
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
POLICY AND PRACTICE REVIEWS article
Front. Rehabil. Sci. , 03 May 2022
Sec. Strengthening Rehabilitation in Health Systems
Volume 3 - 2022 | https://doi.org/10.3389/fresc.2022.873436
This article is part of the Research Topic Pursuing quality education in Physical and Rehabilitation Medicine View all 11 articles
 Ana Maria Posada-Borrero*
Ana Maria Posada-Borrero* Daniel Felipe Patiño-Lugo
Daniel Felipe Patiño-Lugo Jesus Alberto Plata-Contreras
Jesus Alberto Plata-Contreras Juan Carlos Velasquez-Correa
Juan Carlos Velasquez-Correa Luz Helena Lugo-Agudelo
Luz Helena Lugo-AgudeloBackground and Aim: Knowledge translation processes are necessary for improving patients' and communities' health outcomes. The aim of this study was to systematically develop evidence-based recommendations for people over 16 years of age who are in risk for or have suffered a lower limb amputation for medical reasons (vascular, diabetes mellitus) or trauma (civilian or military trauma) in order to improve function, quality of life, decrease complications and morbidity.
Methods: Following the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach we developed a Clinical Practice Guideline (CPG) for lower limb amputees with funding from the Ministry of Health in Colombia and participation of a multidisciplinary group. We included patients' preferences. Based on the scope, purposes and objectives the questions were elaborated with the PECOT strategy. The evidence search was performed for each question in the main databases: Cochrane Library, Embase and PubMed, without time limit or language restriction. Teams were formed with thematic experts and clinical epidemiologists to review the clinical studies, describe the evidence, and evaluate the quality of the body of evidence with the GRADE methodology. The recommendations were made according to the judgments proposed by the GRADE working group. We conducted a stakeholder's dialogue as a mechanism for the external validation of the guideline implementation.
Results: The CPG included 43 recommendations related to the diagnosis, surgical treatment, rehabilitation, prescription and adaptation of the prosthesis. They were strong in favor 37.2, weak in favor 53.5, strong against 2.3, Weak against 7.0%. Quality of evidence was high in 0, moderate in 11.6, low in 58.1, and very low 30.2%.
Discussion: In 93% of the recommendations, the quality of the evidence was between low and very low. This is why it was so important to validate and discuss each recommendation with an expanded multidisciplinary group. The research group identified 25 interventions and five milestones to be prioritized in the implementation and in the stakeholder's dialogue participants identified opportunities and barriers for implementation of recommendations.
Conclusion: It is necessary to develop a national policy for implementation strategies of CPG recommendations that promotes the necessary arrangements for the provision of services for diagnosis, treatment, and rehabilitation of individuals with amputations.
Evidence-based clinical practice guidelines (CPG) are a fundamental tool for reforming medical care and strengthening health systems to achieve better health outcomes for patients and their communities (1, 2). However, despite the rigorous systematic synthesis of the scientific evidence contained in high-quality CPG, not all of them can be easily and directly translated into practice (3, 4).
In 2008, the Colombian Ministry of Health and Social Protection (MoH), financed the development of the methodological guideline for the development of evidence-based CPG in Colombia, this guideline was updated in the year 2014 (5). Between 2008 and 2016, the MoH in Colombia financed and convened the elaboration of 58 national CPG that were elaborated with the best methodological standards, by professionals from recognized universities in Colombia, with the participation of scientific associations, healthcare professionals and patients and caregivers. The purpose was to reduce unjustified variability in medical practice, improve the efficient management of resources, and be able to offer patients the most effective and safest interventions (6). A CPG implementation manual was also developed, with general suggestions about how to implement these CPGs in the different healthcare provider institutions (7).
In 2013, through a call of the Administrative Department of Science, Technology and Innovation (nowadays Minciencias) and financed by the MoH, we developed the “Clinical Practice Guideline for diagnosis and preoperative, intraoperative and postoperative treatment of the amputee, the prescription of the prosthesis and comprehensive rehabilitation” (8). An interdisciplinary group involved in the care of amputee patients from different cities in Colombia participated in its preparation. This guideline was updated in 2018.
One of the most consistent findings of clinical and health services research is the challenge to translate research evidence into practice (1). This have been reported around the world in different income level countries and in different sectors of care, such as primary or specialty care (1).
The US National Center for Dissemination Research on Disability defines knowledge transfer as “The collaborative and systematic review, evaluation, identification, aggregation, and practical application of high-quality research on disability and rehabilitation by key stakeholders, in order to improve the lives of people with disabilities” (9). This definition recognizes that there is a wide range of stakeholders for knowledge transfer, including policy makers; health providers; end users, researchers and industry. It is important that these transfer processes are implemented, especially in low and middle-income countries, strengthening the rehabilitation of people with disabilities.
The aim of this study was to systematically develop evidence-based recommendations for people over 16 years of age who are in risk for or have suffered a lower limb amputation for medical reasons (vascular, diabetes mellitus) or trauma (civilian or military trauma) in order to improve function, quality of life, decrease complications and morbidity.
