 Manuel Neves1*
Manuel Neves1* Rita Gerivaz2Graça Esteves3Rui Bergantim4Gisela Ferreira5Henrique Coelho6Celina Afonso7Delfim Duarte8Anabela Neves9Helena Matos Silva10Joana Caetano1
Rita Gerivaz2Graça Esteves3Rui Bergantim4Gisela Ferreira5Henrique Coelho6Celina Afonso7Delfim Duarte8Anabela Neves9Helena Matos Silva10Joana Caetano1 Rita Jaime11Catarina Geraldes12
Rita Jaime11Catarina Geraldes12 Paulo Lúcio1
Paulo Lúcio1- 1Hemato-Oncology Unit, Champalimaud Center for the Unknown, Lisbon, Portugal
- 2Hematology Unit, Unidade Local de Saúde Almada-Seixal, Lisboa, Portugal
- 3Hematology & Transplantation Unit, Unidade Local de Saúde Santa Maria, Lisboa, Portugal
- 4Hematology Department, Unidade Local de Saúde de S. João, Porto, Portugal
- 5Hematology Department, Unidade Local de Saúde da Região de Aveiro, Aveiro, Portugal
- 6Hemato-Oncology Unit, Unidade Local de Saúde de Matosinhos, Gaia, Portugal
- 7Hematology Unit, Unidade Local de Saúde de Lisboa Ocidental, Lisboa, Portugal
- 8Department of Hematology and Bone Marrow Transplantation, Instituto Português de Oncologia do Porto Francisco Gentil, Porto, Portugal
- 9Hemato-Oncology Unit, Unidade Local de Saúde da Arrábida, Setubal, Portugal
- 10Hemato-Oncology Unit, Unidade Local de Saúde de Viseu Dão-Lafões Viseu, Viseu, Portugal
- 11Medical Affairs, Janssen-Cilag Farmacêutica, Oeiras, Portugal
- 12Hematology Department, Unidade Local de Saúde de Coimbra, Coimbra, Portugal
Background: Multiple myeloma (MM) is an incurable hematologic malignancy, and even though the complete response (CR) rate has been growing, a high percentage of patients continues to relapse. Recent research showed that most relapses may be related to the persistence of measurable residual disease (MRD). In this study, we intended to evaluate the MRD status in MM patients who reached CR in their second or third lines of treatment.
Methods: This was a cross-sectional, multicentre, non-interventional study to describe the MRD status in patients with relapsed or refractory MM (rrMM), with documented CR; adult male and female patients, from 11 Portuguese sites, in their second or third line of treatment were included. Bone marrow MRD was assessed through next-generation flow cytometry (NGF) technology.
Results: Among the 68 subjects who gave informed consent, 48 were considered eligible for the study. Of the 48 subjects with confirmed CR, 31 (64.6%) had undetectable MRD levels. The incidence of undetectable MRD was lower in International Staging System (ISS) III patients compared with ISS I/II patients (60% vs. 70.8%; p = 0.45), and lower in patients treated without daratumumab-containing regimens compared with those treated with daratumumab-containing regimens (57.1% vs. 75.0%; p = 0.30). Notably, despite the small sample size, the incidence of undetectable MRD was significantly lower in patients with high-risk cytogenetics compared to those with standard risk (33.3% vs. 76.0%; p = 0.04).
Discussion: Our results highlight the possibility of achieving undetectable MRD in the rrMM setting, especially in earlier stages and with highly effective protocols. We expect that this work leverages the implementation of larger real-world evidence studies in rrMM patients, in which MRD may also be defined as a primary endpoint.
1 Introduction
Multiple myeloma (MM) is a chronic hematologic malignancy. Despite the increase in overall responses to treatments and in disease progression-free survival outcomes, most patients will eventually relapse (1). MM is characterized by a dysregulation and clonal proliferation of malignant plasma cells in the bone marrow, which generally secrete an anomalous monoclonal immunoglobulin called M protein, causing bone lytic lesions, anemia, hypercalcemia, and kidney failure (2). In the setting of hematological cancers, MM is the second most common disease, with almost 180,000 cases worldwide and 120,000 deaths reported in 2020 (3, 4).
Even though MM is still an incurable disease, over the last decade, advances in the knowledge of its molecular pathogenesis and the development of a variety of innovative treatments, which can modify the course of the disease, have been changing both the prognosis and treatment approaches (1, 5–7). As a result, the number of patients reaching complete response (CR), in both first line and relapse settings, is increasing (8). Nevertheless, about 40% of patients who achieve CR will relapse and 20% will die within four years after the initial treatment (9). In this context, CR seems an insufficient surrogate to predict prolonged survival outcomes (10). Indeed, M protein analysis and conventional cytological cell morphology techniques are insufficient to detect persistent disease (9).
In MM, most relapses may be related to the persistence of undetectable measurable residual disease (MRD) that is beyond the detection limit of current clinical response criteria (11–13). Several studies showed that MRD negativity was associated with longer progression-free survival (PFS) and overall survival (OS) (14, 15). In the absence of official guidelines and considering the impact of these data, the scientific community came to consider that MRD is one of the most relevant prognosis parameters and will become an effective tool to guide clinical decisions in MM (12, 13, 15). In fact, MRD was used in the Multiple Myeloma XI trial to evaluate the best duration of maintenance treatment, after transplant (16).
Among a variety of techniques, multiparametric flow cytometry assays, such as next-generation flow cytometry (NGF), and next-generation sequencing (NGS) comply with most of the criteria defined for MRD testing: high-range applicability, high sensitivity and specificity, feasibility, accessibility, quickness, small sample size requirement, reproducibility, proven clinical value and cost-effectiveness (7). Compared with NGS, NGF shows similar sensitivity (10−5), but is faster (3–4 h) and does not require the collection of a diagnostic sample to identify the dominant clone, which facilitates its use in a real-world setting (1, 7).
The inclusion of MRD in the recently revised International Myeloma Working Group (IMWG) response criteria represents a strong recognition by the international myeloma community of the relevance of MRD monitoring in the scope of new drug development as a guide to clinical decisions (7). In fact, data from clinical trials indicate that discriminating the MRD status in MM patients who reach CR is relevant to determine the clinical implications of the “CR status” and its prognostic value in the real-world setting for patients with relapsed or refractory multiple myeloma (rrMM) (17, 18). However, MRD monitoring for relapsed/refractory patients is not yet a current clinical practice.
