorted to active or passive psychological tactics, and changed their sleep schedules when under work-related stress (41, 42). Additional measures to ensure routine work include increasing food intake, regular exercise, and preserving physical strength (41).
Female healthcare professionals claimed that family, society, and the goodwill of patients encouraged them to battle the pandemic and brought them happiness (34, 41). Additionally, they reported that social support was critical for feeling valued (41). Pre-employment training aided in the conversion of negative emotions to good ones. Participants expressed considerable support for government directives on social distancing to protect themselves and those in danger. Healthcare providers were a source of information that could be relied upon. Competence in learning, coordinated support, and government-provided prevention and control training equipped them to confront and resolve problems (37). Nurses at work developed coping techniques such as self-mirroring, self-preservation, and self-transcendence. This alleviated fear and infection while providing compassionate treatment in partnership with colleagues (32).
Changes in daily routine and cessation of social activities were cited as coping mechanisms, resulting in a dearth of leisure, social, and outdoor activities (39). Regardless of the epidemic, women used measures such as avoidance, and hygienic practices, social/physical distancing, movement limitation for self and visitors to the home, monitoring the situation via news broadcasts, and modifying/canceling trip plans (30, 31, 33). Some women decided to delay childbearing to prevent putting the child at risk (31, 39, 43). Financial support was stated to have been supplied by the spouse and family to help with the problem (28, 31, 33, 35, 39, 43).
Using COREQ, we presented the quality assessment of the studies (Supplementary Material 1). It is a complete and coherent checklist of 32 items divided into three categories: research team and reflexivity, study design, and findings analysis. Many studies were presented regarding interviewer credentials and the interviewer's relationship with the participants. Almost all of the articles provided comprehensive theoretical frameworks and participant recruitment strategies. All of the studies adhered to the standard guidelines for analysis and reporting. None of the studies used repeat interviews, and only a few studies documented participant non-participation and member-check approaches.
Women's reproductive health is determined to be significantly harmed as a result of impeded reproductive, maternity, and child health care due to human resource constraints, as reported by 66% of nations (45). Disruptions in health services increased demand for home births, either out of fear or insufficient support in institutions (46–48). Lack of knowledge or information, lack of permission from family or husband to access facility, geographical barrier, lack of understanding of prevention methods, and fear of infection were the top barriers women faced in accessing health care (49). Frequent policy changes left end users, and service providers perplexed about how to deal with the situation, resulting in a negative impact on sexual and reproductive health services (50, 51).
Globally, domestic violence against women has escalated, exposing these victims to sexual assault and distress (52). Reduced access to alcohol and tobacco products frequently increased violent behavior, exacerbating domestic abuse. Additionally, a dearth of contraception during pandemics exacerbated undesired pregnancies (53). During emergencies, exposure to hygienic goods has decreased, posing health dangers (54). Job loss has economic consequences, making it even more difficult for women of low social status, particularly in developing countries, to get proper maternal health care; this exacerbates anxiety and grief and increases violence against women (52). Pandemics also exacerbate malnutrition among the poor, owing to food instability, resource constraints, and financial insecurity (55). On the other side, physical activity has been reduced due to the lockdown, resulting in a huge increase in the number of obese wealthy individuals; as a result, the risk of non-communicable disease has increased (56).
Women are disproportionately more likely to experience situations in the workplace that demand them to display resilience when they are underrepresented at the top levels of decision-making (57). A resilient person adjusts and responds to stressors in various ways, including embracing the new reality or improvising through efficient coping mechanisms (58). Individuals may have functional or dysfunctional coping strategies; however, positive coping mechanisms are likely to result in improved resilience; hence, coping and resilience, while distinct, are also related. It is necessary to understand the women's capacity to manage and develop resilience in various situations to address women's vulnerabilities (59). It is critical to examine organizational power systems from a resilience and gender viewpoint. As a result, the female perspective on resilience challenges the mainstream masculine discourse on resilience in the context of pandemics (59).
Despite obstacles, women remained resilient, adapting to their circumstances in various ways. Throughout the pandemic, the avoidance of travel, visiting or meeting new people, and going to work were embraced to cope with the crisis (60, 61). Positive outcomes are associated with problem-solving strategies, whereas emotional coping mechanisms such as blaming, avoiding, and ruminating have negative consequences for depression and anxiety (62). Self-care activities such as hygiene and social support aided in managing the pandemic condition (60, 63).
