 Dominika Lisiecka
Dominika Lisiecka Áine Kearns
Áine Kearns William Evans
William Evans Dawn Farrell
Dawn Farrell
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Rehabil. Sci. , 24 July 2024
Sec. Translational Research in Rehabilitation
Volume 5 - 2024 | https://doi.org/10.3389/fresc.2024.1393368
This article is part of the Research Topic Aspiration Management and Rehabilitation View all 8 articles
Introduction: Aspiration pneumonia (AP) is an infection of the lungs caused by inhalation of material. The reported incidences vary across literature and clinical populations and is associated with high morbidity and mortality. Management of AP is best carried out by a multidisciplinary team.
Methods: This aim of this review was to collate and describe the available evidence on AP to develop a greater understanding of the concept of AP as it is represented in the nursing literature. As a collaborative team, we undertook the six stages of a systematic mapping review. We searched for the term aspiration pneumonia in 200 peer reviewed nursing journals across 10 databases, over a ten-year period (2013–2023).
Results: In this review, 293 papers were coded. Dysphagia, oral health and tube feeding emerged as the most frequent risk factors for AP, and the most reported factors for preventing this condition. Mortality was the most commonly described consequence of AP, followed by hospitalisations and morbidity. Multiple management approaches were reported including dysphagia assessment, risk evaluation, oral care and texture modification of food and fluids. The role of nurses and interprofessional collaborations were described.
Discussion: Despite limited evidence related to the topic of AP in the nursing literature, the complexity of the causes, prevention, management and consequences of AP emerged. Certain factors, such as dysphagia, oral health, and tube feeding, were described under prevention, cause and management of AP. The importance of multidisciplinary approach in the management and prevention of AP was presented.
Aspiration pneumonia (AP) is a bacterial infection of the lungs caused by the aspiration of pathogens into lungs (1, 2). The examples of fluid which may contain pathogens are oropharyngeal secretions (3). Respiratory symptoms of AP can include tachypnea, dyspnea, cough, adventitious breath sounds, and hypoxia (4). Non-respiratory symptoms, more commonly seen in older adults, include mental status changes, falls, loss of appetite, and altered functional status (4).
AP is not an easy condition to diagnose (5), with absence of a clear definition and clinical consensus (6). The prevalence of AP is difficult to measure due to a lack of biomarkers, therefore the true incidence rate remain unknown (3). A recent paper explained challenges associated with distinguishing AP from hospital acquired pneumonia and community acquired pneumonia (6). The authors proposed to call pneumonia occurring in older frail people frailty-associated pneumonia (6).
AP is most prevalent in people with a learning disability, neurological or upper gastrointestinal conditions, and older adults (5). Conditions that increase the risk for AP include stroke, drug overdose, alcohol abuse, seizures, general anaesthesia, head trauma, intracranial masses, dementia, oesophageal strictures, gastroesophageal reflux, pseudobulbar palsy, tracheostomy, NG tube feeding, bronchoscopy and protracted vomiting (3). The evidence highlights the possible association between poor oral health and a risk of AP (7, 8), especially in older adults (8, 9). Oral health is essential for the overall health and wellbeing of individuals and particularly older adults who often reside in care settings and rely on caregivers to support oral health practices (9). Furthermore, this vulnerable group often have more limited access to professional oral health care (9). The evidence also confirms a positive relationship between the presence of AP with dysphagia (5, 6, 8, 10). Bosch et al. (2022) found that dysphagia was most frequently associated with the diagnosis of AP (48.2%), with dysphagia significantly linked to AP in hospitalised patients (11).
The consequences of AP include morbidity and mortality as well as a prolonged hospital stay (3, 5, 12) and increased treatment cost (13, 14). The outcomes depend on the volume of aspiration, patient age, general lung health, presence of any comorbidity, and time to diagnosis (15). The management and prevention of AP require a collaborative multidisciplinary team approach and nurses and speech & language therapists are important members of this team (3, 5, 16, 17). It is known that increasing the knowledge of nursing staff regarding evidence-based care for the prevention and management of AP, particularly in groups at risk of dysphagia, will improve patient outcomes and reduce the incidence of AP and mortality (18). Yet, there is little insight into the focus of nursing literature on the topic of AP. Therefore, we were interested to investigate how AP is represented in the nursing literature.
The aim of this review was not to ask or answer a specific research question on AP. Instead, the aim was to collate and describe available evidence to develop a greater understanding of the concept of AP as it is represented in the nursing literature. Therefore, a mapping review methodology was considered appropriate for this review due to the anticipated heterogeneity of the available research within the field of nursing. The mapping review method was developed by the Evidence for Policy and Practice Information and Co-ordinating Centre (EPPI-Centre), Institute of Education, London, to investigate research on a broad subject of interest (19, 20). This type of review aims to categorise, describe and map available evidence on a broad subject of interest, into an inductively developed framework. There is no standardised guidance document available equivalent to the PRISMA-P for mapping review protocols. Therefore, the methodology used in this review aligned with many of the processes described in James et al. (19) and O'Cathain et al. (21).
James et al. describes six stages of systematic mapping processes (19). Stage 1 of the review process involves the establishment of the team. In this review, the team included researchers with experience in a range of review methodologies and with professional backgrounds in nursing and speech and language therapy. In this first stage, the scope of the review was discussed and defined. The scope was intended to cover a broad review that explored the term aspiration pneumonia in the nursing literature over a ten-year period (2013–2023). When searching the evidence, as part of Stage 2, the authors obtained the list of all nursing journals available through the library of a higher education institution in the Republic of Ireland that provides pre- and post-registration nursing education programmes. During this stage, 453 journals were identified. Of these, 200 journals were categorised as peer-reviewed. During October 2023, the term aspiration pneumonia was searched within each of these journals.
Stage 3 involves screening and full text retrieval. However, due to the nature of the research question which sought to map the available evidence on AP in nursing literature, the title and abstracts were not screened. Instead, all retrieved records were added to EndNote and full texts were retrieved, where possible. A small number of full texts could not be retrieved and these records were excluded from the analysis. In addition, records of conference proceedings, book chapters, and duplicates were also removed.
In order to progress to Stage 4, which involves coding and production of an evidence map, the records were imported into NVivo. The data extracted from the articles included: country, year of publication, context of the study (e.g., population, setting etc.). In addition, three key pieces of data were extracted and analysed: frequency of term aspiration pneumonia, location of term within the article and additional information regarding AP. The latter was coded using a coding framework developed by the research team. It included codes related to cause and risk factors, prevention, management and consequences of AP. If papers clearly identified the knowledge gaps and recommended future research directions in relation to AP, these data were also extracted. A sample of 55 papers (10%) were independently coded by three researchers in order to develop the coding framework. Any disagreements were discussed and resolved through consensus. The remaining texts were coded first by one researcher using the agreed framework to produce a systematic map database within NVivo. A second researcher then coded the content under subcategories of codes within the coding framework.
Stage 5 is an optional critical appraisal stage as quality assessment of included papers is not required in mapping reviews (19, 20). Due to the nature of the review question and the heterogeneity among research designs within the included articles of the review, this stage was not considered appropriate for this review. The final stage, Stage 6, requires the research team to describe the findings. Here, the systematic map database can be used to describe the scope of the research and identify knowledge clusters and gaps (19). Descriptive statistics, tables and charts were utilised as helpful ways of easily visualising the data. An online data mapping software programme was used to produce a choropleth map of countries included in the review (https://www.datawrapper.de/maps/choropleth-map).
We identified 200 peer reviewed nursing journals across 10 databases in the University's library. We searched for the term aspiration pneumonia within each journal, which identified 605 records (for details see Supplementary Appendix S1). We were able to obtain a full text for 557/605 records. Papers were excluded for the following reasons: abstracts only (n = 10), duplicates (n = 1). During the coding phase, an additional 253 records were excluded due to the following reasons: no AP in the body of the paper (n = 171), AP reported once in the paper without sufficient information which would enable the coding (n = 75), conference abstract (n = 3), Chinese language (n = 2), a poem (n = 1), a book chapter (n = 1). The final sample consisted of n = 293 (see Figure 1). The data are presented below in the format based on the coding framework developed by the authors' team. The most prevalent themes are described in text and supplemented by figures.
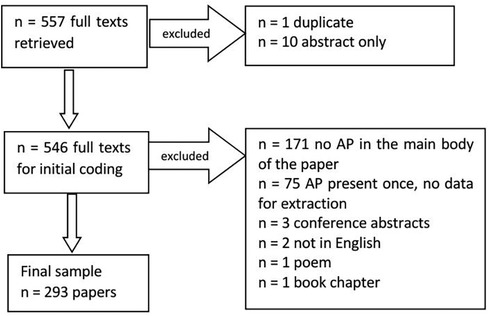
Figure 1 Data screening flowchart.
There was a high heterogeneity of papers, including experts' opinion articles, primary and secondary research papers, practice guidelines and recommendations. In 55% of records (n = 162) the term AP was reported once only within the body of the paper. However, there was sufficient information provided to allow for content coding. In terms of the location of the term aspiration pneumonia within the papers (i.e., whether this term was present in the introduction and background, methods, results or discussion sections), we were able to establish this for 167 (57%) of the sample (the remaining n = 126 papers did not use the IMRaD structure). In the 167 records, the term aspiration pneumonia was reported 204 times in the background and introduction to the paper, 29 times in the methods section, 74 times in the results section, and 93 times in the discussion.
Within the included papers, the average number of publications per year is 26. This drops to a low of 17 in 2013, and 18 in 2019, while the highest publication rate is 2020 when there were 38 papers (Figure 2).
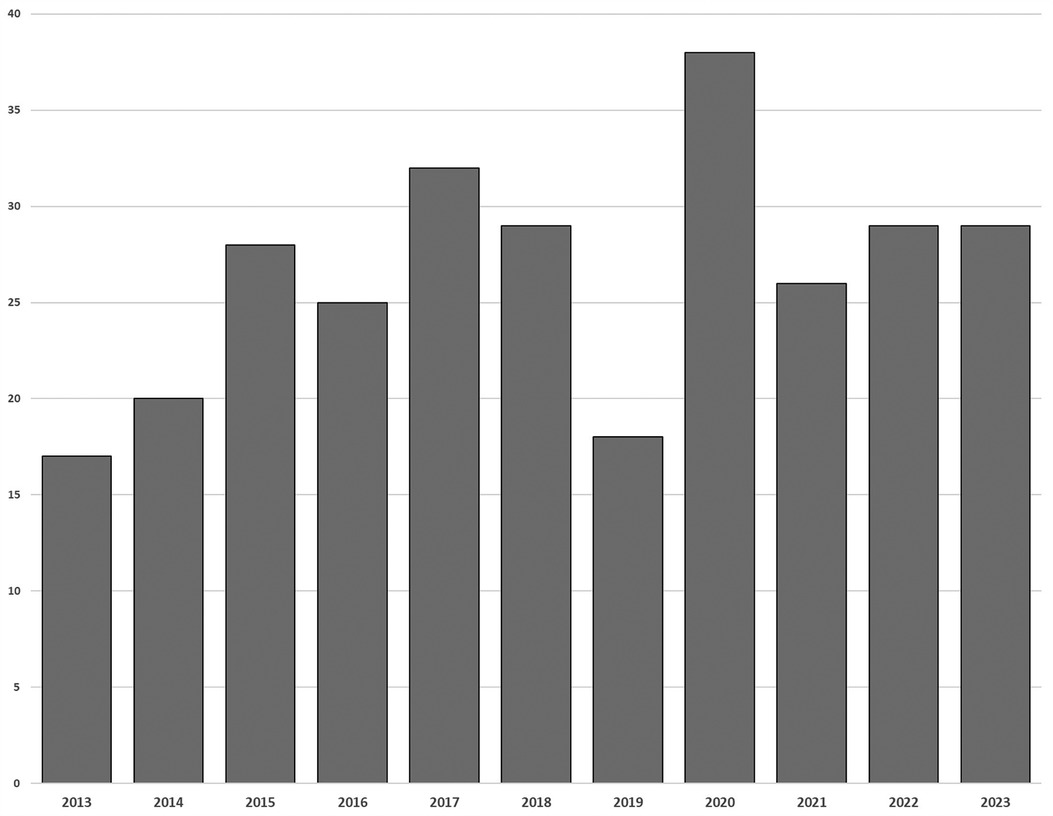
Figure 2 Frequency of publication.
