 Mette Kaasgaard
Mette Kaasgaard Uffe Bodtger1,2
Uffe Bodtger1,2- 1Pulmonary Research Unit (PLUZ), Department of Medicine, Zealand University Hospital Roskilde and Naestved, Naestved Hospital, Naestved, Denmark
- 2Department of Regional Health Research, Faculty of Health Sciences, University of Southern Denmark, Odense, Denmark
- 3Department of Medicine, Lillebaelt Hospital, Vejle, Denmark
- 4Department of Cardiothoracic and Vascular Surgery, Odense University Hospital, Odense, Denmark
- 5Danish Lung Cancer Registry, Odense, Denmark
Background: Surgical resection is the preferred treatment for localised non-small cell lung cancer (NSCLC). Rehabilitation is central in the management of the associated impaired quality of life, high symptom burden, deconditioning, and social-existential vulnerability. Yet, optimal content and delivery of rehabilitation are not yet defined. Therefore, we aimed to investigate the current rehabilitation offers, attendance rate, and perceived relevance related to content or delivery. Moreover, we investigated the current symptom burden in the patients.
Methods: We conducted an observational cohort study in patients who had undergone surgical resection for NSCLC 4–6 months earlier at Odense University Hospital, Denmark. We retrieved demographic data from patient registries, and interviewed patients via telephone concerning availability, uptake, and attendance rate of any rehabilitation offer in their local primary care setting; content and delivery; benefits of attending, experienced relevance and “symptom burden generally” (specially developed questions); and “symptom burden here and now” [Edmonton Symptom Assessment Scale (ESAS)].
Results: We approached 128 patients, reached 115, and interviewed the 100 (87%) patients who consented. In total, 88% (88/100) had received a rehabilitation offer, and 75% (66/88) had participated in programmes that either targeted NSCLC (23%) or were general cancer rehabilitation (33%), pulmonary rehabilitation (12%), online (1%), or other (33%). Disease-specific rehabilitation was significantly related to the highest attendance rate and perception of relevance. High attendance (≥75%) was, moreover, significantly related to the offer being delivered by a physiotherapist and having a focus on physical exercise. General symptoms were physically oriented [dyspnoea (65%), pain (47%), fatigue (78%)] and “mild” in ESAS scoring. No differences were observed in any baseline characteristics.
Conclusions: Rehabilitation after surgical resection for localised NSCLC is delivered heterogeneously in Denmark. Disease-specific rehabilitation was positively related to attendance rate and to the perceived relevance of the offer.
Introduction
Lung cancer is now the most common cancer worldwide (1), including in Denmark, where the incidence is 5,000 new cases/year, representing 13% of all cancer incidences. At the same time, 5-year survival is increasing, leading to a higher prevalence of long-term survivors (2–6). The main curative treatment for non-small cell lung cancer (NSCLC) is surgical resection of low-stage lung cancer (localised disease with no metastatic spread). Curative treatment may also be achieved using stereotactic radiation therapy (low-stage disease) or concomitant radio-chemotherapy (locally advanced disease) (3, 7).
However, compared to age-matched controls, patients with lung cancer—including the proportion who have undergone surgical resection for NSCLC—have persistently reduced quality of life (QoL), decreased psychological wellbeing, reduced physical and social activity, risk of deconditioning, are marked by symptom clusters (e.g., dyspnoea, cough, pain, fatigue, and dysphonia) and, often, have comorbidities [some of which tobacco related, such as chronic obstructive pulmonary disease (COPD)] (3–5, 8–11).
Besides clinical assessment in a respiratory or oncology outpatient clinic and a computed tomography (CT) scan (7, 10, 12), the recommended follow-up programme includes a relevant rehabilitation offer with, e.g., exercise training, smoking cessation, patient education on self-management to support physical capacity and QoL, and to improve the prognosis (3, 5, 9, 12–15).
However, there is no standardised, lung cancer-specific rehabilitation programme available that addresses the specific needs of the patients after intended curative treatment in lung cancer, including respiratory aspects, QoL, long-term decline in physical capacity, and overall physical and social activity (5, 8, 16), but, as an example, pulmonary rehabilitation (PR) is a multidisciplinary, multi-faceted, and comprehensive intervention based on evidence-based activities (duration: 8–12 weeks), recommended by the European Respiratory Society (ERS) and American Thoracic Society (ATS) to reduce symptoms, increase QoL, and optimise functional capacity (3, 5, 17, 18). A specific core outcome set—specifically for lung cancer rehabilitation—is under development, given a large heterogeneity in outcomes and preferred measures (19) and given that patients with lung cancer are marked by a different and greater symptom burden compared to other cancer types (20).
In Denmark, rehabilitation after a surgical procedure for NSCLC is offered in a municipal primary care setting, but there is a lack of knowledge about the actual availability, uptake, and types of offers, as well as the attendance rate, content and delivery, and perceptions and benefits of the current programmes (10, 16).
Aims and hypotheses
In this study, we aimed to investigate the availability, uptake, and type of the current rehabilitation offers in primary care settings after a surgical procedure for NSCLC in Denmark, and whether the attendance rate and perceived relevance were related to the type, content, and delivery aspects of the offers. Moreover, we aimed to investigate the needs and symptom burden of the patients 4–6 months after the surgical procedure. We hypothesised that (1) the availability, uptake, and content of the current rehabilitation offer are heterogeneous; (2) the attendance rate and perceived benefits and relevance are related to the type, content, and delivery aspects of the current rehabilitation offer; and (3) patients display a significant symptom burden after their surgical procedure.
Methods
Study design and oversight
We conducted an observational study, during which patients were interviewed via telephone between 2 February and 20 March 2024. The study was performed in accordance with the Helsinki II Declaration and obtained all obligatory approvals on 23 November 2023 from the Head Department of Cardiothoracic and Vascular Surgery, Dept. T, Odense University Hospital, the Hospital Director of Lillebaelt Hospital, and the Southern Region of Denmark (J.nr.24/511).
Participants
We included patients who had undergone surgical resection of stage I or II NSCLC at the Cardiothoracic and Vascular Surgery, Dept. T, Odense University Hospital, Denmark, within the previous year. Patients had been referred for the surgical procedure from the respiratory departments at Zealand University Hospital, Lillebaelt Hospital, and Odense University Hospital. After the surgical procedure, a referral is sent to the patient's municipality which is then obliged to provide a suitable rehabilitation offer.
We aimed to include a total of 100 patients in our study, excluding the proportion who would not consent and who were not reachable across three contact attempts. To ensure that we included patients who had completed any rehabilitation offer after their surgery, we contacted patients, starting with those who had undergone a surgical procedure 4 months before the study.
Data collection procedure
We retrieved data from the following sources: (1) Demographic and clinical data from the Danish Lung Cancer Registry and electronic medical files, and (2) patient-reported data from telephone-based interviews using a specially developed questionnaire with closed questions (see elaboration under the Outcomes section).
