 Amanda Wilkinson
Amanda Wilkinson Chris Higgs
Chris Higgs Tim Stokes
Tim Stokes Jack Dummer3
Jack Dummer3 Leigh Hale
Leigh Hale
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Rehabil. Sci. , 21 June 2022
Sec. Disability, Rehabilitation, and Inclusion
Volume 3 - 2022 | https://doi.org/10.3389/fresc.2022.904007
This article is part of the Research Topic Challenging the concept of Self-management support in unique and diverse populations View all 5 articles
People living rurally frequently experience health disparities especially if living with a long-term condition (LTC) or multi-morbidity. Self-management support is a key component of LTC management and commonly included in rehabilitation programmes to enhance ability to self-manage health and encourage physical activity. Such programmes are however often condition focussed and despite evidence for their effectiveness, are not always feasible to deliver in rural settings. Generic programmes are arguably more optimal in the rural context and delivery can be face to face or remotely (via telehealth). The aim of this explorative integrative review was to collate and present international evidence for development, delivery, integration, and support of community-based, generic LTC group rehabilitation programmes delivered rurally in person, or remotely using telehealth. Electronic databases were systematically searched using MeSH terms and keywords. For inclusion, articles were screened for relevance to the aim, and practical information pertaining to the aim were extracted, charted, and organized deductively into themes of Development, Delivery, Integration, and Support. Within each theme, data were synthesized inductively into categories (Theory, Context, Interpersonal aspects, and Technology and Programme aspects). Fifty-five studies were included. Five studies contributed information about community based programmes delivered via the internet. Development was the only theme populated by information from all categories. The theme of Support was only populated with information from one category. Our review has drawn together a large body of diverse work. It has focused on finding practical information pertaining to the best ways to develop, deliver, integrate, and support a community-based generic rehabilitation programme for people living with long-term health conditions, delivered rurally and/or potentially via the internet. Practical suggestions were thematically organized into categories of theory, context, interpersonal aspects, and technology and programme aspects. While the findings of this review might appear simple and self-evident, they are perhaps difficult to enact in practice.
Long-term health conditions (LTCs) are any ongoing, long term or recurring health conditions (>6 months) (1). LTCs impact significantly on a person, their family and their wider community (2). Self-management support is a key component in the health care of people living with LTCs. Rehabilitation programmes are important in the management of LTCs and usually comprise of components of exercise and education, with a focus on self-management support so that the person can learn to live and manage their condition (3). A systematic review identified the key features of LTC rehabilitation programmes as being of 4–8 weeks in length, and include education on symptom management, exercise, time to develop and embed self-management skills and self-efficacy, and led by health professional/s together with lay or peer leaders (4). In previous work, we identified that the viability and sustainability of rehabilitation programmes may be contingent on a “closer to home” generic approach catering for people with more than one long-term condition (5). Further, building relationships, not just between the healthcare providers and people attending with LTCs, but between both these groups and the wider community are vital to enable and maintain participation (5, 6). These factors may become even more crucial when working in rural or remote communities to enable health equity and promote supported self-management in a wider context.
Health care for people living with LTCs, particularly in secondary care, has largely been driven by models relating to one condition (7), whereas the increase in prevalence of multi-morbidity demands more complex models of care (8–10). In terms of rehabilitation programmes, LTCs are mostly dealt with as single conditions, for example a current large undertaking by the World Health Organization and Cochrane Rehabilitation is developing a “WHO Package of Rehabilitation Interventions” (11). This project is developing rehabilitation guidelines for 20 separate health conditions as opposed to grouping conditions together by functional outcomes (12). For many LTCs, one of the mainstays of management is exercise or physical activity. Whilst specific conditions have specific exercise guidelines [for example, cardiac rehabilitation, (13) pulmonary rehabilitation (14)], in reality, the optimal exercise regimen (i.e., exercise type, intensity, duration, and frequency) is remarkably similar across LTCs (3). The benefits of condition-specific rehabilitation include high evidence in improving exercise capacity, symptoms, health related quality of life, and reducing hospitalization (15, 16). The challenges to condition specific rehabilitation include having available healthcare professional specialists to run it, sufficient class attendees, and the nonsensical approach of people living with multiple morbidity attending specific rehabilitation programmes for each condition they are diagnosed with. Many LTC rehabilitation classes are delivered from a secondary care (hospital) setting, and thus become, and are perceived to be, “medicalised” in nature (16, 17). Conducting generic, as opposed to single condition, LTC rehabilitation programmes is an emerging concept.
Despite robust evidence for benefit of LTC rehabilitation (15), in many countries in the world attendance at rehabilitation programmes is hindered by many factors, and particularly in urban or remote areas (18–21). Inequities in healthcare provision are compounded by distance from health services, reduced access to primary and specialist care clinicians, and reduced socio-economic status and low health literacy (21–23). In New Zealand, rural towns have the lowest socioeconomic status, highest proportion of Māori, and the highest avoidable and amenable mortality rates. Telehealth (delivery of healthcare when patients and healthcare professionals are in separate locations) (24) may be a possibility for delivering healthcare. Delivering generic community-based rehabilitation programmes in rural areas in person or by using telehealth may provide more equitable access to services beneficial to improving the health and wellbeing of those living with long-term conditions, and to a population in need of such a service (25). However challenges remain to using both approaches and in particular telehealth (such as equitable access to the internet, cost of technology, security breaches, technological and software limitations, changes in patient expectations and engagement, difficulty in maintaining therapeutic relationship and reading non-verbal cues) (26, 27).
Nevertheless, informal consultation suggests that the potential benefits of offering a generic programme in person or by using telehealth include (i) healthcare delivered closer to home to remove some of the barriers for consumers through using community facilities (church and community halls, local gyms) set up for in person or telehealth delivery of a proactive programme enabling people to take control of their own health and make healthy choices; and (ii) potential reduced requirements for acute care by keeping people fitter and independently living at home. Whilst Mulligan, Wilkinson (4) identified the components of a generic community rehabilitation programme for people with LTCs, these were not specific to a rural setting or indeed one delivered using telehealth. This explorative integrative review thus sought information pertaining to international practice in developing, delivering, sustaining, and supporting a community-based, generic LTC group rehabilitation programme delivered rurally in person or remotely using telehealth.
As our review was exploratory, we employed an integrative review method as it has the broadest type of search remit, allowing for multiple study types and methodologies to be included in the review (28, 29). The inclusion of such diverse literature provides the opportunity to gather a greater scope of articles and gain a deeper understanding of the topic to answer the research question more effectively.
An initial search of Google Scholar was undertaken to explore potential search terms relating to the research question. After discussion with a subject librarian and individual research team members, and exploration of OVID Medline, a table of potential search terms and their associated MeSH terms was developed (see Table 1). A methodical search (30) of Google Scholar, SCOPUS, TRIP, Cochrane, EBSCO (CINAHL), JBI, OVID (Medline, Embase, Emcare, Psychinfo) and SCiello was then undertaken (November-December 2020) using combinations of MeSH terms and keywords (as appropriate for each database). All searches used Boolean operators “AND” and “OR”. Discussion with experts in the field and searching of relevant journals (such as Journal of Rural Health) were also undertaken to generate further potential articles. Reference lists of potential articles were not searched for further potential articles.