This study aimed to assess the bone marrow MRD status in rrMM patients who reached CR and were in their second or third line of treatment.
2 Methods
2.1 Study design
This was a cross-sectional, multicenter, non-interventional study to describe the MRD status in MM patients with documented CR, in the real-world setting. The cross-sectional design enabled the collection of a sufficient number of defined variables to address the study objectives in a short period of time.
The study included adult male and female patients with rrMM, in their second or third line of treatment. Patients were selected at the hematology outpatient clinics of 11 Portuguese sites.
Participating sites were encouraged to enroll patients in a consecutive manner during their regular appointments, to minimize bias in patient selection. At each site, the physician determined patients’ eligibility for data collection, based on the following inclusion criteria: i) male or female with ≥ 18 years of age; ii) confirmed diagnosis of rrMM; iii) currently in their second or third line of treatment; and iv) CR documented by serum and urine negative immunofixation or by serum negative Hydrashift immunofixation, in patients treated with daratumumab for immunoglobulin G (IgG) MM who achieve very good partial response (VGPR).
Prior to data collection, all patients and/or their legally acceptable representative, where applicable, signed a participation agreement/informed consent form (ICF), approved by the local Independent Ethics Committee, allowing for data collection and source data verification, in accordance with local requirements and sponsor policy.
2.2 Clinical management
The decision to participate in this study did not, in any way, impact the standard of care that the patients were receiving or any benefits to which they were otherwise entitled. The treatment decision was taken prior to the inclusion of the patient in the study and was independent from the decision to participate. All aspects of treatment and clinical management of patients were in accordance with local clinical practice and applicable local regulations and at the discretion of the responsible physician (or treating physician, when different). The sponsor did not provide treatment, nor were patients reimbursed for purchasing any treatments to treat their pathology.
Where available, data were collected from the patients’ clinical records, at enrolment and when the result of the MRD assessment was obtained; baseline data were not available. The maximum time interval for data collection was 30 days, from enrolment (i.e., the moment when eligibility was determined) until the MRD assessment result was obtained. Data collection included demographic data, diagnosis and medical history, MM characteristics, prior and current antimyeloma treatments, assessment of treatment response, cytogenetic characteristics, and MRD status after treatment completion. Patients were considered as high-risk when having at least one of the cytogenetic abnormalities related to poor prognosis, including translocations t(4;14), t(14;16), t(14;20), del (17p), TP53 mutation, and chromosome 1q gain/amplification; patients with t(11;14), t(6;14) and/or trisomies were considered to have standard-risk (19). Patients were also classified according to the International Staging System (ISS) as stage I (serum beta2-microglobulin < 3.5 mg/L and serum albumin ≥ 3.5 g/dL), II (neither stage I nor stage III), or III (serum beta2-microglobulin ≥ 5.5 mg/L) (20).
The end of the study was determined by the collection of data related to the result of the MRD test for the last participating patient. The overall duration of the study, including recruitment, was approximately 27 months.
2.3 Measures of clinical response
The response to the antimyeloma treatment was assessed in all patients with suspected CR (in the absence of bone marrow analysis results), through the analysis of serum and urine samples by immunofixation electrophoretic techniques. If the response available at the participating site raised doubts and CR was not obvious, a repetition of the assessment could be considered; the patient was enrolled in the study only if CR was confirmed.
As anti-CD38 monoclonal antibodies (MoAb), such as daratumumab, may interfere with the assessment of CR through immunofixation electrophoretic techniques, in patients treated with this class of drug and documented VGPR, a specific immunofixation electrophoresis reflex assay (Hydrashift) was used for confirmation purposes, as indicated in the inclusion criteria. CR was assumed in those patients with a negative Hydrashift result (21).
2.4 Minimal residual disease measurement
MM MRD in bone marrow was assessed by the NGF method, using the standardized 2-tube 8-color EuroFlow approach (22). The sensitivity of this technique is 10−5 (0.001%), with thresholds for the lower limit of detection (LLOD) of 20 cells in 2x106 nucleated BM cells and the lower limit of quantification (LLOQ) of 50 cells in 5x106 nucleated BM cells. Undetectable MRD was defined as the absence of tumor plasma cells within 100,000 bone marrow cells (105). Our goal, in terms of collected cells, was set at 107, which corresponds to a total of 10,000,000 cells across the two tubes, specifically 5,000,000 cells per tube. Of note, not all acquired cells are suitable for analysis, as some may be debris or doublets, and these were excluded from the total count. Consequently, the minimum number of analyzed cells was not 100,000, but rather 1,000,000 (106).
2.5 Statistical analysis
No formal hypothesis tests were planned. Descriptive statistics were used to assess the key objectives of this study and to summarize the data collected.
Continuous variables were summarized using descriptive statistics, i.e., number of non-missing observations (n), mean, standard deviation (SD), median, minimum, and maximum. Categorical variables were summarized by absolute and relative frequencies. Data were also summarized according to MRD status. Descriptive statistics were used to characterize demographic and clinical characteristics, and previous lines of treatment by bone marrow MRD status.
The prevalence of MRD in patients who reached CR was estimated by sample proportion (p) and its 95% confidence interval: p = r/n, where r was the number of patients with bone marrow MRD and n was the total number of evaluated MM patients who reached CR and were in their second or third line of treatment (excluding those with unknown bone marrow MRD status).
A Chi-squared test was applied to evaluate the statistical significance of the differences of MRD results between subgroups. A p-value below 0.05 was considered statistically significant.
A multivariable logistic regression was used to investigate the association between the MRD status and clinical characteristics and treatment background. Age (continuous variable), and cytogenic risk, extramedullary plasmacytoma and line of treatment (categorical variables) were identified as clinically relevant, by a medical expert, and included in the logistic regression. Variable selection was, therefore, based on the considered clinical significance.
3 Results
3.1 Study population
Sixty-eight (68) patients were enrolled in the study. Eighteen (18) subjects were not included since they did not comply with one or more of the inclusion criteria; 2 subjects did not have available MRD results. Overall, 48 patients were considered eligible for the study. The demographic and clinical characteristics of the enrolled patients are compiled in Table 1.
