 Delena Amsters
Delena Amsters- 1Spinal Outreach Team, Queensland Spinal Cord Injuries Service, Metro South Health, Brisbane, QLD, Australia
- 2The Hopkins Centre, Menzies Health Institute, Griffith University, Brisbane, QLD, Australia
- 3Transitional Rehabilitation Program, Queensland Spinal Cord Injuries Service, Metro South Health, Brisbane, QLD, Australia
- 4Central Queensland Centre for Rural and Remote Health, James Cook University, Emerald, QLD, Australia
Background: Greater understanding of the influences on participation in life after spinal cord injury (SCI) can inform rehabilitation theory and practice. Careful qualitative inquiry can reveal subjective meanings associated with the relevant experiences, strategies, and perceptions of those with lived experience of SCI. A search of literature, followed by a thematic synthesis of qualitative studies, was undertaken to bring together these insights in a meaningful way.
Methods: The research question guiding the literature review and synthesis was, What do people with SCI perceive to be the influences on their participation in life? Three critical databases were searched for qualitative studies examining influences on participation in life after SCI. Peer-reviewed studies published after 2006, involving adults with SCI living in countries with advanced economies, were included. Data were extracted from 24 articles and subjected to three-level thematic synthesis—the coding of primary data from the studies, the development of descriptive themes based on an organization of those codes, and the generation of analytical themes.
Results: The synthesis yielded five analytical themes, supported by 17 descriptive themes. The analytical themes were (1) external contextual influences, (2) personal physical context, (3) personal psychological context, (4) potential moderators of participation outcomes, and (5) temporal dimensions of participating in life after SCI.
Interpretation: These themes highlight the complex interactions that shape participation from the perspective of people with SCI. Closer examination of the potential moderators may provide insights into effective rehabilitation interventions.
Conclusions: Synthesis of qualitative inquiry provides valuable insights into the perceptions of influences on participation in life from the point of view of people with SCI. The findings of this synthesis are instructive for rehabilitation theory and practice. It can complement what we learn from using the ICF to understand participation.
Background
Participation is a dimension of human functioning, described in the World Health Organization's International Classification of Functioning, Disability and Health (ICF) as involvement in a life situation (1). Despite the simplicity of this definition, participation is recognized as a highly complex construct (2). The term participation is often used holistically to capture those aspects of human functioning that relate to socially defined tasks and roles (3, 4). This encompasses, but is not limited to, creating and maintaining interpersonal relationships, assisting or caring for others, undertaking education, working for remuneration or volunteering, partaking in recreation or leisure pursuits, and engaging in civic activities (1).
Participation is depicted in the ICF as one of the interactive components of functioning—along with body functions and structures, and activities. All components are subject to the impacts of heath conditions, environmental factors and personal factors (5). As such, the ICF reflects a biopsychosocial approach to understanding the multiple, complex, and dynamic influences on human functioning, in the presence of health disorders or disease (6).
When examining participation from the perspective of people with spinal cord injury (SCI), each individual's understanding of what is meant by the term is likely to differ based on personal experiences and context (7, 8). As well as being seen as a term for describing the regular roles and tasks of life, some people with SCI also equate participation with such things as sense of autonomy, having choices in life and experiencing societal inclusion (9). Conceptualizing and measuring participation are important steps toward defining clinical outcomes for people with spinal cord injury (SCI), however developing an understanding of what influences participation is likely to contribute directly to enabling them to attain these outcomes. Recognizing the influences on participation in life after SCI can also inform rehabilitation theory and practice (10).
The International Classification of Functioning, Disability and Health (ICF) is the pre-eminent taxonomy for describing human functioning (including participation in life situations) in the presence of health conditions (11). The potential influences on participation recognized by the ICF are extremely broad in scope—covering personal characteristics, environmental variables, and impairments of body structure and function. The ICF provides rehabilitation practitioners with a structure within which to assess the function of a person with SCI (5). However, while the ICF structure classifies key dimensions, it does not reveal the full breadth and complexity of influences on participation in life after SCI.
Qualitative inquiry provides a means of exploring influences on participation in life after SCI. While the ICF codifies barriers to and facilitators of participation, qualitative approaches can add additional nuance by revealing subjective meanings underlying the experiences, strategies, or perceptions of those with lived experience of SCI.
In 2018 we published a study about determinants of participation in life after SCI. These determinants were proposed after examination of the narratives of allies with SCI (12). That work was preceded by a comprehensive mapping exercise of both qualitative and quantitative literature about participation in life after SCI (13). The current article presents an up-to-date literature search (December, 2021) and thematic synthesis of one component of literature identified in that map, namely peer reviewed qualitative studies relating to, or describing, influences on participation in life after SCI. The purpose of this targeted search and thematic synthesis is to continue to build our understanding of the lived experience of participation in life after SCI, to further inform rehabilitation theory and practice.
Methods
Review Question
Our specific review question was (using the lens of published research): What do people with SCI perceive to be the influences on their participation in life? The spider approach (sample, phenomenon of interest, design, evaluation, and research type) was used to develop a search strategy to inform this question (14). The sample was people with SCI, the phenomenon of interest was participation in life, the design of studies was interviews or other methods which elicit personal perceptions, the construct under evaluation was influences on participation, and research type was qualitative.
Literature Search
A mapping approach to literature review facilitates a comprehensive overview of a body of literature, which can form the basis for targeted explorations to answer specific questions (15). The previous literature mapping exercise (13) informed the search strategy for the current review, with the addition of terms to narrow the search to articles about qualitative studies. CINAHL, Medline, and PsycInfo databases were searched using the search strings shown in Supplementary Material 1.
Articles considered within scope were those which described studies examining one or more influences on participation for people with adult-onset SCI, published between 2006 and 2021 (inclusive). Only peer reviewed journal articles that presented primary qualitative research were included. Articles presenting mixed methods work were included if the qualitative component reported direct quotations and clear paraphrasing of participant responses. Opinion pieces, editorials, and reviews were considered outside scope.
A risk in secondary analysis of qualitative data is de-contextualizing findings (16). Therefore, to optimize transferability across health and social care systems, our search was limited to studies conducted in countries with highly developed economies (17) with a predominant “Western” culture.
The searches yielded 522 unique articles. Article screening was managed using COVIDENCETM software. Two reviewers independently screened each article for relevance, by reviewing abstract and title. Contentious articles were discussed, until consensus was reached. The full texts of the remaining 110 articles were independently examined by two reviewers. Where reviewers were not in agreeance on inclusion, it was sent to a third reviewer for adjudication. Articles were excluded at this stage of screening if the studies they described either failed to examine influences on participation or made minimal mention of influences on participation and would thus have limited capacity to inform the synthesis.
Based on the overview provided by the mapping exercise, articles which primarily examined employment, recreation and leisure, or interpersonal relationships, rather than participation or community integration, were excluded. As the search strings did not explicitly include employment, recreation, and leisure or interpersonal relationships, this could not be considered a comprehensive literature search of these domains, so it was agreed to exclude them from the final list of articles for this current synthesis.
The tally of articles within the scope of the topic and relevant to the research question was 55. This comprised 23 primary articles with a general or exploratory approach to understanding participation and 32 secondary articles which had a particular focus or addressed a specific issue associated with participation (Figure 1). The decision was made to exclude these 32 secondary articles, since their focus was on specific topics such as the influence of aging, or physical activity or pain relief, which might confound the synthesis. However, a list of these articles and their attributes can be found in Supplementary Material 3.