The main guideline developer group consisted of 14 people, including physicians, physiatrists, orthopedists, vascular surgeons, experts in prosthetics, psychiatrists, physiotherapists, occupational therapists, clinical epidemiologists, public health doctors, economists, a documentary librarian, and undergraduate and postgraduate students. A group of professionals from different universities and scientific societies validated the different stages of the process. A focus group of 24 people with amputations of different causes and their relatives were linked to the process in two moments, when the questions were chosen and at the end of the recommendations. The developer group received a training process with different international centers as the McMaster University, the National Institute for Health and Clinical Excellence (NICE) and the New Zealand Guidelines Group. The users of the CPG are all the professionals who were involved in the development: surgeons, physiatrists, other professionals in the area of rehabilitation, insurers, health providers and political decision makers.
All the professionals who participated in the development made a declaration of interests at the beginning and each year. These are published as supplementary files within the CPG document (8).
The financing entity was the Ministry of Health and Social Protection, none of the people from this entity participated in the group developing the CPG. The Ministry carried out permanent monitoring to guarantee compliance with the methodology and schedules.
CPG for lower limb amputees were searched for, and an evaluation of quality was made with the AGREE II Instrument. Six CPG were evaluated independently by two professionals from the group. Only three with a score greater than 60 in the methodological domain were selected, which were used as information during development. (8).
The development of the CPG followed the GRADE (Grading of Recommendations Assessment, Development and Evaluation) methodology (10, 11). For the elaboration of the recommendations of the CPG, within the guideline development group (GDG), a process of prioritization of the topics of interest was carried out and the most important were selected. Subsequently, clinical questions were formulated and a systematic review of the available evidence was made on each one. This process was done between 2014 and 2015. The main recommendations were updated in 2018.
Based on the scope, purposes and objectives of the guideline, the questions were elaborated with the PECOT strategy (Population, Exposure or intervention, Comparison, Outcomes and Time). Then the developer group and the patients independently rated the importance of each outcome from 1 to 9, according to the GRADE classification (11). According to the average scores of the developer group, the outcomes were classified as: critical (7-9), important non-critical (4-6) or not important (1-3). The evaluation of the quality of the body of evidence is done by selecting the critical and important outcomes.
For each question, a list of MeSH terms was prepared according to the population, the intervention and the comparison. The evidence search was performed in the main databases: Cochrane Library, Embase and PubMed, and in secondary databases such as Lilacs/Bireme, Current Controlled Trials, TripDatabase and Google Scholar. There was no language restriction. For the selection of the evidence, inclusion criteria were established with respect to the methodological design, the population and the minimum quality characteristics. Systematic reviews and meta-analyses (secondary or aggregative studies), which analyzed primary studies related to the question, were initially sought. Additionally, clinical trials and observational studies were identified.
The quality of the evidence was evaluated for systematic reviews and meta-analyses with the AMSTAR (12); for diagnostic studies the QUADAS (13); and with the STROBE for observational studies (14). The quality of the body of evidence was assessed according to the concepts of the GRADE methodology (11), by qualifying each outcome. This process was done by orthopedic doctors, physiatrists, and clinical epidemiologists, who were experts in the GRADE methodology. GRADE publications can be accessed on the website https://www.gradeworkinggroup.org/.
Systematic reviews of clinical trials start with high quality (level 1), while reviews of observational studies start with low quality (level 4). The aspects that can lower the quality of a randomized controlled trial are: Risk of bias, inconsistency of the results, indirect evidence, imprecision of the results and publication bias. Observational studies, although they can lower quality with the aforementioned aspects, also they can increase it if they include some favorable methodological aspects. The three aspects that can increase the quality of are the presence of a large effect size (Relative Risk, >2.0 or <0.5); evidence of a gradient dose-response relationship and the absence of residual bias or confounding factors (15–20).
The quality of the evidence is related to the confidence that the true effect is close to the estimated effect. Four levels are defined: very low, low, moderate and high (11). Most of the quality of the evidence for this guideline was low or very low quality of evidence.
Following the GRADE system, the elaboration of the recommendations does not only take into account the quality of the evidence, but also a series of aspects or judgments based on the following criteria: The priority of the problem, the magnitude of the desirable and undesirable effects, the certainty of the evidence, the values of the interested parties, the balance between desirable and undesirable effects, the resources required, the cost-effectiveness, equity, acceptability and feasibility. With these criteria, a summary table of judgments was created and the direction and strength of the recommendation were defined (21). The strength of the recommendations is rated in four categories: Strong (recommended to do), weak in favor (suggested to do), strong against (recommended not to do), weak against (suggested not to do) (21). During face-to-face sessions with the entire guideline development group, the evidence for each question, the quality of the body of evidence, and the judgments were presented. With the foregoing, a recommendation was drawn up that was subsequently validated by an extended group with thematic experts and representatives of scientific societies and universities.
Five economic evaluations were made during the development of the CPG to assess the cost-effectiveness of five of the interventions and help the guideline development group in the decision-making.
In the development of a CPG, it is recommended including the perspective of the patients for the preparation of the recommendations. Thus, people with lower limb amputation were invited to define their priorities in three categories: complications, activities and prosthetic adaptation; using the GRADE methodology. In addition, their preferences of the treatment options in the recommendations with greater uncertainty and with low quality of evidence were evaluated.
