 Shazal Kumar Das1Md Bakhtiar2
Shazal Kumar Das1Md Bakhtiar2 Saiba Muhammad Sabrin1*Michael Curtin3Ehsanur Rahman4Zahid Bin Sultan Nahid5Zakia Rahman5Md. Furatul Haque5
Saiba Muhammad Sabrin1*Michael Curtin3Ehsanur Rahman4Zahid Bin Sultan Nahid5Zakia Rahman5Md. Furatul Haque5 Md. Fazlul Karim Patwary6Md. Jahangir Alam7Md. Emran Hossain1Md. Atiar Rahman8Shafiqul Islam9Md. Ashfaquzzaman8
Md. Fazlul Karim Patwary6Md. Jahangir Alam7Md. Emran Hossain1Md. Atiar Rahman8Shafiqul Islam9Md. Ashfaquzzaman8 Md. Anowar Khasru Parvez6*
Md. Anowar Khasru Parvez6*
- 1Department of Physiotherapy, Bangladesh Health Professions Institute, Dhaka, Bangladesh
- 2Department of Physiotherapy, Khwaja Badrudduja Modern Hospital, Gazipur, Bangladesh
- 3School of Allied Health, Exercise and Sports Sciences, Charles Sturt University, Albury, NSW, Australia
- 4Department of Physiotherapy, Jashore University of Science and Technology, Jashore, Bangladesh
- 5Department of Physiotherapy, SAIC College of Medical Science and Technology, Dhaka, Bangladesh
- 6Department of Microbiology, Jahangirnagar University, Dhaka, Bangladesh
- 7Department of Physiotherapy, Mymensingh College of Phsyiotherapy and Health Science, Mymensigh, Bangladesh
- 8Department of Physiotherapy, Centre for the Rehabilitation of the Paralysed, Dhaka, Bangladesh
- 9Department of Physiotherapy, Chittagong Medical College, Chittagong, Bangladesh
Design: Prospective, cross-sectional study.
Objectives: To determine the functional outcome and home and social integration of people who had spinal cord injury and completed their inpatient rehabilitation.
Setting: Centre for the Rehabilitation of the Paralysed (CRP), Bangladesh.
Methods: Spinal Cord Independence Measure (SCIM) and Community Integration Questionnaire (CIQ) were used to analyse the relationship between the functional outcome and home and social integration at the end of rehabilitation. Descriptive and inferential statistics were performed to analyse the data.
Results: A total of two hundred participants (181 men and 19 women) were recruited for the study. Among the participants, 92.5% of them reported a history of trauma or accident, including road traffic accidents, falls and other injuries. Approximately 60% of participants presented with paraplegia and 62.5% of participants were categorized on the ASIA Impairment Scale (AIS) as Grade A, complete spinal cord injury. Participants with paraplegia and participants with a Grade B, incomplete injury, on the AIS were functionally more independent (p = 0.011)) compared with participants with tetraplegia and other AIS grades. Participants with paraplegia reported having a more active lifestyle (p = 0.040) in their home and social activities compared to those with tetraplegia. There was no significant association found between functional independence at pre-discharged and community integration one-month post-discharge of the people with SCI.
Conclusion: A month after discharge, there is no statistically significant relationship between community reintegration and functional independence. A measure of functional independence may not be a suitable indicator of community integration. It is proposed that to monitor a person's community integration the CIQ could be used with a measure of quality of life as this would indicate a person's contentment with their level of community integration.
Introduction
A spinal cord injury (SCI) can result in significant levels of impairment and lifestyle disruption (1, 2). The functional independence of people with a SCI is significantly lower than that of the population in general as a SCI usually causes severe locomotor impairment, due to paralysis of the muscles. Depending on the level and completeness of the lesion, a person with SCI can be independent or require assistance with a range of everyday activities (3). Secondary conditions and complications, such as age, concomitant injuries, level of injury, injury mechanism, pressure ulcers, urinary and/or respiratory infections, pain, and severity of spasticity, may impact on the level of independence of a person with a SCI (4) and in turn affect the outcome of their community re-integration (5, 6).
Loni et al. (7) have suggested that because of improved medical and rehabilitation services, more people with a SCI are surviving and their life expectancy has increased. In-patient rehabilitation following a SCI focuses on assisting a person to obtain a level of functional independence (7). An effective rehabilitation program can reduce patient-associated costs (e.g., length of hospital stay), lead to some level of independence (8, 9), and enhance overall quality of life (7).
A key marker of successful rehabilitation following spinal cord injury/disease is to facilitate the transition from inpatient hospital care to being able to participate in a range of roles back in their community (10, 11). Community re-integration refers to a person with SCI being able to participate in community life and being able to effectively perform their roles in community settings (11, 12). Hitzig et al. (10, p. S80) suggests that “meaningful participation in occupations or employment and/or the ability to engage in societal roles holds significant implications for one's health and wellbeing”. Many people with SCI find it difficult to transition from the supportive and accessible environment of the hospital and inpatient rehabilitation setting back into their community (10, 13, 14).
It is suggested that to enable successful community re-integration inpatient programs need to develop the self-efficacy and ability to manage their own life of person who has had a SCI (11). Successful community re-integration requires the translation of all the skills learnt as an inpatient into the community, the acceptance of family and friends of the person's decisions and choices, support from peers, having an accessible house, be able to move around the community, participate in work, leisure, and education activities of choice, and engage in satisfying social relationships (11, 13–16). Barclay et al. (17) found that successful community integration needs to take into consideration person factors (e.g., complications from the SCI such as fatigue, incontinence), physical and institutional environmental factors (e.g., transport issues, accessibility, inadequate support services), and social and cultural environmental factors (e.g., social networks, negative social attitudes, reliance on family and friends). Furthermore, social and community participation in which the person with SCI is establishing and maintaining close relationships is key to successful community integration (13).