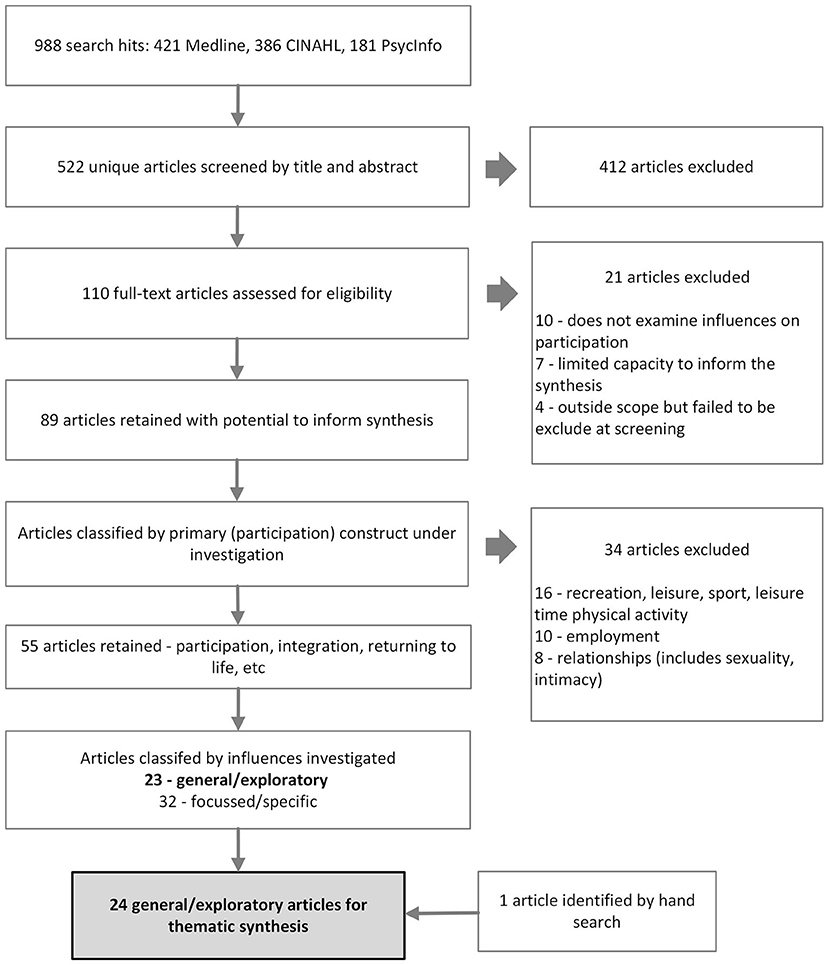
Figure 1. Process of literature search and screening.
Finally, hand searching of reference lists of the included articles was also undertaken. This resulted in one further article, taking the final tally to 24. The search, selection and screening process is summarized by Figure 1.
Study Attributes
Basic attributes were recorded for each of the 24 studies which met the inclusion criteria. Attributes included:
• Country in which the study was conducted
• Purpose of the study
• Data collection methods
• Method of data analysis
• Target demography (e.g., people with non-traumatic etiology)
• Number of participants
• Inclusion of participants other than people with SCI
Recognizing that formal quality appraisal of such studies is of limited value (16), we noted that restricting our synthesis to peer reviewed studies cataloged in the three principal databases for disability and rehabilitation literature was a suitable proxy for baseline quality.
Thematic Synthesis of Reported Data
The results sections of the primary studies (24 articles) categorized as general/exploratory, were distilled via the thematic synthesis approach of Thomas and Harden (16). To ensure precision and rigor of our synthesis, we considered only the Results section of studies as containing data for coding. Further, to remain as close as possible to the “voice” of people with SCI, we limited our analysis to direct quotes and instances of explicit paraphrasing from primary data. We avoided including interpretive content. Coding of units of meaning (most frequently sentences or paragraphs) was based on manifest content. Codes were often labeled using words or phrases from the studies themselves. All data were initially coded by one reviewer.
This approach had three stages: coding of all relevant direct quotes from the results sections of each of the studies; the development of descriptive themes based on organization of those codes; and the generation of analytical themes that propose new interpretations of the data. Descriptive themes emerged during the coding process and were refined at the conclusion of coding. Eighteen themes emerged after condensing similar codes and clustering related codes. Trustworthiness of coding and theme generation was determined by performing a backwards audit. This was conducted by two reviewers. They were tasked with checking themes against the original data set. They also assessed each theme for internal coherence, consistency, and distinctiveness (18). This backwards audit process resulted in collapsing two descriptive themes into one, renaming of one theme, a secondary search for data to support the continued inclusion of one theme, and the moving of some exemplar quotes between themes.
Finally, the remaining 17 descriptive themes were considered from an analytical or interpretive perspective with reference to the original research question. All reviewers participated in shaping the analytical themes.
Results
The studies described in 24 qualitative research articles were examined to inform the answer to the research question What do people with SCI perceive to be the influences on their participation in life? Articles were from Australia (n = 5), United States of America (n = 4), Belgium (n = 3), United Kingdom (n = 2), Canada (n = 2), Sweden (n = 2), as well as single articles from a variety of European countries. Study sample sizes ranged from one to 54 participants. The total number of participants across articles was 352. However, studies may be reported across multiple articles therefore each article may not represent a unique set of participants.
Semi-structured interviews with thematic analysis was the most frequent method of data collection and analysis. Table 1 provides a summary of the attributes of the studies described in the 24 articles. Details of the attributes of each study can be found in Supplementary Material 2.
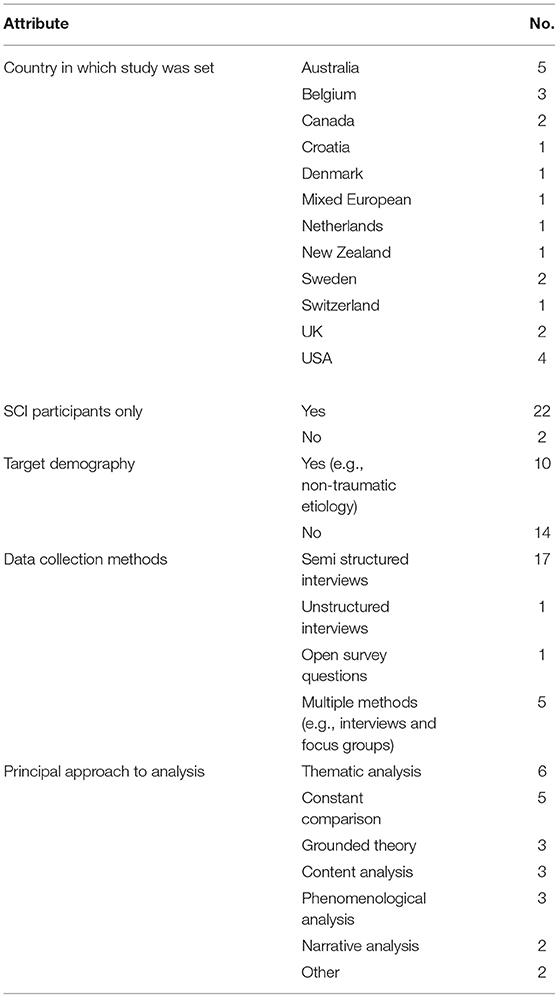
Table 1. Summary of attributes of articles in synthesis (n = 24).
The analysis resulted in the identification of 17 descriptive themes. Consideration of these themes with respect to the research question guided the creation of five overarching analytical themes. These analytical themes were (A) the external contextual influences, (B) the personal physical state, (C) the personal psychological state, (D) the potential moderators of participation outcomes, and (E) the temporal dimensions of participating in life after SCI. We labeled these analytical themes collectively as the interconnected elements that influence participation after SCI (see Figure 2).