In terms of the geographical spread of the papers included in this review, there was representation of all continents within the included papers. The majority came from United States of America (n = 83, 28%), followed by the United Kingdom (n = 68, 23%), Australia (n = 21, 7%), China (n = 17, 6%), Korea (n = 12, 4%), and Taiwan (n = 10, 3%) (Figure 3).
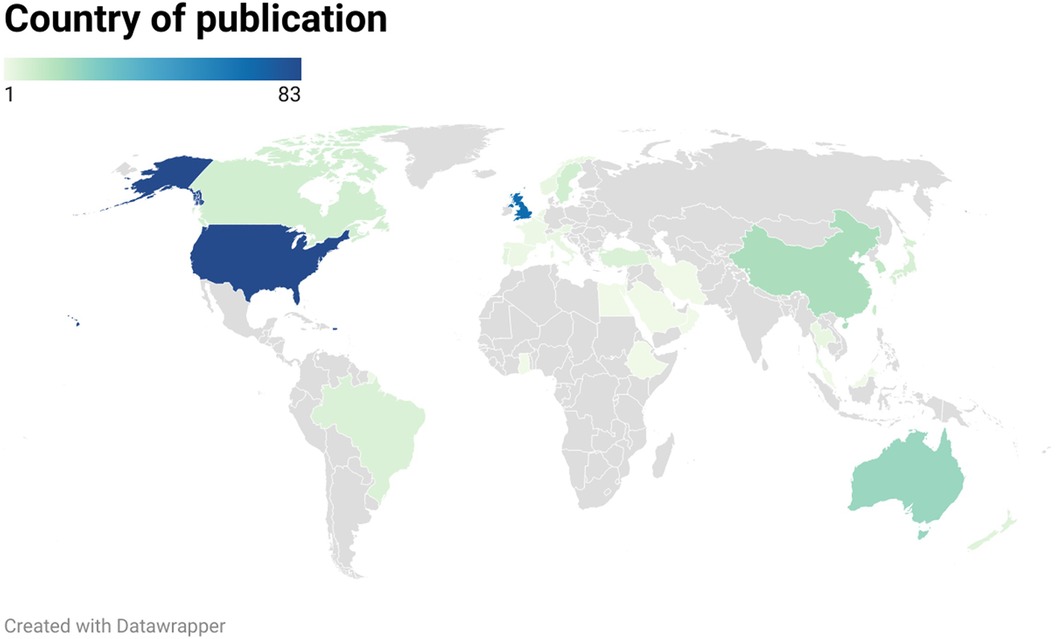
Figure 3 Location of papers.
Due to the high heterogeneity of papers, the context, setting, and populations could not be easily identified for all records. We noted a higher prevalence of papers on the topic of tube feeding, stroke, older person, dysphagia, and oral hygiene (Figure 4). The included papers focused on the range of populations across the lifespan, but were primarily focused on adult. The vast majority of papers were not focused on AP. There were twenty studies that included the term aspiration pneumonia in their methods section (this term occurred 29 times across the twenty papers, as per Section 3.1). The term was searched within a chart or medical records review (14, 22–24), as well as in a literature review (25, 26). Two studies referenced AP in a case description (22, 27). AP was listed as an outcome when investigating oral care (28, 29) and gastric residual volume (23, 30). AP was listed as a diagnosis for some participants in two studies (31, 32). It was also listed as a secondary outcome when investigating gastrointestinal ulcers (33). One study investigated reasons for developing AP and constipation (34). AP was also listed as a symptom when investigating the prevalence of dysphagia (35), included to develop clinical practice guidelines for aspiration (36), and to translate and validate the Self-Care for Aspiration Pneumonia Prevention Scale (37). AP was listed as an exclusion criterion in two studies (38, 39).
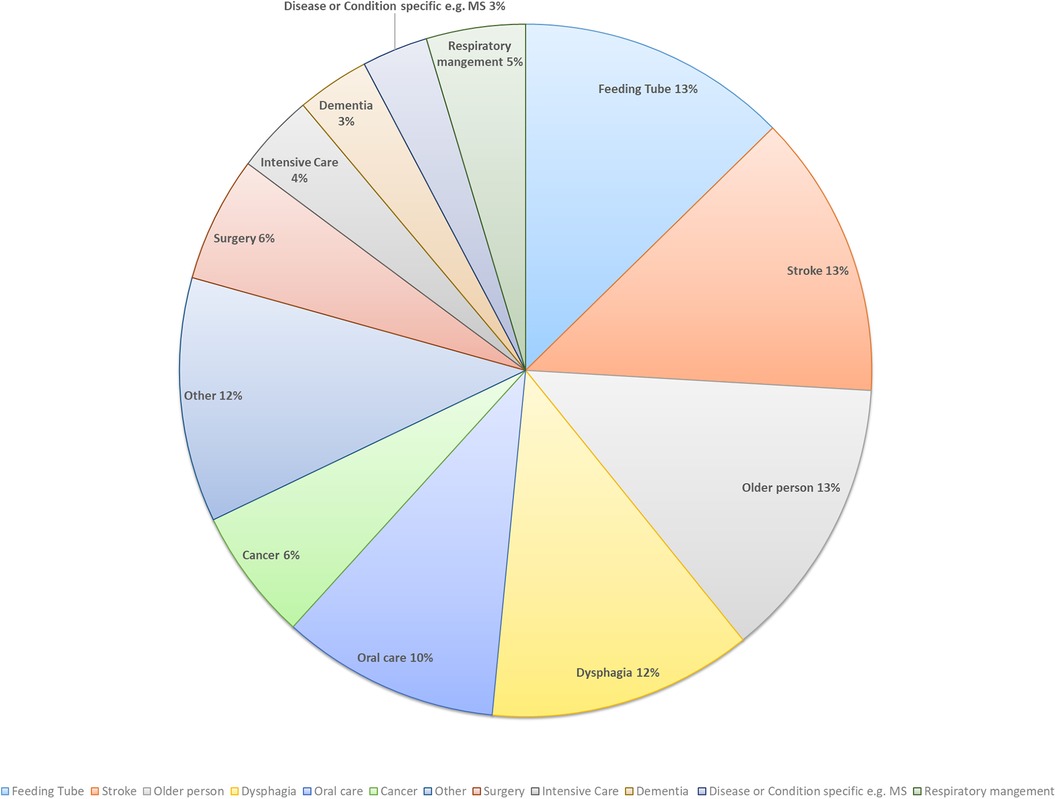
Figure 4 Context of papers.
Over half (52%) of the papers reported the cause and risk factors for developing AP. The top three were dysphagia, poor oral health and hygiene, and tube feeding. The most prevalent cause was dysphagia, represented in 51 papers (2, 8, 14, 17, 31, 33, 35, 40–83). This was followed by poor oral health and hygiene, reported in 38 papers (1, 2, 17, 28, 29, 45, 48, 51, 57, 59, 66, 68, 82–108), and tube feeding, noted in 27 papers (2, 12, 17, 26, 51, 60, 63, 72, 109–126). A number of papers (n = 33) presented single occurrence causes, for example obstructive sleep apnoea (127) or male gender (51) (Figure 5).
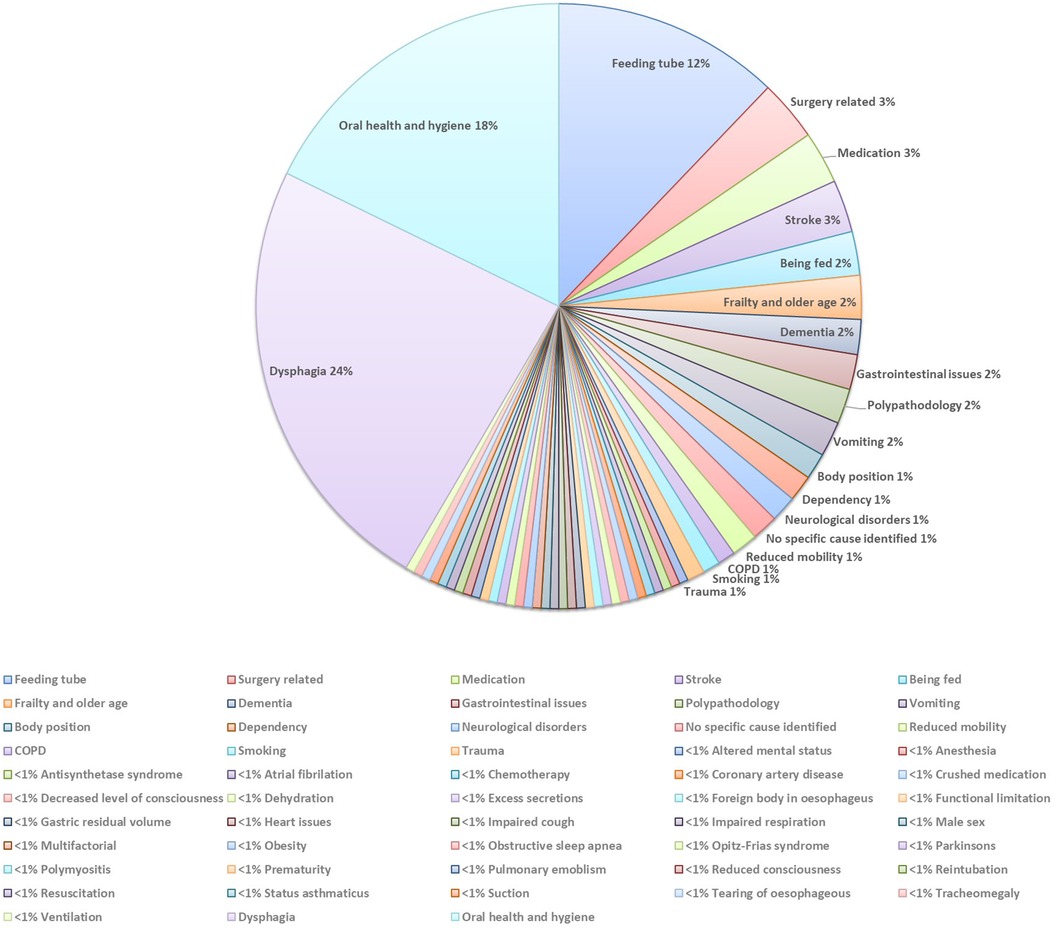
Figure 5 The cause and risk factors of AP.
Fifty-two papers (18%) reported on the management of people with AP (Figure 6). Within these papers, there were descriptions of the management of people with AP co-occurring with accounts of the prevention of this condition. The papers described a multidisciplinary approach when managing people with or at risk of AP. The team members included nurses (4, 14, 35, 42, 57, 95, 113, 128–132), speech & language therapists (8, 57, 88, 132–134), physiotherapist (34), and nursing aids (135). Nurses were identified as holding many responsibilities, for example, to identify and monitor the changes in a patient's status (14, 57, 131), coordinate input from other professionals (14, 57), make appropriate multidisciplinary referrals (14). Nurses were also responsible for providing education on the management of AP (129), assessing or screening for dysphagia (113, 132), helping to balance quality of life with medical risk associated with AP (35), providing oral care (4, 128), correct positioning (4), and support at mealtimes (4, 42).
