 Andy Kerr
Andy Kerr Madeleine Ann Grealy
Madeleine Ann Grealy Anja Kuschmann2
Anja Kuschmann2
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Rehabil. Sci., 07 January 2022
Sec. Disability, Rehabilitation, and Inclusion
Volume 2 - 2021 | https://doi.org/10.3389/fresc.2021.820929
This article is part of the Research TopicAffordable Technology for Rehabilitation in Low Resource SettingsView all 4 articles
Background: The prevalence of disabling conditions is increasing globally. Rehabilitation improves function and quality of life across many conditions, particularly when applied intensively. The limited workforce, however, cannot deliver evidence-based intensive rehabilitation. By providing individuals with the tools for self- rehabilitation, technology helps bridge the gap between evidence and practise. Few people, however, can access rehabilitation technology. Barriers such as cost, training, education, portability and poor design stand in the way of equitable access. Our group of engineers and researchers have established a centre dedicated to developing accessible technology through close, frequent engagement with users and industry.
Methods: The centre employs a co-creation model, coupling engineering and science with user experience and industrial partnerships to develop accessible technology and associated processes. Due to the complexity and size of the challenge the initial focus is stroke. Recruited through a medical charity, participants, with a wide range of disabilities, use prototype and commercial technology during an 8-week rehabilitation programme with supervision from health professionals. The centre includes de-weighting systems, neurostimulation, virtual reality, treadmills, bespoke rehab games, communication apps, powered exercise equipment and gamified resistance equipment. Standard outcome measures (International Classification of Functioning, Disability and Health) are recorded before, during, immediately after, and 3 months after the intervention and used in combination with an interview to design the initial rehabilitation programme, which is reviewed fortnightly. Qualitative methods (surveys and interviews) are used to capture personal experiences of the programme and individual technology and an advisory group of stroke survivors help interpret outcomes to feed into the technology design process. Ethical approval has been granted for a pilot cohort study with stroke survivors, which is currently underway (01/09/2021–31/12/2021) investigating acceptability and feasibility, due to report findings in 2022.
Discussion: Through partnerships, research collaborations and a co-creation model a new centre dedicated to the development of accessible rehabilitation technology has been launched and currently undergoing acceptability and feasibility testing with stroke survivors. The centre, through its close engagement with users and industry, has the potential to transform the way rehabilitation technology is developed and help revolutionise the way rehabilitation is delivered.
Since the industrial revolution improvements in disease prevention (lifestyle, diet, housing, sanitation and education) have had a transformative effect on the health and longevity of most humans. This has been matched by cures for many diseases through surgical and drug interventions. Where disease and injury can't be cured there are well-developed nursing and medical procedures to maintain an individual's quality of life and palliative care to support the dying (1).
The undoubted success of these health strategies has resulted in people living longer, healthier lives (2). The ageing population and improved survival rates from diseases like stroke, however, mean levels of disability have increased (3). Rehabilitation is known to improve the quality of life, and function, of people living with disability (4–6) as well as reducing the burden on acute health services (7). It is estimated that 2.41 billion people live with health conditions known to benefit from rehabilitation (8), however, access to recommended levels of rehabilitation is grossly unequal across the globe and even in high income countries are typically well-below guideline levels (9–11).
Technology has long been suggested as a means to bridge the gap between evidence-based rehabilitation and what can realistically be provided by health services (12). While there is undoubted potential in this approach, technology needs to be developed with access as a core principle (13), otherwise the gross inequities in the provision of rehabilitation will persist. Developing accessible technology; user friendly, self-managed, cost effective and available for domestic homes or local leisure centres should be seen as a priority for industry, developers and funders.
In this paper we detail the methods employed by the first engineering department (in Scotland) dedicated to using a co-creation framework for designing rehabilitation technology and outline the initial feasibility study. The intention of this approach is to produce technology that is useful; meaning both effective for recovery and accessible to all who need it.
