 Teodoro del Ser1*
Teodoro del Ser1* Elizabeth Valeriano-Lorenzo1
Elizabeth Valeriano-Lorenzo1 Luis Jáñez-Escalada1,2
Luis Jáñez-Escalada1,2 Marina Ávila-Villanueva1
Marina Ávila-Villanueva1 Belén Frades1
Belén Frades1 María-Ascensión Zea1
María-Ascensión Zea1 Meritxell Valentí1
Meritxell Valentí1 Linda Zhang3
Linda Zhang3 Miguel A. Fernández-Blázquez1
Miguel A. Fernández-Blázquez1- 1Clinical Department, Alzheimer's Center Reina Sofia—CIEN Foundation, Madrid, Spain
- 2Institute of Knowledge Technology, Complutense University, Madrid, Spain
- 3Neuroimaging Department, Alzheimer's Center Reina Sofia—CIEN Foundation, Madrid, Spain
Background: The relative importance of different components of cognitive reserve (CR), as well as their differences by gender, are poorly established.
Objective: To explore several dimensions of CR, their differences by gender, and their effects on cognitive performance and trajectory in a cohort of older people without relevant psychiatric, neurologic, or systemic conditions.
Methods: Twenty-one variables related to the education, occupation, social activities, and life habits of 1,093 home-dwelling and cognitively healthy individuals, between 68 and 86 years old, were explored using factorial analyses to delineate several dimensions of CR. These dimensions were contrasted with baseline cognitive performance, follow-up over 5 years of participants' cognitive trajectory, conversion to mild cognitive impairment (MCI), and brain volumes using regression and growth curve models, controlling for gender, age, marital status, number of medications, trait anxiety, depression, and ApoE genotype.
Results: Five highly intercorrelated dimensions of CR were identified, with some differences in their structure and effects based on gender. Three of them, education/occupation, midlife cognitive activities, and leisure activities, were significantly associated with late-life cognitive performance, accounting for more than 20% of its variance. The education/occupation had positive effect on the rate of cognitive decline during the 5-year follow up in individuals with final diagnosis of MCI but showed a reduced risk for MCI in men. None of these dimensions showed significant relationships with gray or white matter volumes.
Conclusion: Proxy markers of CR can be represented by five interrelated dimensions. Education/occupation, midlife cognitive activities, and leisure activities are associated with better cognitive performance in old age and provide a buffer against cognitive impairment. Education/occupation may delay the clinical onset of MCI and is also associated with the rate of change in cognitive performance.
Introduction
Epidemiological, clinical, neuropsychological, and neuroimaging studies have shown that cognitive training and other social and mentally stimulating activities have protective effects against the clinical and cognitive manifestations of neural injuries or neurodegeneration (Ikanga et al., 2017; Stern et al., 2018; Nunes and Silva Nunes, 2021). Cognitive reserve (CR) is a theoretical construct proposed to account for those observations in clinical, epidemiological (Stern et al., 2018), and cognitively healthy (CH) cohorts (Opdebeeck et al., 2016). Individuals with higher proxy markers of CR demonstrate better cognitive performance and lower rates of prevalent and incident dementia (Pettigrew and Soldan, 2019).
There is a lack of consensus on the best measure of CR construct (Harrison et al., 2015; Nogueira et al., 2022). It is usually operationalized as education level (O'Shea et al., 2015), but other variables, such as occupation attainment (Hakiki et al., 2021); reading level (O'Shea et al., 2015); intelligence quotient (Whalley et al., 2015), engagement in cognitively stimulating activities (Opdebeeck et al., 2016), a composite of education, labor, leisure, and social activities (Harrison et al., 2015); or a questionnaire designed for this purpose (Nucci et al., 2012; Kartschmit et al., 2019), are also used as proxies of CR. CR is assumed to accumulate over a life span (Xu et al., 2019; Song et al., 2022) with different components (Rouillard et al., 2017), but the relative importance of the effects of each one on cognitive performance and prevention or delay of late decline has not been comprehensively tested (Rouillard et al., 2017). The relationships between the level of CR and longitudinal cognitive trajectories and outcomes in CH people, as well as its structural brain substrates, are also unclear (Pettigrew and Soldan, 2019).
This study has three main objectives: the first one is to identify the internal structure of CR and quantify its different dimensions by means of a multidimensional analysis of a set of cognitive, social, and leisure activities undertaken during childhood and adulthood by a cohort of CH older people. The second one is to examine in the longitudinal assessment of this cohort the associations of these CR dimensions with a baseline cognitive performance, the clinical status over a 5-year follow-up, and the cognitive trajectory of individuals with persistent cognitive normality and those who converted to mild cognitive impairment (MCI). Finally, the associations of these CR dimensions with some measures of brain volume, as proxy markers of brain reserve, have been also ascertained (Supplementary Table 1). Our analyses were guided by three hypotheses: (a) several different dimensions can be disclosed in the CR construct; (b) CR dimensions have a positive but different effect on cognitive performance, cognitive decline, and cognitive trajectory; and (c) CR may have a positive effect on brain volume (Supplementary Table 1). Since the components of these CR dimensions, as well as cognitive trajectories in older cohorts (Levine et al., 2021) and brain volumes show differences between men and women, the analyses have also been performed by gender.
Methods
Setting and subjects
The Vallecas Project is an ongoing single-center, multidisciplinary, observational, longitudinal cohort study planned to identify early markers of cognitive impairment in the elderly (Olazarán et al., 2015). The participants are home-dwelling volunteers aged 68 to 86 years at baseline, without previous relevant psychiatric (schizophrenia, bipolar disorder, major depression), neurologic (stroke with cognitive or motor sequelae, head trauma with loss of consciousness, structural brain lesions, epilepsy, brain infections, mental retardation), or systemic (active carcinoma, alcohol or drug abuse, nutritional deficiencies) disorders. They were recruited between 2011 and 2013 through radio, TV, and leaflet campaigns and through visits to centers for the elderly in Madrid, Spain. After giving informed consent, they undertook annual systematic assessments (Figure 1) including sociodemographic data, family history of neurological and psychiatric diseases, medical history, lifestyle habits, neurological and neuropsychological exams, blood collection, and brain magnetic resonance imaging (MRI) scans. The Vallecas Project was approved by the Ethics Committee of the Carlos III Health Institute.
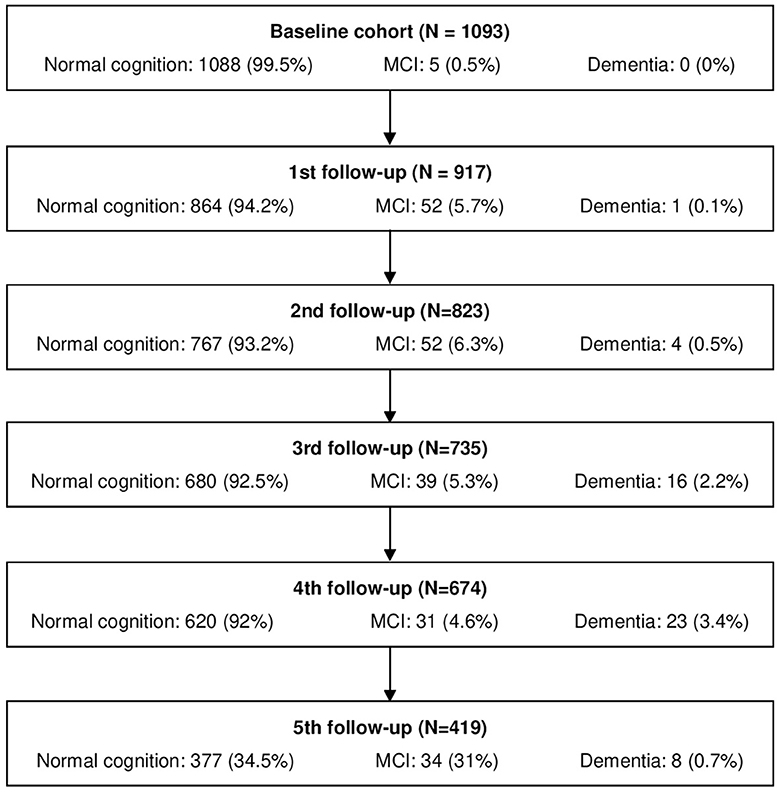
Figure 1. Individuals in the survey at every yearly assessment. MCI, mild cognitive impairment.
A total of 2,077 individuals were screened, of which 1,169 were finally included in the Vallecas Project database. This study has been performed with the data obtained at baseline and in five follow-up assessments of 1,093 participants (702 women, 64.2%) who provided the selected variables, accounting for 4,235 person-year assessments and aged 74.1 ± 3.9 years at baseline.
Variables
Five sets of variables were selected from the Vallecas Project database:
Reserve-related variables according to the current definition of CR (Harrison et al., 2015; Ikanga et al., 2017; Stern et al., 2018) recorded at baseline.
(a) Education: education level (less than primary school, primary school, high school, more than high school), number of languages spoken (Spanish; two languages from Spain; Spanish and one foreign language; three or more languages), additional professional education in adulthood (none; 1–2 courses; 2–5 courses; >5 courses)
(b) Occupation: occupation level (not qualified, manual worker, qualified worker, professional, manager) and years worked
(c) Life habits in midlife (30–65 years): A questionnaire was designed for the purposes of this project using the Lifetime of Experiences Questionnaire (Valenzuela and Sachdev, 2007) as a model. Thus, 16 items referring to everyday activities that require or provide cognitive experience were selected (artistic activities, social activities, light physical exercise, moderate physical exercise, news and newspapers, electronic devices, music listening, reading, writing, traveling, hobbies, card games, intellectual games, collecting, attending lectures, and attending shows). Participants scored every item on a 5-point scale (0: never; 1: less than once a month; 2: every month; 3: every 2 weeks; 4: every week). Of these life habits, 1–30% were missing data for several variables. Because the missing data were not randomly missing, multiple imputations were obtained based on the maximal likelihood multiple imputation method. No data were available about the life habits during the participants' young adulthood.
All the CR-related quantitative variables were standardized, and the ordinal variables were treated with the conditional median scoring approach (Chen and Wang, 2014) to obtain z-scores and better fit the requirements of factor analyses.
Cognitive assessments
An extensive neuropsychological battery was administered at every visit to the Vallecas Project (Olazarán et al., 2015). We selected for this study a subset of cognitive parameters that track most of the cognitive spectrum and are associated with a higher risk of conversion to MCI (Fernández-Blázquez et al., 2016; Del Ser et al., 2019): general cognitive status [Mini Mental State Examination [MMSE] (Folstein et al., 1975)], episodic memory [total immediate and delayed recall in the Free and Cued Selective Reminding Test (Buschke, 1984)], language (fluency of animals in 1 min), visuo-constructive ability [clock drawing test (Cacho et al., 1999)], and attention and executive functioning [digit-symbol test (Wechsler, 1997)]. The scores in those tests recorded at baseline and at five annual assessments were taken for analyses. The raw scores, excluding MMSE, were transformed to z-scores and averaged to obtain a global z-composite cognitive score for every individual at every assessment. To handle data sets with omissions due to the attrition of the cohort, cognitive data lost during the follow-up were obtained by multiple imputations based on the predictive mean matching method, especially recommended for non-normally distributed variables, using 50 imputed data pools.
Clinical diagnosis
The cognitive status of every participant was diagnosed at baseline and at every follow-up visit with a consensus between the neurologist and the neuropsychologist, taking into account their age, functional status, cognitive performance (Olazarán et al., 2015), and brain MRIs indicating CH, MCI, or dementia. The criteria from the National Institute on Aging-Alzheimer's Association (Albert et al., 2011) and from the Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision (Olazarán et al., 2015), were used to diagnose MCI and dementia, respectively. The age at the time of the MCI diagnosis was established for every individual.
Groups
The individuals were divided into two groups according to their diagnosis during the follow-up: those who were CH throughout the follow-up period and those who converted to MCI at any time during the follow-up period.
Brain volumes and atrophy
At baseline (Olazarán et al., 2015), 974 3T MRI brain scans were available from 974 participants. A T1-weighted image for every subject was segmented into gray matter, white matter, and cerebrospinal fluid (CSF) volumes using SPM12 software (http://www.fil.ion.ucl.ac.uk/spm/, version 6225), and total intracranial volume (TIV) was obtained by summing the three volumes. The percentage of TIV represented by CSF was calculated as a proxy of brain atrophy, and the gray and white matter volumes were corrected by TIV.
Covariates
ApoE genotypes [rs429358 and rs7412, determined by real-time polymerase chain reaction (Calero et al., 2009)], gender, and age, as well as the number of medications taken, trait anxiety [State-Trait Anxiety Inventory (Spielberger et al., 1970)], marital status (non-married [single, divorced, or widowed] vs. married), and depressive symptoms [Geriatric Depression Scale (Sheikh and Yesavage, 1986)] at baseline, were used as covariates. Brain atrophy was also a covariate to better assess the effects of CR dimensions, separating out their interactions with aged brain status (Stern et al., 2018).
Statistical analyses
Internal structure of CR
A factor analysis of 21 variables was performed to determine the underlying dimensions of CR. The 1,093 cases from the sample were randomly separated into two groups: an exploratory factor analysis (EFA) was performed for one group and a confirmatory factor analysis (CFA) was performed for the other group as a cross-validation procedure (Anderson and Gerbing, 1988) of the model. Multivariate normality (p < 0.05), kurtosis, and asymmetry tests (indices > 2) were previously checked.
EFA
The unweighted least squares for factorial estimation and the oblique rotation solution were used. The best model was selected according to the following criteria: (1) communality of the variables; (2) goodness of fit according to the chi-square difference test (Δχ2), Tucker–Lewis index (TLI; ≥0.95), and root mean square error of approximation (RMSEA; ≤ 0.05); (3) average variance extracted for the model; (4) factor loadings; and (5) correspondence of the obtained factors with previous literature.