As the incidence of SCI is significantly higher in non-developed countries compared with developed countries (18) it is important to consider the rehabilitation outcomes for people with a SCI who live in developing countries, where there may be limited services and resources for rehabilitation and community integration. Where rehabilitation is provided for people with a SCI who live in a developing country the outcome of successful community re-integration is expected as this is a common outcome of all SCI rehabilitation programs (10, 11). In Bangladesh, the Centre for the Rehabilitation of the Paralysed (CRP), is a specialized SCI facility that admits nearly 350 people each year (19). Rahman et al. (20) found that by the end of their in-patient rehabilitation at CRP many people with SCI had a positive perception of their level of function and their QOL. However, other authors found that post-discharge people with SCI experience an increase in functional limitations and a decrease in their QOL (21–23). Hossain et al. (21) concluded that most people with SCI who were living in the community, three to six years post-discharged from CRP were housebound, jobless, living in poverty, and had pressure ulcers. As a result of these findings, it is important to investigate the community re-integration of people with SCI who have completed their rehabilitation at CRP to inform and guide better outcomes.
At CRP there has been no research to date conducted to determine the relationship between functional independence at discharge and outcome of community integration. As the level of function independence at discharge has been shown to correlate with community integration (11, 13, 14, 16), it is proposed that, knowing the functional independence of people at discharge at CRP may provide some indication of the support they will require to re-integrate into their community providing a baseline for monitoring their support needs post-discharge. The focus of this study was to establish a baseline correlation between the functional independence of a person with a SCI at the end of their inpatient rehabilitation at CRP and their community re-integration one-month post-discharge.
Research question
What is the relationship between functional independence at discharge and community integration one-month post-discharge of people with a SCI who attended in-patient rehabilitation at CRP?
Methods
Study design
A prospective cross-sectional study design was used to explore the functional outcome level of people who had SCI on completion of inpatient rehabilitation at CRP and their level of community integration (home and social) one-month post-discharge. This study was approved by the ethics committee of Centre for the Rehabilitation of the Paralysed, Bangladesh (CRP-R&E-0401-0401), and the Pabna University of Science and Technology, Pabna, Bangladesh (ERC/FBST/PUST/2022-116).
Sample size
Men and women, 18 years of age or older, who has a spinal cord injury, were at the end of their inpatient rehabilitation at CRP, and who lived in a community relatively close to CRP, were invited to participate in the study. Due to funding issues, the study was only opened to participants who lived in a community relatively close to the CRP so that they could be easily followed up in person one month post-discharge. The recruitment process of study participants spanned approximately nine months and continued until 200 people who met the inclusion criteria agreed to participate.
Measurement tools
The following demographic information was collected for each participant: age, gender, education level, marital status, employment, and type of injury. In addition, two survey instruments were used to collect data: the Spinal Cord Independence Measure (SCIM) and the Community Integration Questionnaire (CIQ).
The SCIM is a widely used instrument to measure functioning in everyday life activities of people with SCI (24). Fekete et al. (24, p. 40) stated that the main advantages of the SCIM over other functional assessments “are its sensitivity to changes in performance of tasks that are relevant for SCI patients, and the fact that it measures not only the burden of care, but also achievements, which have medical, psychological or social relevance for SCI patients”. This scale consists of 19 daily activity items arranged into three domains: mobility (9 items, scores ranging from 0 to 40), respiration and sphincter management (4 items, scores ranging from 0 to 40), and self-care (6 items, scores range from 0 to 20). A person's overall SCIM score can vary from 0 to 100, with higher scores representing better levels of competence or independence (20). The SCIM has been proven to be valid, responsive, and has excellent intra-rater and inter-rater reliability among rehabilitation professionals (25–27). Itzkovich et al. (28, p. 1926) stated that the SCIM was “an efficient measure for functional assessment of SCI patients and can be safely used for clinical and research trials”.
The CIQ provides a reliable and objective assessment of home and social integration and productive activities (29). The CIQ contains 15 items that assess community integration across three domains: home integration (scores range from 0 to 10 with questions relating to activities such as meal preparation, housework, and childcare); social integration (scores range from 1 to 12 points with questions relating to activities such as shopping, visiting friends, leisure activities); and productive activity (scores range from 0 to 7 points with questions relating to activities such as work, education, and volunteer activities) (30). A person's overall CIQ score can vary from 0 to 29 points. Gontkovsky et al. (31) found that the CIQ was a valid measure for examining community integration for people with SCI. In a systematic review conducted by Turcotte et al. (32) the CIQ was noted to have internal consistency for adults with SCI. Furthermore, Callaway et al. (29, p. 228) stated that the CIQ is frequently used in SCI research because it demonstrated “good criterion and construct validity, test-retest reliability, inter-rater reliability, and full-scale internal reliability”. For the purposes of this study only the domains of home integration and social interaction were used; hence the overall score varies from 0 to 22 points. It was decided not to include the productive activity domain because it did not match the study objectives. Higher scores indicate better community integration.
Data collection procedure
Participants were recruited to the study towards the end of their in-patient rehabilitation. The SCIM was completed just prior to discharge and the CIQ was completed one-month later. The delay in completing the CIQ was to allow each participant a month to transition from in-patient rehabilitation back into their community. The SCIM took approximately 15–20 min to complete and the CIQ took approximately 10–15 min to complete. A member of the research team asked the questions and recorded each person's responses to assist with the accurate completion of the surveys.
Data analysis
The Statistical Package for Social Sciences (SPSS), Windows version 22, (IBM, Armonk, NY, USA), was used to organize and analyse the data. Descriptive analysis, using frequency and percentage, was completed for different sociodemographic data: age, gender, education level, marital status, employment, and type of injury.
The Kolmogrov-Smirnov test was used to determine whether the SCIM and the CIQ data were normally distributed. As the data for both dependent variables did not have a normal distribution, the non-parametric inferential Mann-Whitney U and the Kruskal Wallis tests were used to analyse the data. The Mann-Whitney-U-test was used to test the homogeneity between two independent categories (i.e., age, gender, cause of injury and type of injury) (33) and the Kruskal–Wallis test was used to test the homogeneity between more than two independent categories (i.e., marital status, education, skeletal level of injury, ASIA scale, occupation and monthly income) (34).
Multiple logistic regressions were used to observe the impact of predictor variables (like socio-demographic and clinical characteristics) upon dependent variables (functional independence and community integration). Spearman correlation coefficient was performed to find the association between functional independence prior to discharge and community integration one month after discharge.
