
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Child Adolesc. Psychiatry , 13 December 2023
Sec. Developmental Psychopathology and Mental Health
Volume 2 - 2023 | https://doi.org/10.3389/frcha.2023.1114850
This article is part of the Research Topic Rising Stars in Developmental Psychopathology and Mental Health: 2024 View all 3 articles
 Vera Lees1
Vera Lees1 Rosie Hay1Helen Bould1,2,3Alex S. F. Kwong2
Rosie Hay1Helen Bould1,2,3Alex S. F. Kwong2 Daniel Major-Smith4,5
Daniel Major-Smith4,5 Daphne Kounali2
Daphne Kounali2 Rebecca M. Pearson2,6*
Rebecca M. Pearson2,6*
Background: The Covid-19 pandemic and related public health measures, including lockdowns and school closures, have impacted on mental health of children.
Aims and hypothesis: We hypothesised that there would be an association between maintaining a routine during lockdown and both lower emotional and behavioural difficulties in children and lower parental anxiety. Routine was taken as keeping to the same basic activities such as mealtimes and bedtimes. We also hypothesised that children of ‘keyworker’ parents would have fewer emotional and behavioural symptoms due to having maintained more normal routines. The key reason was that children of keyworkers still attended school or nursery and parents would have been getting up and coming home at the same times as pre-Covid. Keyworker status was defined as those whose work was essential to Covid-19 response, including work in health and social care and other key sectors.
Methods: We used data from the Avon Longitudinal Study of Parents and Children (ALSPAC) to explore associations between maintaining a routine, and emotional and behavioural difficulties in children, using linear regression models. All eligible ALSPAC-G2 participants were sent the survey and the responders are representative of the eligible G2 population. We included measures of parental anxiety. We separately explored associations with having a keyworker parent. We used the Carey Infant Temperament Questionnaire and the Revised Rutter Parent Scale for Preschool Children to establish levels of emotional and behavioural difficulties. The measures were chosen to match previous waves in multi-generations in ALSPAC where they had been shown to be predictive of later mental health in children. The scales measure emotional and behavioural problems.
Results: Two hundred eighty-nine parents completed questionnaires about their 411 children. Keeping a routine was associated with emotional and behavioural difficulty scores 5.0 points lower (95% CI −10.0 to −0.1), p = 0.045 than not keeping a routine. Parents who reported keeping a routine had anxiety scores 4.3 points lower (95% CI −7.5 to −1.1), p = 0.009 than those who did not. Children of keyworkers tended to have lower emotional and behavioural difficulty scores [−3.1 (95%CI −6.26 to 0.08), p = 0.056] than children of non-keyworkers. All models were adjusted for relevant potential confounders.
Conclusion: Maintaining a routine may be beneficial for both child emotional wellbeing and parental anxiety, although it is also possible that lower parental anxiety levels made maintaining a routine easier. Being the child of a keyworker parent during lockdown may have been protective for child emotional wellbeing.
The Covid-19 pandemic affected populations across the globe, sparing no one (1). Families with small children had additional challenges not only to support their children with education, but also to explain, contain and navigate their children's emotions at times of global uncertainty and unpredictability. Many parents continued to work from home at the same time (2). Reactions to Covid-19 can present a once in a lifetime opportunity to find out about family life at times when families had to deal with health threats as well as the loss of social contacts (2). With such losses there are associated anxieties (3). Babore et al., observed that parents’ experiences during the lockdown, including prohibition of all relational contacts outside of the home and inability to access support, job insecurity and ill health of friends and loved ones, likely impacted parents’ distress levels, with a possible impact on children's well-being (4).
Parenting stress has been shown to impact on the emotional wellbeing of their children, with association between maternal anxiety and psychological difficulties in their children (4–6). Parents with higher perceived parenting stress were less sensitive to their children's needs and showed more dysfunctional interactions with their children (4). Similarly, Morelli et al. found that parental distress impacted on the emotional regulation of their children and that this was magnified in children with a chronic health condition and their parents (7, 8). Masi et al. examined the impact of the pandemic on children with neurodevelopmental disabilities, and found that these children were exercising less, had increased television and digital media use, had a poorer diet and poorer sleep quality during the Covid-19 pandemic (9). We can infer that routine had changed for these families during the pandemic (9). From this previous research, it is understandable that pressures from a pandemic may result in increased parental stress within a family system and subsequently impact on the emotional wellbeing of children and young people during this time.
However, Co-Space Study, set up to increase understanding of how families coped throughout the Covid-19 pandemic, in one of their earlier reports surveying parents in August 2020 found that lockdown was beneficial to young children despite childcare challenges. According to parents’ reports children's emotional problems did not increase or decrease during the month of the survey. Additionally, employed parents/carers, but not those who were unemployed, reported a reduction in their child's behavioural and restless/attentional difficulties over the one-month period, however the changes were subtle (10).
Overall accumulating global evidence suggests that the Covid-19 pandemic and associated public health measures including self-isolation, lockdowns and school closures have had a significant negative impact on the mental health of children and young people (11–13). There have been increases in mental distress, eating disorders and self-harm amongst children and young people (13). Data on younger children is lacking, but our own previous work indicates a rise in emotional and behavioural symptoms in primary school aged and younger children (14). It is important to understand factors implicated in such rises, particularly those which could be protective for children and young people. A better understanding of protective factors gives potential to target appropriate intervention to support the mental health of younger children in the event of future pandemics or Covid-19 suppression measures.
