 Shauna L. Rohner
Shauna L. Rohner Florence Bernays3
Florence Bernays3 Andreas Maercker
Andreas Maercker Myriam V. Thoma
Myriam V. Thoma- 1Competence Centre for Mental Health, Department of Health, OST—University of Applied Sciences of Eastern Switzerland, St. Gallen, Switzerland
- 2University Research Priority Program “Dynamics of Healthy Aging”, University of Zurich, Zurich, Switzerland
- 3Department of Business Administration, Chair of Human Resource Management and Leadership, University of Zurich, Zurich, Switzerland
- 4Psychopathology and Clinical Intervention, Institute of Psychology, University of Zurich, Zurich, Switzerland
Objective: While early-life adversity can have negative effects on health and wellbeing that persist across the lifespan, some individuals show indications of resilience. Resilience can be understood as a dynamic coping process involving the mobilization of resources in response to adversity exposure. Sense of coherence—revised (SOC-R), an ability linked to health maintenance in the face of adversity, may be influential in this process. However, research is lacking on the mechanisms underpinning SOC-R and resilience-related resources and their impact on the (mental) health of individuals exposed to early-life adversity. Therefore, this study examined the role of SOC-R and selected resilience-related resources in the relationship between early-life adversity and later-life health and wellbeing.
Method: Participants were N = 531 Irish (older) adults (58.2% female, mean age = 59.5 years, range = 50–86 years). Standardized questionnaires assessed retrospective reports of early-life adversity, as well as current physical and mental health, satisfaction with life, SOC-R, and resilience-related resources (self-efficacy, optimism, social support). A multiple mediation analysis tested the indirect effects of the resources and a moderated mediation tested for conditional dependence on SOC-R.
Results: For mental health and satisfaction with life, significant partial mediations were found for all three resources. Only optimism showed a significant partial mediation for physical health. In the moderated mediation, SOC-R significantly moderated the associations between early-life adversity and self-efficacy (b = .06, t = 3.65, p = .001), optimism (b = .04, t = 2.60, p = .009), and social support (b = .08, t = 3.75, p < .001). The indirect effects were larger at high rather than low SOC-R, indicating that the mediating effects of the resources were greater for individuals with a stronger SOC-R.
Conclusion: A strong SOC-R may have a beneficial influence on health and wellbeing by mitigating the detrimental effect of early-life adversity on the resources self-efficacy, optimism, and social support. Future avenues for research include the expanded assessment of resources and the potential role of SOC-R in successful ageing through the selection and adaptation of goals and resources into older age. SOC-R may represent a promising target for psychotherapeutic interventions promoting resilience in survivors of early-life adversity.
1. Introduction
Trauma or adversity in childhood and adolescence can take many forms, including abuse, neglect, extreme poverty, parental loss, and domestic or community violence (1). As childhood and adolescence represent a stress-sensitive period of physiological development, such early-life adversity can have long-lasting effects on the physiological systems that regulate the stress-response, with negative implications for health and wellbeing that can persist across the lifespan [e.g., (2, 3)]. For instance, a recent systematic review and meta-analysis of 23 longitudinal cohort studies examined the link between exposure to early-life adversity and adult-diagnosed depression, anxiety, psychotic disorder, or bipolar disorder (4). Significant associations were found between various indicators of early-life adversity and the diagnosis of a mental health disorder in later adulthood, including physical neglect (OR = 1.93, 95% CI 1.31–2.85), being a victim of bullying (OR = 2.36, 95% CI 1.45–3.86), and multiple trauma exposure (OR = 3.11, 95% CI 1.36–7.14). Similarly for physical health, studies of individuals with and without childhood trauma exposure indicate that those who experienced early-life adversity report worse physical health outcomes in middle adulthood [e.g., higher cardiometabolic risk (5); more self-reported health problems and lower perceived quality of physical health (6)]; as well as in older adulthood [e.g., higher incidence of diabetes, cardiovascular problems, and stroke (7)]. Such research not only highlights the link between early-life adversity and later life (psycho)pathology, but also hints at the broader consequences, such as the associated burden and costs on health and social care systems (8).
Despite this, not all those who experience early-life adversity display clinically relevant symptomatology. For instance, a recent study with Swiss older adult survivors of child welfare-related maltreatment found that despite severe and often prolonged early-life adversity, approximately 30% of survivors did not meet the full diagnostic criteria for a current or lifetime DSM-5 disorder (9). In addition, a longitudinal prospective study in the United States assessed children who were at risk or exposed to child maltreatment and found that 48% still demonstrated adaptive functioning across behavioral, social, and developmental domains (10). Similarly, a recent study by Yoon et al. (11) assessed a high-risk sample of children involved in the child welfare system in the United States. Findings showed that 56% could be classified into a multi-domain resilience profile, exhibiting positive adaptation and competence across all domains of cognitive, emotional, social, and behavioral functioning. Evidence of these heterogenous (mental) health outcomes following early-life adversity points to the potential for resilience, referring to relatively stable, healthy levels of psychological and physical functioning despite significant stress, trauma, or adversity (12). For instance, seminal research on resilience identified positive adjustment or adaptive trajectories in children exposed to significant adversities, including war, terrorism, disasters, and maltreatment (13–15).
Theoretical models of resilience, such as the multi-system model of resilience [MSMR (16)], or the socio-interpersonal model of trauma sequalae (17), view resilience as a dynamic coping process involving the mobilization and interaction of resources in response to adversity exposure. The MSMR suggests that resilience capacity is shaped by multiple resources, including traits, psychological personality-correlates, protective factors, and social and community structures (16). Applying this to trauma and adversity, the socio-interpersonal model depicts these resources on the level of the individual, close relationships, and distant social contexts. It proposes that interactions between and across these levels determine how adversity is mitigated or intensified, which in turn, influences response outcomes (17). The application of these conceptual frameworks to empirical data can aid in the identification of key resilience-related resources in the relationship between early-life adversity and later-life health and wellbeing.
These protective or promotive resources can be broadly categorized into positive resources within the individual, such as self-efficacy, and positive resources external to the individual, such as social support (16, 18). With regard to early-life adversity, research on individual attributes or internal resilience resources has identified several key characteristics or personality traits (e.g., self-efficacy, mastery, hardiness, persistence, emotional reactivity) that may help buffer against negative outcomes (19). For example, a study of protective factors in children exposed to maltreatment in the home identified optimism, self-efficacy, and adaptability as key individual resources linked to fewer posttraumatic stress disorder (PTSD) symptoms (20). Regarding later-life mental health, a longitudinal population-based birth cohort analysis in the United Kingdom by Cosco and colleagues (21) examined resilience resources in older adults with a history of early-life adversity. Results identified individual and social resources (e.g., education, social support, neighborhood cohesion) associated with lower levels of mental distress in later life. These resources partly mediated the relationship between early-life adversity and later-life mental distress, with the effect of social support being the greatest (21).
Furthermore, systematic reviews on resilience and protective factors in individuals with a history of early-life adversity provide support for several individual and external resources linked to better health and wellbeing [e.g., self-efficacy; optimism; coping skills; interpersonal competence or the ability to interact or work with others; and social support in the form of practical, tangible, or emotional assistance or comfort from family, peers, community, or significant others (22, 23)]. However, these individual and external resources do not act in isolation, but rather interact to impact (mental) health outcomes (16, 24). Although emerging research has attempted to characterize the links between early-life adversity and the expression of psychopathology or resilience [e.g., (25, 26)], the interplay of relevant mechanisms remains largely unclear. Ongoing research attention is therefore required to clarify the mechanisms underpinning the pathways to (mental) health and wellbeing following early-life adversity. A better understanding of the mechanistic pathways could help identify whether, and how, the negative (mental) health consequences of early-life adversity could be mitigated or prevented, and adaptive outcomes promoted.
One resilience-related aspect that may be influential in this process is sense of coherence (SOC). The original SOC concept developed by Antonovsky (27) suggests that the way in which individuals view their lives can have an influence on their health. This concept was further refined by Bachem and Maercker (28), with a sense of coherence—revised (SOC-R) describing an individual's ability to perceive, integrate, and balance positive and negative life experiences in order to maintain their health and wellbeing. The SOC-R construct is comprised of three theoretical dimensions, with a focus on health maintenance and dealing with the ambiguity of challenges: Managing and dealing with difficult situations (manageability), balancing positive and negative experiences and feelings (balance), and considering different perspectives and understanding connections (reflection) (28). SOC-R may play a key role in maintaining health and wellbeing after exposure to early-life adversity, as it is proposed to develop and strengthen early in life by successfully overcoming challenging experiences. Consequently, according to the theoretical assumptions of SOC-R, individuals with a strong SOC-R are assumed to be better at utilizing available and appropriate resources to overcome stress and adversity in later life (28, 29).
Previous research, mainly with the original SOC concept, has demonstrated associations with key resilience-related resources and better (mental) health outcomes. For instance, research examining predictors of distress in patients with cancer found that a stronger SOC was associated with higher levels of optimism, which was linked to fewer symptoms of depression and anxiety than those with weaker SOC and lower levels of optimism (30). In addition, research by Wiesmann and colleagues (31) on the experience of bodily pain found that the resources self-esteem, self-efficacy, optimism, and social support had an indirect effect on pain through SOC. A recent study by Sölva and colleagues (32) used latent class analysis to identify distinct classes of adaptation in trauma-exposed children and adolescents in residential care in Austria. Results revealed a resilient class characterized by lower levels of symptom severity (i.e., dissociative symptoms, internalizing and externalizing problems, interpersonal problems, and thought problems); as well as highest levels of the protective factors SOC, self-efficacy, peer support, and caregiver social and emotional support (32). While such research indicates the potential protective influence of SOC, few studies have examined the interaction of resilience-related resources, particularly not with the more recently refined SOC-R.