During pandemics, women are at an increased risk. Furthermore, more than 70% of community health workers worldwide are female. During pandemics, multifactorial challenges are exacerbated in a unique way among women. To combat health disparities during pandemics, gender-informed policies are required. There is a need for a more in-depth understanding of the potentially gendered nature of crisis response and the identification of new research avenues.
Regardless of their roles and responsibilities in society, women faced a slew of health-related challenges during pandemics. Gender inequity during pandemics should not be overlooked in reporting. Women must have equal rights and opportunities, free of discrimination, which necessitates immediate action to improve women's rights and achieve the SDGs. Women's engagement in pandemic-related services should be investigated, as this will aid in the development of strategies to reduce vulnerabilities.
MRS and SD designed the systematic review under the supervision of KCS. MRS and SD synthesized and analyzed the data, drafted manuscript, and revised the drafts based on comments from other co-authors. KCS and SP reviewed the various versions of this manuscript and provided constructive comments. All authors read and approved the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors acknowledge Dr. B Sahoo Library Scientist for their support.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frhs.2022.847753/full#supplementary-material
1. Huremović D. Brief History of Pandemics (Pandemics Throughout History). InPsychiatry of Pandemics. Springer, Cham (2019). p. 7–35.
2. Qiu W, Rutherford S, Mao A, Chu C. The pandemic and its impacts. Health Culture Soc. (2017) 9:1–1. doi: 10.5195/hcs.2017.221
3. Goyal MK, Gupta AK editors. Integrated Risk of Pandemic: Covid-19 Impacts, Resilience and Recommendations. Berlin: Springer (2020).
4. Gupta R, Sheng X, Balcilar M, Ji Q. Time-varying impact of pandemics on global output growth. Finance Res Lett. (2021) 41:1544–6123. doi: 10.1016/j.frl.2020.101823
5. Das P, Bisai S, Ghosh S. Impact of pandemics on income inequality: lessons from the past. Int Rev Appl Econ. (2021) 35:832–50. doi: 10.1080/02692171.2021.1921712
6. Furceri D, Loungani MP, Ostry MJ, Pizzuto P. Will COVID-19 Have Long-Lasting Effects on Inequality? Evidence from Past Pandemics. International Monetary Fund (2021).
7. Ayittey FK, Dhar BK, Anani G, Chiwero NB. Gendered burdens and impacts of SARS-CoV-2: a review. Health Care Women Int. (2020) 41:1210–25. doi: 10.1080/07399332.2020.1809664
8. Connor J, Madhavan S, Mokashi M, Amanuel H, Johnson NR, Pace LE, et al. Health risks and outcomes that disproportionately affect women during the Covid-19 pandemic: a review. Soc Sci Med. (2020) 266:113364. doi: 10.1016/j.socscimed.2020.113364
9. Sánchez OR, Vale DB, Rodrigues L, Surita FG. Violence against women during the COVID-19 pandemic: an integrative review. Int J Gynecol Obstet. (2020) 151:180–7. doi: 10.1002/ijgo.13365
10. Farfán CR, Hsu YC, Pavez F, Dugarova E. Gender Inequality and the COVID-19 Crisis: A Human Development Perspective. United Nations Development Programme (2020).
11. Van den Eynde J, De Vos K, Van Daalen KR, Oosterlinck W. Women and COVID-19: a one-man show? Front Cardiovasc Med. (2020) 7:596583. doi: 10.3389/fcvm.2020.596583
12. Thibaut F, van Wijngaarden-Cremers PJ. Women's mental health in the time of Covid-19 pandemic. Front Glob Womens Health. (2020) 1:588372. doi: 10.3389/fgwh.2020.588372
13. Azcona G, Bhatt A, Encarnacion J, Plazaola-Castaño J, Seck P, Staab S. From insights to action: Gender equality in the wake of COVID-19. United Nations Entity for Gender Equality the Empowerment of Women (UN Women). (2020). Available online at: https://www.tandis.odihr.pl/handle/20500.12389/22632
14. Burki T. The indirect impact of COVID-19 on women. Lancet Infect Dis. (2020) 20:904–5. doi: 10.1016/S1473-3099(20)30568-5
15. UN Women. In Focus: Women the Sustainable Development Goals (SDGs): SDG 5: Gender Equality. (2021). Available online at: https://www.unwomen.org/en/news/in-focus/women-and-the-sdgs/sdg-5-gender-equality (accessed August 8, 2021).