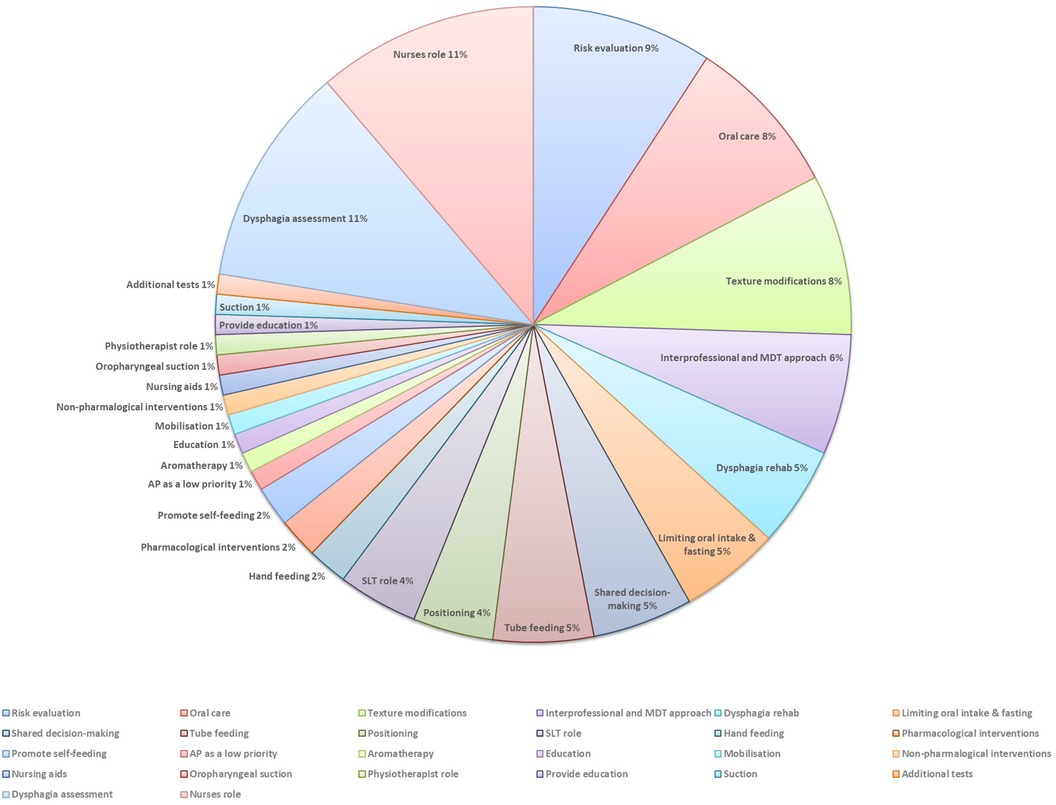
Figure 6 The management of AP.
Dysphagia assessment was presented as important in managing people with or at risk of AP. Through the identification of people with swallowing problems, dysphagia assessment could help to reduce the negative impact of AP (49, 136, 137), such as morbidity and mortality (49, 137). Food and fluid texture modifications were noted in the management of people with dysphagia who have or are at risk of AP (57, 131, 138–143). However, their benefits were reported as questionable (138), with one paper stating that thickened fluid “does not reduce AP in all patients and can pose other risks for physical health and psychological well-being” (57).
Risk mitigation or evaluation in the context of the management of AP emerged in some papers (8, 35, 49, 138, 144–148), and the importance of shared decision-making and balancing quality of life with a medical risk of AP was outlined (35, 138, 146). Risk of AP was predominantly linked with the presence of dysphagia (8, 35, 138, 145, 146, 148).
Tube feeding was also noted within the papers that referenced managing people with AP. While some papers stated that tube feeding, such as nasogastric tube, is introduced due to AP (14, 113), others reported that this does not reduced the risk of AP (144, 149).
The importance of adequate oral care for people with or at risk of AP was reported (139, 98, 92, 150, 39, 90, 151, 152). The included papers identified the implementation of oral hygiene in both the management and prevention of AP.
Thirty papers (10%) described consequences of AP. Mortality was the most frequently reported (n = 31 papers) (8, 12, 14, 26, 36, 40, 45, 49, 53, 68, 74, 90, 102, 111, 120, 126, 137, 143, 150, 153–164). The second most common consequence was hospitalisations (n = 12 papers) (8, 12, 14, 34, 38, 45, 53, 95, 111, 126, 165, 166), followed by morbidity (n = 6 papers) (8, 45, 74, 156, 159, 161). Three papers stated AP increases treatment cost (14, 165, 166) and decreases rehabilitation outcomes (12, 14, 59). Other consequences were reported in two or less papers (Figure 7).
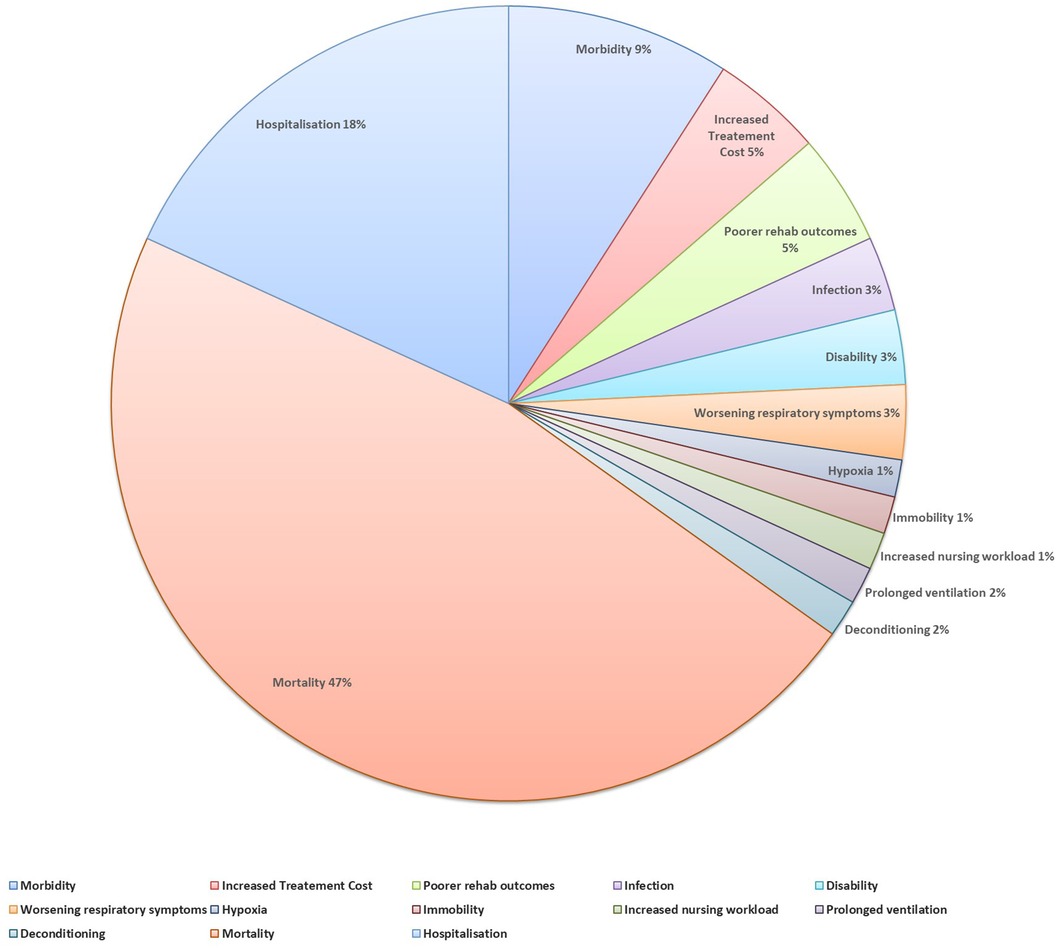
Figure 7 The consequences of AP.
Forty-six papers (16%) described the prevention of AP. The most commonly reported way of preventing AP was appropriate management of dysphagia (n = 13 papers) (14, 17, 34, 36, 48, 58, 61, 63, 113, 167–170). Nurses role in preventing AP was reported in nine papers (14, 34, 36, 95, 113, 132, 167, 171, 172). In particular, five papers outline the role for nurses in screening people for dysphagia, as this can reduce the risk of AP (14, 58, 63, 113).
Another method of preventing AP was appropriate oral care, for example brushing teeth after meals, cleaning tongue, or cleaning dentures (n = 12 papers) (34, 39, 45, 69, 88, 90, 101, 102, 111, 173, 174). It was recommended that nurses incorporate oral care into their daily routines (88, 90). One paper reported the need for nurses to engage in periodic hands-on training to improve their knowledge and skills in providing quality oral care (90). In addition to preventing AP, oral care was noted to be potentially a cost saving option that not only improves oral health, but has a positive impact on systemic health (173).
Tube feeding was described as an option when attempting to prevent AP (n = 10 papers) (26, 123, 144, 157, 171, 175–179). Some papers highlighted risk factors associated with tube feeding. For example, tube feeding may increase vomiting and subsequently increase the risk of AP (26). In the same paper, the authors recommended a new nasogastric tube flushing technique, maintaining an upright body position and ensuring proper placement of feeding tube to reduce the risk of AP. It was noted that the tube feeding regime (continuous vs. intermittent) may also play a role in the prevention of AP (176). One paper drew attention to the lack of evidence to support tube feeding over oral feeding for people with advanced dementia (144). Papers also identified limiting oral intake, in the context of surgery (158, 180–183) or dysphagia (51, 113, 145, 163), as a strategy to prevent AP. Other prevention strategies are presented in the Figure 8.
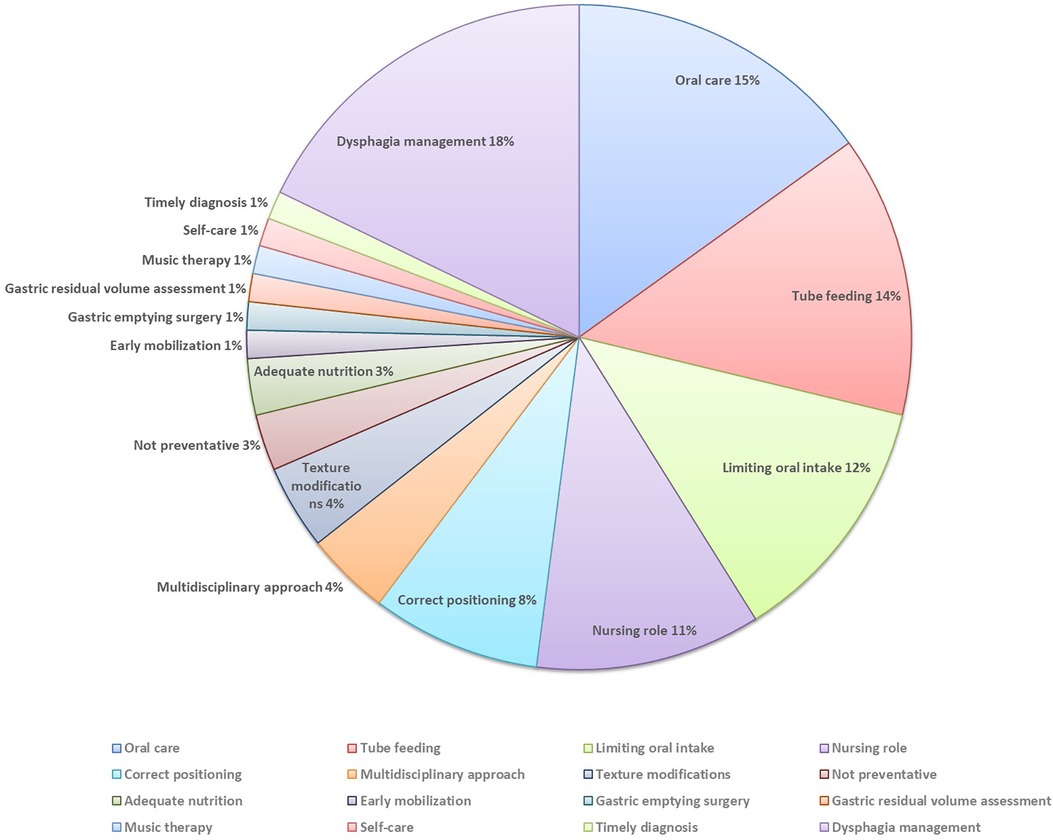
Figure 8 The prevention of AP.