Results
Participant demographics and clinical information
Two-hundred people with SCI injuries participated in this study. The demographic and clinical characteristics of the participants are summarised in Table 1. The mean age of the participants was 35.68 ± 12.58 years. There were 181 men and 19 women respondents. Most of the participants identified as Muslim (n = 186), eleven identified as Hindu, and most of the participants were married (n = 152). Sixty participants completed primary education, 51 completed secondary school education, 23 completed higher secondary education, 25 completed a bachelor or higher degree, and the remaining 41 indicated they had not attended school. Thirty-five participants reported their occupation as farmer, 34 as day labourer, 36 as businessman, 15 as housewife, and 56 indicated they had other employment/occupations such as student, construction worker and rickshaw puller. Most of the participants had a monthly income between 100 and 200 United States Dollar (USD). Most participants had a traumatic SCI (n = 185), and 120 had a paraplegic injury. According to the American Spinal Injury Association (ASIA) Impairment Scale (AIS), 125 participants had complete A, 19 had incomplete B, 27 had incomplete C, and 29 had incomplete D spinal cord injury.
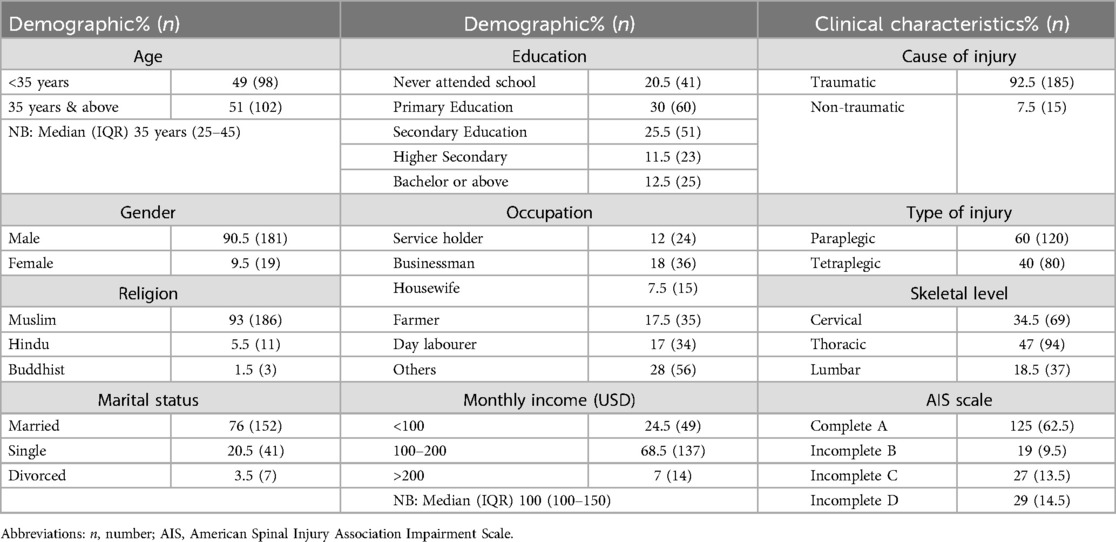
Table 1. Demographic and clinical characteristics of the participants.
The ASIA Impairment Scale (AIS) is a means of classifying the severity of SCI (35). The AIS defines a complete SCI injury as “no preservation of motor and/or sensory function more than three segments below the neurological level of injury” and an incomplete SCI injury as “some preservation of sensory and/or motor function more than three segments below the neurological level of injury” (36, p. 3–4). The AIS uses the letters A–E to distinguish the different types of neurological injuries (Table 2).
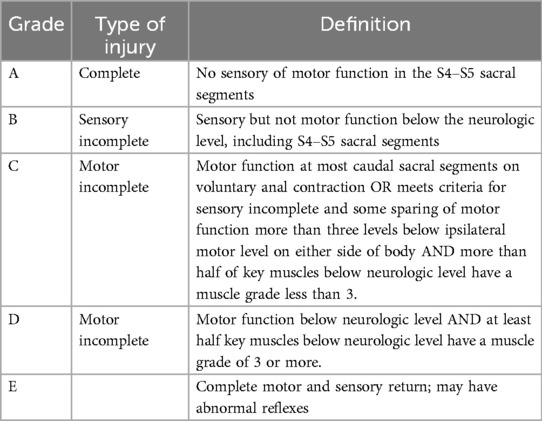
Table 2. American spinal injury association impairment scale (AIS) (35, p. 1557).
Spinal cord independence measure (SCIM)
The median score and p-value for each domain and the total score of SCIM associated with each demographic characteristic are presented in Table 3. Participants who never attended school and completed secondary and bachelor-level education had significantly higher scores with their functional independence level in the domains of self-care (p = 0.023), mobility (p = 0.013), and overall independence level. Participants with a paraplegic injury (lumbar skeletal level) had significant functional independence on mobility (p = 0.011) and overall independence (p = 0.042) measurement.
