 Josée Aoun
Josée Aoun Michel Spodenkiewicz
Michel Spodenkiewicz Catherine Marimoutou1
Catherine Marimoutou1
- 1CIC-EC 1410, Inserm, CHU de La Réunion, Saint-Pierre, France
- 2Moods Team, Inserm UMR-1018, CESP, Le Kremlin-Bicêtre, France
- 3McGill Group for Suicide Studies, Department of Psychiatry, Douglas Mental Health University Institute, McGill University, Montréal, QC, Canada
Introduction: Despite the extensive implementation of suicide prevention strategies targeting suicidal thoughts and behaviors (STB) in adolescents, there remains a concerning lack of improvement in the situation. In this comprehensive scoping review, our objective was to provide insights into prevention methods for suicidal thoughts and behaviors directed towards adolescents, including their effectiveness, public perception, and potential adaptations.
Method: A scoping review was conducted, encompassing 71 articles including systematic review, clinical trials and qualitative studies for a wider understanding. Most articles included focus generally on adolescents aged 10–20.
Results: No single intervention has shown expected effectiveness, collective efforts have laid a solid foundation for suicide prevention. Promising interventions include cognitive-behavioral therapy (CBT) and incorporating Technology-based interventions. However, challenges persist in promoting help-seeking behaviors and addressing barriers such as stigma, the natural impulsive nature of adolescents and difficulty in selecting and defining data and designs.
Discussion: This review underscores the need for a holistic approach to suicide prevention, integrating social, emotional, and psychological dimensions. Successful interventions target underlying issues like depression and loneliness rather than solely focusing on suicidal thoughts and behaviors (STB). Combining direct and indirect interventions is a sensible approach for both immediate and long-term results. Understanding Generation Z's unique needs, influenced by technology and diverse perspectives, is crucial for effective prevention.
Conclusion: Involving adolescents and adopting patient-centered healthcare with outcome measures like Patient Perceived Outcome Measures can enhance suicide prevention efforts by prioritizing safety and patient experiences.
1 Introduction
Suicidal thoughts and behaviors (STB) involve thinking about or talking about suicide, making plans to end one's life, attempting suicide, and engaging in self-harm actions that can be fatal (1, 2). Negative self-appraisal stands out as a leading predictor of reasons for dying, emphasizing its notable association with suicidality. Depressed and suicidal individuals commonly exhibit irrational thought patterns characterized by themes of self-depreciation and low self-esteem (3).
The number of youth seeking help for STB through emergency departments, emergency hotlines, aid centers, and similar resources have increased (4–7). People with STB experience ongoing distress, leading to persistent sufferance and frequent utilization of mental health facilities (8). They may not necessarily die of suicide (9), but even professionals are still unable to predict accurately who will (10).
Therefore, the objective of suicide prevention should not only focus on reducing death by suicide, but also on addressing and alleviating suicidal thoughts and behaviors, a primary risk factor for suicide alongside the major risk factors for suicidal thoughts and behaviors (11).
Adolescence is a period of vulnerability that increases the likelihood of developing STB, which can persist into adulthood and become chronic, hindering positive personal development. The adolescence phase is normally characterized by significant changes in the brain and body, including hormonal fluctuations associated with puberty, which impact mood, impulse control, and adequate decision-making abilities (12). Heightened impulsivity, quick mood changes and difficulties rationalizing risks and consequences, are all risk factor that render adolescents more vulnerable to STB (13, 14). There are some physical and biological evidences, on these risks. Brain imaging shows that group differences in surface area in the prefrontal, temporal and parietal regions, as well as in the volume of several subcortical nuclei are associated with the occurrence of suicide attempts in depressed adolescents (12, 15). Additionally, distinct patterns of serotonergic abnormalities, disruptions in the hypothalamic-pituitary-adrenal (HPA) axis, and irregularities in growth hormone (GH) secretion are associated with suicidal behaviors in adolescents (12). Exposure to suicidal behavior, particularly within the family context, and childhood adversities like abuse, neglect, and family conflict also increase the risk of STB (16). The motivation behind suicide attempts among adolescents often relates to interpersonal problems rather than financial or illness-related issues like adults (17).
Traditionally prevention is classified as primary secondary and tertiary but there is a rapid escalation of the classification of universal and selective prevention since suicidal thoughts and behavior like addiction is hard to classify as other disorders as present or absent. Universal and selective prevention are two key approaches in the continuum of prevention strategies (18, 19).
Universal prevention strategies aim to address the entire population's mental health and reduce suicide risk by removing barriers to care and increasing access to support systems. These strategies encompass public education campaigns, school-based programs, means restriction efforts, media education on responsible reporting, and crisis response plans within educational settings. By targeting the entire population rather than just high-risk individuals, universal strategies seek to enhance social support networks and coping skills on a community-wide scale.
In contrast, selective prevention strategies focus on specific high-risk groups within the population, aiming to identify and intervene with vulnerable individuals before suicidal behaviors manifest. These strategies involve screening programs, gatekeeper training for frontline caregivers, support groups tailored to at-risk populations, and improved access to crisis services and treatment. By honing in on factors such as age, sex, occupation, or family history, selective prevention endeavors to prevent the onset of suicidal behaviors among specific subpopulations, thus contributing to a more nuanced and targeted approach to suicide prevention efforts.
This classification can be applied to study feasible prevention methods in young people (20).
The objective of this literature review is to offer a comprehensive overview of prevention methods for suicidal thoughts and behaviors in adolescents. The literature search involves a comprehensive and systematic approach to identify and gather relevant studies to map the existing literature on prevention of suicidal thoughts and behaviors. It includes insights into the nature of prevention methods, their effectiveness, public perception about these methods and possible adaptations.
1.1 Identifying the research question
Is there an observable improvement in the effectiveness of both selective and universal prevention methods? Which specific approaches demonstrate significant results, and what are the identified gaps or deficiencies within current prevention methodologies?
2 Search method
This scoping follows Arksey and O'Malley's 5 stages of conducting a scoping review (21). A comprehensive literature review was conducted to examine the current knowledge regarding prevention efforts. Relevant articles were identified through searches conducted in databases such as ScienceDirect, PubMed, and Google Scholar. The search query used was {(suicide[Title/Abstract]) AND (prevention[Title/Abstract])) AND (adolescent[MeSH Terms])}. The search was concluded on April 26, 2023, and encompassed a total of 3,493 unique articles.
2.1 Identifying relevant studies and study selection
The inclusion criteria focused on
• Articles published after 2010 to ensure a contemporary approach that considers technological and social advancements, while excluding outdated methods.
• Qualitative studies, controlled trials, and systematic reviews.
The exclusion criteria focused on
• Articles of literature and narrative review, as well as editorials and commentaries, were excluded from the analysis because narrative reviews are more likely to include only research selected by the authors, which introduces bias.