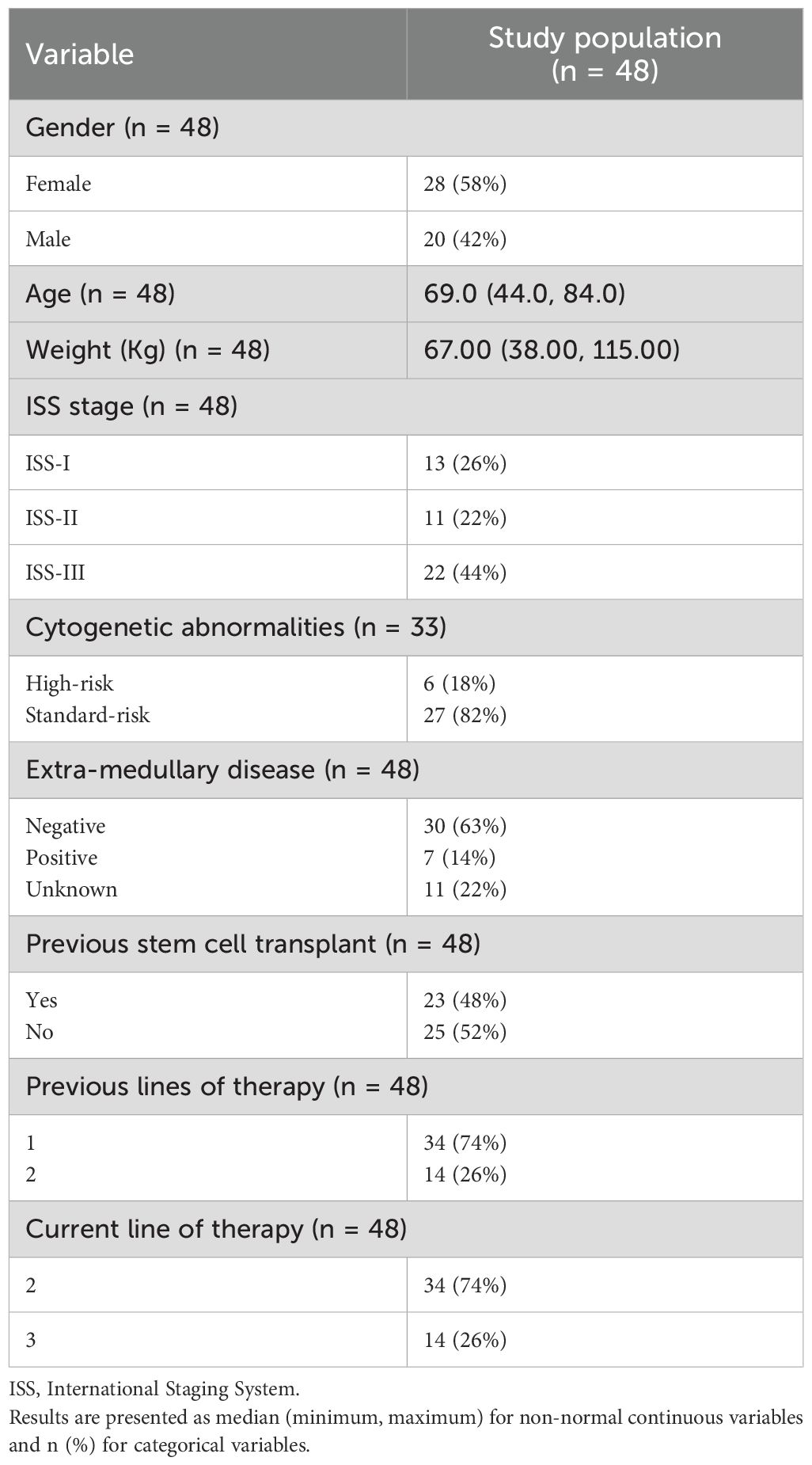
Table 1. Demographic and clinical characteristics of the study population.
3.2 Previous and current medication regimens
In first line treatment, most patients received bortezomib-based regimens, namely the combination of bortezomib, cyclophosphamide, and dexamethasone (VCd, 37.5%). The most frequent therapy in second line was the combination of daratumumab, lenalidomide, and dexamethasone (DRd, 21.4%). Regarding current line of treatment, most patients, either in their second or third line of treatment, received protocols that included therapy with immunomodulatory (38% and 43%, respectively) or daratumumab-based combinations (44% and 36%, respectively) (Table 2, Figure 1).
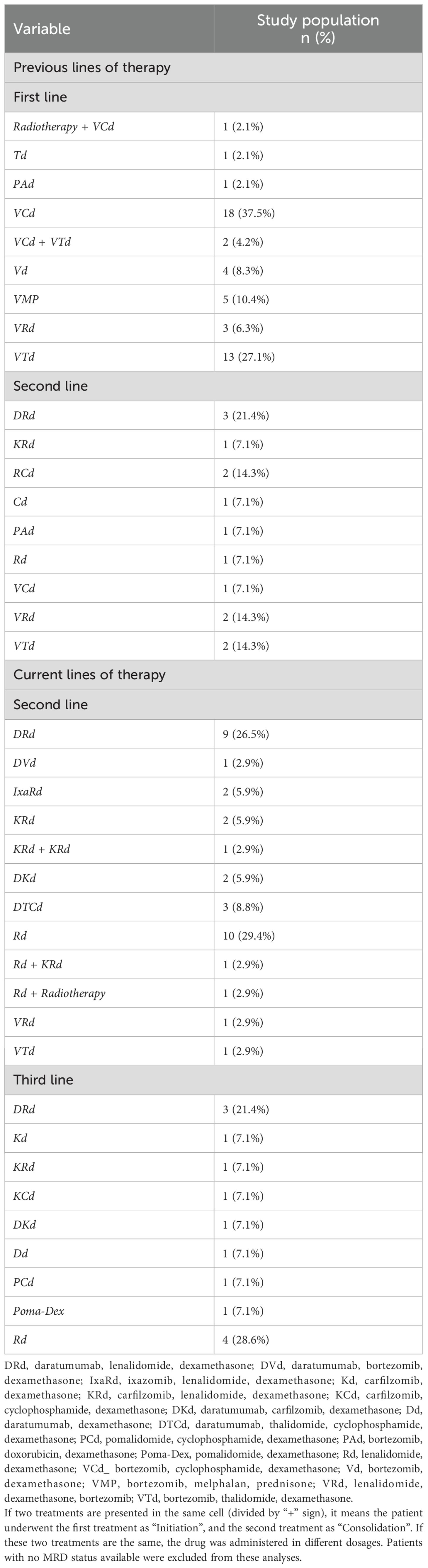
Table 2. Previous and current lines of treatment.
