 Jonathan Rioual1
Jonathan Rioual1 Célia Perret1
Célia Perret1 Catherine Arnaud1,2
Catherine Arnaud1,2 Nicolas Vidart d’Egurbide Bagazgoïtia1*
Nicolas Vidart d’Egurbide Bagazgoïtia1* on behalf the SPARCLE3 collaborative group
on behalf the SPARCLE3 collaborative group
- 1UMR 1295 CERPOP, Inserm, Toulouse University III Paul Sabatier, Team SPHERE, Toulouse, France
- 2Clinical Epidemiology Unit, University Hospital, Toulouse, France
Introduction: Optimizing care for young adults with cerebral palsy is crucial for their physical and psychological well-being. The inadequacy of proximal environment may play a role in the provision of health services. The aim of this study is to explore the association between unmet environmental needs in the physical, social and attitudinal domains and unmet healthcare needs in four interventions: physiotherapy, occupational therapy, speech therapy and psychological counselling.
Methods: Young adults with cerebral palsy were recruited in the SPARCLE3 European multicenter cross-sectional study. Healthcare needs and coverages were assessed using the Youth Health Care, Satisfaction, Utilization and Needs questionnaire. The need and availability of environmental factors in physical, social and attitudinal domains were collected using the European Adult Environment Questionnaire. Logistic regressions were conducted separately for each intervention to measure associations between unmet environmental needs and unmet healthcare needs.
Results: We studied 310 young adults with cerebral palsy, with a mean age of 24.3 years; 37.4% could not walk independently, 51.5% had an IQ below 70, 34.2% had severe communication difficulties. The most commonly expressed need was physiotherapy (81.6% of participants). Unmet healthcare needs were reported by 20.9%, 32.4%, 40.3% and 49.0% of participants requiring physiotherapy, occupational therapy, psychological counselling and speech therapy, respectively. The physical environment was never significantly associated with unmet healthcare needs. In contrast, the social environment was significantly associated with unmet healthcare needs across all interventions, with odds ratios over 2.5, depending on the number of unmet needs and the nature of intervention needed. With regard to the attitudinal environment, when at least one unmet attitudinal environmental need was reported, the odds of also reporting an unmet healthcare need were of 3.68 for speech therapy and 3.77 for physiotherapy. The latter association was significant only for individuals with severe motor impairment.
Discussion: Our results highlight the importance of the social and attitudinal environment in meeting healthcare needs in young adults with cerebral palsy. The lack of correlation between unmet healthcare needs and the physical environment suggests that it can be partly compensated for by social support.
Introduction
The 2006 United Nations Convention on the Rights of Persons with Disabilities (1) underlines the obligation of Member States to take appropriate measures to ensure access for persons with disabilities to all aspects of life in order to promote their full participation in society on the basis of equal opportunities. Access to health services is one the major obstacles to equal opportunity for people with disabilities, particularly those with cerebral palsy.
Cerebral palsy (CP) is a complex condition that requires lifelong multidisciplinary care (2, 3). This care encompasses, among other things, access to specialized medical services, rehabilitation interventions, and psychological counselling. Optimizing and personalizing care is of paramount importance in meeting the specific needs of individuals with CP and maximizing their physical and psychological well-being (4). Medical advances have enabled individuals with CP to live longer, bringing their life expectancy closer to that of the general population (5). However, with improved survival come new health challenges. Young adults with CP face specific health issues, including a variety of clinical manifestations associated with CP (6) and early deterioration in health status (7). Compared with the general population, these young adults experience reduced walking ability, increased pain and fatigue, and mental health problems. It is therefore crucial to take account of these specific needs to provide them with appropriate care.
However, young adults with CP often have less access to health services in adulthood than they did in childhood (8) and face complex and varied barriers, such as a lack of specialized services tailored to adults or limited knowledge about adult CP among health professionals, that lead to gaps in continuity of care. As the International Classification of Functioning, Disability and Health (ICF) has defined disability since 2001 as resulting from a dynamic interaction between “body functions and structures” and “personal and environmental contextual factors”, we should also consider the inadequacy of the environment as a potential barrier to accessing health services.
There is little in-depth research specifically examining the overall impact of the environment on access to care for young adults with CP. The majority of existing studies have focused mainly on the medical and clinical aspects of care (9, 10), paying less attention to environmental factors likely to influence access to care. However, in the case of chronic conditions such as CP, it is often easier to modify an individual's environment than their abilities or bodily functions (11). It is therefore crucial to understand the extent to which inadequate physical, social, and attitudinal environments are associated with access to care among these young adults. To do this, we used unmet health needs as an indicator, which allows us to capture participants' actual experiences of accessing healthcare.
We aimed to explore the association between unmet environmental needs and unmet healthcare needs by focusing on four types of intervention: physiotherapy, occupational therapy, speech therapy, and psychological counselling. We hypothesized that the accumulation of unmet needs in the environment is associated with compounded unmet needs in health domains in young adults with CP.
Methods
Design and population
We used data from SPARCLE3, a European multicenter observational population-based cross-sectional study designed to investigate the impact of the environment on participation and quality of life of young adults with CP. The design and methods of the study have been described elsewhere (12). Briefly, the study population consisted of young adults diagnosed with CP as defined by the Surveillance of Cerebral Palsy in Europe (SCPE) network (13). They were born between 1991 and 1997, and were aged between 22 and 27 years at the time of data collection (2018–2020). They were randomly selected from regional registries in France, Sweden and Italy, and recruited from various sources in two other regions in Germany and Portugal.
Data collection
Research assistants trained for the study visited the young adults with CP and conducted the interviews under identical conditions, with a logical flow and a fixed order for completing the questionnaires. Whenever possible, young adults completed the questionnaires themselves, with research assistants providing assistance as needed. When this was not possible, a relative or a personal assistant closely involved in their daily lives acted as a proxy.
