
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Rehabil. Sci., 05 May 2023
Sec. Disability, Rehabilitation, and Inclusion
Volume 4 - 2023 | https://doi.org/10.3389/fresc.2023.1069464
This article is part of the Research TopicUnderstanding Developmental Disability in Children, Youth, and Young Adults: Views on Physical and Mental Health and Functioning from Diagnosis to SupportView all 7 articles
 Amanda Amalfi1Jia Yin Li1Vanessa Théberge-Lamoureux1Carmen Tang1
Amanda Amalfi1Jia Yin Li1Vanessa Théberge-Lamoureux1Carmen Tang1 Emilie Rinaldi1Pranamika Khayargoli1
Emilie Rinaldi1Pranamika Khayargoli1 Dana Anaby1,2*†
Dana Anaby1,2*†
Aim: Decreased participation and complex transitions into adulthood among youth with disabilities may impede their well-being. To advance knowledge on the co-occurrence of mental health problems and physical disability, this brief report describes the frequency of mental health problems, measured by the Behavior Assessment System of Children (BASC-3), among transition-aged youth (14–25 years) with physical disabilities and examines the association between mental health problems and sex, age, and number of functional issues.
Methods: Thirty-three participants completed a demographic questionnaire and the BASC-3. Frequency of BASC-3 scales falling within 3 categories: “within norms”, “at risk”, and “clinically significant” were described. Crosstabs and Chi-square tests were used to examine the association between BASC-3 scales and sex, age (< and ≥ 20), and number of functional issues (< and ≥ 6).
Results: Overall, “somatization”, “self-esteem”, “depression” and “sense of inadequacy” were the most common subscales being at risk. Participants with a higher number of functional issues (≥6) were more likely to fall within “at risk” or “clinically significant” categories across 20 (out of 22) BASC-3 scales, and female participants tended to fall more within “at risk” or “clinically significant” categories for 8 of BASC-3 scales. Younger participants (<20) were ranked in the “at risk” or “clinically significant” categories for 7 scales.
Conclusions: Findings lend further support for the occurrence of mental health problems emerging in youth with physical disabilities and highlight initial trends especially across functional levels. Further investigation of such co-occurrences and the factors that affect their development is needed.
Children and youth with physical disabilities often experience lower levels of participation compared to their peers without physical disabilities (1–4). Decreased opportunities to participate in activities and build relationships among individuals with disabilities often result in social isolation, decreased quality of life and higher prevalence of mental health problems (5–7). Examples of barriers to their participation include stigma, negative attitude towards disability, lack of inclusivity, limited opportunities and resources addressing the specific needs of this population (8, 9).
Along with decreased participation, youth with physical disabilities also experience more complex transitions into adulthood that may adversely affect their quality of life and well-being. Adolescence and young adulthood are marked by pronounced psychological and physical changes (10). Mental health problems or initial subclinical symptoms are likely to appear during this sensitive period, causing psychosocial and participation pattern disruptions (11, 12). Moreover, the sudden termination of children's healthcare services, as well as lack of continuity and guidance into new services can add further complexity into the transitioning process of this population (13, 14). Furthermore, clinicians in the field of physical rehabilitation often tend to focus mainly on the youth's physical impairments, and their psychosocial functions, such as their mental health, typically may receive little attention (15). Emerging/early symptoms of mental health problems can deteriorate if left untreated during adolescence (16).
Evidence on the co-occurrence of physical disabilities and mental health problems is emerging. A meta-analysis of 8 studies among children and youth with cerebral palsy conducted by Downs et al. (15) suggests that mental health symptoms are common. Similarly, a recent scoping review by Lal et al. (17) indicated that most studies examining such co-occurrences pertained to youth and young adults with cerebral palsy, with fewer studies including other physical conditions such as juvenile arthritis and spina bifida. In addition, the most common age range across studies was 13–17 (17). Thus, examining co-occurrences in a broader age range that covers the transition-aged period, across various types of physical disabilities, is needed. Using psychometrically sound measures that can broadly assess aspects of mental health problems in terms of individual's behaviors and emotions, is warranted. An example of such measure is the Behavior Assessment System of Children-Third Edition (BASC-3). The BASC-3 is a multicomponent instrument intended for individuals aged 2–25, that allows for evaluation of numerous behaviors pertaining to a range of mental health components and includes clinical norms by age and sex (18).
To better understand the occurrence of mental health problems among transition-aged youth living with physical disabilities, this brief research report aimed to describe the frequency of mental health problems, as measured by the BASC-3, among youth aged 14–25 years with physical disabilities who experience different levels of mobility restriction in a large Canadian province where both English and French are common spoken languages. It also aimed to describe the frequency of mental health problems according to sex, age, and complexity of youth's condition in terms of number functional issues among this population.