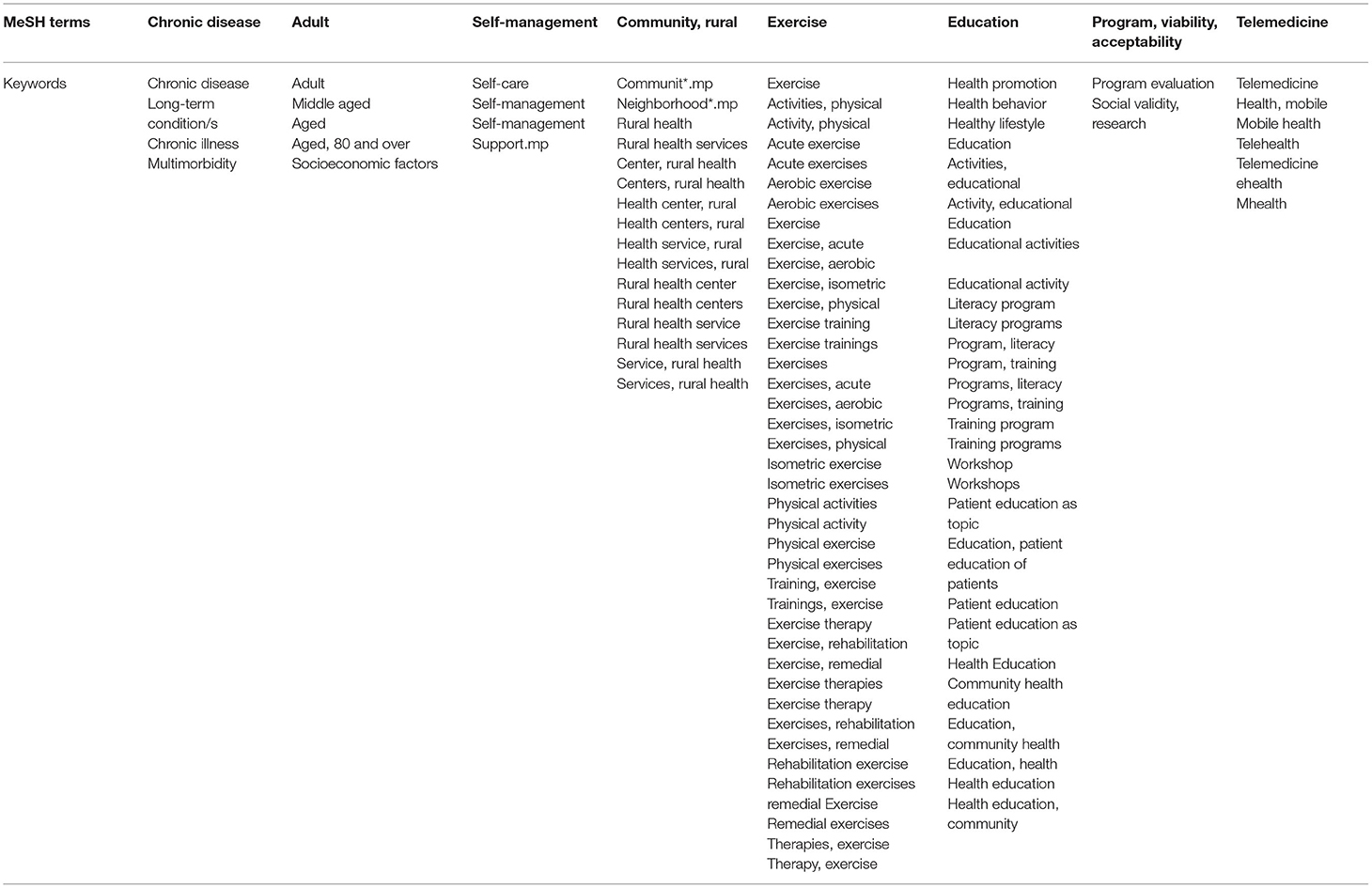
Table 1. Generic database list of MeSH and keyword search terms.
Potential articles were title and abstract screened for relevance to the research question and had to include key terms of “Chronic illness/disease/long-term conditions”, “Adult”, “Community, rural” and “Self-management” combined with terms of “Exercise”, “Education”, “Program, viability, acceptability”, and “Telemedicine” as appropriate to the individual databases (see Table 1). Articles were not included if they discussed home-based interventions delivered to one person, were delivered in a hospital or outpatient setting, included children/young people, or were not written in English. Extracted data required relevance to the research question with a focus on practical information pertaining to themes of development, delivery, integration, and ongoing support of a community-based, generic rehabilitation programme for people living with long-term health conditions (irrespective of the type of condition) delivered rurally and/or potentially via the internet (see Table 2 for definitions of themes). The full article was read if it were unclear in the abstract if it were relevant to the research aim. One author (AW) was responsible for decisions around suitability of articles for inclusion. Given the nature of this explorative integrative review and expected capture of publications with diverse study designs, included studies were not quality appraised.

Table 2. Definition of themes.
Data analysis, undertaken by one author (AW), involved extracting information pertaining to author, year, country or paper methodology, aim, and “demographics” of the study, review or report. This information was tabulated into an overall summary of included studies (see Table 3). Data pertaining to practical information about how to develop, deliver, integrate, and support a remotely delivered programme was then extracted from included studies. Through discussion and consensus by two authors (AW, LH) this information was deductively organized into “themes” (development, delivery, integration and support). These themes were derived from the research question, which was informed by multiple collaborative conversations with community stakeholders and modified from the RE-AIM framework (54) Data within each “theme” was then inductively (84) synthesized, again by the two authors, into five categories.
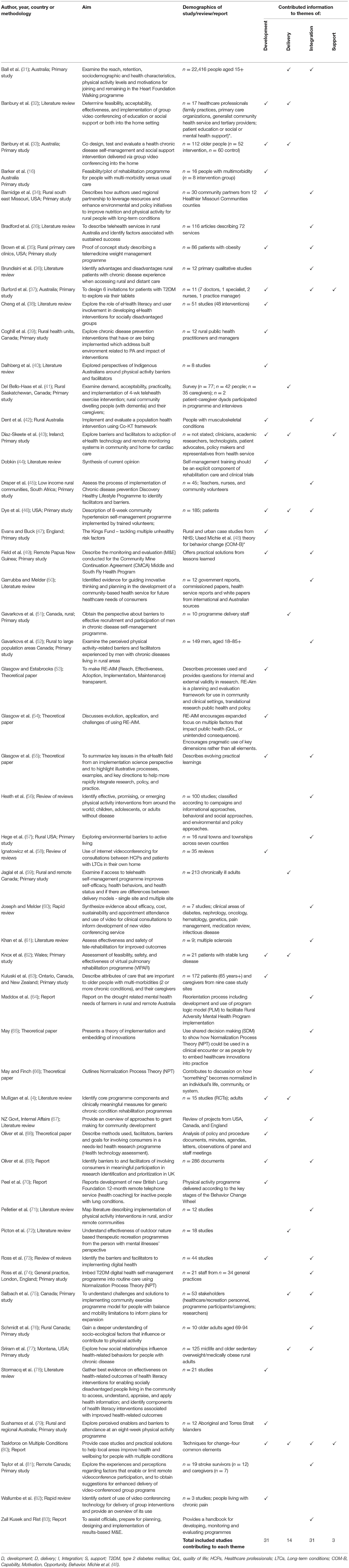
Table 3. Summary of included studies.