One possible protective candidate, which evidence suggests is helpful in children’s daily life, is maintaining routine (17). Routine helps us plan, deliver, predict what to expect, and may protect us from anxiety during stressful times (16, 17). Structure and consistency are important for children; for example, keeping regular mealtimes and bedtimes can help children feel safe and secure (17). Predictability and familiarity are especially important for children who are still learning and growing, and has also been shown to be important in the context of adolescent mental health (18).
Routines have also been suggested as an area of focus for intervention among families living in chaotic households with young children who present with behavioural problems and bedtime resistant behaviour (19). The Covid-19 pandemic and responses to mitigate its effect significantly disrupted routine for both children and their parents. Family routines were upset by the disruption of engagement with most activities, educational, work, social and even basic established routines such as shopping (1, 2). Babore also highlights that the social distancing measures associated with the pandemic and related changes to childcare routines meant many mothers developed new routines and set new limitations with their children (4).
The UK entered its first national lockdown on 23rd March 2020. Lockdown meant that schools were closed to children, other than children of keyworkers and those considered vulnerable. The British government specified categories of these keyworkers whose work was essential to Covid-19 response, including work in health and social care and other key sectors (20). Children defined as vulnerable included those on child protection plans with local authorities and those who struggled to engage with education remotely (18). For many children during lockdown, their normal routine completely disappeared: their schooling changed, their social contacts, hobbies and childcare changed; and many were no longer able to be in contact with grandparents and extended family. Parents’ routines also changed, with some multitasking home-working with home-schooling or childcare, and others being furloughed from employment. Restrictions were partially lifted with children in nursery, Reception, Year 1 and Year 6 able to return from 1st June 2020. From 15th June 2020, Year 10 and Year 12 were permitted limited contact to help prepare for exams.
One study has found that the pandemic has affected behaviours of children and adolescents, in that it has led to decreased physical activity and disrupted sleep patterns (21). The NHS Digital Survey of Mental Health of Children and Young People also demonstrated significant changes for children and young people in terms of their education and usual activities due to the Covid-19 pandemic (22).
In addition to routines supporting children's mental health, childcare availability and the associated routines may also impact parental mental health, including anxiety (17). Research shows that parents’ individual distress has been associated with poor mental health in children. Specifically, depression and anxiety in mothers were shown as risk factors for depressive and anxiety symptoms in children (4). Previous research into the consequences of being quarantined during the H1N1 influenza outbreak, found that stressful isolation resulted in increased psychological distress in parents which subsequently impacted on the wellbeing of their children (23).
As the previous research suggests that routine has a protective role for children's mental health, we hypothesised that keeping to routine would be associated with fewer emotional and behavioural difficulties in children during unprecedented public health crisis and we examined the associations between routine and emotional and behavioural difficulties. As evidence suggests routine can impact and reduce anxiety in parents, we hypothesised an association with routine and lower parental anxiety. We explored the impact of Covid-19 on children of keyworkers. Keyworker parents were more likely to have maintained their usual routine, therefore we hypothesised that being a keyworker parent would be associated with fewer emotional and behavioural problems in children. Their children were able to continue attend educational setting during lockdown, therefore they may have been less affected by routine disruption. However, children may have been more worried both about themselves catching the virus and their parents being at risk of Covid as frontline workers. To demonstrate an association between routine and a child and parental stress this study will highlight that routine was associated with reduced stress in both a child and a parent and thus may be a mutual protective factor.
The Avon Longitudinal Study of Parents and Children (ALSPAC) is an ongoing population-based study that recruited pregnant women residing in Avon in the south west of England with expected delivery dates between 1st April 1991 and 31st December 1992 (24–26). The cohort consists of mothers and their partners (G0) associated with 15,454 pregnancies, resulting in 15,589 foetuses (G1) of which 14,901 were alive at 1 year of age. In 2012, ALSPAC began recruiting and collecting data on the next generation, G2, the children of the G1 participants and grandchildren of the originally recruited G0 women (also known as the ‘children of the children of the 90s’). G2 participants can join the study at any time (from early pregnancy onwards), through an open cohort (27). As with the original study, data are being collected from both parents (at least one of whom is a G1 participant) and their children. The study website contains details of all data available through a fully searchable data dictionary (http://www.bristol.ac.uk/alspac/researchers/our-data/).
In June 2020, G1 parents (mean age ∼28 years) completed a questionnaire about each of their G2 children (27), and a questionnaire about themselves (28). These questionnaires were completed early in the Covid-19 pandemic (between 26th May and 5th July 2020), as part of ALSPAC's Covid-19 data collection strategy (29). Study data were collected and managed using REDCap electronic data capture tools hosted at the University of Bristol (30). REDCap is a secure web application for building and managing online surveys and databases.
Participants were asked whether they kept a similar routine (e.g., bedtime, mealtimes) to how things were before the official lockdown was announced on 23rd March 2020, with response options “no, not at all”, “yes, a bit”, “yes, a lot” and, “yes, completely”. The latter two categories were combined into one due to low frequency of participants endorsing the original separate categories, resulting in three categories in total.