Between July and November 2014, people with amputation in two institutions that provide health services in two cities of the country were invited. The inclusion criteria were people from 18 to 65 years old, who had a major lower limb amputation of any level and cause and who could attend a meeting with the researchers. Children and upper limb amputees were excluded. A convenience sampling was used, with the people who responded to the call. The objectives of the CPG and their participation, the instruments that were applied and doubts were resolved were explained at the meeting. In the group of 20 patients studied in one of the cities, the preferences of the CPG questions in which there was greater uncertainty at the time of presentation of the evidence synthesis were also evaluated.
One search strategy is presented as an example in Table 1, for one of the surgical recommendations, elaborated during the updating of the CPG. All the other search strategies can be consulted in the complete document of the CPG (8).
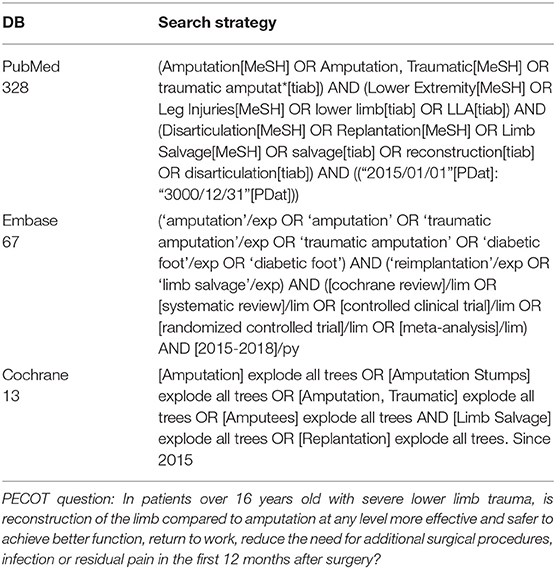
Table 1. Example of the search strategy and results in data bases for one of the CPG questions in the 2018 update.
Forty-three recommendations were made. Nine on the decision of amputation; five on preoperative interventions including: preoperative regional analgesia, cardiovascular reconditioning, psychological support, prophylactic antibiotics, and intraoperative tourniquet use; ten on amputation techniques; ten on the components of the prosthesis, feet, knees, sockets, liners, as well as orthoses for partial amputation and the adaptation of immediate postoperative prostheses. Nine for the post-prosthetic phase, including functioning scales to evaluate the use of prostheses; treatment for neuropathic and phantom limb pain; cardiopulmonary, physical and occupational rehabilitation; ergonomic adaptations and psychosocial interventions. Comprehensive rehabilitation compared to the usual care model was also evaluated and this was a strong recommendation in favor. The synthesis of the quality of the evidence and the strength of the recommendations can be seen in Table 2, and Figures 1, 2.
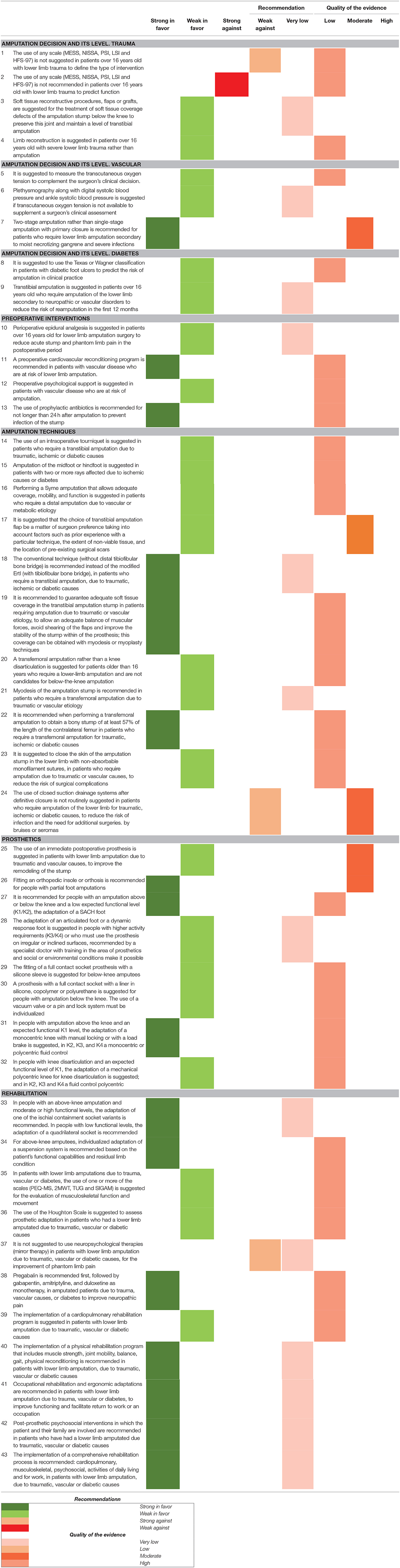
Table 2. Recommendations with quality of evidence and strength of recommendation (n = 43).