This brief research report presents baseline results (in terms of the presence of mental health problems) of a clinical trial that examined the effect of an intervention aimed to improve participation in leisure community-based activities on outcomes at the body function level using the specific subscales of the BASC-3 among other motor-related outcomes. As such, the present study is cross-sectional in nature. A total of 33 youth aged 14 to 25 years old (mean age: 20.24) were included from both sexes who spoke either English or French. Youth with a physical disability, presenting with restricted mobility (requiring adaptive equipment, physical aid, or external support/supervision), as well as multiple diagnostic categories were included. Participants were excluded if they were in their first year of recovery from severe brain injury or orthopedic surgery or if they were recovering from botulinum toxin treatment 6 months prior to the study or anticipated during the study. Youth with neurodegenerative disorders and/or significant intellectual delays were also excluded, as the latter had the potential to impact self-completion of any necessary forms and assessments.
Convenience sampling was used to recruit youth from three large rehabilitation centers/hospitals in the Greater Montreal area. Consent forms were obtained online via Research Electronic Data Capture (RedCap) from all participants followed by the completion of a demographic questionnaire. The full BASC-3 was then completed online by the youth through the Q global platform (18) and generated encrypted summary reports were stored in a secured platform. Ethics approval was obtained by the Centre for Interdisciplinary Research in Rehabilitation of Greater Montreal (CRIR).
Behavior Assessment System for Children- Third Edition (BASC-3). The BASC-3 was used to measure behaviors and emotions that pertain to aspects of mental health. It is a multicomponent instrument that takes self-reported measures to analyze behavioral and emotional aspects of children and youth (2–25 years old) (18). Two different self-reported forms of the BASC-3 were used in this study: the adolescent form (for ages 12–21 years) and the college form (for ages 18–25 years), that provide comparable results. This measure contains 175 different items pertaining to certain behaviors or emotions, that are categorized into 16 clinical and adaptive subscales (e.g., anxiety, social stress) from which content and composite scales are generated (see Table 1 for details). Each BASC-3 assessment takes 20–30 min to complete. Youth are asked to rate if and how often they experience items on either a True/False scale, or a 4-point Likert scale with options: “Never”, “Sometimes”, “Often” and “Almost always”. Examples of items include “I feel sad”, “I worry a lot of the time” or “I am left out of things”, among others. The Q-global platform is used for immediate scoring and reporting of the completed adolescent and college self-reported forms (18). Responses from each item generate a score, which are summed to obtain a raw score per subscale. T scores and percentiles are generated for each subscale using the raw scores. The T-score is then placed within one of three categories: “within norms” (T-scores < 59), “at risk” (T-scores ranging from 60 to 69 for clinical scales and 31–40 for adaptive scales) or “clinically significant” (T-scores ≥70 for clinical scales and ≤30 for adaptive scales). The BASC-3 is a valid and reliable tool; evidence of internal consistency ranges from 0.71–0.97 for ages 12–25 years. Test-retest reliability ranges from 0.72–0.90 across scales (18). Evidence of correlations between the BASC-3 with various measures of behavior has also been examined, where for example, moderate or high correlations between self-reported clinical scale scores of the BASC-3 and similar Achenbach System of Empirically Based Assessment Youth Self-Report Form syndrome scale scores were seen, supporting its construct validity. Factor analysis was also confirmed by grouping of scales into composites, supporting the domains of the BASC-3 and, hence, its structural validity. The BASC–3 also offers a number of scales that help detect threat to validity (18).
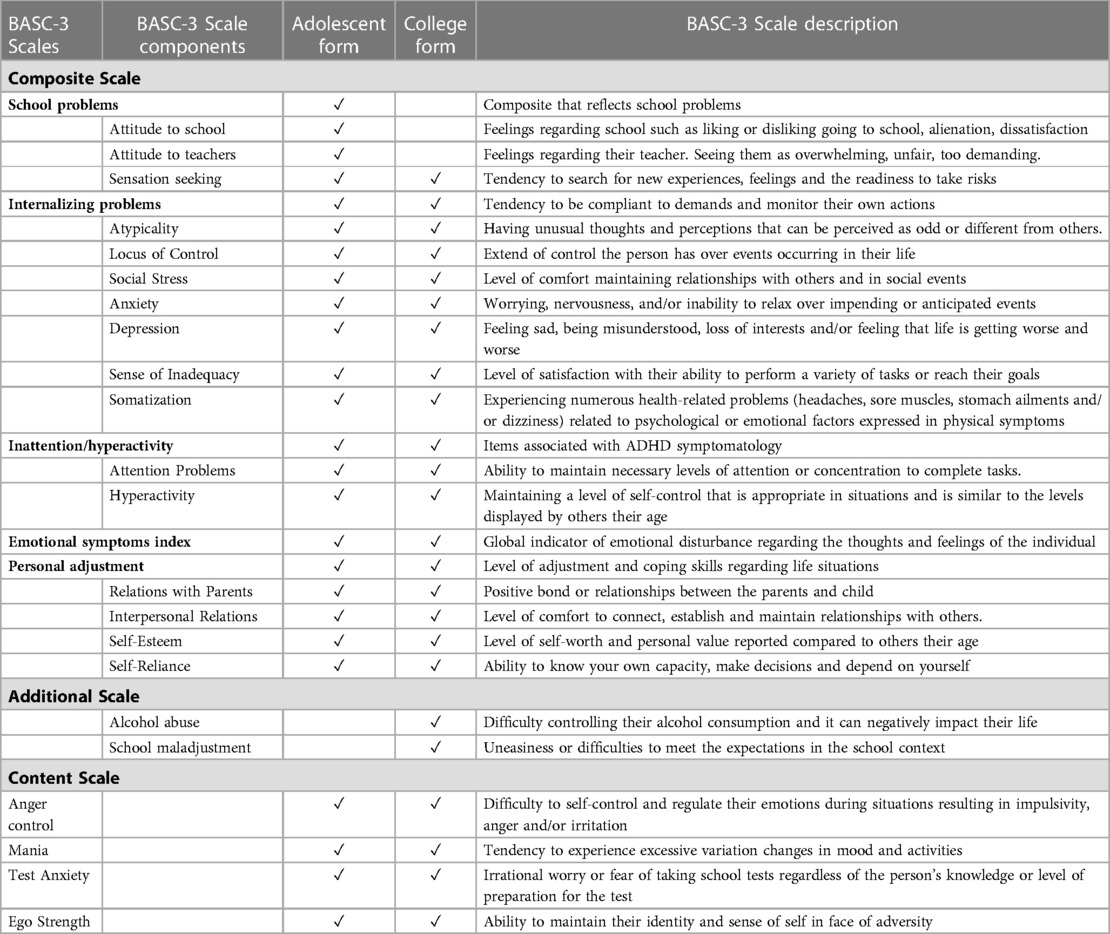
Table 1. Types of self-reported BASC-3 scales.