Five papers identified the following knowledge gaps related to AP which should be further explored:
- the mechanism between sputum suction and AP (33)
- the routine checking of gastric residuals in people receiving gastrostomy feeding and risk of AP (23)
- the evaluation of the effectiveness of the various oral health interventions in reducing AP (60, 101)
- the support for nursing education to promote oral health interventions and reduce AP (101)
- the increased demands on the nursing resources when caring for patients with poststroke complications, such as AP or nasogastric feeding (14).
This review aimed to map how the term aspiration pneumonia has been represented in the nursing literature within the last decade. We were interested to research this literature as nursing is the largest health care profession (184) and is at the forefront of patient care delivery. This care extends to providing support to people with AP. The findings discussed below represent how the term aspiration pneumonia is perceived in nursing literature.
We discovered that 293 papers included the term aspiration pneumonia in this review. However, the volume of information regarding AP within each paper was limited. Despite this limited volume, we were able to establish that within the nursing literature, the causes, prevention, management and consequences of AP are complex, with some options, for example tube feeding, being considered as a potential help, and as a risk. We also noted that dysphagia, oral health, and tube feeding emerged across prevention, cause and management of AP. Mortality, hospitalisation and morbidity were the most frequent consequences of AP noted in this review.
Dysphagia has emerged as being closely connected to AP in this review. Dysphagia is forefront as a cause and risk factor for AP. Swallow assessment was identified as key for the management of people with/at risk of AP. In addition, the management of dysphagia is important for prevention of AP. It is recognised in the wider literature that although pharyngeal stage dysphagia may lead to aspiration (185), the relationship between aspiration and developing AP is complex and multifaceted (186, 187). There are many factors that should also be considered as potential predictors of AP particularly in older adults, including the presence of co-morbidities and individuals' mobility or ambulation (8, 188). Aspiration does not always lead to AP, for example, approximately half of healthy adults aspirate during sleep (189). Aspiration, and in particular silent aspiration, has been observed in healthy adults across the lifespan during flexible endoscopic evaluation of swallowing (190), and yet no differences have been noted between healthy older adult aspirators and non-aspirators on pulmonary computed tomography, suggesting that there may be a broad range of normal swallowing that includes asymptomatic aspiration (191).
The current review has identified that a multidisciplinary approach is perceived as important in the management of dysphagia, however the studies included in this review have not specified how exactly this approach should be provided. This multidisciplinary approach is in keeping with existing literature on the management of dysphagia across the lifespan (192–195), with one study stating that in the context of stroke an integrated team approach and pathway of care decreases the prevalence of AP (195). Dysphagia screening can be effectively performed by trained nurses and it has been shown that the early identification of dysphagia by nurses reduces AP rate in patients post stroke (196). In addition, screening undertaken by trained nurses may be effective in detecting dysphagia, reducing the time patients are kept nil-by-mouth, and is considered to be in a patient's best interest (197). Swallowing screening by a nurse may also improve the appropriateness of referrals to speech & language therapy for dysphagia services (197).
In addition to dysphagia, oral care emerged across prevention and management of AP and as a cause and risk factor for this condition. Despite the fact that oral health is considered as essential for healthy ageing, it is one of the most neglected aspects of care for older people (91, 198). Nurses play a very important role in the oral health care of their patients in terms of the assessment, planning and implementation of care. A recent scoping review has described personal care, such as oral care, to be ranked as the second fundamental of nursing in caring for older adults (199). However, research has shown that this fundamental aspect of nursing care can often be overlooked or down-prioritised (200, 201). Mitchell et al. found that most community nurses reported providing information about oral health to older adults living at home, however they were not involved in the direct provision of oral care as a routine practice and it was very much dependent on the individual patient (202). The authors called for greater interprofessional collaboration and clearer delineation of roles with oral health professionals in enhancing oral health outcomes in vulnerable groups (202).
A range of clinical cohorts may require short or long-term tube feeding (203). In our review, the link between tube feeding and AP emerged as being complex. The presence of tube feeding was identified as a risk factor for AP. Tube feeding was also identified as a management option and a mechanism of prevention of AP in the context of dysphagia. The rates of AP in people receiving tube feeding were reported between 4% and 95% in a recent review (204). AP is a common cause of death in people receiving tube feeding (204, 205). Despite the risks, tube feeding is a well-established management option for dysphagia, where nutrition and hydration requirements may not be met orally (12). The role of a nurse in supporting the safety of people receiving tube feeding has been recognised (112). This role related to nurses' involvement in swallow screening, onwards referrals, coordinating input from other professionals, and assisting the person with dysphagia during meals.
The findings of our review indicated that AP has not been researched in-depth in the nursing journals over the last decade. Our findings are sourced from journals in the field of nursing only. We have identified the complex nature of AP and the reporting of a multidisciplinary approach in the prevention and management of the condition. It is likely that this review provides only a snapshoot of literature that informs nursing practice. The research team included two nurses and two speech & language therapists therefore represented two professional perspectives within the discussion of findings.
This is the first study to glean insights into the representation of the term aspiration pneumonia in published, peer-reviewed nursing literature. However, this study has potential limitations. The eligible studies in this mapping review were not quality assessed as it was not deemed appropriate or relevant for the purpose of this study aimed at providing a descriptive overview of the published, peer reviewed nursing literature on aspiration pneumonia. The search undertaken for this study was limited to one Higher Education Institution library and refined to peer-reviewed journals. Records such as book chapters were excluded which may have limited insights into the topic. However, due to the volume of potential literature we decided that focusing on peer-reviewed journal articles was the preferred option for logistical reasons.
In conclusion, this mapping review highlights the lack of attention given to the topic of AP in the nursing literature, as evidenced by the overall limited focus on AP within the eligible studies reviewed. Despite this, the studies reviewed found a diverse range of causes or risk factors for developing AP, with dysphagia, poor oral health and hygiene, and tube feeding identified as the most common. The study reveals that the management of AP requires a multidisciplinary approach and nurses play a central role with responsibility for a complex range of care interventions, including dysphagia assessment, diet modifications, tube feeding and oral care. Many consequences of AP were identified in the review, such as mortality, hospitalisation and morbidity. Preventive strategies for AP in terms of appropriate management of dysphagia, oral care and tube feeding were illustrated. The study highlights a number of knowledge gaps for future research. Further research on the nurses' role in the management of AP and dysphagia, as well as their involvement in providing oral care, is indicated. In addition, country and culturally specific differences in the management of AP should be explored.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
DL: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. ÁK: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. WE: Formal Analysis, Investigation, Writing – original draft, Writing – review & editing. DF: Formal Analysis, Investigation, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
The publication fee will be covered by the Department of Nursing and Healthcare Sciences in Munster Technological University.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fresc.2024.1393368/full#supplementary-material
1. Ab. Malik N, Mohamad Yatim S, Hussein N, Mohamad H, McGrath C. Oral hygiene practices and knowledge among stroke-care nurses: a multicentre cross-sectional study. J Clin Nurs. (2018) 27(9-10):1913–9. doi: 10.1111/jocn.14241
2. Miles A, Lee YY, McLellan N, Gillham M. Implementing a systematic care pathway for management of dysphagia after cardiothoracic surgery. Intensive Crit Care Nurse. (2022) 70:103224. doi: 10.1016/j.iccn.2022.103224
3. Sanivarapu RR, Gibson J. Aspiration pneumonia. In: StatPearls. Treasure Island (FL): StatPearls Publishing (2024). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK568770/ (Accessed February 28, 2024).
4. Tamburri LM, Hollender KD, Orzano D. Protecting patient safety and preventing modifiable complications after acute ischemic stroke. Crit Care Nurse. (2020) 40(1):56–65. doi: 10.4037/ccn2020859
5. Simpson AJ, Allen JL, Chatwin M, Crawford H, Elverson J, Ewan V, et al. BTS clinical statement on aspiration pneumonia. Thorax. (2023) 78(Suppl 1):s3–21. doi: 10.1136/thorax-2022-219699
6. Smithard DG, Yoshimatsu Y. Pneumonia, aspiration pneumonia, or frailty-associated pneumonia? Geriatrics. (2022) 7(5):1–10. doi: 10.3390/geriatrics7050115
7. Hamad M, Nativ-Zeltzer N. Aspiration pneumonia and oral health. Curr Otorhinolaryngol Rep. (2023) 11(2):161–5. doi: 10.1007/s40136-023-00455-4
8. van der Maarel-Wierink CD, van der Putten GJ, De Visschere LM, Bronkhorst EM, de Baat C, Schols JM. Risk of aspiration in care home residents and associated factors. J Gerontol Nurs. (2015) 41(2):26–31. doi: 10.3928/00989134-20140807-99
9. Khadka S, Khan S, King A, Goldberg LR, Crocombe L, Bettiol S. Poor oral hygiene, oral microorganisms and aspiration pneumonia risk in older people in residential aged care: a systematic review. Age Ageing. (2021) 50(1):81–7. doi: 10.1093/ageing/afaa102
10. Chang MC, Choo YJ, Seo KC, Yang S. The relationship between dysphagia and pneumonia in acute stroke patients: a systematic review and meta-analysis. Front Neurol. (2022) 13:834240. doi: 10.3389/fneur.2022.834240