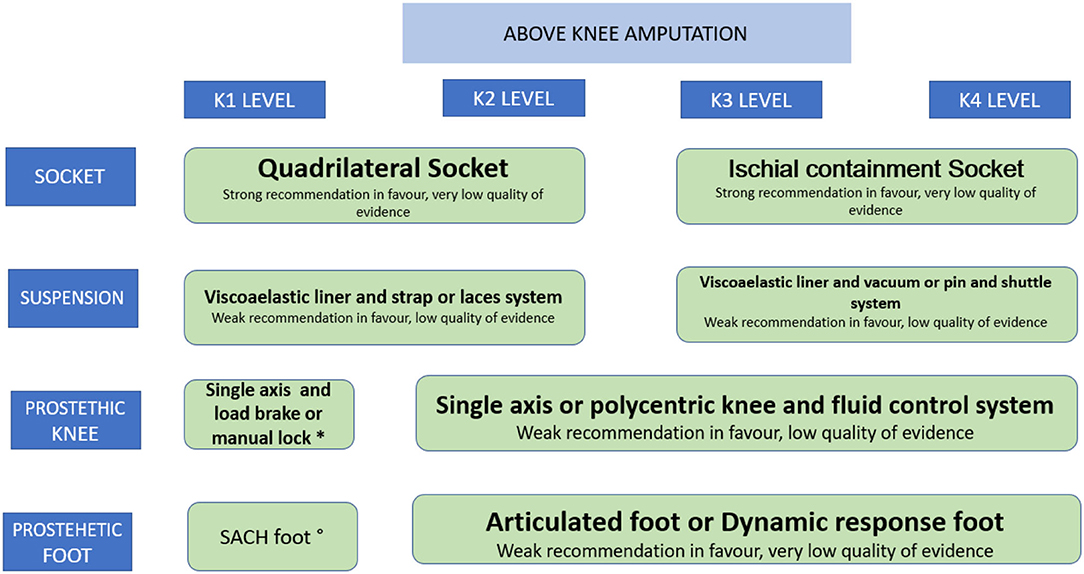
Figure 1. Recommendations for the prescription of the prosthesis in amputations above the knee. *Weak recommendation in favour. low quality of evidence. °Strong recommendation in favour. low quality of evidence.
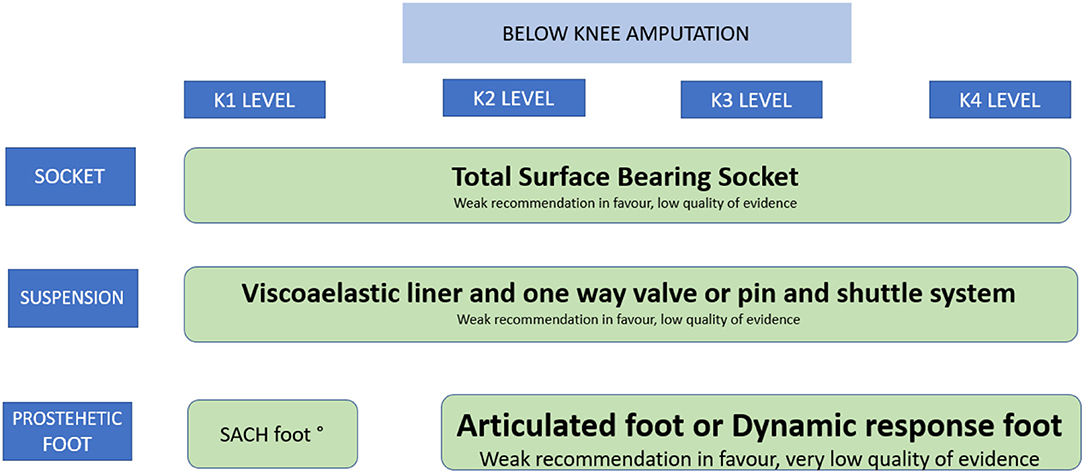
Figure 2. Recommendations for the prescription of the prosthesis in amputations below the knee. °Strong recommendation in favour. low quality of evidence.
The distribution of the 43 recommendations, according to the quality of the evidence, was: high 0%, moderate 7.5%, low 57.5%, very low 35%. And according to the strength of the recommendations, their distribution was: Strongly in favor 37.2%; weak in favor 53.48%; strong against 2.32%; weak against 6.97%. In updating the prioritized questions, a recommendation changed from Weak in favor to Strong in favor, leaving the distribution as follows: Strong in favor 58.3%, weak in favor 41.6%.
As part of the participation of patients in the development of the CPG, they were invited to assess the importance of each outcome of the recommendations (22). Patients chose stump infection in 31.7%, death in 22%, stump reoperation in 22%, and phantom pain in 12.2% as the most important outcomes for them. The most important activities in the rehabilitation process were walking in 51.2%, returning to work in 17.1%, having a good quality of life in 14.6% and participating in social activities in 7.3%. Twenty patients participated in the evaluation of preferences. Of them, 95% prefer to keep the knee to a transfemoral amputation, 60% prefer amputation in the first surgery than reconstruction, 75% agree with the need for psychological support, 85% agree with a supervised exercise plan after amputation and, only 45% agree with the use of an immediate prosthesis (22).
The results of the first economic evaluation concluded that, after a careful selection of patients and intervention by a multidisciplinary team, limb reconstruction was a dominant strategy compared to primary amputation in the long term (23).
In the second evaluation, the adaptation of an articulated foot was not a cost-effective strategy compared to a SACH foot, in patients with a low level of activity (8).