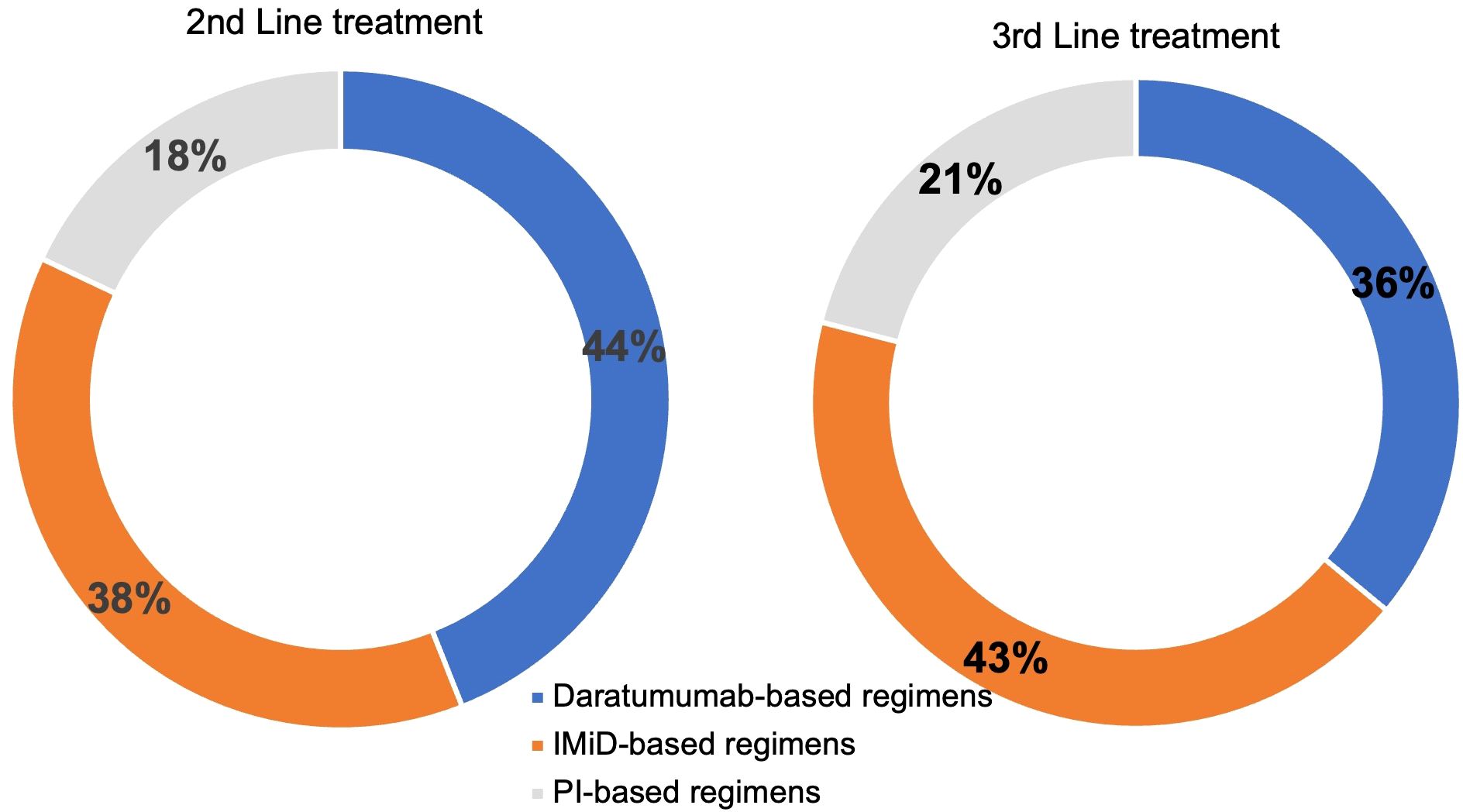
Figure 1. Current lines of treatment. Daratumab-based regimens: daratumumab, lenalidomide, dexamethasone (DRd); daratumumab, bortezomib, dexamethasone (DVd); daratumumab, carfilzomib, dexamethasone (DKd), daratumab, thalidomide, cyclophosphamide, dexamethasone (DTCd); daratumab, dexamethasone (Dd). IMiD-based regimens: lenalidomide, dexamethasone (Rd), Rd plus radiotherapy; lenalidomide, dexamethasone, bortezomib (VRd); pomalidomide, dexamethasone (Poma-Dex); pomalidomide, cyclophosphamide, dexamethasone (PCd). PI-based regimens: bortezomib, thalidomide, dexamethasone (VTd); ixazomib, lenalidomide, dexamethasone (IxaRd); carfilzomib, lenalidomide, dexamethasone (KRd); carfilzomib, dexamethasone (Kd); carfilzomib, cyclophosphamide, dexamethasone (KCd).
3.3 Relationship between minimal residual disease (MRD) status and clinical and treatment background
Of the 48 subjects with confirmed CR and available MRD status, 31 (64.6%) achieved undetectable MRD after second and third treatment were completed. The incidence of undetectable MRD was lower in ISS III patients compared with ISS I/II patients (60% vs. 70.8%; p = 0.45), lower in patients who did not have previous transplant vs. patients who had previous transplant (56.0% vs. 73.9%; p = 0.20), and also lower in patients treated without daratumumab-containing regimens vs. those treated with daratumumab-containing regimens (57.1% vs. 75.0%; p = 0.30). For patients with high-risk cytogenetics vs. standard risk, the incidence of undetectable MRD was significantly lower (33.3% vs. 76.0%; p = 0.04) (Figure 2, Table 3).