The search resulted in 24,485 potential articles from which 55 studies were included in the review (Figure 1). A mixture of primary studies (n = 27), reviews (n = 18), theoretical papers (n = 6) and reports (n = 4) were included. Five studies related to community-based programmes delivered to a group remotely via the internet [Banbury et al., Australia, older persons with chronic disease (33); Del Bello-Haas, Canada, persons with dementia and their carers (41); Jaglal et al., Canada, Chronic Disease Self-Management programme delivered via video conference (59); Knox et al., Wales, lung disease (62); Taylor et al., Canada, stroke survivors (81)]. The other 22 primary studies were about in-person delivery of a rehabilitation programme to a group of people. Table 3 also provides an indication of which studies contributed information to the themes.
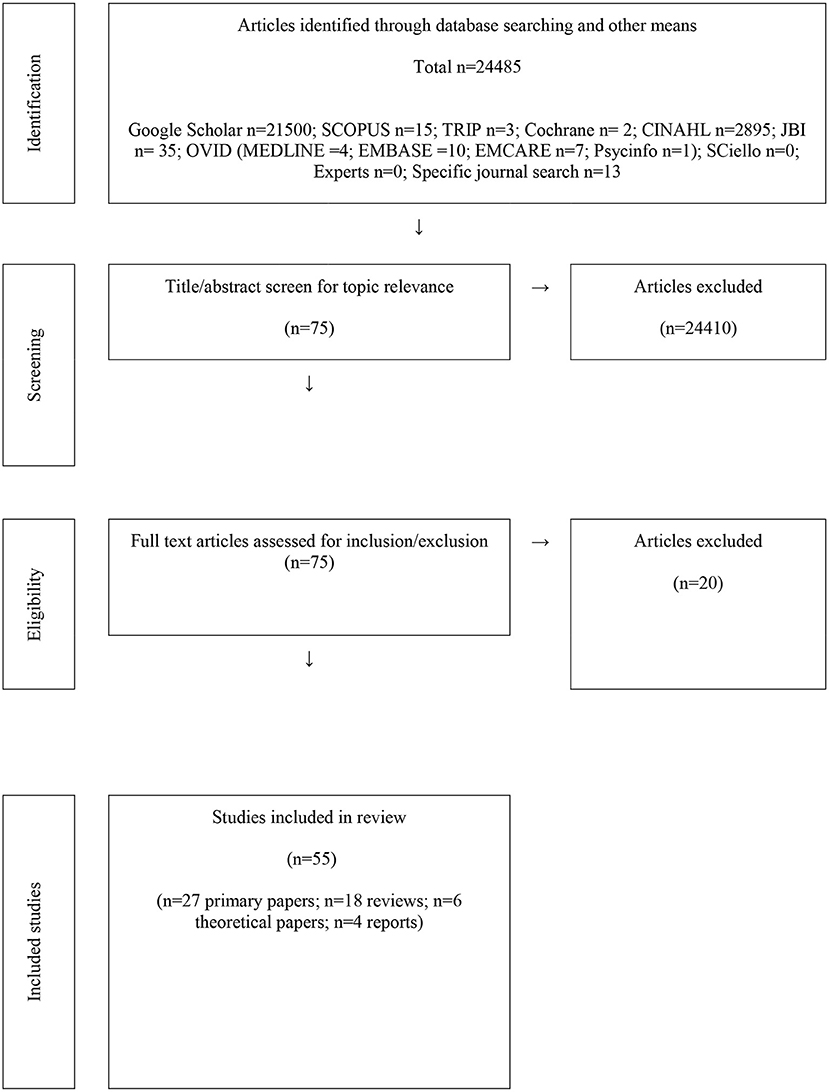
Figure 1. Summary of process of total data through the review.
From the inductive analysis, five categories were derived, theory, context, interpersonal aspects, technology, and programme aspects. Table 4 details the contribution of these categories to the themes. Development was the only theme populated by all categories. Only one category contributed to the theme of Support. The categories are summarized below.
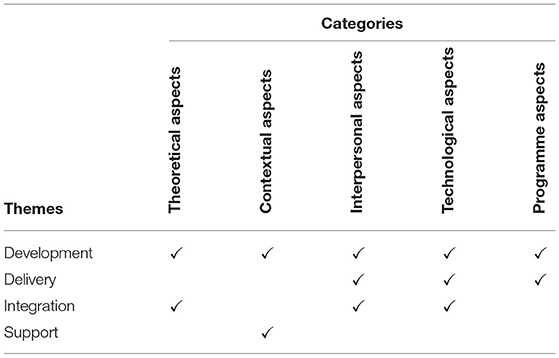
Table 4. Summary of categories contributing to themes.
This category contributed information to two themes, “Development” and “Integration”. A framework or theory should be used to both guide development of a rehabilitation programme and its implementation and maintenance (49, 50, 53–55, 64, 70). Use of a theoretical framework makes explicit what the health professional is addressing (66, 70) and thus may also facilitate personal growth for participants (65). Recommended is to develop, with the end-users, goals and a well-defined, efficient (procedures and process, cost), inclusive and adaptable implementation plan (underpinned by an implementation theory) that includes a sustainability plan for the programme/initiative (32, 34, 37, 39, 42, 43, 47, 49, 67, 73). These goals, plans and definitions of success can be identified upfront and need constant reviewing (49, 73). In rural and remote settings, flexibility and creativity are important and need to be utilized in programme design and delivery (42, 71). Focus on outcomes rather than outputs and identify and address barriers (16, 32, 33, 44, 73). Be cognisant of the fact that “one size does not fit all” (67) and that the community needs to want and own the programme or initiative (55, 63, 67–69). Note however, that a community development approach is more time intensive (34, 37, 67, 69).
The category of “Context” contributed information to the themes of “Development” and “Support”. Context is important and collated local knowledge should drive selection of intervention and assessment (47). This necessitates local consultations to find out what people want, need, and prefer (37, 43, 50, 69, 80). Also, of importance is a readiness assessment, for example identification of attitudes to the programme components and intention or readiness to attend (42, 73, 83). A continuing process for identifying and addressing barriers needs to be developed (42, 47, 51, 53, 57, 73, 74, 79, 81). It is important to create an environment whereby attendees become active in managing their own requirements (43). Further, any data collected must be securely stored and privacy is maintained (41, 43, 82). Development of a plan for ongoing infrastructure investment (26, 43, 60) and staff training was emphasized.
Three themes, “Development, Delivery and Integration” had contributing information from the “Interpersonal aspects” category. Working together on “the project” is essential (33, 34, 39, 69). Create an interactive environment (33) that facilitates development of relationship/social cohesiveness between the participants, spouses, family, and friends (33, 40, 41, 55, 56, 67, 71, 72, 76, 77, 80, 82). Focus on grass roots engagement, identifying shared goals and outcomes, building local resources and networks (67). Ensure projects are community owned and driven, that leadership is representative and inclusive (67). This builds relationships and a collaborative environment that values the contribution of everyone (34). Be aware though that it takes time to learn to work together (53). Build capacity in individuals, groups, and other stakeholders (67). Attract influential members (67). People may need training and require payment for their time (35, 68). Ensure programme is well supported by highly trained staff and volunteers (32, 41, 42, 68, 73). Encourage peer support by using male and female role models/lay leaders (4, 59) and via discussion, sharing of stories within the group (33, 81).