CFA
The best model selected from the EFA was tested using CFA. Every observed variable was fixed to its respective latent dimension following the structure of CR explored with the EFA. The factor loadings and the correlations between the latent variables were estimated. The weighted least square means and the adjusted variance were used as methods for estimation. The average variance extracted and the construct reliability were analyzed.
Multigroup invariance analysis
In the final structure of CR, with five latent dimensions, the whole sample was tested with a multigroup invariance analysis by gender to determine if the model of CR was measured consistently in both groups. Configural, weak metric, and partial-weak metric invariances, as nested models, were compared to test the hypotheses that the number of factors (configural invariance), and the factor loadings (weak metric invariance) were similar across groups. The Δχ2 and the difference of CFI of < 0.01 were used to compare the two models (Vandenberg and Lance, 2000).
Relationships of CR dimensions
Association of CR dimensions with cognitive performance
Multiple regression analyses were performed with every cognitive test score as the dependent variable and the factorial scores in the CR dimensions as independent predictors. These analyses were performed for the sample of 973 individuals (334 men, 631 women) who had factorial scores in the CR dimensions and had provided data for all the cognitive variables and the nine covariates.
Association of cognitive reserve dimensions with MCI
Cox regression analyses were performed with those who converted to MCI during the 5-year follow-up as a dependent variable. Time to event was the time from baseline until the exam when the diagnosis of MCI was made or until the last exam in persistently CH cases who were censored by the date of their last assessment. These analyses were performed for 843 individuals (300 men, 543 women) who were followed up for 4.24 ± 1.5 years with at least one follow-up visit, including 94 (37 men, 57 women) who had converted to MCI.
In all these analyses, the dimensions of CR, the demographic covariates, and brain atrophy were introduced in independent blocks to reduce the effect of collinearity and multiple testing. The regression analyses were performed separately for every gender group, using the factorial scores of the CR dimensions in the corresponding factorial model and for the whole group, introducing gender as a covariate.
Association of CR dimensions with cognitive trajectory
Latent growth curve models (LGCMs) of the composite z-scores along the five follow-up assessments were performed in a sample of 973 subjects according to the structural equation modeling framework. First, a multiple indicators multiple causes model was performed to examine the effect of the diagnosis on the cognitive trajectory. It was expected that CH subjects and MCI converters had different baseline cognitive levels and rates of change across time. Second, linear and quadratic unconditional models by the cognitive-diagnosis group were compared to find the best model fit. Since these models were nested within each other, Δχ2 was used to select the best model. Finally, a conditional LGCM was performed (see Figure 2). It tested the influence of the CR dimensions and covariates on the growth factors of each diagnostic group (CH and MCI). The covariates considered in the analysis were age, marital status, number of medications, trait anxiety, depression, brain atrophy at baseline, gender, and number of ApoE-ε4 and ApoE-ε2 alleles.

Figure 2. Path diagram of conditional latent growth model fitted to cognitive reserve, adjusted by relevant covariates. 1Five dimensions of Cognitive reserve: education/occupation, midlife cognitive activities, leisure activities, cultural activities, and physical activities. Nine covariates such as age at baseline, marital status, number of medications, trait anxiety and depression scores at baseline, gender, number of ApoE-ε4 and ApoE-ε2 alleles, and atrophy. I, intercept; S, linear slope; Q, quadratic slope; CCS, cognitive composite score; bl, score at baseline; fu1, score at first follow-up; fu2, score at second follow-up; fu3, score at third follow-up; fu4, score at fourth follow-up; fu5, score at fifth follow-up. 1This diagram represents the latent growth curve model used for the group of individuals diagnosed with mild cognitive impairment. The model used in the group of cognitively healthy cases did not include the quadratic slope.
Association of CR dimensions with brain volumes
Similar multiple regression analyses were performed by gender, using gray matter and total volumes corrected by TIV as dependent variables and the same covariates.
R program (version 4.0.3) was employed for the factor analyses, using libraries such as psych version 2.2–5 (Revelle, 2022), lavaan version 0.6–8 (Rosseel, 2012), sem version 3.1–11 package (Fox et al., 2020), to address multiple imputations of missing data; mice version 3.13.0 (van Buuren and Groothuis-Oudshoorn, 2011), to perform the growth curve modeling; and semTools version 0.5–6 (Jorgensen et al., 2022) and SPSS (version 20), for the regression and Cox analyses. The standardized coefficients, βs, of variables and the adjusted coefficients of determination (R2) as measures of size effect are presented to respectively capture the relative effect and the explained variance of CR dimensions and covariates in the regression analyses.
Results
The demographic and clinical data of participants at baseline are summarized in Table 1. After a follow-up of 4.2 ± 1.5 years (range: 0.97–6.75 years), 112 participants (10.3%) were diagnosed with MCI at the age of 78.4 ± 4.1 years, and 31 of them (2.8%) progressed to dementia (Table 1 and Figure 1); 20 additional individuals had a diagnosis of MCI but reverted to healthy cognition before the last assessment and were considered to have cognitively normal health for the longitudinal analyses.
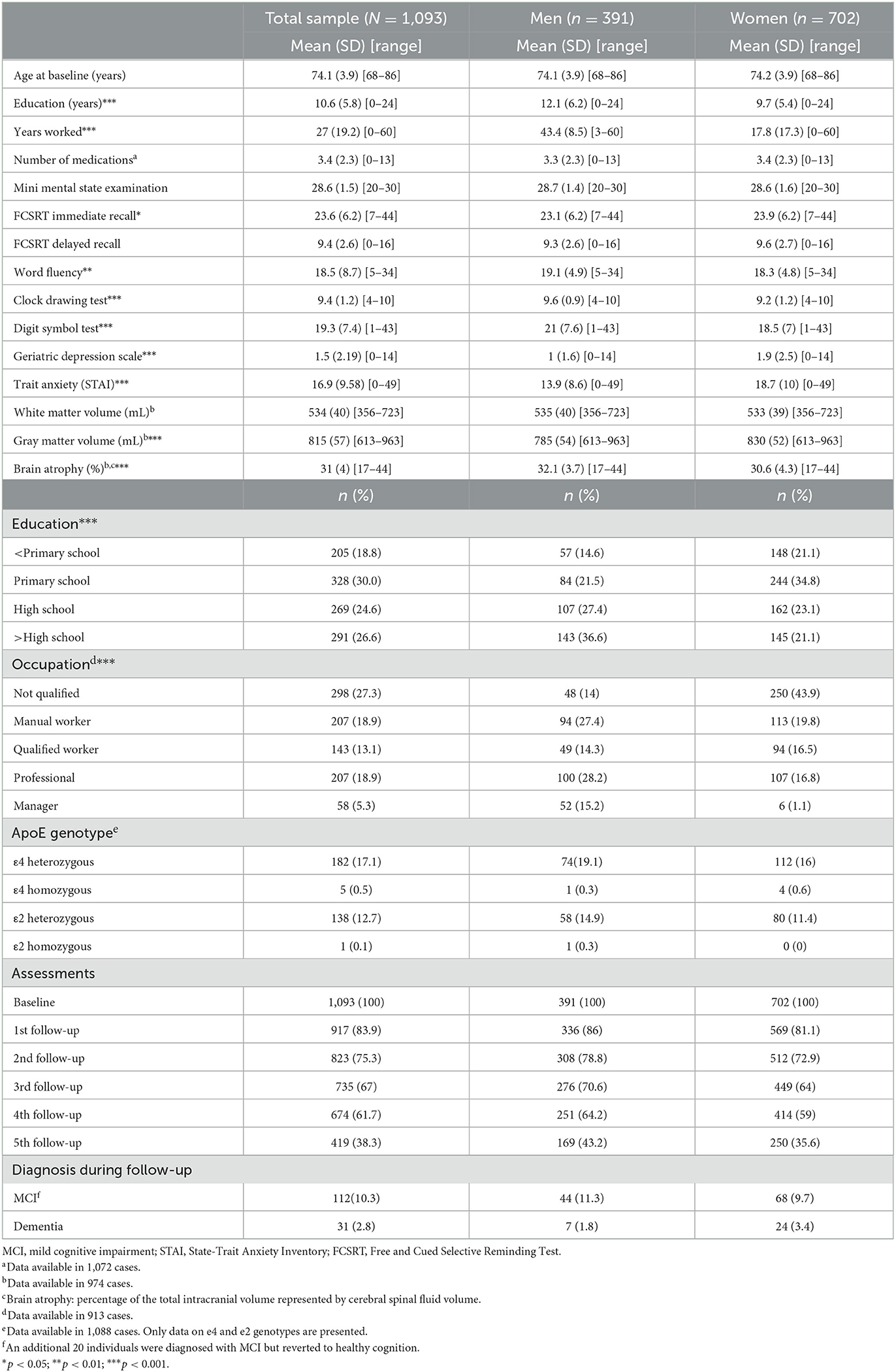
Table 1. Baseline features of the cohort.
Women had significantly lower education levels, occupation attainment, and time at work; lower scores in word fluency, the clock drawing test, and the digit symbol test; more gray matter volume and less brain atrophy; and higher scores for immediate memory, depressive symptoms, and trait anxiety (Table 1).
Internal structure of CR
EFA
An EFA was conducted with a subset of 543 subjects. The preliminary evaluations about its adequacy showed an measure of sampling adequacy of 0.89 on the Kaiser–Meyer–Olkin test and a significant Bartlett's test of sphericity (p < 0.0001). The first parallel analysis suggested five factors with observed eigenvalues greater than estimated eigenvalues. Then, factor solutions with oblimin rotation were analyzed for three models with four, five, and six factors (Supplementary Table 2). The model of five factors was selected because it explained 47% of the total variance and showed acceptable goodness of fit indices (TLI = 0.932, RMSEA = 0.05, CI 90% [0.04, 0.06]), communalities between 0.18 and 0.84, and a clearer structure of the factor loadings of the observed variables.
CFA
A structure of five CR dimensions from 21 observed variables was analyzed in the second randomly split sample of 550 subjects. The goodness of fit indices showed very good values: CFI = 0.96, TLI = 0.98, RMSEA = 0.045, CI 90% [0.041, 0.049], and standardized root mean square residual = 0.047, indicating a good fit between the model and the observed data. The omega index, between 0.61 and 0.83, indicates a high reliability of the factors. The factor loadings were also higher with values ranging from 0.32 to 0.88.
Multigroup invariance analysis
The structure of five CR dimensions obtained in the CFA was tested for multigroup invariance by gender. The Δχ2 and the difference in the CFI index demonstrated configurational invariance but not weak metric invariance. Two models of partial-weak metric invariance with three and five freed parameters were examined. After testing the four nested models, only configurational invariance was achieved (Supplementary Table 3), indicating that the structure of the five CR dimensions is the same for both genders, but the factor loadings are different between men and women.
Finally, the factor loadings (Tables 2a, b) and the factorial scores were obtained separately for men and women. According to the factor loadings, the five factors were labeled education/occupation, midlife cognitive activities, leisure activities, cultural activities, and physical activities. Each factor had an extracted variance from 29% to 52%. The five factors were significantly correlated between them in both models (r = 0.21–0.79; Tables 2a, b). The factor scores obtained for every individual were recorded and introduced in the following regression analyses.

Table 2a. Confirmatory factor analysis of 21 variables related to cognitive reserve in the sample of 702 women: factor loadings and correlations.
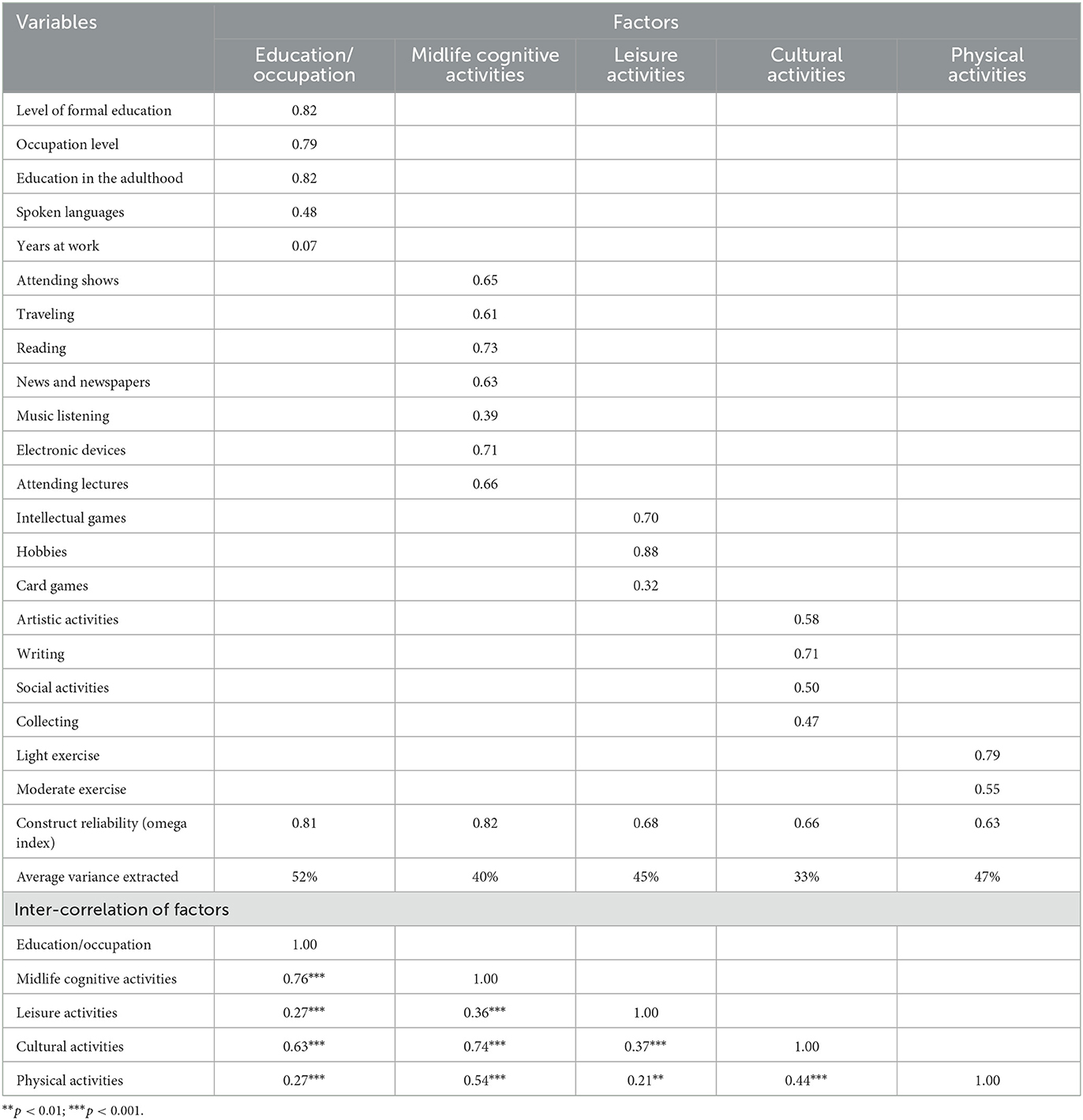
Table 2b. Confirmatory factor analysis of 21 variables related to cognitive reserve in the sample of 391 men: factor loadings and correlations.