11. Bosch G, Comas M, Domingo L, Guillen-Sola A, Duarte E, Castells X, et al. Dysphagia in hospitalized patients: prevalence, related factors and impact on aspiration pneumonia and mortality. Eur J Clin Invest. (2023) 53(4):e13930. doi: 10.1111/eci.13930
12. Rowat A. Dysphagia, nutrition and hydration post stroke. Br J Nurs. (2014) 23(12):634. doi: 10.12968/bjon.2014.23.12.634
13. Welte T, Torres A, Nathwani D. Clinical and economic burden of community-acquired pneumonia among adults in Europe. Thorax. (2012) 67(1):71–9. doi: 10.1136/thx.2009.129502
14. Schwarz M, Coccetti A, Murdoch A, Cardell E. The impact of aspiration pneumonia and nasogastric feeding on clinical outcomes in stroke patients: a retrospective cohort study. J Clin Nurs. (2018) 27(1-2):e235–41. doi: 10.1111/jocn.13922
15. Kollmeier BR, Keenaghan M. Aspiration Risk. Treasure Island (FL): StatPearls Publishing (2023). https://www.ncbi.nlm.nih.gov/books/NBK470169/
16. Long AF, Kneafsey R, Ryan J, Berry J. The role of the nurse within the multi-professional rehabilitation team. J Adv Nurs. (2002) 37(1):70–8. doi: 10.1046/j.1365-2648.2002.02059.x
17. McFarlane M, Miles A, Atwal P, Parmar P. Interdisciplinary management of dysphagia following stroke. Br J Neurosci Nurs. (2014) 10(1):13–20. doi: 10.12968/bjnn.2014.10.1.13
18. Santos JMLG, Ribeiro O, Jesus LMT, Sa-Couto P, Matos MAC. Recommendations of good practice to prevent aspiration pneumonia in older adults at risk of oropharyngeal dysphagia living in nursing homes: a modified e-Delphi study protocol. Int J Lang Commun Disord. (2023) 59:1223–31. doi: 10.1111/1460-6984.12985
19. James KL, Randall NP, Haddaway NR. A methodology for systematic mapping in environmental sciences. Environ Evid. (2016) 5(1):7. doi: 10.1186/s13750-016-0059-6
20. Grant MJ, Booth A. A typology of reviews: an analysis of 14 review types and associated methodologies. Health Inf Libr J. (2009) 26(2):91–108. doi: 10.1111/j.1471-1842.2009.00848.x
21. O’Cathain A, Thomas KJ, Drabble SJ, Rudolph A, Hewison J. What can qualitative research do for randomised controlled trials? A systematic mapping review. BMJ Open. (2013) 3(6):1–15. doi: 10.1136/bmjopen-2013-002889
22. Bloomer MJ, Botti M, Runacres F, Poon P, Barnfield J, Hutchinson AM. End-of-life care for older people in subacute care: a retrospective clinical audit. Collegian. (2019) 23(1):22–7. doi: 10.1016/j.colegn.2018.02.005
23. Gately T, Lima J, Gonzalians T. Sub acute gastric residuals elimination change project. Rehabil Nurs. (2015) 40(2):127–9. doi: 10.1002/rnj.167
24. Sarabia-Cobo CM, Perez V, de Lorena P, Dominguez E, Hermosilla C, Nunez MJ, et al. The incidence and prognostic implications of dysphagia in elderly patients institutionalized: a multicenter study in Spain. Appl Nurs Res. (2016) 30:e6–9. doi: 10.1016/j.apnr.2015.07.001
25. Kjeldsen CL, Hansen MS, Jensen K, Holm A, Haahr A, Dreyer P. Patients’ experience of thirst while being conscious and mechanically ventilated in the intensive care unit. Nurs Crit Care. (2018) 23(2):75–81. doi: 10.1111/nicc.12277
26. Bani Hani M, Ihim I, Harps J, Cunningham SC. A breath of fresh air: a quality-improvement study comparing an air-circulating technique versus conventional technique to prevent nasogastric tube dysfunction. BMC Nurs. (2015) 14:63. doi: 10.1186/s12912-015-0111-9
27. Bradway C, Cotter VT, Darrah NJ, Gibbs VD, Hadley D, Kim EH, et al. An interprofessional education simulation workshop: health professions learning palliative care communication. J Nurs Educ. (2018) 57(8):493–7. doi: 10.3928/01484834-20180720-08
28. Haresaku S, Kubota K, Miyoshi M, Iino H, Monji M, Aoki H, et al. Effect of educational environments on nursing faculty members’ perceptions regarding oral care. Jpn J Nurs Sci. (2019) 16(4):364–72. doi: 10.1111/jjns.12247
29. Haresaku S, Miyoshi M, Kubota K, Obuse M, Aoki H, Nakashima F, et al. Current status and future prospects for oral care education in bachelor of nursing curriculums: a Japanese cross-sectional study. Jpn J Nurs Sci. (2023) 20(2):e12521. doi: 10.1111/jjns.12521
30. Smith M, Smith M, Robinson KN. Using nurse-driven protocols to eliminate routine gastric residual volume measurements: a retrospective study. Crit Care Nurse. (2022) 42(4):e1–10. doi: 10.4037/ccn2022584
31. Kim JY, Lee YW, Kim HS, Lee EH. The mediating and moderating effects of meaning in life on the relationship between depression and quality of life in patients with dysphagia. J Clin Nurs. (2019) 28(15-16):2782–9. doi: 10.1111/jocn.14907
32. Palesjö C, Nordgren L, Asp M. Being in a critical illness-recovery process: a phenomenological hermeneutical study. J Clin Nurs. (2015) 24(23-24):3494–502. doi: 10.1111/jocn.13002
33. Chang WP, Chen HM, Wu JR, Tsai HT, Ho CF, Lin YH. Adverse effects of non-intubated airway suctioning: a clinical data-based study. J Clin Nurs. (2023) 32(5-6):726–35. doi: 10.1111/jocn.16307
34. Feo R, Urry K, Conroy T, Kitson AL. Why reducing avoidable hospital readmissions is a “wicked” problem for leaders: a qualitative exploration of nursing and allied health perceptions. J Adv Nurs. (2023) 79(3):1031–43. doi: 10.1111/jan.15220
35. Park YH, Han HR, Oh BM, Lee J, Park JA, Yu SJ, et al. Prevalence and associated factors of dysphagia in nursing home residents. Geriatr Nurs. (2013) 34(3):212–7. doi: 10.1016/j.gerinurse.2013.02.014
36. Sugama J, Ishibasi M, Ota E, Kamakura Y, Saitoh E, Sanada H, et al. Japanese clinical practice guidelines for aspiration and pharyngeal residual assessment during eating and swallowing for nursing care. Jpn J Nurs Sci. (2022) 19(4):e12496. doi: 10.1111/jjns.12496
37. Yang Z, Chen F, Zhang Y, Pan S, Lu Y, Zhang H. Translation of the Chinese version of the self-care for aspiration pneumonia prevention scale and its validation among Chinese community dwelling elderly with risk of dysphasia. Nurs Open. (2022) 9(3):1902–11. doi: 10.1002/nop2.940
38. Pitthayapong S, Thiangtam W, Powwattana A, Leelacharas S, Waters CM. A community based program for family caregivers for post stroke survivors in Thailand. Asian Nurs Res Korean Soc Nurs Sci. (2017) 11(2):150–7. doi: 10.1016/j.anr.2017.05.009
39. Chen SC, Weng LC, Tsai SC, Wang SM, Han HM. Effectiveness of oral rinsing solutions on mucus, odor, and plaque in the hospitalized elderly in Taiwan. Clin Nurs Res. (2019) 28(6):762–76. doi: 10.1177/1054773817744151
41. Gibson J. NICE on transcutaneous neuromuscular electrical stimulation. Br J Neurosci Nurs. (2014) 10:5–5. doi: 10.12968/bjnn.2014.10.Sup6.5
42. Herron-Foster BJ, Bustos JJ. Special needs: caring for the older adult with down syndrome. Medsurg Nurs. (2014) 23(4):225–37. 25318335.25318335
43. Ilott I, Bennett B, Gerrish K, Pownall S, Jones A, Garth A. Evaluating a novel approach to enhancing dysphagia management: workplace-based, blended e-learning. J Clin Nurs. (2014) 23(9-10):1354–64. doi: 10.1111/jocn.12409
44. McLaughlin L, Mahon S. A meta-analysis of the relationship among impaired taste and treatment, treatment type, and tumor site in head and neck cancer treatment survivors. Oncol Nurs Forum. (2014) 41(3):E194–202. doi: 10.1188/14.ONF.E194-E202
45. van der Maarel-Wierink CD, Meijers JM, De Visschere LM, de Baat C, Halfens RJ, Schols JM. Subjective dysphagia in older care home residents: a cross-sectional, multi-centre point prevalence measurement. Int J Nurs Stud. (2014) 51(6):875–81. doi: 10.1016/j.ijnurstu.2013.10.016
46. Brook S. The dysphagia diet: maintaining adequate nutrition. Nurs Resid Care. (2015) 17(5):248–50. doi: 10.12968/nrec.2015.17.5.248
47. Eccleston CE, Lea EJ, McInerney F, Crisp E, Marlow A, Robinson AL. An investigation of nursing students’ knowledge of dementia: a questionnaire study. Nurse Educ Today. (2015) 35(6):800–5. doi: 10.1016/j.nedt.2015.02.019
48. Erwin A, Brook S. Dysphagia: an SLT and dietetic perspective. Nurs Resid Care. (2015) 17(3):131–6. doi: 10.12968/nrec.2015.17.3.131
49. Huhn-Matesic EK. Developing and testing a bedside aspiration screen to protect stroke patients from aspiration and mortality: expanding nursing practice and partnership. Clin Sch Rev. (2015) 8(1):117–24. doi: 10.1891/1939-2095.8.1.117
50. Park YH, Bang HL, Han HR, Chang HK. Dysphagia screening measures for use in nursing homes: a systematic review. J Korean Acad Nurs. (2015) 45(1):1–3. doi: 10.4040/jkan.2015.45.1.1
51. Benfield J, Michou E. Dysphagia screening and assessment in the stroke unit. Br J Neurosci Nurs. (2016) 12(Sup2):S24–8. doi: 10.12968/bjnn.2016.12.Sup2.S24
52. Koyama T, Shamoto H, Anzai H, Koganei Y, Maeda K, Wakabayashi H. Multidisciplinary comprehensive care for early recommencement of oral intake in older adults with severe pneumonia. J Gerontol Nurs. (2016) 42(10):21–9. doi: 10.3928/00989134-20160913-05
53. Chen PC, Chuang CH, Leong CP, Guo SE, Hsin YJ. Systematic review and meta-analysis of the diagnostic accuracy of the water swallow test for screening aspiration in stroke patients. J Adv Nurs. (2016) 72(11):2575–86. doi: 10.1111/jan.13013
54. De Witt Jansen B, Brazil K, Passmore P, Buchanan H, Maxwell D, McIlfactrick SJ, et al. Nurses’ experiences of pain management for people with advanced dementia approaching the end of life: a qualitative study. J Clin Nurs. (2017) 26(9-10):1234–44. doi: 10.1111/jocn.13442
55. Habermann B, Shin JY. Preferences and concerns for care needs in advanced Parkinson’s disease: a qualitative study of couples. J Clin Nurs. (2017) 26(11-12):1650–6. doi: 10.1111/jocn.13565
56. Anderson L. Delivering artificial nutrition and hydration safely by feeding pumps. Br J Nurs. (2018) 27(18):1032–3. doi: 10.12968/bjon.2018.27.18.1032
57. Atkinson K, O’Kane L. Thickener and beyond: an individualised approach to dysphagia management. Br J Neurosci Nurs. (2018) 14(Sup2):S13–9. doi: 10.12968/bjnn.2018.14.Sup2.S13
58. Christensen M, Trapl M. Development of a modified swallowing screening tool to manage post-extubation dysphagia. Nurs Crit Care. (2018) 23(2):102–7. doi: 10.1111/nicc.12333
59. Clare CS. Role of the nurse in stroke rehabilitation. Nurs Stand. (2018) 33(7):59–66. doi: 10.7748/ns.2018.e11194
60. Jenson H. Improving oral care in hospitalized non-ventilated patients: standardizing products and protocol. Medsurg Nurs. (2018) 27(1):38–45. Available online at: https://digitalcommons.providence.org/publications/885
61. Kennedy MS. Journal publishing: a review of the basics. Semin Oncol Nurs. (2018) 34(4):361–71. WB Saunders. doi: 10.1016/j.soncn.2018.09.004
62. Lamure J, Chevalier M, Rathelot P, Mignolet F, Precheur I. In vitro screening of the antibacterial and anti-candida properties of crushed nonantimicrobial drugs frequently prescribed in nursing homes. Res Gerontol Nurs. (2018) 11(2):82–90. doi: 10.3928/19404921-20180131-01
63. de Jesus Oliveira I, da Mota LAN, Freitas SV, Ferreira PL. Dysphagia screening tools for acute stroke patients available for nurses: a systematic review. Nurs Pract Today. (2019) 6(3):103–15.
64. Kable A, Baker A, Pond D, Southgate E, Turner A, Levi C. Health professionals’ perspectives on the discharge process and continuity of care for stroke survivors discharged home in regional Australia: a qualitative, descriptive study. Nurs Health Sci. (2019) 21(2):253–61. doi: 10.1111/nhs.12590
65. de Jesus Oliveira I, Rodrigues Couto G, Neves da Mota LA. Nurses’ preferred items for dysphagia screening in acute stroke patients: a qualitative study. Nurs Pract Today. (2020) 7(3):226–33.