Young adults with CP were asked about their healthcare needs, coverage and satisfaction of those needs, in various healthcare domains, using the short form of Youth Health Care, Satisfaction, Utilization and Needs (YHC-SUN) questionnaire (14). In this study, we considered only rehabilitation domains (physiotherapy, occupational therapy, speech therapy) and psychological counselling.
Information regarding the physical, social and attitudinal environment was collected using the European Adult Environment Questionnaire (EAEQ), a questionnaire developed as part of SPARCLE3, were which assesses the adequacy of 61 environmental factors (EF). Content density, diversity ratios and bandwidth index indicate that the EAEQ content links fairly well to the environmental classification of the ICF Core Set for adults with CP (15). Two types of information were available: the need of the EF and its availability in the event of need, or only its availability when the need was considered a priori to be common to all individuals. The responses were categorized as “unmet environmental need” when the response “Needed and not available” was provided, and “met environmental need” when the responses “Not needed” or “Needed and available” were ticked, depending on the item. In each domain of the environment, items related to access to care were selected a priori (9, 4 and 3 items in the physical, social, attitudinal domains, respectively, Supplementary Table S1).
Standardized information on impairments and comorbidities was collected: walking ability (using the Gross Motor Function Classification System, GMFCS (16) levels grouped into walkers (GMFCS I–III) and non-walkers (GMFCS IV–V)) and communication performance (Functional Communication Classification System, FCCS) (17), effective communication Yes (FCCS I–II)/No (FCCS III–V)). Intellectual ability was assessed with formal IQ testing or using an algorithm based on a set of questions to proxies (18), and thereafter categorized as <70/≥70. Young adults also reported their pain over the past week (not at all/once or twice/frequent) and seizures in the year predating interview [No (with or without medication)/Yes].
We also collected personal and family contextual factors: population size of area of residence (>200,000/3,000–200,000/<3,000 inhabitants), lifestyle [living alone independently/accompanied (family/partner)/ in care facilities], personal and parental highest education level completed (did not complete secondary education/secondary education/tertiary education), and perceived wealth (no or minimal financial difficulties/financial difficulties).
Statistical analyses
Four subgroups of people were identified according to the health needs they reported to require for physiotherapy, occupational therapy, speech therapy, or psychological counselling (19). We first described the distribution of impairments, comorbidities, and contextual factors in the whole sample and in subgroups. The proportion of young adults who reported unmet environmental needs was estimated in the same subgroups. In addition, for each environmental domain, we plotted the proportion of individuals with unmet health needs against the number of unmet environmental needs (discrete variable) to determine categories, considering individuals with no unmet needs as the reference class, and a minimum of five individuals in each category.
Thereafter, separate analyses were carried out for physiotherapy, occupational therapy, speech therapy, and psychological counselling subgroups to assess the role of environmental factors on the satisfaction of healthcare needs. Bivariate comparisons relating the proportion of individuals with unmet health needs to socio-demographic and impairments characteristics were carried out. We then performed logistic regressions to estimate odds ratios (ORs) and their 95% confidence intervals (95% CI) which measured associations between unmet environmental needs in each domain and unmet physiotherapy/occupational therapy/speech therapy/psychological counselling need. All models were adjusted for country due to the recruitment (20) and policies for people with disabilities diversity across countries, and sex (21). Model 1 was consistently adjusted for GMFCS (22) and Model 2 for the size of the unit of residence and lifestyle (10, 23), as these were described in the literature as potential confounders. To identify potential additional confounding factors, two successive stepwise selections were then performed: the first added clinical variables (intellectual ability, seizures communication performance and frequency of pain) to Models 1, while the second included sociodemographic variables (education, wealth, and parental highest education level) in addition to Models 2, with the aim of minimizing the number of variables introduced into the models. Multivariate models were used to control for significant variables in separate analyses (p < 0.20) and these models were reduced using a descending step-by-step method with p < 0.05 as criterion for statistical significance. Participants with missing data for one or more variables in the different models were few, and they were excluded from the analyses.
Finally, sensitivity analyses were conducted. First, we considered only individuals who self-completed the questionnaires. Second, to examine the impact of each country on the results, with constraints of the small sample sizes, we excluded participants from each country one by one.
All analyses were performed using R (version 4.1.2, R Core Team, 2021).
Results
Our sample consisted of 310 young adults with CP, with a mean age of 24.3 years [standard deviation (SD) 1.6 years], and a male-to-female ratio of 1.2. Table 1 shows impairments and socio-demographic characteristics. Briefly, 37.4% of individuals could not walk independently (GMFCS IV–V), 51.5% had an IQ < 70, and 34.2% had severe communication difficulties (FCCS III-V). Around 12% (11.7%) lived alone. In terms of healthcare needs, physiotherapy was the most frequently mentioned (81.6% of participants), followed by occupational therapy (47.7%), psychological counselling (40.0%), and speech therapy (31.6%). Of the participants who reported all rehabilitation needs (physiotherapy, speech therapy and occupational therapy, n = 72), 56.9% had a GMFCS IV–V, 66.7% had a FCCS level III to V, and a small proportion (4.2%) lived alone. Three quarters (75%) of those who reported a need for speech therapy, whether or not they expressed other needs, had not completed secondary education, compared with 58.0% in the total sample. The group of young adults who said they needed psychological counselling, alone or in combination with other needs, had less severe motor (33.1% with GMFCS IV–V) and cognitive (86.7% with an IQ < 70) impairments than the group as a whole. They were also more likely to live alone than participants as a whole (16.1%).