Existing research on SOC-R has mainly established its role in the relationship between adversity and health outcomes. For example, research by Thoma and colleagues (33) with a representative German sample identified a moderating effect of SOC-R in the relationship between trauma exposure and mental health. A strong SOC-R was associated with lower depression scores compared to those with a weaker SOC-R, even at high levels of childhood neglect and lifetime traumatic events (33). In addition, a study on emergency medical service rescue workers who were regularly exposed to potentially traumatic on-duty events found that a higher SOC-R was associated with less post-traumatic, depressive, and somatic symptoms (34).
Initial studies focusing on SOC-R in adult and older adult samples have demonstrated a moderating or mediating influence in the relationship between adversity, stress, and mental (health) outcomes. For instance, a study with Swiss older adults identified the SOC-R manageability subscale as a significant moderator, with higher SOC-R manageability linked to better general mental health across all levels of chronic stress (35). Similarly, recent research with Irish older adults found that those with a stronger SOC-R reported better mental health, even at high levels of acute perceived stress (36). As a next step, research is needed that incorporates key resilience-related resources into the model with SOC-R to obtain a more complete picture of the mechanisms underpinning health and wellbeing following exposure to early-life adversity.
It was therefore the aim of this study to examine the role of SOC-R and resilience-related resources in the relationship between early-life adversity and later-life health and wellbeing. To select key resilience-related resources that encompass a range of individual protective factors, psychological personality-correlates, and socio-interpersonal factors, conceptual frameworks and theoretical models of resilience were first consulted [i.e., (16, 17)]. These factors were further refined for relevance to the study sample and research questions by drawing on empirical studies in individuals with a history of early-life adversity [e.g., (21–23, 32)], to identify resources commonly linked to adaptive outcomes or resilience. As a result of this process, self-efficacy, optimism, and social support were selected as key internal and external resources for inclusion into the model with SOC-R. Given that individuals with a strong SOC-R should be better able to utilize their resources to successfully overcome adversity (28, 29); a moderated mediation model was assessed with SOC-R as the moderator. This tested whether the mediation effects of the resources differed depending on the level of SOC-R. Specifically, it was hypothesized that the mediating effects of the resources would be greater for participants with a stronger SOC-R.
2. Materials and methods
2.1. Study design and procedure
This study assesses data from a cross-sectional quantitative questionnaire survey, conducted in Ireland between June and December 2018 as part of the larger Swiss National Science Foundation (SNSF) funded project “Differential aging trajectories in high-risk individuals with past experiences of early adversity”, within the SNSF National Research Program 76 “Welfare and Coercion—Past, Present, and Future” (http://www.nrp76.ch/en). The study was conducted by a research team of the Psychological Institute at the University of Zurich, in collaboration with University College Dublin, National College of Ireland, and Ulster University. The study procedure was approved by the Ethics Committee of the Faculty of Arts and Social Sciences in the University of Zurich, Switzerland (ID 18.6.1), and the Human Research Ethics Committee—Humanities in University College Dublin, Ireland (ID HS-18-30-Carr). Written informed consent was provided by all participants in accordance with the Declaration of Helsinki.
2.2. Participants and procedure
Eligible participants were Irish individuals, native English speakers, and aged 50 years or older. The sample size of 531 was considered sufficient to conduct the moderated mediation analyses based on the established guidelines of a minimum of 5–10 observations per estimated parameter (37), the minimum of 200 participants for mediation analyses (38), and the sample sizes of previous empirical studies using moderated mediation analyses [e.g., (39)]. Recruitment methods included flyers posted in public and community spaces (e.g., libraries, adult education centers), online advertisements, radio interviews with the study lead (first author), and networks of the study collaborators. Interested individuals contacted the study team by email or telephone and were screened for eligibility. Qualtrics survey management software was additionally used to recruit the target population and reduce sampling or self-selection biases (40). This helped to ensure a more equal distribution of cohort characteristics, such as age, gender, socio-economic status, and education level. For representativeness, the sample from each research panel was proportioned to the general population and then randomized. Some participants did not meet the inclusion or quality check criteria and were screened out, resulting in an overall response rate of 97.5%. Eligible participants could either complete the paper-pencil questionnaire survey or the online survey programmed with Unipark software (41). The questionnaire survey consisted of the information sheet, the informed consent form, the study questionnaires (randomized to avoid sequence and order effects), a debriefing sheet, and a list of psychosocial support options.
2.3. Measures
2.3.1. Socio-demographic information
Participants first completed a questionnaire to collect socio-demographic information, including age, gender, relationship status, highest level of education, and employment status.
2.3.2. Sense of coherence—revised
The SOC-R scale assessed sense of coherence—revised, i.e., the way individuals perceive, integrate, and balance positive and negative life experiences in order to maintain health and wellbeing (28). Built on three theoretical dimensions of manageability, balance, and reflection, the SOC-R scale consists of 13 items rated on a five-point Likert scale (from 1 = “not at all true” to 5 = “extremely true”). It yields a total score, with higher scores indicating higher SOC-R. Previous studies have shown convergent and discriminant validity through moderate correlations with measures of mental health, such as depression (r = −.46, p < .05), anxiety (r = −.33, p < .05), and prolonged grief (r = −.48, p < .05); as well as good internal consistencies of between α = .75 and α = .87 (28, 33, 42). A good internal consistency of α = .86 was shown in the current study.
2.3.3. Early-life adversity
The Adverse Childhood Experiences—International Questionnaire [ACE-IQ, (1)] assessed the following categories of early-life adversity experienced up until 18 years old: Physical, emotional, or sexual abuse; physical or emotional neglect; violence against household members; living with household members who were substance abusers, who were mentally ill or suicidal, or who were imprisoned; having one or no parents, parental separation, or divorce; bullying; community violence; and collective violence. Each early-life adversity category was scored as 0 = “no” or 1 = “yes”, resulting in a total score ranging from 0 to 13, with higher scores indicating higher levels of exposure to early-life adversity (1). Previous research has shown good discriminant validity (F-value = 13.90, p < 0.001), good convergent validity with the Childhood Trauma Questionnaire—Short Form (r = 0.85, p < 0.001), and a good internal consistency of α = .85 (43). An acceptable internal consistency of α = .70 was shown in the current study.
2.3.4. Health and wellbeing
2.3.4.1. Physical and mental health
The 36-item Short Form Health Survey version 1 (SF-36) assessed physical and mental health (44). Summary scores were calculated for physical health (physical component summary; PCS) and mental health (mental component summary; MCS) using eight weighted subscales: Physical functioning, bodily pain, role limitations due to physical health problems, role limitations due to emotional problems, emotional wellbeing, social functioning, energy/fatigue, general health perceptions (44). Studies have shown good construct validity for the SF-36 in groups with long- and short-term illnesses, as well as good internal consistencies of α = .92 for PCS and α = .91 for MCS (45, 46). Acceptable internal consistencies of α = .74 (PCS) and α = .77 (MCS) were shown in the current study.
2.3.4.2. Satisfaction with life
The Satisfaction with Life Scale (SWLS) was used as an index of subjective wellbeing with regard to overall quality of and satisfaction with life (47). It consists of five items, rated on a seven-point Likert scale (from 1 = “strongly disagree” to 7 = “strongly agree”), with higher scores indicating higher life satisfaction. The SWLS has previously shown convergent validity through moderately strong correlations with other measures of subjective wellbeing, such as happiness (r = .58) and affect balance (r = .50); as well as a good internal consistency of α = .87 (47). A good internal consistency of α = .91 was shown in the current study.
2.3.5. Resources
2.3.5.1. Self-efficacy
The General Self-Efficacy Scale (GSE) assessed perceived self-efficacy in coping with difficult life circumstances (48). It consists of 10 items, rated on a four-point Likert scale (from 1 = “not at all true” to 4 = “exactly true”). It yields a total score, with higher scores indicating higher perceived self-efficacy. The GSE has shown convergent and discriminant validity through moderate to strong correlations with measures such as anxiety (r = −.43) and optimism (r = .60); as well as an acceptable to good internal consistency of between α = .75 and α = .91 (49). A good internal consistency of α = .84 was shown in the current study.
2.3.5.2. Optimism
The Life Orientation Test—Revised (LOT-R) assessed the level of dispositional optimism in relation to expectations about one's future (50). It consists of six items (plus four filler items), rated on a four-point Likert scale (from 0 = “strongly disagree” to 4 = “strongly agree”). It yields a total score, with higher scores indicating higher levels of optimism. The LOT-R has shown convergent and discriminant validity through moderate to strong correlations with measures such as self-mastery (r = .48), self-esteem (r = .50), and trait anxiety (r = −.53); as well as an acceptable internal consistency of α = .78 (50). A good internal consistency of α = .85 was shown in the current study.
2.3.5.3. Social support
The short form of the Interpersonal Support Evaluation List (ISEL-12) assessed perceived social support (51). It consists of 12 items, rated on a four-point Likert scale (from 0 = “definitely false” to 3 = “definitely true”). The ISEL-12 yields a total score, with higher scores indicating higher perceived social support. Previous studies have shown convergent validity through moderate correlations with measures such as social network integration (r = .33) and life engagement (r = .40); as well as good internal consistency of between α = .80 and α = .90 (52, 53). A good internal consistency of α = .87 was shown in the current study.