Demographic questionnaire. The demographic questionnaire contained 14 different questions created by the research team. Listed questions were related to sex, age, type of community, spoken languages, living situation, education, engaged activities, functional issues, health conditions, rehabilitation services received (e.g., occupational therapy, physical therapy, and speech language pathology) and mental health services received (e.g., counseling). More specifically, the current study looked at age, sex, and functional issues within the questionnaire. Age was noted in years and sex was categorized as male or female. To capture the complexity of participants' condition, as used in a study by Anaby et al. (19) to predict participation outcomes, a list of 11 functional issues were presented to the participants, in which they reported if they had either “No problem”, “Little problem” or “Big problem”. Participants were considered to have one functional issue if they checked off either “Little problem” or “Big problem”. The number of functional issues ranged from 0 to 11. Functional issues looked at motor, cognitive, learning, and sensory components. Examples of functional issues included “moving around”, “using your hands to do activities”, “managing emotions”, “learning new information”, etc.
Descriptive statistics were used to report the frequency (presented in percentages) of observed mental health problems falling in categories “within norms”, “at risk”, and “clinically significant” for the entire sample. A bar chart was created to illustrate the percentage of participants who ranked “at risk” and “clinically significant” for each BASC-3 scale. A fourth category named “at risk and above” was created by combining “at risk” and “clinically significant” categories. To examine the association between the presence of mental health problems and variables of sex, age and number of functional issues, crosstabs and Chi-Square or Fisher Exact tests were performed. To do so, the data was divided into 2 subgroups for variables of sex (female, male), number of functional issues (<6 and ≥6) and age (<20 and ≥20) based on the median. Chi-Square tests were performed to generate 2 × 2 crosstabulation tables to explore the relationship between 2 BASC categories (“within norms” and “at risk and above”) of each BASC-3 subscale and the 2 categories of each of the 3 variables (sex, number of functional issues, age). The significance of association between subscales and the 3 variables were determined using the p-value of Pearson Chi-Square, but when Chi-Square's assumption of cell counts with less that 5 or less than 20% was violated, the p-value of Fisher's Exact Test was used (20, 21). Trends between subgroups of each variable were identified using the expected and observed count of each subscale category, allowing us to examine the likelihood of specific subgroups to fall within the two BASC categories. When analyzing the association between the BASC-3 subscales and the three variables, the following subscales were excluded because they were not present in both adolescent and college forms: alcohol abuse, school maladjustment, attitude to school, attitude to teachers and school problems. All analysis was done using SPSS version 28. Results were deemed statistically significant at p < 0.05.
Thirty-three youth aged 14–25 years (mean 20.24; SD = ±3.05; median = 20) participated in the study. Nineteen youth reported types of services received; 5 (26.4%) of which reported not receiving neither physiotherapy, occupational therapy, counseling, nor speech-language pathology and 14 (73.6%) participants responded to receiving at least one of these services. The number of services received ranged from 0 to 4 (median and mode were 1), with occupational therapy being the most common service received. Eight reported receiving counseling. The majority (90%) lived with at least one of their family members and the remaining (10%) lived alone or with their significant other. Youth reported up to 11 functional issues (mean = 5.3; median = 6). The two most frequently reported functional issues were moving around (69.7%) and managing emotions (68.8%). Youth reported 1–6 health conditions (mean = 2.06; median = 1.0). The two most frequent health conditions were orthopedic/movement difficulties (69.7%) and health impairments (24.2%) as detailed in Table 2.