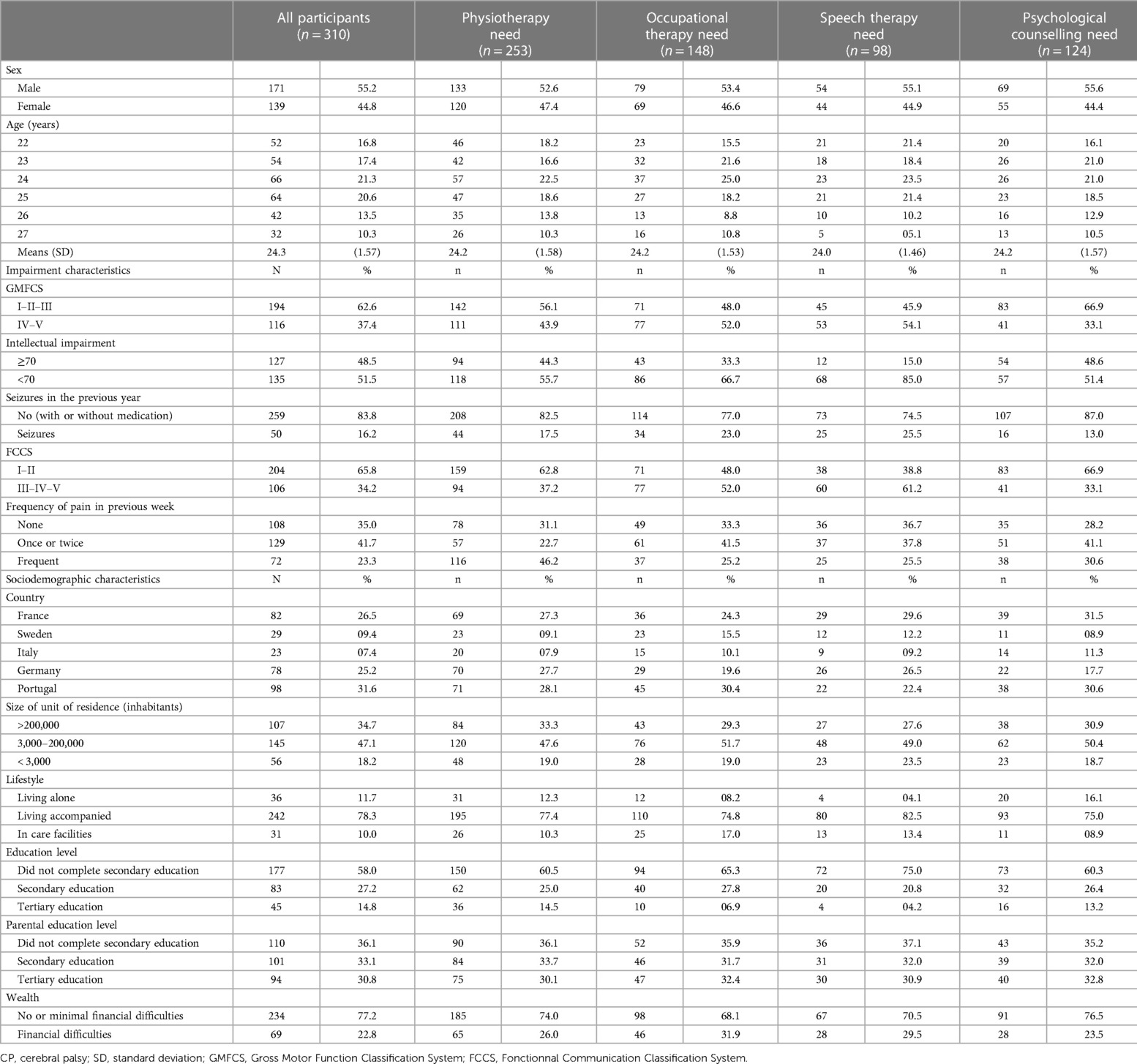
Table 1. Characteristics of young adults with CP across the entire sample and by health needs subgroups.
Table 2 shows the distribution of unmet environmental needs in the physical, social and attitudinal domains, for the whole sample and for each group that reported a healthcare need, while the responses for each EF are provided in Supplementary Table S2. The proportion of subjects reporting the highest number of unmet environmental needs per domain (4–9, 2–4 and 1–3 for the physical, social, attitudinal environments, respectively) is lowest for the social environment, overall and for each group of expressed healthcare needs. In the subgroup of individuals who reported requiring all three rehabilitation interventions, unmet needs were high: 73.2%, 38.9% and 40.8% of individuals with at least one unmet need in the physical, social, and attitudinal environments, respectively, compared to 62.1%, 27.3%, 32.7% for the same environmental domains in the whole sample. Individuals who reported a need for psychological counseling also had a higher prevalence of unmet environmental needs in all three domains compared to the whole population, with 66.9%, 32.3%, and 38.8% of individuals with at least one unmet need in each domain of environment.
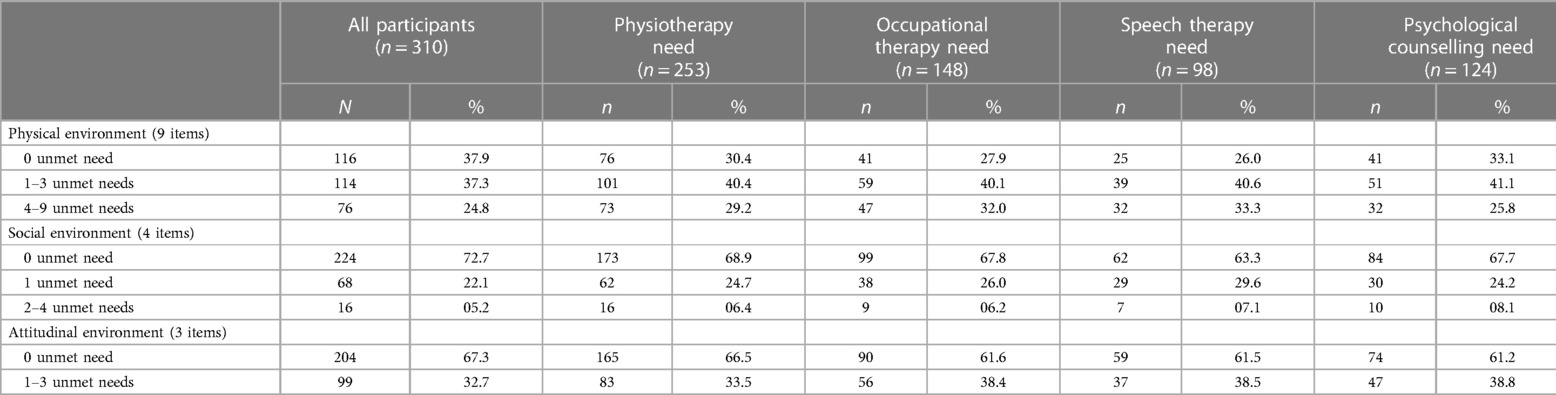
Table 2. Distribution of unmet needs in the three environmental domains within the total population and by healthcare needs subgroup.