Relationships of CR dimensions
CR dimensions and cognitive performance at baseline
The multiple regression analyses performed on the cognitive data showed that the education/occupation dimension was significantly associated with almost all the cognitive test scores (β: 0.127–0.522, p < 0.001, for most of them; Table 3a) except the clock drawing test and immediate and delayed memory in men; the leisure activities dimension was associated in both genders with immediate memory (β: .096, p < 0.01), word fluency, digit symbol test, and the composite score (β: 0.151, 0.159, and 0.141, respectively; p < 0.001; Table 3a); the midlife cognitive activities dimension was associated with immediate memory in the whole group and with the digit symbol test in women (β: 0.177 and 0.184, respectively; p < 0.05; Table 3a); and physical activities was negatively associated with the digit symbol test in men (β: −0.119, p < 0.05).
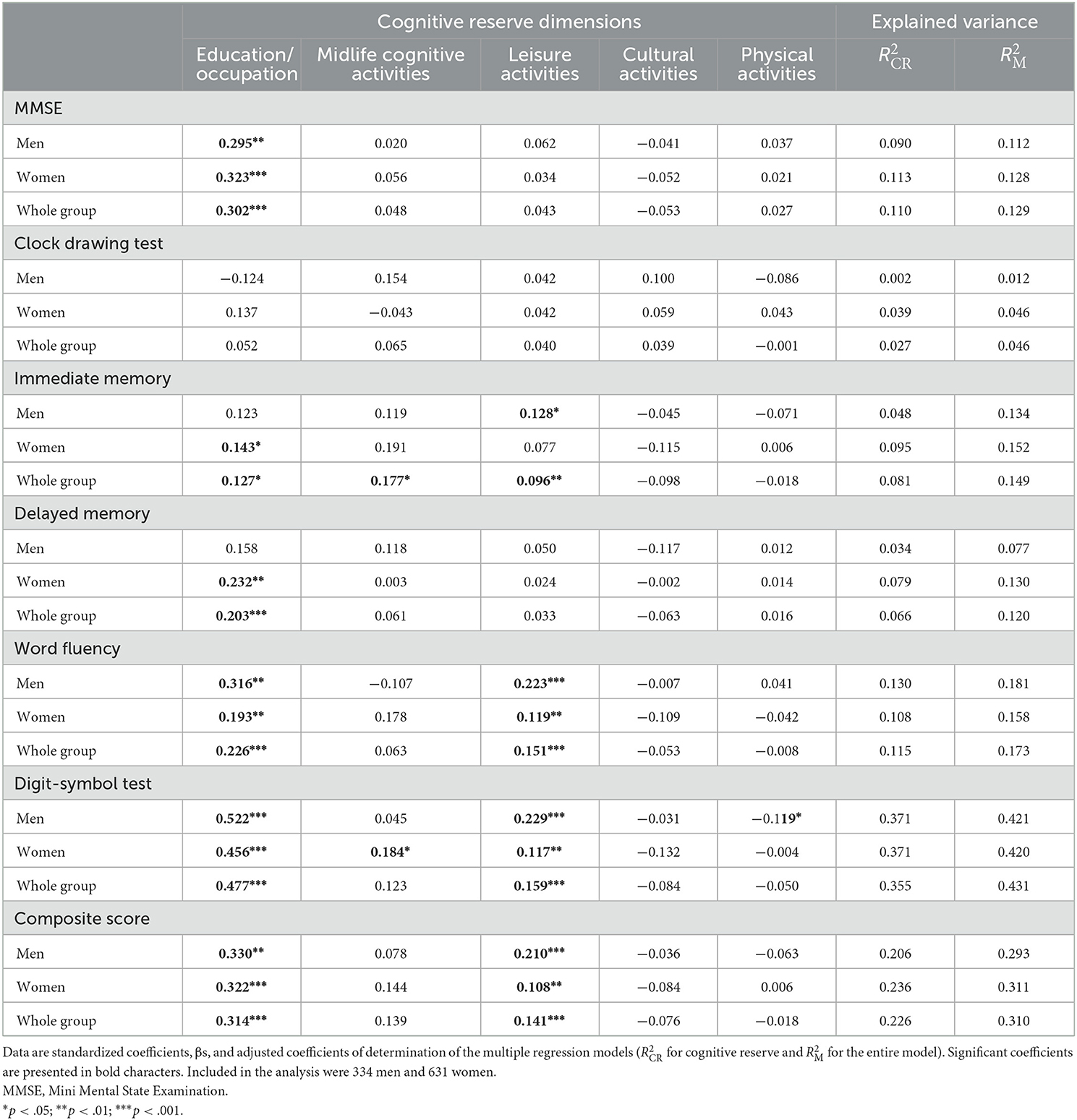
Table 3a. Association of cognitive reserve dimensions with cognitive performance by gender.
Small but significant negative effects of gender were found in the clock drawing test, word fluency, digit symbol test, and composite score (β standardized coefficients: −0.119, −0.104, −0.169, and −0.092, respectively; Table 3b). Age and depressive symptoms were significantly and negatively associated with many cognitive scores for both genders (β: −0.106 to −0.218 and −0.078 to −0.225, respectively; Table 3b), whereas trait anxiety was positively associated (β: .067–.158; Table 3b) and the number of drugs was negatively associated (β: −0.081 to 0.115; Table 3b) with several cognitive scores, mainly in women. Brain atrophy showed a significant negative association with immediate memory and the digit symbol tests in men (β: −0.115 and –.112, p < 0.05; Table 3b) and with delayed memory, word fluency, and composite scores for both genders (β: −0.077, −0.096, and −0.081, respectively, p < 0.05; Table 3b).
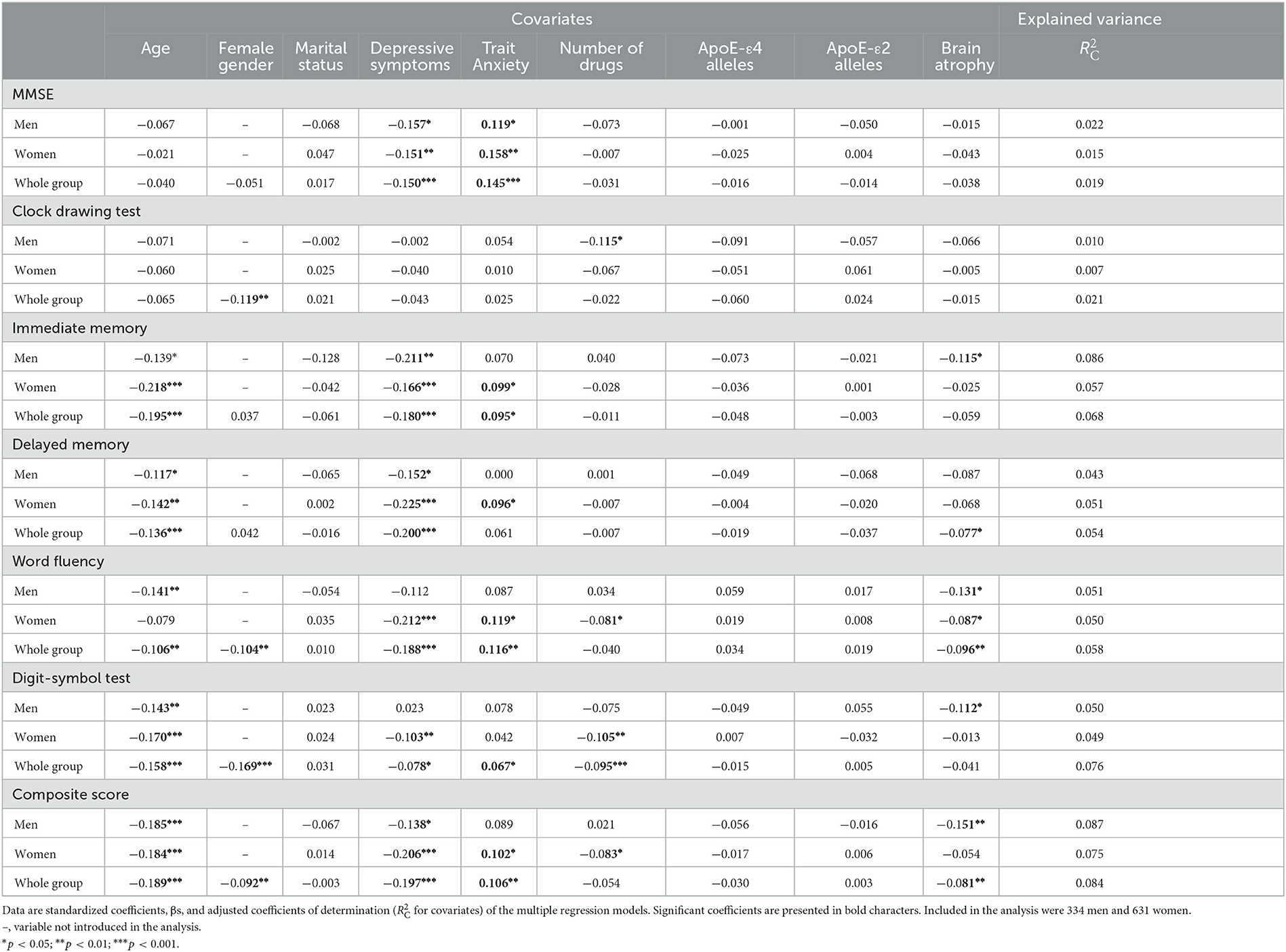
Table 3b. Association of covariates with cognitive performance by gender.
The cultural activities dimension was not significantly associated with any cognitive score. The CR dimensions only explained 3% to 13% of the variance of the cognitive scores, with the exception of the digit symbol test and the overall composite score whose explained variances were substantially higher: 37% and 23%, respectively.
CR dimensions and MCI
In the Cox regression analyses, education/occupation was significantly associated with a reduced risk of conversion to MCI in men, whereas age, depressive symptoms, ApoE-ε4 alleles, and brain atrophy were significantly associated with an increased risk for both genders (Table 4) and marital status with reduced risk, especially in women.
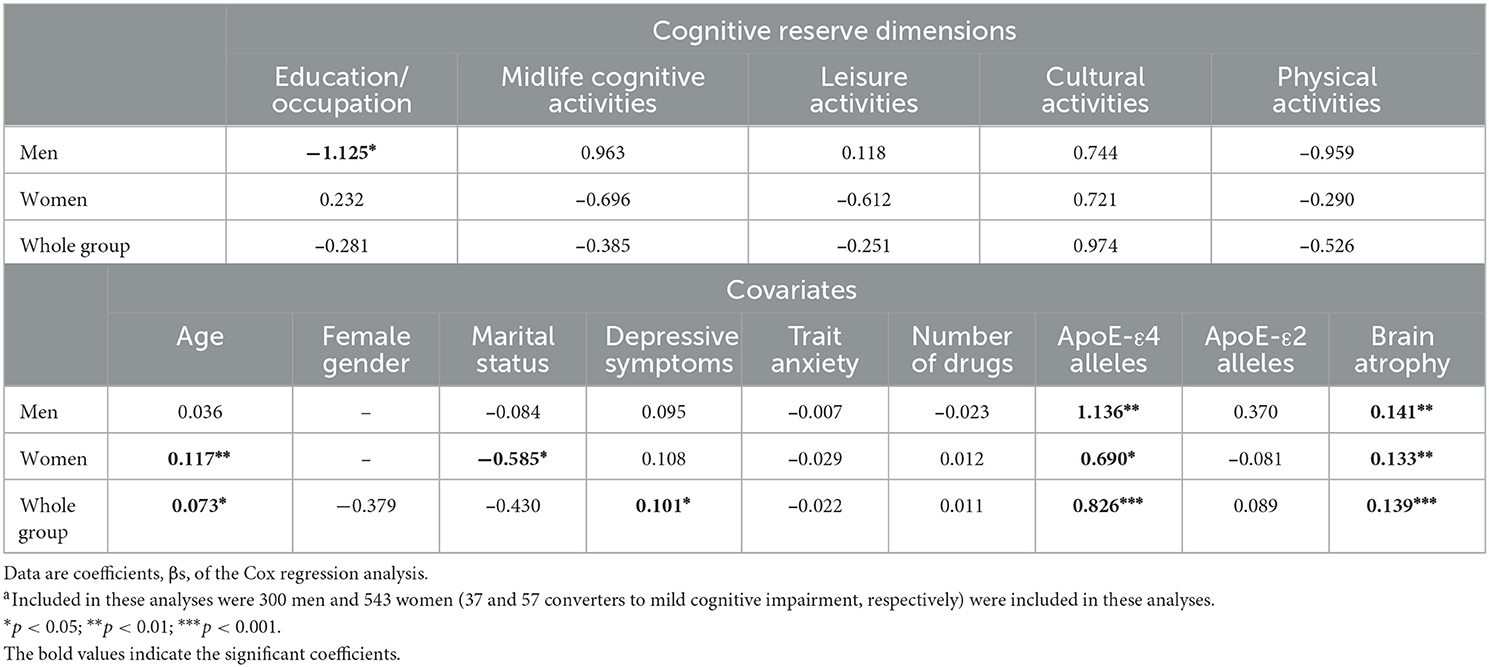
Table 4. Association of cognitive reserve dimensions with conversion to mild cognitive impairment by gendera.