• Articles that did not directly address suicide prevention
This broad inclusion is essential for a comprehensive understanding of the complex clinical and social nature of STB in adolescents. Qualitative studies provide rich insights into experiences and perspectives, informing intervention and policy development. Controlled trials evaluate the effectiveness of interventions, while systematic reviews synthesize evidence for reliable conclusions. This holistic approach enhances understanding, validity, and evidence-based decision-making. This type of rapid review might not describe research findings in any detail but is a useful way of mapping fields of study where it is difficult to visualise the range of material that might be available.
This scoping review was conducted according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Statement [Supplementary Material]. The screening and inclusion process is presented Figure 1.
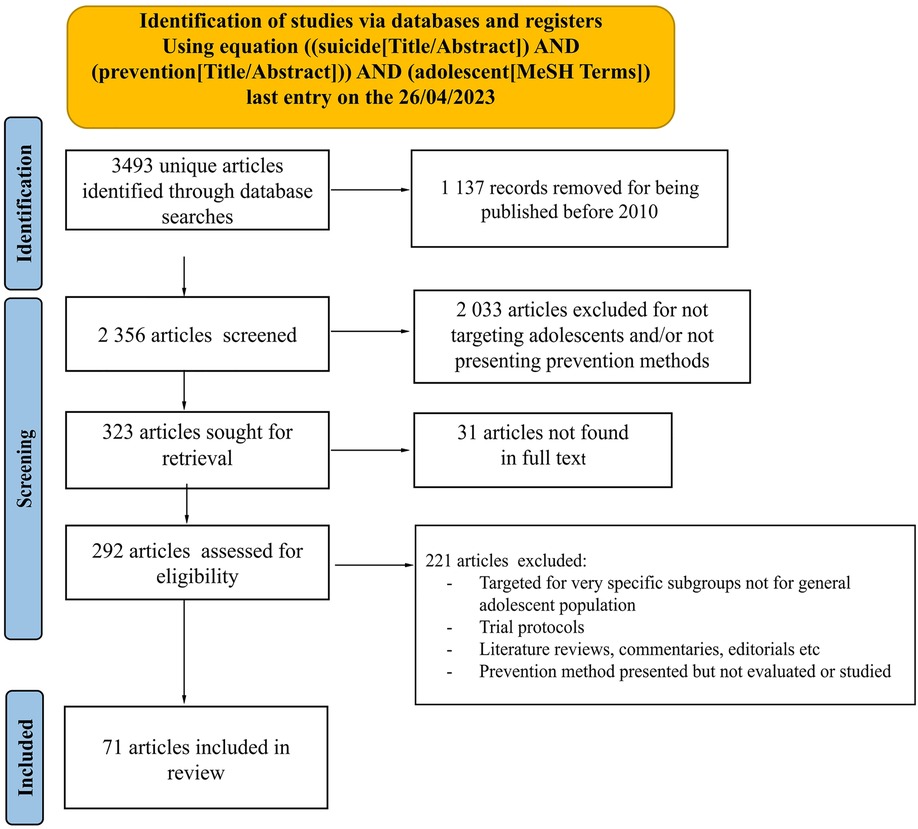
Figure 1. Prisma flowchart: identification and inclusion process.
We sequentially evaluated the titles, abstracts and then full text of all publications identified by our searches for potentially relevant publications. Disagreements were solved by consensus between the reviewers. Descriptive data were manually extracted from eligible articles. To avoid any potential misinterpretation or misrepresentation of the original findings, we quoted findings with minimal syntax modifications to ensure accuracy when conveying results of included articles. Quoted outcomes have been classified in Supplementary Table S1 detailing the author's interpretations and satisfaction of their results.
3 Results
All included articles and their main results have been grouped in the table.
In this review, we included 10 systematic reviews (22–31) and 1 meta-analysis (32) encompassing 318 studies. Despite the large number of studies included, several systematic reviews identified limited evidence regarding effective interventions for preventing adolescent suicide. The findings from these reviews were generally underwhelming, as 10 out of 11 of them revealed minimal to no effect in most studies. However, it is worth noting that the studies focusing on cognitive-behavioral therapy (CBT) methods showed some promising outcomes.
3.1 On selective prevention
3.1.1 Cognitive-behavioral therapy (CBT)
Has demonstrated effectiveness as a preventive measure against suicide. In this review, we included seven studies that explored various applications of CBT, such as BriefCBT (33), MoodRegulation-CBT (34), the adaptation of CBT into a mobile app called MEMO (35), and programs like CATCH-IT (36, 37) and EMPATHY (38). Notably, the CATCH-IT program showed significant result satisfaction. These interventions effectively target the vulnerabilities of hopelessness and difficulties in coping, which are associated with suicidal behavior. Additionally, dialectical behaviors therapy (DBT) (39, 40) has shown efficacy in preventing suicide attempts. However, the scalability of DBT and individual psychodynamic psychotherapies limits their effectiveness on a larger scale.
3.1.2 Medication and hospitalization
A study examined the frequency of lithium, clozapine, and electroconvulsive therapy (ECT) use and its correlation with suicide deaths. The findings indicated an inverse correlation between the prevalence of suicide and the frequency of using these medications, but this effect was observed mainly among male adolescents (41). While hospitalization is considered a reliable means of ensuring the safety of adolescents, both staff and patients have negative experiences (42–44), particularly in the emergency department, according to surveys and interviews, details of the interviews include reports of hospital staff displaying rudeness towards adolescents and expressing opinions that these individuals have no business being in an emergency department setting. Furthermore, participants highlighted excruciatingly long waiting times, with some indicating that the experience exacerbated their already intense subjective feelings of (STB). Some adolescents even reported being reluctant to seek help again due to their negative encounters, obstructing the promotion of help-seeking behaviors.
3.1.3 Gatekeeper programs
Due to scalability concerns, community programs offer a more viable approach. We have included multiple community and caregiver-based programs that have demonstrated significant outcomes. The primary objective of these programs is to enhance knowledge about appropriate responses and actions when faced with someone at risk of suicide, while simultaneously addressing barriers to accessing care. For example, the P and C CARE programs (45, 46), Connect program (47), and the Family Bereavement Program (FBP) have exhibited notable effectiveness, with the latter showing long-lasting effects on STB even up to a 15-year follow-up period for FBP in one study (48). Additionally, various community education programs have been implemented, specifically targeting different types of caregivers to increase their knowledge and risk management skills.
3.1.4 Coping skills program
Programs that are addressed to adolescents who have STB, such as Surviving the Teens (49, 50), Sources of Strength (51, 52), The Listening Guide (53), and Youth Awareness of Mental Health (54), share a common objective of providing adolescents with essential coping skills and risk management strategies.
3.1.5 Interventions on depression and ill being
In addition, numerous interventions originally developed to target depression or general states of ill-being, have been found to be effective in reducing suicidal thoughts and behaviors (STB), as indicated by various studies included in this review (Supplementary Table S1). The one meta-analysis specifically highlighted a multivariate meta-regression analysis that indicated that studies specifically aimed at targeting STBs had a significantly lower effect size for suicide attempts (32). Therefore, direct methods of prevention of STB appear less effective than indirect methods that target risk factors of STB such as ill being and Depression.