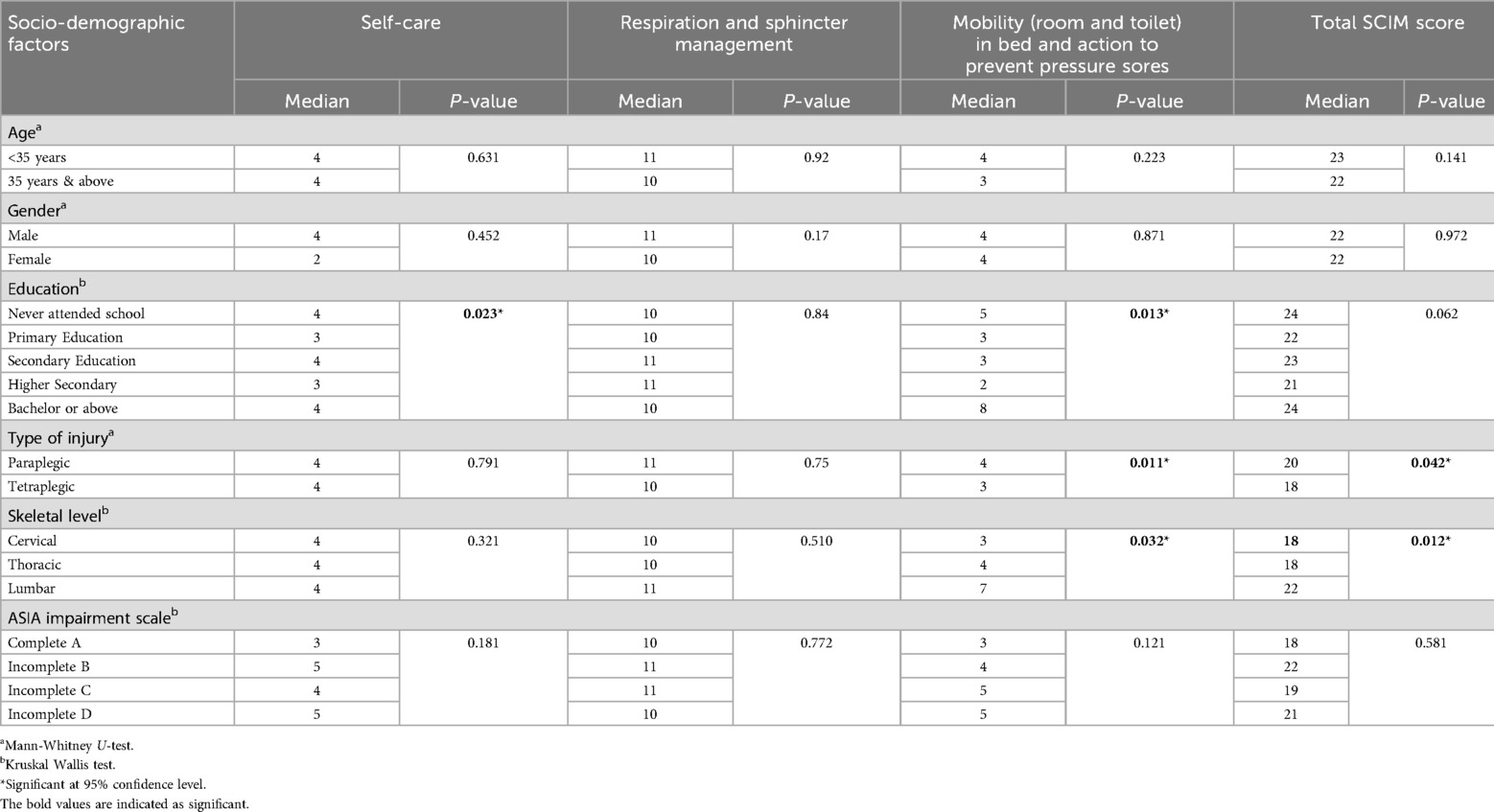
Table 3. Median scores and P-value of demographic and clinical factors for spinal cord independence measure (SCIM) domains.
Community integration questionnaire
The median score and p value for each domain score of community integration associated with each demographic characteristic are presented in Table 4. Participants with a paraplegic injury (thoracic skeletal level) and those with a complete A or incomplete B injury were significantly more independent (p = 0.013) in home integration activities such as grocery shopping, preparing meals, and childcare compared with other participants. Participants with a paraplegic injury were also significantly more independent (p = 0.040) in social integration activities such as paying bills, shopping, and visiting friends or relatives compared to those with a tetraplegic injury.
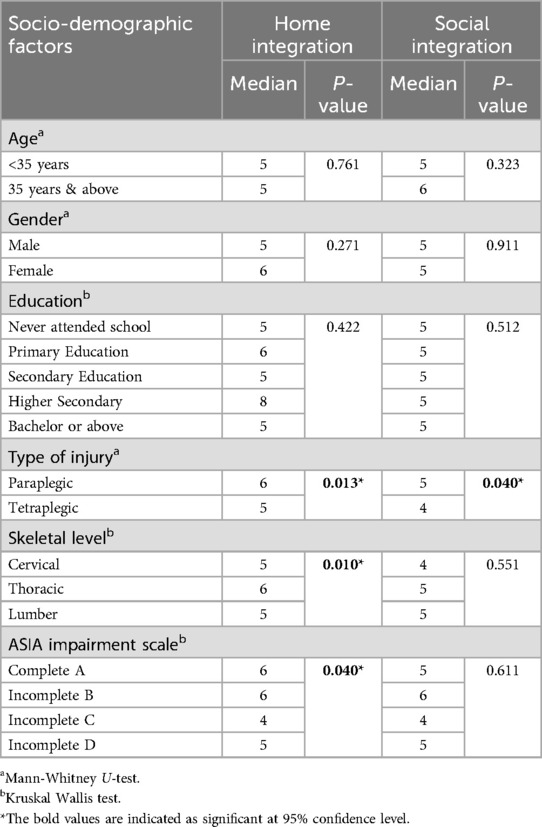
Table 4. Median scores and P-values of demographic and clinical factors for community integration questionnaire domains.
Multiple regression analysis
The multiple regression analysis of demographic and clinical variables on functional independence and community integration is presented in Table 5. Participants with a cervical [OR = 0.278, 95% CI: 0.114, 0.675] or thoracic level injury [OR = 0.398, 95% CI: 0.169, 0.935] were significantly less functionally independent compared with those with a lumbar level injury. People with a paraplegic injury were more likely to have a high level of functional independence [OR = 2.178, 95% CI: 1.380, 3.537] compared to those with a tetraplegic injury. Participants with an incomplete D SCI had higher functional independence scores [OR = 2.867, 95% CI: 1.333, 3.508] compared to those with a complete A SCI.