G1 parents were asked whether they were a keyworker, or whether their work had been classified as critical to the Covid-19 response, with options “yes”, “no”, or “don’t know”.
Parents who participated in the Covid-19 survey completed one of two assessments regarding their child's feelings and behaviour since the lockdown. The assessment version depended on the child's age. Parents of children less than 36 months old (henceforth referred to as younger children) completed the mood and distractibility subscales of the Carey Infant Temperament Questionnaire (ITQ) (31). Parents of older children (ages 36 months and older) completed the Revised Rutter Parent Scale for Preschool Children (32). Measures which were the same as, or as close as possible to the two used during the pandemic were selected from assessments completed by G1 parents before the pandemic. The same standardised scores were used (32).
Parental anxiety was measured using the GAD-7, a 7-item questionnaire with scores ranging between 0 and 21, with scores >10 indicating probable generalised anxiety disorder (33).
The following covariates were included: maternal age in years (continuous variable); parity (continuous variable); maternal education (binary variable: GCSE equivalent or below, or A level or above); child’s age in years (continuous) and child’s gender (binary).
Linear regression models were employed, with standardised emotional behavioural problems as the outcome, and routine and keyworker status as separate categorical exposure variables. Analyses were adjusted for relevant confounding variables for the specific association under investigation considering the relationship with the exposures and outcomes. Relevant variables included child age, gender and maternal education, maternal age, parental anxiety and parity. Amongst the ALSPAC-G2 children, there were 122 sib-sets, and therefore we accounted for clustering using robust standard errors, clustered on parent ID (34–36). We also ran linear regression models of the association between maternal anxiety and routine. The relationship between child emotional difficulties and parent anxiety is likely to be complex and bi-directional therefore we did not include the two variables in the same model and rather in this work present the associations with routine. All analyses were adjusted for child age, gender and maternal education, maternal age and parity and were conducted in Stata v.15/MP. Linear regression was chosen due to the simple nature of the analysis question and interpretability of the coefficients. The coefficients are the estimated effects.
Mixed effects linear regression would have been an alternative way of modelling this data and would lead to more efficient estimates albeit with slightly different interpretation. The implemented approach leads to the most conservative estimates for standard errors (34–36).
The design in relation to the analysis is cross sectional, the exposure and outcome used in the paper are measured at the same time.
In total, 411 G2 children had questionnaire data, completed by their 289 parents, 234 parents had complete data. This resulted to 328 out of 411 children having complete data. Because there are multiple different questionnaires with different information 83 were missing at least one answer on one of the surveys. Of these 411 G2 children, 214 (52%) were male. The median age for G2 children was 34 months (IQR 16–71 months) (28). Of the 411 children, 404 had complete data on keeping a routine. Of those with data, 41 (10%) did not keep the same routine; 182 (44%) kept the same routine “a bit”, 181 (44%) kept the same routine either “a lot” or “completely”.
Of the 411 children, 328 had complete data including for all covariates. The analyses reported here concern the children with complete data. The reason for incomplete parental data is that at the time when the first Covid-19 survey was rolled out, the participating parents’ children were not old enough to have participated in the scheduled ALSPAC clinics where detailed assessments and demographic data are collected (11). There were no differences in the difficulty scores between the children excluded because there was no parental data and those included in the adjusted analyses. This reduced statistical power but there was no evidence that those with missing data were different in key variables (for example they were not higher on anxiety scores), therefore there is unlikely to be any systematic biases.
We found a linear pattern between the extent of keeping routine and lower emotional and behavioural difficulties in the children (Figure 1). This association was not altered by clustering by maternal ID, or by adjusting for child gender, maternal parity, maternal and child age, maternal educational background (Table 1; higher difficulties scores indicate more emotional and behavioural difficulties). Compared to families where no routine was kept, children of those parents reporting keeping “a lot” or “completely” the same routine to before lockdown had emotional and behavioural difficulty scores 5 points lower (95% CI −10.02 to −0.12; p = 0.045). There was less evidence of a difference in emotional and behavioural difficulties between those reporting keeping the same routine “a bit” in comparison to those not keeping the same routine at all.
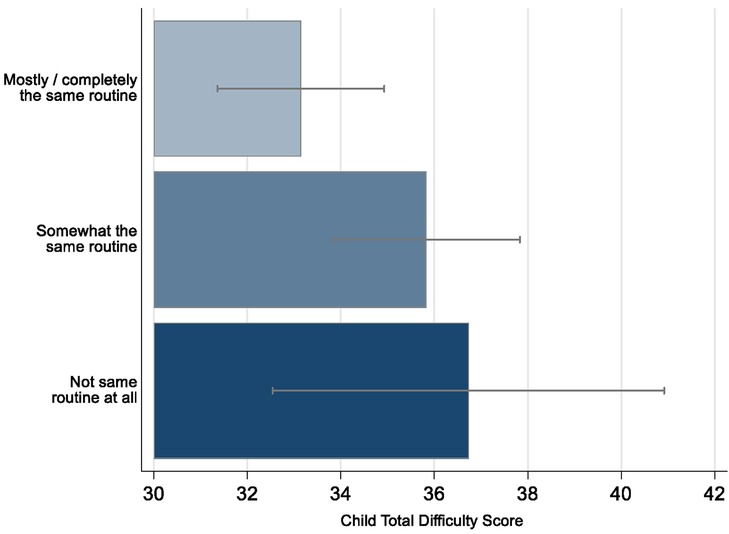
Figure 1. COVID-19 pandemic related total difficulty scores in children by keeping routine in ALSPAC. The error bars represent 95% CI.