2.3.6. Data analysis
Statistical analyses were performed using R version 3.6.2. Less than 1% missing values were observed on a (sub)scale level, such that the average proportion of missingness across participants was 0.005%. A multiple iterative imputation technique, including predictive mean matching, was used to impute missing values by applying a chained random forest algorithm (5,000 trees calculated) using the package “missRanger”, which is a suitable algorithm for imputing mixed-type data, while maintaining variability on a realistic level (54). A multiple imputation technique was used as this method has been shown to produce more accurate and less biased estimates as it accounts for uncertainty in the data while also using less computational power compared to other techniques (55). It is also necessary to consider the complexity of the method and check that the amount of missingness is not substantial to ensure that the imputed data does not considerably influence the results and conclusions. Influential outliers, defined by a Cook's distance value greater than four times the mean (56), were analyzed for all outcome variables. Three observations were within this range, but as the results did not differ when excluding these observations, they were included in the final analysis.
2.3.6.1. Moderated mediation analysis
In a first step, intercorrelations of study variables were analyzed by computing Pearson's correlations coefficients. Given that empirical studies have demonstrated a mediating role of the selected internal and external resources [e.g., (21, 57)], a multiple mediation analysis was performed in a second step to test within a combined model the indirect effects of self-efficacy, optimism, and social support as parallel mediators of the relationship between early-life adversity (ACE-IQ) and the health and wellbeing indicators (i.e., physical and mental health and satisfaction with life). Following Preacher and Hayes (58), a parallel mediation model was applied using a structural equation framework (package “lavaan”), while including age and gender as covariates. According to the conditions of mediation analysis outlined by Baron and Kenny (59), to support a mediation the predictor must be significantly related to the outcome and the mediator, and the mediator must be significantly related to the outcome variable. In the case of multiple mediation, it is beneficial to test multiple mediators simultaneously in one model as the indirect effects are then separated from the effects of other mediators (60). Indirect effects were estimated using the bootstrapping technique (5,000 resamples). As indirect effects can follow a skewed distribution (61), bias-corrected and accelerated percentile confidence intervals were reported for indirect effects, as these have been shown to be more accurate than the percentile technique (62). Statistical significance of an indirect effect was assumed when the confidence interval did not contain zero. Finally, the theoretical assumptions of SOC-R suggest that it develops and is strengthened early in life by overcoming adverse experiences, and that a strong SOC-R is linked to better use of available resources (28, 29). Therefore, a moderated mediation was conducted in the third step, with SOC-R added as a moderator of the relationship between ELA and the resources, testing whether SOC-R moderated the mediations from the previous step. To do so, significant interactions must be given between the predictor (early-life adversity) and the moderator (SOC-R) to test whether the indirect effects vary at different values of the moderator. In addition, the indirect effects of the mediators (i.e., self-efficacy, optimism, social support) must differ across different levels of the moderator (SOC-R) (63, 64). Thus, to test whether mediation effects differed depending on the level of SOC-R (i.e., high vs. low), indirect effects were investigated at one standard deviation (SD) above and below the mean of SOC-R. In line with previous studies examining the link between early-life adversity and (mental) health [e.g., (65)], age and gender were included as covariates in all equations to support the robustness of the findings irrespective of individual characteristics. Corrections for multiple comparisons were not applied as this may inflate the risk of Type II error and is rather advised for confirmatory studies (66). Furthermore, predictors were mean-centered for all equations to facilitate the interpretation of estimates. P-values < .05 were considered statistically significant. To test for potential multicollinearity, Variance Inflation Factors (VIF) were calculated for all predictor variables in the model. As all VIF were below the value of 4 (no VIF exceeded the value of 1.7), multicollinearity was not considered an issue in the present results (67).
3. Results
The following analyses examine the role of sense of coherence—revised (SOC-R) and resilience-related resources in the relationship between early-life adversity (ELA) and later-life health and wellbeing. A moderated mediation model tests whether the mediation effects of the resources differ depending on the level of SOC-R (i.e., the moderator). Specifically, it was hypothesized that in the relationship between early-life adversity and later-life (mental) health and wellbeing, the mediating effects of the resources would be greater for participants with a stronger SOC-R.
3.1. Sample characteristics
A total of 532 participants were recruited, with one participant excluded due to high missingness (>40%), which was above the recommended threshold of less than 10% missingness (68). The final sample consisted of N = 531 participants, 58.2% female (n = 310), with a mean age of 59.5 years (SD = 7.1, range = 50–86 years). The majority of the sample was married (n = 337, 63.5%), indicated university as their highest level of education (n = 240, 45.2%), and were employed (n = 262, 49.3%). See Table 1 for an overview of the sample characteristics.
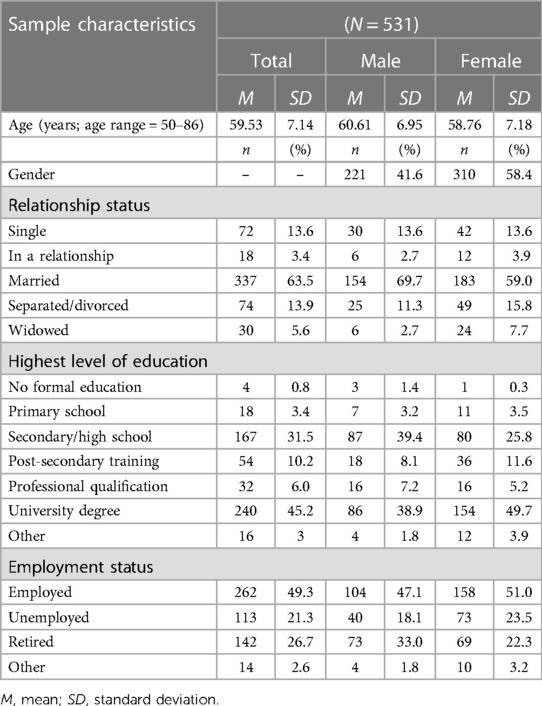
Table 1. Sample characteristics.
3.2. Correlation analysis
Intercorrelations of the study variables are shown in Table 2. The majority of coefficients indicated moderate to strong correlations among study variables. For self-efficacy, Pearson's correlation coefficients suggested a small but significant negative association with early-life adversity (ELA) (r = −.13, p = .004), a small but significant positive association with physical health (r = .11, p = .013), and significant moderate and positive associations with mental health (r = .49, p < .001) and satisfaction with life (r = .44, p < .001). For optimism, a small but significant negative correlation was also found with ELA (r = −.21, p < .001), a small but significant positive correlation with physical health (r = .17, p < .001), and significant moderate and positive associations with mental health (r = .48, p < .001) and satisfaction with life (r = .52, p < .001). For social support, a small but significant negative correlation was also found with ELA (r = −.27, p = .004), a small but significant positive association with physical health (r = .11, p = .008), and significant moderate and positive associations with mental health (r = .49, p < .001) and satisfaction with life (r = .48, p < .001). Furthermore, significant correlations of small to moderate size were also found between ELA and the health and wellbeing indicators (physical health: r = −.26, p < .001; mental health: r = −.38, p < .001; satisfaction with life: r = −.27, p < .001). This enabled the testing of self-efficacy, optimism, and social support as mediators of the corresponding relationships between ELA and the health and wellbeing indicators. To ensure that possible deviations from normality did not bias the results of the correlation analysis, Spearman's rank correlations were also calculated for all of the above relationships, revealing that the results did not differ from the Pearson's correlation analysis.
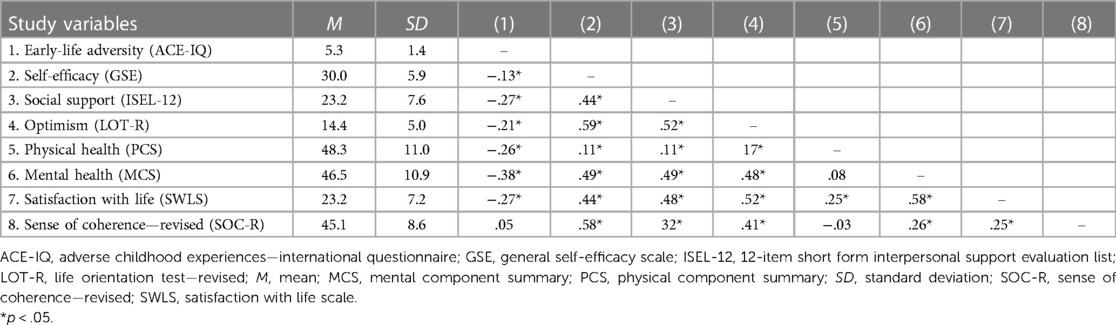
Table 2. Means, standard deviations, and intercorrelations of study variables.
3.3. Mediation analysis
A multiple mediation analysis was first conducted to investigate whether self-efficacy, optimism, and social support mediated the relationships between ELA and the health and wellbeing indicators. Results found that all three resources were significant mediators for mental health and satisfaction with life); whereas only optimism was a significant mediator for physical health. Results are outlined in detail below. See Table 3 for the estimates of direct and indirect effects of the multiple mediation analysis.