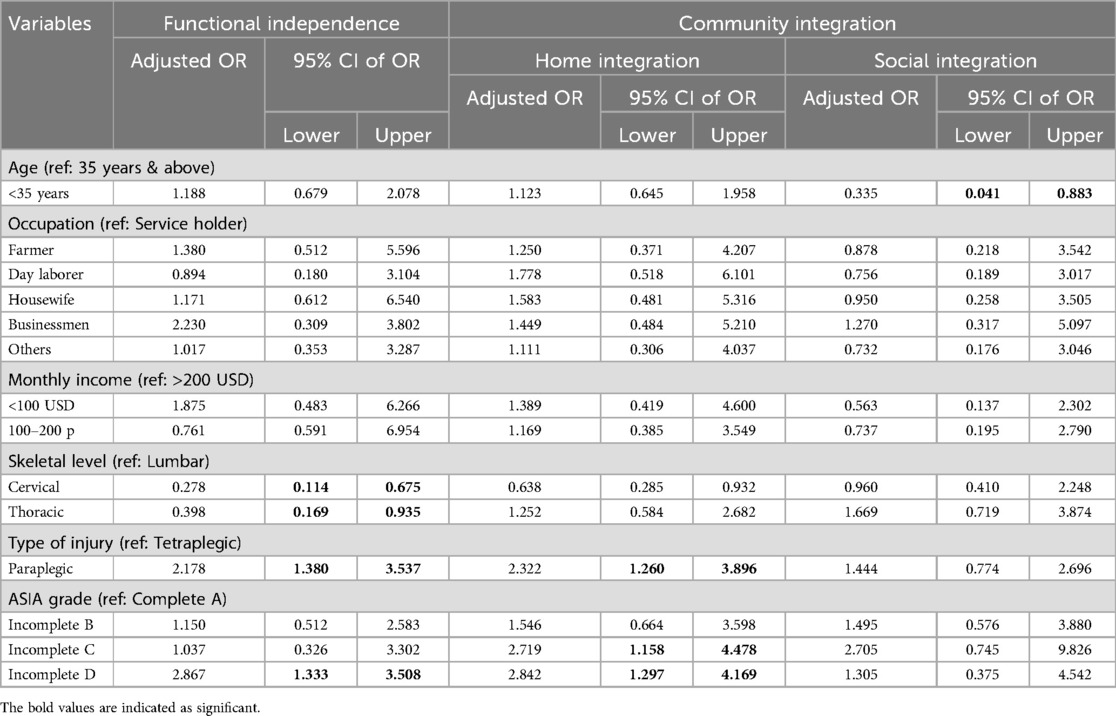
Table 5. Multiple regression analysis of demographic and clinical variables on functional independence and community integration.
Participants 35 year of age and above had significantly higher social integration compared to those below 35 years [OR 0.635: 95% CI: 0.141, 0.983]. People with a paraplegic injury were more likely to have good home integration [OR = 2.322, 95% CI: 1.260, 3.896] compared to those with a tetraplegic injury. Those with an incomplete Level C injury had significantly better home integration [OR = 2.719, 95% CI: 1.158, 4.478] compared those with a complete A SCI.
Relationship between spinal cord injury measure (SCIM) and community integration questionnaire (CIQ)
The correlation analysis of the relationship between the SCIM and CIQ is presented in Table 6. These results indicate that higher levels of functional independence did not indicate better community integration. Although the relationship was not significant the result suggests a negative correlation between overall SCIM score and scores in both domains of CIQ.
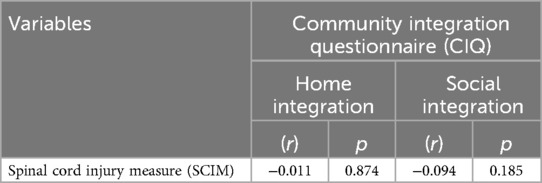
Table 6. Correlation between spinal cord injury measure (SCIM) and community integration questionnaire (CIQ) (spearman correlation coefficient).
Discussion
The aim of this study was to determine if there was a relationship between the level of functional independence and community integration of people with SCI who had completed their rehabilitation at CRP. Functional independence and community integration were considered to be important measures as they can provide an indication of how effectively a person with SCI may participate in everyday activities when back in their community (37, 38).
It was expected that there would be a positive correlation between the results of the SCIM and CIQ; however, the findings suggest a potentially negative correlation between the overall SCIM scores and scores of both domains of CIQ. Loni et al. (7) found a positive relationship between improvements in functional independence because of inpatient rehabilitation and the life satisfaction, but no significant relationship between improvements in functional independence and the total quality of life score of people with SCIs. These researchers indicated that the short time frame of their study possibly impacted the results, and that measurements of quality of life and life satisfaction would benefit from being investigated over a longer period post-rehabilitation (7). In the current study it is likely that measuring community re-integration with the CIQ one-month post-discharge does not accurately capture how successful community re-integration has been. This is because it can take longer than a month for a person who has had a SCI to recalibrate and learn how to live with a SCI when they return to their community (7, 39).
It is also possible that the concepts measured on SCIM and the CIQ are not closely related in that a person's level of physical independence may not be a key factor in determining successful community reintegration. Based on the findings in their study Loni et al. (7) suggested that “non-physical factors, such as psychological, social and emotional factors, might play a pivotal role in shaping the quality of life and life satisfaction among individuals with spinal cord injury” (p. 6). Perhaps these same non-physical factors contribute to, and impact, the effectiveness of community integration.
Although there was no relationship found between SCIM and CIQ there were other findings that required exploration. The data presented in Tables 3–5 provide a summary of the relationship between demographic and clinical variables, and functional independence and home and social integration outcomes.
Age was found to be associated with social integration. Participants below 35 years of age had lower social integration compared to those who were aged 35 years and above. This is different to other research that indicates that community and social reintegration generally declines as people with a SCI age (5, 40). Charlifue and Gerhart (5) indicated that this is in line with typical aging, and, for this reason, it is not necessarily a cause for concern if people with a SCI “report that they are content with their levels of community integration” (p. 99). The finding that participants under the age of 35 years scored lower on social participation is different to the findings of other studies. Charlifue and Gerhart (5) stated that in many communities it is “individuals who are aging, regardless of whether or not they have a disability, [that] may be marginalized and not afforded opportunities to maximize community integration” (p. 92). In Bangladesh the lower social integration score may reflect that the participants under 35 years of age felt they were a burden to their family and to society. This may be due to the potential impact the SCI has on their health, family responsibilities and employment prospects. These participants may find it more challenging to transition “from the safety of the artificial hospital environment with the associated supports, both physical and social, and [plunge] into environments that are hostile towards people with disabilities” (11, p. 3845). Hence, these participants may be initially less content with their perceived levels of community integration.
It is not surprising to find that participants with a lower-level SCI (i.e., paraplegia) had significantly higher levels of functional independence and home and social integration compared with those who had a higher level of injury (i.e., tetraplegia). These findings can be explained by the relationship between the extent of muscle paralysis and sensory loss, and the higher risk of secondary complications, such as pressure ulcers, with the limitations on a person's functional independence and community integration (41, 42). Trgovevic and Milicevic found that people who had a paraplegic injury had better achievements in “home integration in comparison to achievements in persons with tetraplegia” (43, p. 189). However, in social integration these authors found no significant different. This is different to the findings in the present study. One reason for this difference may be the context in which participants were living, with participants in Bosnia and Herzegovina (43) experiencing better, environmental, health and social-welfare conditions compared with participants in Bangladesh. In their critical review of social and community participation following spinal cord injury, Barclay et al. (11) found a statistically significant relationship “between fewer barriers and increased community integration” (p. 16). It is possible that there may be more environmental barriers that a person with spinal cord injuries must negotiate when they return to live in a community in a developing country such as Bangladesh compared to returning to live in a community in a developed country such as Bosnia and Herzegovina. In relation to secondary complications, Lala et al. (44) indicated that people with pressure ulcers found it harder to take part in community activities than people without pressure ulcers. People with tetraplegia aremore at risk of pressure ulcers, which may partially explain why they had less mobility in their own homes and in the society compared to people with paraplegia (44).