Data from the Danish Lung Cancer Registry were retrieved on 18 January 2024 by the chief physician, EJ, relating to the last 200 patients who had undergone surgery within the last 12 months at the Cardiothoracic and Vascular Surgery, Dept. T, Odense University Hospital. Data were transferred to Professor, DMSc, Head of Research, OH, and variables of interest were entered by two project nurses (specialists in respiratory care at the Respiratory Research Unit, Department of Medicine, Lillebaelt Hospital, Vejle, Denmark) who also retrieved specific data from patient records and collected patient-reported data via telephone.
The overall data collection procedure was developed and defined by the principal investigator, MK, and OH and AL. The specific content of the questionnaire was developed by MK and discussed with OH, EJ, AL, and with the project nurses. The project nurses, moreover, conducted a face-validity procedure in four patients (before the onset of collection of patient-reported data) to ensure that the study scope and questions were found to be relevant, understandable, and sufficiently comprehensive by the patients.
For the interviews, patients were approached by the time at which any rehabilitation offer would recently have been completed, i.e., starting with those operated on 4 months before the study. They received information about the study and their basic rights and were then able to provide their consent to participate in the study.
All data were entered directly into a secure web-based database, SurveyXact, by Ramboll (Rambøll Management Consulting, Aarhus, Denmark). On 25 March 2024, data were imported into statistical software STATA 18 (StataCorp LLC, TX, USA), anonymised, cleaned, and prepared for analysis.
Outcomes
Data from the Danish Lung Cancer Registry
Data from the Danish Lung Cancer Registry comprised baseline demographic data, NSCLC stage, surgery type and classification, any adjuvant treatment, and date of surgical procedure.
Data from patient registry
Data from the patient registry comprised data about performance status, body mass index (BMI), and predicted forced expiratory volume in the first second (FEV1) percentage, all of which were collected and registered 2–6 weeks prior to the surgical procedure.
Patient-reported data collected via telephone
We collected data on self-reported characteristics, using the specially developed questionnaire, and on socio-demographic information (municipality, educational level, employment status, and civil status), smoking status, and self-reported comorbidities and medicine consumption.
Patient-reported data covered the following aspects:
Availability, uptake, and attendance rate of rehabilitation offer:
Availability and uptake (e.g., received information about the offer (yes/no), time of information since the surgical procedure, acceptance of the offer (yes/no), and single-choice questions across categories on any reasons behind non-acceptance, attendance rate, or dropout).
Content and delivery of the offer:
Content of the rehabilitation offer: (a) “External” characteristics using single-choice questions (setting, type, group-based/individual, and distance to offer); (b) “internal” characteristics using single-choice or multiple-choice questions (duration, frequency, facilitator type, intensity and load, with aspects and elements included).
Evaluation of participation—perceived benefits and relevance
1. Perceived benefits from participation: (a) self-experienced (physical fitness, strength, pain, breathing control, dyspnoea, knowledge about disease/body, confidence/hope, symptom burden, and social network); (b) informed by healthcare professional (e.g., physical capacity test or patient-reported questionnaire).
2. Overall evaluation: Experienced satisfaction with the rehabilitation offer, perceived alignments with the patients' needs, perceived relevance, any missing aspects and elements, and perceived appropriateness of the group (if it was a group-based offer).
3. Self-reported evaluation of the level of physical and social activity at present, compared to before the surgical procedure.
Symptom burden:
1. Symptoms after surgery, generally: specially developed questions about aspects/symptoms related to respiration, pain, fatigue, vigilance, mood, worry about the future, anxiety, loneliness/isolation, vocal function, and cough [Question: “Have you experienced (…) since the surgical procedure to a degree where it felt prominent to you?” (yes/no)].
2. Symptoms at present, using the “Distress scale,” Edmonton Symptom Assessment System (ESAS), which is a valid and reliable tool to assist in the assessment of nine common symptoms experienced by cancer patients (21). Each symptom's severity at the time of assessment is rated from 0 to 10 (0 = symptom absent; 10 = worst possible severity; individual scores in clinical practice: 0 = none, 1–3 = mild, 4–6 = moderate, 7–10 = severe) (21, 22). We calculated sub-scores (23–25): (1) ESAS physical score (six items: pain, fatigue, nausea, drowsiness, appetite, and dyspnoea; scoring range: 0–60), (2) ESAS psychological score (two items: depression and anxiety, scoring range: 0–20), and (3) ESAS total symptom distress score (containing all nine aspects/symptoms, i.e., both physical score, emotional score, and the global item, wellbeing, scoring range: 0–90).
The needs of patients if “non-participant” or if “no offer”:
1. Engagement in physical activity independently.
2. Extent to which the patient would have liked an offer (to a high degree, to a medium degree, not at all, not certain).
Analysis
The plan for the analysis was prepared by MK and discussed with OH, AL, and UB. Analyses were performed by MK, using statistical software STATA 18.0 (StataCorp LLC, TX, USA).
Descriptive analyses
Initially, we described the overall included study cohort. Continuous data were described as mean ± standard deviation and categorical data were described with the number and percentage. Differences between groups were tested using Student's t-test (two-tailed), paired-samples t-test, χ2, or Fischer's exact test. Statistical significance was reached at p < 0.05.
Analyses and sub-group analyses
We performed stratified analyses to investigate characteristics in the overall study cohort and sub-groups related to study outcomes and hypotheses:
1. Availability, uptake/acceptance, and content of the offer [stratified into (a) received offer (yes/no), (b) acceptance of the offer (i.e., “non-participant” vs. “participant”].
2. Attendance rate and dropout rate [stratified in “low attendance rate or dropout” (i.e., less than 74% attendance or dropout during the programme) vs. “high attendance rate” (i.e., 75% attendance rate or more) consistent with previous reported rehabilitation attendance rates (26)].
3. Perceived benefits and relevance related to the quality of the offer (i.e., content and delivery).
4. Symptom burden after the surgical procedure and at present.
The STROBE statement checklist for cohort studies was consulted for the reporting of the data.
Results
Characteristics
Participants
The participant flow is depicted in Figure 1. Initially, 128 patients were approached; however, 13 were not reachable. Out of the 115 who were reachable (90%), 100 patients provided consent and were included in the study (87% of 115). The participants represented two Danish regions [Southern Region: n = 68 (68%); Zealand Region: n = 23 (32%)] and, in total, 35 municipalities (Supplementary Table S1). Across the total cohort included there was an equal distribution between men and women (44% vs. 56%) with a mean age of 72 ± 8; a mean BMI of 27 ± 5, and a mean pre-operative FEV1% of 47 ± 20 (Supplementary Table S1).