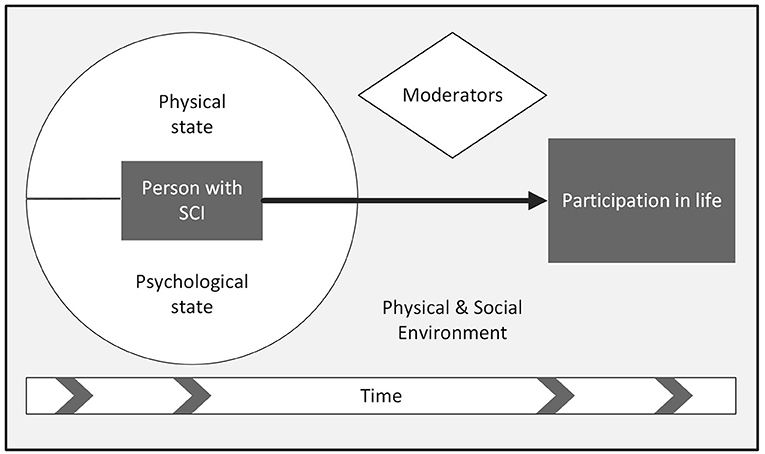
Figure 2. Interconnected elements that influence participation after SCI.
The External Contextual Influences
The first analytical theme, (A) external contextual influences, encompassed two descriptive themes—(A1) the physical environment will always pose challenges and (A2) society (people) can help or hinder. Representative quotes for each theme are presented in Table 2A.
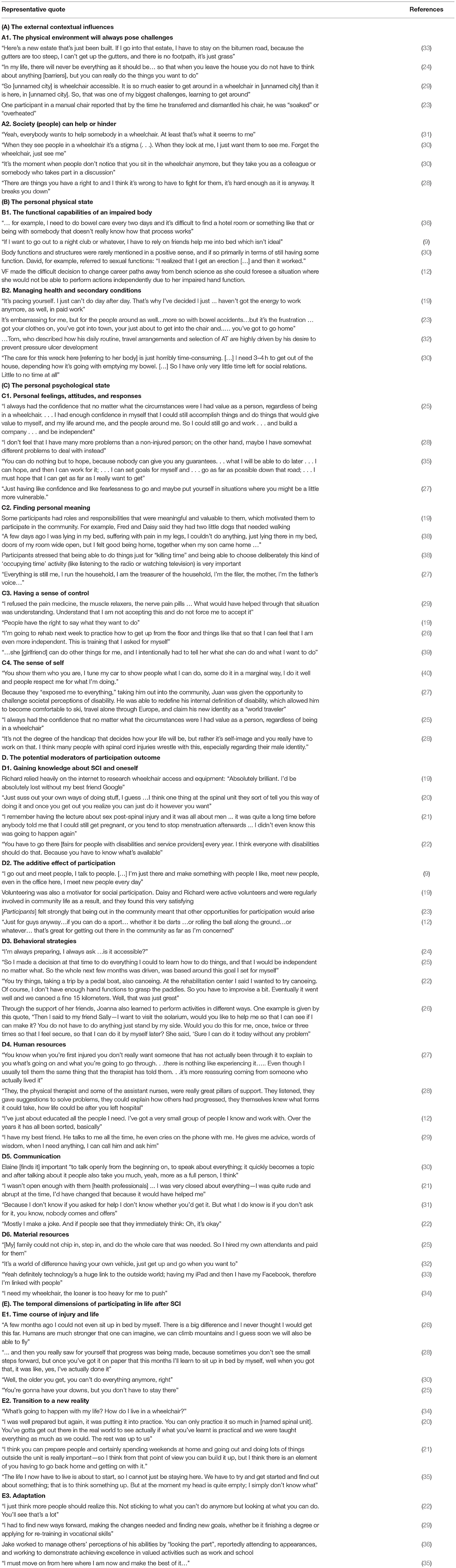
Table 2. Analytical themes and descriptive themes with representative quotes.
Although in many countries, progress is being made to improve access to built environments for people with mobility impairments, the physical environment will always pose challenges (9, 12, 19, 25, 27–30, 32, 33, 36, 37). There is an acceptance by some that accessibility will always be an issue despite advocacy and policy changes which can reduce barriers. As one participant noted, “In my life, there will never be everything as it should be… so that when you leave the house you do not have to think about anything [barriers], but you can really do the things you want to do” [(25), p. 415].
Individuals face different physical environmental challenges depending on where they live. Footpaths, curb cuts and other infrastructure will vary from one community to the next (19, 29) and the influence of prevailing weather and climatic conditions will vary (23, 32). Sense of physical safety was also mentioned (19, 27). Conversely, environmental challenges that seem to be ubiquitous are those related to transport—including accessible parking and public and private transport services, (26, 29, 32–34) and public bathroom facilities (12, 19, 22, 27, 29).
Across multiple studies, participants reported the need to be proactive to judge whether environmental barriers would be encountered when they ventured to new places (19, 22, 27, 30, 32, 36, 37). One participant described the effect on spontaneity, “…that you almost have to make a terrain assessment beforehand…where am I going, what are the conditions …if only I didn't need to do that” [(32), p. 189]. And being incorrectly advised on accessibility is always a risk (19, 32).
Society (people) can help and hinder the participation of people with SCI. As well as physical safety, participants reported a sense of emotional safety in their communities, related to familiarity and a sense of belonging (26, 38). While the support of others in the community is generally welcomed, data suggest that people with SCI would rather ask for help than have others offer it (12, 22, 32, 36). The quality of assistance when rendered may also be a problem (27, 37).
There is understandable sensitivity to what is viewed as condescending or thoughtless behaviors (25, 29, 31, 32). “Yeah, everybody wants to help somebody in a wheelchair,” said one participant [(30), p. 912], or “they're talking over you,” said another [(38), p. 470]. People with SCI describe a desire to be seen as “ordinary” and for the wheelchair to be of no consequence to others in society. “When they look at me I just want them to see me,” said one participant [(38), p. 470].
People with SCI may become worn down by issues of physical access and societal attitudes. This may lead some to constrain their activities, only visiting places that have proved accessible in the past (12, 19, 32), declining social invitations (23), and becoming bound to their own homes (36).
There is also a sense that people with SCI must contest bureaucracies to gain access to formal sources of funding and support. “There are things you have a right to and I think it's wrong to have to fight for them, it's hard enough as it is anyway. It breaks you down,” remarked a participant in relation to obtaining services [(32), p. 188]. The negative effect of “gatekeepers” was noted by participants across a number of studies (19, 25, 28, 32).
The Personal Physical State
The second analytical theme, (B) the personal physical state, comprised two descriptive themes—(B1) the functional capabilities of an impaired body, and (B2) managing health and secondary conditions. Representative quotes for each theme are presented in Table 2B.
Each individual's degree of impairment and functional capacity will influence their participation choices and the manner in which they participate (12, 20, 23, 29, 30, 33, 36, 38). Being able to transfer independently and/or drive a car are key examples of the direct impact on participation, and achieving certain levels of functional mobility (9, 30).
The perspective that people who sustain incomplete injuries and those who can walk “stand a chance” of achieving participation outcomes is held by some with SCI and doubtless more broadly in society (23). However, altered bladder, bowel, and sexual function (the hidden aspects of SCI) were described by some participants as profoundly impacting participation (12, 19, 22, 23, 29, 30, 36, 37).
Managing the SCI body is, for some, “horribly time consuming” [(27), p. 902] taking time away from participating in life (24). There is also a requirement for vigilance, particularly in relation to skin integrity. One participant stated, “pressure sore…it's at the back of my mind all the time” [(11), p. 7]. The secondary health conditions experienced by people with SCI—skin breakdown, incontinence, fatigue and persistent pain—are a significant impediment to participation (12, 19, 22, 23).
“It's embarrassing for me, but for the people around as well...more so with bowel accidents…but it's the frustration … got your clothes on, you've got into town, [you're] just about to get into the chair and..…you've got to go home,” said a participant [(24), p. 4].
The Personal Psychological State
The third analytical theme, (C) the personal psychological state was evident across four descriptive themes—(C1) personal feelings, attitudes, and responses (C2) finding personal meaning, (C3) having a sense of control, and (C4) the sense of self . Representative quotes for each theme are presented in Table 2C.