The proportion of individuals who reported unmet healthcare needs was the lowest for physiotherapy (20.9%), followed by occupational therapy (32.4%), psychological counselling (40.3%), and speech therapy (49.0%). Table 3 shows to what extent the proportion of individuals with unmet healthcare needs varied according to nature and severity of impairments, country of residence and socio-demographic characteristics. We observed a lower proportion of people with unmet healthcare needs for all types of rehabilitation interventions in young adults with GMFCS IV–V compared to those with GMFCS I–III. Significant differences between countries were observed for physiotherapy unmet needs (from 7.1% of the participants in Germany to 31.0% in Portugal; p = 0.004) and occupational therapy unmet needs (from 4.1% in France to 44.4% in Portugal, p = 0.010).
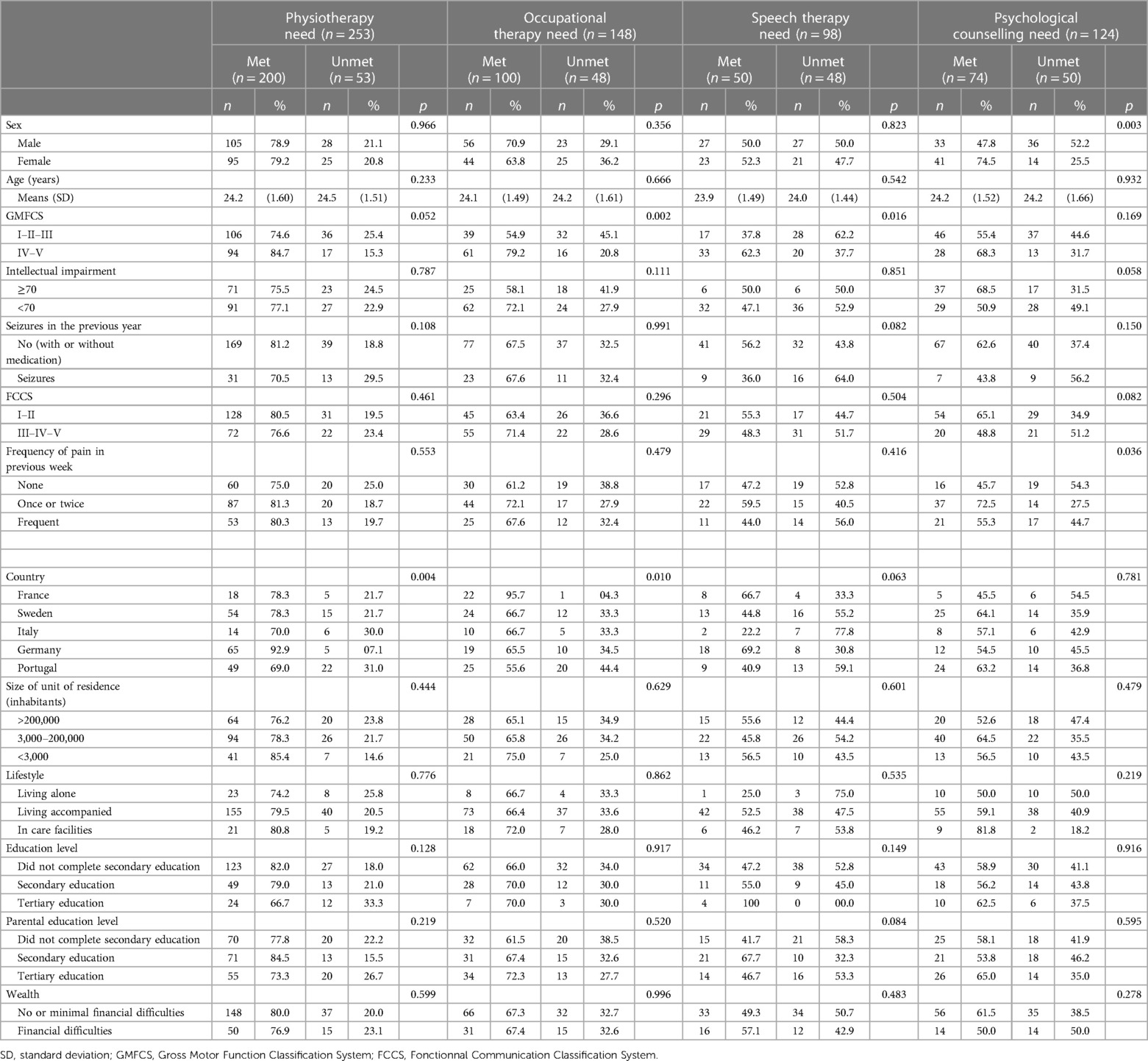
Table 3. Distribution of healthcare needs met and unmet within the four subgroups of healthcare needs.