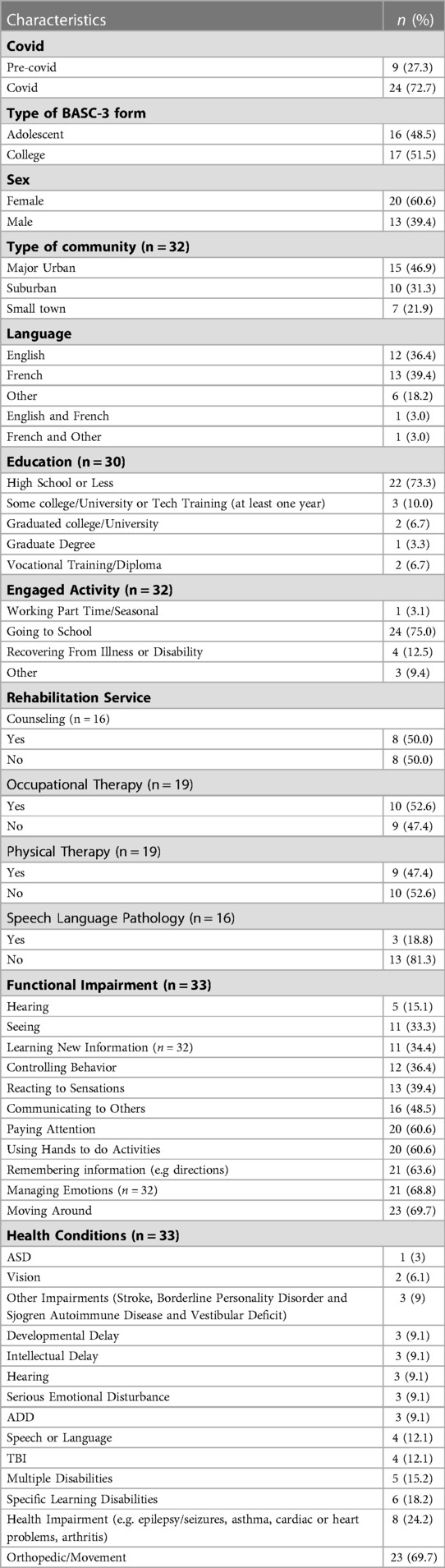
Table 2. Demographic characteristics of participants (n = 33).
Frequency of occurrences of self-reported mental health problems across BASC-3 categories (n = 33):
As shown in Figure 1, all BASC-3 scales had at least one participant who fell in the “at risk” category, indicating that all BASC-3 scales representing a range of mental health problems were relevant for youth with disabilities in our studied sample.
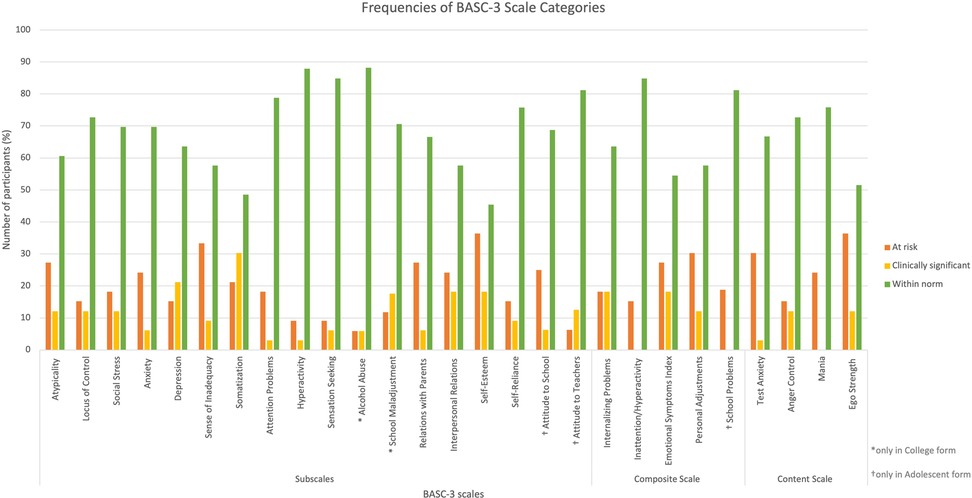
Figure 1. Frequencies of At risk and clinically significant scores for each BASC-3 scale.
For the BASC-3 subscales, the most frequent subscales falling “within norms” were hyperactivity (87.9%) closely followed by sensation seeking (84.8%), while the least common ones were somatization (48.5%) and sense of inadequacy (57.6%). With respect to the composite scales, inattention/hyperactivity (84.8%) followed by internalizing problems (63.6%) ranked most frequently “within norms” while the least common ones were emotional symptoms index (54.5%) and personal adjustments (57.6%). With respect to content scales, mania (75.8%) ranked most frequently “within norms” followed by anger control (72.7%) while ego strength (51.5%) and test anxiety (66.7%) were the least common ones.
For the BASC-3 subscales, as shown in Figure 1, the most frequent subscales for which participants ranked “at risk” were self-esteem (36.4%) closely followed by sense of inadequacy (33.3%) while the least common ones were hyperactivity (9.1%) and sensation seeking (9.1%). With respect to the composite scales, personal adjustments (30.3%) ranked most frequently “at risk” closely followed by emotional symptoms index (27.3%) while the least common ones were inattention/hyperactivity (15.2%) and internalizing problems (18.2%). With respect to content scales, ego strength (36.4%) ranked most frequently “at risk” followed by test anxiety (30.3%) while anger control (15.2%) and mania (24.2%) were the least common ones.