CR dimensions and cognitive trajectory
The estimated initial level of the cognitive performance trajectory in CH individuals was i = 0.069; the corresponding initial value for individuals with an MCI diagnosis was significantly lower (−0.615, p < 0.01). In addition, the linear rate of change of the CH group was positive and significant (s = 0.017, p < 0.0001) but decreased (−0.149) across time in the MCI group (Figures 3A, B), confirming the research hypothesis and supporting a separate LGCM analysis for the diagnostic group.
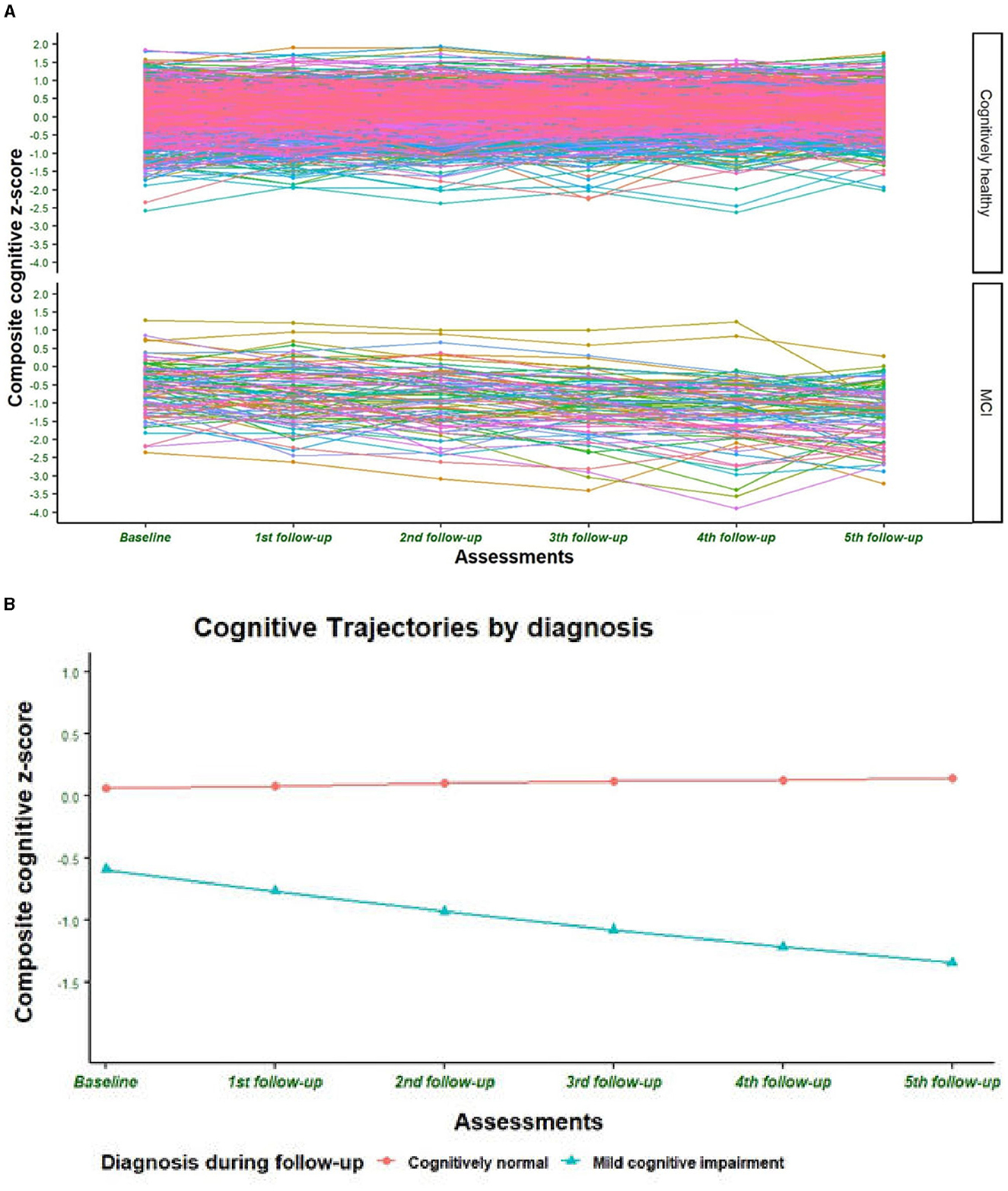
Figure 3. (A) Individual cognitive trajectories during follow-up by clinical diagnosis. The figure presents the trajectory of the composite cognitive z-score of randomly selected subjects. (B) Cognitive trajectory during follow-up by clinical diagnosis. The figure presents the estimated trajectory of the composite cognitive z-score according to the first unconditional latent growth curve model where only clinical diagnosis was introduced as an independent factor.
The second step was to select the best unconditional LGCM with the right shape of growth. The goodness of fit indices of the linear and the quadratic models were statistically similar for the CH subjects (χ2 = 14.958, df = 16; Δχ2: 6.52, p = 0.473), but they were better in the quadratic model (χ2 = 10.945, df = 12; Δχ2 = 27.33, p < 0.0001) for the subjects with MCI diagnosis (Table 5a). Therefore, a linear LGCM was performed for CH subjects and a quadratic LGCM for the MCI group with the five CR dimensions as exogenous variables and nine covariates in each model. A positive and significant association was observed between education/occupation and leisure activities with the initial levels of cognitive composite score in both groups (Table 5b and Figures 4A, B), in accordance with the regression analyses of the baseline data. The education/occupation dimension also has a negative and significant association with the rate of cognitive change in the MCI group (Figure 4A). Finally, the intercept is significantly and negatively associated with its slope in the CH group (Table 5b). For the MCI group, the higher the rate of linear change (first year), the lower the rate of quadratic change (latter years of the study) in cognitive function (Table 5b). The complete parameters estimated are shown in Supplementary Table 3.
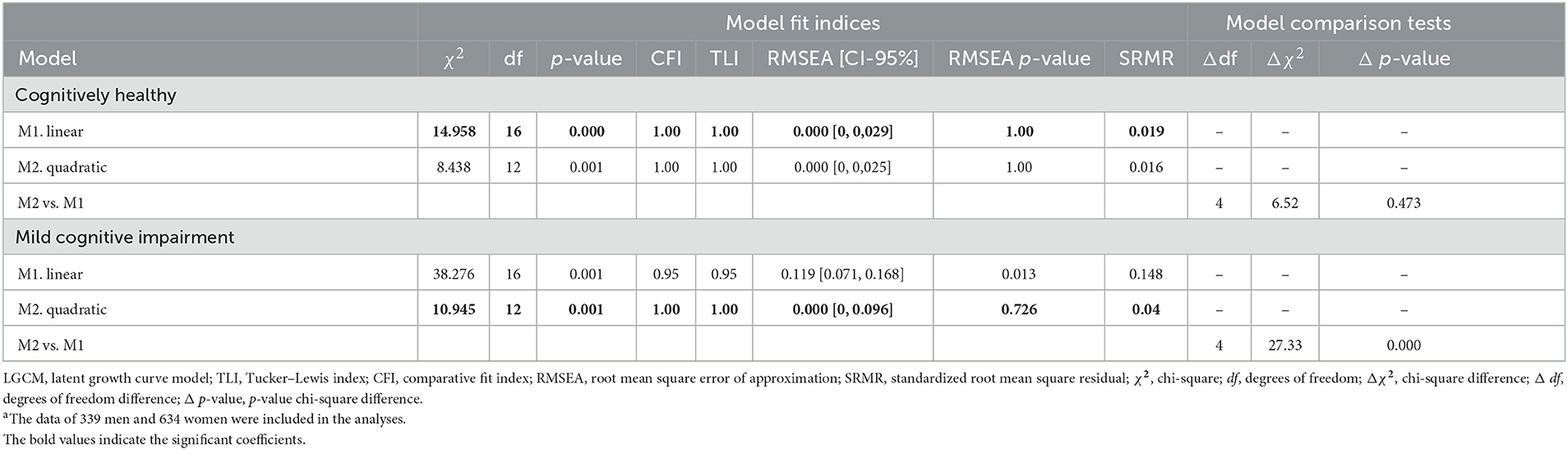
Table 5a. Unconditional latent growth curve model of the composite cognitive scorea by final diagnosis.
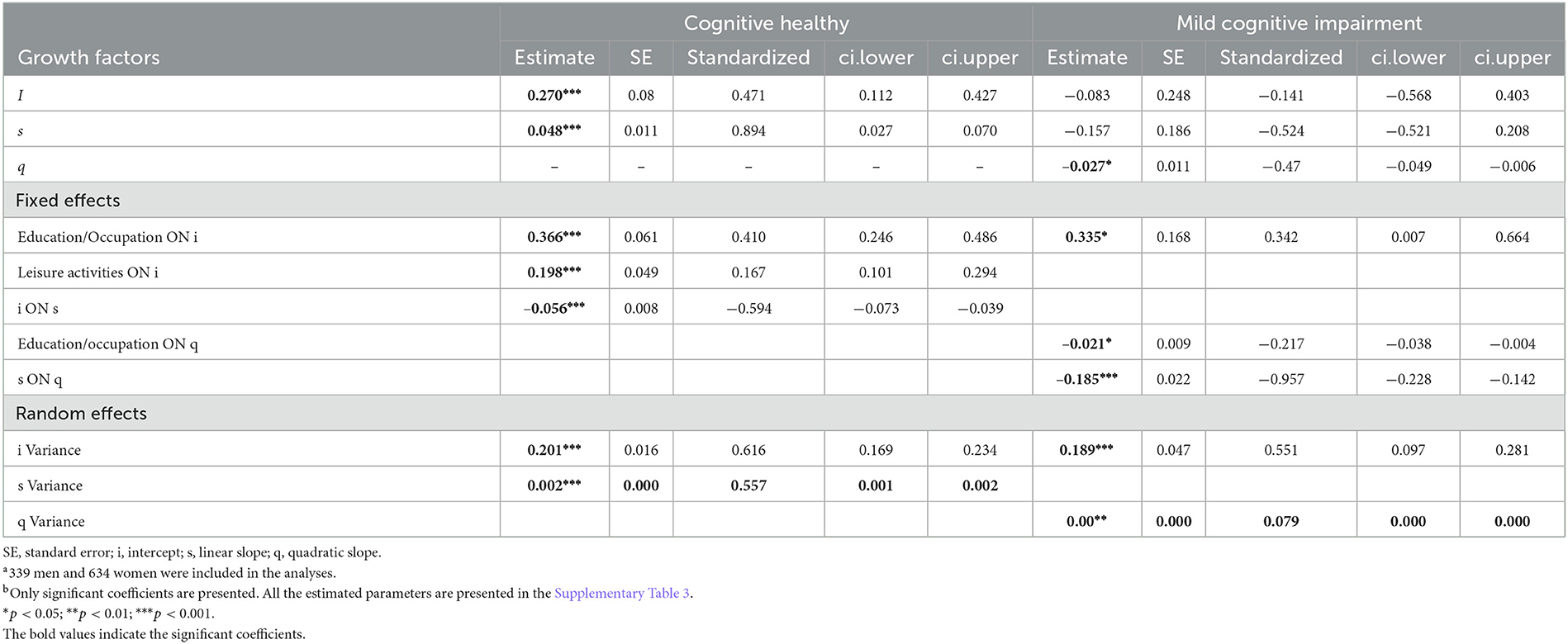
Table 5b. Conditional latent growth curve model of the composite cognitive scorea with five cognitive reserve dimensions as exogenous variables.b
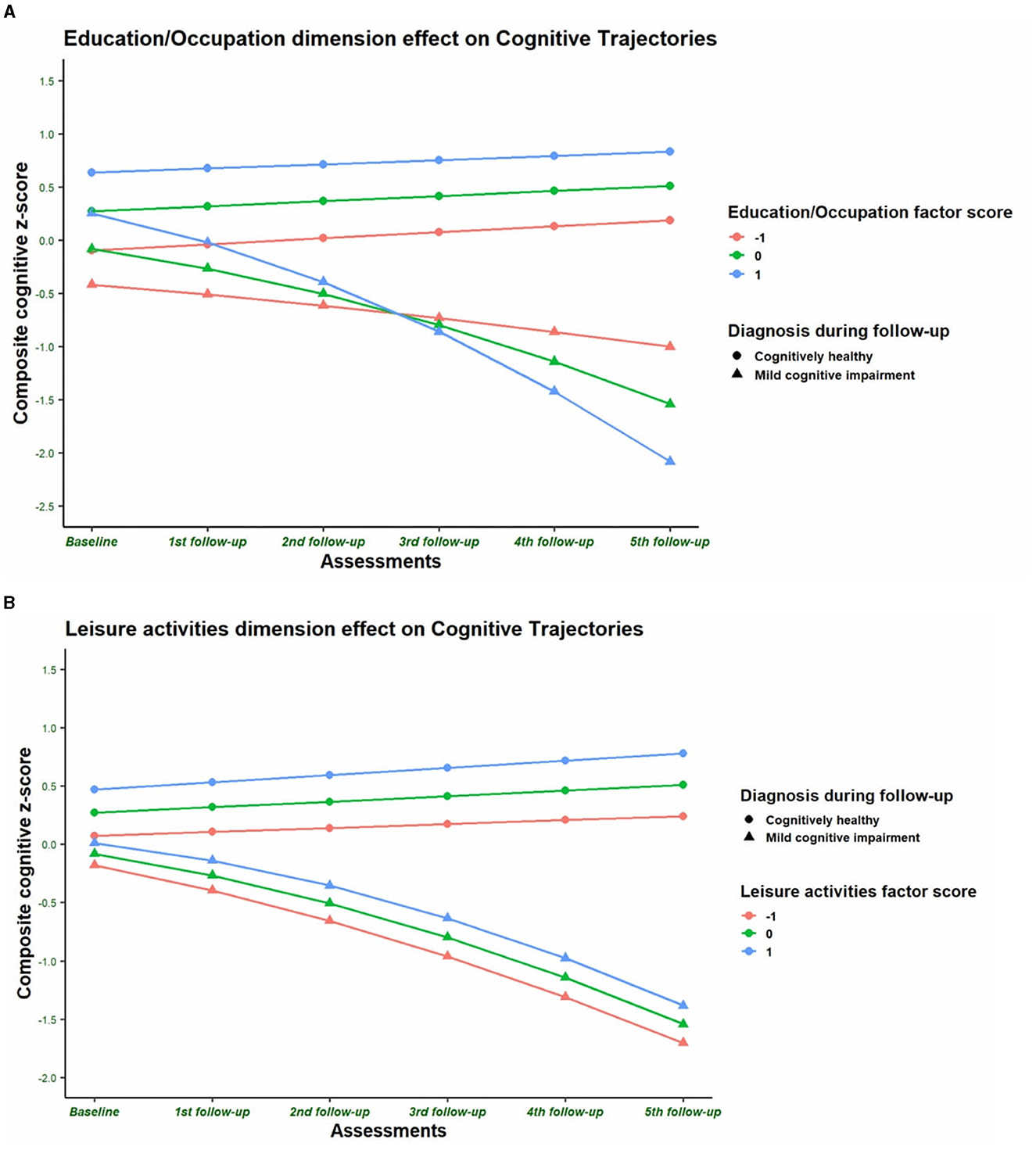
Figure 4. (A) Education/Occupation dimension effects on cognitive function across time by clinical diagnosis. (A) presents the estimated trajectories of composite cognitive z-score in the conditional latent growth curve model of individuals with three different levels of score in the cognitive recognition dimension Education/Occupation. The factor score is significantly and positively associated with the cognitive composite score (CCS) initial level of cognitively healthy subjects (p < 0.0001) and for subjects with a diagnosis of mild cognitive impairment (MCI) after follow-up (p = 0.045). Education/occupation factor score is also negatively associated with the rate of change of CCS (p = 0.015) in subjects with MCI diagnosis. The latter means that the higher the cognitive reserve in terms of education/occupation, the higher the acceleration of the change of rate of CCS in the group of MCI subjects. The conditional latent growth curve model was adjusted by covariates such as age at baseline (centered at 70 years old), gender (0 = men, 1 = women), marital status (0 = married, 1 = other), number of medications, trait anxiety and depression scores at baseline, and number of ApoE-ε4 and ApoE-ε2 alleles. (B) Leisure activities dimension effects on cognitive function across time by clinical diagnosis. (B) presents the estimated trajectories of composite cognitive z-score in the conditional latent growth curve model of individuals with three different levels of score in the cognitive reserve dimension leisure activities. The factor score is significantly and positively associated with the cognitive composite score initial level of cognitively healthy subjects (p < 0.0001). The conditional latent growth curve model was adjusted by covariates such as age at baseline (centered at 70 years old), gender (0 = men, 1 = women), marital status (0 = married, 1 = other), number of medications, trait anxiety and depression scores at baseline, and number of ApoE-ε4 and ApoE-ε2 alleles.