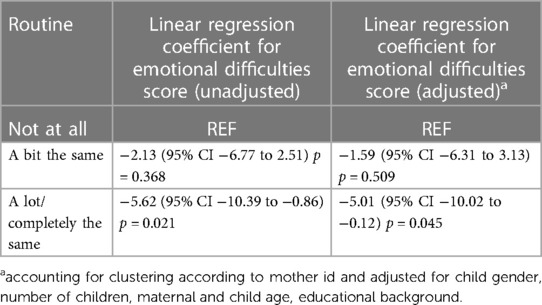
Table 1. Linear regression comparing the association between the extent of routine and child difficulties score.
Parents of 314 G2 children had data on anxiety measured in the second Covid-19 questionnaire and on childcare routines. Parents who kept to a routine were less anxious than those who did not, again finding a linear pattern (Figure 2). A mean GAD score of 11.2 (95% CI 9.82–12.51) (indicating probable generalised anxiety disorder) was found in the group that did not follow a routine at all. Parents who kept to the same routine “a bit” had a mean GAD score of 8.9 (95% CI 8.28–9.54). Those parents who followed “a lot/completely the same” routine had mean GAD score of 7.5 (95% CI 6.78–8.20). Table 2 shows the results of the linear regression analyses describing the association between routine and parental anxiety. The magnitude of change in anxiety scores is considered clinically meaningful, with such changes in symptoms of similar magnitude being associated with improvement following clinical interventions like Cognitive Behavioural Therapy (CBT) and perceived feelings of feeling better (37).

Figure 2. COVID-19 pandemic related parental anxiety score by keeping routine in ALSPAC. Error bars represent 95% CIs.
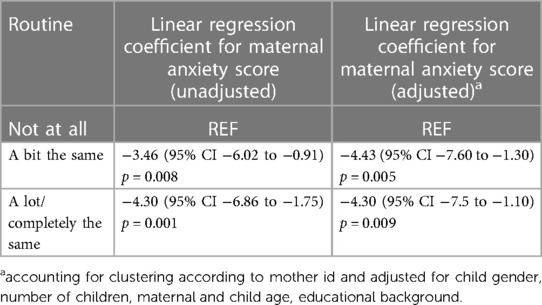
Table 2. Linear regression comparing the association between the extent of routine and maternal anxiety scores.
In the model taking into account maternal and child age, gender, maternal education and parity there was evidence that, compared to families where no routine was kept at all, parents who kept “a lot/completely the same routine” to before lockdown, had anxiety scores on average 4.3 points lower (95% CI −7.5 to −1.1; p = 0.009). Those who kept the same routine “a bit” had parental anxiety scores on average 4.4 points lower (95% CI −7.60 to −1.30; p = 0.005) than those who did not keep the same routine at all (Table 2).
147 children had one or both parents who were keyworkers; and 160 had one or both parents who were not keyworkers. Parents were counted more than once if they had more than one child.
Children with at least one keyworker parent were more likely to have kept similar routine to before lockdown than children with no keyworker parent {Figure 3, [Chi2 (2) 22.13, p < 0.001]}, whilst they were less likely to report they kept to ’somewhat same routine’ and no differences were apparent for ‘not at all same routine’.
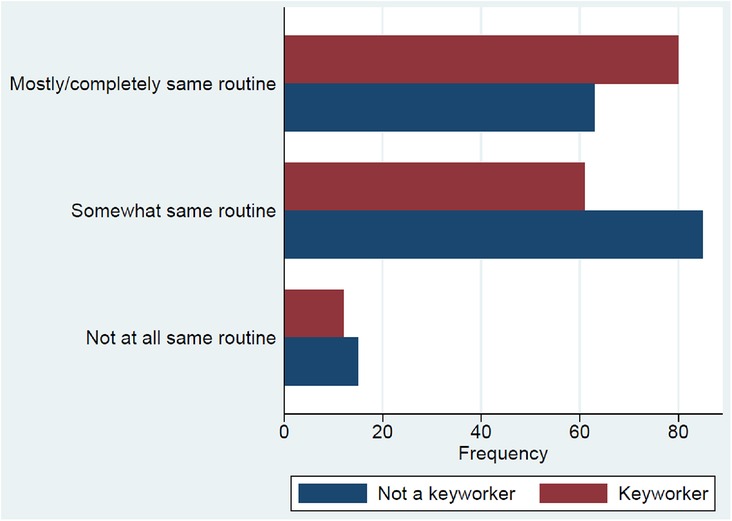
Figure 3. Routine kept by keyworker and non-keyworker parents.
Children of keyworkers were also reported to have fewer emotional and behavioural difficulties during lockdown than children of non-keyworkers (Figure 4). After adjusting for maternal and child age, maternal education, gender, and parental anxiety, keyworker children scored on average 3 points lower (95% CI −6.26–0.08; p = 0.056) than children of non-keyworkers. However, the evidence against an effect of this magnitude occurring under the null hypothesis is weaker, relative to some of our other results (Table 3).