The most frequent “clinically significant” BASC-3 subscales were somatization (30.3%) followed by depression (21.2%) whereas the least common ones were attention problems (3.0%) and hyperactivity (3.0%). With respect to the composite scales, internalizing problems (18.2%) and emotional symptoms index (18.2%) ranked most frequently “clinically significant” while the least common one was personal adjustments (12.1%). None of the scores pertaining to inattention/hyperactivity fell within the “clinically significant” category. As for the content scales, anger control and ego strength (12.1%) ranked most frequently “clinically significant” while test anxiety (3.0%) was the least common one. None of the scores pertaining to mania fell within the “clinically significant” category.
In total, participants ranked most frequently “at risk and above” for self-esteem (54.5%) closely followed by somatization (51.5%) while least frequently for hyperactivity (12.1%) and sensation seeking (15.2%). With regards to the composite scales, emotional symptoms index (45.5%) closely followed by personal adjustments (42.4%) ranked most frequently “at risk and above” while the least common ones were inattention/hyperactivity (15.2%) and internalizing problems (36.4%). With respect to content scales, ego strength (48.5%) and test anxiety (33.3%) ranked most frequently “at risk and above” while the least common ones were mania (24.2%) and anger control (27.3%).
Among female participants, atypicality, sense of inadequacy, self-esteem, test anxiety, and ego strength were most frequently ranked “at risk” (45%), while somatization was most frequently ranked “clinically significant” (45%) and “at risk and above” (70%). Within the male participants, emotional symptoms index was the most frequent scale ranked “at risk” (30.8%), while self-esteem was the most frequent subscale ranked “clinically significant” (23.1%) and “at risk and above” (46.2%).
Overall, nine scales indicated a trend with sex, among which three were statistically significant (see Table 3). Female compared to male participants fell in “at risk and above” in eight scales: atypicality, social stress, anxiety, depression, somatization, relationship with parents, internalizing problems, and text anxiety. Among them, a statistically significant trend was observed for three scales including atypicality, somatization and text anxiety. In contrast, males fell in “at risk and above” for sensation seeking scale, yet this association was not statistically significant.

Table 3. Associations between BASC-3 scales and sex, number of functional issues and age.
Among the sub-group of participants with higher number of functional issues (≥6), atypicality, self-esteem, test anxiety and ego strength were most frequently ranked “at risk” (41.2%), while somatization was most frequently ranked “clinically significant” (47.1%) and “at risk and above” (70.6%). Amongst participants with lower number of functional issues (<6), sense of inadequacy, self-esteem, emotional symptoms index, personal adjustments, and ego strength were most frequently ranked “at risk” (31.3%), while self-esteem was most frequently ranked “clinically significant” (18.8%) and “at risk and above” (50.1%).
In general, the crosstab analysis revealed that descriptively those with greater number of functional issues fell within the “at risk and above” category for most of the BASC-3 scales (20/22). The association between number of functional issues and presence of mental health problems (ranked “at risk and above”) was statistically significant in six scales. Specifically, youth with higher number of functional issues tended to experience depression, somatization, inattention/hyperactivity, problems with interpersonal relations, and to internalize problems, whereas those with lower number of functional issues were significantly more likely to seek sensations.
For younger participants, aged below 20 years, anxiety, personal adjustments, mania, and ego strength were most frequently ranked “at risk” (42.9%), while depression, somatization, self-esteem, and anger control were most frequently ranked “clinically significant” (21.4%), and somatization and self-esteem “at risk and above” (57.1%). Within participants aged 20 and above, self-esteem was most frequently ranked “at risk” (36.8%), while somatization was most frequently ranked “clinically significant” (36.8%) and self-esteem “at risk and above” (52.6%).
Overall, a descriptive trend between the presence of mental health problems and age groups was observed in seven BASC-3 scales, where younger participants (aged below 20 years) were more likely to fall within the “at risk and above” category than the older group (aged 20 years and above). The BASC-3 subscales that showed significant association with age were hyperactivity and mania, revealing that younger participants were significantly more likely to fall within the “at risk and above” category than the older group (see Table 3). A similar trend (yet non-significant) was observed for anxiety, social stress, sensation seeking, inattention/hyperactivity, and test anxiety.
This brief research report provides additional evidence for the occurrences of emerging mental health problems, measured by a comprehensive self-reported assessment (BASC-3), among transition-aged youth with physical disabilities. It also describes these co-occurrences across sex, age, and functional issues. Overall, when looking at the entire sample, “somatization”, “self-esteem”, “depression” and “sense of inadequacy” were the most common areas where youth reported difficulties, falling within the “at risk” or “clinical significant” categories. Similarly, Gorter et al. (22) found that depressive and anxious symptoms were commonly present in adolescents and young adults with cerebral palsy. Another study described a higher risk of depression for adults living with cerebral palsy compared to adults without cerebral palsy (23). Our findings indicated that “somatization”, referring to physical health symptoms related to emotional state, was the most frequent subscale. This is worth reflecting on. It is unclear whether the frequency of somatization was found due to youth's actual emotional state or was observed rather due to the physical discomfort emerging from the complex nature of the youth's physical condition. Thus, further investigation of the origin of somatization is needed. This is of particular importance as previous research indicated that mental health symptoms were associated with fatigue and pain among youth with cerebral palsy (22).