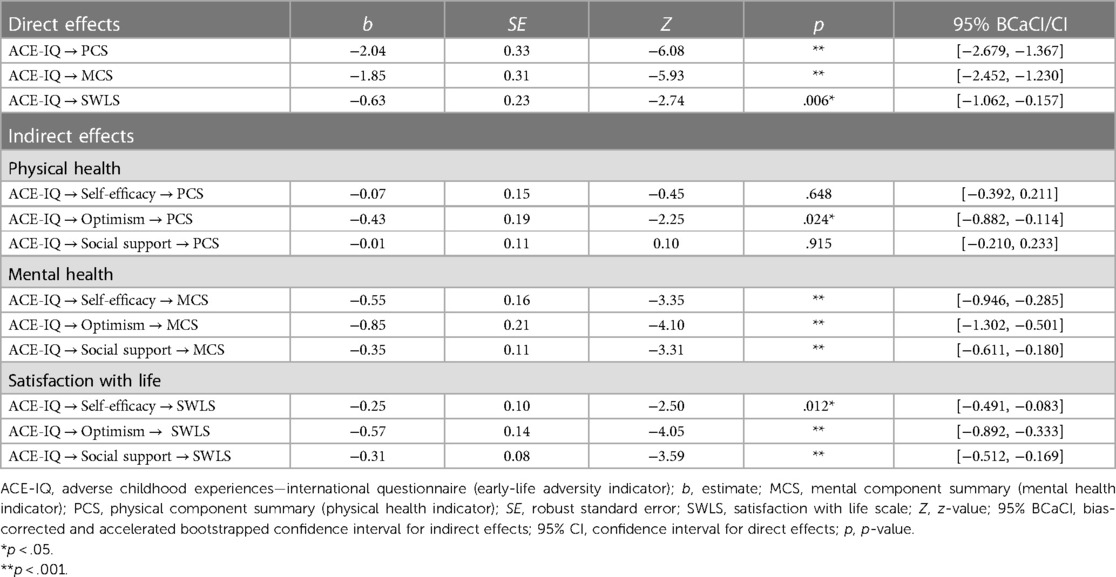
Table 3. Direct and indirect effects of the mediation analyses.
3.3.1. Physical health
Regarding ELA and physical health, a significant indirect effect was found for optimism (b = −0.43, SE = 0.19, p = .024). No significant indirect effects were found for self-efficacy (b = −0.07, SE = 0.15, p = .648) or social support (b = −0.01, SE = 0.11, p = .915). As the direct effect between ELA and physical health remained significant (b = −2.04, SE = 0.33, p < .001) the results indicate that optimism partially mediated the association between ELA and physical health.
3.3.2. Mental health
Regarding ELA and mental health, significant indirect effects were found for self-efficacy (b = −0.55, SE = 0.16, p < .001), optimism (b = −0.85, SE = 0.21, p < .001), as well as social support (b = −0.35, SE = 0.11, p < .001). As the direct effect between ELA and mental health remained significant (b = −1.85, SE = 0.31, p < .001), the results indicate that self-efficacy, optimism, and social support partially mediated the association between ELA and mental health.
3.3.3. Satisfaction with life
Regarding ELA and satisfaction with life, significant indirect effects were found for self-efficacy (b = −0.25, SE = 0.10, p = .012), optimism (b = −0.57, SE = 0.14, p < .001), as well as social support (b = −0.31, SE = 0.08, p < .001). As the direct effect between ELA and satisfaction with life remained significant (b = −0.63, SE = 0.23, p = .006), results indicate that self-efficacy, optimism, and social support partially mediated the association between ELA and satisfaction with life.
3.4. Moderated mediation analysis
In the next step, moderated mediation analyses were conducted to investigate whether SOC-R moderated the significant indirect effects from the previous mediation analyses. Results found significant indirect effects for all health and wellbeing indicators (i.e., physical and mental health, satisfaction with life) when SOC-R was included as a moderator, with the indirect effects larger at high rather than low levels of SOC-R. Results are outlined in detail below. Figure 1 illustrates the proposed moderated mediation model.
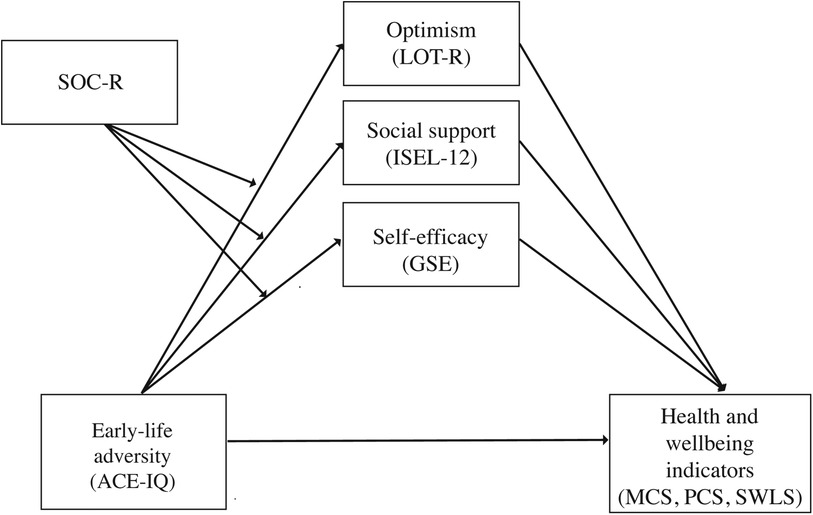
Figure 1. The proposed moderated mediation model, with SOC-R moderating the indirect effects of self-efficacy, optimism, and social support on early-life adversity and health and wellbeing. ACE-IQ, Adverse Childhood Experiences—International Questionnaire; GSE, general self-efficacy scale; ISEL-12, 12-item short form interpersonal support evaluation list; LOT-R, life orientation test—revised; MCS, mental component summary; PCS, physical component summary; SOC-R, sense of coherence—revised; SWLS, satisfaction with life scale.
First, it was tested whether SOC-R moderated the relationships between ELA and the three mediators (i.e., self-efficacy, optimism, social support). SOC-R significantly moderated the associations between ELA and self-efficacy (b = .06, t = 3.65, p = .001), between ELA and optimism (b = .04, t = 2.60, p = .009), and between ELA and social support (b = .08, t = 3.75, p < .001), such that the negative association between ELA and the resources became weaker at high levels of SOC-R. This allowed for the testing of the indirect effects of the relationships between ELA and the health and wellbeing indicators for conditional dependence on SOC-R. See Table 4 for the conditional indirect effects across all health and wellbeing indicators. See Figure 2 for the significant moderations by SOC-R of the relationship between ELA and the three mediators (i.e., self-efficacy, optimism, social support).
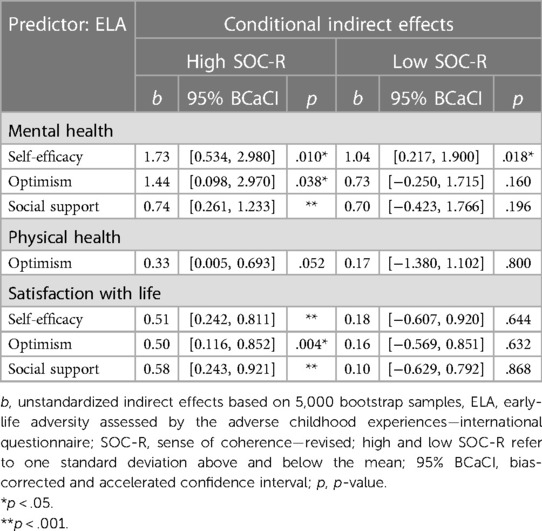
Table 4. Conditional indirect effects for the moderator SOC-R.
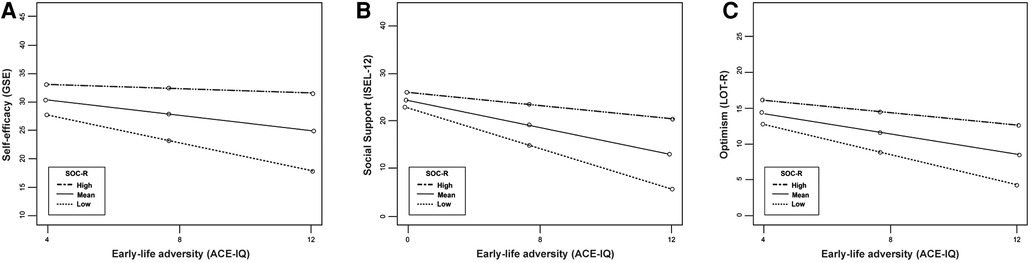
Figure 2. Significant moderation by SOC-R in the relationships between early-life adversity and the resources (A: self-efficacy, B: social support, C: optimism). ACE-IQ, Adverse Childhood Experiences—International Questionnaire; GSE, general self-efficacy scale; ISEL-12, 12-item short form interpersonal support evaluation list; LOT-R, life orientation test—revised; SOC-R, sense of coherence—revised; high and low SOC-R refer to one standard deviation above and below the mean.
3.4.1. Physical health
Regarding the partial mediation of ELA and physical health, the indirect effect of optimism was only marginally significant at high levels of SOC-R (b = 0.33, 95% BCaCI [0.005, 0.693], p = .052), and not significant at low levels of SOC-R (b = −0.17, 95% BCaCI [−1.380, 1.102], p = .800). The indirect effect of optimism showed an average increase of 94% at high (compared to low) levels of SOC-R. This could cautiously indicate that the mediating effect of optimism on the relationship between ELA and physical health was stronger when participants reported high levels of SOC-R. However, caution should be emphasized given that the p-value is very close to the standard significance threshold of .05.