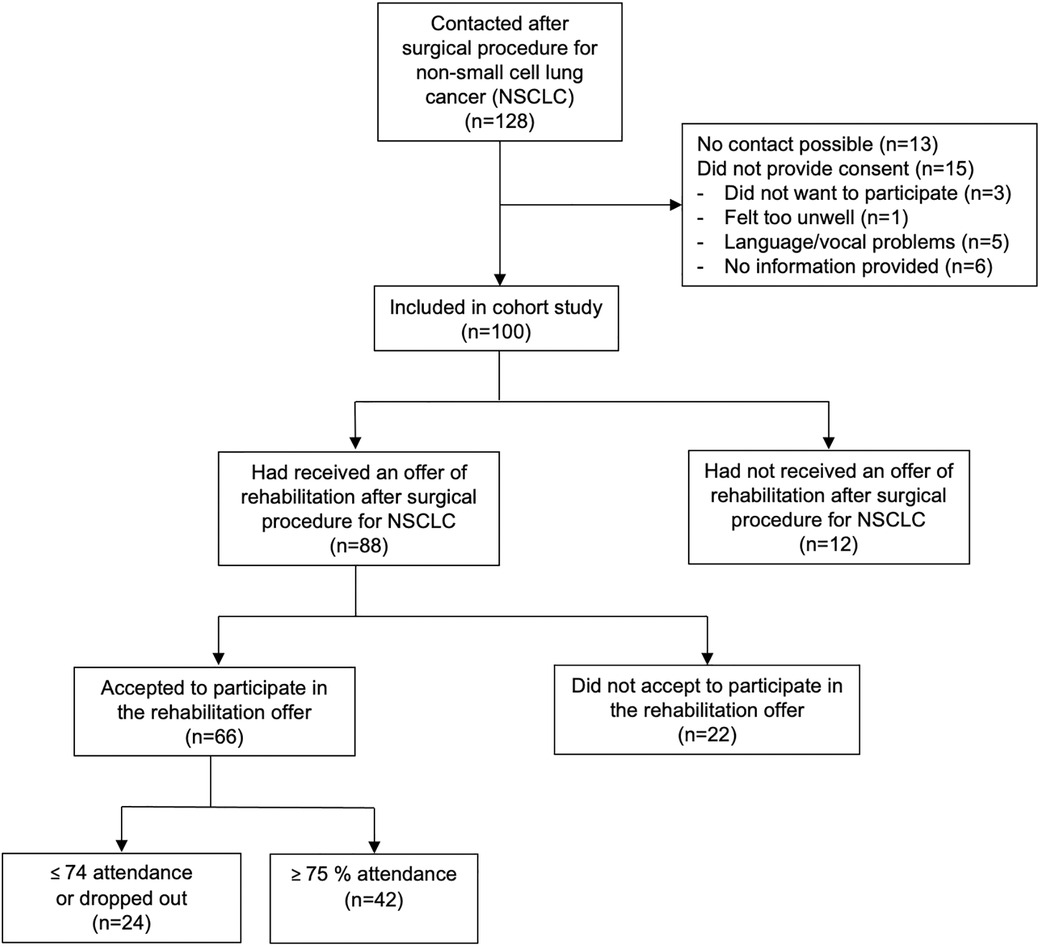
Figure 1. Cohort flow diagram.
The current rehabilitation offers
Table 1 shows that out of the 88 (88% of 100) who had received an offer of rehabilitation in primary care, 66 (75% of 88) had accepted the offer (i.e., were a participant) (see Figure 1). The vast majority (93%) were contacted by their municipality and most (80%) were contacted within 14 days of the operation.
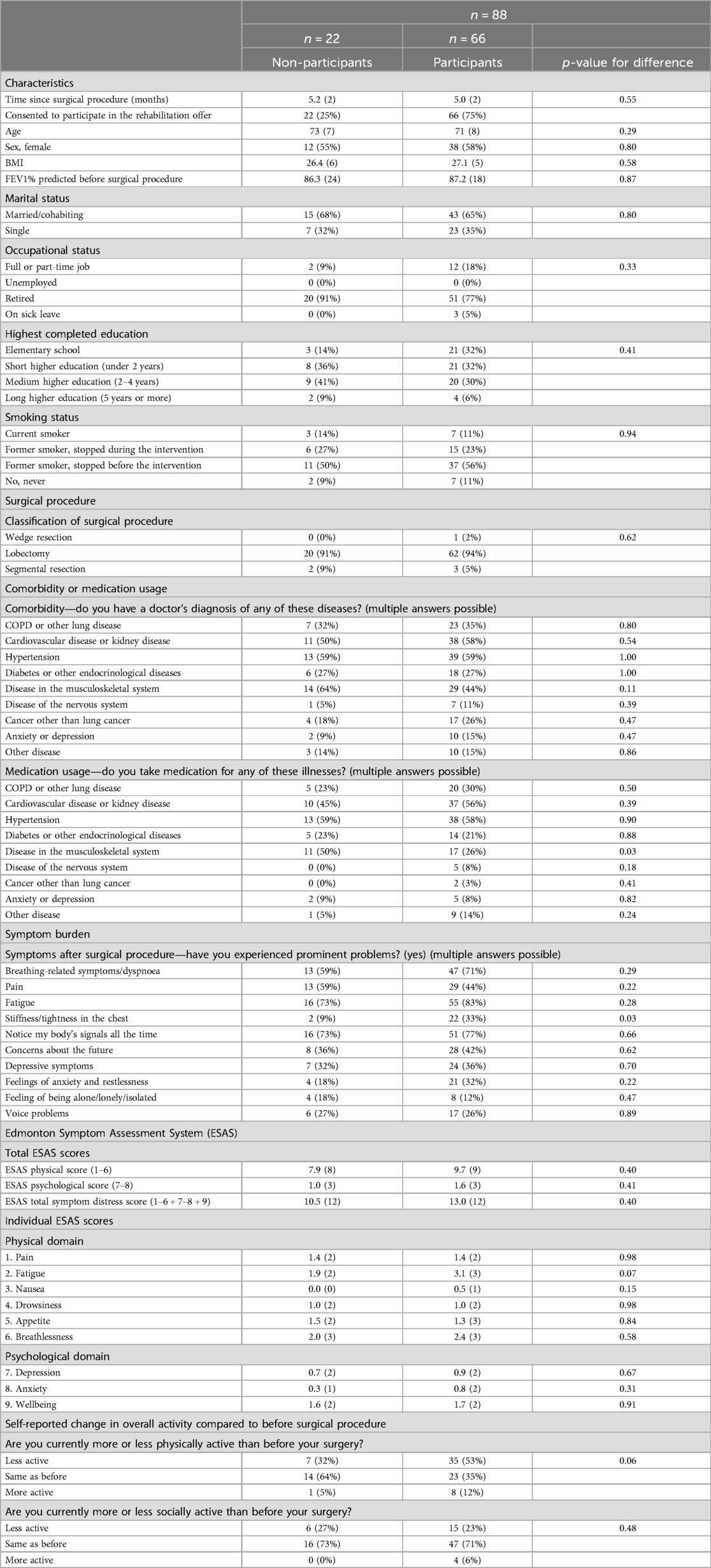
Table 1. Characteristics, symptom burden, and activity in non-participants vs participants.
As depicted in Table 2, the majority of the participants (n = 66) started rehab within a month after surgery (71%). Most often, the rehabilitation offer was delivered in a community-based healthcare centre (86%). For 30 (46%) participants, the programme lasted 6–12 weeks but was longer for 29 (45%). A frequency of “more than once a week” was reported by 75% and “once a week” by 14%. The type of rehabilitation offer varied between a special offer that targeted lung cancer (23%), mixed cancer rehabilitation (33%), pulmonary rehabilitation (12%), online (2%), or other (including at home with instructions from a physiotherapist, with other diseases, or not specified) (33%). We observed no overall differences between non-participants and participants (Tables 2, 3).