66. Ferguson C, George A, Villarosa AR, Kong AC, Bhole S, Ajwani S. Exploring nursing and allied health perspectives of quality oral care after stroke: a qualitative study. Eur J Cardiovasc Nurs. (2020) 19(6):505–12. doi: 10.1177/1474515119886798
67. Jack-Waugh A, Brown M, Henderson J, Holland S, Sharp B. Delivering personal care for people with advanced dementia. Nurs Older People. (2020) 32(5):18–25. doi: 10.7748/nop.2020.e1191
68. Jung C, Molinari N, Bouhlel A, Ruimy R, Prêcheur I. Thickened drinks and oral nutritional supplements as potential reservoirs of oral microorganisms: microbial assays in vitro. Res Gerontol Nurs. (2020) 13(4):203–9. doi: 10.3928/19404921-20200220-01
69. Woon C. Improving oral care for hospitalised patients: choosing appropriate products. Br J Nurs. (2020) 29(9):520–5. doi: 10.12968/bjon.2020.29.9.520
70. Banda KJ, Chu H, Kao CC, Voss J, Chiu HL, Chang PC, et al. Swallowing exercises for head and neck cancer patients: a systematic review and meta-analysis of randomized control trials. Int J Nurs Stud. (2021) 114:103827. doi: 10.1016/j.ijnurstu.2020.103827
71. Artiles CE, Regan J, Donnellan C. Dysphagia screening in residential care settings: a scoping review. Int J Nurs Stud. (2021) 114:103813. doi: 10.1016/j.ijnurstu.2020.103813
73. Yang W, Nie W, Zhou X, Guo W, Mou J, Yong J, et al. Review of prophylactic swallowing interventions for head and neck cancer. Int J Nurs Stud. (2021) 123:104074. doi: 10.1016/j.ijnurstu.2021.104074
74. Bernardes RA, Cruz A, Neves H, Parola V, Catela N. Screening tools designed to assess and evaluate oropharyngeal dysphagia in adult patients: a scoping review. Nurs Rep. (2022) 12(2):245–58. doi: 10.3390/nursrep12020025
75. Cooper AL, Mazzer J, Martin-Robins D, Brown JA. A point prevalence study of palliative care need and referral rates in adult inpatients. J Clin Nurs. (2022) 31(21-22):3144–54. doi: 10.1111/jocn.16148
76. Do N, Mitchell S, Sturgill L, Khemani P, Sin MK. Speech and swallowing problems in Parkinson’s disease. J Nurse Pract. (2022) 18(8):848–51. doi: 10.1016/j.nurpra.2022.05.019
77. Eastburn K. Association between patient-reported symptoms of dysphagia and psychological distress in head and neck cancer survivors. Number 1/January 2022. (2022) 49(1):81–9. doi: 10.1188/22.ONF.81-89
78. Li C, Qiu C, Shi Y, Yang T, Shao X, Zheng D. Experiences and perceptions of stroke patients living with dysphagia: a qualitative meta-synthesis. J Clin Nurs. (2022) 31(7-8):820–31. doi: 10.1111/jocn.15995
79. Li Y, Xu Z, Zhang X, Ma D, Meng X, Zhang M, et al. Predictors of complete oral feeding resumption after feeding tube placement in patients with stroke and dysphagia: a systematic review. J Clin Nurs. (2023) 32(11-12):2533–46. doi: 10.1111/jocn.16404
80. Lin R, Chen H, Chen L, Lin X, He J, Li H. Effects of a spray-based oropharyngeal moisturising programme for patients following endotracheal extubation after cardiac surgery: a randomised, controlled three-arm trial. Int J Nurs Stud. (2022) 130:104214. doi: 10.1016/j.ijnurstu.2022.104214
81. McGinley JM, Marsack-Topolewski CN. A comparative case study of hospice and hospital end-of-life care for aging adults with developmental disabilities. Glob Qual Nurs Res. (2022) 9:23333936221087626. doi: 10.1177/23333936221087626
82. Cardoso AF, Ribeiro LE, Santos T, Pinto M, Rocha C, Magalhães J, et al. Oral hygiene in patients with stroke: a best practice implementation project protocol. Nurs Rep. (2023) 13(1):148–56. doi: 10.3390/nursrep13010016
83. Hsu WC, Tsai HH, Weng LC, Wang YW. The experience of eating for older nursing home residents with dysphagia: a qualitative descriptive study. Int J Older People Nurs. (2023) 18(6):e12566. doi: 10.1111/opn.12566
84. Chipps E, Gatens C, Genter L, Musto M, Dubis-Bohn A, Gliemmo M, et al. Pilot study of an oral care protocol on poststroke survivors. Rehabil Nurs J. (2014) 39(6):294–304. doi: 10.1002/rnj.154
85. Kosevich G, Leinfelder A, Sandin KJ, Swift E, Taber S, Weber R, et al. Nurse practitioners in medical rehabilitation settings: a description of practice roles and patterns. J Am Assoc Nurse Pract. (2014) 26(4):194–201. doi: 10.1002/2327-6924.12038
86. Horne M, McCracken G, Walls A, Tyrrell PJ, Smith CJ. Organisation, practice and experiences of mouth hygiene in stroke unit care: a mixed-methods study. J Clin Nurs. (2015) 24(5-6):728–38. doi: 10.1111/jocn.12665
87. Goh CE, Guay MP, Lim MY, Lim SM, Loke SY, Toh HE, et al. Correlates of attitudes and perceived behavioural control towards oral care provision among trained and untrained nursing home caregivers in Singapore. J Clin Nurs. (2016) 25(11-12):1624–33. doi: 10.1111/jocn.13162
88. Ajwani S, Jayanti S, Burkolter N, Anderson C, Bhole S, Itaoui R, et al. Integrated oral health care for stroke patients–a scoping review. J Clin Nurs. (2017) 26(7-8):891–901. doi: 10.1111/jocn.13520
89. Celik GG, Eser I. Examination of intensive care unit patients’ oral health. Int J Nurs Pract. (2017) 23(6):e12592. doi: 10.1111/ijn.12592
90. Choi JS, Yi YJ, Donnelly LR. Oral health of older residents in care and community dwellers: nursing implications. Int Nurs Rev. (2017) 64(4):602–9. doi: 10.1111/inr.12417
91. Coker E, Ploeg J, Kaasalainen S, Carter N. Nurses’ oral hygiene care practices with hospitalised older adults in postacute settings. Int J Older People Nurs. (2017) 12(1):e12124. doi: 10.1111/opn.12124
92. Jablonski RA, Winstead V, Azuero A, Ptacek T, Jones-Townsend C, Byrd E, et al. Feasibility of providing safe mouth care and collecting oral and fecal microbiome samples from nursing home residents with dysphagia: proof of concept study. J Gerontol Nurs. (2017) 43(9):9–15. doi: 10.3928/00989134-20170811-04
93. Andersson M, Wilde-Larsson B, Carlsson E, Persenius M. Older people’s perceptions of the quality of oral care in short-term care units: a cross-sectional study. Int J Older People Nurs. (2018) 13(2):e12185. doi: 10.1111/opn.12185
94. Lewis A, Edwards S, Whiting G, Donnelly F. Evaluating student learning outcomes in oral health knowledge and skills. J Clin Nurs. (2018) 27(11-12):2438–49. doi: 10.1111/jocn.14082
95. Bhagat V, Hoang H, Crocombe LA, Goldberg LR. Incorporating oral health care education in undergraduate nursing curricula—a systematic review. BMC Nurs. (2020) 19(1):66. doi: 10.1186/s12912-020-00454-6
96. Bhagat V, Hoang H, Crocombe LA, Goldberg LR. Australian nursing students’ perception, knowledge, and attitude towards oral healthcare of older people and associated factors: a national cross-sectional survey. BMC Nurs. (2023) 22(1):190. doi: 10.1186/s12912-023-01366-x
97. Blackman I, Henderson J, Weger K, Willis E. Causal links associated with missed residential aged care. J Nurs Manag. (2020) 28(8):1909–17. doi: 10.1111/jonm.12889
98. Bellander L, Andersson P, Nordvall D, Hägglin C. Oral health among older adults in nursing homes: a survey in a national quality register, the senior alert. Nurs Open. (2021) 8(3):1262–74. doi: 10.1002/nop2.743
99. Chen L, Gu L, Li X, Chen W, Zhang L. Oral health matters in cognitive impaired aged residents in geriatric care facilities: a cross-sectional survey. Nurs Open. (2021) 8(2):792–8. doi: 10.1002/nop2.683
100. Krausch-Hofmann S, Palmers E, Declerck D, Duyck J. Development of practice guidelines for daily oral care in care-dependent older adults to complement the InterRAI suite of instruments using a modified delphi approach. Int J Older People Nurs. (2021) 16(1):e12351. doi: 10.1111/opn.12351
101. El-Rabbany M, Zaghlol N, Bhandari M, Azarpazhooh A. Prophylactic oral health procedures to prevent hospital-acquired and ventilator-associated pneumonia: a systematic review. Int J Nurs Stud. (2015) 52(1):452–64. doi: 10.1016/j.ijnurstu.2014.07.010
102. Axelsson M, Bahtsevani C, Neziraj M, Persson K, Kumlien C. A registry study of oral health problems and preventive interventions among older persons receiving municipal healthcare–PROSENIOR. Nurs Open. (2023) 10(2):525–34. doi: 10.1002/nop2.1318
103. Carter N. Oral health is important and should be part of a care plan: enabling older people to look after their teeth helps prevent serious disease and allows them to maintain their dignity. Nurs Older People. (2018) 30(4):14. doi: 10.7748/nop.30.4.14.s13
104. Hoben M, Clarke A, Huynh KT, Kobagi N, Kent A, Hu H, et al. Barriers and facilitators in providing oral care to nursing home residents, from the perspective of care aides: a systematic review and meta-analysis. Int J Nurs Stud. (2017) 73:34–51. doi: 10.1016/j.ijnurstu.2017.05.003
105. Kim Y, Ku HM, Jun MK. Knowledge evaluation of oral diseases and perception of cooperation with dental experts for oral care of nurses in intensive care units in Korea: a preliminary study. Nurs Rep. (2023) 13(1):528–38. doi: 10.3390/nursrep13010048
106. Kolanowski AM, Resnick B, Beck C, Grady PA. Advances in nonpharmacological interventions, 2011–2012. Res Gerontol Nurs. (2013) 6(1):5–8. doi: 10.3928/19404921-20121204-03
107. Lewis A, Harvey G, Hogan M, Kitson A. Can oral healthcare for older people be embedded into routine community aged care practice? A realist evaluation using normalisation process theory. Int J Nurs Stud. (2019) 94:32–41. doi: 10.1016/j.ijnurstu.2018.12.016
108. Wong G, Koo TF, Fethney J, Chen R. Assessing oral health literacy of university nursing students: a cross-sectional exploratory study. Nurse Educ Pract. (2021) 53:103066. doi: 10.1016/j.nepr.2021.103066
109. Hannah E, John RM. Everything the nurse practitioner should know about pediatric feeding tubes. J Am Assoc Nurse Pract. (2013) 25(11):567–77. doi: 10.1002/2327-6924.12075
110. Kells M, Kelly-Weeder S. Nasogastric tube feeding for individuals with anorexia nervosa: an integrative review. J Am Psychiatr Nurses Assoc. (2016) 22(6):449–68. doi: 10.1177/1078390316657872
111. Anderson L. Fine-bore nasogastric tube feeding: reducing the risks. Br J Nurs. (2018) 27(12):674–5. doi: 10.12968/bjon.2018.27.12.674
112. Anderson L. Enteral feeding tubes: an overview of nursing care. Br J Nurs. (2019) 28(12):748–54. doi: 10.12968/bjon.2019.28.12.748
113. Kim H, Suh Y. Changes in the dysphagia and nutritional status of patients with brain injury. J Clin Nurs. (2018) 27(7-8):1581–8. doi: 10.1111/jocn.14226
114. Lim ML, Yong BY, Mar MQ, Ang SY, Chan MM, Lam M, et al. Caring for patients on home enteral nutrition: reported complications by home carers and perspectives of community nurses. J Clin Nurs. (2018) 27(13-14):2825–35. doi: 10.1111/jocn.14347
115. Price C. Nutrition: reducing the hypermetabolic response to thermal injury. Br J Nurs. (2018) 27(12):661–70. doi: 10.12968/bjon.2018.27.12.661
116. Evans PT, Smith MC, Collins NE, Prendergast KM, Schneeberger SJ, Kopp EB, et al. Multidisciplinary bedside procedure service. J Nurse Pract. (2020) 16(4):290–3. doi: 10.1016/j.nurpra.2020.01.020
117. Hochwald IH, Yakov G, Radomyslsky Z, Danon Y, Nissanholtz-Gannot R. Ethical challenges in end-stage dementia: perspectives of professionals and family care-givers. Nurs Ethics. (2021) 28(7-8):1228–43. doi: 10.1177/0969733021999748