The category of “Technology” contributed information to themes of “Development”, “Delivery”, and “Integration”. Synthesized findings suggest programmes should use technology that is simple, easy to use, adaptable, compatible with existing systems and cost effective (58, 73). Be cognisant of and action regulatory standards, ethics, privacy, security, and storage issues for any data collected (43, 55, 73, 82). Consider use of tools, such as the Universal Design Survey, to assess IT needs/requirements of programme leaders and participants, and train people to use the technology (43). Use creative ways to assist attendees to remember session dates and times (74) and develop telehealth etiquette with them (59). Use innovative ways such as slides and videos to enhance group discussion (33). Plan for interruptions and disconnections to the video feed (35, 81) and hearing issues for attendees (62, 82). Consider where equipment (conferencing and exercise equipment) will be stored (41) and ensure room set up is easy for telehealth and exercise (41, 81). Train the trainers in telehealth etiquette and equipment use, conduct practice teaching sessions (35, 59), and prior to sessions provide a reminder session to review procedures (59) Embed regular monitoring and evaluation (M&E) into all aspects of the programme (49, 66, 73, 83). Involve the team in evaluation and communicate M&E information in multiple ways to stakeholders (49). Link any data collection with existing activities and processes (49, 73).
Two Themes, “Development” and “Delivery” had information derived from Category 5: “Programme aspects”. Include/invite/involve people (end-users) in development (33, 34, 39, 69) and provide/create a manual for participants and leaders (46). Address health literacy requirements (4, 55) through use of an ehealth literacy framework (38, 78). Consider use of clinically meaningful assessment and evaluation measures (4), and collection of attendance rates, cost effectiveness (61) and other pertinent data. Include exercise with clear guidance. Advertise the programme in a variety of ways (31, 46), understand and address barriers to attending the programme (42, 47, 51–53, 57, 73, 74, 79, 81), and provide flexibility in programme delivery (e.g., times and places) (35, 42, 51, 55, 64, 79, 85). Need to consider the class size and instructor-to-participant ratio (75) and who will attend, including the minimum level of walking ability, if including physical activity (75). Programme length is recommended to be 4–8 weeks, and use lay and peer led (4) “buddy coaches” with teaching skills to work with the attendees (46).
This integrative review explored literature for international evidence for developing, delivering, sustaining, and supporting a rural or internet delivered, community-wide, generic long-term conditions rehabilitation programme. While the review has several potential limitations (its explorative nature and broad approach, lack of quality appraisal of included studies, and an inherent risk of bias through one author working on inclusion of studies and data extraction), the review nevertheless provides a practical, important and timely contribution to the wider literature. Information gleaned and synthesized from the included studies suggest practical, fundamental points for consideration and were organized into categories of theory, context, interpersonal aspects, technology and programme aspects. The practical implications arising from our findings are summarized in Box 1.
Box 1. Summary of practical implications arising from findings of the review.
• Co-development with community end-users should drive intervention and assessment choices and thereby facilitate local ownership of the programme.
• Building local resources, networks, capacity and leadership that is representative and inclusive is important.
• Ensure flexible programme design and delivery.
• Place importance on relationships, social cohesiveness and peer support between attendees, partners, family, and friends, and on highly trained staff and
• volunteers.
• Adopt simple, cost effective technology that is easy to use, adaptable and compatible with existing systems.
• Assess information technology needs of programme leaders and participants, and train people to use the technology.
• Address health literacy requirements.
• Be cognizant of and action regulatory and ethical standards for data collected, plan for interruptions to the video feed, and for hearing issues for attendees.
• Advertise the programme widely and work to understand and address barriers to attendance.
When creating, delivering, sustaining, and supporting a generic rehabilitation programme, the findings from this review suggest the programme needs to be underpinned by “theory.” Such theory is often derived from the field of implementation science (86). Davidoff, Dixon-Woods (87) suggest that while the word “theory” might be an abstract or irrelevant academic term to some, they contend that all people “find and use reasons–and thus theorize” (p. 229) daily. They propose the challenge is to “make explicit the informal and formal theories” (p. 230) people use because this may highlight assumptions, weaknesses, or contradictions in the proposed intervention programme's hypothesis, and expose any lack of consensus among the team (87). Use of what is termed a “small theory” or “programme theory” provides a framework for outlining programme components, expected outcomes and their assessment methods (87). Additionally the theory assists to make explicit and clear the assumptions and rationale linking “processes and inputs to outcomes … and conditions (or context) necessary for effectiveness” (p. 230) (87). Many people skip working out the programme theory and rush to implementation, thus limiting “learning that can inform planning of future interventions” (p. 232) (87). Choosing a theory may not be that straight forward. Lynch, Mudge (88) and Nilsen (86) in their debate papers provide useful summary for understanding available theories (current at time of publication of their papers), and a starting point and pragmatic guide for selection of “theory/ies” to underpin programmes/interventions.
This review highlighted the importance of interpersonal factors for developing, delivering, sustaining, and supporting a programme. Working together with the people to whom it matters on programme development requires time to build relationships, talk, acknowledge and share power, reflect, and return repeatedly to these processes as the programme is developed, delivered, and evaluated (89, 90). Time that is often not always available in the research arena because of constraints applied by funders and commissioners, or even because of a difference in world views between team members and community members (a biomedical v a bio-psycho-social viewpoint). While time may not be “available,” relationships are integral to care and healing processes (91). Development and maintenance of meaningful relationships with other people is acknowledged to lead to improvement in wellbeing and health (92–95). The concept of relationship-centered care, argued to be the founding principle for all healthcare provision (91), may provide a framework for understanding the interrelated relationships necessary when working on programme development together with people to whom it matters.
Linked with the importance of developing meaningful relationships and working together with stakeholders (individuals, groups, communities, policy makers) are issues of pertaining to the context, particularly of valuing local knowledge about what is wanted, needed, and preferred. For developers, there are many ways to approach this depending on the philosophical and methodological viewpoint. For example, in included studies where the programme developers have already defined the topic of interest, to a study where the developers join with a community of stakeholders, and the community discuss what needs to be explored (96) (using a Participatory Action Research or co-design approach). Such stakeholder involvement can range from defining the issue/s, developing the programme, through to contributing as a participant, or interest only in the outcomes of the programme development project (97). Boaz, Hanney (97) suggest the literature assessing the impact of stakeholder engagement is limited but an increasing area of interest. They put forward three design principles for stakeholder engagement of organizational, values, and practices (with supporting literature) for developers to consider when thinking about stakeholder engagement and promoting impact of project development (97).