While the research team have a number of questions related to the specific effects of rehabilitation and optimisation of a technological approach to self-rehabilitation, the primary questions for the centre are initially concerned with acceptability and feasibility of the overall approach, including safety, adverse events, participant acceptability, recruitment, required levels of supervision, participant training and motivation.
The guiding principle of the centre is co-creation through frequent and intensive user engagement. To enable this we have established a fully operational rehabilitation clinic equipped with commercially available, and prototype, rehabilitation technology, including de-weighting systems, non-invasive neurostimulation, virtual reality, treadmill, bespoke video games and tablet apps, powered exercise and gamified resistance equipment (see Table 1 for details). The clinic is staffed by a rehabilitation professional who designs and supervises an 8-week programme, based on an initial assessment of needs and agreed goals, delivered, exclusively, through the available technology.
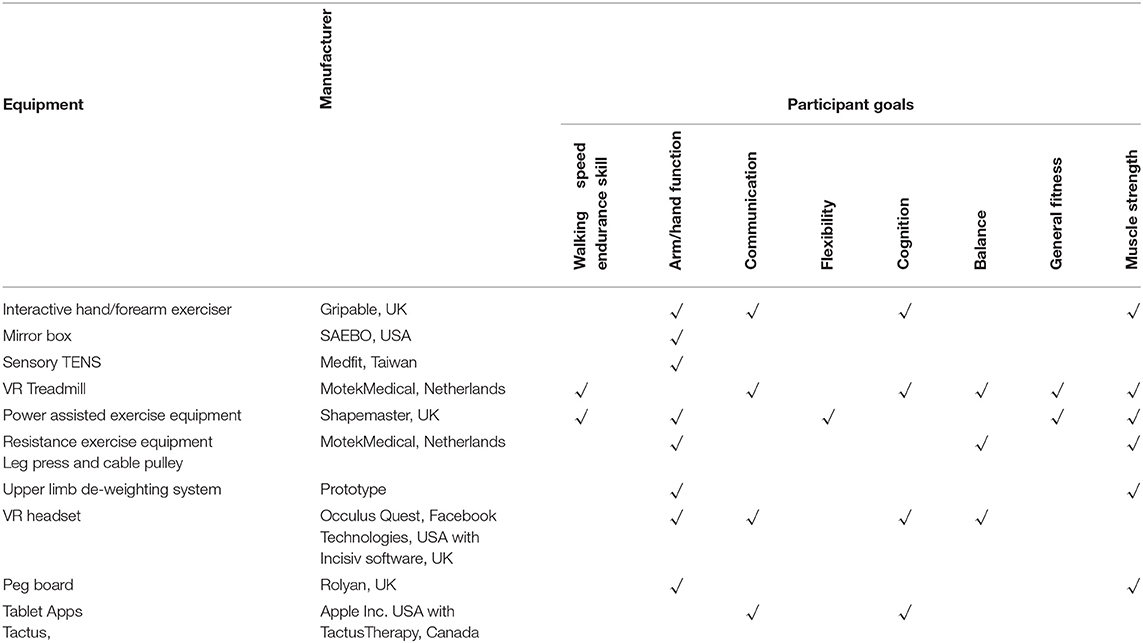
Table 1. Details of equipment used and corresponding participant goals.
A pilot cohort study with stroke survivors (n = 7) has been designed to test the feasibility of this approach as well as participant acceptability. A mixed methods approach will be used to answer the key questions, including recruitment rates, retention rates, adverse events, programme compliance, level of assistance/supervision required, change in function and participant opinions on specific pieces of technology as well as the overall programme. Recruitment to the pilot commenced on 01/09/2021 and will end on 18/11/2021.
Potential participants are recruited through an open invitation distributed to local support groups organised by our medical charity partner, Chest Heart and Stroke Scotland (CHSS). Individuals subsequently contacting the centre are assessed for eligibility based on the criteria detailed in Table 2. The study has institutional ethical approval (UEC20/08).