3.2 On universal scale prevention
Government programs have also played a significant role in addressing suicide prevention, with, for example, the Garret Lee Smith (GLS) memorial program emerging as a prominent example in the US (55, 56). This program involves community-wide efforts, funding for research, and the development of tools to combat suicide. According to the authors, over a 7-year period, the absence of the program would have resulted in 13.3 more deaths per 100,000 youths (55). Simultaneously, another study showed there were no significant difference in terms of adult suicide mortality rates the year after the implementation, making it specific for adolescents (56).
3.2.1 Community principles
A qualitative study included in this review examined how monks in Thailand adhere to doctrines for well-being and are generally joyful, with Buddhism playing a role (57). Their beliefs align with many suicide prevention principles such as knowledge of life after death, early identification of mental disorders and help seeking, and measures to control suicide methods, alcohol, and drug abuse.
3.3 Help seeking methods
Despite the implementation of numerous strategies and programs, the majority of studies have revealed that help-seeking behaviors among adolescents has not increased significantly (Supplementary Table S1). Various barriers contribute to this reluctance, including the stigma surrounding mental illness halting help seeking (22, 44, 47, 58, 59). Additionally, a lack of knowledge about available resources and how to access them poses a significant obstacle and is where gatekeeper programs could come in handy. Moreover, a lack of trust in mental health professionals or discomfort in discussing personal problems with them hinders help-seeking efforts (42, 43, 59–62). A panel of experts participated in a Delphi survey included in this review, which aimed to explore the efficacy of suicide prevention programs. Although it was emphasized that these programs should be tailored and adapted, experts identified that providing information about where to seek help was the most effective component of these programs (28). With regard to help seeking, they suggested that adolescents often confide in their friends, indicating the importance of gatekeeper programs targeting fellow adolescents to provide support and encourage assistance-seeking (28, 62).
Adolescents show overall satisfaction with suicide prevention programs and demonstrate willingness to actively contribute ideas for suicide prevention efforts. Parents, especially mothers, expressed interest in becoming essential allies in suicide prevention, as their engagement has proven to be of significant importance in addressing this issue (40, 45). In most studies, parental presence seems to be a driving factor for suicide prevention, with one study consisting of interviews of young people provided that parents and teachers were the most influential for adolescents compared to other actors like counselors or public workers (63).
3.4 Use of technology
A common theme is also the use of technology based prevention. Mobile-based technologies have demonstrated effectiveness in assessing and managing risk among vulnerable young people. Mobile apps provide increased accessibility to therapeutic interventions, particularly for at-risk individuals who may not actively seek help. They offer the opportunity for evidence-based interventions to be accessed multiple times a day, precisely when needed the most. Some examples of technology-based interventions for a selective prevention of suicide included in this review are the #chatsafeguidelines (64, 65), CalmHarm app (66), MEMO (35), and SafePlan app (67), all showed promising feasibility acceptance. Moreover, teenagers often confide in their friends, utilizing social platforms such as Instagram, including features like close friends’ stories (62), to seek support and share their experiences. These platforms can also play a role in improving help-seeking behavior. The findings extracted from the remainder of included articles (67–92) are synthesized and presented in Supplementary Table 1.
4 Discussion
The purpose of this review is to provide a comprehensive understanding of suicide prevention. Descriptive data were manually extracted from eligible articles by directly quoting the findings from clinical trials, expert analyses from systematic reviews, and the direct citations of adolescents and the general public regarding prevention strategies. While some results of suicide prevention interventions have been deemed unsatisfactory by critics and the authors themselves, this only highlights the complex nature of STB. We also observed that the most challenging aspect of suicide prevention lies in identifying and reaching out to those who suffer from STB and encouraging them to seek the necessary help.
This task becomes particularly intricate when dealing with adolescents, as they may not explicitly express a desire to die but exhibit behaviors and communication that contribute to their own depreciation. We found that help-seeking behaviors is halted by the stigma and past negative experiences, and these feelings can be partially alleviated when parents become supportive allies. Additionally, technology and its scalability factor can play a facilitative role. Therapies, which have proved to be effective, such as Cognitive Behavioral Therapy (CBT), can be adapted in the development of community programs, online guidelines, and mobile apps aimed at encouraging adolescents to seek help before self-harm occurs.
Participants of the different included studies seemed to be interested in being active members in modulating and adapting prevention methods. Surveys and qualitative studies have revealed that adolescents provide valuable insights and ideas, even when not explicitly solicited for solutions. All groups of participants (parents, counselors, mental health care professionals and adolescents) have expressed satisfaction and willingness to engage in prevention programs, despite some quantitative results falling short of expectations, highlighting a potential gap in proving method effectiveness, notably for help seeking behavior. While some critics undermine the impact of prevention programs and whether they should keep receiving funding, no alternative or specific program has emerged as the definitive solution. Even though intervention programs may not have demonstrated ground-breaking results, they still play a crucial role in initiating conversations about suicide and gradually dismantling the associated stigma (93–95), a major barrier to seeking help.
While opinions differ on how best to prevent STB, the existing research suggests that interventions targeting underlying issues like depression, loneliness, and hopelessness have been successful in indirectly reducing STB. One of the pillars of suicide prevention according to the WHO website is “foster socio-emotional life skills in adolescents”, this approach considers that adolescents needs help in developing skills that allow them to manage emotions, develop a sense of identity and empathy (96–98). STB is a symptom of deeper suffering with the root cause, general ill-being, targeted through interventions. Therefore, we emphasize the importance of treating the root causes using methods not directed towards STB, but towards underlying causes, for long-term results. In contrast, direct interventions on STB tended to have more immediate effects, which in times of crisis or extreme risks for a suicide attempt, could be very valuable (99). It could encourage patients to stay hopeful in their treatment alongside healthy momentary sufferance relief. Combining both direct and indirect interventions could be a sensible approach.
4.1 Study limitations
There were some questions raised when going through all the studies included in this review. One was the lack of detailed information about the interventions or programs being studied, especially regarding the items included in prevention programs. In order to gain a better understanding, a basic online search had to be made to visit the websites of these interventions while being mindful that websites could be biased as it was presented by the creators of the programs. Another bias was found in studies funded by program contributors.
The challenges in suicide prevention encompass two main aspects: inadequate availability of data (100) and insufficient research design (101, 102). These limitations impede our ability to accurately estimate suicide rates, evaluate the effectiveness of prevention programs and assess the impact of interventions. To overcome these challenges, it is crucial to enhance data collection and evaluation processes, taking into consideration that STB and suicide itself are not registered in a systematic uniform way worldwide. If the same coding system was implemented, this could enable us to effectively monitor the success of prevention interventions and closely track cases of hospitalized suicide attempts. The 10th revision of the International Statistical Classification of Diseases and Related Health Problems (103) identifies some elements of self-harm and also suicide attempts with a code classification, however the broad nature of suicidal thoughts and behaviors makes their classification complicated since different schools of thoughts have different agreement to what is considered suicide behavior (104, 105).
Furthermore, our research indicated a limited mention on the role of bullying in STB among adolescents. Despite bullying being associated with STB reported in emergency department (106), it was not generally addressed in the interventions and programs we reviewed. Especially noting that any participation in bullying is linked to STB in adolescnets (107).