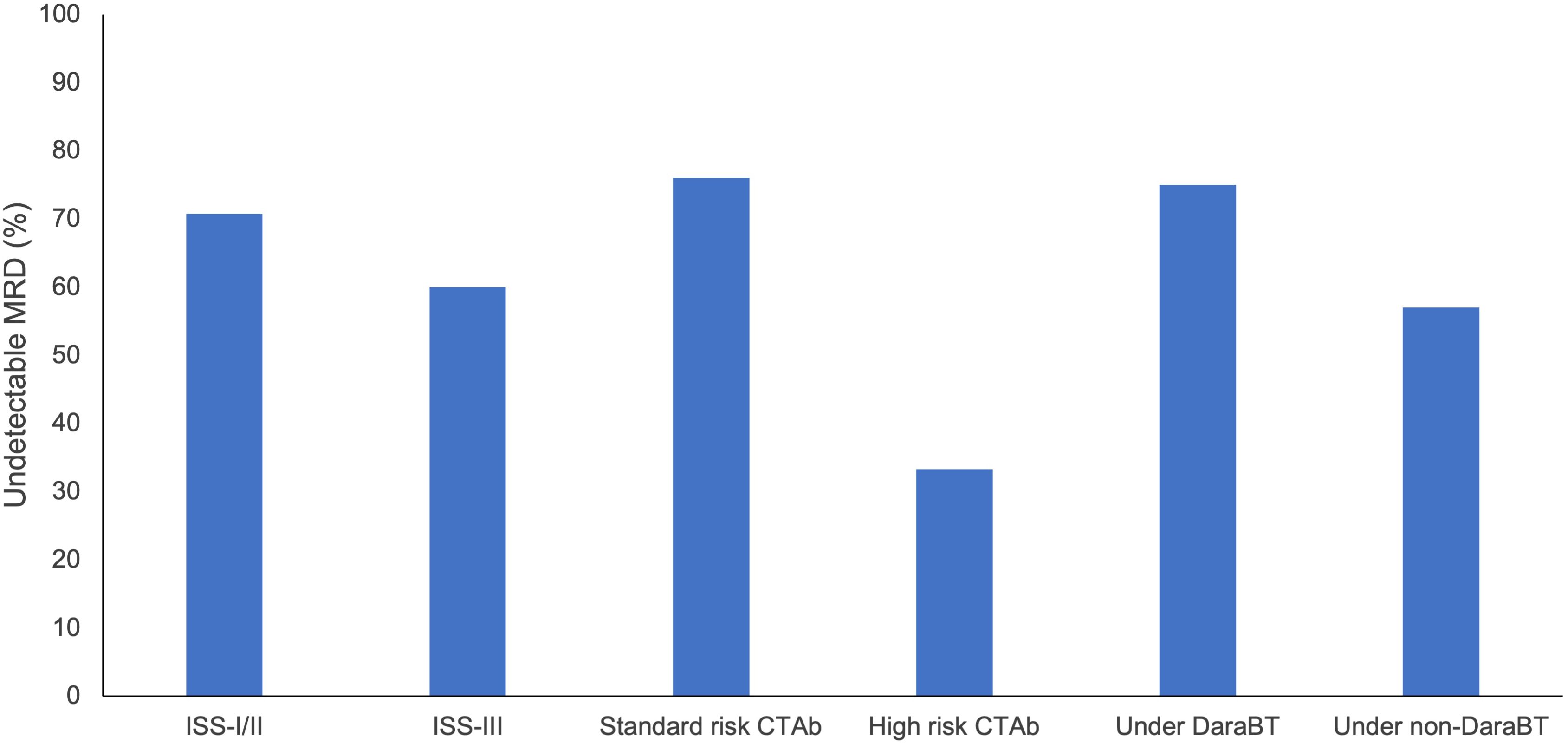
Figure 2. Undetectable MRD according to ISS, risk for cytogenetic abnormalities, and treatment. CT Ab, Cytogenetic abnormalities; DaraBT, Daratumumab base treatments; ISS, International staging system; MRD, Minimal residual disease; Non-DaraBT, Non-daratumumab base treatment.
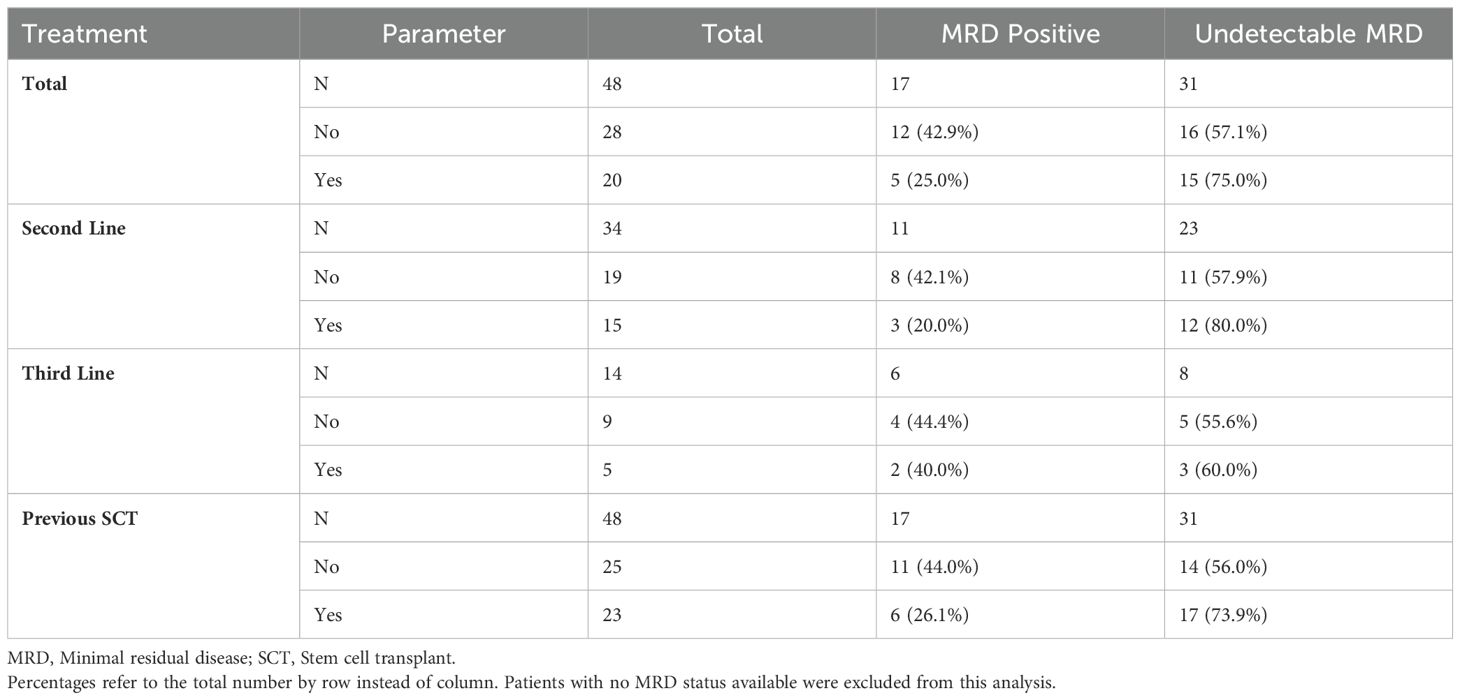
Table 3. Summary of treatment with daratumumab and stem cell transplant by bone marrow MRD status.