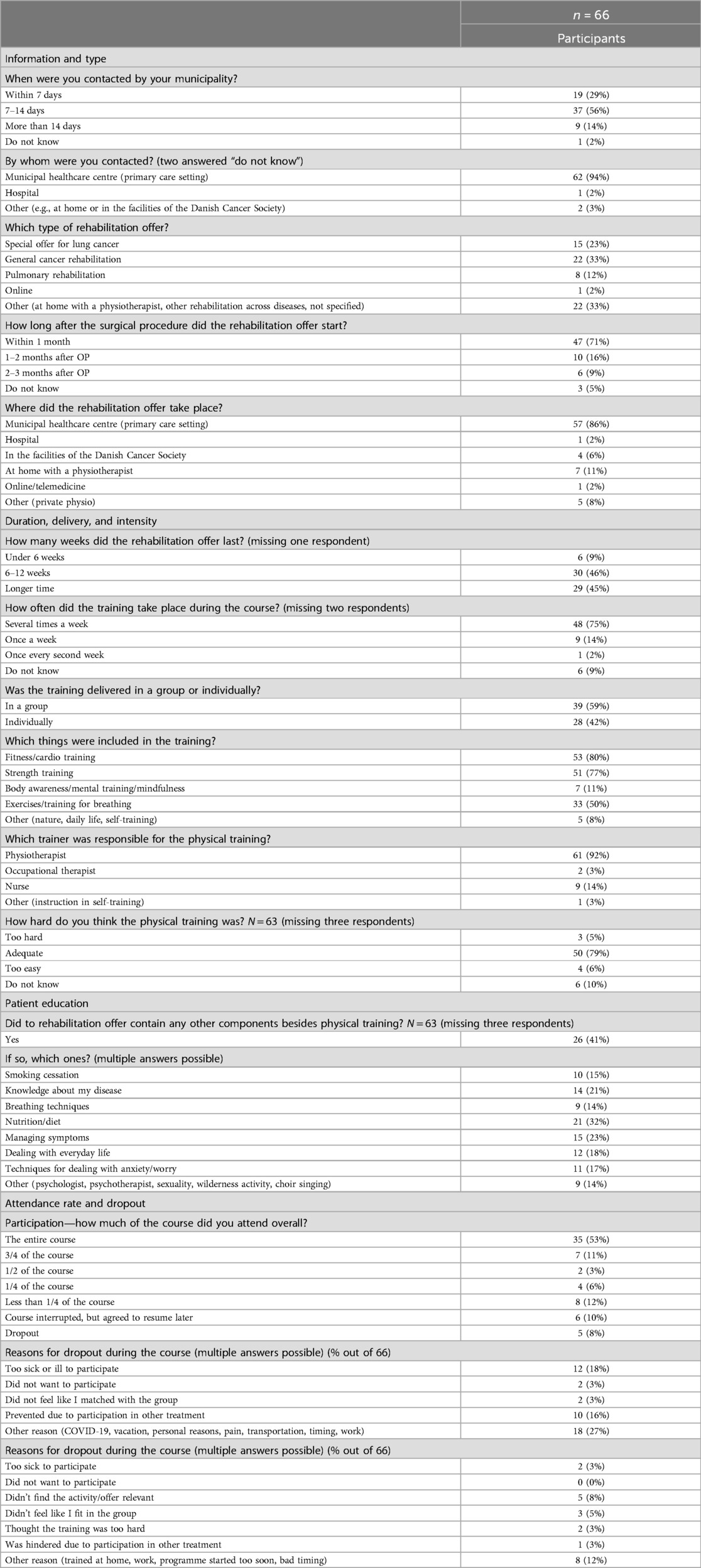
Table 2. Characteristics of the rehabilitation offers provided to participants.
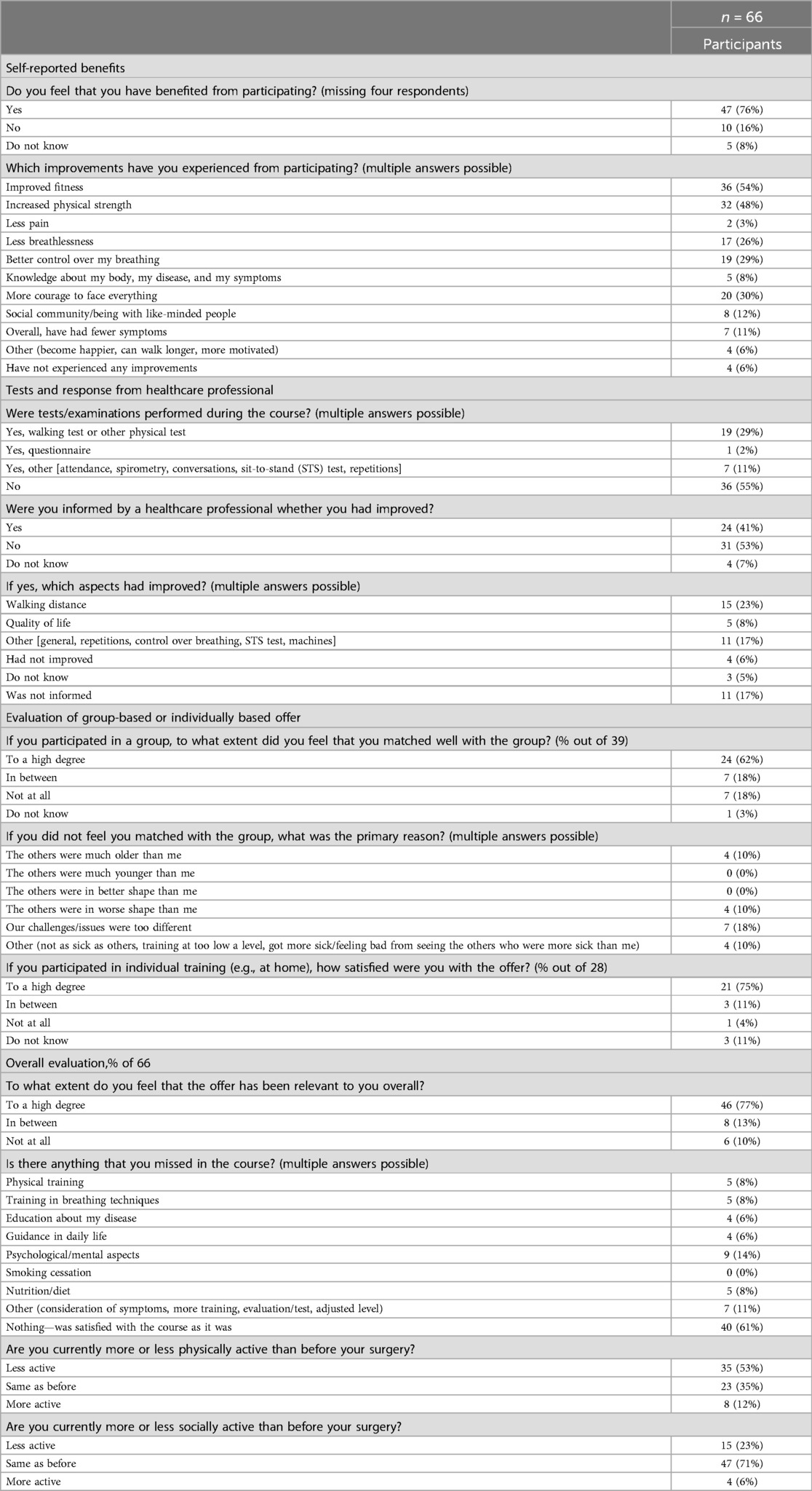
Table 3. Benefits and evaluation of the offer provided to participants.