This study has several limitations. The search terms use while extensive are not exhaustive and could have omitted multiple studies with concrete effective prevention methods. Selecting comprehensive search terms can be challenging, especially when targeted prevention for teens is relatively limited compared to adults. This study solely relied on excerpts from the included articles. This descriptive approach may lack the depth and rigor of an analytical study, potentially leading to oversimplification of complex data. By solely relying on quoted findings, there is a risk of bias as the interpretation of results may be influenced by the authors of the included studies. This review focused on finding gaps in prevention method studies directed towards adolescents. Many included studies focused on Europe and North America and East Asia limiting our understanding of prevention studies in other parts of the world.
4.2 Perspectives: understanding Generation Z perspective to adapt prevention strategies
Generation Z or Gen Z for short, born between the mid-to-late 1990s and the early 2010s experiencing a dynamic demographic landscape (108). Renowned for being digital natives, they are the first cohort to grow up with widespread access to technology and the internet, displaying impressive proficiency in utilizing various technological platforms and social media. Additionally, Gen Z is widely recognized for their social-mindedness and progressive outlook, actively advocating for issues such as climate change, social justice, and equality. They demand purpose and accountability from institutions, tirelessly striving for greater equity and sustainability (108, 109).
When considering suicide prevention methods for adolescents, it is important to note that generations do not have the same adolescence, each generation has its particularities. Millennials who experienced their adolescence from mid 1980s to mid 1990s cannot be compared to the adolescence of our current young generation GenZ since the socio-cultural and economic situation of the globe is now vastly different. In addition, our scientific understanding of adolescence has seen major improvements, and we now know that adolescents are in a distinct stage of development that differs greatly from adulthood.
Although we are gradually improving destigmatizing mental health problems and encouraging expression, we are often reluctant to listen to and understand adolescents when they confide in us, and to take rational steps to direct them to the help they need. Understanding the unique needs of adolescents, fostering social support, and providing constructive guidance are crucial.
Care approaches that integrate social aspects are proving more effective than medical treatment alone (110). This holistic approach considers the adolescent in his or her entirety, considering cultural, social, and psychological dimensions, with the aim of promoting well-being. Interventions are focusing mainly on listening, patience and empowerment, so as to prepare the teenager to face their own difficulties (111). The aim is to provide them with the resources they need to develop their skills and find the answers specific to them by themselves. Prevention efforts focus on promoting healthy coping mechanisms, rational thinking, and a positive mindset, not only for suicidal adolescents but for their whole entourage. Involving adolescents in both prevention plans and prevention initiatives utilizing technology could maximize effectiveness.
Healthcare primarily focuses on reducing symptoms, minimizing disability, and enhancing the quality of life, which are aspects that can only be adequately assessed by patients themselves. Patients genuinely appreciate being involved in their healthcare decisions, and this active participation can lead to additional health benefits.
Using patient-reported outcome measures (PROMs) helps to avoid observer bias, which could be inevitable if clinicians were to assess their own practice (112). By considering patients’ perspectives and experiences, the process enhances the public accountability of health services and healthcare professionals, leading to a more patient-centred and transparent healthcare system (113, 114).
5 Conclusion
The efforts aimed at preventing suicide have significantly increased, initiating conversations and challenging the stigma surrounding STB. Although no single approach has shown outstanding efficacy, these endeavors have laid a solid foundation for future progress. Technological advancements provide a promising avenue to address scalability issues and enhance help-seeking processes, offering autonomy and anonymity. However, there is a need to adapt these methods to different socio-economic contexts, while also considering the unique challenges faced by new generations. To achieve meaningful impact, ongoing work is required to ensure that prevention strategies align with modern issues and cater to diverse populations. Combining technological innovations with a comprehensive understanding of societal factors, can allow continuing suicide prevention efforts and foster more support and resilience.
Author contributions
JA: Writing – original draft, Visualization, Resources, Methodology, Investigation, Funding acquisition, Formal Analysis, Data curation, Conceptualization. MS: Writing – review & editing, Validation, Supervision, Project administration, Methodology, Investigation, Conceptualization. CM: Writing – review & editing, Validation, Supervision, Conceptualization.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This work is included within the first author's PhD grant, funded directly by the Department of Reunion Island and the Regional Health Agency of Reunion Island.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frcha.2024.1367075/full#supplementary-material
References
1. O'Connor RC, Nock MK. The psychology of suicidal behaviour. Lancet Psychiatry. (2014) 1(1):73–85. doi: 10.1016/S2215-0366(14)70222-6
2. Regier DA, Kuhl EA, Kupfer DJ. The DSM-5: classification and criteria changes. World Psychiatry. (2013) 12(2):92–8. doi: 10.1002/wps.20050
3. Madsen J, Harris KM. Negative self-appraisal: personal reasons for dying as indicators of suicidality. PLoS One. (2021) 16(2):e0246341. doi: 10.1371/journal.pone.0246341
4. Rømer TB, Christensen RHB, Blomberg SN, Folke F, Christensen HC, Benros ME. Psychiatric admissions, referrals, and suicidal behavior before and during the COVID-19 pandemic in Denmark: a time-trend study. Acta Psychiatr Scand. (2021) 144(6):553–62. doi: 10.1111/acps.13369