The findings suggest that the more complete the spinal cord injury the lower the levels of functional independence and home and social integration. At the completion of inpatient rehabilitation at CRP, a participant with an AIS grade D (incomplete) SCI (refer to Table 2) had better functional outcomes, and higher home and social integration than a participant with an AIS grade A (complete) SCI (refer to Table 2). This finding is consistent with other research that found people who have an incomplete SCI often have better functional outcomes compared with those with a complete SCI (45). McKinley et al. (46) and Whiteneck et al. (47) stated that, completeness of damage and degree of neurological impairment are crucial indicators of functional prognosis and social reintegration following SCI.
There was an association found between participants' educational level and the domains of self-care and mobility in bed and action to prevent pressure sores according to the results of the SCIM scale. Participants who either never attended school or who had a bachelor degree had greater independence in this domain, compared with those who had attend primary, secondary and higher education. This finding is difficult to explain and requires further investigation. No other research was found that focused on the connection between education level and functional outcomes for people with SCI.
The findings of this study must be considered in the light of several limitations. Only a small number of women were included as participants in this study. Although this may reflect the proportion of men and women who were inpatients at CRP at the time of the study, the inclusion of more women in the study would lead to greater confidence in the findings being representative of the functional independence and home and social integration of women with SCI living in Bangladesh. The generalisability of the findings is also impacted by the fact that this study was conducted at only one institute in one country. A further limitation is that the SCIM was completed at the end of rehabilitation and the completion of the CIQ was at one-month post-discharge. Hence, the findings only provide a baseline for functional outcome and community integration measures at around the time of discharge.
Future research could focus on following up participants at regular intervals post-discharge to monitor their home and social integration to identify any factors that may impact on a person's community integration over time. There is some evidence to suggest that a person's functional independence, as determined by the SCIM, is relatively stable over time (48). However, although functional independence may be stable, a person's community integration could change over time, particularly because of secondary complications and ageing (5, 21, 23). As functional independence may not be a suitable indicator of community integration it may be more relevant to monitor community integration along with other factors, such as perceptions of quality of life as was done my Moller et al. (48) and proposed by Rahman et al. (20), to identify support and intervention needs of people with SCI post-discharge. There would be benefit in increasing the proportion of women who participate in the study to determine if there are functional independence and/or social and home integration outcomes that are more specific to women.
Conclusion
Although no statistically significant relationship was found between functional independence and community integration one month post-discharge, the findings from this study provide a baseline for measuring and monitoring the level of functional independence and community integration of people with SCI who completed their rehabilitation at CRP. The level of functional independence was related to the level and completeness of spinal cord injury, and age and level of education were factors identified as having a significant relationship with level of home and social community integration. It has been suggested that functional independence may not change over time; however, the level of community integration may change due to multiple factors including age, secondary complications, social support, and quality of life. This could mean that a measure of functional independence is not a reliable indicator of community integration. To objectively monitor a person's community integration over time post-discharge it may be more relevant to use a tool such as the CIQ, with a measure of their QOL and/or life satisfaction. This would at least provide a measure of a person's contentment with their life that can be considered alongside their community integration outcomes. This may contribute to identifying any support and interventions a person may require that will contribute to successful community integration.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Centre for the Rehabilitation of the Paralysed, Bangladesh (CRP-R&E-0401-0401), and Pabna University of Science and Technology, Pabna, Bangladesh (ERC/FBST/PUST/2022-116). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
SD: Conceptualization, Methodology, Writing – review & editing. MdB: Writing – review & editing, Methodology. SS: Formal Analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing. MC: Writing – original draft, Writing – review & editing. ER: Investigation, Methodology, Writing – original draft, Writing – review & editing. ZN: Conceptualization, Writing – review & editing. ZR: Writing – review & editing. MdFH: Methodology, Software, Writing – review & editing. MdFKP: Formal Analysis, Writing – review & editing. MdJA: Methodology, Writing – review & editing. MdEH: Writing – review & editing. MdAR: Writing – review & editing. SI: Writing – review & editing. MdA: Writing – review & editing. MdAKP: Conceptualization, Methodology, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We are very thankful to all the participants for the voluntary participation. Also, we truly acknowledge the assistance of Proshoun Rakshit Himel and Shahid Afridi. SKD is the PhD student of Department of Pharmacy at Pabna University of Science and Technology, Pabna, Bangladesh.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Kawanishi CY, Greguol M. Physical activity, quality of life, and functional autonomy of adults with spinal cord injuries. Adapt Phys Activ Q. (2013) 30(4):317–37. doi: 10.1123/apaq.30.4.317
2. World Health Organization, & International Spinal Cord Society. International Perspectives on Spinal Cord Injury. Geneva: World Health Organization (2013).