118. Kwok MW, Glass GF Jr, Loke S, Loi JN, Chan EY. I see, I learn, I do: development and evaluation of a video-enhanced nasogastric tube feeding training programme for caregivers. Nurs Open. (2023) 10(4):2357–65. doi: 10.1002/nop2.1491
119. Best C. How to set up and administer an enteral feed via a nasogastric tube. Nurs Stand. (2017) 31(45):42–7. doi: 10.7748/ns.2017.e10509
120. Brotfain E, Erblat A, Luft P, Elir A, Gruenbaum BF, Livshiz-Riven I, et al. Nurse-performed ultrasound assessment of gastric residual volume and enteral nasogastric tube placement in the general intensive care unit. Intensive and Critical Care Nursing. (2022) 69:103183. doi: 10.1016/j.iccn.2021.103183
121. Cao L, Zhang L, Wang X, Chinese Critical Ultrasound Study Group. Ultrasound applications to support nursing care in critically ill COVID-19 patients. Intensive Crit Care Nurs. (2020) 61:102918. doi: 10.1016/j.iccn.2020.102918
122. Fan PE, Tan SB, Farah GI, Cheok PG, Chock WT, Sutha W, et al. Adequacy of different measurement methods in determining nasogastric tube insertion lengths: an observational study. Int J Nurs Stud. (2019) 92:73–8. doi: 10.1016/j.ijnurstu.2019.01.003
123. Guenter P. ENFit® feeding tube connectors: a primer for the radiology nurse. J Radiol Nurs. (2016) 35(4):296–9. doi: 10.1016/j.jradnu.2016.10.004
124. de Oliveira Santos SC, Woith W, de Freitas MI, Zeferino EB. Methods to determine the internal length of nasogastric feeding tubes: an integrative review. Int J Nurs Stud. (2016) 61:95–103. doi: 10.1016/j.ijnurstu.2016.06.004
125. Simons S, Remington R. The percutaneous endoscopic gastrostomy tube: a nurse’s guide to PEG tubes. Medsurg Nurs. (2013) 22(2):77–83.23802493
126. Tsai HH, Tsai YF, Liu CY. Advance directives and mortality rates among nursing home residents in Taiwan: a retrospective, longitudinal study. Int J Nurs Stud. (2017) 68:9–15. doi: 10.1016/j.ijnurstu.2016.12.006
127. Spence DL, Han T, McGuire J, Couture D. Obstructive sleep apnea and the adult perioperative patient. J Perianesth Nurs. (2015) 30(6):528–45. doi: 10.1016/j.jopan.2014.07.014
128. Higginson R, Parry A. Emergency airway management: common ventilation techniques. Br J Nurs. (2013) 22(7):366–8. 370–1. doi: 10.12968/bjon.2013.22.7.366
129. Balusik B. Management of dysphagia in patients with head and neck cancer. Clin J Oncol Nurs. (2014) 18(2):149–50. doi: 10.1188/14.CJON.149-150
130. Symons VC, McMurray A. Factors influencing nurses to withhold surgical patients’ oral medications pre- and postoperatively. Collegian. (2014) 21(4):267–74. doi: 10.1016/j.colegn.2013.05.004
131. Atkinson K. Neurological conditions and acute dysphagia. Br J Nurs. (2019) 28(8):490–2. doi: 10.12968/bjon.2019.28.8.490
132. Arulvarathan C, Ding Y. A retrospective pilot study on patients who deteriorated while admitted to a neurovascular ward. Br J Neurosci Nurs. (2017) 13(6):282–7. doi: 10.12968/bjnn.2017.13.6.282
133. Pu D, Yiu EML, Chan KMK. Factors associated with signs of aspiration in older adults: a prospective study. Geriatr Nurs. (2020) 41(5):635–40. doi: 10.1016/j.gerinurse.2020.03.019
134. Sanders C. Taking an acute stroke service to the next level: how an advanced nurse practitioner programme transformed our practice and improved access and outcomes for our patients. Nurs Stand. (2020) 34(5):72–4. doi: 10.7748/ns.35.4.72.s22
135. Chiang CK, Hwu YJ. Feeding experiences of nursing aides for residents with dysphagia. Geriatr Nurs. (2018) 39(4):436–42. doi: 10.1016/j.gerinurse.2017.12.016
136. Park KD, Kim TH, Lee SH. The gugging swallowing screen in dysphagia screening for patients with stroke: a systematic review. Int J Nurs Stud. (2020) 107:103588. doi: 10.1016/j.ijnurstu.2020.103588
137. Sivertsen J, Graverholt B, Espehaug B. Dysphagia screening after acute stroke: a quality improvement project using criteria-based clinical audit. BMC Nurs. (2017) 16:27. doi: 10.1186/s12912-017-0222-6
138. Atkinson K. Shared decision making in dysphagia. Br J Nurs. (2022) 31(13):S21–4. doi: 10.12968/bjon.2022.31.13.S21
139. Barber C. Management of bulbar symptoms in motor neurone disease: a community speech and language therapist perspective. Br J Neurosci Nurs. (2015) 11(1):41–6. doi: 10.12968/bjnn.2015.11.1.41
140. Jackson J, Morrissette PJ. Exploring the experience of Canadian registered psychiatric nurses: a phenomenological study. J Psychiatr Ment Health Nurs. (2014) 21(2):138–44. doi: 10.1111/jpm.12064
141. Kenedi H, Campbell-Vance J, Reynolds J, Foreman M, Dollaghan C, Graybeal D, et al. Implementation and analysis of a free water protocol in acute trauma and stroke patients. Crit Care Nurse. (2019) 39(3):e9–17. doi: 10.4037/ccn2019238
142. Nazarko L. Risks associated with thickening powder. Nurs Resid Care. (2015) 17(4):127–127. doi: 10.12968/nrec.2015.17.3.127
143. Tanner DC, Culbertson WR. Avoiding negative dysphagia outcomes. Online J Issues Nurs. (2014) 19(2):3. doi: 10.3912/OJIN.Vol19No02PPT03
144. Stefanacci RG, Haimowitz D. Assisting with food glorious food. Geriatr Nurs. (2016) 37(2):150–2. doi: 10.1016/j.gerinurse.2016.02.007
145. Bell N, Brammer L. A team approach to supporting the nutritional needs of patients living with multiple sclerosis. Br J Community Nurs. (2017) 22(3):124–8. doi: 10.12968/bjcn.2017.22.3.124
146. Dieplinger A, Kundt FS, Lorenzl S. Palliative care nursing for patients with neurological diseases: what makes the difference? Br J Nurs. (2017) 26(6):356–9. doi: 10.12968/bjon.2017.26.6.356
147. Bail K, Gibson D, Hind A, Strickland K, Paterson C, Merrick E, et al. 'It enables the carers to see the person first': qualitative evaluation of point-of-care digital management system in residential aged care. J Clin Nurs. (2023) 32(1-2):174–90. doi: 10.1111/jocn.16285
148. Luckett T, Pond D, Mitchell G, Chenoweth L, Amgarth-Duff I, Disalvo D, et al. Eating and drinking-related care for persons with advanced dementia in long-term care. Collegian. (2023) 30(4):548–56. doi: 10.1016/j.colegn.2023.03.005
149. Matarasso Greenfeld S, Gil E, Agmon M. A bridge to cross: tube feeding and the barriers to implementation of palliative care for the advanced dementia patient. J Clin Nurs. (2022) 31(13-14):1826–34. doi: 10.1111/jocn.15437
150. Oda K, Montayre J, Parsons J, Boyd M. Oral care in hospital settings: breaking the vicious circle of older adult deconditioning. J Gerontol Nurs. (2021) 47(6):7–12. doi: 10.3928/00989134-20210507-01
151. Fjeld KG, Eide H, Mowe M, Hove LH, Willumsen T. Dental hygiene registration: development, and reliability and validity testing of an assessment scale designed for nurses in institutions. J Clin Nurs. (2017) 26(13-14):1845–53. doi: 10.1111/jocn.13452
152. Hilton S, Sheppard JJ, Hemsley B. Feasibility of implementing oral health guidelines in residential care settings: views of nursing staff and residential care workers. Appl Nurs Res. (2016) 30:194–203. doi: 10.1016/j.apnr.2015.10.005
153. Atakro CA. Knowledge of Ghanaian graduating undergraduate nurses about ageing. SAGE Open Nursing. (2021) 7:23779608211020957. doi: 10.1177/23779608211020957
154. Crawford D, Dearmun A. Opitz-Frias syndrome. Nurs Child Young People 2014. (2017) 29(10):20. doi: 10.7748/ncyp.29.10.20.s24
155. Hunt A, Harding K. ‘Check me for sepsis, that’s all I ask': a deteriorating patient with a learning disability can present with the most common triggers for this deadly condition. Emerg Nurse. (2019) 27(5):11. doi: 10.7748/en.27.5.11.s9
156. John JS, Berger L. Using the gugging swallowing screen (GUSS) for dysphagia screening in acute stroke patients. J Contin Educ Nurs. (2015) 46(3):103–4157. doi: 10.3928/00220124-20150220-12
157. Lennard C. Best interest versus advance decisions to refuse treatment in advance care planning for neurodegenerative illness. Br J Nurs. (2018) 27(21):1261–7. doi: 10.12968/bjon.2018.27.21.1261
158. Denkyi L. An exploration of pre-operative fasting practices in adult patients having elective surgery. Br J Nurs. (2020) 29(7):436–41. doi: 10.12968/bjon.2020.29.7.436
159. Mestecky AM. Research roundup. Br J Neurosci Nurs. (2013) 9(6):308–9. doi: 10.12968/bjnn.2013.9.6.308
160. Miller S. Assessment of airway defenses in the neurologically impaired patient. Medsurg. Nurs. (2017) 26(2):113–8.30304592
161. Ojo O. The role of nutrition and hydration in disease prevention and patient safety. Br J Nurs. (2017) 26(18):1020–2. doi: 10.12968/bjon.2017.26.18.1020
162. Saez LR, Harrison J, Hill J. How common is dysphagia in older adults living at home and what are the potential risk factors? Br J Community Nurs. (2023) 28(1):16–20. doi: 10.12968/bjcn.2023.28.1.16
163. Yoshida M, Miura Y, Yabunaka K, Sato N, Matsumoto M, Yamada M, et al. Efficacy of an education program for nurses that concerns the use of point-of-care ultrasound to monitor for aspiration and pharyngeal post-swallow residue: a prospective, descriptive study. Nurse Educ Pract. (2020) 44:102749. doi: 10.1016/j.nepr.2020.102749
164. Zheng XZ, Xiong QJ, Liu D, Wei K, Lai Y. Effectiveness of acupuncture therapy on postoperative nausea and vomiting after gynecologic surgery: a meta-analysis and systematic review. J Perianesth Nurs. (2021) 36(5):564–72. doi: 10.1016/j.jopan.2020.12.005
165. Gozaloff B, Ellison J, Drayton A, Abro J. Treating post-operative nausea and vomiting with isoprophly alcohol inhalation. J Perianesth Nurs. (2016) 31(4):e18–9. doi: 10.1016/j.jopan.2016.04.044
166. Semerci R, Akgun Kostak M, Taskin C. The effect of using an interactive mobile application for the management of chemotherapy-induced nausea and vomiting in children: randomized controlled study. Eur J Oncol Nurs. (2022) 58:102121. doi: 10.1016/j.ejon.2022.102121
167. Cummings J, Soomans D, O’Laughlin J, Snapp V, Jodoin A, Proco H, et al. Sensitivity and specificity o f a nurse dysphagia screen in stroke patients. Medsurg Nurs. (2015) 24(4):219–22.26434033
168. Miura Y, Tamai N, Kitamura A, Yoshida M, Takahashi T, Mugita Y, et al. Diagnostic accuracy of ultrasound examination in detecting aspiration and pharyngeal residue in patients with dysphagia: a systematic review and meta-analysis. Jpn J Nurs Sci. (2021) 18(2):e12396. doi: 10.1111/jjns.12396
169. Perry L, Hamilton S, Williams J, Jones S. Nursing interventions for improving nutritional status and outcomes of stroke patients: descriptive reviews of processes and outcomes. Worldviews Evid Based Nurs. (2013) 10(1):17–40. doi: 10.1111/j.1741-6787.2012.00255.x
170. Zhang H, Zheng L, Tang M, Guo F, Yang L, Liu S, et al. Developing strategies “SATIA”: how to manage dysphagia in older people? A Delphi panel consensus. Nurs Open. (2023) 10(4):2376–91. doi: 10.1002/nop2.1493
171. Kalani Z, Ebrahimi S, Fallahzadeh H. Effects of the liaison nurse management on the infectious stroke complications: a randomized controlled trial. BMC Nurs. (2022) 21(1):29. doi: 10.1186/s12912-021-00802-0
172. Bordonada K. The impact of the nurse navigator on patients on a colorectal surgery pathway. Medsurg Nurs. (2020) 29(2):109–16.