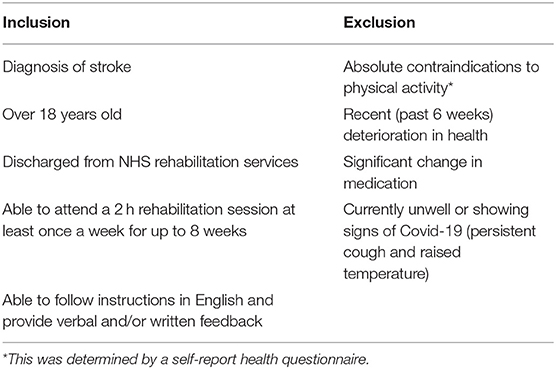
Table 2. Eligibility criteria.
Once eligibility has been established an initial appointment is made to complete the informed consent process and let participants become familiar with the centre and some of the technology they may use. Participants, along with the research team, are also asked to adhere to the institutional Covid-19 restrictions during this period, including social distancing, mask wearing and carrying out two lateral flow tests per week.
The 8-week, technology enabled, rehabilitation programme is structured around the broad principles of intensity, feedback, cognitive engagement and aerobic activity (14) to address the goals identified by the participant and scores recorded from the outcome measures (see Table 3). Rest periods and time to become familiar with the technology are factored into the sessions along with non-invasive priming techniques such as mirror therapy and sensory TENS (29) which participants will be encouraged to use at the start of each session. Figure 1 provides an overview of the flow of participants through the centre.
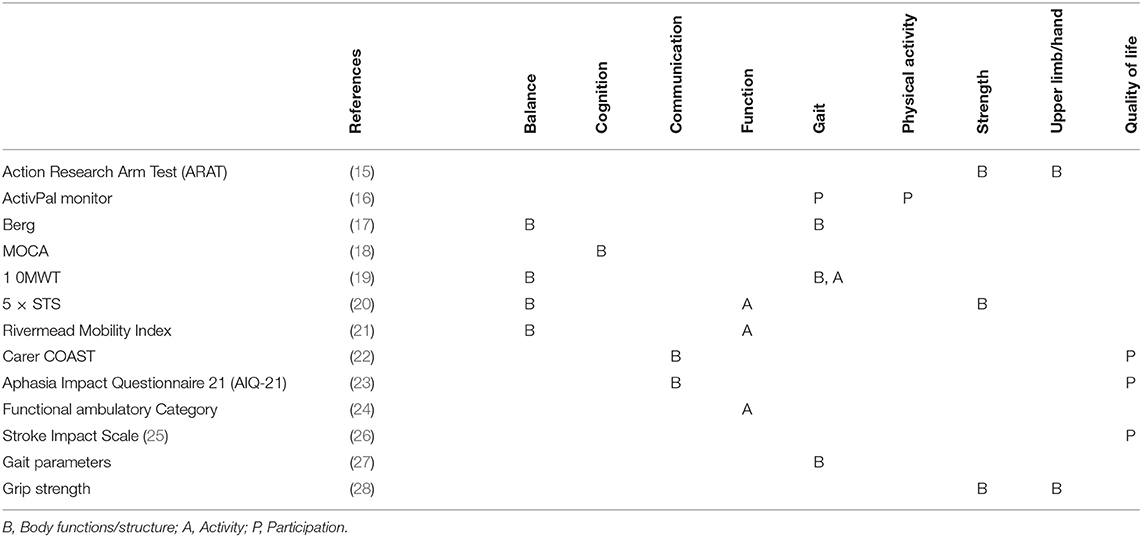
Table 3. Outcome measures used in pilot matched to the ICF framework.