Several associations (or trends) were observed between mental health issues and personal factors with a more pronounced association with complexity of the youth's condition. Specifically, youth with higher number of functional issues were more likely to fall within the “at risk and above” category for most of the BASC-3 scales, except for hyperactivity and sensation seeking. Although these associations were not statistically significant across all scales, it is important to reflect on the identified trends as prior research has shown similar findings. For example, Lindén-Boström & Persson (24) found that youth (13–18 years old) with multiple impairments had a higher probability of developing poorer mental health. This may be explained by the overall lower levels of participation evident in this population (25) as lower rates of participation have been associated with a greater occurrence of mental health problems among youth (26). To decrease the prevalence of mental health issues amongst youth with disabilities, Granlund et al. (27) suggested that interventions should be focused on increasing participation levels, to increase overall well-being and indirectly improve mental health. A study by Anaby et al. (28) demonstrated that after a small group of youth (15–25 years old) participated in a meaningful activity for 8 weeks, at least one component of the affective body function (e.g., anxiety, sense of inadequacy) measured by the BASC-3, showed significant improvement. Thus, to mitigate the occurrence of mental health problems in youth with physical disabilities, further research should conduct larger scale participation-focused interventions for youth with physical disabilities.
Some initial trends were observed across the sexes where nine scales of the BASC-3 showed a trend or an association with sex. Specifically, female adolescents, in comparison to male participants, were significantly more likely to fall with the “at risk and above” category on eight scales including self-esteem, test anxiety, atypicality and somatization. Our findings are similar to what has been establish in literature, showing sex differences for mental health in general (24). Females are more likely to be affected by depression, psychological distress, and anxiety than males depending on the context (29, 30). Furthermore, socio-cultural, psychological, and biological factors can be important but not inclusive factors to explain these disparities (31, 32). Gender-related beliefs and participation in different activities or social roles can also have an incidence on the results (29).
Age also appeared to be an important factor in some of the BASC domains. Results demonstrated that participants in the younger age group ranked more “at risk and above” compared to participants in the older age group across 7 (out of 22) subscales. Similarly, a study by Brossard-Racine et al. (33) found that younger adolescents with cerebral palsy scored higher in most subscales of the Strengths and Difficulties Questionnaire, a screening questionnaire that measures behavioral and emotional problems in children and adolescents, compared to their older peers, which suggests that these problems appeared during earlier childhood (34). These findings, in combination with the findings of the present study, may indicate the value of early intervention in younger adolescents to address existing mental health issues as well as the prevention of the latter to further develop into mental illness. Intervention and prevention of mental health issues can be done through the increase of their participation, as decreased activity participation can lead to higher prevalence of mental health problems in youth with physical disabilities (6, 7, 27). In addition, self-esteem was the most frequent subscale observed to be “at risk” for both the older and younger age groups. This suggests that self-esteem of youth with physical disabilities is affected throughout their adolescence and early adulthood, regardless of the age, which may be due to pre-conceived notions of others towards their disability, as research showed that perceived disability stigma is correlated with self-esteem in adolescents with physical disabilities (35).
Our results, based on the BASC-3 clinical norms, suggest that youth with physical disabilities are at a greater risk of mental health problems, evident in 12% to 54% of our sample (those falling under categories of “at risk” or “clinically significant”) and comparable to emerging findings (15, 17). The findings also shed light on the applicability and uniqueness of the BASC-3 as a comprehensive self-rated measure to assess aspects related to mental health issues in this population. Specifically, it was observed that all scales from the BASC-3 had at least one participant that fell above at risk. This suggests the relevancy of each scale that represents the various mental health problems experienced by our sample group depicted by the BASC-3 and, thus, may be considered for use in future studies.
Generalizability of the findings towards the larger population of youth with physical disabilities may be impacted by sampling strategy (convenience sampling) as well as inclusion and exclusion criteria, where individuals presenting with an intellectual delay, or a neurodegenerative disorder were excluded. When looking at data analysis, given that sampling distribution has an approximate chi-square distribution, a small sample size can impact accuracy of the approximation (36). Furthermore, 72.7% of the sample data was collected during the COVID-19 pandemic, which may affect findings. Further larger studies considering both adolescents and college-aged young adults are also needed, especially those combining a qualitative element. This may allow for greater insights on co-occurrences between mental health problems and physical disability. Lastly, further studies should include other factors that may explain mental health problems such as participation and social support, factors known to affect youth's well-being (5).
The datasets presented in this article are not readily available because; The dataset must remain strictly confidential and not be shared in order to respect participants’ preferences. This is particularly important as the dataset includes sensitive information on youth's mental health and involves a relatively small sample size that may be identified. Requests to access the datasets should be directed toZGFuYS5hbmFieUBtY2dpbGwuY2E=.