The idea of assessing readiness for change/engagement by people, communities, and organizations would also seem useful. Yet terminology used in the area is confused, and there is no gold standard assessment available as instruments available are tailored to specific contexts and/or interventions (98). Miake-Lye, Delevan (98), in their systematic review of organizational readiness assessments mapped to the Consolidated Framework for Implementation Research (CFIR), suggest the seven most frequent CFIR constructs identified (readiness for implementation, implementation climate, other personal attributes, structural characteristics, networks and communications, self-efficacy, and culture) could provide something to consider when developing or tailoring a readiness assessment. Miake-Lye, Delevan (98) made only minor amendments to classify items, suggesting readiness for change is captured in the CFIR, with one addition relating to teams. It seems using a broad framework such as the CFIR may be another useful tool for programme developers.
The main findings from the review regarding “Technology” highlight attention to the principles of “KISS” (keep it simple stupid) (99) and Universal Design (100, 101), and integration of health and eHealth literacy concepts (38) across all phases of implementation of the programme to facilitate access to the programme for a wider range of people. Additionally, the importance of embedding monitoring and evaluation processes within all phases of programme “development” seems pertinent to assess effectiveness of an intervention.
Many of the practical tips embedded in “Programme aspects” reiterate the importance of attending to the interpersonal factors discussed above. Further findings highlighted the importance of addressing health literacy requirements of participants. Health literacy is important and much has been written about it (78, 102–105). However, “health literacy” is greater than individual competencies alone, it also includes community, services, and health system literacy capacities (106) and all these areas need to be considered and addressed when developing a programme or intervention.
Our review has drawn together a large body of diverse work. It has focused on finding practical information pertaining to the best ways to develop, deliver, integrate, and support a community-based group generic rehabilitation programme for people living with long-term health conditions, delivered rurally in person and/or potentially via the internet. Practical suggestions were thematically organized into categories of “theory”, “context”, “interpersonal aspects”, and “technology” and “programme aspects”. Box 1 provides a summary of the practical implications derived from the review. While the findings of this review might appear simple and self-evident, they may be difficult to enact in practice.
Conception and design: LH, TS, CH, and JD. Data collection: AW. Data analysis and interpretation and drafting original article: AW and LH. All authors critical revision of article and final approval of version to be published.
This work was supported by the Health Research Council of New Zealand [Grant Number 20/1167].
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ministry of Health. Long-Term Conditions (2020). Available onlillne at: https://www.health.govt.nz/our-work/diseases-and-conditions/long-term-conditions#1 (accessed February 2022).
2. Ministry of Health (NZ). Self-Management Support for People with Long Term Conditions. 2 ed. Wellington, New Zealand: Minstry of Health (2016).
3. de Souto Barreto P. Exercise for multimorbid patients in primary care: one prescription for all? Sports Med (2017) 47:2143–53. doi: 10.1007/s40279-017-0725-z
4. Mulligan H, Wilkinson A, Chen D, Nijhof C, Kwan N, Lindup A, et al. Components of community rehabilitation programme for adults with chronic conditions: a systematic review. Int J Nurs Stud (2019) 97:114–29. doi: 10.1016/j.ijnurstu.2019.05.013
5. Stokes T, Wilkinson A, Jayakaran P, Higgs C, Keen D, Mani R, et al. Implementation of the diabetes community exercise and education programme (Dcep) for the management of type 2 diabetes: qualitative process evaluation. BMJ Open (2022). 12:e059853. doi: 10.1136/bmjopen-2021-059853
6. Hale L, Higgs C, Keen D, Smith C. It is ‘All About Relationships' in lifestyle programmes for adults living with type two diabetes underpinned by a person/whānau-centred care approach. Front. Rehabilitat. Sci. (2022) 3:829542. doi: 10.3389/fresc.2022.829542
7. Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet (2012) 380:37–43. doi: 10.1016/S0140-6736(12)60240-2
8. Caughey GE, Roughead EE. Multimorbidity research challenges: where to go from here? J Comorbid (2011) 1:8–10. doi: 10.15256/joc.2011.1.9
9. Stokes T. Multimorbidity and clinical guidelines: problem or opportunity? N Z Med J (2018) 131:1472. Available online at: http://www.nzma.org.nz/journal/read-the-journal/all-issues/2010-2019/2018/vol-131-no-1472-23-march-2018/7523 (accessed March 23, 2018).
10. Stokes T, Tumilty E, Doolan-Noble F, Gauld R. Multimorbidity, clinical decision making and health care delivery in new zealand primary care: a qualitative study. BMC Fam Pract (2017) 18:51. doi: 10.1186/s12875-017-0622-4
11. Rauch A, Negrini S, Cieza A. Toward strengthening rehabilitation in health systems: methods used to develop a who package of rehabilitation interventions. Arch Phys Med Rehabil (2019) 100:2205–11. doi: 10.1016/j.apmr.2019.06.002
12. Kirby RL. Who package of rehabilitation interventions: some concerns about methodology. Arch Phys Med Rehabil (2020) 101:1095. doi: 10.1016/j.apmr.2019.12.018
13. Gielen S, Laughlin MH, O'Conner C, Duncker DJ. Exercise training in patients with heart disease: review of beneficial effects and clinical recommendations. Prog Cardiovasc Dis (2015) 57:347–55. doi: 10.1016/j.pcad.2014.10.001
14. Alison JA, McKeough ZJ, Johnston K, McNamara RJ, Spencer LM, Jenkins SC, et al. Australian and New Zealand pulmonary rehabilitation guidelines. Respirology (2017) 22:800–19. doi: 10.1111/resp.13025
15. World Health Organisation. Rehabilitation. World Report on Disabilities. Geneva: World Health Organisation (2011).
16. Barker K, Holland AE, Lee AL, Haines T, Ritchie K, Boote C, et al. Multimorbidity rehabilitation versus disease-specific rehabilitation in people with chronic diseases: a pilot randomized controlled trial. Pilot Feasibil Stud (2018) 4:181. doi: 10.1186/s40814-018-0369-2
17. Valderas JM, Starfield B, Sibbald B, Salisbury C, Roland M. Defining comorbidity: implications for understanding health and health services. Ann Fam Med (2009) 7:357–63. doi: 10.1370/afm.983
18. Levack WM, Weatherall M, Reeve JC, Mans C, Mauro A. Uptake of pulmonary rehabilitation in New Zealand by people with chronic obstructive pulmonary disease in 2009. N Z Med J (2012) 125:23–33. Available online at: https://assets-global.website-files.com/5e332a62c703f653182faf47/5e332a62c703f6ee8a2fdf1a_levack.pdf
19. Pack QR, Squires RW, Lopez-Jimenez F, Lichtman SW, Rodriguez-Escudero JP, Lindenauer PK, et al. Participation rates, process monitoring, and quality improvement among cardiac rehabilitation programs in the united states: a national survey. J Cardiopulm Rehabil Prev (2015) 35:173–80. doi: 10.1097/HCR.0000000000000108
20. Leclair LL, Zawaly K, Korall AMB, Edwards J, Katz A, Sibley KM. Exploring the delivery of community rehabilitation services for older people in an urban canadian setting: perspectives of service providers, managers and health system administrators. Health Social Care in the Commun. 00:1–10. doi: 10.1111/hsc.13662
21. Disler R, Glenister K, Wright J. Rural chronic disease research patterns in the United Kingdom, United States, Canada, Australia and New Zealand: a systematic integrative review. BMC Public Health (2020) 20:770. doi: 10.1186/s12889-020-08912-1
22. Dummer J, Tumilty E, Hannah D, McAuley K, Baxter J, Doolan-Noble F, et al. Health care utilisation and health needs of people with severe copd in the Southern Region of New Zealand: a retrospective case note review. COPD (2020) 17:136–42. doi: 10.1080/15412555.2020.1724275
23. Smith KB, Humphreys JS, Wilson MG. Addressing the health disadvantage of rural populations: how does epidemiological evidence inform rural health policies and research? Aust J Rural Health (2008) 16:56–66. doi: 10.1111/j.1440-1584.2008.00953.x
24. Ministry of Health (NZ). Telehealth: Ministry of Health (2017). Available online at: https://www.health.govt.nz/our-work/digital-health/other-digital-health-initiatives/telehealth (accessed February 2022).