Primary study outcome
Attendance rate related to type, content, and delivery, to perceived benefits, and to relevance of the rehabilitation offer
Table 4 shows that a high attendance rate was related to the type, content, and delivery of the rehabilitation offer. Among those with high attendance, a larger proportion was offered a disease-specific offer (high: 31% vs. low or dropout: 8%; p = 0.04), the offer was delivered more often delivered by a physiotherapist (98% vs. 83%; p = 0.04), and the offer more often comprised physical exercise components more often (fitness: 88% vs. 67%; p = 0.04, strength: 86% vs. 62%; p = 0.03).
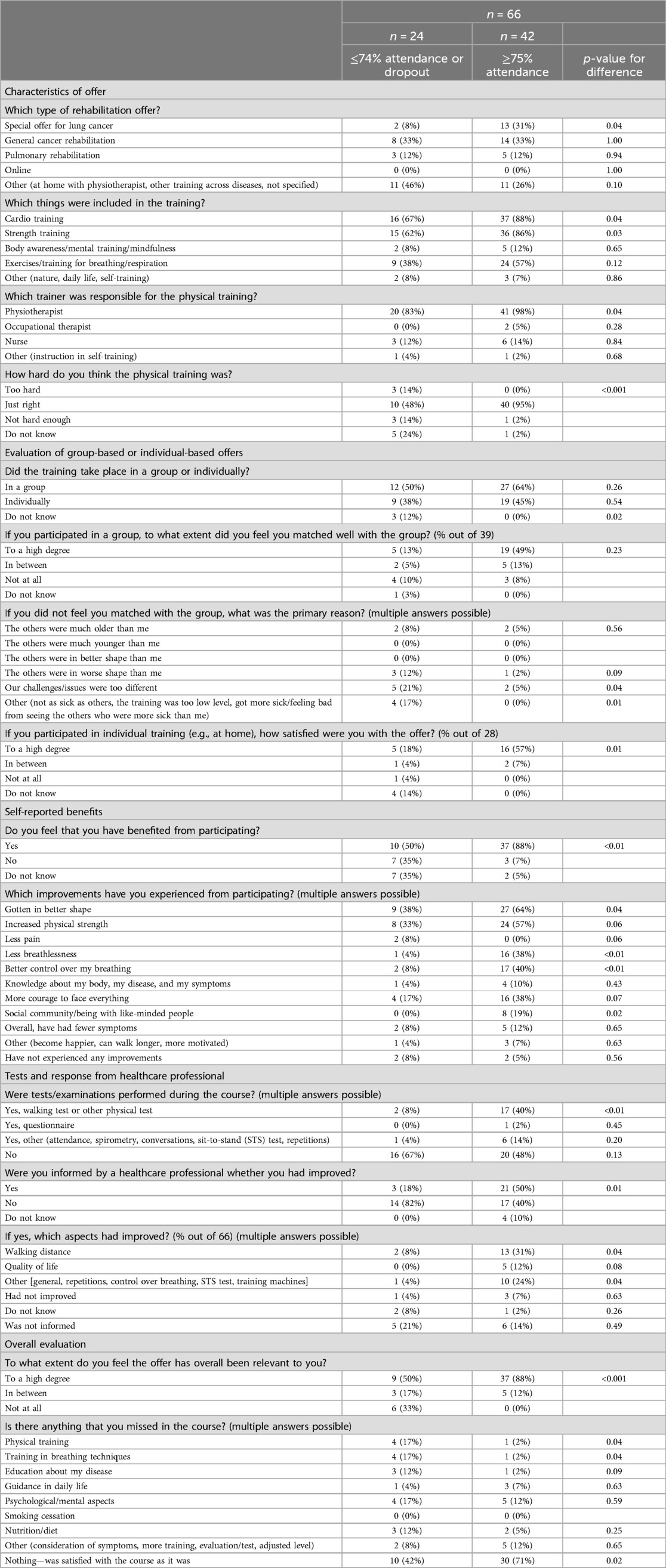
Table 4. Benefits and evaluation of the offer related to low vs high attendance.
In addition, a high attendance rate was related to perceived benefits (88% vs. 50%; p ≤ 0.01), including improved fitness (64% vs. 38%; p = 0.04), less dyspnoea (38% vs. 4%; p ≤ 0.01), enhanced breathing control (40% vs. 8%; p ≤ 0.01), and positive socialising with peers (19% vs. 0%; p = 0.02) (Table 4). A larger proportion of those with a high attendance rate had performed a walking distance test compared to those with a low attendance rate or who had dropped out (40% vs. 8%; p ≤ 0.01). Furthermore, a greater proportion of those with a high attendance rate had been informed by a health professional about any improvements (50% vs. 18%; p = 0.01) and had improved their walking distance during the programme (31% vs. 8%; p = 0.04).
There was no difference between group-based and individual-based delivery (p = 0.23), but fewer of those with a low attendance rate or who had dropped out found that they matched well with the other participants in their group (p = 0.04; p = 0.01) and fewer were content with individual-based delivery (18% vs. 57%; p = 0.01). Furthermore, fewer of those with a low attendance rate or who had dropped out found the intensity and load appropriate (48% vs. 95%; p ≤ 0.001), fewer were satisfied with the offer (18% vs. 57%; p = 0.02), and fewer found the offer relevant (50% vs. 88%; p ≤ 0.001).
We observed no differences in characteristics between those with a high attendance rate [42 (64%)] and those with a low attendance rate or who had dropped out [24 (36%)] (Supplementary Table S2).
Secondary outcomes
Symptom burden of patients in general and at present
In the overall cohort (n = 100) (Supplementary Table S1), the most dominant symptoms that participants reported having experienced since the surgical procedure were physically oriented [dyspnoea (65%), pain (47%), fatigue (78%), vigilance (74%)], psychologically oriented [worry about the future (40%), mood/depression (35%), anxiety (29%)], and vocal problems (27%).
At present, however, no individual item in the ESAS tool was above “mild” in all the analyses, reflecting experienced symptoms “here and now” (Supplementary Table S1 and Tables 1–4). We observed no overall differences in ESAS scoring between non-participants and participants (Table 1) or between those with a high attendance rate and those with a low attendance rate or who dropped out (Table 4).