The studies involving human participants were reviewed and approved by The Research Ethics Board (REB) of the Centre for Interdisciplinary Research in Rehabilitation of Greater Montreal (CRIR). Written informed consent to participate in this study was provided by the participants.
DA conceived and designed the study and supervised its implementation. AA, JIL, VTL, CT, and ER analyzed the data and interpreted the findings. All authors drafted the manuscript. DA and PK validated the data analysis and led the revisions of the manuscript. All authors contributed to the article and approved the submitted version.
This work by supported by funding provided by the Canadian Institutes of Health Research (CIHR).
We would like to thank the youth who participated in the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Tonkin BL, Ogilvie BD, Greenwood SA, Law MC, Anaby DR. The participation of children and youth with disabilities in activities outside of school: a scoping review: étude de délimitation de l’étendue de la participation des enfants et des jeunes handicapés à des activités en dehors du contexte scolaire. Can J Occup Ther. (2014) 81(4):226–36. doi: 10.1177/0008417414550998
2. Bedell G, Coster W, Law M, Liljenquist K, Kao Y-C, Teplicky R, et al. Community participation, supports, and barriers of school-age children with and without disabilities. Arch Phys Med Rehabil. (2013) 94(2):315–23. doi: 10.1016/j.apmr.2012.09.024
3. Engel-Yeger B, Jarus T, Anaby D, Law M. Differences in patterns of participation between youths with cerebral palsy and typically developing peers. Am J Occup Ther. (2009) 63(1):96–104. doi: 10.5014/ajot.63.1.96
4. Augustine L, Lygnegård F, Granlund M. Trajectories of participation, mental health, and mental health problems in adolescents with self-reported neurodevelopmental disorders. Disabil Rehabil. (2022) 44(9):1595–608. doi: 10.1080/09638288.2021.1955304
5. Longo E, Badia M, Begoña Orgaz M, Gómez-Vela M. Comparing parent and child reports of health-related quality of life and their relationship with leisure participation in children and adolescents with cerebral palsy. Res Dev Disabil. (2017) 71:214–22. doi: 10.1016/j.ridd.2017.09.020
6. Williams TL, Smith B, Papathomas A. The barriers, benefits and facilitators of leisure time physical activity among people with spinal cord injury: a meta-synthesis of qualitative findings. Health Psychol Rev. (2014) 8(4):404–25. doi: 10.1080/17437199.2014.898406
7. Reedman SE, Sakzewski L, Boyd RN. A systematic review and meta-analysis of the efficacy of therapy and behaviour change interventions to increase physical activity participation in children with cerebral palsy. Dev Med Child Neurol. (2016) 58(Supplement 6):28. doi: 10.1111/dmcn.13315
8. Shields N, Synnot A. Perceived barriers and facilitators to participation in physical activity for children with disability: a qualitative study. BMC Pediatr. (2016) 16(1):1–10. doi: 10.1186/s12887-016-0544-7
9. Anaby D, Hand C, Bradley L, DiRezze B, Forhan M, DiGiacomo A, et al. The effect of the environment on participation of children and youth with disabilities: a scoping review. Disabil Rehabil. (2013) 35(19):1589–98. doi: 10.3109/09638288.2012.748840
10. Arango C, Díaz-Caneja CM, McGorry PD, Rapoport J, Sommer IE, Vorstman JA, et al. Preventive strategies for mental health. The Lancet Psychiatry. (2018) 5(7):591–604. doi: 10.1016/S2215-0366(18)30057-9
11. Stewart DA, Law MC, Rosenbaum P, Willms DG. A qualitative study of the transition to adulthood for youth with physical disabilities. Phys Occup Ther Pediatr. (2002) 21(4):3–21. doi: 10.1080/J006v21n04_02
12. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry. (2005) 62(6):593–602. doi: 10.1001/archpsyc.62.6.593
13. King GA, Baldwin PJ, Currie M, Evans J. Planning successful transitions from school to adult roles for youth with disabilities. Children's Health Care. (2005) 34(3):193–216. doi: 10.1207/s15326888chc3403_3
14. Pandey S, Agarwal S. Transition to adulthood for youth with disability: issues for the disabled child and family. IOSR J Humanit and Soc Sci (IOSR-JHSS). (2013) 17(3):41–5. doi: 10.9790/0837-1734145
15. Downs J, Blackmore AM, Epstein A, Skoss R, Langdon K, Jacoby P, et al. The prevalence of mental health disorders and symptoms in children and adolescents with cerebral palsy: a systematic review and meta-analysis. Dev Med Child Neurol. (2018) 60(1):30–8. doi: 10.1111/dmcn.13555
16. Majnemer A. Measures for children with developmental disabilities: An ICF-CY approach. London: Mac Keith Press (2012).
17. Lal S, Tremblay S, Starcevic D, Mauger-Lavigne M, Anaby D. Mental health problems among adolescents and young adults with childhood-onset physical disabilities: a scoping review. Front Rehabil Sci. (2022) 3:1–17. doi: 10.3389/fresc.2022.904586.