CR dimensions and brain volumes
The gray matter and total brain volumes were not significantly associated with any CR dimension and were negatively associated with age (β: −0.214 to 0.259, p < 0.001) and depressive symptoms (β: −0.091 to .273, p < 0.05) in both genders and with the number of medications in men (β: −0.108 and 0.130, respectively; p < 0.05; Table 6).
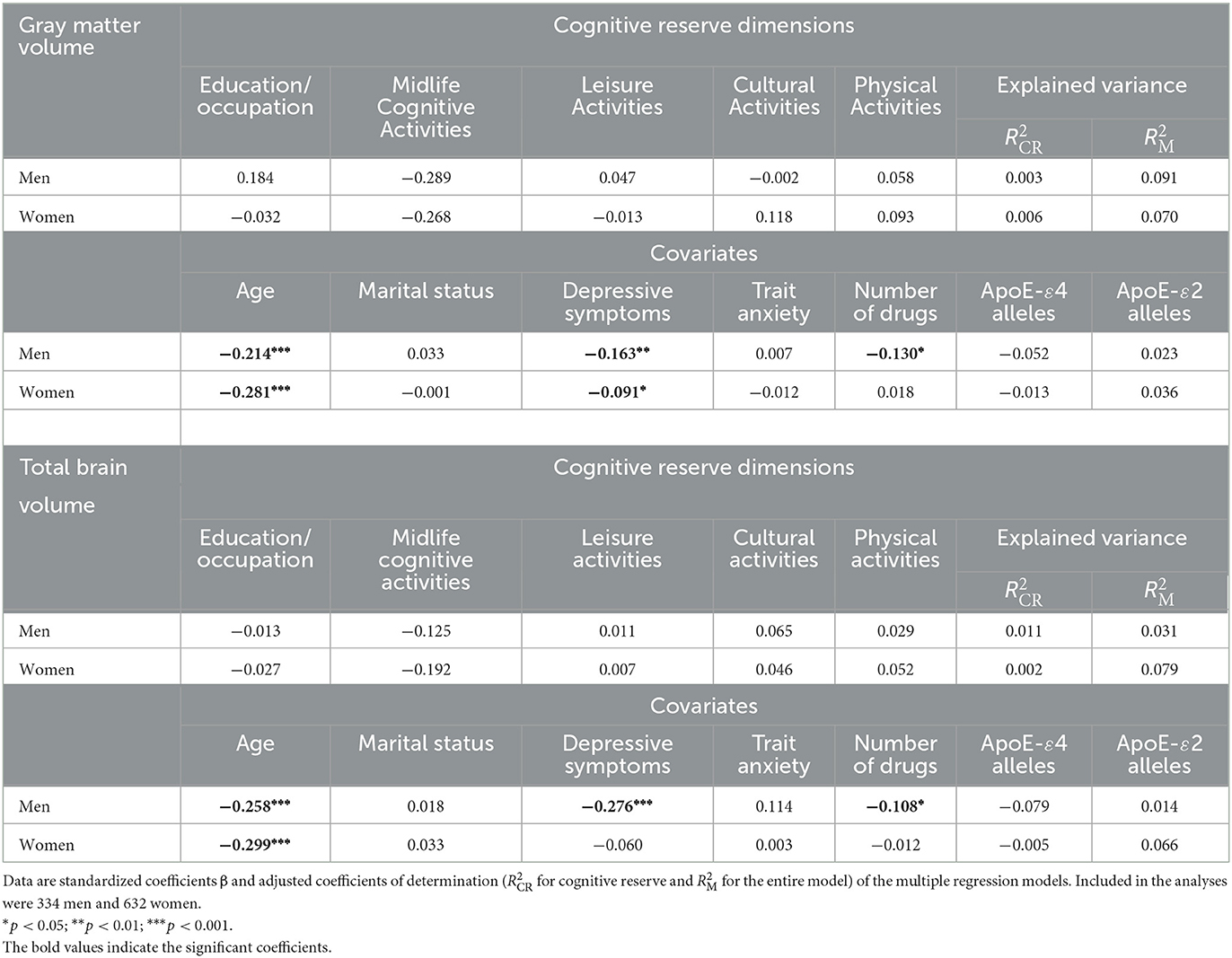
Table 6. Association of cognitive reserve dimensions with brain volumes corrected by total intracranial volume by gender.
Discussion
This study explored the dimensionality of CR and the relative association of every CR dimension with cognitive performance, trajectory, decline, and gross brain structure in a cohort of CH older adult volunteers without major neurological, systemic, or psychiatric conditions. Our hypotheses were partially confirmed: five interrelated dimensions of CR have been identified; three of them, education/occupation, midlife cognitive activities, and leisure activities, are associated with better cognitive performance and provide a buffer against cognitive impairment. A person's education/occupation may delay the clinical onset of MCI and is also associated with the rate of change in cognitive performance in the MCI group. However, these CR dimensions are not related to structural brain volumes.
The multivariate analyses of a set of 21 sociodemographic and lifestyle data, selected in accordance with the conceptual framework of the CR construct, disclosed five dimensions representing the educational, late cognitive, leisure, cultural, and physical activities from childhood to midlife adulthood in this cohort of older adult volunteers. These dimensions are rather similar to other proxy markers arbitrarily selected in previous reports (Harrison et al., 2015; Rouillard et al., 2017), but they have been empirically identified and quantified for every individual with a statistical objective tool and support the assessment of their effect size on the cognitive performance and trajectory of the cohort.
An unsurprising finding is that these five CR dimensions are highly interrelated. Consequently, the strength and relative association of every dimension with cognitive performance and trajectory could be better ascertained if all of them were considered in the statistical models. A second relevant finding is that the relative loadings of the variables presumably related to CR are significantly different between men and women. Long-lasting social and cultural norms and habits determine marked differences by gender in education, occupation, and daily activities that are supposed to generate CR (Hassing, 2020). Moreover, some biological differences in cognitive abilities may also determine a gender-specific CR (Sundermann et al., 2016) and differences in its metabolic and functional neural substrate (Malpetti et al., 2017). Therefore, it would be useful to take into account the gender effect in the analysis of CR.
The education/occupation dimension is significantly associated with almost all the cognitive domains (memory, language, visuo-constructive ability, and executive functioning) in both genders, in accordance with other previous dimensional analyses (Harrison et al., 2015; Rouillard et al., 2017; Feldberg et al., 2021) and its common use as a proxy marker of CR (Stern et al., 2018). The leisure activities dimension is also associated with several cognitive domains, and midlife cognitive activities showed modest additional relevance (Feldberg et al., 2021). Education/occupation and leisure activities strongly explain overall cognition (21% and 24% of the variance of the composite score for men and women, respectively) and seem to represent a lifestyle open to experience and engagement in stimulating actions in early and midlife associated with enhanced cognitive performance level in old age (Ihle et al., 2016). It should be emphasized that all the associations of CR with cognitive performance described in Table 3a have been observed after controlling for the estimated brain atrophy as a proxy of the overall aging effects on the brain (Stern et al., 2018).
Education, professional occupation, and participation in cognitively stimulating activities share an underlying process and are the most relevant factors of CR contributing to late cognitive functioning according to a meta-analysis of 135 studies (Opdebeeck et al., 2016) and other dimensional studies (Rouillard et al., 2017). Our study has simultaneously analyzed five dimensions of CR, verified their high collinearity, and shown that education/occupation (a marker of formal schooling and labor attainment), leisure activities, and midlife cognitive activities (surrogates of informal and cultural interests and abilities) are the main dimensions of CR associated with cognitive performance.
Previous reports (Darby et al., 2017; Lavrencic et al., 2018a; Narbutas et al., 2021) have indicated that CR differentially affects individual cognitive domains. It is significantly associated with attention, executive functions, verbal and working memory, orientation, and semantic knowledge but is not related to emotion perception, processing speed, visuospatial tasks, or motor performance. Our results showed a significant association of some CR dimensions with all the cognitive domains that we have examined. All the cognitive tests selected for our study, which are useful in assessing the cognitive decline and the transition from healthy cognitive aging to MCI (Cherbuin et al., 2010; Mura et al., 2014), as well as the overall composite score, are significantly influenced by the education/occupation dimension. However, the digit symbol test is the most strongly associated with CR dimensions that explain 37% of its variance. This finding suggests that attention, executive functions, memory, and speed of information processing assessed by the digit symbol test (Jaeger, 2018) are most related to CR as a construct. The overall estimate of the impact of CR on cognitive functioning, approximately 30% of explained variance, is in accordance with a recently published study (Martin et al., 2022).
Many previous reports also indicate that age (Lenehan et al., 2015; Li et al., 2017), depressive symptoms (Murphy and O'Leary, 2010; Rock et al., 2014; O'Shea et al., 2015; Lara et al., 2022), number of medications (Cheng et al., 2018; Khezrian et al., 2019), and brain atrophy (Stern et al., 2018) are negatively associated with cognitive performance. In contrast, trait anxiety facilitates performance in several of our cognitive tests, probably because both trait (Salthouse, 2012) and state anxiety (Potvin et al., 2013; Martinussen et al., 2019) have an inverted U-shaped relationship with cognitive performance; high levels are harmful but moderate levels may be beneficial.
A recent consensus definition of CR (Stern et al., 2018) suggests that, optimally, CR should moderate the relationship between brain and cognitive changes. However, there is no relevant brain pathology in our cohort, although age, atrophy, and other covariates can be considered surrogates of neural attrition. For this reason, the crossover analyses of the relative influence of every dimension of CR on cognitive performance at baseline are addressed within a reflective model (Jones et al., 2011). Our data indicate that CR explains more variance than these covariates. None of the CR dimensions showed a significant relationship with cognitive trajectory in the group of CH older adults during the follow-up. The latter finding has also been observed in other studies, which indicates that CR has little impact on the cognitive trajectory during aging and does not determine slower cognitive decline in CH individuals (Lane et al., 2017; Soldan et al., 2017; Lavrencic et al., 2018b; Williams et al., 2021), even in the oldest-old individuals (Hakiki et al., 2021), and no less cognitive decline post-retirement in individuals with more complex occupations (Lane et al., 2017). However, these findings should be considered with caution; protective effects on cognitive health and performance might be observed after longer periods of observation (Li et al., 2021) or in the presence of brain pathologies or functional impairment (Ihle et al., 2020). Our data and those of a similar follow-up study (Tucker-Drob et al., 2009) obtained from a cohort of CH people indicate that CR reflects the persistence of earlier differences in cognitive functioning rather than differential rates of age-associated cognitive decline. A recent revision of published data concludes that educational attainment influences late-life cognitive function primarily by contributing to individual differences in cognitive skills that emerge in early adulthood but persist into older age. The authors propose a threshold model to account for the association between educational attainment and late-life cognitive decline and dementia risk (Lövdén et al., 2020). This model is also in accordance with the association of higher CR with a faster decline observed in our group of converters to MCI and in other cohorts of MCI (Soldan et al., 2017; Kato et al., 2022) or individuals with dementia (van Loenhoud et al., 2022).