Additionally, it was observed that patients treated with daratumumab-containing regimens achieved 80.0% and 60% undetectable MRD in the second and third line of treatment, respectively (Table 3).
4 Discussion
In this cross-sectional, multicenter, non-interventional study, we evaluated the MRD status (by NGF 10−5) of patients with rrMM, in the second or third line of treatment, in a clinical practice setting. Our results showed that the prevalence of undetectable MRD status was around 65%. Our findings align with those of a similar real-world study presented by the Spanish Myeloma Group (GEM), in which the rate of undetectable MRD reported in MM patients, who achieved CR in the first and subsequent lines of therapy, was 73% (23).
The low number of patients included in our study prevents us from drawing definitive conclusions. Nonetheless, our results reinforce the unfavorable prognosis associated with some subgroups within the MM population. For instance, ISS III subgroup of patients showed lower rates of undetectable MRD values. Even though this result was not statistically significant, probably due to the low number of included patients, this observation is consistent with the prognostic implications outlined by the ISS staging definition (20). Importantly, the undetectable MRD rate was significantly lower in patients with a high risk of cytogenetic abnormalities, which are recognized as the most widely accepted predictors of poor prognosis in MM (24). In this setting, it has been proposed that the concomitant characterization of MRD persistent clones may enhance the prognostic value of MRD, providing additional information for the development of novel therapeutic strategies for refractory MM (24). This study has limitations that need to be addressed. Our ability to generalize the results is hindered by our small sample size, which hampers the statistical significance of these results and the assessment of effectiveness with specific groups. Therefore, further research in larger cohorts and with more robust designs is warranted. Moreover, there is the possibility of residual confounding due to treatment selection biases inherent to any nonrandomized observational study, which should be considered.
Even though the evaluation of MRD has been increasingly conducted in clinical settings, it has not become a standard procedure in the Portuguese clinical practice. Despite this, physicians and researchers are well informed of the advances in this area and many centers are equipped with the appropriate technology for MRD evaluation. This establishes the foundation for incorporating MRD routine evaluation into practice. At this point, the most relevant limitations to a broader applicability are related to the quality of the collected bone marrow samples (due to the difficulties encountered at the aspiration procedure), the potential for false negatives, and variations in sensitivity among methodologies used for MRD determination across different centers (9, 14). Technical pitfalls regarding methodology might be overcome using validated, reproducible, and semi-automated procedures, like the Euroflow assay (7, 25); sample-related limitations might be overcome by changing bone marrow samples to liquid biopsies. Blood-based MRD analysis would reduce the invasiveness of the procedure and ensure easier access to samples for routine monitoring, thus promoting the assessment of MRD in clinical practice. Additionally, it could help to identify disseminated disease, decreasing the possibility of false negatives. This option is being adopted in other oncological diseases, providing an accessible tool to monitor disease progression throughout its course, with fewer burdens for patients and accurate results, which have proven to be of great value to guide therapeutic decisions (26, 27).
In MM, some techniques such as mass spectrometry (MS) and circulating plasma cell (CPC) detection by NGF have been explored as alternatives to BM-based tests for MRD and may enter clinical routines in the future (28, 29).
The findings herein described support the relevance of MRD testing in the real-world rrMM setting and confirm that it is possible to achieve high-quality responses, including CR and undetectable MRD with the currently available treatment protocols, especially for second and third lines of treatment. The impact of MRD in the context of rrMM is being explored and discussed (14, 30). The emergence of new therapeutic options, particularly T-cell redirecting therapies (31), reinforces the evaluation of MRD in the relapse setting. These novel options, such as bispecific antibodies (32–34), are associated with achieving deep responses, but are indicated only when disease progression or unacceptable toxicity occur. Consequently, monitoring MRD status in these patients may be crucial for deciding on therapy suspension in the future.
We expect that our results stimulate a more robust and consequential debate regarding the potential implementation of MRD evaluation into clinical practice of MM in Portugal.
Several topics of MM management remain unclear: the role of MRD in real world clinical practice and in the relapsing context, patients’ stratification based on MRD status, or treatment suspension or de-escalation in cases upon confirmation of undetectable MRD. In fact, an objective discussion focused on the clinical trials that are investigating different first-line treatment approaches based on MRD should be encouraged among specialists, with the ultimate objective of establishing a consensus on the most appropriate and sustainable long-term maintenance therapy. Moreover, the possibility of converting MRD negativity into positivity warrants thorough discussion and clarification, particularly in cases of early relapse.