A great deal of the data found in these articles relates to the theme personal feelings and attitudes of participants toward participating in life with SCI. Feelings expressed ranged from embarrassed (19, 23, 31), frustrated (23, 25, 32, 36), and guilty (19, 31, 36, 37), to motivated (12, 19, 22, 25–27, 30, 33, 36), positive (21, 22, 25) and of value to others (25, 27, 35).
Attitudes that encompass flexibility of perspective and the capacity to reframe positively, were part of the psychological context that was linked with positive participation by some participants (22, 25, 27–30, 36, 37). Said one participant, “You have fun in a different way; you find other things, other means, and other ways to have fun” [(32), p. 188]. Closely aligned with flexibility and reframing is the need to frequently weigh up the costs and benefits of acts of participation (12, 23, 24, 27, 32, 36). “Some people have said I should go swimming, said one participant [(11), p. 7].” “But I couldn't be bothered…the time it would take.”
Positive feelings about participation in life are created for some through finding personal meaning. Common to some participants across studies was finding meaning through parenting or grandparenting (19, 27–29, 38), undertaking fulfilling employment (9, 12, 25, 36), studying or retraining (26, 29, 36), participating in sport (12, 27), or volunteering (9, 19, 37). For some, meaning was created through participation in activities that were not possible or expected before SCI. “I've been on the Board of Directors [of a housing initiative] for many years. That has been a very, very positive thing, you see. Something else that I never expected to do in my life either is be involved with boards. Like I said, it was probably out of my realm before” [(28), p. 1463].
Some participants expressed that they had found meaning through advocacy and activism (12, 25, 32). But meaning is not always derived in such an overt manner. More subtle ways of finding personal meaning were expressed through creating and maintaining a sense of connectedness and belonging (9, 24, 27, 31, 32, 38). Participants also clearly voiced their decisions NOT to engage in certain roles—employment (19, 23, 37) and sport (12–19, 33, 36, 37) being two examples evident in the data. Choosing to “kill time…[to] clear [the] mind” by completing puzzles or other “non-productive” and solitary pursuits is an important consideration in understanding perceptions of participation in life after SCI [(22), p. 351].
Finding personal meaning is closely linked in this data set with participants having a sense of personal control over their participation choices (9, 12, 20, 22, 26, 27, 30, 32, 36, 38, 39). Conversely, many participants expressed the negative impact on their sense of personal control wrought by physical dependency (9, 19, 20, 28, 30, 37), and feelings of insecurity (24, 26, 27, 31, 38). A participant likened this to a return to childhood that is “like you're a little kid again” having to let people know where you are going [(31), p. 1168].
Having a sense of autonomy in the way one participates in life is, to many, the very essence of participation. As one participant explained, “Organizing this barbeque became a part of my life…Some of the neighbors suggested to take over this task,…but I refused,…they can help me, that is no problem, but I will take the lead, just like I did last year and the years before” [(35), p. 5].
The final descriptive theme, grouped within analytical theme C, is the sense of self . Participation choices can be a direct result of participants enacting who they are, or who they have become since their SCI (21, 22, 25–28, 30, 36, 38, 39). “I've had jobs that I'm generally proud of …,” said one participant. “Those things have been image enhancing for me [(28), p. 1461].” And another said “You show them who you are, I tune my car to show people what I can do [(35), p. 650].”
Conversely one participant said, “…it was my life if I could fix the roof-gutter or clean the drive-way, this is how I'm conceived…what if I cannot longer…who the hell will I be [(35), p. 7]?” This disconnect between the sense of self and the limitation imposed by an impaired body is not impossible to reconcile for some. Participants described some specific examples—engaging with community activities in an organizational rather than physical capacity (25, 39), continuing to enjoy music despite not being able to play the instrument they had previously (38) or substituting new hobbies in place of old hobbies (22). Spirituality and religious beliefs were another form in which participants expressed an ongoing sense of self (22, 25). Being a good friend, someone others can count on, might also remain a constant despite SCI (27, 30).
The Potential Moderators of Participation Outcomes
The fourth analytical theme, (D) the potential moderators of participation outcomes, encompassed six descriptive themes—(D1) gaining knowledge about SCI and oneself , (D2) the additive effect of participation, (D3) behavioral strategies, (D4) human resources, (D5) communication, and (D6) material resources. Representative quotes for each theme are presented in Table 2D.
Gaining knowledge about SCI and oneself is a fundamental way in which people with SCI can give themselves the best possible platform for participation in life. This knowledge ranges across learning self-care routines and knowing how to reduce the incidence of secondary conditions (20, 22, 25, 26, 28, 29), knowledge of equipment and technology (12, 19, 22, 32, 33), hobbies and leisure options (12, 22, 25, 33), and understanding how to access sources of support and funding (19, 25, 32). Participants described receiving information and training during rehabilitation programs. Sometimes this was viewed positively and sometimes it was viewed as ill-timed or inadequate (20, 21, 28, 29). Much of the learning described by participants takes place separately from traditional rehabilitation through trial and error (22, 26), learning from peers (12, 21, 22, 25, 27–29, 32, 33, 37), and personal lived experience (22, 27, 32, 34). Rehabilitation was seen by one participant as “…preparing me to [leave] to a basic level” [(20), p. 538].
The second moderator of participation outcomes identified in the data, was the additive effect of participation (23). Engaging in sport and recreation (12, 22, 25, 30, 33), volunteering (19, 25, 37, 38), or doing paid work (9, 21, 25), were influential in opening up other opportunities for participants, including social participation (19, 27, 37). When it comes to participation in life, a progressive confidence can arise through trying and succeeding or failing and learning. “I have been thinking about finding some sort of job to start off…hopefully that might lead me to something else somewhere else…,” said one participant [(24), p. 5].
The two descriptive themes, behavioral strategies, and human resources were the two largest in terms of volume of data derived from the 24 articles. Participants described a number of behaviors they had adopted to improve their participation outcomes, including developing habits and routines (12, 26, 32, 35–37), being organized and planning ahead (19, 22, 24, 27, 28, 33, 36), setting goals and pushing oneself (13, 22, 25–27, 29, 35, 36), and embracing problem solving (12, 19, 22, 35). Exercising assertiveness when necessary (12, 19, 22, 25, 32) and, conversely, using techniques to put others at ease (12, 22, 27, 32) and engaging in reciprocity (12, 22, 26, 27), were examples of behavioral strategies employed when dealing with people.
Some of these behavioral strategies are not without personal cost. “I wish you were free to do what you want without needing to think,” said one participant in relation to the need for constant planning [(32), p. 189].
The impact which human resources have on the participation of a person with SCI cannot be overstated. First and possibly foremost is the participation leverage created by friends and family (9, 12, 19, 21, 22, 26–29, 32, 33, 36–38). “After I got out of the hospital they [friends and family] did help a lot. They'd help keep me motivated. Make sure I had things to do. And was not just sitting at home, sitting around,” said one participant [(29), p. 83]. And another remarked,“[Meeting my wife] totally changed my life . . . she's been the biggest impact on my life” [(28), p. 1,464]. But friends and family can also impede the participation of people with SCI. Said one participant, “Sometimes when she [mom] talks to me ... I'm having 14-year-old flash backs where she's trying to tell me what to do, and I'm like I'm 28 years old, a grown man” [(33), p. 1,504].
The camaraderie that may develop with peers was mentioned as important by many participants, and the value of talking with peer mentors who had been through similar experiences was highly valued (12, 19, 21, 22, 25, 27, 28, 31–33, 37). Health professionals could also be vital resources in the life of people with SCI (19, 27, 29, 33). In praise of her occupational therapist, one participant said “She really helped me. She actually took me down to the nursery [workplace] just to say hello to the people and help me feel comfortable” [(37), p. 583].
Unfortunately, some participants expressed the sentiment that they needed more from health professionals or felt let down in their interactions with professionals. Dissatisfaction stemmed from such things as not understanding the person as an individual (20, 21, 28), being treated with a lack of sensitivity and attention to emotional needs (21, 25, 29), or simply that health professionals lacked sufficient (flexibility of) time to spend with participants (21, 28, 31, 35).