16. UN. Gender Equality And Women's Empowerment – United Nations Sustainable Development. (2019). Available online at: https://www.un.org/sustainabledevelopment/gender-equality/ (accessed August 8, 2021).
17. World Health Organization. Delivered by Women, Led By Men: A Gender And Equity Analysis of the Global Health And Social Workforce. (2019). Available online at: https://www.who.int/hrh/resources/health-observer24/en/
18. Cepeda Z, Arenas C, Vilardo V, Hilton E, Dico-Young T, Green C. Dominican Republic Gender Analysis: A study of the Impact of the Zika Virus On Women, Girls, Boys Men. (2021). Available online at: www.oxfam.org (accessed August 8, 2021).
19. Fraser E. Impact of COVID-19 Pandemic on Violence Against Women and Girls. UKAid VAWG Helpdesk Research Report (accessed March 16, 2020). p. 284.
21. Aldossari M, Chaudhry S. Women and burnout in the context of a pandemic. Gend Work Organ. (2021) 28:826–34. doi: 10.1111/gwao.12567
22. Rodriguez-Jimenez R, Fares-Otero NE, García-Fernández L. Gender-based violence during COVID-19 outbreak in Spain. Psychol Med. (2020) 7:1–2. doi: 10.1017/S0033291720005024
23. Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. (2020) 395:507–13. doi: 10.1016/S0140-6736(20)30211-7
24. Kallem VR, Sharma D. COVID 19 in neonates. J Matern Fetal Neonatal Med. (2020) 35:1–9. doi: 10.1080/14767058.2020.1759542
25. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group*. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
26. Booth A, Hannes K, Harden A, Noyes J, Harris J. COREQ (Consolidated Criteria for Reporting Qualitative Studies). Guidelines for Reporting Health Research: A User's Manual. London: John Wiley and Sons, Ltd (2014). p. 214–26.
27. Clarke V, Braun V, Hayfield N. Thematic analysis. In: Smith JA, editor. Qualitative Psychology: A Practical Guide to Research Methods. London: SAGE Publications (2015). p. 222–48.
28. Anderson EJ, Ernst KC, Martins FF, da Silva Martins C, Koss MP. Women's health perceptions and beliefs related to Zika virus exposure during the 2016 outbreak in northern Brazil. Am J Trop Med Hyg. (2020) 102:629–33. doi: 10.4269/ajtmh.19-0311
29. Linde-Arias AR, Roura M, Siqueira E. Solidarity, vulnerability and mistrust: how context, information and government affect the lives of women in times of Zika. BMC Infect Dis. (2020) 20:263. doi: 10.1186/s12879-020-04987-8
30. Belizan M, Maradiaga E, Roberti J, Casco-Aguilar M, Ortez AF, Avila-Flores JC, et al. Contraception and post abortion services: qualitative analysis of users' perspectives and experiences following Zika epidemic in Honduras. BMC Womens Health. (2020) 20:1–2. doi: 10.1186/s12905-020-01066-7
31. Boyd CA, Gazmararian JA, Thompson WW. Knowledge, attitudes, and behaviors of low-income women considered high priority for receiving the novel influenza A (H1N1) vaccine. Matern Child Health J. (2013) 17:852–61. doi: 10.1007/s10995-012-1063-2
32. Chiang HH, Chen MB, Sue IL. Self-state of nurses in caring for SARS survivors. Nurs Ethics. (2007) 14:18–26. doi: 10.1177/0969733007071353