Bivariate analyses showed an interaction between the severity of gross motor dysfunction and the attitudinal environment in participants who reported a need for physiotherapy. The corresponding models were therefore run separately for individuals with GMFCS IV–V and those with GMFCS I–III. All models were adjusted as follows. In the beginning, all models were adjusted for sex and country of residence. Of the impairments and/or comorbidities, only walking ability was included in Models 1 with the exception of participants requiring speech therapy, for whom communication performance was also retained. Models 2 incorporated these factors, along with retained sociodemographic characteristics, specifically the population size of their unit of residence and lifestyle, without the addition of any other characteristics. The physical environment was never significantly associated with unmet healthcare needs, regardless of the intervention. Conversely, the social environment was associated to varying degrees of unmet healthcare needs in all four interventions. When one unmet need for the social environmental was reported, the odds of also reporting an unmet need for physiotherapy increased more than twofold (OR 2.5; 95% CI: 1.18–5.55). When 2–4 unmet social environmental needs were reported, the odds of reporting unmet occupational therapy and psychological counselling needs were OR 6.58 (95% CI: 1.17–41.38) and 12.89 (95% CI: 2.14–120.91), respectively. A significant trend was observed for speech therapy. With regards to the attitudinal environment, when at least one unmet environmental need was reported, the odds of also reporting an unmet healthcare need increased more than three-fold for speech therapy (OR 3.68; 95% CI: 1.41–10.31) and for physiotherapy (OR 3.77; 95% CI: 1.22–12.80), the latter only in those with severe motor impairment (GMFCS IV–V) (Table 4).
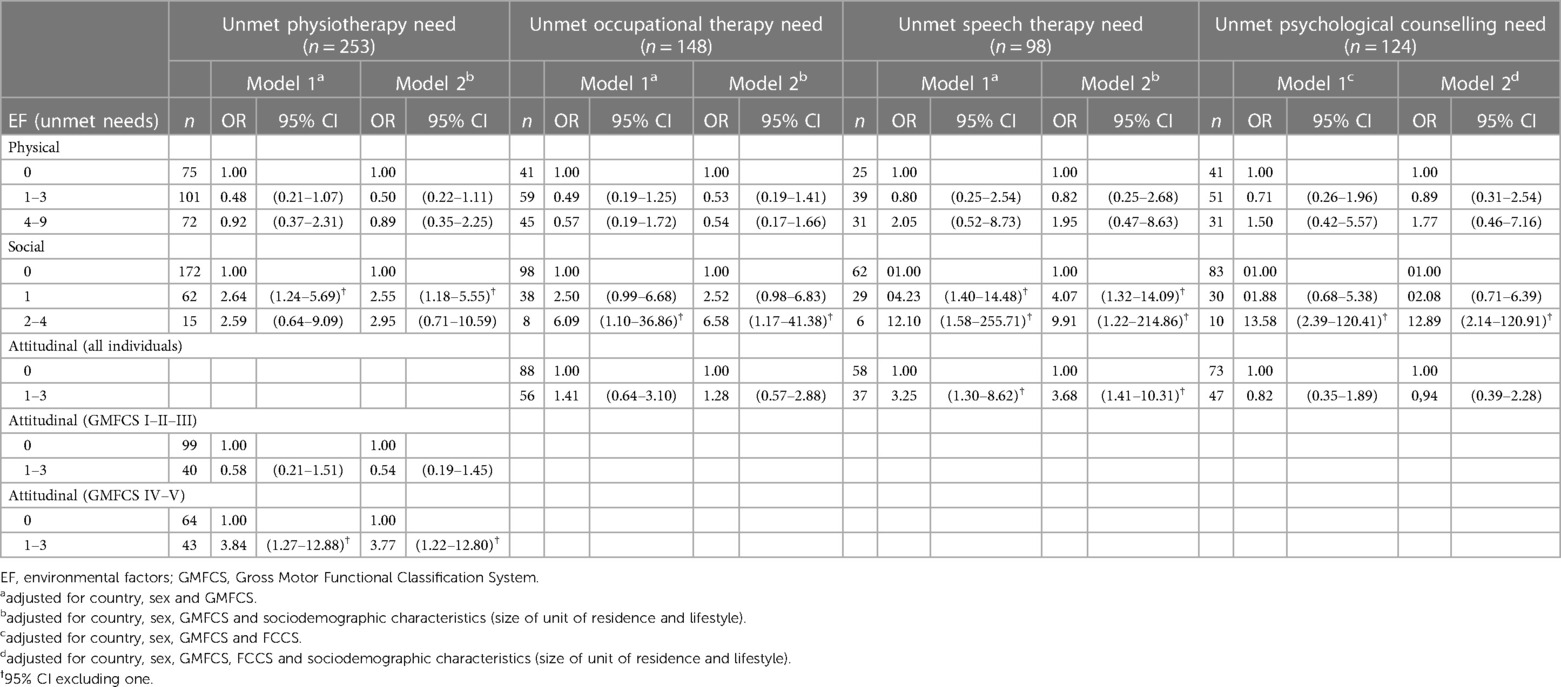
Table 4. Association between the adequacy of EF and unmet health needs in the 4 domains.
The results did not change after excluding individuals with proxy-reports or excluding participants from each country one by one.
Discussion
Key findings
Our study showed that the commonest healthcare need was physiotherapy, which was reported by more than four out of five young adults with CP. Among those who expressed a need for care, the proportion whose need was not met varied according to the type of care required: 20.8%–48.5% for rehabilitation, and 40.3% for psychological counselling. We found an association between an environment inadequate to the specific needs of young people with CP and their care needs. More specifically, the accumulation of unmet needs in the social environment, exploring support from the personal assistant, family and friends, healthcare staff and colleagues, and strangers, was associated with unmet needs in all health domains explored, even taking account of the severity of impairments and the socio-demographic characteristics of the individuals. The lack of supportive attitudes increased by more than 3-fold the odds of also reporting an unmet need for speech therapy and physiotherapy, only among those with the most severely impaired gross motor function in the latter case. Finally, our study showed no association between unmet needs in the physical environment and unmet healthcare needs.