25. Ministry of Health. Mātātuhi Tuawhenua: Health of Rural Māori 2012 Wellington: Ministry of Health (2017).
26. Bradford NK, Caffery LJ, Smith AC. Telehealth services in rural and remote australia: a systematic review of models of care and factors influencing success and sustainability. Rural Remote Health (2016) 16:3808. doi: 10.22605/RRH4268
27. Breton M, Sullivan EE, Deville-Stoetzel N, McKinstry D, DePuccio M, Sriharan A, et al. Telehealth challenges during Covid-19 as reported by primary healthcare physicians in Quebec and Massachusetts. BMC Fam Pract (2021) 22:192. doi: 10.1186/s12875-021-01543-4
28. Noble H, Smith J. Reviewing the literature: choosing a review design. Evidence Based Nursing (2018) 21:39. doi: 10.1136/eb-2018-102895
29. Whittemore R, Knafl K. The integrative review: updated methodology. J Adv Nurs (2005) 52:546–53. doi: 10.1111/j.1365-2648.2005.03621.x
30. Toronto CE, Remington R. A Step-by-Step Guide to Conducting an Integrative Review. Switzerland: Springer (2020). doi: 10.1007/978-3-030-37504-1
31. Ball K, Abbott G, Wilson M, Chisholm M, Sahlqvist S. How to get a nation walking: reach, retention, participant characteristics and programe implications of heart foundation walking, a nationwide australian community-based walking program. Int J Behav Nutr Phys Act (2017) 14. doi: 10.1186/s12966-017-0617-5 (accessed February 2, 2022).
32. Banbury A, Nancarrow S, Dart J, Gray L, Parkinson L. Telehealth interventions delivering home-based support group videoconferencing: systematic review. J Med Internet Res (2018) 20:e25. doi: 10.2196/jmir.8090
33. Banbury A, Nancarrow S, Dart J, Gray L, Dodson S, Osborne R, et al. Adding value to remote monitoring: co-design of a health literacy intervention for older people with chronic disease delivered by telehealth - the telehealth literacy project. Patient Educ Couns. (2020) 103:597–606. doi: 10.1016/j.pec.2019.10.005
34. Barnidge EK, Baker EA, Estlund A, Motton F, Hipp PR, Brownson RC, et al. Participatory regional partnership approach to promote nutrition and physical activity through environmental and policy change in Rural Missouri. Preventing Chronic Disease (2015) 12:E92. doi: 10.5888/pcd12.140593
35. Brown JD, Hales S, Evans TE, Turner T, Sword DO, O'Neil PM, et al. Description, utilisation and results from a telehealth primary care weight management intervention for adults with obesity in South Carolina. J Telemed Telecare (2020) 26:28–35. doi: 10.1177/1357633X18789562
36. Brundisini F, Giacomini M, DeJean D, Vanstone M, Winsor S, Smith A. Chronic disease patients' experiences with accessing health care in rural and remote areas: a systematic review and qualitative meta-synthesis. Ont Health Technol Assess Ser (2013) 13:1–33.
37. Burford S, Park S, Dawda P, Burns J. Participatory research design in mobile health: tablet devices for diabetes self-management. Commun Med (2015) 12:145–56. doi: 10.1558/cam.27120
38. Cheng C, Beauchamp A, Elsworth GR, Osborne RH. Applying the electronic health literacy lens: systematic review of electronic health interventions targeted at socially disadvantaged groups. J Med Internet Res (2020) 22:e18476. doi: 10.2196/18476
39. Coghill C-L, Valaitis RK, Eyles JD. Built environment interventions aimed at improving physical activity levels in rural ontario health units: a descriptive qualitative study. BMC Public Health (2015) 15:464. doi: 10.1186/s12889-015-1786-2
40. Dahlberg EE, Hamilton SJ, Hamid F, Thompson SC. Indigenous Australians perceptions' of physical activity: a qualitative systematic review. Int J Environ Res Public Health (2018) 15:1492. doi: 10.3390/ijerph15071492
41. Dal Bello-Haas VP, O'Connell ME, Morgan DG, Crossley M. Lessons learned: feasibility and acceptability of a telehealth-delivered exercise intervention for rural-dwelling individuals with dementia and their caregivers. Rural Remote Health (2014) 14:2715. doi: 10.22605/RRH2715
42. Dent E, Hoon E, Kitson A, Karnon J, Newbury J, Harvey G, et al. Translating a health service intervention into a rural setting: lessons learned. BMC Health Serv Res (2016) 16:62. doi: 10.1186/s12913-016-1302-0
43. Diaz-Skeete Y, Giggins OM, McQuaid D, Beaney P. Enablers and obstacles to implementing remote monitoring technology in cardiac care: a report from an interactive workshop. Health Informatics J (2019) 26:2280–8. doi: 10.1177/1460458219892175
44. Dobkin BH. Behavioral self-management strategies for practice and exercise should be included in neurologic rehabilitation trials and care. Curr Opin Neurol (2016) 29:693–9. doi: 10.1097/WCO.0000000000000380
45. Draper CE, Nemutandani SM, Grimsrud AT, Rudolph M, Kolbe-Alexander TL, de Kock L, et al. Qualitative evaluation of a physical activity-based chronic disease prevention program in a low-income, rural South African Setting. Rural Remote Health (2010) 10:1467. doi: 10.22605/RRH1467
46. Dye CJ, Williams JE, Evatt JH. Activating patients for sustained chronic disease self-management: thinking beyond clinical outcomes. J Prim Care Community Health (2016) 7:107–12. doi: 10.1177/2150131915626562
47. Evans H, Buck D. Tackling Multiple Unhealthy Risk Factors - Emerging Lessons from Practice UK: The King's Fund (2018). Available online at: https://www.kingsfund.org.uk/publications/tackling-multiple-unhealthy-risk-factors (accessed February 2, 2022).