This study is also expected to leverage the design and implementation of future real-world evidence studies, in the setting of MM and rrMM, in which MRD may be defined as a primary endpoint. This would further clarify the impact of this measurement in the management of MM treatment and encourage its incorporation into current clinical practice.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving humans were approved by Comissão de Ética para a Saúde do Centro Hospitalar Vila Nova de Gaia/Espinho, Comissão de Ética para a Saúde do Centro Hospitalar Universitário Lisboa Norte e do Centro Académico de Lisboa, Comissão de Ética para a Saúde do Centro Hospitalar Lisboa Ocidental, Comissão de Ética para a Saúde da Fundação Champalimaud, Comissão de Ética para a Saúde do Centro Hospitalar Tondela Viseu, Comissão de Ética para a Saúde do Centro Hospitalar Universitário de São João, Comissão de Ética para a Saúde do Hospital Garcia de Orta, Comissão de Ética para a Saúde do Instituto Português de Oncologia do Porto FG EPE, Comissão de Ética para a Saúde do Centro Hospitalar de Setúbal, and Comissão de Ética para a Saúde do Centro Hospitalar Baixo Vouga. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MN: Conceptualization, Data curation, Formal analysis, Funding acquisition, Project administration, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing. RG: Formal analysis, Writing – review & editing. GE: Formal analysis, Writing – review & editing. RB: Formal analysis, Investigation, Writing – review & editing. GF: Formal analysis, Investigation, Writing – review & editing. HC: Formal analysis, Investigation, Writing – review & editing. CA: Formal analysis, Investigation, Writing – review & editing. DD: Formal analysis, Investigation, Writing – review & editing. AN: Formal analysis, Investigation, Writing – review & editing. HS: Formal analysis, Investigation, Writing – review & editing. JC: Formal analysis, Investigation, Writing – review & editing. RJ: Formal analysis, Writing – review & editing. CG: Formal analysis, Investigation, Writing – review & editing. PL: Project administration, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was funded from Janssen-Cilag Farmacêutica Portugal.
Acknowledgments
The authors would like to thank all the patients included in this analysis as well as all the investigators, study coordinators and study teams. Writing assistance was provided by BlueClinical.
Conflict of interest
RB: received honoraria consultancy, research funding, speakers bureau from Amgen, Janssen, BMS, Takeda, and S.P.d.S.-BMS. CG: received honoraria consultancy, scientific lectures, and participation in advisory boards from Celgene/BMS, Janssen, Amgen, Takeda, Sanofi, Pfizer, Gilead, and AbbVie. GE: received honoraria consultancy and speaker fee from Pfizer, AbbVie, Sanofi, and Janssen. HS: received honoraria participation in advisory boards Pfizer, Abbvie, Janssen, Amgen, Roche, Takeda, and Sobi. MN: received honoraria consultancy, scientific lectures and participation in advisory boards from Celgene/BMS, Janssen, Amgen, Takeda, Sanofi, Pfizer, and GSK. PL: received honoraria for speaking and/or participation in advisory boards from AbbVie, Amgen, BeiGene, Janssen, BMS, SOBI, and Takeda.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Fazio M, Del Fabro V, Parrinello NL, Allegra A, Markovic U, Botta C, et al. Multiple myeloma in 2023 ways: from trials to real life. Curr Oncol. (2023) 30:9710–33. doi: 10.3390/curroncol30110705
2. Forster S, Radpour R, Ochsenbein AF. Molecular and immunological mechanisms of clonal evolution in multiple myeloma. Front Immunol. (2023) 14:1243997. doi: 10.3389/fimmu.2023.1243997
3. International Agency for Research on Cancer. Estimated number of incident cases World, both sexes, all ages (2020). Available online at: https://gco.iarc.fr/today/data/factsheets/cancers/35-Multiple-myeloma-fact-sheet.pdf (Accessed November 27, 2023).
4. Becker N. Epidemiology of Multiple Myeloma. In: Moehler T, Goldschmidt H. (eds) Multiple Myeloma. Springer, Berlin, Heidelberg: Recent Results in Cancer Research. (2011). pp. 25–35. doi: 10.1007/978-3-540-85772-3_2.
5. Ludwig H, Sonneveld P, Davies F, Bladé J, Boccadoro M, Cavo M, et al. European perspective on multiple myeloma treatment strategies in 2014. Oncologist. (2014) 19:829–44. doi: 10.1634/theoncologist.2014-0042
6. Ria R. Novel agents and new therapeutic approaches for treatment of multiple myeloma. World J Methodol. (2014) 4:73. doi: 10.5662/wjm.v4.i2.73
7. Kumar S, Paiva B, Anderson KC, Durie B, Landgren O, Moreau P, et al. International Myeloma Working Group consensus criteria for response and minimal residual disease assessment in multiple myeloma. Lancet Oncol. (2016) 17:e328–46. doi: 10.1016/S1470-2045(16)30206-6
8. Chanan-Khan AA, Giralt S. Importance of achieving a complete response in multiple myeloma, and the impact of novel agents. J Clin Oncol. (2010) 28:2612–24. doi: 10.1200/JCO.2009.25.4250
9. Paiva B, Van Dongen JJM, Orfao A. New criteria for response assessment: role of minimal residual disease in multiple myeloma. Blood (2015) 125(20):3059–68. doi: 10.1182/blood-2014-11
10. Martinez-Lopez J, Lahuerta JJ, Pepin F, GonzálezGonz M, Barrio S, Ayala R, et al. Prognostic value of deep sequencing method for minimal residual disease detection in multiple myeloma. Blood (2014) 123(20):3073–9. doi: 10.1182/blood-2014-01
11. Mailankody S, Korde N, Lesokhin AM, Lendvai N, Hassoun H, Stetler-Stevenson M, et al. Minimal residual disease in multiple myeloma: Bringing the bench to the bedside. Nat Rev Clin Oncol. (2015) 12:286–95. doi: 10.1038/nrclinonc.2014.239
12. Landgren O, Rajkumar SV. New developments in diagnosis, prognosis, and assessment of response in multiple myeloma. Clin Cancer Res. (2016) 22:5428–33. doi: 10.1158/1078-0432.CCR-16-0866