CR has been considered a relevant factor in delaying the clinical onset of cognitive decline due to neurological disease (Soldan et al., 2017; Stern et al., 2018; Pettigrew and Soldan, 2019; van Loenhoud et al., 2019; Xu et al., 2019). The incidence of MCI is more protracted in elderly people with better estimates of CR (Soldan et al., 2017; van Loenhoud et al., 2019), although CR proxies interact with gray matter volume (van Loenhoud et al., 2019) or ApoE ε4 and ε2 alleles (Pettigrew et al., 2013; Mazzeo et al., 2019; Xu et al., 2019). In this regard, in our cohort, we have also observed a risk reduction associated with the CR dimension education/occupation, but with marked differences by gender; this effect is significant only for men. Several previous studies have found that high education (Tervo et al., 2004; Rapp et al., 2013; Jia et al., 2020; Zhang et al., 2021) is protective against MCI, but other dimensions of CR were not considered, and the effect of gender was usually not reported. Differences in exposure to education and work activities by gender can determine the relevance of this CR dimension in the conversion to MCI (Liu et al., 2021). As reported in many studies, age (Middleton et al., 2007; Hughes et al., 2014; Hamer et al., 2018; Lavrencic et al., 2018b); ApoE-ε4 alleles (Tervo et al., 2004; Kryscio et al., 2006; Luck et al., 2010; Lipnicki et al., 2016); being widowed, divorced, or living alone (Jia et al., 2020); brain atrophy (Jack et al., 2005; van Loenhoud et al., 2019); and depressive symptoms (Gao et al., 2013) are positively associated with conversion to MCI in our cohort. Protective and risk factors for MCI vary by age (Sachdev et al., 2012; Wang et al., 2017) and gender (Lee et al., 2011; Sachdev et al., 2012) and may also interact between them (Hughes et al., 2014). Our data point out that CR dimensions interact with sex and other risk factors for MCI.
Finally, none of the five dimensions of CR built up during childhood and adulthood is significantly associated with baseline brain volumes in this cohort. In accordance with many previous studies, age (Sigurdsson et al., 2011; Dickie et al., 2013), depressive symptoms (Zhang et al., 2020), and the number of medications (Dieleman et al., 2017) also show negative associations. Environmental enrichment and cognitive training have produced increased brain size in experimental animal models (Milgram et al., 2006; Gelfo et al., 2017), but the effects of CR on neural tissue and brain reserve are probably mainly produced by neurogenesis (Steiner et al., 2006; Xu et al., 2015; Saraulli et al., 2017), angiogenesis (He et al., 2017), synaptic density (Ramos-Miguel et al., 2018), or connectivity (Arenaza-Urquijo et al., 2013; Bozzali et al., 2015; Perani et al., 2017; van Balkom et al., 2020; Varela-López et al., 2022). Although global volumetric assessments can hardly capture these tiny structural effects, there are recent reports of higher gray matter volume and metabolism (Arenaza-Urquijo et al., 2013) and increased cortical surface area and thickness (Andrews et al., 2021) in more educated healthy people. However, a recent study indicated that CR modulates cortical architecture only at the pre-dementia stage (Serra et al., 2022). Our study and other recent studies (Valsdóttir et al., 2022) have not been able to detect volumetric changes associated with CR dimensions, perhaps because these measures are not sensitive enough to assess brain reserve at this macroscopic level (Christensen et al., 2009). More precise cortical assessments could disclose positive findings. The studies of the effect of CR on the burden of neurodegenerative lesions are also controversial, showing no relationship (Del Ser et al., 1999; Wolf et al., 2019) or an inverse (Oveisgharan et al., 2020) relationship, probably due to similar methodological limitations and differences.
This study has some limitations. The cohort is not population-based; the selection methods and the exclusion criteria included education level, and the percentage of women was significantly higher than that of the general population of Madrid (https://datos.madrid.es) (Olazarán et al., 2015). The identification of CR dimensions is based on an extensive but limited set of sociodemographic and lifestyle variables that determine the factorial model obtained. Moreover, we have only gross structural and cross-sectional data as surrogates of brain reserve, which may not be sensitive enough to detect the biological substrate of CR probably based on functional connectivity, neural networks, and synaptic density. In addition, the reported associations between CR dimensions and cognitive performances, particularly those of midlife cognitive activities and leisure activities, may be due to reverse causality. We are aware that the relationships between CR, cognitive performance, and intelligence are very complex (Hu et al., 2022). A 5-year follow-up is short when studying the effects of CR on late cognitive abilities that may have been mainly produced during younger ages. Finally, it must be emphasized that our data, as well as other similar studies, do not prove a definite causal relationship between CR proxies and late-life cognitive performance; the alternative explanation that individuals with higher cognitive abilities at a young age are especially involved in the activities related to CR cannot be ruled out.
In summary, our study identified five dimensions of CR derived from the analysis of a set of 21 variables of early and intermediate life activities. These dimensions are highly interrelated, and their structures are similar for men and women, although they have some different components and loadings. Only three of them, education/occupation, midlife cognitive activities, and leisure activities, showed a significant association with cognitive performance late in life, but they were not associated with gross brain volumes. Although these dimensions of CR have no significant relationship with the cognitive trajectories along the 5-year follow-up period, the dimension education/occupation is associated with a risk reduction of MCI for men. These findings not only support the frequent use of education and occupation as proxy markers of CR but also indicate that other dimensions, such as midlife cognitive activities and leisure activities, and gender differences should also be considered. Our findings are also in accordance with the hypothesis that high CR reduces the risk of developing MCI and dementia because it determines better cognitive performance, provides a buffer against the clinical expression of brain disease (Rusmaully et al., 2017), delays the onset of symptoms (Soldan et al., 2017; Lavrencic et al., 2018b), and reduces the effect of neurodegenerative burden (Rusmaully et al., 2017) or the levels of cerebrovascular disease (Del Ser et al., 1999; Pettigrew et al., 2019). CR has no relevant effect on the cognitive trajectory of CH older adults (Soldan et al., 2017; Lavrencic et al., 2018b) but, in contrast, is associated with faster decline in those with MCI (Soldan et al., 2017).
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: Data can be available to any interested researcher upon request. Requests to access these datasets should be directed to TdS, dGRlbHNlckBmdW5kYWNpb25jaWVuLmVz.
Ethics statement
The studies involving humans were approved by Ethics Committee of the Carlos III Health Institute, Madrid, Spain. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
TdS: study concept and design, study supervision, data analysis and interpretation, statistical analysis supervision, and drafting of the manuscript. EV-L: study design, statistical analysis, data analysis and interpretation, and manuscript revision. LJ-E: statistical analysis and interpretation of data and manuscript revision. MÁ-V and LZ: acquisition of neuropsychological data and analysis and interpretation of data and manuscript revision. MV and M-AZ: acquisition of clinical data and analysis and interpretation of data and manuscript revision. MF-B: study design, study supervision, acquisition of neuropsychological data, and analysis and interpretation of data and manuscript revision. All authors contributed to the article and approved the submitted version.
Funding
This work was sponsored by Queen Sofia Foundation and Carlos III Health Institute. Several authors are current employees at the Alzheimer's Disease Research Unit funded by these institutions in Madrid, Spain, and have worked in the Vallecas Project, where all the data for this study were collected. The Vallecas Project is registered at the JPND Global Cohort Portal.
Acknowledgments
We are indebted to all the volunteers who participated in the Vallecas Project.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frdem.2023.1099059/full#supplementary-material
Abbreviations
CFA, confirmatory factor analysis; CH, cognitively healthy; CR, cognitive reserve; CSF, cerebrospinal fluid; EFA, exploratory factor analysis; FCSRT, Free and cued selective reminding test; i, level at the intercept; LGCM, latent growth curve models; MCI, mild cognitive impairment; MMSE, Mini Mental State Examination; s, linear slope; q, quadratic slope; TIV, total intracranial volume; TLI, Tucker–Lewis index; RMSEA, Root mean square error of approximation; SRMR, Standardized root mean square residual.
References
Albert, M. S., Dekosky, S. T., Dickson, D., Dubois, B., Feldman, H. H., Fox, N. C., et al. (2011). The diagnosis of mild cognitive impairment due to Alzheimer's disease: Recommendations from the national institute on aging and Alzheimer's association workgroup. Alzheimer's Dement. (2011) 7, 270–279. doi: 10.1016/j.jalz.2011.03.008
Anderson, J. C., and Gerbing, D. W. (1988). Structural equation modelling in practice: a review and recommended two-step approach. Psychol. Bullet. 103, 411–423. doi: 10.1037/0033-2909.103.3.411
Andrews, S. J., Fulton-Howard, B., O'Reilly, P., Marcora, E., and Goate, A. M. (2021). collaborators of the Alzheimer's disease genetics consortium. causal associations between modifiable risk factors and the Alzheimer's phenome. Ann. Neurol. 89, 54–65. doi: 10.1002/ana.25918
Arenaza-Urquijo, E. M., Landeau, B., La Joie, R., Mevel, K., Mézenge, F., Perrotin, A., et al. (2013). Relationships between years of education and gray matter volume, metabolism and functional connectivity in healthy elders. Neuroimage. (2013) 83:450-457. doi: 10.1016/j.neuroimage.2013.06.053
Bozzali, M., Dowling, C., Serra, L., Spanò, B., Torso, M., Marra, C., et al. (2015). The impact of cognitive reserve on brain functional connectivity in Alzheimer's disease. J. Alzheimers Dis. 44, 243–250. doi: 10.3233/JAD-141824
Buschke, H. (1984). Cued recall in amnesia. J. Clin. Neuropsychol. 6, 433–440. doi: 10.1080/01688638408401233
Cacho, J., García-García, R., Arcaya, J., Vicente, J. L., and Lantada, N. A. (1999). proposal for application and scoring of the Clock Drawing Test in Alzheimer's disease. Rev. Neurol. 28, 648–655. doi: 10.33588/rn.2807.98501
Calero, O., Hortigüela, R., Bullido, M. J., and Calero, M. (2009). Apolipoprotein E genotyping method by real Time PCR, a fast and cost-effective alternative to the TaqMan® and FRET assays. J. Neurosci. Methods. (2009) 183:238-240. doi: 10.1016/j.jneumeth.2009.06.033
Chen, H. C., and Wang, N. S. (2014). The assignment of scores procedure for ordinal categorical data. Sci. World J. 4, 304213. doi: 10.1155/2014/304213
Cheng, C. M., Chang, W. H., Chiu, Y. C., Sun, Y., Lee, H. J., Tang, L. Y., et al. (2018). Association of polypharmacy with mild cognitive impairment and cognitive ability: a nationwide survey in Taiwan. J. Clin. Psychiatry 79, 17. doi: 10.4088/JCP.17m12043
Cherbuin, N., Sachdev, P., and Anstey, K. J. (2010). Neuropsychological predictors of transition from healthy cognitive aging to mild cognitive impairment: the PATH through life study. Am. J. Geriatr. Psychiatry 18, 723–733. doi: 10.1097/JGP.0b013e3181cdecf1
Christensen, H., Batterham, P. J., Mackinnon, A. J., Anstey, K. J., Wen, W., Sachdev, P. S., et al. (2009). Education, atrophy, and cognitive change in an epidemiological sample in early old age. Am. J. Geriatr. Psychiatry 17, 218–226. doi: 10.1097/JGP.0b013e3181961a84
Darby, R. R., Brickhouse, M., Wolk, D. A., and Dickerson, B. C. (2017). Alzheimer's disease neuroimaging initiative. Effects of cognitive reserve depend on executive and semantic demands of the task. J. Neurol. Neurosurg. Psychiatry 88, 794–802. doi: 10.1136/jnnp-2017-315719
Del Ser, T., Hachinski, V., Merskey, H., and Munoz, D. G. (1999). An autopsy-verified study of the effect of education on degenerative dementia. Brain 122, 2309–2319. doi: 10.1093/brain/122.12.2309
Del Ser, T., Zea, M. A., Valentí, M., Olazarán, J., López-Álvarez, J., Rebollo-Vázquez, A., et al. (2019). Effects of commonly prescribed drugs on cognition and mild cognitive impairment in healthy elderly people. J. Psychopharmacol. 33, 965–974. doi: 10.1177/0269881119857206
Dickie, D. A., Job, D. E., Gonzalez, D. R., Shenkin, S. D., Ahearn, T. S., Murray, A. D., et al. (2013). Variance in brain volume with advancing age: implications for defining the limits of normality PLoS ONE 8, e84093. doi: 10.1371/journal.pone.0084093
Dieleman, N., Koek, H. L., and Hendrikse, J. (2017). Short-term mechanisms influencing volumetric brain dynamics. Neuroimage Clin. 16, 507–513. doi: 10.1016/j.nicl.2017.09.002
Feldberg, C., Barreyro, J. P., Tartaglini, M. F., Hermida, P. D., Moya García, L., et al. (2021). Estimation of cognitive reserve and its impact on cognitive performance in older adults. Appl. Neuropsychol. Adult 6, 1–11. doi: 10.1080/23279095.2021.2002864
Fernández-Blázquez, M. A., Ávila-Villanueva, M., Maestú, F., and Medina, M. (2016). Specific features of subjective cognitive decline predict faster conversion to mild cognitive impairment. J. Alzheimers Dis. 52, 271–281. doi: 10.3233/JAD-150956
Folstein, M. F., Folstein, S. E., and McHugh, P. R. (1975). “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J. Psychiatry Res. 12, 189–198. doi: 10.1016/0022-3956(75)90026-6
Fox, J., Nie, Z., and Byrnes, J. (2020). Sem: structural equation models. R Package Version 3, 1-11.