Strengths and limitations
This cross-sectional study enrolled 310 young adults with CP, making it one of the largest studies ever conducted in this population. We identified cases either from population-based registries or from several independent sources, using the same definition of CP, which limited case selection and classification errors. Nevertheless, recruitment in Germany and Portugal, although based on a variety of sources, included rehabilitation centres, hospitals and specialized institutes, which may first result in a lack of sample representativeness, and reduce the proportion of individuals with unmet healthcare needs. It was important to take this potential selection bias into account, given that participants from these two countries represented more than half of our sample (56.8%).
We performed the analyses by pooling self-reported and proxy-reported data to maximize the inclusion in the study of severely impaired people who are not usually included in this type of studies. Although we considered that, irrespective of the respondent, self-report was the best available estimate of environmental adequacy and unmet healthcare needs, we cannot rule out underestimation or overestimation of both these pieces of information when using proxy-reports (24, 25). Nevertheless, our findings did not change when we excluded proxy-reports in our sensitivity analyses.
The measurement of the adequacy of the environment to the specific needs of the target population was based on the EAEQ, a questionnaire developed as part of the SPARCLE study to provide a comprehensive assessment in line with the ICF. As part of this exploratory study, we made choices that respected the contours of this approach. First, we selected EAEQ items in the physical (accessibility of facilities and transport), social and attitudinal environment that were important for access to care. Based on the assumption that the accumulation of unmet needs in the environment was associated with unmet healthcare needs, we summed the items in each environmental domain to create one variable by domain quantifying environmental adequacy. However, due to the low prevalence of unmet needs for some elements of the environment and the lack of existing studies to guide us in our grouping choices, we opted for a graphical categorization. This choice enabled to obtain a sufficient number of individuals per category (at least five), except for the attitudinal domain, which limited the analysis of a potential cumulative effect. Another limitation was that this method assigned the same weight to each EF, which may potentially minimize or maximize their relative contribution (26).
Interpretation
To date, relatively little research has explored the healthcare needs of young adults with CP, focusing more on the utilization of healthcare services. A literature review by Manikandan et al. (21) of 57 studies involving 14,300 adults (mean age 18–48 years) found that 44% had consulted a physiotherapist, 27% an occupational therapist, 16% a speech therapist, and 11% a psychologist or psychiatrist in the past year. Although we did not have a direct measure of health service use, we observed similar frequencies when looking at the proportion of met healthcare needs for occupational therapy and speech therapy (32%; n = 100/310% and 16%; n = 50/310, respectively), while it was higher for physiotherapy (65%; n = 200/310) and psychological counselling (24%; n = 74/310). The high proportion of participants from Germany, where the number of physiotherapists is relatively high (244 physical therapists per 100,000 inhabitants (27) compared with 144 per 100,000 in France (28), for instance) may partly explain this difference.
While the utilization of health services is an important piece of information, measuring the need for these services and assessing how often they are not met are crucial in studying the factors limiting access. We found that, in descending order of frequency, the health care needs expressed were 81.6% for physiotherapy, 47.7% for occupational therapy, 40.0% for psychological counselling and 31.6% for speech therapy. To our knowledge, no recent study has comparable data. A cross-sectional study in Ireland of 40 young people aged 16–22 in transition to adult services found that 67.5% expressed healthcare needs related to mobility (which may partly correlate with physiotherapy), 50% related to positioning (which may partly correlate with occupational therapy), and 26.3% related to speech (likely correlated with speech therapy) (29). Another Anglo-Irish study of 106 14–18 year olds found similar results, with 58.4% of needs related to mobility, 25.5% to positioning, and 21.7% to speech (24).
In the literature, speech therapy has been described as the profession with the highest proportion of unmet needs, ranging from 39% to 70% (24, 29). Conversely, physiotherapy had the lowest proportion (12%−44%) (24, 29). Our results are consistent with these observations. In our study, severe motor impairment (GMFCS IV–V) was associated with better satisfaction of healthcare needs in the four professions, which differs from the data in the literature (9, 24) which showed that the severity of the disability tended to limit access to rehabilitation and psychological counselling. With regard to socio-demographic factors, an American study showed that adult men with disabilities were less likely than women to report at least one unmet healthcare need (60.7% vs. 75.7%) (30). However, we did not find this in our sample, and even found the opposite result for psychological counselling. A French study showed that living in care facilities was associated with a reduction in unmet healthcare needs (23), which was not observed in our study.
To our best knowledge, no publication has specifically evaluated the relationship between unmet healthcare needs of young adults with CP and the adequacy of their environment to meet their specific needs. Therefore, our interpretations are based solely on the results of our study, and we only have the opportunity to put forward a few hypotheses to explain this relationship. Our results highlight the importance of the social environment and support. At this age, greater independence and emancipation, particularly from parents, could partially explain why young adults have greater unmet healthcare needs than children. It may be hypothesized that the lack of association between the physical environment and unmet healthcare needs is due to the fact that the physical environment is often compensated by social support and assistance from family and friends. Thus, a young adult could move around easily if accompanied, even in a less suitable environment, whereas an individual with less support would have more difficulty even in a better adapted physical environment. It is also conceivable that this difference might be liked to cognitive impairments, which often pose more challenges for independent mobility than motor impairments, for which adaptations are usually possible. Our findings suggest that the greater the unmet needs in the social environment, the greater the unmet healthcare needs for occupational therapy, speech therapy, and psychological counselling. However, due to the small number of participants with multiple unmet needs in their social environment, questions arise regarding these concepts, their content, and their implications for access to care for individuals with CP. Consequently, these findings should be interpreted with caution. Our findings indicated that attitudinal support was associated with unmet healthcare needs for speech therapy, which affects most people with severe motor and cognitive impairments, and for physiotherapy in people with severe motor impairments. This suggests that this support is particularly crucial to ensure access to healthcare for these therapies in severely impaired young adults with CP. We did not find this association in individuals who required occupational therapy or psychological counselling.