5. Valdez-Santiago R, Villalobos A, Arenas-Monreal L, González-Forteza C, Hermosillo-de-la-Torre AE, Benjet C, et al. Comparison of suicide attempts among nationally representative samples of Mexican adolescents 12 months before and after the outbreak of the COVID-19 pandemic. J Affect Disord. (2022) 298:65–8. doi: 10.1016/j.jad.2021.10.111
6. Berger G, Häberling I, Lustenberger A, Probst F, Franscini M, Pauli D, et al. The mental distress of our youth in the context of the COVID-19 pandemic. Swiss Med Wkly. (2022) 152. doi: 10.4414/SMW.2022.w30142
7. Pirkis J, Gunnell D, Shin S, Del Pozo-Banos M, Arya V, Aguilar PA, et al. Suicide numbers during the first 9–15 months of the COVID-19 pandemic compared with pre-existing trends: an interrupted time series analysis in 33 countries. EClinicalMedicine. (2022) 51. doi: 10.1016/j.eclinm.2022.101573
8. Alqueza KL, Pagliaccio D, Durham K, Srinivasan A, Stewart JG, Auerbach RP. Suicidal thoughts and behaviors among adolescent psychiatric inpatients. Arch Suicide Res. (2023) 27(2):353–66. doi: 10.1080/13811118.2021.1999874
9. Eldere LV, Claes S, Voorspoels W, Yurdadon C, Sabbe M, Bruffaerts R. Suicidal thoughts and behaviors (STB) among psychiatric emergency patients at the emergency unit of a university hospital in Belgium (UZ Leuven). A longitudinal approach with data from 2003 to 2015. Eur Psychiatry. (2022) 65(S1):S845. doi: 10.1192/j.eurpsy.2022.2189
10. Krychiw JK, Ward-Ciesielski EF. Factors related to suicide’s unpredictability: a qualitative study of adults with lived experience of suicide attempts. Int J Qual Stud Health Well-Being. (2019) 14(1):1650585. doi: 10.1080/17482631.2019.1650585
11. Franklin JC, Ribeiro JD, Fox KR, Bentley KH, Kleiman EM, Huang X, et al. Risk factors for suicidal thoughts and behaviors: a meta-analysis of 50 years of research. Psychol Bull. (2017) 143(2):187. doi: 10.1037/bul0000084
12. Ho TC, Gifuni AJ, Gotlib IH. Psychobiological risk factors for suicidal thoughts and behaviors in adolescence: a consideration of the role of puberty. Mol Psychiatry. (2022) 27(1):606–23. doi: 10.1038/s41380-021-01171-5
13. Lin L, Zhao S, Zhang J. Impulsivity kills some who did not plan to die by suicide: evidence from Chinese rural youths. Omega (Westport). (2019) 79(4):446–60. doi: 10.1177/0030222818786417
14. Romer D. Adolescent risk taking, impulsivity, and brain development: implications for prevention. Dev Psychobiol. (2010) 52(3):263–76. doi: 10.1002/dev.20442
15. Van Heeringen C, Bijttebier S, Godfrin K. Suicidal brains: a review of functional and structural brain studies in association with suicidal behaviour. Neurosci Biobehav Rev. (2011) 35(3):688–98. doi: 10.1016/j.neubiorev.2010.08.007
16. Alvarez-Subiela X, Castellano-Tejedor C, Villar-Cabeza F, Vila-Grifoll M, Palao-Vidal D. Family factors related to suicidal behavior in adolescents. Int J Environ Res Public Health. (2022) 19(16):9892. doi: 10.3390/ijerph19169892
17. Lee J, Bang YS, Min S, Ahn JS, Kim H, Cha YS, et al. Characteristics of adolescents who visit the emergency department following suicide attempts: comparison study between adolescents and adults. BMC Psychiatry. (2019) 19(1):231. doi: 10.1186/s12888-019-2213-5
18. Gordon RS. An operational classification of disease prevention. Public Health Rep. (1983) 98(2):107–9.6856733
19. Cuijpers P. Three decades of drug prevention research. Drugs. (2003) 10(1):7–20. doi: 10.1080/0968763021000018900
20. De Pablo GS, De Micheli A, Solmi M, Oliver D, Catalan A, Verdino V, et al. Universal and selective interventions to prevent poor mental health outcomes in young people: systematic review and meta-analysis. Harv Rev Psychiatry. (2021) 29(3):196–215. doi: 10.1097/HRP.0000000000000294
21. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. (2005) 8(1):19–32. doi: 10.1080/1364557032000119616
22. Torok M, Calear AL, Smart A, Nicolopoulos A, Wong Q. Preventing adolescent suicide: a systematic review of the effectiveness and change mechanisms of suicide prevention gatekeeping training programs for teachers and parents. J Adolesc. (2019) 73:100–12. doi: 10.1016/j.adolescence.2019.04.005
23. Doty B, Bass J, Ryan T, Zhang A, Wilcox H. Systematic review of suicide prevention studies with data on youth and young adults living in low-income and middle-income countries. BMJ Open. (2022) 12(9):e055000. doi: 10.1136/bmjopen-2021-055000
24. Cox G, Hetrick S. Psychosocial interventions for self-harm, suicidal ideation and suicide attempt in children and young people: what? how? who? and where? BMJ Ment Health. (2017) 20(2):35–40.
25. Devenish B, Berk L, Lewis AJ. The treatment of suicidality in adolescents by psychosocial interventions for depression: a systematic literature review. Aust N Z J Psychiatry. (2016) 50(8):726–40. doi: 10.1177/0004867415627374
26. Szlyk H, Tan J. The role of technology and the continuum of care for youth suicidality: systematic review. J Med Internet Res. (2020) 22(10):e18672. doi: 10.2196/18672
27. Morken IS, Dahlgren A, Lunde I, Toven S. The effects of interventions preventing self-harm and suicide in children and adolescents: an overview of systematic reviews. F1000Res. (2019) 8. doi: 10.12688/f1000research.19506.1
28. Grosselli L, Herzog K, Aseltine RH, Balazs J, Carli V, Ciffone J, et al. Dos and don'ts in designing school-based awareness programs for suicide prevention: results of a three-stage Delphi survey. Crisis. (2021).34042491
29. Forte A, Sarli G, Polidori L, Lester D, Pompili M. The role of new technologies to prevent suicide in adolescence: a systematic review of the literature. Medicina (B Aires). (2021) 57(2):109. doi: 10.3390/medicina57020109
30. Aguirre Velasco A, Cruz IS, Billings J, Jimenez M, Rowe S. What are the barriers, facilitators and interventions targeting help-seeking behaviours for common mental health problems in adolescents? A systematic review. BMC Psychiatry. (2020) 20(1):1–22. doi: 10.1186/s12888-020-02659-0
31. Gijzen MW, Rasing SP, Creemers DH, Engels RC, Smit F. Effectiveness of school-based preventive programs in suicidal thoughts and behaviors: a meta-analysis. J Affect Disord. (2022) 298:408–20. doi: 10.1016/j.jad.2021.10.062
32. Sinyor M, Williams M, Mitchell R, Zaheer R, Bryan CJ, Schaffer A, et al. Cognitive behavioral therapy for suicide prevention in youth admitted to hospital following an episode of self-harm: a pilot randomized controlled trial. J Affect Disord. (2020) 266:686–94. doi: 10.1016/j.jad.2020.01.178