48. Michie S, van Stralen MM, West R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement Sci. (2011) 6:42. doi: 10.1186/1748-5908-6-42
49. Field E, Vila M, Runk L, Mactaggart F, Rosewell A, Nathan S. Lessons for health program monitoring and evaluation in a low resource setting. Rural Remote Health (2018) 18:4596. doi: 10.22605/RRH4596
50. Garrubba M, Melder A. Re-Imagining Community Healthcare Services Melbourne, Australia: Centre for Clinical Effectiveness, Monash Health 2019 (2021). Available online at: https://monashhealth.org/wp-content/uploads/2019/06/Community-Health-Strategy_Scoping-Review_FINAL-2019.pdf
51. Gavarkovs AG, Burke SM, Reilly KC, Petrella RJ. Barriers to recruiting men into chronic disease prevention and management programs in rural areas: perspectives of program delivery staff. Am J Mens Health (2016) 10:Np155–np7. doi: 10.1177/1557988315596226
52. Gavarkovs AG, Burke SM, Petrella RJ. The physical activity-related barriers and facilitators perceived by men living in rural communities. Am J Mens Health (2017) 11:1130–2. doi: 10.1177/1557988315598368
53. Glasgow RE, Estabrooks PE. Pragmatic applications of re-aim for health care initiatives in community and clinical settings. Prev Chronic Dis (2018) 15:E02. doi: 10.5888/pcd15.170271
54. Glasgow RE, Harden SM, Gaglio B, Rabin B, Smith ML, Porter GC, et al. Re-aim planning and evaluation framework: adapting to new science and practice with a 20-year review. Front Public Health (2019) 7. doi: 10.3389/fpubh.2019.00064
55. Glasgow RE, Phillips SM, Sanchez MA. Implementation science approaches for integrating ehealth research into practice and policy. Int J Med Inform (2014) 83:e1–11. doi: 10.1016/j.ijmedinf.2013.07.002
56. Heath GW, Parra DC, Sarmiento OL, Andersen LB, Owen N, Goenka S, et al. Evidence-based intervention in physical activity: lessons from around the world. Lancet (2012) 380:272–81. doi: 10.1016/S0140-6736(12)60816-2
57. Hege A, Christiana RW, Battista R, Parkhurst H. Active living in rural appalachia: using the rural active living assessment (Rala) tools to explore environmental barriers. Prev Med Rep (2017) 8:261–6. doi: 10.1016/j.pmedr.2017.11.007
58. Ignatowicz A, Atherton H, Bernstein CJ, Bryce C, Court R, Sturt J, et al. Internet videoconferencing for patient-clinician consultations in long-term conditions: a review of reviews and applications in line with guidelines and recommendations. Digital Health (2019) 5:2055207619845831. doi: 10.1177/2055207619845831
59. Jaglal SB, Haroun VA, Salbach NM, Hawker G, Voth J, Lou W, et al. Increasing access to chronic disease self-management programs in rural and remote communities using telehealth. Telemed J E Health (2013) 19:467–73. doi: 10.1089/tmj.2012.0197
60. Joseph C, Melder A. Telehealth the Use of Video Conferences: A Rapid Review Melbourne, Australia: Centre for Clinical Effectiveness, Monash Health (2018). Available online at: https://monashhealth.org/wp-content/uploads/2019/01/Telehealth-Rapid-Review-Final.pdf
61. Khan F, Amatya B, Kesselring J, Galea M. Telerehabilitation for persons with multiple sclerosis. Cochrane Database Syst Rev (2015) 2015:Cd010508. doi: 10.1002/14651858.CD010508.pub2
62. Knox L, Dunning M, Davies C-A, Mills-Bennet R, Sion TW, Phipps K, et al. Safety, feasibility, and effectiveness of virtual pulmonary rehabilitation in the real world. Int J Chron Obstruct Pulmon Dis (2019) 14:775–80. doi: 10.2147/COPD.S193827
63. Kuluski K, Peckham A, Gill A, Gagnon D, Wong-Cornall C, McKillop A, et al. What is important to older people with multimorbidity and their caregivers? Identifying attributes of person centered care from the user perspective. Int J Integr Care (2019) 19:4. doi: 10.5334/ijic.s3271
64. Maddox S, Read DMY, Powell NN, Caton TJ, Dalton HE, Perkins DA. Reorientation of the rural adversity mental health program: the value of a program logic model. Rural Remote Health (2019) 19:5217. doi: 10.22605/RRH5217
65. May C. Agency and implementation: understanding the embedding of healthcare innovations in practice. Soc Sci Med (2013) 78:26–33. doi: 10.1016/j.socscimed.2012.11.021
66. May C, Finch T. Implementing, embedding, and integrating practices: an outline of normalization process theory. Sociology (2009) 43:535–54. doi: 10.1177/0038038509103208
67. NZ Govt Internal Affairs. Some International Approaches to Community Grant Funding NZ: Author (2011). Available online at: https://www.dia.govt.nz/Resource-material-Our-Policy-Advice-Areas-Community-led-Development (accessed February 2, 2022).
68. Oliver S, Milne R, Bradburn J, Buchanan P, Kerridge L, Walley T, et al. Involving consumers in a needs-led research programme: a pilot project. Health Expect (2001) 4:18–28. doi: 10.1046/j.1369-6513.2001.00113.x (accessed February 2, 2022).
69. Oliver S, Clarke-Jones L, Rees R, Milne R, Buchanan P, Gabbay J, et al. Involving consumers in research and development agenda setting for the nhs: developing an evidence-based approach. Health Technol Assess (2004) 8:1–148. doi: 10.3310/hta8150
70. Peel J, Webb J, Jones AW. A Remote behaviour change service for increasing physical activity in people with chronic lung conditions: intervention development using the behaviour change wheel. Perspect Public Health (2020) 140:16–21. doi: 10.1177/1757913919880928
71. Pelletier CA, Pousette A, Ward K, Keahey R, Fox G, Allison S, et al. Implementation of physical activity interventions in rural, remote, and northern communities: a scoping review. Inquiry (2020) 57:46958020935662. doi: 10.1177/0046958020935662
72. Picton C, Fernandez R, Moxham L, Patterson CF. Experiences of outdoor nature-based therapeutic recreation programs for persons with a mental illness: a qualitative systematic review. JBI Evid Synth (2020) 18:1820–69. doi: 10.11124/JBISRIR-D-19-00263
73. Ross J, Stevenson F, Lau R, Murray E. Factors that influence the implementation of E-health: a systematic review of systematic reviews (an Update). Implementat. Sci (2016) 11:146. doi: 10.1186/s13012-016-0510-7
74. Ross J, Stevenson F, Dack C, Pal K, May C, Michie S, et al. Developing an implementation strategy for a digital health intervention: an example in routine healthcare. BMC Health Serv Res (2018) 18:794. doi: 10.1186/s12913-018-3615-7
75. Salbach NM, Howe J-A, Baldry D, Merali S, Munce SEP. Considerations for expanding community exercise programs incorporating a healthcare-recreation partnership for people with balance and mobility limitations: a mixed methods evaluation. BMC Res Notes (2018) 11:214. doi: 10.1186/s13104-018-3313-x (accessed February 2, 2022).