173. Allen KD, DiBartolo MC, Welsh DL, Brown V. Design of a medical triage evidence-based clinical management protocol and implementation of medical triage on-line training for use by mission of mercy volunteers. J Community Health Nurs. (2015) 32(4):218–30. doi: 10.1080/07370016.2015.1087273
174. Madiloggovit J, Chotechuang N, Trachootham D. Impact of self-tongue brushing on taste perception in Thai older adults: a pilot study. Geriatr Nurs. (2016) 37(2):128–36. doi: 10.1016/j.gerinurse.2015.11.004
175. Crabtree E, Brennan E, Davis A, Coyle A. Improving patient care through nursing engagement in evidence-based practice. Worldviews Evid Based Nurs. (2016) 13(2):172–5. doi: 10.1111/wvn.12126
176. Fabiani A, Sanson G, Bottigliengo D, Dreas L, Zanetti M, Lorenzoni G, et al. Impact of a natural versus commercial enteral-feeding on the occurrence of diarrhea in critically ill cardiac surgery patients. A retrospective cohort study. Int J Nurs Stud. (2020) 108:103605. doi: 10.1016/j.ijnurstu.2020.103605
177. Gabriel S, Ackermann R, Gabriel S, Ackermann C, Swadener-Culpepper L. Evaluation of a nasoenteral feeding tube with balloon to facilitate placement. Crit Care Nurse. (2020) 40(1):37–44. doi: 10.4037/ccn2020845
178. Wu K, Chen Y, Yan C, Huang Z, Wang D, Gui P, et al. Effects of percutaneous endoscopic gastrostomy on survival of patients in a persistent vegetative state after stroke. J Clin Nurs. (2017) 26(19-20):3232–8. doi: 10.1111/jocn.13672
179. Zapka J, Amella E, Magwood G, Madisetti M, Garrow D, Batchelor-Aselage M. Challenges in efficacy research: the case of feeding alternatives in patients with dementia. J Adv Nurs. (2014) 70(9):2072–85. doi: 10.1111/jan.12365
180. Alves do Nascimento L, de Oliveira Lopes MV, Fahl Fonseca L. Development and validation of a new nursing diagnosis: perioperative thirst. Int J Nurs Knowl. (2021) 32(4):253–61. doi: 10.1111/2047-3095.12319
181. Conway A, Chang K, Bittner M, Phan D, Kamboj N, Parotto M, et al. Validating the peri-operative thirst discomfort scale for measuring thirst discomfort prior to procedures. J Radiol Nurs. (2021) 40(1):75–9. doi: 10.1016/j.jradnu.2020.10.006
182. Gümüs K, Pirhan Y, Aydın G, Keloglan S, Tasova V, Kahveci M. The effect of preoperative oral intake of liquid carbohydrate on postoperative stress parameters in patients undergoing laparoscopic cholecystectomy: an experimental study. J Perianesth Nurs. (2021) 36(5):526–31. doi: 10.1016/j.jopan.2020.10.012
183. Denton TD. Southern hospitality: how we changed the npo practice in the emergency department. J Emerg Nurs. (2015) 41(4):317–22. doi: 10.1016/j.jen.2014.12.001
184. Flaubert JL, Le Menestrel S, Williams DR, Wakefield MK. National academies of sciences, engineering, and medicine; national academy of medicine; committee on the the future of nursing 2020-2030: charting a path to achieve health equity. In: Flaubert JL, Le Menestrel S, Williams DR, et al. editors. National Academies of Sciences, Engineering, and Medicine; National Academy of Medicine; Committee on the Future of Nursing 2020–2030. Washington (DC): National Academies Press (US) (2021). https://www.ncbi.nlm.nih.gov/books/NBK573922/
185. Martino R, Foley N, Bhogal S, Diamant N, Speechley M, Teasell R. Dysphagia after stroke. Stroke. (2005) 36(12):2756–63. doi: 10.1161/01.STR.0000190056.76543.eb
186. Hibberd J, Fraser J, Chapman C, McQueen H, Wilson A. Can we use influencing factors to predict aspiration pneumonia in the United Kingdom? Multidiscip Respir Med. (2013) 8(1):39. doi: 10.1186/2049-6958-8-39
187. Langmore SE, Terpenning MS, Schork A, Chen Y, Murray JT, Lopatin D, et al. Predictors of aspiration pneumonia: how important is dysphagia? Dysphagia. (1998) 13(2):69–81. doi: 10.1007/PL00009559
188. Ball L, Meteyard L, Powell RJ. Predictors of aspiration pneumonia: developing a new matrix for speech and language therapists. Eur Arch Otorhinolaryngol. (2023) 280(11):5101–14. doi: 10.1007/s00405-023-08153-z
189. Huxley EJ, Viroslav J, Gray WR, Pierce AK. Pharyngeal aspiration in normal adults and patients with depressed consciousness. Am J Med. (1978) 64(4):564–8. doi: 10.1016/0002-9343(78)90574-0
190. Butler SG, Stuart A, Markley L, Feng X, Kritchevsky SB. Aspiration as a function of age, sex, liquid type, bolus volume, and bolus delivery across the healthy adult life span. Ann Otol Rhinol Laryngol. (2018) 127(1):21–32. doi: 10.1177/0003489417742161
191. Butler SG, Clark H, Baginski SG, Todd JT, Lintzenich C, Leng X. Computed tomography pulmonary findings in healthy older adult aspirators versus nonaspirators. Laryngoscope. (2014) 124(2):494–7. doi: 10.1002/lary.24284
192. Alagiakrishnan K, Bhanji RA, Kurian M. Evaluation and management of oropharyngeal dysphagia in different types of dementia: a systematic review. Arch Gerontol Geriatr. (2013) 56(1):1–9. doi: 10.1016/j.archger.2012.04.011
193. Lawlor CM, Choi S. Diagnosis and management of pediatric dysphagia: a review. JAMA Otolaryngol– Head Neck Surg. (2020) 146(2):183–91. doi: 10.1001/jamaoto.2019.3622
194. Marik PE, Kaplan D. Aspiration pneumonia and dysphagia in the elderly. Chest. (2003) 124(1):328–36. doi: 10.1378/chest.124.1.328
195. Eltringham S, Kilner K, Gee M, Sage K, Bray B, Pownall S, et al. Impact of dysphagia assessment and management on risk of stroke-associated pneumonia: a systematic review. Cerebrovasc Dis. (2018) 46:97–105. doi: 10.1159/000492730
196. Palli C, Fandler S, Doppelhofer K, Niederkorn K, Enzinger C, Vetta C, et al. Early dysphagia screening by trained nurses reduces pneumonia rate in stroke patients: a clinical intervention study. Stroke. (2017) 48(9):2583–5. doi: 10.1161/STROKEAHA.117.018157
197. Hines S, Kynoch K, Munday J. Nursing interventions for identifying and managing acute dysphagia are effective for improving patient outcomes: a systematic review update. J Neurosci Nurs J Am Assoc Neurosci Nurs. (2016) 48(4):215–23. doi: 10.1097/JNN.0000000000000200
198. Sloane P, Zimmerman S, Chen X, Barrick A, Poole P, Reed D, et al. Effect of a person-centered mouth care intervention on care processes and outcomes in three nursing homes. J Am Geriatr Soc. (2013) 61:1158–63. doi: 10.1111/jgs.12317
199. Nordaunet OM, Gjevjon ER, Olsson C, Aagaard H, Borglin G. What about the fundamentals of nursing—its interventions and its continuity among older people in need of home- or facility-based care: a scoping review. BMC Nurs. (2024) 23(1):59. doi: 10.1186/s12912-023-01675-1
200. Chaboyer W, Harbeck E, Lee BO, Grealish L. Missed nursing care: an overview of reviews. Kaohsiung J Med Sci. (2021) 37(2):82–91. doi: 10.1002/kjm2.12308
201. Curtin C, Barrett A, Burke FM, McKenna G, Healy L, Hayes M. Exploring facilitators and barriers associated with oral care for inpatients with dysphagia post-stroke. Gerodontology. (2023):1–11. doi: 10.1111/ger.12709
202. Mitchell G, Stark P, Wilson CB, Tsakos G, Brocklehurst P, Lappin C, et al. “Whose role is it anyway?” experiences of community nurses in the delivery and support of oral health care for older people living at home: a grounded theory study. BMC Nurs. (2023) 22(1):359. doi: 10.1186/s12912-023-01533-0
203. Gramlich L, Hurt RT, Jin J, Mundi MS. Home enteral nutrition: towards a standard of care. Nutrients. (2018) 10(8):1–11. doi: 10.3390/nu10081020
204. Elmahdi A, Eisa M, Omer E. Aspiration pneumonia in enteral feeding: a review on risks and prevention. Nutr Clin Pract Off Publ Am Soc Parenter Enter Nutr. (2023) 38(6):1247–52. doi: 10.1002/ncp.11020
Keywords: aspiration pneumonia, nursing, dysphagia, oral hygiene, tube feeding, mapping review
Citation: Lisiecka D, Kearns Á, Evans W and Farrell D (2024) Aspiration pneumonia in nursing literature—a mapping review. Front. Rehabil. Sci. 5: 1393368. doi: 10.3389/fresc.2024.1393368
Received: 29 February 2024; Accepted: 3 June 2024;
Published: 24 July 2024.
Edited by:
Phyllis Palmer, University of New Mexico, United StatesReviewed by:
Tamer Abou-Elsaad, Mansoura University, Egypt© 2024 Lisiecka, Kearns, Evans and Farrell. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dominika Lisiecka, ZG9taW5pa2EubGlzaWVja2FAbXR1Lmll
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.