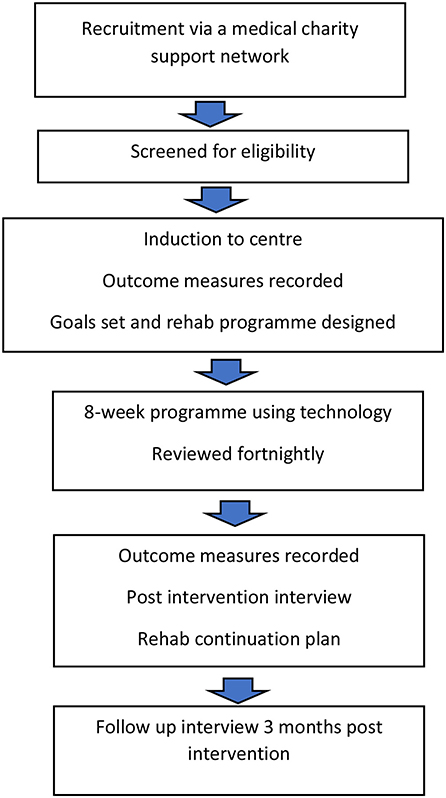
Figure 1. Flow of participants through centre.
Outcome measures were selected based on their reported acceptability (validity and reliability) in the research literature and common place use in the local health service. Details are provided in Table 3, they represent the body structure (B), activity (A) and participation (P) levels of the ICF (25).
A structured rehabilitation programme will then be developed, co-operatively, by the rehabilitation professional and participant including agreed goals, frequency of attendance, duration and details of individual pieces of equipment to be used, see below for example.
Total work time 80 min, with rest, as appropriate, in between activities.
Improve general fitness, standing balance, lower limb strength, walking (symmetry and speed) and range of upper limb movement.
1. Mirror therapy for hand (20 min)
Hand/wrist exercises following suggested guideline.
2. Powered exercise equipment
a. Seated cross trainer, 10 min
b. Recumbent cycling 5 min.
3. Speech therapy app, picture and word matching, 10 min
4. Treadmill (25 min), (see Figure 2) for illustration
a. Balance games to encourage increased loading on weaker side, 5 min
b. Walking in VR environment at comfortable walking speed (0.44 m/s) + 10%, 5 min
c. Balance games to encourage increased loading on weaker side, 5 min
d. Walking game that requires frequent adjustments to position, 5 min.
e. Walking in VR environment at comfortable walking speed with 5 × 20 s periods of fast walking (comfortable walking speed + 20%).
5. Functional squat 10 min—targeting symmetrical loading. 10 Kg load.
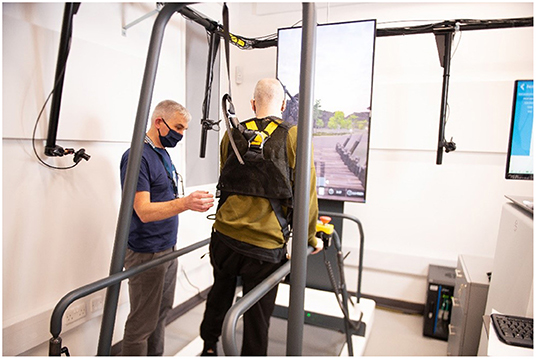
Figure 2. Participant training with an interactive treadmill under supervision.
Following completion of the 8-week programme the outcome measures are repeated. A plan to continue a modified version of the programme will be discussed. Finally, an independent researcher will arrange a time (within the following 2 weeks) for a one to one interview by telephone or free to download teleconferencing software. The interview will be open with the following questions given as a guideline;
(1) How did you find the treadmill/bike/balance trainer/arm trainer/communication app?
Was there anything you found particularly difficult to manage?
Was there anything you found particularly easy to manage?
(2) Technology based feedback on rehabilitation progress
For example:
Did you find the progress information provided by the equipment useful?
Were you able to access it easily enough?
Did you need help understanding it?
(3) Effectiveness
For example:
Did you achieve your overall goal?
Do you think there has been any change in your communication/mobility/balance/confidence/overall quality of life? Can you give a specific example to describe how this aspect has changed?
Was there any particular piece of equipment that you think helped more?
(4) Need for supervision
For example:
How important do you think having someone present was?
Do you think you need a trained person present?
Was there any equipment you feel you could manage without any help?
(5) Potential for home use
For example:
Would you consider using any of the equipment at home or at your local sports centre?
Would you anticipate any difficulties using this equipment at home or your local sports centre?
What support do you think you might need/like to use this equipment at home?