13. Paiva B, Puig N, García-Sanz R, San Miguel JF. Is this the time to introduce minimal residual disease in multiple myeloma clinical practice? Clin Cancer Res. (2015) 21:2001–8. doi: 10.1158/1078-0432.CCR-14-2841
14. Burgos L, Puig N, Cedena MT, Mateos MV, Lahuerta JJ, Paiva B, et al. Measurable residual disease in multiple myeloma: Ready for clinical practice? J Hematol Oncol. (2020) 13(1):82. doi: 10.1186/s13045-020-00911-4
15. Munshi NC, Avet-Loiseau H, Rawstron AC, Owen RG, Child JA, Thakurta A, et al. Association of minimal residual disease with superior survival outcomes in patients with multiple myeloma: A meta-analysis. JAMA Oncol. (2017) 3:28–35. doi: 10.1001/jamaoncol.2016.3160
16. Jackson GH, Davies FE, Pawlyn C, Cairns DA, Striha A, Collett C, et al. Lenalidomide maintenance versus observation for patients with newly diagnosed multiple myeloma (Myeloma XI): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. (2019) 20:57–73. doi: 10.1016/S1470-2045(18)30687-9
17. Lahuerta JJ, Paiva B, Vidriales MB, Cordón L, Cedena MT, Puig N, et al. Depth of response in multiple myeloma: A pooled analysis of three PETHEMA/GEM clinical trials. J Clin Oncol. (2017) 35:2900–10. doi: 10.1200/JCO.2016.69.2517
18. Dhakal B, Usmani S. Daratumumab and lenalidomide maintenance guided by minimal residual disease in multiple myeloma. Hematologist. (2021) 18. doi: 10.1182/hem.V18.6.202166
19. Kadam Amare P, Nikalje Khasnis S, Hande P, Lele H, Wable N, Kaskar S, et al. Cytogenetic abnormalities in multiple myeloma: incidence, prognostic significance, and geographic heterogeneity in Indian and western populations. Cytogenet Genome Res. (2022) 162:529–40. doi: 10.1159/000529191
20. Greipp PR, Miguel JS, Durie BGM, Crowley JJ, Barlogie B, Bladé J, et al. International staging system for multiple myeloma. J Clin Oncol. (2005) 23:3412–20. doi: 10.1200/JCO.2005.04.242
21. McCudden C, Axel AE, Slaets D, Dejoie T, Clemens PL, Frans S, et al. Monitoring multiple myeloma patients treated with daratumumab: teasing out monoclonal antibody interference. Clin Chem Lab Med (CCLM). (2016) 54(6):1095–104. doi: 10.1515/cclm-2015-1031
22. Flores-Montero J, Sanoja-Flores L, Paiva B, Puig N, García-Sánchez O, Böttcher S, et al. Next Generation Flow for highly sensitive and standardized detection of minimal residual disease in multiple myeloma. Leukemia. (2017) 31:2094–103. doi: 10.1038/leu.2017.29
23. Cedena M, Puig N, Paiva B, Pérez A, De Arriba F, Cuéllar C, et al. Enfermedad Mínima residual en la práctica clínica de pacientes con mieloma Múltiple. In: Abstract Book of the LXI Congreso Nacional de la Sociedad Española de Hematología y Hemoterapia. Haematologica, Valencia, Spain (2019). p. 15–5.
24. Hanamura I. Multiple myeloma with high-risk cytogenetics and its treatment approach. Int J Hematol. (2022) 115:762–77. doi: 10.1007/s12185-022-03353-5
25. Stetler-Stevenson M, Paiva B, Stoolman L, Lin P, Jorgensen JL, Orfao A, et al. Consensus guidelines for myeloma minimal residual disease sample staining and data acquisition. Cytometry B Clin Cytom. (2016) 90:26–30. doi: 10.1002/cyto.b.21249
26. Klein-Scory S, Wahner I, Maslova M, Al-Sewaidi Y, Pohl M, Mika T, et al. Evolution of RAS mutational status in liquid biopsies during first-line chemotherapy for metastatic colorectal cancer. Front Oncol. (2020) 10:1115. doi: 10.3389/fonc.2020.01115
27. Bergantim R, Peixoto da Silva S, Polónia B, Barbosa MAG, Albergaria A, Lima J, et al. Detection of measurable residual disease biomarkers in extracellular vesicles from liquid biopsies of multiple myeloma patients—A proof of concept. Int J Mol Sci. (2022) 23:13686. doi: 10.3390/ijms232213686
28. Derman BA, Stefka AT, Jiang K, McIver A, Kubicki T, Jasielec JK, et al. Measurable residual disease assessed by mass spectrometry in peripheral blood in multiple myeloma in a phase II trial of carfilzomib, lenalidomide, dexamethasone and autologous stem cell transplantation. Blood Cancer J. (2021) 11:19. doi: 10.1038/s41408-021-00418-2
29. Sanoja-Flores L, Flores-Montero J, Puig N, Contreras-Sanfeliciano T, Pontes R, Corral-Mateos A, et al. Blood monitoring of circulating tumor plasma cells by next generation flow in multiple myeloma after therapy. Blood. (2019) 134:2218–22. doi: 10.1182/blood.2019002610
30. Cavo M, San-Miguel J, Usmani SZ, Weisel K, Dimopoulos MA, Avet-Loiseau H, et al. Prognostic value of minimal residual disease negativity in myeloma: combined analysis of POLLUX, CASTOR, ALCYONE, and MAIA. Blood. (2022) 139:835–44. doi: 10.1182/blood.2021011101
31. Shim KG, Fonseca R. Measurable residual disease testing in multiple myeloma following T-cell redirecting therapies. Cancers (Basel). (2024) 16:3288. doi: 10.3390/cancers16193288
32. Lesokhin AM, Tomasson MH, Arnulf B, Bahlis NJ, Miles Prince H, Niesvizky R, et al. Elranatamab in relapsed or refractory multiple myeloma: phase 2 MagnetisMM-3 trial results. Nat Med. (2023) 29:2259–67. doi: 10.1038/s41591-023-02528-9
33. Liu L, Krishnan A. Talquetamab in multiple myeloma. Haematologica. (2023) 109(3):718–24. doi: 10.3324/haematol.2023.283931
Keywords: minimal residual disease, multiple myeloma, refractory, relapse, complete response, cross-sectional
Citation: Neves M, Gerivaz R, Esteves G, Bergantim R, Ferreira G, Coelho H, Afonso C, Duarte D, Neves A, Silva HM, Caetano J, Jaime R, Geraldes C and Lúcio P (2024) Prevalence of measurable residual disease in patients with refractory/relapsed multiple myeloma who reached complete response: a cross-sectional multicentric study. Front. Hematol. 3:1480120. doi: 10.3389/frhem.2024.1480120
Received: 13 August 2024; Accepted: 15 November 2024;
Published: 05 December 2024.
Edited by:
Prashant Ramesh Tembhare, Advanced Centre for Treatment, Research and Education in Cancer (ACTREC), IndiaCopyright © 2024 Neves, Gerivaz, Esteves, Bergantim, Ferreira, Coelho, Afonso, Duarte, Neves, Silva, Caetano, Jaime, Geraldes and Lúcio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Manuel Neves, bWxlYW9uZXZlc0BnbWFpbC5jb20=