Self-reported level of physical and social activity compared to before the surgical procedure
In the overall population (n = 100), 48% reported being less physically active compared to before the surgical procedure, whereas 42% were equally active compared to before, and only 10% were more active. Regarding social activity, 25% reported being less socially active, 71% were equally active compared to before, and only 4% were more active. We observed no overall differences between non-participants and participants (Tables 2, 3), or between high attendance and low attendance or dropout (Table 4).
The needs of patients if they were a “non-participant” or if there was no offer
In non-participants and those who did not receive an offer (n = 33), 93% reported having been physically active by themselves more than once a week (88%) since the operation, however, mainly with light intensity and load (91%) (Supplementary Table S2). In those who did not receive an offer (n = 12), one (8%) would have liked an offer, two (17%) were indifferent, six (50%) would not have liked an offer, and three (25%) declared themselves to be uncertain. The majority had had a lobectomy procedure (9/12; 75%) (Supplementary Table S4).
Discussion
In this observational study, we found that attendance rate and perceived benefits and relevance were related to the type, content, and delivery of the current rehabilitation offers, which were delivered in primary care settings after surgical resection for localised NSCLC.
The majority of study participants were invited to participate in rehabilitation (88%) (Table 1), which is in line with the current guidelines (16). It remains unclear why 12 (8% out of 100) apparently reported not having received an invitation for a rehabilitation offer. As was hypothesised, the rehabilitation type and focus were heterogeneous in our study, and only less than one in four received disease-targeted (lung cancer) rehabilitation (Table 2). However, it has previously been addressed that the needs of patients with lung cancer are different from other cancer types, which means that only a disease-specific rehabilitation offer will encompass all relevant aspects (10, 19, 20). Another aspect was the content and delivery of the offers, and we found that a relevant means to define a “high-quality” offer would be whether the offers were disease-specific, comprised physical exercise components, were delivered by physiotherapists, and included measurements and evaluations of the patient’s progress since the programme baseline. In line with our hypotheses, a high attendance rate was related to each of these components (Table 4). At the same time, a high attendance rate was related to the perceived benefits related to physical components, respiratory components, psychosocial aspects, and to whether the participants had found the programme relevant, suitable, and satisfactory. As adherence level and dropout remain persistent challenges (8, 18, 27, 28), these findings support the need to establish disease-specific and “high-quality” rehabilitation programmes with perceived relevant content and outcomes for this particular patient group (10, 19, 20). Exercise training is the gold standard activity across all rehabilitation programmes (5, 18, 27, 29), although a 2018 systematic review by Sommer et al. found only “low quality” evidence regarding exercise capacity and the physical component of HRQoL (5). In contrast, a Cochrane review found “high-quality” evidence regarding exercise capacity, suggested improvements in the physical component of HRQoL, and, moreover, suggested decreased dyspnoea (although with “very low quality” evidence) (15).
Well-known barriers in rehabilitation include lack of motivation and ability to perform physical exercise training. Nevertheless, exercise training is highly significant in improving or preserving physical activity and functional capacity (30), although a 360° approach is needed as, for example, emotional aspects are also important to consider (20). In our study, we found that common reasons for declining to participate included feeling that the rehabilitation offer was not suitable and that the participants could not identify with the other participants in the programme (Supplementary Table S2). Notably, a larger proportion of those with a low attendance rate or who dropped out specifically reported that they did not feel that they matched with the other participants in the group, compared to those with a high attendance rate (Table 4). Therefore, we greatly anticipate the results of the international Delphi consensus study to guide preferred outcomes and measures to further develop and evaluate future disease-specific high-quality rehabilitation programmes for people with lung cancer (19).
In addition, we encourage the investigation of other non-pharmacological and evidence-based activities as supplements or alternatives to exercise training for those who cannot or will not perform exercise training, both within the course of a rehabilitation programme and after the programme. A patient-centred approach may stimulate engagement in relevant and motivational activities and may address both physiological and psychosocial aspects (18, 19, 28, 31). As an example, we recently demonstrated that singing, delivered as a structured training modality, conferred measurable improvements in physical capacity and quality of life equally to physical exercise training and in a dose-response manner within a 10 weeks' community-based pulmonary rehabilitation programme for people with COPD (26, 32). Furthermore, singing may be related to improved respiratory muscle strength and coordination and to improved dyspnoea control (33). Interestingly, an editorial in The European Respiratory Journal suggested that engagement in an activity such as singing may build confidence to participate in exercise training at a later point, either within a rehabilitation programme or independently (34). To further investigate the potential of singing as a structured training modality, we are currently planning a multicentre randomised controlled trial on the effects of singing on exercise capacity, QoL, and symptom burden, specifically for people with NSCLC.
To define the optimal content and delivery of a future disease-specific rehabilitation offer, it is essential to gain further knowledge about the current symptom burden of the patients. In this study, participants reported that they had had multiple symptoms early after the surgical procedure (Table 1 and Supplementary Tables S1, S2), which is in keeping with previous studies in which especially physically oriented symptoms were observed (10, 11). However, we only observed “mild” symptoms from the ESAS questionnaire (21, 22). One explanation for this discrepancy could be that the ESAS questionnaire specifically asks about the symptoms “here and now,” which may influence the participants’ interpretation of the questions. Another explanation could be that lung cancer resection is increasingly often performed as less invasive video- or robot-assisted thoracoscopic surgery, which is associated with a lower symptom burden and better long-term outcomes than open thoracotomy (11, 35), leading to lower participation in rehabilitation and healthy responder selection bias (36). Nevertheless, a less time-specific tool to evaluate symptom burden would likely have to be more relevant, such as the EORTC 30-item Quality of Life Questionnaire (QLQ-C30) (37, 38), which has also been previously been applied in a Danish context and which demonstrated that a proportion of patients had long-term symptoms after a surgical procedure for NSCLC (11).
Notably, a pivotal aspect in the management of lung cancer is smoking cessation (10, 39). In the present study, 15% were currently smokers and 23% had stopped smoking during the programme (Supplementary Table S1). Nevertheless, only 15% reported that smoking cessation was included in the rehabilitation programme (Table 2). This underlines the need to include smoking cessation in future rehabilitation programmes to support smoking cessation and to prevent patients from taking up smoking again (10).
Strengths and limitations
Overall, the present study provides important knowledge for future research and for the further development of relevant and motivating rehabilitation programmes to support patients after a surgical procedure for NSCLC.
Our study has several strengths: First, to our knowledge, this is the first study to investigate the availability, uptake, attendance rate, dropout, and the type, content, and delivery of current rehabilitation offers in a real-life study. Second, the study is based on patient-reported data regarding content and perceived benefits and relevance, reflecting actual patient perspectives outside the scope of research and guidelines. Third, we included important perspectives about the symptom burden after the surgical procedure. Fourth, we included a large proportion of study participants and, overall, found consistency in our findings and with the existing literature. This may all contribute to the generalisability and credibility of the study.
The study also has several limitations. First, it was an observational study and the inclusion of patient perspectives regarding availability, uptake, attendance rate, dropout, and regarding type, content, and delivery may lead to recall bias. Second, the inclusion of only self-reported and subjective data may lead to a risk of design and recall bias. Third, the quality of reporting solely relies on patient-reported perceptions and interpretations and may not correspond to the perspectives and evaluations of health professionals.