18. Reynolds CR, Kamphaus R.W. Behavior assessment system for children (3rd ed.) [Assessment instrument]. Bloomington, MN: Pearson. (2015).
19. Anaby D, Law M, Coster W, Bedell G, Khetani M, Avery L, et al. The mediating role of the environment in explaining participation of children and youth with and without disabilities across home, school, and community. Arch Phys Med Rehabil. (2014) 95(5):908–17. doi: 10.1016/j.apmr.2014.01.005
20. Kim H-Y. Statistical notes for clinical researchers: chi-squared test and Fisher's Exact test. rde. (2017) 42(2):152–5. doi: 10.5395/rde.2017.42.2.152
21. Nowacki A. Chi-square and Fisher's Exact tests. Clevel Clin J Med. (2017) 84(9 suppl 2):e20–e5. doi: 10.3949/ccjm.84.s2.04
22. Gorter JW, Fehlings D, Ferro MA, Gonzalez A, Green AD, Hopmans SN, et al. Correlates of mental health in adolescents and young adults with cerebral palsy: a cross-sectional analysis of the MyStory project. J Clin Med. (2022) 11(11):3060. doi: 10.3390/jcm11113060
23. Smith KJ, Peterson MD, O’Connell NE, Victor C, Liverani S, Anokye N, et al. Risk of depression and anxiety in adults with cerebral palsy. JAMA Neurol. (2019) 76(3):294–300. doi: 10.1001/jamaneurol.2018.4147
24. Lindén-Boström M, Persson C. Disparities in mental health among adolescents with and without impairments. Scand J Public Health. (2015) 43(7):728–35. doi: 10.1177/1403494815589219
25. King G, Law M, Hurley P, Petrenchik T, Schwellnus H. A developmental comparison of the out-of-school recreation and leisure activity participation of boys and girls with and without physical disabilities. International journal of disability. Dev and Educ. (2010) 57(1):77–107. doi: 10.1080/10349120903537988
26. Carlberg L, Granlund M. Achievement and participation in schools for young adolescents with self-reported neuropsychiatric disabilities: a cross-sectional study from the southern part of Sweden. Scand J Public Health. (2019) 47(2):199–206. doi: 10.1177/1403494818788415
27. Granlund M, Imms C, King G, Andersson AK, Augustine L, Brooks R, et al. Definitions and operationalization of mental health problems, wellbeing and participation constructs in children with NDD: distinctions and clarifications. Int J Environ Res Public Health. (2021) 18(4):1656. doi: 10.3390/ijerph18041656
28. Anaby D, Avery L, Gorter JW, Levin MF, Teplicky R, Turner L, et al. Improving body functions through participation in community activities among young people with physical disabilities. Dev Med Child Neurol. (2020) 62(5):640–6. doi: 10.1111/dmcn.14382
29. Salk RH, Hyde JS, Abramson LY. Gender differences in depression in representative national samples: meta-analyses of diagnoses and symptoms. Psychol Bull. (2017) 143(8):783–822. doi: 10.1037/bul0000102
30. Astbury J. Gender disparities in mental health. In: Mental health. Ministerial Round Tables 2001, 54th World Health Assemble, 2001. Geneva, Switzerland: WHO (2001). p. 73–92.
31. Johansen R, Espetvedt MN, Lyshol H, Clench-Aas J, Myklestad I. Mental distress among young adults—gender differences in the role of social support. BMC Public Health. (2021) 21(1):2152. doi: 10.1186/s12889-021-12109-5
32. Otten D, Tibubos AN, Schomerus G, Brähler E, Binder H, Kruse J, et al. Similarities and differences of mental health in women and men: a systematic review of findings in three large German cohorts. Front Public Health. (2021) 9:553071. doi: 10.3389/fpubh.2021.553071
33. Brossard-Racine M, Waknin J, Shikako-Thomas K, Shevell M, Poulin C, Lach L, et al. Behavioral difficulties in adolescents with cerebral palsy. J Child Neurol. (2013) 28(1):27–33. doi: 10.1177/0883073812461942
34. Whitney DG, Warschausky SA, Peterson MD. Mental health disorders and physical risk factors in children with cerebral palsy: a cross-sectional study. Dev Med Child Neurol. (2019) 61(5):579–85. doi: 10.1111/dmcn.14083
Keywords: adolescence, mobility restriction, transition into adulthood, behavioral emotional problems, young adults
Citation: Amalfi A, Li JY, Théberge-Lamoureux V, Tang C, Rinaldi E, Khayargoli P and Anaby D (2023) Mental health problems among transition-aged youth with physical disabilities: an initial evaluation. Front. Rehabil. Sci. 4:1069464. doi: 10.3389/fresc.2023.1069464
Received: 13 October 2022; Accepted: 14 April 2023;
Published: 5 May 2023.
Edited by:
Pamela Bryden, Wilfrid Laurier University, CanadaReviewed by:
Jacqueline Moodley, University of Johannesburg, South Africa© 2023 Amalfi, Li, Théberge-Lamoureux, Tang, Rinaldi, Khayargoli and Anaby. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dana Anaby ZGFuYS5hbmFieUBtY2dpbGwuY2E=
†This author shares senior authorship.
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.