3. Varghese G, Al Yazeedi W, Al Hamawi M, Awad MN, Ferriero G, Giovanazzi E. Spinal cord injury following a mild trauma in homocystinuria-related bone frailty: neurorehabilitation and education on bone health management. Int J Rehab Res. (2017) 40(4):374–76. doi: 10.1097/MRR.0000000000000246
4. Middleton JW, Truman G, Geraghty TJ. Neurological level effect on the discharge functional status of spinal cord injured persons after rehabilitation. Arch Phys Med Rehabil. (1998) 79(11):1428–32. doi: 10.1016/S0003-9993(98)90239-8
5. Charlifue S, Gerhart K. Community integration in spinal cord injury of long duration. NeuroRehabilititation. (2004) 19:91–101. doi: 10.3233/NRE-2004-19203
6. Levi R, Hultling C, Nash MS, Seiger Å. The Stockholm spinal cord injury study: 1. Medical problems in a regional SCI population. Spinal Cord. (1995) 33(6):308–15. doi: 10.1038/sc.1995.70
7. Loni E, Ghorbanzadeh M, Layeghi F, Moein S, Bahiraee M, Bidhendi-Yarandi R. Effective of inpatient rehabilitation on the quality of life and life satisfaction in spinal cord injury. J Spinal Cord Med. (2024):1–7. doi: 10.1080/10790268.2024.2362501
8. Schwartz CE, Stucky B, Rivers CS, Noonan VK, Finkelstein JA, Network R. Quality of life and adaptation in people with spinal cord injury: response shift effects from 1 to 5 years postinjury. Arch Phys Med Rehabil. (2018) 99(8):1599–608. doi: 10.1016/j.apmr.2018.01.028
9. Truchon C, Fallah N, Santos A, Vachon J, Noonan VK, Cheng CL. Impact of therapy on recovery during rehabilitation in patients with traumatic spinal cord injury. J Neurotrauma. (2017) 34(20):2901–9. doi: 10.1089/neu.2016.4932
10. Hitzig S, Jeyathevan G, Farahani F, Noonan V, Linassi G, Routhier F, et al. Development of community participation indicators to advance the quality of spinal cord injury rehabilitation: SCI-high project. J Spinal Cord Med. (2021) 44(Sup 1):S79–93. doi: 10.1080/10790268.2021.1955204
11. Barclay L, Robins L, Migliorini C, Lalor A. Community integration programs and interventions for people with spinal cord injury: a scoping review. Disabil Rehabil. (2021) 43(26):3845–55. doi: 10.1080/09638288.2020.1749889
12. Willer B, Rosenthal M, Kreutzer J, Gordon W, Rempel R. Assessment of community integration following rehabilitation for traumatic brain injury. J Head Trauma Rehabil. (1993) 8:75–87. doi: 10.1097/00001199-199308020-00009
13. Barclay L, McDonald R, Lentin P, Burke-Taylor H. Facilitators and barriers to social and community participation following spinal cord injury. Aust Occup Ther J. (2016) 63:19–28. doi: 10.1111/1440-1630.12241
14. Nunnerley JL, Hay-Smith EJC, Dean SG. Leaving a spinal unit and returning to the wider community: an interpretive phenomenological analysis. Disabil Rehabil. (2013) 35:1164–73. doi: 10.3109/09638288.2012.723789
15. Chang F-H, Coster WJ, Helfrich CA. Community participation measures for people with disabilities: systematic review of content from an international classification of functioning, disability and health perspective. Arch Phys Med Rehabil. (2013) 94:771–81. doi: 10.1016/j.apmr.2012.10.031
16. Dwyer KJ, Mulligan H. Community reintegration following spinal cord injury: insights for health professionals in community rehabilitation services in New Zealand. N Z J Physiother. (2015) 43:75–85. doi: 10.15619/NZJP/43.3.02
17. Barclay L, Lentin P, McDonald R, Bourke-Taylor H. Understanding the factors that influence social and community participation as perceived by people with non-traumatic spinal cord injury. Br J Occup Ther. (2017) 80(10):577–86. doi: 10.1177/0308022617713699
18. Sabre L, Remmer S, Adams A, Väli M, Rekand T, Asser T, et al. Impact of fatal cases on the epidemiology of traumatic spinal cord injury in Estonia. Eur J Neurol. (2015) 22(5):768–72. doi: 10.1111/ene.12478
19. Centre for Rehabilitation of the Paralyzed. Annual Report: July 2019 to June 2020. Bangladesh: CRP Printing Press (2020).
20. Rahman E, Bardhan N, Curtin M, Islam MS, Patwary MFK, Das SK. As assessment of disability and quality of life in people with spinal cord injury upon discharge from a Bangladesh rehabilitation unit. Spinal Cord. (2022) 61(1):37–42. doi: 10.1038/s41393-022-00852-4
21. Hossain MS, Rahman MA, Bowden JL, Quadir MM, Herbert RD, Harvey LA. Psychological and socioecononmic status, complications and quality of life in people with spinal cord injuries after discharge from hospital in Bangladesh: a cohort study. Spinal Cord. (2016) 54(6):483–9. doi: 10.1038/sc.2015.179
22. Kader M, Perera NK, Hossain MS, Islam R. Socio-demographic and injury-related factors contributing to activity limitations and participation restrictions in people with spinal cord injury in Bangladesh. Spinal Cord. (2018) 56(3):239–46. doi: 10.1038/s41393-017-0001-y
23. Hossain MS, Islam MS, Rahman MA, Glinsky JV, Herbert RD, Ducharme S, et al. Health status, quality of life and socioeconomic situation of people with spinal cord injuries six years after discharge from a hospital in Bangladesh. Spinal Cord. (2019) 57(8):652–61. doi: 10.1038/s41393-019-0261-9
24. Fekete C, Eriks-Hoogland I, Baumberger M, Catz A, Itzkovich M, Lüthi H, et al. Development and validation of a self-report version of the spinal cord independence measure (SCIM III). Spinal Cord. (2013) 51(1):40–7. doi: 10.1038/sc.2012.87
25. Wirth B, van Hedel HJ, Kometer B, Dietz V, Curt A. Changes in activity after a complete spinal cord injury as measured by the spinal cord independence measure II (SCIM II). Neurorehabil Neural Repair. (2008) 22(2):145–53. doi: 10.1177/1545968307306240
26. Catz A, Itzkovich M, Elkayam K, Michaeli D, Gelernter I, Benjamini Y, et al. Reliability validity and responsiveness of the spinal cord independence measure 4th version in a multicultural setup. Arch Phys Med Rehabil. (2022) 103:430–40. doi: 10.1016/j.apmr.2021.07.811