In the third, in a sample of 113 patients analyzed in a cross-sectional study, the total contact socket was a cost-effective strategy compared to a patellar-tendon-bearing (PTB) type (8). However, it is not possible to determine if this result can be extrapolated to other populations of patients with amputations below the knee in Colombia.
In the fourth economic evaluation, Pregabalin was found to be the strategy with the greatest net benefit, so it can be considered first-line treatment of phantom pain or residual pain in lower limb patients with amputation (24). Gabapentin and amitriptyline had similar, albeit lower, net benefits and could also be considered at the discretion and experience of the treating physician. More research is needed on the effectiveness of medications in patients with lower limb amputation.
In the fifth economic evaluation on the cost-effectiveness of prophylactic antibiotics, it was found that this is a dominant strategy and it is unlikely that the uncertainty surrounding the costs and benefits changes the results, the use of this intervention is recommended in Colombia (25).
As a final result of the CPG, the implementation process was described based on planning, implementation activities, monitoring and evaluation. Structure, process and outcome indicators were defined. Structure indicators were the availability of surgical and rehabilitation services. Process indicators were the proportion of patients with prostheses and in a rehabilitation program, according to the recommendations of the guidelines. Outcome indicators were the proportion of patients with reamputation, the proportion of patients adapted to prosthesis, and the proportion of professionals who follow the recommendations of the CPG.
This article described the methods and results of the elaboration of an evidence-based CPG for the care of people with lower limb amputations.
The elaboration of the CPG started with the formation of a multidisciplinary group that received training in methods form international and national universities and centers. The guideline included 43 recommendations, where nine were about the amputation decision and the level of amputation; five on preoperative interventions; 10 on amputation techniques; 10 on prosthetic components and nine on post-prosthetic rehabilitation. In 93% of the recommendations, the quality of the evidence was between low and very low. This is why it was so important, on a permanent basis, to validate and discuss each recommendation with an expanded multidisciplinary group with experience in treating lower-limb amputees. The socialization was carried out with different actors interested in the care of these patients.
This CPG was evaluated by international experts using the AGREE II instrument, with a score of 94/100, and was recommended for its implementation in Colombia. During the development, other CPG were evaluated, in which the scope and purpose domain had scores between 65.3 and 98.6%; in the stakeholder involvement between 54.1 and 97.2%; in the rigor of development between 25.0 and 85.9%; in the domain of clarity of presentation between 62.5 and 95.8; in applicability between 18.8 and 93.8%; and in editorial independence between 14.1 and 7.9% (8). This is in agreement with an article that evaluated the quality of the evidence of four CPG with 217 recommendations and found that the quality of the evidence was low (26). In addition, in the rehabilitation questions only 6.9% came from randomized clinical trials (RCT), systematic reviews or meta-analyses.
Although there were three CPG that had a score >60 in the methodological domain of the AGREII rating (27–29), they were not adapted because many of the questions raised by the developer group did not coincide with the questions of the guidelines. And the second reason was because the methodological guideline of Colombia (7) recommends that the guidelines in Colombia must be developed with the GRADE methodology and the guidelines did not follow this methodology at the time of the CPG search.
The research group identified 25 interventions and five milestones to be prioritized in the implementation. The milestones included re-amputation, reinterventions due to infectious processes, prosthetic adaptation, return to work and independence in activities of daily living (30).
We conducted a stakeholder's dialogue as a mechanism for the external validation of the Guideline implementation (31). Fifty-four actors participated in this forum, including: professionals from the MoH, representatives from health insurance companies, health provider institutions, academic professionals, scientific associations and thematic experts from different areas, patients, undergraduate and postgraduate students. In this dialogue participants emphasized the need to build integrated rehabilitation programs that are close to the patients in order to guarantee access to the health services with the minimum displacement of the patient. It is important to include care in the area of mental health. Successful prosthetic adaptation also depends on family support, training in activities of daily living, modification of the home and community environment, and occupational reintegration. Users must be guaranteed that they have sufficient and timely information, and continuous training, so that they are active actors in their surgical and rehabilitation process, through knowledge of their rights.
Insurers must recognize their responsibility in the care, rehabilitation and risk management of their insured population. Extramural actions must be included that allow the decentralization of rehabilitation services.
For the stakeholder participants it is important to have an information system for all personnel in charge, and to be able to measure the quality of care and the outcomes in patients. The referral and counter-referral process should be strengthened so that patients residing in rural and dispersed areas can access services in the main cities. In addition, implement a system in which patients are referred to centers where their needs can be effectively responded to. It is important for the country to involve these aspects in medical training and related professions, as well as continuing education for professionals involved in patient care, including evidence-based medicine and CPG training.
Several facilitators must be involved to improve patient accessibility such as technological tools, telemedicine and tele-rehabilitation (32, 33). These strategies were strengthened during the SARS2 COVID 19 pandemic.