(6) Future plans
For example:
Now that you have completed the rehabilitation programme will you continue any activities/rehabilitation exercises?
Do you have any plans to continue with rehabilitation?
(7) Ideas for improvement
For example:
Now that you have experienced rehabilitation using machines and equipment do you have any suggestions for improvement?
Thinking about the specific equipment you used do you think we could improve it?
Do you have any ideas of your own that might help people recover from stroke?
How do you think we could improve the overall experience for you?
The primary objective for the pilot study is to assess feasibility and acceptability. Data on compliance (sessions completed as percentage of planned), recruitment (people consenting as percentage of those volunteering) and rates of adverse events will be reported with descriptive statistics. Acceptability will be explored from a thematic analysis of the interview transcripts.
In addition any change in the outcome measures (before and after the intervention) will be described with 95% confidence intervals (if data are normally distributed) or interquartile range (if not).
In this paper we have outlined the rationale for a co-creation centre in rehabilitation technology, provided some of the operational detail and outlined the methods for our pilot study designed to test feasibility and acceptability of the overall approach before we plan future research.
Our pilot study is currently underway with seven stroke survivors participating. Once all participants have completed the programme a 6-week review period will be used to collate findings and implement any changes through discussion with our user group of stroke survivors. Once this has been completed, the project will move into a new phase with plans to recruit greater number of participants to our technology enabled rehabilitation programme.
Based on outcomes from the pilot we expect to make changes to operational processes such as recruitment, outcome measures, induction and even the way the individual programmes are structured, however the very positive views expressed by participants to the media, so far (see quotes below for the first two participants), have encouraged us to continue planning future projects, including, but not limited to:
• New devices to improve hand function for more severely affected individuals
• The use of machine learning to tailor individual rehab programmes on a continuous basis
• Recruitment of sub-acute stroke participants.
#1 “I love the sessions, even though they go so quickly. I think the long-term plan is that this unit will act like a drop-in gym for those who need it, which would be fantastic. And if something like this could be available across the country, it would be even better. It would be a shame for people to miss out” (30).
#2 “It was taking me 40 seconds to walk up down the gym and now I can do it in 12 seconds. That's just in the space of a couple of weeks,” (31).
Despite mounting evidence on the positive effect of rehabilitation, recovery from stroke and other disabling conditions continues to be both disappointing and highly variable (14, 32) leading many researchers to explore the factors that could enable a more personalised, self-managed approach (33), with technology a key enabler (34). If this model of rehabilitation could be widely delivered, removing issues of access, not only would it improve equity but may also realise higher levels of recovery by delivering levels of rehabilitation indicated by research (35).
The optimal “dose” of rehabilitation remains unknown (35), a more technological approach may unlock greater potential for recovery but we, as a community of researchers and engineers, need to understand how this approach can work, equitably, in the real world and continually refine the necessary technology through co-creation with the users.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by University of Strathclyde Ethics Committee. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individuals for the publication of any potentially identifiable images or data included in this article.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
The centre was part funded by the Sir Jules Thorn Charitable Trust.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank Sir Jules Thorn Charitable Trust for funding the purchase of all the rehabilitation equipment.
1. Stucki G, Bickenbach J, Gutenbrunner C, Melvin J. Rehabilitation: the health strategy of the 21st century. J Rehabil Med. (2018) 50:309–16. doi: 10.2340/16501977-2200