33. Högberg G, Hällström T. Mood regulation focused CBT based on memory reconsolidation, reduced suicidal ideation and depression in youth in a randomised controlled study. Int J Environ Res Public Health. (2018) 15(5):921. doi: 10.3390/ijerph15050921
34. Whittaker R, Merry S, Stasiak K, McDowell H, Doherty I, Shepherd M, et al. MEMO—a mobile phone depression prevention intervention for adolescents: development process and postprogram findings on acceptability from a randomized controlled trial. J Med Internet Res. (2012) 14(1):e1857. doi: 10.2196/jmir.1857
35. Dickter B, Bunge EL, Brown LM, Leykin Y, Soares EE, Van Voorhees B, et al. Impact of an online depression prevention intervention on suicide risk factors for adolescents and young adults. Mhealth. (2019) 5. doi: 10.21037/mhealth.2019.04.01
36. Soares EE, Giordano BL, Rogers J, Leykin Y, Cordova M, Van Voorhees B, et al. The effects of engagement with an online depression prevention program for adolescents on suicide risk factors. J Technol Behav Sci. (2022) 7(3):307–14. doi: 10.1007/s41347-022-00249-3
37. Silverstone PH, Bercov M, Suen VY, Allen A, Cribben I, Goodrick J, et al. Long-term results from the empowering a multimodal pathway toward healthy youth program, a multimodal school-based approach, show marked reductions in suicidality, depression, and anxiety in 6,227 students in grades 6–12 (aged 11–18). Front Psychiatry. (2017) 8:81. doi: 10.3389/fpsyt.2017.00081
38. Kennard B, Mayes T, King J, Moorehead A, Wolfe K, Hughes J, et al. The development and feasibility outcomes of a youth suicide prevention intensive outpatient program. J Adolesc Health. (2019) 64(3):362–9. doi: 10.1016/j.jadohealth.2018.09.015
39. Babeva KN, Klomhaus AM, Sugar CA, Fitzpatrick O, Asarnow JR. Adolescent suicide attempt prevention: predictors of response to a cognitive–behavioral family and youth centered intervention. Suicide Life Threat Behav. (2020) 50(1):56–71. doi: 10.1111/sltb.12573
40. Desai Boström AE, Andersson P, Rask-Andersen M, Jarbin H, Lundberg J, Jokinen J. Regional clozapine, ECT and lithium usage inversely associated with excess suicide rates in male adolescents. Nat Commun. (2023) 14(1):1281. doi: 10.1038/s41467-023-36973-4
41. Byrne SJ, Bellairs-Walsh I, Rice SM, Bendall S, Lamblin M, Boubis E, et al. A qualitative account of young people’s experiences seeking care from emergency departments for self-harm. Int J Environ Res Public Health. (2021) 18(6):2892. doi: 10.3390/ijerph18062892
42. Freeman J, Strauss P, Hamilton S, Pugh C, Browne K, Caren S, et al. They told me “This Isn’ta Hotel”: young people’s experiences and perceptions of care when presenting to the emergency department with suicide-related behaviour. Int J Environ Res Public Health. (2022) 19(3):1377. doi: 10.3390/ijerph19031377
43. Libon J, Alganion J, Hilario C. Youth perspectives on barriers and opportunities for the development of a peer support model to promote mental health and prevent suicide. West J Nurs Res. (2023) 45(3):208–14. doi: 10.1177/01939459221115695
44. Hooven C. Parents-CARE: a suicide prevention program for parents of at-risk youth. J Child Adolesc Psychiatr Nurs. (2013) 26(1):85–95. doi: 10.1111/jcap.12025
45. Hooven C, Walsh E, Pike KC, Herting JR. Promoting CARE: including parents in youth suicide prevention. Fam Community Health. (2012) 35(3):225. doi: 10.1097/FCH.0b013e318250bcf9
46. Bean G, Baber KM. Connect: an effective community-based youth suicide prevention program. Suicide Life Threat Behav. (2011) 41(1):87–97. doi: 10.1111/j.1943-278X.2010.00006.x
47. Sandler I, Tein JY, Wolchik S, Ayers TS. The effects of the family bereavement program to reduce suicide ideation and/or attempts of parentally bereaved children six and fifteen years later. Suicide Life Threat Behav. (2016) 46:S32–8. doi: 10.1111/sltb.12256
48. King KA, Strunk CM, Sorter MT. Preliminary effectiveness of surviving the Teens® suicide prevention and depression awareness program on adolescents’ suicidality and self-efficacy in performing help-seeking behaviors. J Sch Health. (2011) 81:581–90. doi: 10.1111/j.1746-1561.2011.00630.x
49. Strunk CM, King KA, Vidourek RA, Sorter MT. Effectiveness of the surviving the Teens® suicide prevention and depression awareness program: an impact evaluation utilizing a comparison group. Health Educ Behav. (2014) 41(6):605–13. doi: 10.1177/1090198114531774
50. Calear AL, McCallum SM, Christensen H, Mackinnon AJ, Nicolopoulos A, Brewer JL, et al. The sources of strength Australia project: a cluster randomised controlled trial of a peer-connectedness school-based program to promote help-seeking in adolescents. J Affect Disord. (2022) 299:435–43. doi: 10.1016/j.jad.2021.12.043
51. Wyman PA, Brown CH, LoMurray M, Schmeelk-Cone K, Petrova M, Yu Q, et al. An outcome evaluation of the sources of strength suicide prevention program delivered by adolescent peer leaders in high schools. Am J Public Health. (2010) 100(9):1653–61. doi: 10.2105/AJPH.2009.190025
52. Ohlmann C, Kwee J, Lees R. Listening for the voices of resilience: a group of Adolescents’ experiences with a suicide prevention education program. Int J Child Youth Family Studies. (2014) 5(1):24–46. doi: 10.18357/ijcyfs.ohlmannc.512014
53. Lindow JC, Hughes JL, South C, Gutierrez L, Bannister E, Trivedi MH, et al. Feasibility and acceptability of the youth aware of mental health (YAM) intervention in US adolescents. Arch Suicide Res. (2020) 24(2):269–84. doi: 10.1080/13811118.2019.1624667
54. Godoy Garraza L, Kuiper N, Goldston D, McKeon R, Walrath C. Long-term impact of the garrett lee smith youth suicide prevention program on youth suicide mortality, 2006–2015. J Child Psychol Psychiatry. (2019) 60(10):1142–7. doi: 10.1111/jcpp.13058
55. Walrath C, Garraza LG, Reid H, Goldston DB, McKeon R. Impact of the garrett lee smith youth suicide prevention program on suicide mortality. Am J Public Health. (2015) 105(5):986–93. doi: 10.2105/AJPH.2014.302496
56. Chamlong Disayavanish M, Primprao Disayavanish M, Tala Thammaroj M, Surut Jianmongkol M, Kimaporn Kamanarong M, Somjit Prueksaritanond M. A buddhist approach to suicide prevention. J Med Assoc Thail. (2007) 90(8):1680–8.
57. Vendetti T, Hill J. Linking public schools and community mental health services: a model for youth suicide prevention. R I Med J. (2018) 101(4):36–8.