The most important barriers and facilitators found in a qualitative study made by the research group and that were decisive for the implementation of the CPG for amputees included challenges related to the governance and financial arrangements of the Colombian health systems (34). For example, the Colombian health system could mandate that health care institutions establish procedures to adapt CPGs for amputee patients. At the time, health institutions are only required to have CPG for the most 10 prevalent health conditions; and amputations do not meet that requirement. Regarding financial arrangements, policymakers could ensure that access to the promotion, prevention, diagnosis, treatment, and rehabilitation of individuals with amputations does not depend on the type of patient insurance (34). In the systematic meta-review, there was greater emphasis on the barriers related to professionals, such as lack of credibility in the evidence, lack of training in CPG, the absence of a leader, and difficulties with the work team. Patients identified the lack of information from health professionals as difficulties, expressing the need for prostheses to be adapted according to their context (35).
The results of investments in research and training of health personnel to improve the quality of care are not being taken into account in health practice settings and many patients are not receiving the best possible care. This represents a gap between medical advances and clinical practice. Similar findings have been reported around the world in both developed and developing settings, in primary and specialty care (1).
For health professionals in charge of caring for amputees, it is important to emphasize the need for patients to receive the most effective and safe interventions. Patients need to receive this intervention in time to reduce functional limitations and achieve occupational reintegration and social participation for amputees.
Rehabilitation services must be comprehensive and available in a place that is close to patients to reduce the possibility of loss in the continuity of care. In the country, travel is paid for by patients and their families and this can be an even greater barrier if they must go to different places for their treatment. Comprehensive rehabilitation must involve mental health aspects to prepare amputees in the phase of acceptance and mourning for the loss of their limb and provide support in rehabilitation. Also, comprehensive rehabilitation must include physiatrist care, physical and occupational therapy, cardiopulmonary rehabilitation, psychology care and very importantly access to the prosthesis and its adaptation. All of the above will make possible for amputees to return to their usual occupation and integrate into society.
Professionals must have the necessary training, time and incentives to achieve a change in professional practice.
In Colombia, administrative procedures with insurers companies are lengthy and amputee patients must take multiple steps to obtain approval for each of the interventions and devices necessary for their rehabilitation (36, 37). The rehabilitation program should be approved as a package of interventions based on the recommendations of the CPG.
One limitation of the study is not having the final results of the implementation project to make better analyzes of the situations presented.
It is not enough to prepare a CPG of very good quality, to elaborate a comprehensive health care pathway and to assess the barriers and facilitators for recommendations implementation, to improve the healthcare process of people with lower limb amputations in Colombia. It is necessary to develop a national policy that promotes the necessary arrangements for the provision of services as coordination of care amongst different providers, communications between them, continuity of care, package of care, referral systems, shared care, multidisciplinary teams, planning the transition of care from hospital to the community, health information systems development. Financial and governance arrangements and finally implementation strategies targeted at healthcare organizations, at healthcare workers, and in a specific type of practice.
All authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the manuscript.
Article financed by the Ministry of Science, Technology and Innovation - Minciencias, under contract 738 of 2017, project called: Efectividad de una estrategia basada en Telesalud para mejorar la implementación de la guía de práctica clínica para el diagnóstico y tratamiento preoperatorio, intraoperatorio y postoperatorio de la persona amputada, la prescripción de la prótesis y la rehabilitación integral en instituciones de salud en Antioquia: un estudio de intervención aleatorizado por conglomerados de hospitales.
JP-C is the technical director at Mahavir K-mina, a non-governmental organization that manufactures lower limb exoskeletal prostheses.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank the CPG Development Group.
1. Grimshaw JM, Eccles MP, Lavis JN, Hill SJ, Squires JE. Knowledge translation of research findings. Implement Sci. (2012) 7:50. doi: 10.1186/1748-5908-7-50