2. WHO. World Health Statistics 2021: Monitoring Health for the SDGs, Sustainable Development Goals. Geneva: WHO (2021).
3. Chatterji S, Byles J, Cutler D. Health, functioning, and disability in older adults-present status and future implications (vol 385, pg 563, 2015). Lancet. (2015) 385:508. doi: 10.1016/S0140-6736(14)61462-8
4. Moreau NG, Bodkin AW, Bjornson K, Hobbs A, Soileau M, Lahasky K. Effectiveness of rehabilitation interventions to improve gait speed in children with cerebral palsy: systematic review and meta-analysis. Phys Ther. (2016) 96:1938–54. doi: 10.2522/ptj.20150401
5. Nguyen C, Lefevre-Colau MM, Poiraudeau S, Rannou F. Rehabilitation (exercise and strength training) and osteoarthritis: a critical narrative review. Ann Phys Rehabil Med. (2016) 59:190–5. doi: 10.1016/j.rehab.2016.02.010
6. Platz T. Evidence-based guidelines and clinical pathways in stroke rehabilitation-an international perspective. Front Neurol. (2019) 10:200. doi: 10.3389/fneur.2019.00200
7. Stucki G, Stier-Jarmer M, Grill E, Melvin J. Rationale and principles of early rehabilitation care after an acute injury or illness. Disabil Rehabil. (2005) 27:353–9. doi: 10.1080/09638280400014105
8. Cieza A, Causey K, Kamenov K, Hanson SW, Chatterji S, Vos T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. (2021) 396:2006–17. doi: 10.1016/S0140-6736(20)32340-0
9. Gimigliano F, Negrini S. The World Health Organization “Rehabilitation 2030: a call for action”. Eur J Phys Rehabil Med. (2017) 53:155–68. doi: 10.23736/S1973-9087.17.04746-3
10. Kerr A, Dawson J, Robertson C, Rowe P, Quinn TJ. Sit to stand activity during stroke rehabilitation. Top Stroke Rehabil. (2017) 24:562–6. doi: 10.1080/10749357.2017.1374687
11. Bernhardt J, Urimubenshi G, Gandhi DBC, Eng JJ. Stroke rehabilitation in low-income and middle-income countries: a call to action. Lancet. (2020) 396:1452–62. doi: 10.1016/S0140-6736(20)31313-1
12. Loureiro RC, Harwin WS, Nagai K, Johnson M. Advances in upper limb stroke rehabilitation: a technology push. Med Biol Eng Comput. (2011) 49:1103–18. doi: 10.1007/s11517-011-0797-0
13. Kerr A, Smith M, Reid L, Baillie L. Adoption of stroke rehabilitation technologies by the user community: qualitative study. JMIR Rehabil Assist Technol. (2018) 5:e15. doi: 10.2196/rehab.9219
14. Langhorne P, Coupar F, Pollock A. Motor recovery after stroke: a systematic review. Lancet Neurol. (2009) 8:741–754. doi: 10.1016/S1474-4422(09)70150-4
15. Chen HF, Lin KC, Wu CY, Chen CL. Rasch validation and predictive validity of the action research arm test in patients receiving stroke rehabilitation. Arch Phys Med Rehabil. (2012) 93:1039–45. doi: 10.1016/j.apmr.2011.11.033
16. Klenk J, Buchele G, Lindemann U, Kaufmann S, Peter R, Laszlo R, et al. Concurrent validity of activPAL and activPAL3 accelerometers in older adults. J Aging Phys Act. (2016) 24:444–50. doi: 10.1123/japa.2015-0178
17. Blum L, Korner-Bitensky N. Usefulness of the berg balance scale in stroke rehabilitation: a systematic review. Phys Ther. (2008) 88:559–66. doi: 10.2522/ptj.20070205
18. Wu CY, Hung SJ, Lin KC, Chen KH, Chen P, Tsay PK. Responsiveness, minimal clinically important difference, and validity of the MoCA in stroke rehabilitation. Occup Ther Int. (2019) 1–7. doi: 10.1155/2019/2517658
19. Persson CU, Hansson PO, Sunnerhagen KS. Clinical tests performed in acute stroke identify the risk of falling during the first year: postural stroke study in Gothenburg (Postgot). J Rehabil Med. (2011) 43:348–53. doi: 10.2340/16501977-0677
20. Mong YQ, Teo TW, Ng SS. 5-repetition sit-to-stand test in subjects with chronic stroke: reliability and validity. Arch Phys Med Rehabil. (2010) 91:407–13. doi: 10.1016/j.apmr.2009.10.030