58. Crosby Budinger M, Cwik MF, Riddle MA. Awareness, attitudes, and use of crisis hotlines among youth at-risk for suicide. Suicide Life Threat Behav. (2015) 45(2):192–8. doi: 10.1111/sltb.12112
59. Inscoe AB, Donisch K, Cheek S, Stokes C, Goldston DB, Asarnow JR. Trauma-informed care for youth suicide prevention: a qualitative analysis of caregivers’ perspectives. Psychol Trauma Theory Res Pract Policy. (2022) 14(4):653. doi: 10.1037/tra0001054
60. Chen SS, Lam TP, Lam KF, Lo TL, Chao DV, Mak KY, et al. Motivations for online expression, willingness of online help-seeking, and the risk of suicide among Hong Kong youths: a mixed-methods study. Cyberpsychol Behav Soc Netw. (2022) 25(6):384–91. doi: 10.1089/cyber.2022.0007
61. Chen SS, Lam TP, Lam KF, Lo TL, Chao DV, Mak KY, et al. The use of close friends on Instagram, help-seeking willingness, and suicidality among Hong Kong youth: exploratory sequential mixed methods study. J Med Internet Res. (2022) 24(10):e37695. doi: 10.2196/37695
62. Olejniczak D, Jabłkowska-Górecka K, Panczyk M, Gotlib J, Walewska-Zielecka B. Analysis of adolescents’ opinions on suicide prevention. Psychiatr Pol. (2019) 53(2):359–70. doi: 10.12740/PP/OnlineFirst/81754
63. Robinson J, Hill NT, Thorn P, Battersby R, Teh Z, Reavley NJ, et al. The# chatsafe project. Developing guidelines to help young people communicate safely about suicide on social media: a Delphi study. PLoS One. (2018) 13(11):e0206584.30439958
64. Robinson J, Teh Z, Lamblin M, Hill NT, La Sala L, Thorn P. Globalization of the# chatsafe guidelines: using social media for youth suicide prevention. Early Interv Psychiatry. (2021) 15(5):1409–13. doi: 10.1111/eip.13044
65. Hubbard M. Suicide prevention: reducing self-harm in adolescents using the smart phone app “calm harm”. SRC/JMCN-160. J Med Clin Nurs. (2022) 148:2–7. doi: 10.47363/JMCN/2022(3)148
66. O'Grady C, Melia R, Bogue J, O’Sullivan M, Young K, Duggan J. A mobile health approach for improving outcomes in suicide prevention (SafePlan). J Med Internet Res. (2020) 22(7):e17481. doi: 10.2196/17481
67. Johnson LA, Parsons ME. Adolescent suicide prevention in a school setting: use of a gatekeeper program. NASN Sch Nurse. (2012) 27(6):312–7. doi: 10.1177/1942602X12454459
68. Jenner E, Jenner LW, Matthews-Sterling M, Butts JK, Williams TE. Awareness effects of a youth suicide prevention media campaign in Louisiana. Suicide Life Threat Behav. (2010) 40(4):394–406. doi: 10.1521/suli.2010.40.4.394
69. Freedenthal S. Adolescent help-seeking and the yellow ribbon suicide prevention program: an evaluation. Suicide Life Threat Behav. (2010) 40(6):628–39. doi: 10.1521/suli.2010.40.6.628
70. Chagnon F, Houle J, Marcoux I, Renaud J. Control-group study of an intervention training program for youth suicide prevention. Suicide Life Threat Behav. (2007) 37(2):135–44. doi: 10.1521/suli.2007.37.2.135
71. Bagatelas PH, Hunt JI. Assessing the quality of patient responses to a psychosocial intervention implemented on an adolescent psychiatric inpatient unit: devising the safety plan quality metric. R I Med J. (2022) 105(4):22–5.
72. Xavier A, Otero P, Blanco V, Vázquez FL. Efficacy of a problem-solving intervention for the indicated prevention of suicidal risk in young Brazilians: randomized controlled trial. Suicide Life Threat Behav. (2019) 49(6):1746–61. doi: 10.1111/sltb.12568
73. Grummitt LR, Debenham J, Kelly E, Barrett EL, Champion K, Conrod P, et al. Selective personality-targeted prevention of suicidal ideation in young adolescents: post hoc analysis of data collected in a cluster randomised controlled trial. Med J Aust. (2022) 216(10):525–9. doi: 10.5694/mja2.51536
74. Mouchabac S, Leray P, Adrien V, Gollier-Briant F, Bonnot O. Prevention of suicidal relapses in adolescents with a smartphone application: Bayesian network analysis of a preclinical trial using in silico patient simulations. J Med Internet Res. (2021) 23(9):e24560. doi: 10.2196/24560
75. MacDonald S, Sampson C, Biddle L, Yeon Kwak S, Scourfield J, Evans R. Theorising health professionals’ prevention and management practices with children and young people experiencing self-harm: a qualitative hospital-based case study. Sociol Health Illn. (2021) 43(1):201–19. doi: 10.1111/1467-9566.13211
76. Kennard BD, Goldstein T, Foxwell AA, McMakin DL, Wolfe K, Biernesser C, et al. As safe as possible (ASAP): a brief app-supported inpatient intervention to prevent postdischarge suicidal behavior in hospitalized, suicidal adolescents. Am J Psychiatry. (2018) 175(9):864–72. doi: 10.1176/appi.ajp.2018.17101151
77. Czyz EK, King CA, Prouty D, Micol VJ, Walton M, Nahum-Shani I. Adaptive intervention for prevention of adolescent suicidal behavior after hospitalization: a pilot sequential multiple assignment randomized trial. J Child Psychol Psychiatry. (2021) 62(8):1019–31. doi: 10.1111/jcpp.13383
78. Mancinelli-Hough K, Lucas Breda K, Karl C, Wentland BA. Don’t ask, won’t tell: suicide screening in the pediatric perioperative setting. Compr Child Adolesc Nurs. (2022) 45(4):395–402. doi: 10.1080/24694193.2022.2060376
79. Lindquist-Grantz R, Abraczinskas M. Using youth participatory action research as a health intervention in community settings. Health Promot Pract. (2020) 21(4):573–81. doi: 10.1177/1524839918818831
80. Cohen R, Rifkin-Zybutz R, Moran P, Biddle L. Web-based support services to help prevent suicide in young people and students: a mixed-methods, user-informed review of characteristics and effective elements. Health Soc Care Community. (2022).
81. Totura CM, Kutash K, Labouliere CD, Karver MS. Evaluating active parental consent procedures for school programming: addressing the sensitive topic of suicide prevention. J Sch Health. (2017) 87(2):114–20. doi: 10.1111/josh.12473
82. Kutcher S, Wei Y, Behzadi P. School-and community-based youth suicide prevention interventions: hot idea, hot air, or sham? Can J Psychiatry. (2017) 62(6):381–7. doi: 10.1177/0706743716659245
83. Rani MR, Krupanidhi S. A study to assess the effectiveness of structured teaching programme on suicide prevention among adolescents at selected higher secondary schools in Krishna District, Andhra Pradesh. Int J Adv Res. (2020) 6(9):219–23.
84. Kaur G, Sathish R. Effectiveness of information education and communication on knowledge regarding suicide and its prevention among adolescents in selected schools of panipat. Int J Nurs Educ. (2020) 12(1):11–4.