76. Schmidt L, Rempel G, Murray TC, McHugh T-L, Vallance JK. Exploring beliefs around physical activity among older adults in rural Canada. Int J Qual Stud Health (2016) 11:32914. doi: 10.3402/qhw.v11.32914
77. Sriram U, Morgan EH, Graham ML, Folta SC, Seguin RA. Support and sabotage: a qualitative study of social influences on health behaviors among rural adults. J Rural Health (2018) 34:88–97. doi: 10.1111/jrh.12232
78. Stormacq C, Wosinski J, Boillat E, Van den Broucke S. Effects of health literacy interventions on health-related outcomes in socioeconomically disadvantaged adults living in the community: a systematic review. JBI Evid Synth (2020) 18:1389–469. doi: 10.11124/JBISRIR-D-18-00023
79. Sushames A, Engelberg T, Gebel K. Perceived barriers and enablers to participation in a community-tailored physical activity program with indigenous australians in a regional and rural setting: a qualitative study. Int J Equity Health (2017) 16:172. doi: 10.1186/s12939-017-0664-1
80. Taskforce on Multiple Conditions. The Multiple Conditions Guidebook UK: Richmond Group of Charities, Guy's St Thomas' Charity the Royal College of General Practitioners (2019). Available online at: https://richmondgroupofcharities.org.uk/sites/default/files/multiple_conditions_report_a4_digital_spreads_noembargo_1.pdf
81. Taylor DM, Stone SD, Huijbregts MP. Remote participants' experiences with a group-based stroke self-management program using videoconference technology. Rural Remote Health (2012) 12:1947. doi: 10.22605/RRH1947
82. Walumbe J, Belton J, Denneny D. Pain management programmes via video conferencing: a rapid review. Scand J Pain (2021) 21:32–40. doi: 10.1515/sjpain-2020-0112 (accessed February 2, 2022).
83. Zall Kusek J, Rist RC. Ten Steps to a Results-Based Monitoring Evaluation System: A Handbook for Development Practitioners Washington, DC: The World Bank (2004). Available online at: https://openknowledge.worldbank.org/handle/10986/14926
84. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
85. Barker K, Holland AE, Lee AL, Ritchie K, Boote C, Lowe S, et al. A rehabilitation programme for people with multimorbidity versus usual care: a pilot randomized controlled trial. J Comorb (2018) 8:2235042x18783918. doi: 10.1177/2235042X18783918
86. Nilsen P. Making sense of implementation theories, models and frameworks. Implementation Science (2015) 10:53. doi: 10.1186/s13012-015-0242-0
87. Davidoff F, Dixon-Woods M, Leviton L, Michie S. Demystifying theory and its use in improvement. BMJ Quality Safety (2015) 24:228. doi: 10.1136/bmjqs-2014-003627
88. Lynch EA, Mudge A, Knowles S, Kitson AL, Hunter SC, Harvey G. “There Is Nothing So Practical as a Good Theory”: a pragmatic guide for selecting theoretical approaches for implementation projects. BMC Health Serv Res (2018) 18:857. doi: 10.1186/s12913-018-3671-z
89. Grant H, Nelson G, Mitchell T. Negotiating the Challenges of Participatory Action Research: Relationships, Power, Participation, Change and Credibility (2008 2022/02/16). In: The SAGE Handbook of Action Research. SAGE Publications Ltd. 2nd. Available online at: https://methods.sagepub.com/book/the-sage-handbook-of-action-research
90. Walker S, Eketone A, Gibbs A. An exploration of Kaupapa Māori research, its principles, processes and applications. Int J Soc Res Methodol (2006) 9:331–44. doi: 10.1080/13645570600916049
91. Beach M, Inui T. Relationship-centered care research network. Relationship-centered care a constructive reframing. J Gen Intern Med (2006) 21:S3–8. doi: 10.1111/j.1525-1497.2006.00302.x (accessed February 2, 2022).
92. Seppala E, Rossomando T, Doty J. Social connection and compassion: important predictors of health and well-being. Social Res (2013) 80:411–30. doi: 10.1353/sor.2013.0027
93. Sirven N, Debrand T. Social participation and healthy ageing: an international comparison using share data. Soc Sci Med (2008) 67:2017–26. doi: 10.1016/j.socscimed.2008.09.056
94. Wilkinson A, Atlas J, Fagan K, Mulligan H. Client perceptions of engaging with a health and social care navigation service: a qualitative study. Chronic Illn (2019) 18:169–80. doi: 10.1177/1742395320937046
95. Zavaleta D, Samuel K, Mills C. Ophi Working Paper No. 67 Social Isolation: A Conceptual and Measurement Proposal Oxford Poverty & Human Development Initiative. University of Oxford (2014). doi: 10.35648/20.500.12413/11781/ii029
96. Wada M, Sixsmith J, Harwood G, Cosco TD, Fang ML, Sixsmith A, et al. Protocol for co-creating research project lay summaries with stakeholders: guideline development for canada's age-well network. Res Involv Engagem (2020) 6:22. doi: 10.1186/s40900-020-00197-3
97. Boaz A, Hanney S, Borst R, O'Shea A, Kok M. How to engage stakeholders in research: design principles to support improvement. Health Res Policy Syst (2018) 16:60. doi: 10.1186/s12961-018-0337-6
98. Miake-Lye IM, Delevan DM, Ganz DA, Mittman BS, Finley EP. Unpacking organizational readiness for change: an updated systematic review and content analysis of assessments. BMC Health Serv Res (2020) 20:106. doi: 10.1186/s12913-020-4926-z
99. Di Marco L, Leone A, Murana G, Pacini D. The application of the “kiss principle” for the treatment of type a acute aortic dissection: is this always right? J Thorac Dis (2018) 10:S3884–S6. doi: 10.21037/jtd.2018.08.132
100. Carr K, Weir PL, Azar D, Azar NR. Universal design: a step toward successful aging. J Aging Res (2013) 2013:324624. doi: 10.1155/2013/324624
101. Story MF. Maximising usability: the principles of universal design. Assistive Technol (1998) 10:4–12. doi: 10.1080/10400435.1998.10131955
102. Levasseur M, Carrier A. Do rehabilitation professionals need to consider their clients' health literacy for effective practice? Clin Rehabil (2010) 24:756–65. doi: 10.1177/0269215509360752
103. van der Gaag M, Heijmans M, Spoiala C, Rademakers J. The importance of health literacy for self-management: a scoping review of reviews. Chronic Illness. 18:234–54. doi: 10.1177/17423953211035472
104. Brabers AEM, Rademakers JJDJM, Groenewegen PP, van Dijk L, de Jong JD. What role does health literacy play in patients' involvement in medical decision-making? PLoS ONE (2017) 12:e0173316-e. doi: 10.1371/journal.pone.0173316
105. Liu C, Wang D, Liu C, Jiang J, Wang X, Chen H, et al. What is the meaning of health literacy? A systematic review and qualitative synthesis. Fam Med Community Health (2020) 8:e000351. doi: 10.1136/fmch-2020-000351
Keywords: community, long-term conditions, rehabilitation programmes, rural, telehealth
Citation: Wilkinson A, Higgs C, Stokes T, Dummer J and Hale L (2022) How to Best Develop and Deliver Generic Long-Term Condition Rehabilitation Programmes in Rural Settings: An Integrative Review. Front. Rehabilit. Sci. 3:904007. doi: 10.3389/fresc.2022.904007
Received: 25 March 2022; Accepted: 16 May 2022;
Published: 21 June 2022.
Edited by:
Nuno Barbosa Rocha, Polytechnic of Porto, PortugalReviewed by:
Marc Beaumont, Université de Bretagne Occidentale, FranceCopyright © 2022 Wilkinson, Higgs, Stokes, Dummer and Hale. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Leigh Hale, bGVpZ2guaGFsZUBvdGFnby5hYy5ueg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.