21. Hsieh CL, Hsueh IP, Mao HF. Validity and responsiveness of the rivermead mobility index in stroke patients. Scand J Rehabil Med. (2000) 32:140–2. doi: 10.1080/003655000750045497
22. Long A, Hesketh A, Bowen A. Communication outcome after stroke: a new measure of the carer's perspective. Clin Rehabil. (2009) 23:846–56. doi: 10.1177/0269215509336055
23. Swinburn K, Best W, Beeke S, Cruice M, Smith L, Willis EP, et al. A concise patient reported outcome measure for people with aphasia: the aphasia impact questionnaire 21. Aphasiology. (2019) 33:1035–60. doi: 10.1080/02687038.2018.1517406
24. Mehrholz J, Wagner K, Rutte K, Meissner D, Pohl M. Predictive validity and responsiveness of the Functional Ambulation Category in hemiparetic patients after stroke. Arch Phys Med Rehabil. (2007) 88:1314–9. doi: 10.1016/j.apmr.2007.06.764
25. Stucki G, Cieza A, Ewert T, Kostanjsek N, Chatterji S, Ustun TB. Application of the International Classification of Functioning, Disability and Health (ICF) in clinical practice. Disabil Rehabil. (2002) 24:281–2. doi: 10.1080/09638280110105222
26. Edwards B, O'Connell B. Internal consistency and validity of the stroke impact scale 2.0 (SIS 2.0) and SIS-16 in an Australian sample. Qual Life Res. (2003) 12:1127–35. doi: 10.1023/A:1026109920478
27. Balasubramanian CK, Neptune RR, Kautz SA. Variability in spatiotemporal step characteristics and its relationship to walking performance post-stroke. Gait Post. (2009) 29:408–14. doi: 10.1016/j.gaitpost.2008.10.061
28. Bertrand AM, Fournier K, Brasey MGW, Kaiser ML, Frischknecht R, Diserens K. Reliability of maximal grip strength measurements and grip strength recovery following a stroke. J Hand Ther. (2015) 28:356–63. doi: 10.1016/j.jht.2015.04.004
29. Harmsen WJ, Bussmann JBJ, Selles RW, Hurkmans HLP, Ribbers GM. A mirror therapy-based action observation protocol to improve motor learning after stroke. Neurorehabil Neural Repair. (2015) 29:509–16. doi: 10.1177/1545968314558598
30. Fotheringham. 'Revolution in Stroke Care' - New Partnership Boost for Glasgow Charity Up for Share of £20k. Glasgow: Glasgow Evening Times.
32. Gelaw AY, Janakiraman B, Gebremeskel BF, Ravichandran H. Effectiveness of home-based rehabilitation in improving physical function of persons with stroke and other physical disability: a systematic review of randomized controlled trials. J Stroke Cerebrovasc Dis. (2020) 29:1–8. doi: 10.1016/j.jstrokecerebrovasdis.2020.104800
33. Wouters EFM, Wouters B, Augustin IML, Houben-Wilke S, Vanfleteren L, Franssen FME. Personalised pulmonary rehabilitation in COPD. Eur Respir Rev. (2018) 27:147. doi: 10.1183/16000617.0125-2017
34. Harris NR, Sthapit D. Towards a personalised rehabilitation system for post stroke treatment. In: 2016 IEEE Sensors Applications Symposium (Sas 2016) Proceedings. (2016). p. 217–21.
Keywords: rehabilitation, technology, accessible, stroke, co-creation
Citation: Kerr A, Grealy MA, Kuschmann A, Rutherford R and Rowe P (2022) A Co-creation Centre for Accessible Rehabilitation Technology. Front. Rehabilit. Sci. 2:820929. doi: 10.3389/fresc.2021.820929
Received: 23 November 2021; Accepted: 13 December 2021;
Published: 07 January 2022.
Edited by:
John M. Solomon, Manipal Academy of Higher Education, IndiaReviewed by:
Alessandro Giustini, Istituto di Riabilitazione Santo Stefano, ItalyCopyright © 2022 Kerr, Grealy, Kuschmann, Rutherford and Rowe. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andy Kerr, YS5rZXJyQHN0cmF0aC5hYy51aw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.