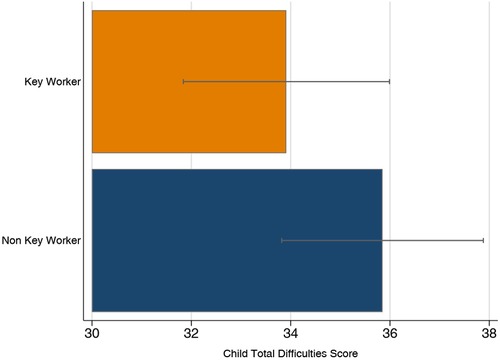
Figure 4. Difficulty scores for children of keyworkers and non-keyworkers. Error bars represent 95% CIs.

Table 3. Linear regression comparing the association between parental keyworker status and child difficulties scores.
We report evidence of an observed linear pattern between the extent to which parents perceived that routine stayed the same and lower emotional and behavioural difficulties scores in children, as well as lower anxiety in parents. Our results are consistent with previous studies that link parental mental health to the emotional wellbeing of children during Covid-19 (4, 22). It is also consistent with research reporting protective effects of routine on children's wellbeing outside of the pandemic (15, 38).
The mechanisms to explain the association remain unclear from this research alone. However, some speculation is possible. The onset of the Covid-19 pandemic and public health responses to it brought about significant changes for society, not least for the family unit and routines for families. Firstly, as descried by Lebow, changes in family dynamics as a consequence of the pandemic are likely to present multiple challenges due to suddenly unpredictable daily activities (3). Practical changes in times that would be normally structured around work and school were suddenly changed. In this explanation we argue that the change in routine impacted both parent and child independently to each other.
Secondly, the routine and structure may have been a consequence of less anxiety in the parent, their personality traits or indeed their own coping strategies to manage the pandemic. It is well known, Babore showed, that the effect of mothers’ individual distress on children's depression was mediated by mothers’ parenting stress (4). Given that maternal anxiety, routine and child emotional symptoms were all measured around the same time and it was not possible to track the precise time course of the impact on family dynamics both explanations remain possible. Either way our findings highlight that keeping a routine may be linked to positive outcomes, whether or not that is directly felt by the child or via improving mothers’ mood. Indeed, it is increasingly understood that emotional symptoms in families are transactional, bi-directional and in reality, hard to disentangle. Thus, although the mediating role of parenting stress on child mental health can be examined in longitudinal stuides (4), adjusting for maternal anxiety here would lead to uninterpretable results.
It is also not possible to draw firm conclusions on what specific aspect of routine may be significant in terms of being protective for children from this research. However, in this paper, routine refers to bedtimes and mealtimes, not wider routines like childcare settings, schooling, exercise/physical activity, and socialising and therefore it may be hypothesised that even simple and predictable habits such as times of eating and sleeping are linked to positive outcomes.
There is little previous research that has considered how being a ‘keyworker’ parent may affect children's emotional wellbeing. This is likely, in part, due to the fact that the term keyworker appears to be unique to the United Kingdom and became a specific concept during Covid-19 to consider ‘essential’ workforce in the short term. However, our findings that keyworker parents were more likely to keep routines, and a suggestion that emotional and behavioural difficulties scores were lower in children of keyworkers than those of non-keyworkers was in line with our hypothesis that parents’ work schedule continued without change. In addition, in the UK keyworker children were able to attend their education provision, albeit with an amended education programme, they also maintained more friendships and social routines. There was also a greater sense of being valued and purpose of those families who were keyworkers and this could provide a further explanation given that sense of purpose is associated with lower stress levels (39).
The data was from self-report which may not have reflected reality, for example, a parent may have perceived their routine was similar but actually objective data may have shown they were not. For example, getting up later or perhaps eating at different times. Passive data collection in phones could be a more objective way to study routine in the future, although this was not feasible in this study.
Whilst we have described evidence from other research that the lockdown has had a negative impact on the emotional wellbeing, there have also been some studies that found that the mental health and wellbeing of children and young people actually improved during the lockdown period. This was particularly true for young people who had poor mental health pre-pandemic and those who had difficulties with school and peer relationships at school (40, 41). A survey carried out by Pavlopoulou in 2020, whilst only a small cohort, demonstrated that while lockdown may have increased pressures for some autistic young people, others found that having less social pressure, lesser sensory challenges, and having more available time to spend on their own interests, was actually beneficial (42). However, they did identify that less support and lack of adapted work online, added to challenges for the families of autistic young people. This indicates that an individualised approach to stressful life events would be advisable.
This is a novel study looking at the effect of Covid-19 pandemic on younger children, using longitudinal pre and during pandemic data from the ALSPAC cohort.
The median age of the children in our study was 34 months. It is possible that the results may have been different if our cohort had included older children, as their increased awareness and understanding of Covid-19 and their keyworker parents being exposed to the virus could mean that their anxiety would be higher, even if their routines were maintained. Including adolescents in this study was not possible due to the demographic of the G2 cohort. In addition, it is possible that the relatively young age of the parents means that they have less stability in jobs and therefore this may contribute to how well routine could be maintained.