85. Labouliere CD, Tarquini SJ, Totura CM, Kutash K, Karver MS. Revisiting the concept of knowledge: how much is learned by students participating in suicide prevention gatekeeper training? Crisis. (2015) 36(4):274. doi: 10.1027/0227-5910/a000323
86. Totura CM, Labouliere CD, Gryglewicz K, Karver MS. The role of youth trainee–trainer alliance and involvement in school-based prevention: a moderated-mediation model of student gatekeeper suicide prevention training. Adm Policy Ment Health Ment Health Serv Res. (2019) 46:209–19. doi: 10.1007/s10488-018-0907-5
87. Heinz A, Catunda C, van Duin C, Willems H. Suicide prevention: using the number of health complaints as an indirect alternative for screening suicidal adolescents. J Affect Disord. (2020) 260:61–6. doi: 10.1016/j.jad.2019.08.025
88. Breux P, Boccio DE. Improving schools’ readiness for involvement in suicide prevention: an evaluation of the creating suicide safety in schools (CSSS) workshop. Int J Environ Res Public Health. (2019) 16(12):2165. doi: 10.3390/ijerph16122165
89. Bailey E, Spittal MJ, Pirkis J, Gould M, Robinson J. Universal suicide prevention in young people. Crisis. (2017).
90. Vaughn LM, Sunny CE, Lindquist-Grantz R, King C, Brent D, Boyd S, et al. Successful suicide screening in the pediatric emergency department: youth, parent, researcher, and clinician perspectives. Arch Suicide Res. (2020) 24(Supp 1):124–41. doi: 10.1080/13811118.2018.1541034
91. Asarnow JR, Hughes JL, Babeva KN, Sugar CA. Cognitive-behavioral family treatment for suicide attempt prevention: a randomized controlled trial. J Am Acad Child Adolesc Psychiatry. (2017) 56(6):506–14. doi: 10.1016/j.jaac.2017.03.015
92. Calear AL, Christensen H, Freeman A, Fenton K, Busby Grant J, Van Spijker B, et al. A systematic review of psychosocial suicide prevention interventions for youth. Eur Child Adolesc Psychiatry. (2016) 25:467–82. doi: 10.1007/s00787-015-0783-4
93. Oexle N, Waldmann T, Staiger T, Xu Z, Rüsch N. Mental illness stigma and suicidality: the role of public and individual stigma. Epidemiol Psychiatr Sci. (2018) 27(2):169–75. doi: 10.1017/S2045796016000949
94. Massé JC, T.-Brault MM. Maladie mentale et stigmatisation ou comment on devient un malade mental pour la vie. Santé Ment Au Qué. (2006) 4(1):73–83. doi: 10.7202/030048ar
95. Benoist J. Logiques de la stigmatisation, éthique de la destigmatisation. Inf Psychiatr. (2007) 83(8):649–54.
96. Mondi CF, Giovanelli A, Reynolds AJ. Fostering socio-emotional learning through early childhood intervention. Int J Child Care Educ Policy. (2021) 15(1):6. doi: 10.1186/s40723-021-00084-8
97. Sancassiani F, Pintus E, Holte A, Paulus P, Moro MF, Cossu G, et al. Enhancing the emotional and social skills of the youth to promote their wellbeing and positive development: a systematic review of universal school-based randomized controlled trials. Clin Pract Epidemiol Ment Health CP EMH. (2015) 11(Suppl 1 M2):21–40. doi: 10.2174/1745017901511010021
98. Portela-Pino I, Alvariñas-Villaverde M, Pino-Juste M. Socio-Emotional skills in adolescence. Influence of personal and extracurricular variables. Int J Environ Res Public Health. (2021) 18(9):4811. doi: 10.3390/ijerph18094811
99. Meerwijk EL, Parekh A, Oquendo MA, Allen IE, Franck LS, Lee KA. Direct versus indirect psychosocial and behavioural interventions to prevent suicide and suicide attempts: a systematic review and meta-analysis. Lancet Psychiatry. (2016) 3(6):544–54. doi: 10.1016/S2215-0366(16)00064-X
100. Yarborough BJH, Ahmedani BK, Boggs JM, Beck A, Coleman KJ, Sterling S, et al. Challenges of population-based measurement of suicide prevention activities across multiple health systems. eGEMs:7(1):13. doi: 10.5334/egems.277
101. Thorell L, Wahlin K, Ranstam J. Improper study design precludes valid effect estimates in important suicide prevention research. Int J Methods Psychiatr Res. (2019) 28(3):e1786. doi: 10.1002/mpr.1786
102. Wasserman D. Evaluating suicide prevention: various approaches needed. World Psychiatry. (2004) 3(3):153–4.16633481
103. International Statistical Classification of Diseases and Related Health Problems. 10th Revision Geneva: World Health Organization (2019).
104. Simon GE, Shortreed SM, Boggs JM, Clarke GN, Rossom RC, Richards JE, et al. Accuracy of ICD-10-CM encounter diagnoses from health records for identifying self-harm events. J Am Med Inform Assoc. (2022) 29(12):2023–31. doi: 10.1093/jamia/ocac144
105. McCarthy M, Saini P, Nathan R, McIntyre J. Improve coding practices for patients in suicidal crisis. Br Med J. (2021) 375.
106. Alavi N, Reshetukha T, Prost E, Antoniak K, Patel C, Sajid S, et al. Relationship between bullying and suicidal behaviour in youth presenting to the emergency department. J Can Acad Child Adolesc Psychiatry. (2017) 26(2):70–7.28747929
107. Holt MK, Vivolo-Kantor AM, Polanin JR, Holland KM, DeGue S, Matjasko JL, et al. Bullying and suicidal ideation and behaviors: a meta-analysis. Pediatrics. (2015) 135(2):e496–509. doi: 10.1542/peds.2014-1864
108. Rochford L. Contrepoint-Millenials, Y, Z… Et après? Inf Soc. (2016) (4):26. doi: 10.3917/inso.195.0026
109. Jauffrit M. Passerons-nous aussi à côté de la génération z? Le pentagone de formation et le système entrepreneurial. Projectics/Proyéctica/Projectique. (2022) 33(3):21–41. doi: 10.3917/proj.033.0021
110. Miller R, Glasby J, Dickinson H. Integrated health and social care in England: ten years on. Int J Integr Care:21(4):6. doi: 10.5334/ijic.5666
111. Rey L, Mérida-López S, Sánchez-Álvarez N, Extremera N. When and how do emotional intelligence and flourishing protect against suicide risk in adolescent bullying victims? Int J Environ Res Public Health. (2019) 16(12):2114. doi: 10.3390/ijerph16122114
112. Black N. Patient reported outcome measures could help transform healthcare. Br Med J. (2013) 346.
113. Philpot LM, Barnes SA, Brown RM, Austin JA, James CS, Stanford RH, et al. Barriers and benefits to the use of patient-reported outcome measures in routine clinical care: a qualitative study. Am J Med Qual. (2018) 33(4):359–64. doi: 10.1177/1062860617745986
Keywords: adolescents, suicide ideation, suicide attempt, suicidal thoughts and behaviors, early intervention, prevention
Citation: Aoun J, Spodenkiewicz M and Marimoutou C (2024) Scoping review on prevention of suicidal thoughts and behaviors in adolescents: methods, effectiveness and future directions. Front. Child Adolesc. Psychiatry 3:1367075. doi: 10.3389/frcha.2024.1367075
Received: 8 January 2024; Accepted: 8 May 2024;
Published: 10 June 2024.
Edited by:
Pooja Saini, Liverpool John Moores University, United KingdomReviewed by:
Molly McCarthy, Liverpool John Moores University, United KingdomJean-Daniel Carrier, Université de Sherbrooke, Canada
© 2024 Aoun, Spodenkiewicz and Marimoutou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Josée Aoun, YW91bi5qb3NlZUBnbWFpbC5jb20=; Michel Spodenkiewicz, bWljaGVsLnNwb2RlbmtpZXdpY3pAdW5pdi1yZXVuaW9uLmZy