Conclusion
Rehabilitation after surgical resection for non-small cell lung cancer is delivered heterogeneously in Denmark with less than 25% receiving a disease-specific rehabilitation offer. Nevertheless, a disease-specific and high-quality rehabilitation programme was positively related to a high attendance rate, to reported benefits, and to perceived relevance of the offer.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the head of Department of Cardiac, Thoracic and Vascular Surgery, Odense University Hospital, the hospital director of Lillebaelt Hospital, and Southern Region of Denmark (J.nr.24/511). The studies were conducted in accordance with the local legislation and institutional requirements. As the study was based on a survey and was a clinically affiliated project, the local ethics committee required no formal application, and written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin.
Author contributions
MK: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. UB: Resources, Validation, Writing – review & editing. AL: Conceptualization, Resources, Validation, Writing – review & editing. EJ: Conceptualization, Resources, Validation, Writing – review & editing. OH: Conceptualization, Project administration, Resources, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article from Danish Health Foundation: 21-B-0081, Danish Lung Foundation's Research Fund: A47, The Danish National Research Center for Lung Cancer, Danish Cancer Society: AP5; AP9, Region Zealand: R22A622, Danish Cancer Society: R355-A20616-23-S3 and Novo Nordisk Foundation: 0083460.
Acknowledgments
The authors would like to thank all study participants for their willingness to participate in the study. We also thank project nurses Lene Kjærgård Horsted and Bente Grøn, Respiratory Research Unit, Department of Medicine, Hospital Lillebaelt, Vejle Hospital, for their efforts in relation to data collection.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fresc.2024.1447767/full#supplementary-material
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. (2018) 68(6):394–424. doi: 10.3322/caac.21492
2. Gouliaev A, Hilberg O, Christensen NL, Rasmussen T, Ibsen R, Løkke A. Comorbidity among Danish lung cancer patients before and after initial cancer diagnosis. Eur Clin Respir J. (2021) 8(1):1861579. doi: 10.1080/20018525.2020.1861579
3. Gibson GJ, Loddenkemper R, Sibille Y, Society ER, Lundbäck B. The European Lung White Book: Respiratory Health and Disease in Europe. Sheffield: European Respiratory Society (2013). Available online at: https://books.google.dk/books?id=-C_fnQEACAAJ
4. Dansk Lunge Cancer Gruppe. Lungecancer—Visitation, Diagnose, Stadie. Copenhagen: Klinisk Retningslinje│Kræft (2020) Version 2.0. Available online at: https://www.lungecancer.dk/wpcontent/uploads/2020/12/DLCG_visitation_diagn_stadie_AdmGodk141220.pdf
5. Sommer M, Staerkind M, Christensen J, Vibe-Petersen J, Larsen K, Pedersen J, et al. Effect of postsurgical rehabilitation programmes in patients operated for lung cancer: a systematic review and meta-analysis. J Rehabil Med. (2018) 50(3):236–45. doi: 10.2340/16501977-2292
6. Jakobsen E, Rasmussen TR, Green A. Mortality and survival of lung cancer in Denmark: results from the Danish lung cancer group 2000–2012. Acta Oncol (Madr). (2016) 55(sup2):2–9. doi: 10.3109/0284186X.2016.1150608
7. Dansk Lunge Cancer Gruppe. DLCG. Lungecancer—kirurgisk Behandling. Copenhagen: Kliniske Retningslinjer|KrÆft (2020). Available online at: https://www.lungecancer.dk/wp-content/uploads/2020/05/DLCG_Kirurgisk-behandling_v.2.0_AdmGodk150520.pdf
8. Nwosu AC, Bayly JL, Gaunt KE, Mayland CR. Lung cancer and rehabilitation—what are the barriers? Results of a questionnaire survey and the development of regional lung cancer rehabilitation standards and guidelines. Support Care Cancer. (2012) 20(12):3247–54. doi: 10.1007/s00520-012-1472-1
9. Illini O, Valipour A, Gattinger D, Petrovic M, Fabikan H, Hochmair MJ, et al. Effectiveness of outpatient pulmonary rehabilitation in patients with surgically resected lung cancer: a retrospective real-world analysis. Cancers (Basel). (2022) 14(14):3479. doi: 10.3390/cancers14143479
10. Borg M, Lokke A, Rasmussen TR. Symptoms and lung function follow-up after lung cancer resection. Dan Med J. (2021) 68(10):A02210115.34558410
11. Bendixen M, Jørgensen OD, Kronborg C, Andersen C, Licht PB. Postoperative pain and quality of life after lobectomy via video-assisted thoracoscopic surgery or anterolateral thoracotomy for early stage lung cancer: a randomised controlled trial. Lancet Oncol. (2016) 17(6):836–44. doi: 10.1016/S1470-2045(16)00173-X
12. Sundhedsstyrelsen. Pakkeforlob for lungekraft. For fagfolk. Elektronisk ISBN nr.: 978-87-7014-022-5. Version 2.1. (2018). Danish Health Authority. Available online at: https://www.sst.dk/-/media/Udgivelser/2018/Lungekraeft/Pakkeforlob-forlungekraft-2018.ashx?sc_lang=da&hash=0312B32A6CB7E1473CA0DE4D38877BA5
13. Bradley A, Marshall A, Stonehewer L, Reaper L, Parker K, Bevan-Smith E, et al. Pulmonary rehabilitation programme for patients undergoing curative lung cancer surgery. Eur J Cardiothorac Surg. (2013) 44(4):e266–71. doi: 10.1093/ejcts/ezt381
14. Shannon VR. Role of pulmonary rehabilitation in the management of patients with lung cancer. Curr Opin Pulm Med. (2010) 16(4):334–9. doi: 10.1097/MCP.0b013e32833a897d
15. Cavalheri V, Burtin C, Formico VR, Nonoyama ML, Jenkins S, Spruit MA, et al. Exercise training undertaken by people within 12 months of lung resection for non-small cell lung cancer. Cochrane Database Syst Rev. (2019) 6(6):CD009955. doi: 10.1002/14651858.CD009955.pub3
16. Bjerno Nielsen DM, Bilde L. Temarapport om viden om kvalitet i kraftpatientforlob. Rehabilitering og palliative indsatser i forbindelse med kraft. Copenhagen: Kraftens Bekampelse (Danish Cancer Society) (2021). ISBN 978-87-7064-435-8. Available online at: https://mediebibliotek.cancer.dk/m/49eba58b3f34e8d4/original/Rehabiliteringog-palliative-indsatser-rapport.pdf
17. Rochester CL, Vogiatzis I, Holland AE, Lareau SC, Marciniuk DD, Puhan MA, et al. An official American thoracic society/European respiratory society policy statement: enhancing implementation, use, and delivery of pulmonary rehabilitation. Am J Respir Crit Care Med. (2015) 192(11):1373–86. doi: 10.1164/rccm.201510-1966ST