The population in the sample is limited in ethnic diversity and geographical spread, which may limit the generalisability of our results to other populations. It was not possible to mitigate this, as the cohort have self-selected into the ALSPAC study. We acknowledge that there may be differences in the results if the demographic of the participants was more diverse. In addition, ALSPAC has incomplete recruitment and loss to follow-up; the current recruitment at a relatively young age and the focus of analyses in cross-generational effects are more specific to ALSPAG-G2 (25). Furthermore, whilst we have attempted to adjust for factors that may confound the relationship between routine and emotional and behavioural difficulties, it is possible that residual confounding from unmeasured variables may affect this apparent relationship.
The cross-sectional nature of this work means that, although we have described an association between keeping routine and fewer behavioural and emotional difficulties in children, we are unable to determine the direction of causality, i.e., we cannot conclude that keeping to routine leads to lower emotional and behavioural difficulties, since it is also possible that children having fewer emotional and behavioural difficulties makes it easier to follow a routine. Furthermore, the phrasing of the questions on “routines” compares current routine to pre-lockdown routine. If there was little routine pre-lockdown, then answering “yes, completely” to maintaining routine during lockdown could still indicate lack of routine.
Importantly, child emotional and behavioural difficulties are reported by the parent. This is potentially subject to reporter bias. For example, where a parent is struggling with their own mental health, a child's usual behaviour may be perceived as more challenging because the parent is finding their child's behaviour more difficult to manage rather than because the child's behaviour has changed significantly (46). There is conflicting empirical evidence on the existence of systematic bias in the rating of child's behavioural and emotional problems and this is affected by the parent's mental health characteristics. However, previous work and sensitivity analyses using the same sample, did not find any evidence to support this (44). Our previous work demonstrated that while there are differences between parent and teacher or parent and child report of emotional symptoms, these differences are not associated with maternal depression or anxiety and therefore it is unlikely to be systematically biased by maternal depression or anxiety (45).
This is further supported by other studies suggesting that biases are negligible and that any differences in behaviours linked to reporters maybe the result of cross-situation differences in child behaviour, differential abilities of parents in recognising psychological problems and/or direct and indirect genetic confounding (46).
Whilst we have acknowledged the potential bias, though negligible, parent report measure was still felt to be the most appropriate way to gather a large amount of information for this research as there would not be a reliable way to gather information from the children themselves, due to their young age. Parents are the most appropriate people to report on observed differences in their children pre pandemic and during the pandemic in this cohort.
As Ofsted report emphasizes, school closures have resulted in children regressing in their learning as well as increasing mental health distress, eating disorders and self-harm (13, 46). Our research suggests an increase in emotional and behavioural difficulties, associated with difficulties maintaining childcare routines during the same period. We demonstrate that routines are associated with good mental health, both in children and in parents. Whilst we cannot confirm the direction of causality from these data alone, if causal, this would suggest that interventions to facilitate routines could help prevent difficulties. Most parenting advice regarding lockdown mentions keeping routine and this research supports that advice. Since it is possible that parents with higher levels of anxiety are less likely to have kept to the same routine, it may be that families need different levels of support to achieve this aim. Furthermore, it is possible that parents who are able to maintain a routine are more likely to be of the temperament to complete questionnaires which may introduce a reporting bias.
Our results also suggest that it is important to support parents’ mental health. Keeping childcare provision open may also mean that routines can be more consistent and may reduce anxiety for parents who are juggling work and childcare responsibilities. During future pandemics, public health services should support parents, and particularly mothers, in reducing individual distress and parenting stress, as these are also associated with children's depression (4).
Due to the breadth of data collection capturing multiple exposures, we were not able to identify specific roles of keyworker parents, or whether they started a new role as a keyworker during the pandemic. This would be an interesting area to consider in future research. This is a large cohort survey, which has highlighted the potential role of routine on emotional wellbeing. It has generated direction for more in depth research into specifics of routine, which may be captured by future studies using validated questionnaires to look at bedtime routine, for example.
In the event of a pandemic in the future, parents might benefit from being given information that would support them in maintaining a routine. For example, an online advice and guidance page with suggestions on how to achieve this. Similarly, information that is tailored for families of children with specific needs, such as neurodiversity or learning disability, would be beneficial for parents in these difficult circumstances. Now that online platforms are readily available and familiar to many, support programmes could be developed to ensure parents feel supported with helping their family keep to a routine.