2. Kruk ME, Gage AD, Arsenault C, Jordan K, Leslie HH, Roder-DeWan S, et al. High-quality health systems in the sustainable development goals era: time for a revolution. Lancet Glob Health. (2018) 6:e1196–252. doi: 10.1016/S2214-109X(18)30386-3
3. Moberg J, Oxman AD, Rosenbaum S, Schünemann HJ, Guyatt G, Flottorp S, et al. The GRADE evidence to decision (EtD) framework for health system and public health decisions. Health Res Policy Syst. (2018) 16:45. doi: 10.1186/s12961-018-0320-2
4. McGlynn EA, Asch SM, Adams J, Keesey J, Hicks J, DeCristofaro A, et al. The quality of health care delivered to adults in the United States. N Engl J Med. (2003) 348:2635–45. doi: 10.1056/NEJMsa022615
5. Carrasquilla G, Pulido A, De la Hoz A, et al. Guía Metodológica para la elaboración de Guías de Práctica Clínica con Evaluación Económica en el Sistema General de Seguridad Social en Salud Colombiano. Available online at: https://www.iets.org.co/Guia_Metodologica_2014
6. Lugo-Agudelo LH, Senior JM, Ramírez P. Pastor- Durango María del Pilar. Aspectos metodológicos de las Guías de Práctica Clínica realizadas en la Universidad de Antioquia con base en la guía metodológica del Ministerio de Salud y Protección de Colombia Suplemento. IATREIA. (2016) 29:S11–41. Available online at: https://revistas.udea.edu.co/index.php/iatreia/article/view/323691
7. Ministerio de Salud y Protección Social. Manual de implementación de guías de práctica clínica basadas en evidencia, en instituciones prestadoras de servicios de salud en Colombia [Internet]. 2014. Available online at: https://www.minsalud.gov.co/salud/Documents/Manual_Implementacion2014 (accessed 2021 2, December)
8. Salinas F, Ahunca L, Muñoz D, Vélez D, Sierra J, Lugo L, et al. Guía de práctica clínica para el diagnóstico y tratamiento preoperatorio, intraoperatorio y posoperatorio de la persona amputada, la prescripción de la prótesis y la rehabilitación integral [Internet]. Ministerio de Salud y Protección Social. Available online at: https://gpc.minsalud.gov.co/gpc_sites/GPC_Amputacion
9. National Center for Dissemination of Disability Research. What is knowledge translation? Technical brief number 10. 2005. Available online at: https://ktdrr.org/ktlibrary/articles_pubs/ncddrwork/focus/focus10/Focus10.pdf
10. Guyatt G, Oxman A, Aklm E, Kunze R, Vistc G, Brozec J, el al. GRADE guidelines: 1. Introduction. GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. (2011) 64:383–94. doi: 10.1016/j.jclinepi.2010.04.026
11. Balshem H, Helfand M, Schunemann HJ, Oxman AD, Kunz R, Brozek J, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. (2011) 64:401–6. doi: 10.1016/j.jclinepi.2010.07.015
12. Shea BJ1, Grimshaw JM, Wells GA, Boers M. Measurement tool created to assess the methodological quality of systematic reviews. BMC Med Res Methodol. (2007) 7:10. doi: 10.1186/1471-2288-7-10
13. QUADAS-2: A Revised tool for the quality assessment of diagnostic accuracy studies. Annals Internal Med. (2011) 155:529–36. doi: 10.7326/0003-4819-155-8-201110180-00009
14. White RG, Hakim AJ, Salganik MJ, Spiller MW, Johnston LG, Kerr L, et al. Strengthening the Reporting of Observational Studies in Epidemiology for respondent-driven sampling studies: “STROBE-RDS” statement. J Clin Epidemiol. (2015) 68:1463–71. doi: 10.1016/j.jclinepi.2015.04.002
15. Guyatt GH, Oxman AD, Vist G, Kunz R, Brozek J, Alonso-Coello P, et al. GRADE guidelines 4: rating the quality of evidence - risk of bias. J Clin Epidemiol. (2011) 64:407–15. doi: 10.1016/j.jclinepi.2010.07.017
16. Guyatt GH, Oxman AD, Montori V, Vist G, Kunz R, Brozek J, et al. GRADE guidelines 5: rating the quality of evidence - publication bias. J Clin Epidemiol. (2011) 64:1277–82. doi: 10.1016/j.jclinepi.2011.01.011
17. Guyatt G, Oxman AD, Kunz R, Brozek J, Alonso-Coello P, Rind D, et al. GRADE guidelines 6. Rating the quality of evidence - imprecision. J Clin Epidemiol. (2011) 64:1283–93. doi: 10.1016/j.jclinepi.2011.01.012
18. Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et al. The GRADE Working Group.GRADE guidelines: 7. Rating the quality of evidence - inconsistency. J Clin Epidemiol. (2011) 64: 1294–302. doi: 10.1016/j.jclinepi.2011.03.017
19. Guyatt GH, Oxman AD, Kunz R, Woodcock J, Brozek J, Helfand M, et al. The GRADE Working Group.GRADE guidelines: 8. Rating the quality of evidence - indirectness. J Clin Epidemiol. (2011) 64:1303–10. doi: 10.1016/j.jclinepi.2011.04.014
20. Guyatt GH, Oxman AD, Sultan S, Glasziou P, Akl EA, Alonso-Coello P, et al. The GRADE Working Group.GRADE guidelines: 9. Rating up the quality of evidence. J Clin Epidemiol. (2011) 66:736–42. doi: 10.1016/j.jclinepi.2011.06.004
21. Andrews J, Guyatt G, Oxman AD, Alderson P, et al. GRADE guidelines: 15. Going from evidence to recommendations: the significance and presentation of recommendations. J Clin Epidemiol. (2013) (7):719–25. doi: 10.1016/j.jclinepi.2012.03.013
22. Posada-Borrero AM, Plata-Contreras JA, Lugo-Agudelo LH. Participación de los pacientes con amputación del miembro inferior en la elaboración de una guía de práctica clínica en Colombia. Iatreia. (2017) 29:S96–109. Available online at: https://revistas.udea.edu.co/index.php/iatreia/article/view/27085