3.4.2. Mental health
Regarding the partial mediation of ELA and mental health, the indirect effects of self-efficacy were significant at high and low levels of SOC-R, with the size of the indirect effects being larger for high levels of SOC-R (b = 1.73, 95% BCaCI [0.534, 2.980], p = .010), rather than low levels of SOC-R (b = 1.04, 95% BCaCI [0.217, 1.900], p = .018). The indirect effect of self-efficacy showed an average increase of 40% at high (compared to low) levels of SOC-R. For optimism, the indirect effect was significant at high levels of SOC-R (b = 1.44, 95% BCaCI [0.098, 2.970], p = .038), but not at low levels of SOC-R (b = 0.73, 95% BCaCI [−0.250, 1.715], p = .160). The indirect effect of optimism showed an average increase of 49% at high (compared to low) levels of SOC-R. Similarly for social support, the indirect effect was significant at high levels of SOC-R (b = 0.74, 95% BCaCI [0.261, 1.233], p < .001), but not at low levels of SOC-R (b = 0.70, 95% BCaCI [−0.423, 1.766], p = .196). The indirect effect of social support showed an average increase of 5% at high (compared to low) levels of SOC-R. The indirect effects of self-efficacy and optimism were on average 1.6 times larger, and social support was 1.05 times larger, at high levels of SOC-R than at low levels of SOC-R. This indicates that the mediating effects of these resources on the relationship between ELA and mental health were stronger when participants reported high levels of SOC-R.
3.4.3. Satisfaction with life
Regarding the partial mediation of ELA and satisfaction with life, the indirect effects of self-efficacy were significant at high levels of SOC-R (b = 0.51, 95% BCaCI [0.242, 0.811], p < .001), but not at low levels of SOC-R (b = 0.18, 95% BCaCI [−0.607, 0.920], p = .644). The indirect effect of self-efficacy showed an average increase of 64% at high (compared to low) levels of SOC-R. This pattern was also found for optimism (high SOC-R: b = 0.50, 95% BCaCI [0.116, 0.852], p = .004; low SOC-R: b = 0.16, 95% BCaCI [−0.569, 0.851], p = .632); and social support (high SOC-R: b = 0.58, 95% BCaCI [0.243, 0.921], p < .001; low SOC-R: b = 0.10, 95% BCaCI [−0.629, 0.792], p = .868). The indirect effect of optimism showed an average increase of 68% and indirect effect of social support showed an average increase of 82% at high (compared to low) levels of SOC-R. Across the three mediators, the indirect effects were on average 3.9 times larger at high levels of SOC-R than at low levels of SOC-R. This indicates that the mediating effects of self-efficacy, optimism, and social support on the relationship between ELA and satisfaction with life were stronger when participants reported high levels of SOC-R.
4. Discussion
This study examined the role of SOC-R and selected individual and external resilience-related resources in the relationship between early-life adversity and later-life health and wellbeing. A conditional process analysis was conducted, with a multiple mediation analysis performed in a first step, to test the indirect effects of self-efficacy, optimism, and social support as parallel mediators of the relationship between early-life adversity and indicators of health and wellbeing. In a second step, a moderated mediation tested for conditional dependence on SOC-R (i.e., the moderator). The main findings suggest that a strong SOC-R may have a beneficial influence on health and wellbeing by mitigating the detrimental effect of early-life adversity on the resources self-efficacy, optimism, and social support. Specifically, the analysis revealed significant partial mediations for all three resilience-related resources, with significant indirect effects when SOC-R was included as a moderator. The indirect effects were larger at high rather than low levels of SOC-R, indicating that the mediating effects of the resources on health and wellbeing were greater for participants with a strong SOC-R.
With regard to the mediation in the first step, self-efficacy, optimism, and social support were all found to partially mediate the relationship between early-life adversity and mental health, as well as satisfaction with life. While the partial mediation hints at the potential influence of additional resources, the findings are consistent with existing literature on the protective effects of psychosocial resources for those with a history of early-life adversity [e.g., (21, 57, 69)]. However, in relation to physical health, only optimism was shown to be a significant mediator in the present study. While research on early-life adversity and resilience-related resources often focuses on mental health (70), studies have also identified a positive influence of resources on physical health. For instance, research by Sachs-Ericsson and colleagues (71) found that self-efficacy significantly mediated the relationship between childhood abuse and the number of current physical health problems in a sample of older adults. One explanation for this discrepancy may be differences in the operationalization of physical health. The present study employed a subjective self-assessment of physical health rather than an objective or more impartial indicator, such as the number of medical conditions, cardiovascular risk factors (e.g., smoking status, waist-to-hip ratio), or hospitalizations [e.g., (7, 71, 72)]. Another possible explanation for the significant mediation by optimism, may be that optimism is a more vital resource than self-efficacy or social support in relation to physical health. Studies have consistently shown that individuals with higher levels of optimism are more likely to engage in health-promoting behaviors, such as having a healthier diet, being more physically active, and being a non-smoker (73, 74). However, with limited research on resilience-related resources and physical health after early-life adversity, further investigation is required to elucidate the underlying mechanisms for physical health.
Regarding the moderated mediation in the second step, the inclusion of SOC-R into the model resulted in a significant moderation of the relationship between early-life adversity and all three resources. In support of the hypothesis, the mediating effects of the resources were greater for participants with a stronger SOC-R, compared to those with a weaker SOC-R. This suggests that a strong SOC-R may have a beneficial influence on (mental) health by mitigating the detrimental effect of early-life adversity on the resources of self-efficacy, optimism, and social support. These results are also in line with research on the original SOC construct, which showed higher SOC to be linked to higher levels of mental health-related resources [e.g., (30, 75, 76)].
Within the moderated mediation, the largest mediating effects were observed for satisfaction with life, which were on average 3.9 times larger for high SOC-R across the three resources (self-efficacy, optimism, social support). The inclusion of these resources expands on the initial studies on SOC-R, which established a positive association with life satisfaction in the context of (chronic and acute) stress and adversity (35, 36). It is also consistent with earlier research on SOC in older adulthood, such as the study by Wiesmann and Hannich (77), which found that SOC pooled the influence of physical health, everyday competence, social support, and self-esteem on general life satisfaction and satisfaction with health in older age. The findings could suggest that a strong SOC-R may be beneficial in relation to successful ageing processes. For instance, the selective optimization with compensation theory proposes that older adults can foster successful ageing by identifying or reprioritizing goals on which to focus resources and adapting to limitations (78). The current results may indicate that SOC-R could play a role in this process, as those with a strong SOC-R could better identify and utilize their resources to maintain satisfaction with life in older age (28, 35). Future longitudinal studies could assess whether differences in the level of SOC-R are linked to the application of the life management strategies selection, optimization, and compensation [e.g., (79, 80)]; and ultimately, to variations in resource utilization and health outcomes over time.
Regarding the mediating effects for mental health, the indirect effects at high levels of SOC-R were slightly larger for optimism and self-efficacy, followed by social support. This may indicate that for mental health, having a strong SOC-R is particularly relevant for the protective influence of individual (i.e., optimism, self-efficacy) rather than external (i.e., social support) resources. Social support may also have a reduced influence in this particular sample due to the history of early-life adversity, as studies have shown links to lower levels of social support and interpersonal difficulties in adulthood [e.g., (81)]. The current study also assessed overall perceived social support, whereas a more nuanced indicator of social support (e.g., structural, tangible, emotional) may reveal more specific findings regarding the effect on mental health. However, social support should not be overlooked, given the significant indirect effects on both mental health and satisfaction with life in the present study. SOC-R and perceived social support may represent important targets for intervention in this older adult cohort, given the potential for alterations in social functioning [e.g., trust, attachment, or interpersonal issues (82)] in those who experienced early-life adversity; combined with the generally reduced social network in later life [e.g., due to death, reduced mobility, or entry into care home (83)].
Regarding physical health, while the mediating effect of optimism was larger at high levels of SOC-R, this was only marginally significant. These findings on mental and physical health are consistent with the existing literature on SOC-R, which has previously demonstrated associations with mental health, but found limited evidence for a connection with physical health [e.g., (36)]. Similarly, research with the original SOC construct has most often identified strong associations with indicators of positive mental health, rather than physical health (84). For example, a study by Galletta and colleagues (85) assessed the relationship between SOC and health-related quality of life in adults with chronic illnesses. Results found that SOC was directly correlated with mental health, but not the physical health component of quality of life. Rather, SOC showed an indirect effect on physical health through mental health, with the authors concluding that SOC is a psychological process most relevant for mental health-related quality of life (85). However, given the limited research on the revised SOC-R and physical health, further studies should examine this relationship in more detail, with the inclusion of both objective and subjective physical health indicators.
The results of this study highlight several implications and recommendations for research and practice within the field of (mental) health promotion. As the first step in exploring the relationship between SOC-R and resilience-related resources after early-life adversity, the current analysis included self-efficacy, optimism, and social support as well-established psychosocial resilience resources [e.g., (21, 32)]. Given the partial mediating effects of these resources, future studies should expand this model to include additional internal and external psychosocial resources, such as self-esteem, self-compassion, coping beliefs, and attachment (25, 31, 86); as well as neurobiological factors, such as cortisol reactivity, inflammatory (dys-)regulation, and hypothalamic-pituitary-adrenal (HPA) axis function (26, 75). Going beyond interpersonal resources, consideration of the broader cultural and socio-ecological influences on SOC-R could include factors such as cultural value orientations, community cohesion, and utilization of health services (16, 21, 87). Such cultural and societal factors can influence how an individual processes adversity and activates coping resources (17). For example, stigma or silence surrounding child abuse, as well as negative stereotypes and expectations about masculinity, may reduce the likelihood that individuals, particularly men, seek help or access mental health services (75, 88). Replication of this study in other cultures and contexts, with a focus on potential gender differences, may reveal unique relationships between resources that could inform (gender- or culture-specific) targets for intervention [e.g., (89)]. Nevertheless, the current findings identify SOC-R and the psychosocial resources self-efficacy, optimism, and social support as potential intervention targets for older adults affected by early-life adversity, particularly in relation to mental health and satisfaction with life.