Whether it be family and friends, peers, professionals, or organizations, participants saw value in having allies to “navigate” the challenges encountered when attempting to participate in life (34). As one participant stated, “…having somebody to at least guide you or show you ‘this is the way to go', not just a little binder that says how to do your bowels, how to go to the bathroom and watch out for pressure sores … what I am talking about is every day the more complex solutions that would [have] allowed us to figure things out…” [(36), p. 4].
Communication, the fifth descriptive theme within the potential moderators, is a life skill that takes on added importance for people with SCI. Participants recognized a benefit in “openness” in their communication style (12, 21, 26, 27, 30, 31), and displayed examples of the benefits of negotiation skills (27) and use of humor (12, 19, 22). For one participant, to feel safe and confident he needed to communicate explicitly with his partner and neighbors. “I wanted to know if my wife would take care of me, I wanted to know if the next-door neighbors could come over once in a while and see if I am alright that kind of stuff, can you see otherwise I would not feel safe” [(22), p. 352].
The final moderator evident in the data was material resources. Access to personal care support (19, 20, 23, 32), equipment and technology (12, 19, 23, 25, 29, 32–34), and transport (9, 23, 26, 29, 30, 32–34) were integral to participants' successful participation. “I get this electric wheelchair, suddenly I can go down the hallway and I can visit anybody ...,” is a simple statement that encapsulates the power of having the material resources required to participate [(30), p. 910]. Vital to gaining these material resources are adequate sources of funding, provided in a transparent and timely way (12, 19, 24, 25, 29, 30, 32–34, 36). In addition, specialized professional support helps people with SCI through the process of acquiring resources (19, 27, 33).
The Temporal Dimensions of Participating in Life After SCI
The fifth analytical theme, (E) the temporal dimensions of participating in life after SCI, evolved from three descriptive themes—(E1) the time course of injury and life, (E2) the transition to a new reality, and (E3) adaptation. Representative quotes for each theme are presented in Table 2E.
Participation will differ for people with SCI depending on where they are in the time course of injury and life (12, 20, 21, 23, 25–29, 33, 37). For example, a newly injured individual may have a relatively constrained view of their potential to participate in life after SCI. People will not have a full understanding of their participation possibilities. This sentiment was summed up by one participant. “The life I now have to live is about to start, so I cannot just be staying here. We have to try and get started and find out about something; that is to think something up. But . . . at the moment my head is quite empty; I simply don't know what” [(21), p.45].
“People aren't static [(11), p. 4].” People have ups and downs in life (12, 25). Their aspirations, abilities and circumstances will change throughout life. Age at time of injury, as well as the process of aging, are also factors which will influence participation choices and outcomes (30).
The descriptive theme, transition to a new reality speaks to both emotional and pragmatic processes that participants described as they are faced with the reality of SCI (20, 21, 25, 27–29, 34). Leaving a rehabilitation setting to confront the real world (12, 20), and leaving behind the physical and emotional safety (20, 31), speak to a very specific time of transition that is a challenging experience for many. One participant put it thus, “I just wanted to go back in hospital honestly and for somebody who was so keen to get out, I wanted to get back to my support group [(38), p. 467].”
The final descriptive theme, adaptation is a construct that speaks to mind shifts undertaken by people with SCI. Acknowledging change (21, 22, 25, 28, 32, 39, 40), displaying degrees of flexibility in choice making (12, 19, 25, 40) and “find new ways forward” [(36), p. 5] embody this theme.
Discussion
The aim of this thematic synthesis of qualitative research findings was to deepen understanding of the influences on people's participation in life after spinal cord injury. Using a process of thematic analysis and synthesis, the participant quotes drawn from 24 studies, comprising a total of 352 people with SCI from 12 countries, produced five analytical themes which encompass 17 descriptive themes. Considered together, we describe these analytical themes as the interconnected elements that influence participation after SCI.
The results of the thematic synthesis show the ubiquitous influences of the physical environment. Similarly, and unsurprising, is the evidence for the influence of the social environment, along with the health and physical function of individuals with SCI. These influences have featured prominently in much of the observational, quantitative research that has been conducted in this area (41–45).
Perhaps more important for advancing our understanding of the influences on participation, are the number of themes identified that relate to the individual's psychological state. Understanding the individual is acknowledged as important for providing person-centered care after SCI (46). However, extending this understanding of the individual to their inner psychological world—personal attitudes, personal meanings, how they understand control and autonomy, their sense of self and their inner resources, may be far deeper than most practitioners and support personnel would deliberately delve.
Psychotherapeutic interventions may be offered in some instances, principally to augment personal coping (47), however there may be far more scope for addressing each person's internal psychological context through positive psychological programs (48, 49). The interactive nature of personal meaning, sense of control and sense of self is, without doubt, extremely complex. Nonetheless, it may only be through first considering each construct individually that more holistic therapeutic interventions can arise.
The potential moderators of participation outcomes form a substantial portion of the findings of this review. All the moderators described are, to some degree, modifiable. Gaining the knowledge to manage one's body after SCI, and learning, practicing and using behavioral strategies, such as use of assertiveness, habit formation, pre-planning and socially positive communication, may be trainable, at least to some degree, for all with SCI. Involvement in activities to expand participation options (particularly social participation) is something that people with SCI can be supported to undertake—as long as it is individualized to their interests. There have been but a handful of programs touching on these aspects that have been evaluated and reported in the literature (50–55).
Participation outcomes after SCI are not just about what a person knows but who they know. People who sustain an SCI may or may not have a strong network of human resources at the time of injury. We know that some networks will break down while others will not. It would appear that those with robust networks may have a participation head start (56). When this is not the case, proactive measures to aid people to develop their networks of support are important (57).
Optimizing the material resources of equipment, technology, transport, and care support starts with (uncomplicated) access to appropriate levels of funding. However, getting the optimal material resources also rests on much more than just money. Information about, and access to, the latest equipment and technology, as well as professional support to make informed choices is critical (58–60). Similarly, the quality of support staff and their training will always be crucial for people with SCI to leverage the best participation outcomes.
Time is a crucial variable in participation outcomes. The temporal dimensions of participating in life after SCI have been highlighted in previous work on undergoing transitions (61–63), trajectories of outcomes (64, 65), and aging with SCI (66, 67).
Adaptation is the final temporal descriptive theme. The term psychosocial adjustment is the term commonly used in the past which is similar to adaptation (68). However, adaptation may be considered more holistic—encompassing physical adaptations, behavioral adaptations, shifts in mind set and post traumatic growth, all of which may be called on as each person with SCI finds their path through life.
Findings in Relation to Biopsychosocial Models Such as the ICF
It has not been the purpose of this synthesis to replace existing frameworks of understanding but to provide alternate ways through which to view the influences on participation for those with SCI. The results of this synthesis clearly affirm the biopsychosocial foundations of the lived experience of SCI. Though it was not the purpose of this review to use the ICF as a framework for thematic categorization, it is abundantly clear that the results would map strongly to its components. The external contextual influences correspond with the Environment component (physical and societal domains) of the ICF. The personal physical state closely aligns with the ICF components Body Structure and Function, Activities and Participation. The personal psychological state has some overlap with the Mental Functions described in Body Structure and Function but might also overlap with Personal Factors.
The potential moderators of participation outcomes would appear to cross bio, psycho and social elements of influence. Gaining knowledge about SCI and oneself are aspects of managing biological functions. Leveraging the additive effects of participation, and employing behavioral strategies are psychological tools for changing participation outcomes, and, access to human and material resources and communicating effectively are social moderators.
The temporal dimension of participating in life after SCI brings an aspect which is difficult to show in a framework such as the ICF. Classifications are recorded at snapshots in time, so a temporal dimension can be captured by repeating the classification process over time.
