 Philipp Arendt1
Philipp Arendt1 Viola Borchardt-Lohölter
Viola Borchardt-Lohölter Mandy Busse
Mandy Busse- 1Institute for Experimental Immunology, Affiliated to EUROIMMUN Medizinische Labordiagnostika AG, Lübeck, Germany
- 2Department for Experimental Obstetrics and Gynecology, Medical Faculty, Otto-von-Guericke-University of Magdeburg, Magdeburg, Germany
- 3Department of Psychiatry and Psychotherapy, Medical Faculty University Hospital Magdeburg, Otto von Guericke University, Magdeburg, Germany
by Arendt, P., Römpler, K., Brix, B., Borchardt-Lohölter, V., Busse, M., and Busse, S. (2024). Front. Dement. 3:1455619. doi: 10.3389/frdem.2024.1455619
In the published article, there was an error in Figure 1D as published, where the labels of the x-axis in were incorrectly written as “AD (n = 220), DC (n = 218), MCI (n = 73).” The correct labels are “DC (n = 220), MCI (n = 74), AD (n = 219).”
The corrected Figure 1 and its caption appear below.
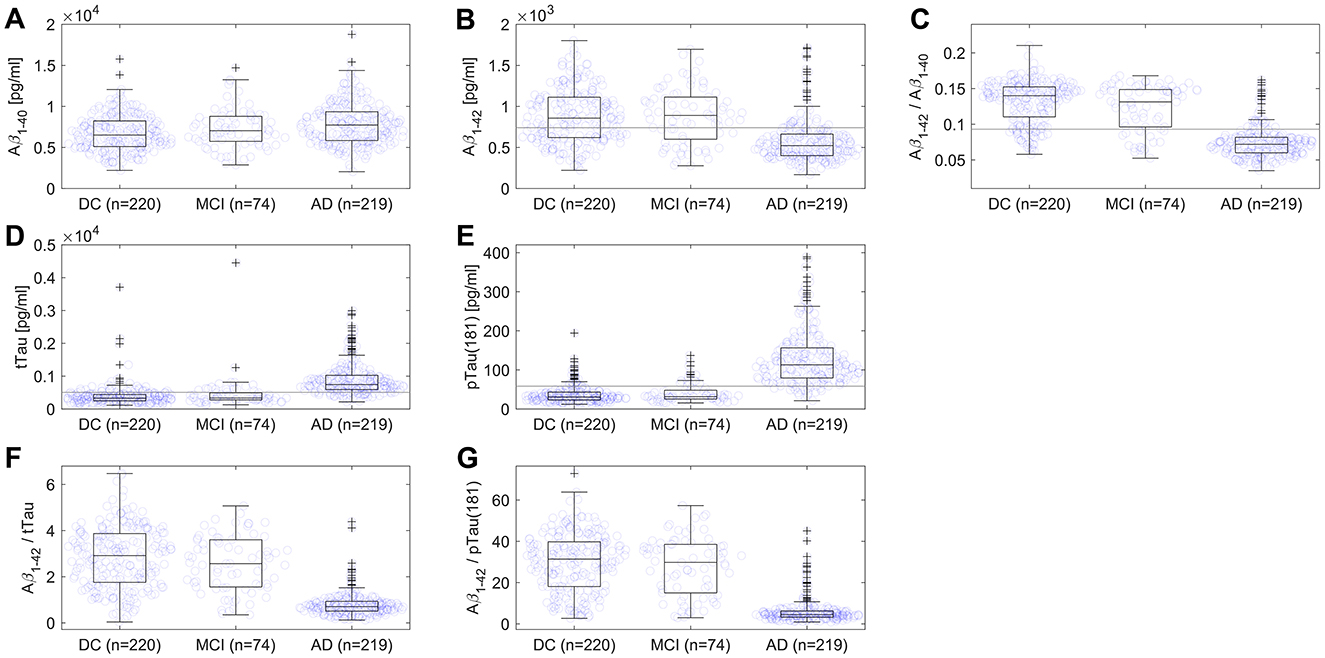
Figure 1. Scatterplots and boxplots comparing values of (A) Aβ1–40, (B) Aβ1–42, (C) ratio Aβ1–42/Aβ1–40, (D) tTau, (E) pTau(181), (F) ratio Aβ1–42/tTau, and (G) ratio Aβ1–42/pTau(181) for 219 Alzheimer's disease (AD) and 220 disease control (DC) patients, and 74 patients with mild cognitive impairment (MCI). On each box, the central mark indicates the median, and the bottom and top edges of the box indicate the 25th and 75th percentiles, respectively. The whiskers extend to the most extreme data points not considered outliers, and outliers are plotted as crosses. The gray line represents the assay's cut-off. One DC patient with Creutzfeldt-Jakob disease and one MCI patient were not displayed in (D) due to very high values of tTau.
The authors apologize for this error and state that this does not change the scientific conclusions of the article in any way. The original article has been updated.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Keywords: Alzheimer's disease, ATN system, beta-amyloid, biomarker, chemiluminescence immunoassay, cerebrospinal fluid, neurodegenerative diseases, mild cognitive impairment
Citation: Arendt P, Römpler K, Brix B, Borchardt-Lohölter V, Busse M and Busse S (2025) Corrigendum: Differentiation of Alzheimer's disease from other neurodegenerative disorders using chemiluminescence immunoassays measuring cerebrospinal fluid biomarkers. Front. Dement. 4:1568275. doi: 10.3389/frdem.2025.1568275
Received: 29 January 2025; Accepted: 06 February 2025;
Published: 17 February 2025.
Edited and reviewed by: Nobuyuki Kobayashi, Jikei University School of Medicine, Japan
Copyright © 2025 Arendt, Römpler, Brix, Borchardt-Lohölter, Busse and Busse. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Viola Borchardt-Lohölter, di5ib3JjaGFyZHQtbG9ob2VsdGVyQGV1cm9pbW11bi5kZQ==