Regarding practice implications, therapeutic intervention approaches that aim to strengthen SOC-R may improve individuals' awareness and utilization of their internal and external resources. For example, a group-based approach to narrative therapy aiming to increase sense of coherence may help to foster a positive self-identity, enhance social support, and promote confidence in coping through resource use by providing a supportive environment for self-reflection and shared coping narratives (90). Applying a salutogenic orientation to health promotion, clinicians could utilize salutogenic dialogue for the improvement of health literacy, i.e., increasing patients' awareness of their strengths, resources, and capabilities with regard to managing their own health conditions [e.g., (91)]. This could enhance patient wellbeing and help facilitate a paradigm shift towards preventive intervention and a salutogenic model of healthcare.
Furthermore, consideration of the limitations of the present study can also provide direction for future research. First, it should be emphasized that this study applied a cross-sectional, retrospective design, which precludes the establishment of causal relations. To provide stronger evidence for causality, future studies using longitudinal, prospective designs should investigate if similar moderating and mediating effects can be observed, exploring the causal directionality of SOC-R, resources, and health and wellbeing. Second, although attempts were made to ensure the sample was proportioned to the general population (40), these findings represent the target sample of Irish (older) adults with experiences of early-life adversity and may therefore not be generalizable. Future research could examine resilience-related resources and (mental) health in younger samples or in larger nationally representative surveys. Third, the scoring of the PCS and MCS as distinct physical and mental dimensions of health status may mask findings on the subscale level, as well as potential links between physical and mental health. Future studies could benefit from the inclusion of more nuanced or correlated indicators of physical and mental health. Fourth, the subjective self-assessment of physical health used in the present study may limit the interpretation of the physical health findings. Future research could include more objective or impartial indicators of physical health to provide a more comprehensive understanding of the relationship between resilience-related resources and physical health. Last, the measure of early-life adversity employed in the present study encompassed several adversity types, including abuse, neglect, and witnessed domestic violence (1). While this provides a comprehensive assessment of early-life adversity, the specific adversity types may have vastly different impacts on (mental) health and wellbeing [e.g., (92)]. In examining the influence of SOC-R and resilience-related resources, future studies could examine the impact of distinct adversity types (e.g., sexual, physical, and emotional abuse; physical and emotional neglect; witnessed violence). In addition, as the current study focused on individual and interpersonal resources, future studies could build on these findings to explore the relationship between SOC-R and broader cultural or socio-ecological resources, such as cultural norms and values, shared religious and spiritual beliefs, or community structures and resources (16, 17). Nevertheless, despite these limitations, the present study represents a useful addition to the literature on the role of SOC-R and resilience-related resources in the relationship between early-life adversity and later-life (mental) health. It also provides preliminary empirical support for the theoretical assumptions of SOC-R, namely, that a strong SOC-R can facilitate the utilization of available and appropriate resources to overcome adversity (28).
4.1. Conclusion
Key findings from the present study suggest that a strong SOC-R may have a beneficial influence on health and wellbeing by mitigating the detrimental effect of early-life adversity on the resources self-efficacy, optimism, and social support. The effects of these resilience-related resources were greater for individuals with a strong (rather than weak) SOC-R. Defined as the ability to perceive, integrate, and balance life experiences in order to facilitate health maintenance; SOC-R was particularly influential for mental health and life satisfaction in this older adult sample with a history of early-life adversity. Regarding the implications, the findings can also highlight potential impacts on the field of mental health promotion. For instance, having a strong SOC-R could be important for healthy or successful ageing, with an avenue for future research focusing on the potential role of SOC-R in the selection and adaptation of goals and resources into older age. Furthermore, given its moderating role between early-life adversity and psychosocial resources, SOC-R may represent a promising target for inclusion in psychotherapeutic interventions. For example, enhancing SOC-R may help to improve awareness and utilization of resources as a pathway to mental health and wellbeing and promote resilience in survivors of childhood trauma or adversity. In sum, by providing initial evidence for a beneficial role of SOC-R and the resilience-related resources self-efficacy, optimism, and social support, this study contributes to the literature and adds to the understanding of the mechanisms underpinning the pathways to (mental) health and wellbeing following early-life adversity.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: The data that support the findings of this study are openly available in the Open Science Framework (OSF) at http://doi.org/10.17605/OSF.IO/K4H2U, identifier: DOI 10.17605/OSF.IO/K4H2U.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethics Committee of the Faculty of Arts and Social Sciences in the University of Zurich, Switzerland (ID 18.6.1), and the Human Research Ethics Committee—Humanities in University College Dublin, Ireland (ID HS-18-30-Carr). The patients/participants provided their written informed consent to participate in this study.
Author contributions
MVT and SLR were responsible for the conceptualization and methodological design of the project, as well as funding acquisition, project administration, resourcing, and supervising. SLR was responsible for the investigation process. FB was responsible for the formal analysis. Writing and preparation of the original draft was done by SLR and FB; with critical review, commenting, and editing by MVT and AM. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by Swiss National Science Foundation, National Research Program 76, “Welfare and Coercion—Past, Present and Future” (grant number 407640_177355/1), as well as the Swiss Government Excellence Scholarship (ESKAS-Nr. 2016.0109) which funded the first author's (SLR) position until August 2019.
Acknowledgments
The authors wish to thank all participants who took part in this study. We would also like to thank Clodagh Cogley, Nathalie Golec, Tina Tanner, Penelope Adams, and Flavia Eigenmann for their assistance in conducting the study. This study was also supported by the University Research Priority Program (URPP) “Dynamics of Healthy Aging” at the University of Zurich.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization (WHO). Adverse childhood experiences international questionnaire (ACE-IQ). (2020). Available at: https://www.who.int/publications/m/item/adverse-childhood-experiences-international-questionnaire-(ace-iq)
2. Humphreys KL, King LS, Sacchet MD, Camacho MC, Colich NL, Ordaz SJ, et al. Evidence for a sensitive period in the effects of early life stress on hippocampal volume. Dev Sci. (2019) 22(3):e12775. doi: 10.1111/desc.12775
3. Nelson CA, Gabard-Durnam LJ. Early adversity and critical periods: neurodevelopmental consequences of violating the expectable environment. Trends Neurosci. (2020) 43(3):133–43. doi: 10.1016/j.tins.2020.01.002
4. McKay MT, Cannon M, Chambers D, Conroy RM, Coughlan H, Dodd P, et al. Childhood trauma and adult mental disorder: a systematic review and meta-analysis of longitudinal cohort studies. Acta Psychiatr Scand. (2021) 143(3):189–205. doi: 10.1111/acps.13268
5. Miller NE, Lacey RE. Childhood adversity and cardiometabolic biomarkers in mid-adulthood in the 1958 British birth cohort. SSM Popul Health (2022) 19: 101260, 1–10. doi: 10.1016/j.ssmph.2022.101260
6. Johnson WF, Huelsnitz CO, Carlson EA, Roisman GI, Englund MM, Miller GE, et al. Childhood abuse and neglect and physical health at midlife: prospective, longitudinal evidence. Dev Psychopathol. (2017) 29(5):1935–46. doi: 10.1017/S095457941700150X
7. Thoma MV, Bernays F, Eising CM, Pfluger V, Rohner SL. Health, stress, and well-being in Swiss adult survivors of child welfare practices and child labor: investigating the mediating role of socio-economic factors. Child Abuse Negl. (2021) 111:104769. doi: 10.1016/j.chiabu.2020.104769
8. Hughes K, Ford K, Bellis MA, Glendinning F, Harrison E, Passmore J. Health and financial costs of adverse childhood experiences in 28 European countries: a systematic review and meta-analysis. Lancet Public Health. (2021) 6(11):e848–57. doi: 10.1016/S2468-2667(21)00232-2
9. Thoma MV, Bernays F, Pfluger V, Eising CM, Rohner SL. An exploratory comparison of resilience profiles of Swiss older adult survivors of child welfare-related maltreatment and controls. Clin Psychol Psychother. (2022) 29(3):1059–67. doi: 10.1002/cpp.2691
10. Dubowitz H, Thompson R, Proctor L, Metzger R, Black MM, English D, et al. Adversity, maltreatment, and resilience in young children. Acad Pediatr. (2016) 16(3):233–9. doi: 10.1016/j.acap.2015.12.005
11. Yoon S, Pei F, Logan J, Helsabeck N, Hamby S, Slesnick N. Early childhood maltreatment and profiles of resilience among child welfare-involved children. Dev Psychopathol. (2022):1–13. Advance online publication. doi: 10.1017/S0954579421001851