18. Holland AE, Cox NS, Houchen-Wolloff L, Rochester CL, Garvey C, ZuWallack R, et al. Defining modern pulmonary rehabilitation. An official American thoracic society workshop report. Annals ATS. (2021) 18(5):e12–29. doi: 10.1513/AnnalsATS.202102-146ST
19. Edbrooke L, Granger CL, Francis JJ, John T, Kaadan N, Halloran E, et al. Rehabilitation outcomes for people with lung cancer (UNITE): protocol for the development of a core outcome set. BMJ Open Resp Res. (2023) 10(1):e001571. doi: 10.1136/bmjresp-2022-001571
20. Morrison EJ, Novotny PJ, Sloan JA, Yang P, Patten CA, Ruddy KJ, et al. Emotional problems, quality of life, and symptom burden in patients with lung cancer. Clin Lung Cancer. (2017) 18(5):497–503. doi: 10.1016/j.cllc.2017.02.008
21. Chang VT, Hwang SS, Feuerman M. Validation of the Edmonton symptom assessment scale. Cancer. (2000) 88(9):2164–71. doi: 10.1002/(SICI)1097-0142(20000501)88:9%3C2164::AID-CNCR24%3E3.0.CO;2-5
22. Hui D, Bruera E. The Edmonton symptom assessment system 25 years later: past, present, and future developments. J Pain Symptom Manage. (2017) 53(3):630–43. doi: 10.1016/j.jpainsymman.2016.10.370
23. Zimmermann C, Burman D, Bandukwala S, Seccareccia D, Kaya E, Bryson J, et al. Nurse and physician inter-rater agreement of three performance status measures in palliative care outpatients. Support Care Cancer. (2010) 18(5):609–16. doi: 10.1007/s00520-009-0700-9
24. Cheung WY, Barmala N, Zarinehbaf S, Rodin G, Le LW, Zimmermann C. The association of physical and psychological symptom burden with time to death among palliative cancer outpatients. J Pain Symptom Manage. (2009) 37(3):297–304. doi: 10.1016/j.jpainsymman.2008.03.008
25. Zimmermann C, Seccareccia D, Clarke A, Warr D, Rodin G. Bringing palliative care to a Canadian cancer center: the palliative care program at princess Margaret hospital. Support Care Cancer. (2006) 14(10):982–7. doi: 10.1007/s00520-006-0093-y
26. Kaasgaard M, Rasmussen DB, Andreasson KH, Hilberg O, Løkke A, Vuust P, et al. Use of singing for lung health as an alternative training modality within pulmonary rehabilitation for COPD: a randomised controlled trial. Eur Respir J. (2022) 59(5):2101142. doi: 10.1183/13993003.01142-2021
27. Cavalheri V, Tahirah F, Nonoyama M, Jenkins S, Hill K. Exercise training for people following lung resection for non-small cell lung cancer—a Cochrane systematic review. Cancer Treat Rev. (2014) 40(4):585–94. doi: 10.1016/j.ctrv.2013.11.001
28. Oates GR, Niranjan SJ, Ott C, Scarinci IC, Schumann C, Parekh T, et al. Adherence to pulmonary rehabilitation in COPD: a qualitative exploration of patient perspectives on barriers and facilitators. J Cardiopulm Rehabil Prev. (2019) 39(5):344–9. doi: 10.1097/HCR.0000000000000436
29. Spruit MA, Singh SJ, Garvey C, ZuWallack R, Nici L, Rochester C, et al. An official American thoracic society/European respiratory society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. (2013) 188(8):e13–64. doi: 10.1164/rccm.201309-1634ST
30. Granger CL, McDonald CF, Irving L, Clark RA, Gough K, Murnane A, et al. Low physical activity levels and functional decline in individuals with lung cancer. Lung Cancer. (2014) 83(2):292–9. doi: 10.1016/j.lungcan.2013.11.014
31. Peixoto Boaventura RD, Meira L, Santos V, Gomes I, Gaspar L, Martins P, et al. Factors influencing pulmonary rehabilitation adherence—surely is not simple. In: 12 Rehabilitation and Chronic Care. Sheffield: European Respiratory Society (2016). p. PA694. doi: 10.1183/13993003.congress-2016.PA694
32. Kaasgaard M, Bech Rasmussen D, Andreasson K, Løkke A, Vuust P, Hilberg O, et al. Adherence to singing training vs. physical training in COPD rehabilitation. In: Rehabilitation and Chronic Care. Sheffield: European Respiratory Society (2021). p. PA320. doi: 10.1183/13993003.congress-2021.PA320
33. Kaasgaard M, Rasmussen DB, Løkke A, Vuust P, Hilberg O, Bodtger U. Physiological changes related to 10 weeks of singing for lung health in patients with COPD. BMJ Open Resp Res. (2022) 9(1):e001206. doi: 10.1136/bmjresp-2022-001206
34. Soriano JB, Hopkinson NS. Sing out for COPD! Eur Respir J. (2022) 59(5):2102961. doi: 10.1183/13993003.02961-2021
35. Wu H, Jin R, Yang S, Park BJ, Li H. Long-term and short-term outcomes of robot- versus video-assisted anatomic lung resection in lung cancer: a systematic review and meta-analysis. Eur J Cardiothorac Surg. (2021) 59(4):732–40. doi: 10.1093/ejcts/ezaa426
36. Enzenbach C, Wicklein B, Wirkner K, Loeffler M. Evaluating selection bias in a population-based cohort study with low baseline participation: the LIFE-adult-study. BMC Med Res Methodol. (2019) 19(1):135. doi: 10.1186/s12874-019-0779-8
37. Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et al. The European organization for research and treatment of cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. JNCI J Natl Cancer Inst. (1993) 85(5):365–76. doi: 10.1093/jnci/85.5.365
38. Bergman B, Aaronson NK, Ahmedzai S, Kaasa S, Sullivan M. The EORTC QLQ-LC13: a modular supplement to the EORTC core quality of life questionnaire (QLQ-C30) for use in lung cancer clinical trials. Eur J Cancer. (1994) 30(5):635–42. doi: 10.1016/0959-8049(94)90535-5
Keywords: rehabilitation, lung cancer, attendance rate, exercise training, quality of life, symptom burden
Citation: Kaasgaard M, Bodtger U, Løkke A, Jakobsen E and Hilberg O (2024) Attendance rate and perceived relevance related to type, content, and delivery of current rehabilitation programmes after surgical resection for non-small cell lung cancer. Front. Rehabil. Sci. 5:1447767. doi: 10.3389/fresc.2024.1447767
Received: 12 June 2024; Accepted: 5 November 2024;
Published: 10 December 2024.
Edited by:
Eleonora Volpato, Fondazione Don Carlo Gnocchi Onlus (IRCCS), ItalyReviewed by:
Liz Steed, Queen Mary University of London, United KingdomLissa Spencer, Royal Prince Alfred Hospital, Australia
Copyright: © 2024 Kaasgaard, Bodtger, Løkke, Jakobsen and Hilberg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mette Kaasgaard, bWthYXNnYWFyZEBoZWFsdGguc2R1LmRr