Conclusion
Our study showed that the adequacy of the environment, both social and attitudinal, can have an impact on unmet healthcare needs in different therapeutic areas in young adults with CP. It sheds valuable light on the factors influencing unmet health needs in this population. However, further research is needed to better understand and delineate these two environmental domains and deeper explore their relationship with access to healthcare.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by in France: The data were collected and stored in accordance with the reference methodology MR003 [Declaration No. 2205849 at the Commission for Data Protection and Liberties (CNIL)] each patient having been informed individually of the research under Article L1122–1 of the Public Health Code. In Germany: Ethikkommission der Universität zu Lübeck [AZ 18–172]. In Italy: Comitato Etico Lazio 1c/o A.O. San CamillobForlanini, Piazza Carlo Forlanini1, 00151 Roma [2143/CE Lazio 1]. In Portugal: Conselho de Ética e Deontologia, Universidade de Aveiro [CED-UA n.o 33/2018]. In Sweden: Regional Ethical Review Board in Göteborg, Sweden. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
SPARCLE 3 collaborative group
Joaquim J. M. Alvarelhão, Jérôme Fauconnier, Kate Himmelmann, Marco Marcelli, Silke Schmidt and Ute Thyen.
Author contributions
JR: Writing – original draft. CP: Writing – review & editing. CA: Writing – review & editing, Supervision. NV: Supervision, Writing – original draft.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This work was supported by the Deutsche Forschungsgemeinschaft (DFG) and the French Agence Nationale de la Recherche (ANR) [DFG-ANR N°316684170] in Germany and France, the Sunnerdahls Handikappfond, the Swedish state under the agreement between Swedish government and the country councils, the ALF-agreement (ALFGBG-726001) in Sweden, the Fondazione Carivit in Italy and the Federação das Associações Portuguesas de Paralisia Cerebral e Santa Casa da Misericórdia de Lisboa in Portugal. The funders were not involved in any way in the preparation of this manuscript or the decision to submit it.
Acknowledgments
The authors thank the young adults and their families for their generous participation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fresc.2024.1294999/full#supplementary-material
References
1. United Nations. Convention of the Rights of Persons with Disabilities. New-York: United Nations (2006).
2. Beatty PW, Hagglund KJ, Neri MT, Dhont KR, Clark MJ, Hilton SA. Access to health care services among people with chronic or disabling conditions: patterns and predictors. Arch Phys Med Rehabil. (2003) 84:1417–25. doi: 10.1016/S0003-9993(03)00268-5
4. Benner JL, Hilberink SR, Veenis T, Stam HJ, Van Der Slot WM, Roebroeck ME. Long-term deterioration of perceived health and functioning in adults with cerebral palsy. Arch Phys Med Rehabil. (2017) 98:2196–2205.e1. doi: 10.1016/j.apmr.2017.03.013
5. Blair E, Watson L, Badawi N, Stanley FJ. Life expectancy among people with cerebral palsy in western Australia. Dev Med Child Neurol. (2001) 43:508. doi: 10.1017/S0012162201000949
6. Vitrikas K, Dalton H, Breish D. Cerebral palsy: an overview. Am Fam Physician. (2020) 101:213–20. 32053326.32053326
7. Opheim A, Jahnsen R, Olsson E, Stanghelle JK. Walking function, pain, and fatigue in adults with cerebral palsy: a 7-year follow-up study. Dev Med Child Neurol. (2009) 51:381–8. doi: 10.1111/j.1469-8749.2008.03250.x
8. Roquet M, Garlantezec R, Remy-Neris O, Sacaze E, Gallien P, Ropars J, et al. From childhood to adulthood: health care use in individuals with cerebral palsy. Dev Med Child Neurol. (2018) 60:1271–7. doi: 10.1111/dmcn.14003
9. Nieuwenhuijsen C, Van Der Laar Y, Donkervoort M, Nieuwstraten W, Roebroeck ME, Stam HJ. Unmet needs and health care utilization in young adults with cerebral palsy. Disabil Rehabil. (2008) 30:1254–62. doi: 10.1080/09638280701622929
10. Manikandan M, Casey C, Doyle A, Kerr C, Walsh M, Walsh A, et al. Use of health services and unmet needs among adults with cerebral palsy in Ireland. Dev Med Child Neurol. (2022) 64:1270–80. doi: 10.1111/dmcn.15233
11. Anaby D, Hand C, Bradley L, DiRezze B, Forhan M, DiGiacomo A, et al. The effect of the environment on participation of children and youth with disabilities: a scoping review. Disabil Rehabil. (2013) 35:1589–98. doi: 10.3109/09638288.2012.748840
12. Arnaud C, Duffaut C, Fauconnier J, Schmidt S, Himmelmann K, Marcelli M, et al. Determinants of participation and quality of life of young adults with cerebral palsy: longitudinal approach and comparison with the general population—SPARCLE 3 study protocol. BMC Neurol. (2021) 21:254. doi: 10.1186/s12883-021-02263-z
13. Surveillance of Cerebral Palsy in Europe (SCPE). Surveillance of cerebral palsy in Europe: a collaboration of cerebral palsy surveys and registers. Dev Med Child Neurol. (2000) 42:816–24. doi: 10.1111/j.1469-8749.2000.tb00695.x
14. Schmidt S, Thyen U, Herrmann-Garitz C, Bomba F, Muehlan H. The youth health care measure-satisfaction, utilization, and needs (YHC-SUN)-development of a self-report version of the child health care (CHC-SUN) proxy-measure. BMC Health Serv Res. (2016) 16:189. doi: 10.1186/s12913-016-1419-1