12. Bonanno GA. Loss, trauma, and human resilience: have we underestimated the human capacity to thrive after extremely aversive events? Am Psychol. (2004) 59(1):20–8. doi: 10.1037/0003-066X.59.1.20
13. Bonanno GA. Uses and abuses of the resilience construct: loss, trauma, and health-related adversities. Soc Sci Med. (2012) 74(5):753–6. doi: 10.1016/j.socscimed.2011.11.022
14. Masten AS, Narayan AJ. Child development in the context of disaster, war, and terrorism: pathways of risk and resilience. Annu Rev Psychol. (2012) 63:227–57. doi: 10.1146/annurev-psych-120710-100356
15. Rutter M. Resilience as a dynamic concept. Dev Psychopathol. (2012) 24(2):335–44. doi: 10.1017/S0954579412000028
16. Liu JJW, Reed M, Fung KP. Advancements to the multi-system model of resilience: updates from empirical evidence. Heliyon. (2020) 6(9):e04831. doi: 10.1016/j.heliyon.2020.e04831
17. Maercker A, Horn AB. A socio-interpersonal perspective on PTSD: the case for environments and interpersonal processes. Clin Psychol Psychother. (2013) 20(6):465–81. doi: 10.1002/cpp.1805
18. Zimmerman MA. Resiliency theory: a strengths-based approach to research and practice for adolescent health. Health Educ Behav. (2013) 40(4):381–3. doi: 10.1177/1090198113493782
19. Yoon S, Howell K, Dillard R, Shockley McCarthy K, Rae Napier T, Pei F. Resilience following child maltreatment: definitional considerations and developmental variations. Trauma Violence Abuse. (2021) 22(3):541–59. doi: 10.1177/1524838019869094
20. Day T, Kearney CA. Resilience variables and posttraumatic symptoms among maltreated youth. J Aggress Maltreat Trauma. (2016) 25(9):991–1005. doi: 10.1080/10926771.2016.1236358
21. Cosco T, Hardy R, Howe L, Richards M. Early-life adversity, later-life mental health, and resilience resources: a longitudinal population-based birth cohort analysis. Int Psychogeriatr. (2019) 31(9):1249–58. doi: 10.1017/S1041610218001795
22. Domhardt M, Münzer A, Fegert JM, Goldbeck L. Resilience in survivors of child sexual abuse: a systematic review of the literature. Trauma Violence Abuse. (2015) 16(4):476–1493. doi: 10.1177/1524838014557288
23. Meng X, Fleury MJ, Xiang YT, Li M, D’Arcy C. Resilience and protective factors among people with a history of child maltreatment: a systematic review. Soc Psychiatry Psychiatr Epidemiol. (2018) 53(5):453–75. doi: 10.1007/s00127-018-1485-2
24. Masten AS, Lucke CM, Nelson KM, Stallworthy IC. Resilience in development and psychopathology: multisystem perspectives. Annu Rev Clin Psychol. (2021) 17:521–49. doi: 10.1146/annurev-clinpsy-081219-120307
25. Höltge J, Rohner SL, Heim EM, Nater U, Thoma MV. Differential pathways from child maltreatment types to insecure adult attachment styles via psychological and social resources: a Bayesian network analysis. J Interpers Violence. (2023) 38(11–12):7089–114. doi: 10.1177/08862605221140039
26. Kuzminskaite E, Penninx BWJH, van Harmelen AL, Elzinga BM, Hovens JGFM, Vinkers CH. Childhood trauma in adult depressive and anxiety disorders: an integrated review on psychological and biological mechanisms in the NESDA cohort. J Affect Disord. (2021) 283:179–91. doi: 10.1016/j.jad.2021.01.054
28. Bachem R, Maercker A. Development and psychometric evaluation of a revised sense of coherence scale. Eur J Psychol Assess. (2018) 34(3):206–15. doi: 10.1027/1015-5759/a000323
29. Antonovsky A. The salutogenic model as a theory to guide health promotion. Health Promot Int. (1996) 11(1):11–8. doi: 10.1093/heapro/11.1.11
30. Gustavsson-Lilius M, Julkunen J, Keskivaara P, Lipsanen J, Hietanen P. Predictors of distress in cancer patients and their partners: the role of optimism in the sense of coherence construct. Psychol Health. (2012) 27(2):178–95. doi: 10.1080/08870446.2010.484064
31. Wiesmann U, Dezutter J, Hannich H-J. Sense of coherence and pain experience in older age. Int Psychogeriatr. (2014) 26(1):123–33. doi: 10.1017/S1041610213001695
32. Sölva K, Haselgruber A, Lueger-Schuster B. Resilience in the face of adversity: classes of positive adaptation in trauma-exposed children and adolescents in residential care. BMC Psychol. (2023) 11:30, 1–13. doi: 10.1186/s40359-023-01049-x
33. Thoma MV, Mc Gee SL, Fegert JM, Glaesmer H, Brähler E, Maercker A. Evaluation of the revised sense of coherence scale in a representative German sample. PLoS One. (2018) 13(12):e0209550. doi: 10.1371/journal.pone.0209550
34. Behnke A, Conrad D, Kolassa I-T, Rojas R. Higher sense of coherence is associated with better mental and physical health in emergency medical services: results from investigations on the revised sense of coherence scale (SOC-R) in rescue workers. Eur J Psychotraumatol. (2019) 10(1):1606628, 1–12. doi: 10.1080/20008198.2019.1606628
35. Mc Gee SL, Höltge J, Maercker A, Thoma MV. Sense of coherence and stress-related resilience: investigating the mediating and moderating mechanisms in the development of resilience following stress or adversity. Front Psychiatry. (2018) 9:378. doi: 10.3389/fpsyt.2018.00378
36. Rohner SL, Bernays F, Maercker A, Thoma MV. Salutary mechanisms in the relationship between stress and health: the mediating and moderating roles of sense of coherence-revised. Stress Health. (2022) 38(2):388–401. doi: 10.1002/smi.3093
37. Bentler PM, Chou C-P. Practical issues in structural modeling. Sociol Methods Res. (1987) 16(1):78–117. doi: 10.1177/0049124187016001004
38. Boomsma A. Nonconvergence, improper solutions, and starting values in LISREL maximum likelihood estimation. Psychometrika. (1985) 50(2):229–42. doi: 10.1007/BF02294248
39. Majeed M, Irshad M, Fatima T, Khan J, Hassan MM. Relationship between problematic social media usage and employee depression: a moderated mediation model of mindfulness and fear of COVID-19. Front Psychol. (2020) 11:557987, 1–13. doi: 10.3389/fpsyg.2020.557987
40. Qualtrics. Qualtrics (computer software) (2018). Available at: https://www.qualtrics.com.
41. Unipark & QuestBack. Unipark EFS survey software (computer software) (2018). Globalpark AG. Available at: http://www.unipark.com/de/.
42. Mc Gee SL, Höltge J, Maercker A, Thoma MV. Evaluation of the revised sense of coherence scale in a sample of older adults: a means to assess resilience aspects. Aging Ment Health. (2018) 22(11):1438–47. doi: 10.1080/13607863.2017.1364348
43. Christoforou R, Ferreira NB. Psychometric assessment of adverse childhood experiences international questionnaire (ACE-IQ) with adults engaging in non-suicidal self-injury. Mediterr J Clin Psychol. (2020) 8:3. doi: 10.6092/2282-1619/mjcp-2601
44. Ware JE, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. (1992) 30(6):473–83. doi: 10.1097/00005650-199206000-00002
45. Jenkinson C, Coulter A, Wright L. Short form 36 (SF36) health survey questionnaire: normative data for adults of working age. Br Med J. (1993) 306(6890):1437–40. doi: 10.1136/bmj.306.6890.1437
46. Ware JE, Kosinski M, Bayliss MS, McHorney CA, Rogers WH, Raczek A. Comparison of methods for the scoring and statistical analysis of SF-36 health profile and summary measures: summary of results from the medical outcomes study. Med Care. (1995) 33(Suppl 4):264–79.
47. Diener E, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale. J Pers Assess. (1985) 49(1):71–5. doi: 10.1207/s15327752jpa4901_13
48. Schwarzer R, Jerusalem M. Generalized self-efficacy scale. In: Weinman J, Wright S, Johnston M, editors. Measures in health psychology: A user’s portfolio. Causal and control beliefs. Windsor: NFER-NELSON (1995). p. 35–7.
49. Scholz U, Doña BG, Sud S, Schwarzer R. Is general self-efficacy a universal construct? Psychometric findings from 25 countries. Eur J Psychol Assess. (2002) 18(3):242–51. doi: 10.1027/1015-5759.18.3.242
50. Scheier MF, Carver CS, Bridges MW. Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): a reevaluation of the life orientation test. J Pers Soc Psychol. (1994) 67(6):1063–78. doi: 10.1037/0022-3514.67.6.1063
51. Cohen S, Mermelstein R, Kamarck T, Hoberman HM. Measuring the functional components of social support. In: Sarason IG, Sarason BR, editors. Social support: Theory, research and applications. NATO ASI series, vol 24. Dordrecht: Springer (1985). p. 73–94. doi: 10.1007/978-94-009-5115-0_5
52. Cohen S. (2008). Basic psychometrics for the ISEL 12 item scale. Available at: https://www.cmu.edu/dietrich/psychology/stress-immunity-disease-lab/scales/index.html.
53. Merz EL, Roesch SC, Malcarne VL, Penedo FJ, Llabre MM, Weitzman OB, et al. Validation of interpersonal support evaluation list-12 (ISEL-12) scores among english- and Spanish-speaking Hispanics/Latinos from the HCHS/SOL sociocultural ancillary study. Psychol Assess. (2014) 26(2):384–94. doi: 10.1037/a0035248
54. Stekhoven DJ, Bühlmann P. Missforest–non-parametric missing value imputation for mixed-type data. Bioinformatics. (2012) 28(1):112–8. doi: 10.1093/bioinformatics/btr597
55. Sinharay S, Stern HS, Russell D. The use of multiple imputation for the analysis of missing data. Psychol Methods. (2001) 6(4):317–29. doi: 10.1037/1082-989X.6.4.317
56. Stevens JP. Outliers and influential data points in regression analysis. Psychol Bull. (1984) 95(2):334–44. doi: 10.1037/0033-2909.95.2.334
57. Su Y, Meng X, Yang G, D’Arcy C. The relationship between childhood maltreatment and mental health problems: coping strategies and social support act as mediators. BMC Psychiatry. (2022) 22(1):359. doi: 10.1186/s12888-022-04001-2
58. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. (2008) 40(3):879–91. doi: 10.3758/brm.40.3.879
59. Baron RM, Kenny DA. The moderator–mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. (1986) 51(6):1173–82. doi: 10.1037/0022-3514.51.6.1173
60. Kenny DA, Kashy D, Bolger N. Data analysis in social psychology. In: Gilbert D, Fiske S, Lindzey G, editors. Handbook of social psychology. 4th ed. Boston, MA: McGraw-Hill (1998). p. 233–65.