23. Ceballos M, Orozco L, Valderrama C, Sanchez L, Valderrama JP, Lugo LH. Cost-utility analysis of reconstruction compared with primary amputation for patients with severe lower limb trauma in Colombia. J Orthop Trauma. (2017) 31:e288–94. doi: 10.1097/BOT.0000000000000883
24. Ceballos-González M, Orozco-Ramírez L, Sierra-Abaunza J, Sánchez-Higuita L, Lugo-Agudelo L. Análisis de costo-efectividad de cinco estrategias farmacológicas para el tratamiento de primera lde pacientes con dolor neuropático en Colombia. IATREIA. (2016) 29:S110–121. Availalble online at: https://revistas.udea.edu.co/index.php/iatreia/article/view/26727
25. Ceballos M, Orozco LE, Valderrama CO, Londoño DI, Lugo LH, Costeffectiveness analysis of the use of a prophylactic antibiotic for patients undergoing lower limb amputation due to diabetes or vascular illness in Colombia. Annals Vasc Surg. (2017) 40: 327–34. doi: 10.1016/j.avsg.2016.07.090
26. Heyns A, Jacobs S, Negrini S, Patrini M, Rauch, A Kiekens C. Systematic review of clinical practice guidelines for individuals with amputation: identification of best evidence for rehabilitation to develop the WHO's package of interventions for rehabilitation. ArcPhysical Med Rehabilit. (2021) 102:1191–7. doi: 10.1016/j.apmr.2020.11.019
27. Rehabilitation of Lower Limb Amputation Working Group. VA/DoD Clinical practice guideline for rehabilitation of lower limb amputation. (2007). Available online at: http://www.healthquality.va.gov/guidelines/Rehab/amp/amp_v652.pdf
28. Broomhead P, Dawes D, Hale C, Clark K, Lambert A, Quinlivan D, et al. Evidence based clinical guidelines for the physiotherapy management of adults with lower limb prostheses. 2nd Ed. London: Chartered Society of Physiotherapy (2012). Available online at: http://www.csp.org.uk/sites/files/csp/secure/bacpar_amputee_rehab_guidelines_2012_1.pdf
29. Jarvis V, Verral T. Prosthetic best practice guidelines. West Yorkshire: RSL Steeper; 2010. Available online at: http://rslsteeper.com/uploads/files/281/rslsteeper_prosthetic_best_practice_guidelines.pdf
30. Giraldo Castaño L, Pinto-Maquilón JK, Lugo-Agudelo LH, Velásquez-Correa JC, Pastor MP, Posada-Borrero AM, et al. Ruta integral de atención en salud para personas con amputaciones de miembro inferior, para mejorar el funcionamiento y la calidad de vida. Rev Fac Nac Salud Pública. (2022) 40:e342981. doi: 10.17533/udea.rfnsp.e342981
31. Grupo de. Rehabilitación en Salud (GRES), Unidad de Evidencia y Deliberación para la Toma de decisiones (UNED). Reporte del diálogo deliberativo: Verificación y validación externa de la Ruta Integral de Atención en Salud RIAS para amputaciones de miembro inferior por causas traum1ticas y neurovasculares (2020).
32. Ekeland AG, Bowes A, Flottorp S. Effectiveness of telemedicine: a systematic review of reviews. Int J Med Inform. (2010) 79:736–71. doi: 10.1016/j.ijmedinf.2010.08.006
33. Anderson L, Sharp GA, Norton RJ, Dalal H, Dean SG, Jolly K, et al. Home-based vs. centre-based cardiac rehabilitation. Cochrane Database Syst Rev. (2017) 6:CD007130. doi: 10.1002/14651858.CD007130.pub4
34. Patiño-Lugo DF, Pastor Durango MDP, Lugo-Agudelo LH, Posada Borrero AM, Ciro Correa V, Plata Contreras JA, et al. Implementation of the clinical practice guideline for individuals with amputations in Colombia: a qualitative study on perceived barriers and facilitators. BMC Health Serv Res. (2020) 20:538. doi: 10.1186/s12913-020-05406-z
35. Correa VC, Lugo-Agudelo LH, Aguirre-Acevedo DC, Contreras JAP, Borrero AMP, Patiño-Lugo DF, et al. Individual, health system, and contextual barriers and facilitators for the implementation of clinical practice guidelines: a systematic metareview. Health Res Policy Syst. (2020) 18:74. doi: 10.1186/s12961-020-00588-8
36. Vargas I, Vazquez ML, Mogollon-Perez AS, Unger JP. Barriers of access to care in a managed competition model: lessons from Colombia. BMC Health Serv Res. (2010) 10:297 Available online at: http://ovidsp.ovid.com/ovidweb.cgi doi: 10.1186/1472-6963-10-297
37. Abadia CE, Oviedo DG. Bureaucratic Itineraries in Colombia. A theoretical and methodological tool to assess managed-care health care systems. Soc Sci Med. (2009) 68:1153–60. doi: 10.1016/j.socscimed.2008.12.049 Available online at: http://www.ncbi.nlm.nih.gov/pubmed/19178990
Keywords: implementation, clinical practical guidelines, lower limb amputation, knowledge translation (KT), rehabilitation
Citation: Posada-Borrero AM, Patiño-Lugo DF, Plata-Contreras JA, Velasquez-Correa JC and Lugo-Agudelo LH (2022) Development of a Clinical Practice Guideline for Lower Limb Amputees. A Knowledge Translation Process in a Middle Income Country. Front. Rehabilit. Sci. 3:873436. doi: 10.3389/fresc.2022.873436
Received: 10 February 2022; Accepted: 11 April 2022;
Published: 03 May 2022.
Edited by:
Maria Gabriella Ceravolo, Marche Polytechnic University, ItalyReviewed by:
Katherine E. Harding, La Trobe University, AustraliaCopyright © 2022 Posada-Borrero, Patiño-Lugo, Plata-Contreras, Velasquez-Correa and Lugo-Agudelo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Maria Posada-Borrero, YW1wb3NhZGFAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.