27. Khamnon N, Amatachaya S, Wattanapan P, Musika N, Jitmongkolsri P, Kongngoen N, et al. Reliability and concurrent validity of the spinal cord independence measure III among rehabilitation professionals. Spinal Cord. (2022) 60:875–81. doi: 10.1038/s41393-022-00807-9
28. Itzhovich M, Gelernter I, Biering-Sorensen F, Weeks C, Laramee MT, Crave B, et al. The spinal cord independence measure (SCIM) version III: reliability and validity in a multi-center international study. Disabil Rehabil. (2007) 29(24):1926–33. doi: 10.1080/09638280601046302
29. Callaway L, Enticott J, Farnworth L, McDonald R, Migliorini C, Willer B. Community integration outcomes of people with spinal cord injury and multiple matched controls: a pilot study. Aust Occup Ther J. (2017) 64:226–34. doi: 10.1111/1440-1630.12350
30. Willer B, Ottenbacher KJ, Coad ML. The community integration questionnaire. A comparative examination. Am J Phys Med Rehabil. (1994) 73(2):103–11. doi: 10.1097/00002060-199404000-00006
31. Gontkovsky S, Russum P, Stokic D. Comparison of the CIQ with CHART short form in assessment community integration in individuals with chronic spinal cord injury: a pilot study. Neurorehabilitation. (2009) 24:185–92. doi: 10.3233/NRE-2009-0467
32. Turcotte S, Beaudoin M, Vallee C, Vincent C, Routhier F. Psychometric properties of the community integration questionnaire: a systematic review of five populations. Clin Rehabil. (2019) 33(11):1775–87. doi: 10.1177/0269215519867998
33. Nachar N. The Mann-Whitney U: a test for assessing whether two independent samples come from the same distribution. Tutor Quant Methods Psychol. (2008) 4(1):13–20. doi: 10.20982/tqmp.04.1.p013
34. Bewick V, Cheek L, Ball J. Statistics review 10: further nonparametric methods. Critical Care. (2004) 8(3):1–4. doi: 10.1186/cc2857
35. Kirshblum S, Botticello A, Benedetto J, Donavan J, Marino R, Hsieh S, et al. A comparison of diagnostic stability of the ASIA impairment scale versus frankel classification systems for traumatic spinal cord injury. Arch Phys Med Rehabil. (2020) 101:1556–62. doi: 10.1016/j.apmr.2020.05.016
36. American Spinal Injury Association. Standard for Neurological Classification of Spinal Injured Patients. 3rd ed. Chicago: American Spinal Injury Association (1990).
37. Szeliga E, Brzozowska-Magoń A, Borys R, Wolan-Nieroda A, Walicka-Cupryś K. The relationship between physical activity level and functional Status of subjects with high spinal cord injury. Int J Environ Res Public Health. (2022) 19(3):1787. doi: 10.3390/ijerph19031787
38. Carr JJ, Kendall MB, Amsters DI, Pershouse KJ, Kuipers P, Buettner P, et al. Community participation for individuals with spinal cord injury living in Queensland, Australia. Spinal Cord. (2017) 55(2):192–7. doi: 10.1038/sc.2016.169
39. van Leeuwen CM, Post MW, van Asbeck FW, Bongers-Janssen HM, van der Woude LH, de Groot S, et al. Life satisfaction in people with spinal cord injury during the first five years after discharge from inpatient rehabilitation. Disabil Rehabil. (2012) 34(1):76–83. doi: 10.3109/09638288.2011.587089
40. Chin B, Murphy ML, Cohen S. Age moderates the association between social integration and diurnal cortisol measures. Psychoneuroendocrinology. (2018) 90:102–9. doi: 10.1016/j.psyneuen.2018.02.008
41. Sezer N, Akkuş S, Uğurlu FG. Chronic complications of spinal cord injury. World J Orthop. (2015) 6(1):24. doi: 10.5312/wjo.v6.i1.24
42. Ahmed N, Quadir MM, Rahman MA, Alamgir H. Community integration and life satisfaction among individuals with spinal cord injury living in the community after receiving institutional care in Bangladesh. Disabil Rehabil. (2018) 40(9):1033–40. doi: 10.1080/09638288.2017.1283713
43. Trgovčević S, Milićević M. Social integration of adult person with spinal cord injury. In: Kulic M, Ilic-stosovic D, editors. Education and Rehabilitation of Adult Person with Disabilities: Thematic Collection of International Importance. Bosnia and Herzegovina: University of East Sarajevo (2014). p. 175–90.
44. Lala D, Dumont FS, Leblond J, Houghton PE, Noreau L. Impact of pressure ulcers on individuals living with a spinal cord injury. Arch Phys Med Rehabil. (2014) 95(12):2312–9. doi: 10.1016/j.apmr.2014.08.003
45. Kirshblum S, Millis S, McKinley W, Tulsky D. Late neurologic recovery after traumatic spinal cord injury. Arch Phys Med Rehabil. (2004) 85(11):1811–7. doi: 10.1016/j.apmr.2004.03.015
46. McKinley W, Santos K, Meade M, Brooke K. Incidence and outcomes of spinal cord injury clinical syndromes. J Spinal Cord Med. (2007) 30(3):215–24. doi: 10.1080/10790268.2007.11753929
47. Whiteneck G, Tate D, Charlifue S. Predicting community reintegration after spinal cord injury from demographic and injury characteristics. Arch Phys Med Rehabil. (1999) 80(11):1485–91. doi: 10.1016/S0003-9993(99)90262-9
Keywords: prospective, community integration, spinal cord injury, cross sectional study, functional independence
Citation: Das SK, Bakhtiar Md, Sabrin SM, Curtin M, Rahman E, Nahid ZBS, Rahman Z, Haque MdF, Patwary MdFK, Alam MdJ, Hossain MdE, Rahman MdA, Islam S, Ashfaquzzaman Md and Parvez MdAK (2024) Relationship between functional independence and community integration of people with spinal cord injury in Bangladesh. Front. Rehabil. Sci. 5:1435656. doi: 10.3389/fresc.2024.1435656
Received: 20 May 2024; Accepted: 18 November 2024;
Published: 11 December 2024.
Edited by:
Mert Doğan, Akdeniz University, TürkiyeReviewed by:
Elham Loni, University of Social Welfare and Rehabilitation Sciences, IranOrkun Tahir Aran, Hacettepe University, Türkiye
Ceyhun Türkmen, Cankiri Karatekin University, Türkiye
Copyright: © 2024 Das, Bakhtiar, Sabrin, Curtin, Rahman, Nahid, Rahman, Haque, Patwary, Alam, Hossain, Rahman, Islam, Ashfaquzzaman and Parvez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Saiba Muhammad Sabrin, c2FpYmFtZHNhYnJpbkBnbWFpbC5jb20=; Md. Anowar Khasru Parvez, a2hhc3J1NzNAanVuaXYuZWR1