61. MacKinnon DP, Lockwood CM, Williams J. Confidence limits for the indirect effect: distribution of the product and resampling methods. Multivariate Behav Res. (2004) 39(1):99–128. doi: 10.1207/s15327906mbr3901_4
62. Scharkow M. Bootstrapping. In: Matthes J, Davis CS, Potter RF, editors. The international encyclopedia of communication research methods. Hoboken, NJ: John Wiley & Sons (2017). doi: 10.1002/9781118901731.iecrm0017
64. Preacher KJ, Rucker DD, Hayes AF. Addressing moderated mediation hypotheses: theory, methods, and prescriptions. Multivariate Behav Res. (2007) 42(1):185–227. doi: 10.1080/00273170701341316
65. Crandall A, Miller JR, Cheung A, Novilla LK, Glade R, Novilla MLB, et al. ACEs and counter-ACEs: how positive and negative childhood experiences influence adult health. Child Abuse Negl. (2019) 96:104089, 1–9. doi: 10.1016/j.chiabu.2019.104089
66. Bender R, Lange S. Adjusting for multiple testing—when and how? J Clin Epidemiol. (2001) 54(4):343–9. doi: 10.1016/s0895-4356(00)00314-0
67. Akinwande MO, Dikko HG, Samson A. Variance inflation factor: as a condition for the inclusion of suppressor variable(s) in regression analysis. Open J Stat. (2015) 5(7):754–67. doi: 10.4236/ojs.2015.57075
68. Dong Y, Peng CY. Principled missing data methods for researchers. SpringerPlus. (2013) 2(1):222, 1–17. doi: 10.1186/2193-1801-2-222
69. Herrenkohl TI, Jung H, Klika JB, Mason WA, Brown EC, Leeb RT, et al. Mediating and moderating effects of social support in the study of child abuse and adult physical and mental health. Am J Orthopsychiatry. (2016) 86(5):573–83. doi: 10.1037/ort0000136
70. Afifi TO, MacMillan HL, Boyle M, Cheung K, Taillieu T, Turner S, et al. Child abuse and physical health in adulthood. Health Rep. (2016) 27(3):10–8.26983007
71. Sachs-Ericsson N, Medley AN, Kendall-Tackett K, Taylor J. Childhood abuse and current health problems among older adults: the mediating role of self-efficacy. Psychol Violence. (2011) 1(2):106–20. doi: 10.1037/a0023139
72. Non AL, Román JC, Clausing ES, Gilman SE, Loucks EB, Buka SL, et al. Optimism and social support predict healthier adult behaviors despite socially disadvantaged childhoods. Int J Behav Med. (2020) 27(2):200–12. doi: 10.1007/s12529-020-09849-w
73. Scheier MF, Carver CS. Dispositional optimism and physical health: a long look back, a quick look forward. Am Psychol. (2018) 73(9):1082–94. doi: 10.1037/amp0000384
74. Trudel-Fitzgerald C, James P, Kim ES, Zevon ES, Grodstein F, Kubzansky LD. Prospective associations of happiness and optimism with lifestyle over up to two decades. Prev Med. (2019) 126:105754, 1–16. doi: 10.1016/j.ypmed.2019.105754
75. Idan O, Eriksson M, Al-Yagon M. Generalized resistance resources in the salutogenic model of health. In: Mittelmark MB, Bauer GF, Vaandrager L, Pelikan JM, Sagy S, Eriksson M, et al. editors. The handbook of salutogenesis. 2nd ed. Cham: Springer (2022). p. 93–106. doi: 10.1007/978-3-030-79515-3_12
76. Trap R, Rejkjær L, Hansen EH. Empirical relations between sense of coherence and self-efficacy, national Danish survey. Health Promot Int. (2016) 31(3):635–43. doi: 10.1093/heapro/dav052
77. Wiesmann U, Hannich H-J. The contribution of resistance resources and sense of coherence to life satisfaction in older age. J Happiness Stud. (2013) 14(3):911–28. doi: 10.1007/s10902-012-9361-3
78. Baltes PB, Baltes MM. Psychological perspectives on successful aging: the model of selective optimization with compensation. In: Baltes PB, Baltes MM, editors. Successful aging: Perspectives from the behavioral sciences. Cambridge: Cambridge University Press. (1990). p. 1–34. doi: 10.1017/CBO9780511665684.003
79. Freund AM, Baltes PB. Life-management strategies of selection, optimization and compensation: measurement by self-report and construct validity. J Pers Soc Psychol. (2002) 82(4):642–62. doi: 10.1037/0022-3514.82.4.642
80. Jopp D, Smith J. Resources and life-management strategies as determinants of successful aging: on the protective effect of selection, optimization, and compensation. Psychol Aging. (2006) 21(2):253–65. doi: 10.1037/0882-7974.21.2.253
81. Sperry DM, Widom CS. Child abuse and neglect, social support, and psychopathology in adulthood: a prospective investigation. Child Abuse Negl. (2013) 37(6):415–25. doi: 10.1016/j.chiabu.2013.02.006
82. Pfaltz MC, Halligan SL, Haim-Nachum S, Sopp MR, Åhs F, Bachem R, et al. Social functioning in individuals affected by childhood maltreatment: establishing a research agenda to inform interventions. Psychother Psychosom. (2022) 91(4):238–51. doi: 10.1159/000523667
83. McLaughlin D, Adams J, Vagenas D, Dobson A. Factors which enhance or inhibit social support: a mixed-methods analysis of social networks in older women. Ageing Soc. (2011) 31(1):18–33. doi: 10.1017/S0144686X10000668
84. Eriksson M. The sense of coherence: the concept and its relationship to health. In: Mittelmark MB, Bauer GF, Vaandrager L, Pelikan JM, Sagy S, Eriksson M, et al. editors. The handbook of salutogenesis. 2nd ed. Cham: Springer (2022). p. 61–8. doi: 10.1007/978-3-030-79515-3_9
85. Galletta M, Cherchi M, Cocco A, Lai G, Manca V, Pau M, et al. Sense of coherence and physical health-related quality of life in Italian chronic patients: the mediating role of the mental component. BMJ Open. (2019) 9(9):e030001. doi: 10.1136/bmjopen-2019-030001
86. Pfluger V, Rohner SL, Eising CM, Maercker A, Thoma MV. Associations between complex trauma exposure in childhood/adolescence and psychopathology in older age: the role of stress coping and coping self-perception. J Child Adolesc Trauma. (2021) 15(3):539–51. doi: 10.1007/s40653-021-00419-0
87. Xiu D, Mc Gee SL, Maercker A. Sense of coherence and posttraumatic growth: the moderating role of value orientation in Chinese and Swiss bereaved parents. J Loss Trauma. (2018) 23(3):259–70. doi: 10.1080/15325024.2018.1436120
88. Rohner SL, Salas Castillo AN, Michel J, Maercker A, Carr A, Thoma MV. A socio-interpersonal perspective on the disclosure of childhood adversity: a qualitative comparative approach in Irish survivors. J Fam Trauma Child Custody Child Dev. (2023). 1–21. Advance online publication. doi: 10.1080/26904586.2023.2177234
89. Bachem R, Makhashvili N, Maercker A, Javakhishvili JD, Aeschlimann A, Pilauri K, et al. University students’ life stressors and mental health in Georgia and German-speaking Switzerland: exploring the role of fatalism, sense of coherence, cross-cultural coping, and help-seeking. Int Perspect Psychol Res Pract Consult. (2023). 12(3):164–74. doi: 10.1027/2157-3891/a000067
90. Langeland E, Gjengedal E, Vinje HF. Building salutogenic capacity: a year of experience from a salutogenic talk-therapy group. Int J Ment Health Promot. (2016) 18(5):247–62. doi: 10.1080/14623730.2016.1230070
91. Rojatz D, Nowak P, Bahrs O, Pelikan JM. The application of salutogenesis in primary care. In: Mittelmark MB, Bauer GF, Vaandrager L, Pelikan JM, Sagy S, Eriksson M, et al. editors. The handbook of salutogenesis. 2nd ed. Cham: Springer. (2022). p. 419–32. doi: 10.1007/978-3-030-79515-3_38
Keywords: early-life adversity, sense of coherence—revised, resilience-related resources, mental health and wellbeing, moderated mediation
Citation: Rohner SL, Bernays F, Maercker A and Thoma MV (2023) Early-life adversity and later-life mental health: a conditional process analysis of sense of coherence and resilience-related resources. Front. Child Adolesc. Psychiatry 2:1213142. doi: 10.3389/frcha.2023.1213142
Received: 27 April 2023; Accepted: 4 August 2023;
Published: 16 August 2023.
Edited by:
Stine Lehmann, University of Bergen, NorwayReviewed by:
Georgios Giannakopoulos, National and Kapodistrian University of Athens, Aghia Sophia Children's Hospital, GreeceAyten Bilgin, University of Essex, United Kingdom
© 2023 Rohner, Bernays, Maercker and Thoma. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shauna L. Rohner c2hhdW5hLnJvaG5lckBvc3QuY2g=