15. Perret C, Alvarelhão JJM, Pennington L, Ehlinger V, Duffaut C, Arnaud C, et al. Assessing the adequacy of the physical, social, and attitudinal environment to the specific needs of young adults with cerebral palsy: the European adult environment questionnaire. Arch Phys Med Rehabil. (2024) 11:S0003-9993(23)00693–7. doi: 10.1016/j.apmr.2023.11.012
16. McCormick A, Brien M, Plourde J, Wood E, Rosenbaum P, McLean J. Stability of the gross motor function classification system in adults with cerebral palsy. Dev Med Child Neurol. (2007) 49:265–9. doi: 10.1111/j.1469-8749.2007.00265.x
17. Hidecker MJC, Paneth N, Rosenbaum PL, Kent RD, Lillie J, Eulenberg JB, et al. Developing and validating the communication function classification system for individuals with cerebral palsy. Dev Med Child Neurol. (2011) 53:704–10. doi: 10.1111/j.1469-8749.2011.03996.x
18. Michelsen SI, Flachs EM, Damsgaard MT, Parkes J, Parkinson K, Rapp M, et al. European Study of frequency of participation of adolescents with and without cerebral palsy. Eur J Paediatr Neurol. (2014) 18:282–94. doi: 10.1016/j.ejpn.2013.12.003
19. Allin S, Grignon M, Le Grand J. Subjective unmet need and utilization of health care services in Canada: what are the equity implications? Soc Sci Med. (2010) 70:465–72. doi: 10.1016/j.socscimed.2009.10.027
20. Dickinson H, Parkinson K, McManus V, Arnaud C, Beckung E, Fauconnier J, et al. Assessment of data quality in a multi-centre cross-sectional study of participation and quality of life of children with cerebral palsy. BMC Public Health. (2006) 6:273. doi: 10.1186/1471-2458-6-273
21. Manikandan M, Walsh A, Kerr C, Walsh M, Ryan J M. Health service use among adults with cerebral palsy: a mixed methods systematic review protocol. BMJ Open. (2020) 10:e035892. doi: 10.1136/bmjopen-2019-035892
22. Nieuwenhuijsen C, Donkervoort M, Nieuwstraten W, Stam HJ, Roebroeck ME. Experienced problems of young adults with cerebral palsy: targets for rehabilitation care. Arch Phys Med Rehabil. (2009) 90:1891–7. doi: 10.1016/j.apmr.2009.06.014
23. Penneau A, Pichetti S, Sermet C. L’hébergement en institution favorise l’accès aux soins des personnes de moins de 60 ans en situation de handicap en France. Une exploitation de l’enquête Handicap-Santé Ménages et Institutions (2008–2009). Questions d’économie de la santé (IRDES) (2015) 1–8.
24. Solanke F, Colver A, McConachie H. On behalf of the transition collaborative group. Are the health needs of young people with cerebral palsy met during transition from child to adult health care? Child Care Health Dev. (2018) 44:355–63. doi: 10.1111/cch.12549
25. Elliott MN, Beckett MK, Chong K, Hambarsoomians K, Hays RD. How do proxy responses and proxy-assisted responses differ from what medicare beneficiaries might have reported about their health care? Health Serv Res. (2008) 43:833–48. doi: 10.1111/j.1475-6773.2007.00820.x
26. Kean J, Malec JF. Towards a better measure of brain injury outcome: new measures or a new metric? Arch Phys Med Rehabil. (2014) 95:1225–8. doi: 10.1016/j.apmr.2014.03.023
27. World physiotherapy. Germany, Annual Membership Census, 2022. London: World physiotherapy (2023). Available online at: Available at: https://world.physio/fr/sites/default/files/2023-01/AMC2022-Germany.pdf (accessed September 13, 2023).
28. Observatoire de la démographie du conseil national de l’ordre des masseurs-kinésithérapeutes. 2022 Démographie des Kinésithérapeutes. Paris: Conseil national de l’ordre des masseurs-kinésithérapeutes (2023). Available online at: Available at: https://www.ordremk.fr/wp-content/uploads/2023/01/rapportdemographiemk_2022-2.pdf (accessed September 13, 2023).
29. Ryan JM, Walsh M, Owens M, Byrne M, Kroll T, Hensey O, et al. Unmet health needs among young adults with cerebral palsy in Ireland: a cross-sectional study. JCM. (2022) 11:4847. doi: 10.3390/jcm11164847
Keywords: cerebral palsy, unmet healthcare needs, environmental needs, impairments, young adults
Citation: Rioual J, Perret C, Arnaud C and Vidart d’Egurbide Bagazgoïtia N (2024) Unmet environmental needs and unmet healthcare needs in a population of young adults with cerebral palsy: what the SPARCLE study tells us. Front. Rehabil. Sci. 5:1294999. doi: 10.3389/fresc.2024.1294999
Received: 15 September 2023; Accepted: 22 January 2024;
Published: 2 February 2024.
Edited by:
Nihad A. Almasri, The University of Jordan, JordanReviewed by:
Silvia Vincentiis, University of São Paulo, BrazilZhuoying Qiu, China Rehabilitation Research Center/WHO Collaborating Center for Family International Classifications, China
© 2024 Rioual, Perret, Arnaud and Vidart d'Egurbide Bagazgoïtia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nicolas Vidart d’Egurbide Bagazgoïtia bmljb2xhcy52aWRhcnRAaW5zZXJtLmZy
Abbreviations CI, confidence interval; CP, Cerebral palsy; EAEQ, European Adult Environment Questionnaire; EF, environmental factors; FCCS, Functional Communication Classification System; GMFCS, Gross Motor Function Classification System; ICF, International Classification of Functioning, Disability and Health; IQ, intelligence quotient; OR, odds ratio; SCPE, Surveillance of Cerebral Palsy in Europe network; SPARCLE, Study of PARticipation of children with Cerebral palsy Living in Europe; YHC-SUN, Youth Health Care, Satisfaction, Utilization and Needs; WHO, World Health Organization.