Implications for Service Provision
It goes without saying that assisting people to optimize their physical capacity will remain a mainstay of rehabilitation. This includes maintaining health and wellness and minimizing secondary complications of SCI. However, the continuing predominance of physical function interventions as the mainstay of rehabilitation therapies for people with SCI, coupled with the medical focus on symptom and bodily system based care (31), should perhaps be questioned.
Understanding the personal psychological context is something that is essential to person centered rehabilitation. It isn't just a matter of intervention when pathological states are diagnosed. It is about positively emphasizing existing psychological strengths and giving people opportunity to develop their capacities where challenges are identified.
There is a great deal of scope in rehabilitation programs for examining moderators and determining if they can be shaped through various interventions. Can the behavioral strategies demonstrated in this data be taught to people with SCI?
Friends and family as moderators of participation outcomes must be an integral part of the rehabilitation process. The power of peer led programs needs to be assessed and refined (69). Bringing together the expertise and perspectives of practitioners and peers may be the best way to optimize knowledge and information provision for people with SCI.
Rehabilitation institutions still tend to operate on models that are heavily weighted toward a single episode of primary rehabilitation (70). Service providers must recognize the evolving nature of each person's personal journey with SCI. Things change with time and services must be more fluid and less fixed. There is no fixed timetable for adaptation to SCI and people with SCI will experience episodic need for support (71). To provide contemporary person-centered rehabilitation services, we need to understand participation in life after SCI as a function of time.
Review Limitations
It is always difficult to put boundaries around the construct of participation. Consequently, the mapping and targeting of articles for this review has been very iterative in nature. Although this is consistent with a hermeneutic approach to literature review (72, 73) bias may be at play in decisions to include or reject certain lines of enquiry. By being as open as possible about each of the iterations, it is hoped that others can judge the merits of the decision making.
Narrowing the context to certain countries with highly developed economies and “western cultures” may be questionable as a strategy for creating homogeneity. The reality is these countries may be comprised of many multicultural communities, First Nations communities and rural and remote communities, all of which may create heterogeneity of experience for people with SCI. In addition, the funding and support structures for people with disability will be very different from one country to the next. As with all qualitative research, each reader must view the results with a degree of caution and reflect on the transferability of findings to differing contexts.
The decision to focus on quotes and paraphrases included in the final manuscript of primary articles may be contentious. Typically, in meta ethnography or qualitative meta synthesis, the entirety of the interpretations and conclusions in the articles would be considered as data (74). However, our interest was to hear the voice of the people with SCI which comes to the fore in these articles. Approaching the synthesis of these articles in a different manner may yield different insights.
We acknowledge that this synthesis relies on data which is weighted toward the early months and years after SCI. The lived experience of rehabilitation and transition to life in the community have understandably been a strong focus of scholarship, which may be compounded by a tendency for participants to re-explore this pivotal time in their lives when asked to describe their lived experiences, despite being many years post injury. While several longitudinal quantitative studies have examined long term outcomes, an important step forward from the current study would be deeper qualitative investigation of the life course experience of SCI.
We believe that to some extent the limitations of the current review are mitigated by the unique approach adopted. Having an overview of the views of 352 participants with SCI across 12 countries, and from a range of study contexts, has enabled us to gain valuable insights into key aspects of participation after SCI.
Next Steps
Our understanding of these interconnected elements that influence participation after SCI can be nuanced by examining the literature which is specific to particular participation constructs (e.g., employment, recreation etc). We can also learn more by examining the mechanism by which specific influences create participation outcomes (e.g., secondary conditions, peer mentoring).
The broad range and the relative priorities of factors identified in the current review provide a potential guide for future funding models and policy statements. In order to meaningfully boost the participation of people with SCI, policy settings and funding equations must recognize the breadth of factors involved and the relative importance of some factors (e.g., psychosocial wellbeing) over others. Most importantly, there is a need for development, evaluation and dissemination of programs that seek to harness these influences on participation.
Conclusion
Synthesis of qualitative inquiry provides valuable insights into the perceptions of influences on participation in life from the point of view of people with SCI. It provides a greater depth than relying on the ICF alone to understand participation. From this synthesis, we surmise that participation outcomes may be enhanced by greater emphasis in rehabilitation settings on understanding a person's psychological state. There also may be capacity to leverage the moderators of participation through specific interventions and programs to improve participation outcomes.
Author Contributions
DA and SS performed the database searches, article selection, and data extraction. DA performed the primary synthesis and created the first draft of this article. MK and PK validated the synthesis. SS, MK, and PK provided significant editing. All authors contributed to the design of this review, contributed to the article, and approved the submitted version.
Funding
Funding for open access publication of this manuscript was provided by the Metro South Health—Study, Education, and Research Trust Account (SERTA).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors acknowledge the previous efforts of the researchers and people with spinal cord injury, which provided the material for this synthesis.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fresc.2022.898143/full#supplementary-material
References
1. World Health Organization. Towards a Common Language for Functioning, Disability and Health. Geneva: WHO (2002).
2. Heinemann A, Lai J, Magasi S, Hammel J, Corrigan J, Bogner J, et al. Measuring participation enfranchisement. Arch Phys Med Rehabil. (2011) 92:564–71. doi: 10.1016/j.apmr.2010.07.220
3. Jette A, Haley S, Kooyoomjian J. Are the ICF activity and participation dimensions distinct? J Rehabil Med. (2003) 35:145–9. doi: 10.1080/16501970310010501
4. Whiteneck G, Dijkers M. Difficult to measure constructs: conceptual and methodological issues concerning participation and environmental factors. Arch Phys Med Rehabil. (2009) 90:S22–35. doi: 10.1016/j.apmr.2009.06.009
5. World Health Organization. How to Use the ICF: A Practical Manual for Using the International Classification of Functioning, Disability and Health (ICF). Geneva: Exposure Draft for Comment (2013).
6. Haslam SA, Haslam C, Jetten J, Cruwys T, Bentley SV. Rethinking the nature of the person at the heart of the biopsychosocial model: exploring social changeways not just personal pathways. Soc Sci Med. (2021) 272:113566. doi: 10.1016/j.socscimed.2020.113566
7. Hammel J, Magasi S, Heinemann A, Whiteneck G, Bogner J, Rodriguez E. What does participation mean? An insider perspective from people with disabilities. Disabil Rehabil. (2008) 30:1445–60. doi: 10.1080/09638280701625534
8. Noreau L, Fougeyrollas P, Post M, Asano M. Participation after spinal cord injury: the evolution of conceptualization and measurement. J Neurol Phys Ther. (2005) 29:147–56. doi: 10.1097/01.NPT.0000282247.15911.dc
9. Ruoranen K, Post MWM, Juvalta S, Reinhardt JD. Participation and integration from the perspective of persons with spinal cord injury from five European Countries. J Rehabil Med. (2015) 47:216–22. doi: 10.2340/16501977-1911
10. Gargaro J, Warren C, Boschen K. Perceived barriers and facilitators to community reintegration after spinal cord injury: a critical review of the literature. Crit Rev Phys Rehabil Med. (2013) 25:101–41. doi: 10.1615/critrevphysrehabilmed.2013007021
11. Stucki G. International Classification of Functioning, Disability, and Health (ICF): a promising framework and classification for rehabilitation medicine. Am J Phys Med Rehabil. (2005) 84:733–40. doi: 10.1097/01.phm.0000179521.70639.83
12. Amsters D, Duncan J, Field V, Smales A, Zillmann L, Kendall M, et al. Determinants of participating in life after spinal cord injury – advice for health professionals arising from an examination of shared narratives. Disabil Rehabil. (2018) 40:3030–40. doi: 10.1080/09638288.2017.1367425
13. Amsters D. What are the Determinants of Participation in Life for People With Spinal Cord Injury, how Might a Knowledge of These Determinants Enhance Rehabilitation? Griffith University (2020). Available online at: https://go.exlibris.link/gxvbr31k
14. Cooke A, Smith D, Booth A. Beyond pico: the spider tool for qualitative evidence synthesis. Qual Health Res. (2012) 22:1435–43. doi: 10.1177/1049732312452938
15. Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, et al. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews. ESRM Methods Programme (2006). Available online at: https://www.Researchgate.net/Profile/Mark_Rodgers4/Publication/233866356_Guidance_on_the_Conduct_of_Narrative_Synthesis_in_Systematic_Reviews_A_Product_From_the_ESRC_Methods_Programme/Links/02e7e5231e8f3a6183000000.pdf (accessed June 22, 2015).
16. Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. (2008) 8:e45. doi: 10.1186/1471-2288-8-45
17. United Nations Development Programme. Human Development Indices and Indicators – 2018 Statistical Update. New York, NY: United Nations Development Programme (2018).
18. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
19. Barclay L, Lentin P, McDonald R, Bourke-Taylor H. Understanding the factors that influence social and community participation as perceived by people with non-Traumatic spinal cord injury. Br J Occup Ther. (2017) 80:577–86. doi: 10.1177/0308022617713699
20. Nunnerley J, Hay-Smith E, Dean S. Leaving a spinal unit and returning to the wider community: an interpretative phenomenological analysis. Disabil Rehabil. (2013) 35:1164–73. doi: 10.3109/09638288.2012.723789
21. Suddick K, O'Neill A. Reintegration and rehabilitation after spinal cord injury: a small-scale pilot study. Int J Ther Rehabil. (2009) 16:535–44. doi: 10.12968/ijtr.2009.16.10.44563
22. van de Ven L, Post M, de Witte L, van den Heuvel W. Strategies for autonomy used by people with cervical spinal cord injury: a qualitative study. Disabil Rehabil. (2008) 30:249–60. doi: 10.1080/09638280701265687
23. Carr J, Kendall M, Amsters D, Pershouse K, Kuipers P, Buettner P, et al. Community participation for individuals with spinal cord injury living in Queensland, Australia. Spinal Cord. (2017) 55:192–7. doi: 10.1038/sc.2016.169
24. Bartolac A, Jokic CS. Understanding the everyday experience of persons with physical disabilities: building a model of social and occupational participation. J Occup Sci. (2019) 26:408–25. doi: 10.1080/14427591.2018.1522597
25. Weitzner E, Surca S, Wiese S, Dion A, Roussos Z, Renwick R, et al. Getting on with life: positive experiences of living with a spinal cord injury. Qual Health Res. (2011) 21:1455–68. doi: 10.1177/1049732311417726
26. Isaksson G, Prellwitz M. One woman's story about her everyday life after a spinal cord injury. Disabil Rehabil Int Multidiscip J. (2010) 32:1376–86. doi: 10.3109/09638280903514762
27. Price P, Stephenson S, Krantz L, Ward K. Beyond my front door: the occupational and social participation of adults with spinal cord injury. OTJR Occup Particip Health. (2011) 31:81–8. doi: 10.3928/15394492-20100521-01
28. Sand Å, Karlberg I, Kreuter M. Spinal cord injured persons' conceptions of hospital care, rehabilitation, and a new life situation. Scand J Occup Ther. (2006) 13:183–92. doi: 10.1080/11038120500542187
29. Hall AG, Karabukayeva A, Rainey C, Kelly RJ, Patterson J, Wade J, et al. Perspectives on life following a traumatic spinal cord injury. Disabil Health J. (2021) 14:101067. doi: 10.1016/j.dhjo.2021.101067
30. Reinhardt J, Ruoranen K, Graf S, Horsewell J, Leiulfsrud A, Post M. ‘It takes two to tango …' revisited: a qualitative study on integration and participation of people living with spinal cord injury in Switzerland. Disabil Soc. (2013) 28:893–907. doi: 10.1080/09687599.2012.732536
31. Dickson A, Ward R, O'Brien G, Allan D, O'Carroll R. Difficulties adjusting to post-discharge life following a spinal cord injury: an interpretative phenomenological analysis. Psychol Health Med. (2011) 16:463–74. doi: 10.1080/13548506.2011.555769
32. Ripat J, Woodgate R. Self-perceived participation among adults with spinal cord injury: a grounded theory Study. Spinal Cord. (2012) 50:908–14. doi: 10.1038/sc.2012.77
33. Barclay L, McDonald R, Lentin P, Bourke-Taylor H. Facilitators and barriers to social and community participation following spinal cord injury. Aust Occup Ther J. (2016) 63:19–28. doi: 10.1111/1440-1630.12241
34. Silver J, Ljungberg I, Libin A, Groah S. Barriers for individuals with spinal cord injury returning to the community: a preliminary classification. Disabil Health J. (2012) 5:190–6. doi: 10.1016/j.dhjo.2012.03.005
35. Angel S, Kirkevold M, Pedersen BD. Getting on with life following a spinal cord injury: regaining meaning through six phases. Int J Qual Stud Health Wellbeing. (2009) 4:39–50. doi: 10.1080/17482620802393492
36. Fritz H, Lysack C, Luborsky M, Messinger S. Long-term community reintegration: concepts, outcomes and dilemmas in the case of a military service member with a spinal cord injury. Disabil Rehabil. (2015) 37:1501–7. doi: 10.3109/09638288.2014.967415
37. Barclay L, Lentin P, Bourke-Taylor H, McDonald R. The experiences of social and community participation of people with non-traumatic spinal cord injury. Aust Occup Ther J. (2019) 66:1–67. doi: 10.1111/1440-1630.12522
38. van de Velde D, Bracke P, van Hove G, Josephsson S, Vanderstraeten G. Perceived participation, experiences from persons with spinal cord injury in their transition period from hospital to home. Int J Rehabil Res. (2010) 33:346–55. doi: 10.1097/MRR.0b013e32833cdf2a
39. van de Velde D, Bracke P, Van Hove G, Josephsson S, Devisch I, Vanderstraeten G. The illusion and the paradox of being autonomous, experiences from persons with spinal cord injury in their transition period from hospital to home. Disabil Rehabil Int Multidiscip J. (2012) 34:491–502. doi: 10.3109/09638288.2011.608149
40. Van de Velde D, Bracke P, Van Hove G, Josephsson S, Vanderstraeten G. How do men with paraplegia choose activities in the light of striving for optimal participation? a qualitative study, based on a phenomenological–hermeneutical. Method Disabil Soc. (2013) 28:645–59. doi: 10.1080/09687599.2012.728795
41. Gross-Hemmi M, Post M, Bienert S, Chamberlain J, Hug K, Jordan X, et al. Participation in people living with spinal cord injury in switzerland: degree and associated factors. Arch Phys Med Rehabil. (2019) 100:1894–906. doi: 10.1016/j.apmr.2019.03.018
42. Ullrich P, Spungen A, Atkinson D, Bombardier C, Chen Y, Erosa N, et al. Activity and participation after spinal cord injury: state-of-the-art report. J Rehabil Res Dev. (2012) 49:155–74. doi: 10.1682/JRRD.2010.06.0108
43. Reinhardt J, Post M. Measurement and evidence of environmental determinants of participation in spinal cord injury: a systematic review of the literature. Top Spinal Cord Inj Rehabil. (2010) 15:26–48. doi: 10.1310/sci1504-26
44. Noreau L, Boschen K. Intersection of participation and environmental factors: a complex interactive process. Arch Phys Med Rehabil. (2010) 91:S44–53. doi: 10.1016/j.apmr.2009.10.037
45. Whiteneck G, Meade M, Dijkers M, Tate D, Bushnik T, Forchheimer M. Environmental factors and their role in participation and life satisfaction after spinal cord injury. Arch Phys Med Rehabil. (2004) 85:1793–803. doi: 10.1016/j.apmr.2004.04.024
46. Jesus TS, Papadimitriou C, Bright FA, Kayes NM, Pinho CS, Cott CA. The person-centered rehabilitation model: framing the concept and practice of person-centered adult physical rehabilitation based on a scoping review and thematic analysis of the literature. Arch Phys Med Rehabil. (2022) 103:106-20. doi: 10.1016/j.apmr.2021.07.465
47. Heinemann A, Wilson C, Huston T, Koval J, Gordon S, Gassaway J, et al. Relationship of psychology inpatient rehabilitation services and patient characteristics to outcomes following spinal cord injury: the scirehab project. J Spinal Cord Med. (2012) 35:578–92. doi: 10.1179/2045772312Y.0000000059
48. Chan J, Chan F, Ditchman N, Phillips B, Chou C. Evaluating snyder's hope theory as a motivational model of participation and life satisfaction for individuals with spinal cord injury: a path analysis. Rehabil Res Policy Educ. (2013) 27:171–85. doi: 10.1891/2168-6653.27.3.171
49. Umucu E, Lee B, Wu J, Chan F, Blake J, Brooks J, et al. Self-efficacy as a mediator for the relationship between secure attachment style and employment status in individuals with spinal cord injuries. J Vocat Rehabil. (2016) 45:97–106. doi: 10.3233/JVR-160814
50. Ekelman BA, Allison DL, Duvnjak D, DiMarino DR, Jodzio J, Iannarelli PV, et al. Wellness program for men with spinal cord injury: participation and meaning. OTJR Occup Particip Health. (2017) 37:30–9. doi: 10.1177/1539449216672170
51. Zinman A, Digout N, Bain P, Haycock S, Hébert D, Hitzig SL. Evaluation of a community reintegration outpatient program service for community-dwelling persons with spinal cord injury. Rehabil Res Pract. (2014) 2014:989025. doi: 10.1155/2014/989025
52. Kolakowsky-Hayner S, Wright J, Shem K, Medel R, Duong T. An effective community-based mentoring program for return to work and school after brain and spinal cord injury. NeuroRehabilitation. (2012) 31:63–73. doi: 10.3233/NRE-2012-0775
53. Bocarro J, Sable J. Finding the Right PATH: exploring familial relationships and the role of a community tr program in the initial years after a spinal cord injury. Ther Recreation J. (2003) 37:58–72.