Gao, Y., Huang, C., Zhao, K., Ma, L., Qiu, X., Zhang, L., et al. (2013). Depression as a risk factor for dementia and mild cognitive impairment: a meta-analysis of longitudinal studies. Int. J. Geriatr. Psychiatry 28, 441–449. doi: 10.1002/gps.3845
Gelfo, F., Mandolesi, L., Serra, L., Sorrentino, G., and Caltagirone, C. (2017). The neuroprotective effects of experience on cognitive functions: evidence from animal studies on the neurobiological bases of brain reserve. Neuroscience (2018) 370:218-235. doi: 10.1016/j.neuroscience.2017.07.065
Hakiki, B., Pancani, S., Portaccio, E., Molino-Lova, R., Sofi, F., Macchi, C., et al. (2021). Impact of occupational complexity on cognitive decline in the oldest-old [published online ahead of print, 2020 Apr 7]. Aging Ment Health 25, 1630–1635. doi: 10.1080/13607863.2020.1746739
Hamer, M., Muniz Terrera, G., and Demakakos, P. (2018). Physical activity and trajectories in cognitive function: english longitudinal study of ageing. J. Epidemiol. Commun. Health 72, 477–483. doi: 10.1136/jech-2017-210228
Harrison, S. L., Sajjad, A., Bramer, W. M., Ikram, M. A., Tiemeier, H., Stephan, B. C., et al. (2015). Exploring strategies to operationalize cognitive reserve: a systematic review of reviews. J. Clin. Exp. Neuropsychol. 37, 253–264. doi: 10.1080/13803395.2014.1002759
Hassing, L. B. (2020). Gender differences in the association between leisure activity in adulthood and cognitive function in old age: a prospective longitudinal population-based study. J. Gerontol. B Psychol. Sci. Soc. Sci. 75, 11–20. doi: 10.1093/geronb/gbx170
He C. Tsipis C. P LaManna J. C. and Xu, K. (2017). Environmental enrichment induces increased cerebral capillary density and improved cognitive function in mice. Adv. Exp. Med. Biol. 977, 175–181. doi: 10.1007/978-3-319-55231-6_24
Hu, Y., Zhang, Y., Zhang, H., Gao, S., Wang, L., Wang, T., et al. (2022). Cognitive performance protects against Alzheimer's disease independently of educational attainment and intelligence. Mol. Psychiatry 4, 1695.
Hughes, T. F., Becker, J. T., Lee, C. W., Chang, C. C., and Ganguli, M. (2014). Independent and combined effects of cognitive and physical activity on incident MCI. Alzheimers Dem. 11, 1377–1284. doi: 10.1016/j.jalz.2014.11.007
Ihle, A., Gouveia, É. R., Gouveia, B. R., Orsholits, D., Oris, M., Kliegel, M., et al. (2020). Solving the puzzle of cognitive reserve effects on cognitive decline: the importance of considering functional impairment. Dement. Geriatr. Cogn. Disord. 49, 349–354. doi: 10.1159/000511768
Ihle, A., Oris, M., Fagot, D., Maggiori, C., and Kliegel, M. (2016). The association of educational attainment, cognitive level of job, and leisure activities during the course of adulthood with cognitive performance in old age: the role of openness to experience. Int. Psychogeriatr. 28, 733–740. doi: 10.1017/S1041610215001933
Ikanga, J., Hill, E. M., and MacDonald, D. A. (2017). The conceptualization and measurement of cognitive reserve using common proxy indicators: testing some tenable reflective and formative models. J. Clin. Exp. Neuropsychol. 39, 72–83. doi: 10.1080/13803395.2016.1201462
Jack, C. R. Jr, Shiung, M. M., Weigand, S. D., O'Brien, P. C., Gunter, J. L., Boeve, B. F., et al. (2005). Brain atrophy rates predict subsequent clinical conversion in normal elderly and amnestic MCI Neurol. 65, 1227–1231. doi: 10.1212/01.wnl.0000180958.22678.91
Jaeger, J. (2018). Digit symbol substitution test: the case for sensitivity over specificity in neuropsychological testing. J. Clin. Psychopharmacol. 38, 513–519. doi: 10.1097/JCP.0000000000000941
Jia, L., Du, Y., Chu, L., Zhang, Z., Li, F., Lyu, D., et al. (2020). Prevalence, risk factors, and management of dementia and mild cognitive impairment in adults aged 60 years or older in China: a cross-sectional study. Lancet Public Health 5, e661–e671. doi: 10.1016/S2468-2667(20)30185-7
Jones, R. N., Manly, J., Glymour, M. M., Rentz, D. M., Jefferson, A. L., Stern, Y., et al. (2011). Conceptual and measurement challenges in research on cognitive reserve. J. Int. Neuropsychol. Soc. 17, 593–601. doi: 10.1017/S1355617710001748
Jorgensen, T. D., Pornprasertmanit, S., Schoemann, A. M., and Rosseel, Y. (2022). semTools: Useful tools for structural equation modeling. R package version 0.5-6. Available online at: https://CRAN.R-project.org/package=semTools
Kartschmit, N., Mikolajczyk, R., Schubert, T., and Lacruz, M. E. (2019). Measuring Cognitive Reserve. (CR) – A systematic review of measurement properties of CR questionnaires for the adult population. PLoS ONE 14, e0219851. doi: 10.1371/journal.pone.0219851
Kato, T., Nishita, Y., Otsuka, R., Inui, Y., Nakamura, A., Kimura, Y., et al. (2022). Effect of cognitive reserve on amnestic mild cognitive impairment due to Alzheimer's disease defined by fluorodeoxyglucose-positron emission tomography. Front. Aging Neurosci. 14, 932906. doi: 10.3389/fnagi.2022.932906
Khezrian, M., McNeil, C. J., Myint, P. K., and Murray, A. D. (2019). The association between polypharmacy and late life deficits in cognitive, physical and emotional capability: a cohort study. Int. J. Clin. Pharm. 41, 251–257. doi: 10.1007/s11096-018-0761-2
Kryscio, R. J., Schmitt, F. A., Salazar, J. C., Mendiondo, M. S., and Markesbery, W. R. (2006). Risk factors for transitions from normal to mild cognitive impairment and dementia. Neurology 66, 828–832. doi: 10.1212/01.wnl.0000203264.71880.45
Lane, A. P., Windsor, T. D., Andel, R., and Luszcz, M. A. (2017). Is occupational complexity associated with cognitive performance or decline? Results from the Australian longitudinal study of ageing. Gerontology 63, 550–559. doi: 10.1159/000475559
Lara, E., Martín-María, N., Miret, M., Olaya, B., Haro, J. M., Ayuso-Mateos, J. L., et al. (2022). Is there a combined effect of depression and cognitive reserve on cognitive function? Findings from a population-based study. Psychol. Health 37, 1132–1147. doi: 10.1080/08870446.2021.1927030
Lavrencic, L. M., Churches, O. F., and Keage, H. A. D. (2018a). Cognitive reserve is not associated with improved performance in all cognitive domains. Appl. Neuropsychol. Adult. 25, 473–485. doi: 10.1080/23279095.2017.1329146
Lavrencic, L. M., Richardson, C., Harrison, S. L., Muniz-Terrera, G., Keage, H. A. D., Brittain, K., et al. (2018b). Is there a link between cognitive reserve and cognitive function in the oldest-old? J. Gerontol. A Biol. Sci. Med. Sci. 73, 499–505. doi: 10.1093/gerona/glx140
Lee, L. K., Shahar, S., Chin, A. V., Mohd Yusoff, N. A., Rajab, N., Aziz, S. A., et al. (2011). Prevalence of gender disparities and predictors affecting the occurrence of mild cognitive impairment. (MCI). Arch. Gerontol. Geriatr 54:185–191. doi: 10.1016/j.archger.2011.03.015
Lenehan, M. E., Summers, M. J., Saunders, N. L., Summers, J. J., and Vickers, J. C. (2015). Relationship between education and age-related cognitive decline: a review of recent research. Psychogeriatrics 15, 154–162. doi: 10.1111/psyg.12083
Levine, D. A., Gross, A. L., Briceño, E. M., Tilton, N., Giordani, B. J., Sussman, J. B., et al. (2021). Sex differences in cognitive decline among US adults. JAMA Netw Open 2, e210169. doi: 10.1001/jamanetworkopen.2021.0169
Li, G., Larson, E. B., Shofer, J. B., Crane, P. K., Gibbons, L. E., McCormick, W., et al. (2017). Cognitive trajectory changes over 20 years before dementia diagnosis: a large cohort study. J. Am. Geriatr. Soc. 65, 2627–2633. doi: 10.1111/jgs.15077
Li, X., Song, R., Qi, X., Xu, H., Yang, W., Kivipelto, M., et al. (2021). Influence of cognitive reserve on cognitive trajectories: role of brain pathologies. Neurology 97, e1695–e1706. doi: 10.1212/WNL.0000000000012728
Lipnicki, D. M., Crawford, J., Kochan, N. A., Trollor, J. N., Draper, B., Reppermund, S., et al. (2016). Risk factors for mild cognitive impairment, dementia and mortality: the sydney memory and ageing study. J. Am. Med. Dir. Assoc. (2017) 18:388–395.
Liu, L. Y., Lu, Y., Shen, L., Li, C. B., Yu, J. T., Yuan, C. R., et al. (2021). Prevalence, risk and protective factors for mild cognitive impairment in a population-based study of Singaporean elderly. J. Psychiatr Res. 145, 111–117. doi: 10.1016/j.jpsychires.2021.11.041
Lövdén, M., Fratiglioni, L., Glymour, M. M., Lindenberger, U., and Tucker-Drob, E. M. (2020). Education and cognitive functioning across the life span. Psychol. Sci. Public Interest 21, 6–41. doi: 10.1177/1529100620920576
Luck, T., Luppa, M., Briel, S., Matschinger, H., König, H. H., Bleich, S., et al. (2010). Mild cognitive impairment: incidence and risk factors: results of the leipzig longitudinal study of the aged. J. Am. Geriatr. Soc. 58, 1903–1910. doi: 10.1111/j.1532-5415.2010.03066.x
Malpetti, M., Ballarini, T., Presotto, L., Garibotto, V., Tettamanti, M., Perani, D., et al. (2017). Gender differences in healthy aging and Alzheimer's Dementia: a 18 F-FDG-PET study of brain and cognitive reserve. Hum. Brain Mapp. 38, 4212–4227. doi: 10.1002/hbm.23659
Martin, P., Gondo, Y., Lee, G., Woodard, J. L., Miller, L. S., Poon, L. W., et al. (2022). Cognitive reserve and cognitive functioning among oldest old adults: findings from the Georgia centenarian study. Exp. Aging Res. 5, 1–13. doi: 10.1080/0361073X.2022.2106717
Martinussen, L. J., Šaltyte Benth, J., Almdahl, I. S., Borza, T., Selbæk, G., Mcpherson, B., et al. (2019). The effect of anxiety on cognition in older adult inpatients with depression: results from a multicenter observational study. Heliyon 5, e02235. doi: 10.1016/j.heliyon.2019.e02235
Mazzeo, S., Padiglioni, S., Bagnoli, S., Bracco, L., Nacmias, B., Sorbi, S., et al. (2019). The dual role of cognitive reserve in subjective cognitive decline and mild cognitive impairment: a 7-year follow-up study. J. Neurol. 266, 487–497. doi: 10.1007/s00415-018-9164-5
Middleton, L., Kirkland, S., and Rockwood, K. (2007). Prevention of CIND by physical activity: different impact on VCI-ND compared with MCI. J. Neurol. Sci. 269, 80–84. doi: 10.1016/j.jns.2007.04.054
Milgram, N. W., Siwak-Tapp, C. T., Araujo, J., and Head, E. (2006). Neuroprotective effects of cognitive enrichment. Ageing Res. Rev. 5, 354–369. doi: 10.1016/j.arr.2006.04.004
Mura, T., Proust-Lima, C., Jacqmin-Gadda, H., Akbaraly, T. N., Touchon, J., et al. (2014). Measuring cognitive change in subjects with prodromal Alzheimer's disease. J. Neurol. Neurosurg. Psychiatry 85, 363–370. doi: 10.1136/jnnp-2013-305078
Murphy, M., and O'Leary, E. (2010). Depression, cognitive reserve and memory performance in older adults. Int. J. Geriatr. Psychiatry 25, 665–671. doi: 10.1002/gps.2404
Narbutas, J., Chylinski, D., Van Egroo, M., Bahri, M. A., Koshmanova, E., Besson, G., et al. (2021). Positive effect of cognitive reserve on episodic memory, executive and attentional functions taking into account amyloid-beta, Tau, and apolipoprotein E status. Front. Aging Neurosci. 13, 666181. doi: 10.3389/fnagi.2021.666181
Nogueira, J., Gerardo, B., Santana, I., Simões, M. R., and Freitas, S. (2022). The assessment of cognitive reserve: a systematic review of the most used quantitative measurement methods of cognitive reserve for aging. Front. Psychol. 13, 847186. doi: 10.3389/fpsyg.2022.847186
Nucci, M., Mapelli, D., and Mondini, S. (2012). Cognitive Reserve Index questionnaire. (CRIq): a new instrument for measuring cognitive reserve. Aging Clin. Exp. Res. 24, 218–26. doi: 10.1037/t53917-000
Nunes, I., and Silva Nunes, M. V. (2021). The influence of cognitive reserve in the protection of the cognitive status after an acquired brain injury: a systematic review. J. Clin. Exp. Neuropsychol. 43, 839–860. doi: 10.1080/13803395.2021.2014788
Olazarán, J., Valentí, M., Frades, B., Zea-Sevilla, M. A., Ávila-Villanueva, M., Fernández-Blázquez, M. A., et al. (2015). The Vallecas project: a cohort to identify early markers and mechanisms of Alzheimer's disease. Front. Aging Neurosci. 7, 181. doi: 10.3389/fnagi.2015.00181
Opdebeeck, C., Martyr, A., and Clare, L. (2016). Cognitive reserve and cognitive function in healthy older people: a meta-analysis. Aging Neuropsychol. Cogn. 23, 40–60. doi: 10.1080/13825585.2015.1041450
O'Shea, D. M., Fieo, R. A., Hamilton, J. L., Zahodne, L. B., Manly, J. J., Stern, Y., et al. (2015). Examining the association between late-life depressive symptoms, cognitive function, and brain volumes in the context of cognitive reserve. Int. J. Geriatr. Psychiatry 30, 614–622. doi: 10.1002/gps.4192
Oveisgharan, S., Wilson, R. S., Yu, L., Schneider, J. A., and Bennett, D. A. (2020). Association of early-life cognitive enrichment with Alzheimer disease pathological changes and cognitive decline. JAMA Neurol. 77, 1–8. doi: 10.1001/jamaneurol.2020.1941
Perani, D., Farsad, M., Ballarini, T., Lubian, F., Malpetti, M., Fracchetti, A., et al. (2017). The impact of bilingualism on brain reserve and metabolic connectivity in Alzheimer's dementia. Proc. Natl. Acad. Sci. USA. 114, 1690–1695. doi: 10.1073/pnas.1610909114
Pettigrew, C., and Soldan, A. (2019). Defining cognitive reserve and implications for cognitive aging. Curr. Neurol. Neurosci. Rep. 19, 1. doi: 10.1007/s11910-019-0917-z
Pettigrew, C., Soldan, A., Li, S., Lu, Y., Wang, M. C., Selnes, O. A., et al. (2013). Relationship of cognitive reserve and ApoE status to the emergence of clinical symptoms in preclinical Alzheimer's disease. Cogn. Neurosci. 4, 136–142. doi: 10.1080/17588928.2013.831820
Pettigrew, C., Soldan, A., Zhu, Y., Cai, Q., Wang, M. C., Moghekar, A., et al. (2019). Cognitive reserve and rate of change in Alzheimer's and cerebrovascular disease biomarkers among cognitively normal individuals. Neurobiol. Aging 88, 33–41. doi: 10.1016/j.neurobiolaging.2019.12.003
Potvin, O., Bergua, V., Meillon, C., Le Goff, M., Bouisson, J., Dartigues, J. F., et al. (2013). State anxiety and cognitive functioning in older adults. Am. J. Geriatr. Psychiatry 21, 915–924. doi: 10.1016/j.jagp.2013.01.029
Ramos-Miguel, A., Jones, A. A., Sawada, K., Barr, A. M., Bayer, T. A., Falkai, P., et al. (2018). Frontotemporal dysregulation of the SNARE protein interactome is associated with faster cognitive decline in old age. Neurobiol. Dis. 114, 31–44. doi: 10.1016/j.nbd.2018.02.006
Rapp, S. R., Espeland, M. A., Manson, J. E., Resnick, S. M., Bryan, N. R., Smoller, S., et al. (2013). Educational attainment, MRI changes, and cognitive function in older postmenopausal women from the women's health initiative memory study. Int. J. Psychiatry Med. 46, 121–143. doi: 10.2190/PM.46.2.a
Revelle, W. (2022). Psych: Procedures for Personality and Psychological Research. Evanston, Illinois: Northwestern University.