33. Dodgson JE, Tarrant M, Chee YO, Watkins A. New mothers' experiences of social disruption and isolation during the severe acute respiratory syndrome outbreak in Hong Kong. Nurs Health Sci. (2010) 12:198–204. doi: 10.1111/j.1442-2018.2010.00520.x
34. Erland E, Dahl B. Midwives' experiences of caring for pregnant women admitted to ebola centres in Sierra Leone. Midwifery. (2017) 55:23–8. doi: 10.1016/j.midw.2017.08.005
35. Flowers P, Davis M, Lohm D, Waller E, Stephenson N. Understanding pandemic influenza behaviour: an exploratory biopsychosocial study. J Health Psychol. (2016) 21:759–69. doi: 10.1177/1359105314537542
36. Gomez HM, Mejia Arbelaez C, Ocampo Cañas JA. A qualitative study of the experiences of pregnant women in accessing healthcare services during the Zika virus epidemic in Villavicencio, Colombia, 2015–2016. Int J Gynecol Obstet. (2020) 148:29–35. doi: 10.1002/ijgo.13045
37. Jones S, Sam B, Bull F, Pieh SB, Lambert J, Mgawadere F, et al. ‘Even when you are afraid, you stay': provision of maternity care during the Ebola virus epidemic: a qualitative study. Midwifery. (2017) 52:19–26. doi: 10.1016/j.midw.2017.05.009
38. Homer CSE, Davies-Tuck M, Dahlen HG, Scarf VL. The impact of planning for COVID-19 on private practising midwives in Australia. Women Birth. (2021) 34:e32–7. doi: 10.1016/j.wombi.2020.09.013
39. Linde AR, Siqueira CE. Women's lives in times of Zika: mosquito-controlled lives? Cad Saude Publica. (2018) 34:e00178917. doi: 10.1590/0102-311X00178917
40. Lynch MM, Mitchell EW, Williams JL, Brumbaugh K, Jones-Bell M, Pinkney DE, et al. Pregnant and recently pregnant women's perceptions about influenza a pandemic (H1N1) 2009: implications for public health and provider communication. Matern Child Health J. (2012) 16:1657–64. doi: 10.1007/s10995-011-0865-y
41. Sun N, Wei L, Shi S, Jiao D, Song R, Ma L, et al. A qualitative study on the psychological experience of caregivers of COVID-19 patients. Am J Infect Control. (2020) 48:592–8. doi: 10.1016/j.ajic.2020.03.018
42. Sabri B, Hartley M, Saha J, Murray S, Glass N, Campbell JC. Effect of COVID-19 pandemic on women's health and safety: a study of immigrant survivors of intimate partner violence. Health Care Women Int. (2020) 41:1294–312. doi: 10.1080/07399332.2020.1833012
43. Tirado V, Morales Mesa SA, Kinsman J, Ekström AM, Restrepo Jaramillo BN. Women's reluctance for pregnancy: experiences and perceptions of Zika virus in Medellin, Colombia. Int J Gynecol Obstet. (2020) 148:36–44. doi: 10.1002/ijgo.13046
44. Williams SN, Armitage CJ, Tampe T, Dienes K. Public perceptions and experiences of social distancing and social isolation during the COVID-19 pandemic: a UK-based focus group study. BMJ Open. (2020) 10:e039334. doi: 10.1136/bmjopen-2020-039334
45. Sidhu S. COVID-19 Continues To Disrupt Essential Health Services in 90 Per Cent of Countries. (2021). Available online at: https://www.unicef.org/press-releases/covid-19-continues-disrupt-essential-health-services-90-cent-countries (accessed August 9, 2021).