54. Hough S, Stone M, Buse D. Dating and relationship psychoeducational group for veterans with spinal cord injury/dysfunction: a historical account of an initial clinical course. Sex Disabil. (2013) 31:337–59. doi: 10.1007/s11195-013-9330-8
55. Barclay L, Robins L, Migliorini C, Lalor A. Community integration programs and interventions for people with spinal cord injury: a scoping review. Disabil Rehabil. (2021) 43:3845–55. doi: 10.1080/09638288.2020.1749889
56. Müller R, Peter C, Cieza A, Geyh S. The role of social support and social skills in people with spinal cord injury-a systematic review of the literature. Spinal Cord. (2012) 50:94–106. doi: 10.1038/sc.2011.116
57. Ward K, Mitchell J, Price P. Occupation-based practice and its relationship to social and occupational participation in adults with spinal cord injury. OTJR Occup Particip Health. (2007) 27:149–56. doi: 10.1177/153944920702700405
58. Gallagher A, Cleary G, Clifford A, McKee J, O'Farrell K, Gowran RJ. ‘Unknown world of wheelchairs' a mixed methods study exploring experiences of wheelchair and seating assistive technology provision for people with spinal cord injury in an irish context. Disabil Rehabil. (2020) 24:1–13. doi: 10.1080/09638288.2020.1814879
59. Dwyer K, Mulligan H. Community reintegration following spinal cord injury: insights for health professionals in community rehabilitation services in New Zealand. NZJ Physiother. (2015) 43:75–85. doi: 10.15619/NZJP/43.3.02
60. Myburg M, Allan E, Nalder E, Schuurs S, Amsters D. Environmental control systems – the experiences of people with spinal cord injury and the implications for prescribers. Disabil Rehabil Assist Technol. (2015) 22:1–9. doi: 10.3109/17483107.2015.1099748
61. Bourke J, Nunnerley J, Sullivan M, Derrett S. Relationships and the transition from spinal units to community for people with a first spinal cord injury: a New Zealand qualitative study. Disabil Health J. (2019) 12:257–62. doi: 10.1016/j.dhjo.2018.09.001
62. Wallace M, Kendall M. Transitional rehabilitation goals for people with spinal cord injury: looking beyond the hospital walls. Disabil Rehabil. (2014) 36:642–50. doi: 10.3109/09638288.2013.805259
63. Kendall MB, Ungerer G, Dorsett P. Bridging the gap: transitional rehabilitation services for people with spinal cord injury. Disabil Rehabil. (2003) 25:1008–15. doi: 10.1080/0963828031000122285
64. de Ruijter L, de Groot S, Adriaansen J, Smit C, Post M. Associations between time since onset of injury and participation in dutch people with long-term spinal cord injury. Spinal Cord. (2018) 56:1134–43. doi: 10.1038/s41393-018-0134-7
65. Barker R, Kendall M, Amsters D, Pershouse K, Haines T, Kuipers P. The relationship between quality of life and disability across the lifespan for people with spinal cord injury. Spinal Cord. (2009) 47:149–55. doi: 10.1038/sc.2008.82
66. Krause JS, Clark JMR, Saunders LL. SCI longitudinal aging study: 40 years of research. Top Spinal Cord Inj Rehabil. (2015) 21:189–200. doi: 10.1310/sci2103-189
67. Kern SB, Hunter LN, Sims AC, Berzins D, Riekena H, Andrews ML, et al. Understanding the changing health care needs of individuals aging with spinal cord injury. Top Spinal Cord Inj Rehabil. (2019) 25:62–73. doi: 10.1310/sci2501-62
68. Chevalier Z, Kennedy P, Sherlock O. Spinal cord injury, coping and psychological adjustment: a literature review. Spinal Cord. (2009) 47:778–82. doi: 10.1038/sc.2009.60
69. Barclay L, Hilton GM A. Scoping review of peer-led interventions following spinal cord injury. Spinal Cord. (2019) 57:626–35. doi: 10.1038/s41393-019-0297-x
70. Barclay L, Lalor A, Migliorini C, Robins L. A comparative examination of models of service delivery intended to support community integration in the immediate period following inpatient rehabilitation for spinal cord injury. Spinal Cord. (2020) 58:528–36. doi: 10.1038/s41393-019-0394-x
71. Kuipers P, Pershouse K, Amsters D, Price G. Long-term adjustment to spinal cord injury: partial support for an episodic stress response model and implications for outcome measurement. SCI Psychosoc Process. (2004) 17:65–78.
72. Boell S, Cecez-Kecmanovic D. Literature reviews and the hermeneutic circle. Aust Acad Res Libr. (2010) 41:129–44. doi: 10.1080/00048623.2010.10721450
73. Greenhalgh T, Thorne S, Malterud K. Time to challenge the spurious hierarchy of systematic over narrative reviews? Eur J Clin Invest. (2018) 48:E12931. doi: 10.1111/eci.12931
Keywords: spinal cord injury, participation, community integration, qualitative inquiry, literature review, thematic synthesis, rehabilitation theory
Citation: Amsters D, Kendall M, Schuurs S and Kuipers P (2022) Influences on Participation in Life After Spinal Cord Injury: Qualitative Inquiry Reveals Interaction of Context and Moderators. Front. Rehabilit. Sci. 3:898143. doi: 10.3389/fresc.2022.898143
Received: 17 March 2022; Accepted: 02 May 2022;
Published: 31 May 2022.
Edited by:
Feng-Hang Chang, Taipei Medical University, TaiwanReviewed by:
Monika Elisabeth Finger, Swiss Paraplegic Research, SwitzerlandZhuoying Qiu, China Rehabilitation Research Center/WHO Collaborating Center for Family International Classifications, China
Copyright © 2022 Amsters, Kendall, Schuurs and Kuipers. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Delena Amsters, Delena.amsters@health.qld.gov.au