Rock, P. L., Roiser, J. P., Riedel, W. J., and Blackwell, A. D. (2014). Cognitive impairment in depression: a systematic review and meta-analysis. Psychol. Med. 44, 2029–2040. doi: 10.1017/S0033291713002535
Rosseel, Y. (2012). Lavaan: an R package for structural equation modeling. J. Stat. Software 48, 1–36. doi: 10.18637/jss.v048.i02
Rouillard, M., Audiffren, M., Albinet, C., Ali Bahri, M., Garraux, G., Collette, F., et al. (2017). Contribution of four lifelong factors of cognitive reserve on late cognition in normal aging and Parkinson's disease. J. Clin. Exp. Neuropsychol. 39, 142–162. doi: 10.1080/13803395.2016.1207755
Rusmaully, J., Dugravot, A., Moatti, J. P., Marmot, M. G., Elbaz, A., Kivimaki, M., et al. (2017). Contribution of cognitive performance and cognitive decline to associations between socioeconomic factors and dementia: a cohort study. PLoS Med. 14, e1002334. doi: 10.1371/journal.pmed.1002334
Sachdev, P. S., Lipnicki, D. M., Crawford, J., Reppermund, S., Kochan, N. A., Trollor, J. N., et al. (2012). Risk profiles for mild cognitive impairment vary by age and sex: the Sydney memory and ageing study. Am. J. Geriatr. Psychiatry 20, 854–865. doi: 10.1097/JGP.0b013e31825461b0
Salthouse, T. A. (2012). How general are the effects of trait anxiety and depressive symptoms on cognitive functioning? Emotion 12, 1075–1084. doi: 10.1037/a0025615
Saraulli, D., Costanzi, M., Mastrorilli, V., and Farioli-Vecchioli, S. (2017). The long run: neuroprotective effects of physical exercise on adult neurogenesis from youth to old age. Curr. Neuropharmacol. 15, 519–533. doi: 10.2174/1570159X14666160412150223
Serra, L., Giancaterino, G., Giulietti, G., Petrosini, L., Di Domenico, C., Marra, C., et al. (2022). Cognitive reserve modulates brain structure and cortical architecture in the Alzheimer's disease. J. Alzheimers Dis. 89, 811–824. doi: 10.3233/JAD-220377
Sheikh, J. I., and Yesavage, J. A. (1986). “Geriatric depression scale. (GDS): recent evidence and development of a shorter version,” in Clinical Gerontology: A Guide to Assessment and Intervention. (New York. The Haworth Press), 165-173. doi: 10.1300/J018v05n01_09
Sigurdsson, S., Aspelund, T., Forsberg, L., Fredriksson, J., Kjartansson, O., Oskarsdottir, B., et al. (2011). Brain tissue volumes in the general population of the elderly: the AGES-Reykjavik study. Neuroimage (2012) 59, 3862–3870. doi: 10.1016/j.neuroimage.2011.11.024
Soldan, A., Pettigrew, C., Cai, Q., Wang, J., Wang, M. C., Moghekar, A., et al. (2017). Cognitive reserve and long-term change in cognition in aging and preclinical Alzheimer's disease. Neurobiol. Aging 60, 164–172. doi: 10.1016/j.neurobiolaging.2017.09.002
Song, S., Stern, Y., and Gu, Y. (2022). Modifiable lifestyle factors and cognitive reserve: a systematic review of current evidence. Ageing Res. Rev. 74, 101551. doi: 10.1016/j.arr.2021.101551
Spielberger, C. D., Gorsuch, R. L., and Lushene, R. E. (1970). Manual for the State-Trait Anxiety Inventory. Palo Alto, CA: Consulting Psychologists Press.
Steiner, B., Wolf, S., and Kempermann, G. (2006). Adult neurogenesis and neurodegenerative disease. Regen. Med. 1, 15–28. doi: 10.2217/17460751.1.1.15
Stern, Y., Arenaza-Urquijo, E. M., Bartrés-Faz, D., Belleville, S., Cantilon, M., Chetelat, G., et al. (2018). Whitepaper: Defining and investigating cognitive reserve, brain reserve, and brain maintenance. Alzheimers Dement. 16, 1305–1311. doi: 10.1016/j.jalz.2018.07.219
Sundermann, E. E., Maki, P. M., Rubin, L. H., Lipton, R. B., Landau, S., Biegon, A., et al. (2016). Female advantage in verbal memory: evidence of sex-specific cognitive reserve. Neurology 87, 1916–1924. doi: 10.1212/WNL.0000000000003288
Tervo, S., Kivipelto, M., Hänninen, T., Vanhanen, M., Hallikainen, M., Mannermaa, A., et al. (2004). Incidence and risk factors for mild cognitive impairment: a population-based 3-year follow-up study of cognitively healthy elderly subjects. Dement. Geriatr. Cogn. Disord. 17, 196–203. doi: 10.1159/000076356
Tucker-Drob, E. M., Johnson, K. E., and Jones, R. N. (2009). The cognitive reserve hypothesis: a longitudinal examination of age-associated declines in reasoning and processing speed. Dev. Psychol. 45, 431–446. doi: 10.1037/a0014012
Valenzuela, M. J., and Sachdev, P. (2007). Assessment of complex mental activity across the lifespan: development of the Lifetime of Experiences Questionnaire. (LEQ). Psychol. Med. 37, 1015–1025. doi: 10.1017/S003329170600938X
Valsdóttir, V., Magnúsdóttir, B. B., Chang, M., Sigurdsson, S., Gudnason, V., Launer, L. J., et al. (2022). Cognition and brain health among older adults in Iceland: the AGES-Reykjavik study. Geroscience 3, 642. doi: 10.1007/s11357-023-00804-7
van Balkom, T. D., van den Heuvel, O. A., Berendse, H. W., van der Werf, Y. D., and Vriend, C. (2020). The effects of cognitive training on brain network activity and connectivity in aging and neurodegenerative diseases: a systematic review. Neuropsychol. Rev. 30, 267–286. doi: 10.1007/s11065-020-09440-w
van Buuren, S., and Groothuis-Oudshoorn, K. (2011). Mice: multivariate imputation by chained equations. R. J. Stat. Software 45, 1–47. doi: 10.18637/jss.v045.i03
van Loenhoud, A. C., Groot, C., Bocancea, D. I., Barkhof, F., Teunissen, C., Scheltens, P., et al. (2022). Association of education and intracranial volume with cognitive trajectories and mortality rates across the Alzheimer disease continuum. Neurology e1679–e1691. doi: 10.1212/WNL.0000000000200116
van Loenhoud, A. C., van der Flier, W. M., Wink, A. M., Dicks, E., Groot, C., Twisk, J., et al. (2019). Cognitive reserve and clinical progression in Alzheimer disease: a paradoxical relationship. Neurology 93, e334–e346. doi: 10.1212/WNL.0000000000007821
Vandenberg, R. J., and Lance, C. E. A. (2000). review and synthesis of the measurement invariance literature: suggestions, practices, and recommendations for organizational research. Org. Res. Methods 3, 4–70. doi: 10.1177/109442810031002
Varela-López, B., Cruz-Gómez, Á. J., Lojo-Seoane, C., Díaz, F., Pereiro, A. X., Zurrón, M., et al. (2022). Cognitive reserve, neurocognitive performance, and high-order resting-state networks in cognitively unimpaired aging. Neurobiol. Aging 117, 151–164. doi: 10.1016/j.neurobiolaging.2022.05.012
Wang, T., Xiao, S., Chen, K., Yang, C., Dong, S., Cheng, Y., et al. (2017). Prevalence, incidence, risk and protective factors of amnestic mild cognitive impairment in the elderly in Shanghai. Curr. Alzheimer Res. 14, 460–466. doi: 10.2174/1567205013666161122094208
Wechsler, D. (1997). Wechsler Adult Intelligence Scale-III. San Antonio, TX: The Psychological Corporation doi: 10.1037/t49755-000
Whalley, L. J., Staff, R. T., Fox, H. C., and Murray, A. D. (2015). Cerebral correlates of cognitive reserve. Psychiatry Res. Neuroimaging 247, 65-70. doi: 10.1016/j.pscychresns.2015.10.012
Williams, B. D., Pendleton, N., and Chandola, T. (2021). Does the association between cognition and education differ between older adults with gradual or rapid trajectories of cognitive decline? Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 1, 1–21.
Wolf, D., Fischer, F. U., and Fellgiebel, A. (2019). Alzheimer's disease neuroimaging initiative. impact of resilience on the association between amyloid-β and longitudinal cognitive decline in cognitively healthy older adults. J. Alzheimers Dis. 70, 361–370. doi: 10.3233/JAD-190370
Xu, H., Yang, R., Qi, X., Dintica, C., Song, R., Bennett, D. A., et al. (2019). Association of lifespan cognitive reserve indicator with dementia risk in the presence of brain pathologies. JAMA Neurol. 76, 1184–1191. doi: 10.1001/jamaneurol.2019.2455
Xu, W., Yu, J. T., Tan, M. S., and Tan, L. (2015). Cognitive reserve and Alzheimer's disease. Mol. Neurobiol. 51, 187–208. doi: 10.1007/s12035-014-8720-y
Zhang, Y., Natale, G., and Clouston, S. (2021). Incidence of mild cognitive impairment, conversion to probable dementia, and mortality. Am. J. Alzheimers Dis. Other Demen. 36, 15333175211012235. doi: 10.1177/15333175211012235
Zhang, Z., Wei, F., Shen, X. N., Ma, Y. H., Chen, K. L., Dong, Q., et al. (2020). Associations of subsyndromal symptomatic depression with cognitive decline and brain atrophy in elderly individuals without dementia: a longitudinal study. J. Affect. Disord. (2020) 274, 262–268. doi: 10.1016/j.jad.2020.05.097
Keywords: cognitive reserve, dimensions, cognitive performance, mild cognitive impairment, brain volume, brain atrophy
Citation: del Ser T, Valeriano-Lorenzo E, Jáñez-Escalada L, Ávila-Villanueva M, Frades B, Zea M-A, Valentí M, Zhang L and Fernández-Blázquez MA (2023) Dimensions of cognitive reserve and their predictive power of cognitive performance and decline in the elderly. Front. Dement. 2:1099059. doi: 10.3389/frdem.2023.1099059
Received: 20 November 2022; Accepted: 03 August 2023;
Published: 31 August 2023.
Edited by:
Carolyn Zhu, Icahn School of Medicine at Mount Sinai, United StatesReviewed by:
Yaakov Stern, Columbia University Irving Medical Center, United StatesCarlo Semenza, University of Padua, Italy
Copyright © 2023 del Ser, Valeriano-Lorenzo, Jáñez-Escalada, Ávila-Villanueva, Frades, Zea, Valentí, Zhang and Fernández-Blázquez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Teodoro del Ser, dGRlbHNlckBmdW5kYWNpb25jaWVuLmVz