We conclude that maintaining routine may be beneficial for children's emotional wellbeing as well as parental anxiety. Thus, maintaining routine may be a mutually protective factor. Further research exploring the direction of causation may provide us with greater understanding. Being the child of a keyworker parent during lockdown may have been protective for child emotional wellbeing. This may be reassuring to keyworkers, however further work to replicate this finding is needed. Whilst this study focused on the importance of maintaining routine during a pandemic, it is reasonable to surmise that during any time of stress, such as moving a house, an illness in a family or other significant change in life, maintain usual routine will be beneficial to emotional wellbeing for both children and parents.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethical approval for the study was obtained from the ALSPAC Ethics and Law Committee and the Local Research Ethics Committees. Informed consent for the use of data collected via questionnaires and clinics was obtained from participants following the recommendations of the ALSPAC Ethics and Law Committee at the time.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
The UK Medical Research Council and Wellcome (Grant ref: 217065/Z/19/Z) and the University of Bristol provide core support for ALSPAC This publication is the work of the authors VL, RH, HB, AK, DM-S, DK, RP and IC will serve as guarantors for the contents of this paper. This work was supported by European Research Council (ERC) under the European Union’s Seventh Framework Programme (grant FP/2007-2013), European Research Council Grant Agreements (grants 758813; MHINT). DM-S, HS, KT, and RP work in or are affiliated with a unit that receives funding from the University of Bristol and UK Medical Research Council (MC_UU_00011/3, MC_UU_00011/6, MC_UU_00011/7) A comprehensive list of grants funding is available on the ALSPAC website (http://www.bristol.ac.uk/alspac/external/documents/grant-acknowledgements.pdf); This research was specifically funded by Wellcome Trust and MRC (102215/2/13/2) and the UoB Faculty Research Director’s Discretionary Fund.
We are extremely grateful to all the families who took part in this study, the midwives for their help in recruiting them, and the whole ALSPAC team, which includes interviewers, computer and laboratory technicians, clerical workers, research scientists, volunteers, managers, receptionists and nurses, particularly during this challenging, uncertain and unprecedented period at the beginning of global pandemic. The content of this manuscript has been presented in part at the Royal College of Psychiatrists Faculty of Child and Adolescent Psychiatry Annual Conference (47).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Pawar M. The global impact of and responses to the COVID-19 pandemic. Int J Community Soc Dev. (2020) 2(2):111–20. doi: 10.1177/2516602620938542
2. Bolisani E, Scarso E, Ipsen C, Kirchner K, Hansen JP. Working from home during COVID-19 pandemic: lessons learned and issues. Management & Marketing. (2020) 15:458–76. doi: 10.2478/mmcks-2020-0027
4. Babore A, Trumello C, Lombardi L, Candelori C, Chirumbolo A, Cattelino E, et al. Mothers’ and children’s mental health during the COVID-19 pandemic lockdown: the mediating role of parenting stress. Child Psychiatry Hum Dev. (2023) 54(1):134–46. doi: 10.1007/s10578-021-01230-6
5. Tsotsi S, Broekman BFP, Sim LW, Shek LP, Tan KH, Chong YS, et al. Maternal anxiety, parenting stress, and preschoolers’ behavior problems: the role of child self-regulation. J Dev Behav Pediatr. (2019) 40(9):696–705. doi: 10.1097/DBP.0000000000000737
6. Spinelli M, Lionetti F, Pastore M, Fasolo M. Parents and children facing the COVID-19 outbreak in Italy. Front Psychol. (2020) 11:1713. doi: 10.3389/fpsyg.2020.01713
7. Morelli M, Cattelino E, Baiocco R, Longobardi E, Trumello C, Babore A, et al. Parents’ psychological factors promote children’s mental health and emotional regulation during the COVID-19 lockdown. Child Abuse Maltreat. (2021) 1:47–63. doi: 10.3280/MAL2021-001004
8. Bramanti SM, Manippa V, Babore A, Dilillo A, Marcellino A, Martucci V, et al. Comparing parental distress and children’s difficulties between parents of children with rheumatic diseases and parents of healthy children in families facing the COVID-19 pandemic. Curr Psychol. (2022) 42:1–10. doi: 10.1007/s12144-022-03589-8
9. Masi A, Mendoza Diaz A, Tully L, Azim SI, Woolfenden S, Efron D, et al. Impact of the COVID-19 pandemic on the well-being of children with neurodevelopmental disabilities and their parents. J Paediatr Child Health. (2021) 57(5):631–6. doi: 10.1111/jpc.15285
10. Co-Space Study (August 2020) Emotional & behavioural difficulties (August 2020) - Co-Space (cospaceoxford.org)
11. Kwong A, Pearson R, Adams M, Northstone K, Tilling K, Smith D, et al. Mental health before and during the COVID-19 pandemic in two longitudinal UK population cohorts. Br J Psychiatry. (2021) 218:1–10. doi: 10.1192/bjp.2020.242
12. Bignardi G, Dalmaijer ES, Anwyl-Irvine AL, Smith TA, Siugzdaite R, Uh S, et al. Longitudinal increases in childhood depression symptoms during the COVID-19 lockdown. Arch Dis Child. (2020) 106(8):791–7. doi: 10.1136/archdischild-2020-320372
13. Ofsted: Children Hardest Hit by COVID-19 Pandemic are Regressing in Basic Skills and Learning 2020. Available at Available at: https://www.gov.uk/government/news/ofsted-children-hardest-hit-by-covid-19-pandemic-are-regressing-in-basic-skills-and-learning (Accessed November 11, 2020).
14. Paul E, Kounali D, Kwong ASF, Smith D, Costantini I, Lawlor DA, et al. Trajectories of child emotional and behavioural difficulties before and during the COVID-19 pandemic in a longitudinal UK cohort. medRxiv. [Preprint] (2021). doi: 10.1101/2021.05.11.21257040
15. Spagnola M, Fiese BH. Family routines and rituals: a context for development in the lives of young children. Infants Young Child. (2007) 80:284–99. doi: 10.1097/01.IYC.0000290352.32170.5a
16. Markson S, Fiese BH. Family rituals as a protective factor for children with asthma. J Pediatr Psychol. (2000) 25(7):471–80. doi: 10.1093/jpepsy/25.7.471
17. Fugue P, Millar Y. Five Ways To Manage Your Wellbeing As A Parent During Lockdown. (2020) BBC Bitesize. Available at: https://www.bbc.co.uk/bitesize/articles/zrmhscw (Accessed November 9, 2020).