46. Ashish KC, Peterson SS, Gurung R, Skalkidou A, Gautam J, Malla H, et al. The perfect storm: Disruptions to institutional delivery care arising from the COVID-19 pandemic in Nepal. J Glob Health. (2021) 11:05010. doi: 10.7189/jogh.11.05010
47. Schmidt CN, Cornejo LN, Rubashkin NA. Trends in home birth information seeking in the United States and United Kingdom during the COVID-19 pandemic. JAMA Netw Open. (2021) 4:e2110310. doi: 10.1001/jamanetworkopen.2021.10310
48. Burki T. Global shortage of personal protective equipment. Lancet Infect Dis. (2020) 20:785–6. doi: 10.1016/S1473-3099(20)30501-6
49. Temesgen K, Wakgari N, Debelo BT, Tafa B, Alemu G, Wondimu F, et al. Maternal health care services utilization amidstCOVID-19 pandemic in West Shoa zone, central Ethiopia. PLoS ONE. (2021) 16:e0249214. doi: 10.1371/journal.pone.0249214
50. Endler M, Al Haidari T, Benedetto C, Chowdhury S, Christilaw J, El Kak F, et al. How the coronavirus disease 2019 pandemic is impacting sexual and reproductive health and rights and response: Results from a global survey of providers, researchers, and policy-makers. Acta Obstet Gynecol Scand. (2021) 100:571–8. doi: 10.1111/aogs.14043
51. Kotlar B, Gerson E, Petrillo S, Langer A, Tiemeier H. The impact of the COVID-19 pandemic on maternal and perinatal health: a scoping review. Reprod Health. (2021) 18:1–39. doi: 10.1186/s12978-021-01070-6
52. Sharma A, Borah SB. Covid-19 and domestic violence: an indirect path to social and economic crisis. J Family Violence. (2020) 1–7. doi: 10.1007/s10896-020-00188-8
53. Dasgupta A, Kantorová V, Ueffing P. The impact of the COVID-19 crisis on meeting needs for family planning: a global scenario by contraceptive methods used. Gates open research. (2020) 4:102. doi: 10.12688/gatesopenres.13148.2
54. Jahan N. Bleeding during the pandemic: the politics of menstruation. Sex Reprod Health Matters. (2020) 28:1801001. doi: 10.1080/26410397.2020.1801001
55. Rahman T, Hasnain MG, Islam A. Food insecurity and mental health of women during COVID-19: evidence from a developing country. PLoS ONE. (2021) 16:e0255392. doi: 10.1371/journal.pone.0255392
56. Al-Musharaf S, Aljuraiban G, Bogis R, Alnafisah R, Aldhwayan M, Tahrani A. Lifestyle changes associated with COVID-19 quarantine among young Saudi women: a prospective study. PLoS ONE. (2021) 16:e0250625. doi: 10.1371/journal.pone.0250625
57. Smyth I, Sweetman C. Introduction: gender and resilience. Gender Dev. (2015). 23:405–14. doi: 10.1080/13552074.2015.1113769
58. Cahn NR, McClain LC. Gendered complications of COVID-19: towards a feminist recovery plan. Geo J Gender L. (2020) 22:1. Available online at: https://scholarship.law.bu.edu/faculty_scholarship/978
59. Women UN, Snyder D. COVID-19 and the Care Economy: Immediate Action And Structural Transformation For A Gender-Responsive Recovery. Gender and COVID-19 Policy Brief Series. New York, NY: UN Women (2020).
60. Frey MK, Chapman-Davis E, Glynn SM, Lin J, Ellis AE, Tomita S, et al. Adapting and avoiding coping strategies for women with ovarian cancer during the COVID-19 pandemic. Gynecol Oncol. (2021) 160:492–8. doi: 10.1016/j.ygyno.2020.11.017
61. Prowse R, Sherratt F, Abizaid A, Gabrys RL, Hellemans KG, Patterson ZR, et al. Coping with the COVID-19 pandemic: examining gender differences in stress and mental health among University students. Front Psychiatry. (2021) 12:650759. doi: 10.3389/fpsyt.2021.650759
62. Fluharty M, Fancourt D. How have people been coping during the COVID-19 pandemic? Patterns and predictors of coping strategies amongst 26,016 UK adults. BMC Psychol. (2021) 9:107. doi: 10.1186/s40359-021-00603-9
Keywords: gender, women, vulnerability, pandemic, SDGs
Citation: Sahay MR, Dubey S, Sahoo RK, Kanungo S, Sahoo KC and Pati S (2022) Health-Related Challenges and Coping Strategies Among Women During Pandemics: A Systematic Review of Qualitative Studies. Front. Health Serv. 2:847753. doi: 10.3389/frhs.2022.847753
Received: 03 January 2022; Accepted: 21 March 2022;
Published: 15 April 2022.
Edited by:
Jacqueline Ponzo, Universidad de la República, UruguayReviewed by:
Baltica Cabieses, Universidad del Desarrollo, ChileCopyright © 2022 Sahay, Dubey, Sahoo, Kanungo, Sahoo and Pati. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Krushna Chandra Sahoo, c2Fob29rcnVzaG5hQHlhaG9vLmNvbQ==; Sanghamitra Pati, ZHJzYW5naGFtaXRyYTEyQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.