18. Lundgren K, Segal R. Parenting During Coronavirus (2020). Available at: https://www.helpguide.org/articles/parenting-family/parenting-during-coronavirus.htm (Accessed November 10, 2020)
19. Larsen KL, Jordan SS. Organized chaos: daily routines link household chaos and child behavior problems. J Child Fam Stud. (2019) 29:1094–107. doi: 10.1007/s10826-019-01645-9
20. Gov.uk. Children Of Critical Workers And Vulnerable Children Who Can Access Schools Or Educational Settings (2020) Available at: https://www.gov.uk/government/publications/coronavirus-covid-19-maintaining-educational-provision/guidance-for-schools-colleges-and-local-authorities-on-maintaining-educational-provision (Accessed July 2, 2021).
21. Bates LC, Zieff G, Stanford K, Moore JB, Kerr ZY, Hanson ED, et al. L. COVID-19 impact on behaviors across the 24-hour day in children and adolescents: physical activity, Sedentary Behavior, and Sleep. Children (Basel). 2020;7(9):138. doi: 10.3390/children7090138
22. Vizard T, Sadler K, Ford T, Newlove-Delgado T, McManus S, Marchaselli F, et al. Mental Health of Children and Young People. Digital NHS. (2020) Available at: https://files.digital.nhs.uk/CB/C41981/mhcyp_2020_rep.pdf (Accessed December 10, 2020).
23. Sprang G, Silman M. Posttraumatic stress disorder in parents and youth after health-related disasters. Disaster Med Public Health Prep. (2013) 7(1):105–10. doi: 10.1017/dmp.2013.22
24. Fraser A, Macdonald-Wallis C, Tilling K, Boyd AW, Golding J, Smith GD, et al. Cohort profile: the avon longitudinal study of parents and children: aLSPAC mothers cohort. Int J Epidemiol. (2013) 42(1):97–110. doi: 10.1093/ije/dys066
25. Northstone K, Lewcock M, Groom A, Boyd A, Macleod J, Timpson N, et al. The avon longitudinal study of parents and children (ALSPAC): an update on the enrolled sample of index children in 2019. Wellcome Open Res. (2019) 4:51. doi: 10.12688/wellcomeopenres.15132.1
26. Boyd A, Golding J, Macleod J, Lawlor DA, Fraser A, Henderson J, et al. Cohort profile: the ‘children of the 90s’; the index offspring of the avon longitudinal study of parents and children (ALSPAC). Int J Epidemiol. (2013) 42:111–27. doi: 10.1093/ije/dys064
27. Lawlor D, Lewcock M, Jones L, Rollings C, Yip V, Smith D, et al. The second generation of the avon longitudinal study of parents and children (ALSPAC-G2): a cohort profile. Wellcome Open Research. (2019) 4:36. doi: 10.12688/wellcomeopenres.15087
28. Smith D, Northstone K, Bowring C, Wells N, Crawford M, Pearson RM, et al. The avon longitudinal study of parents and children - a resource for COVID-19 research: generation 2 questionnaire data capture May-July 2020. Wellcome Open Res. (2021) 5:278. doi: 10.12688/wellcomeopenres.16414.2
29. Northstone K, Smith D, Bowring C, Wells N, Crawford M, Haworth S, et al. The avon longitudinal study of parents and children - a resource for COVID-19 research: questionnaire data capture May-July 2020. Wellcome Open Res. (2020) 5:210. doi: 10.12688/wellcomeopenres.16225.2
30. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. (2009) 42(2):377–81. doi: 10.1016/j.jbi.2008.08.010
31. Carey WB, McDevitt SC. Revision of the infant temperament questionnaire. Revision of the infant temperament questionnaire. Pediatrics. (1978) 61(5):735–9. doi: 10.1542/peds.61.5.735
32. Elander J, Rutter M. Use and development of the rutter parents’ and teachers’ scales. Int J Methods Psychiatr Res. (1996) 6:63–78. doi: 10.1002/(SICI)1234-988X(199607)6:2%3C63::AID-MPR151%3E3.3.CO;2-M
33. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166(10):1092–7. doi: 10.1001/archinte.166.10.1092
34. Rogers WH. Sg17: regression standard errors in clustered samples. In: Done. Newton DH, editor. Stata technical bulletin 13: 19–23. Reprinted in stata technical bulletin reprints. 3: pp. 88–94. College Station, TX: Stata Press (1993).
35. Huber PJ. The behavior of maximum likelihood estimates under non-standard conditions. Proceedings of the fifth Berkeley symposium on mathematical statistics and probability 1 (1967). p. 221–33
37. Button KS, Kounali D, Thomas L, Wiles NJ, Peters TJ, Welton NJ, et al. Minimal clinically important difference on the beck depression inventory–II according to the patient’s perspective. Psychol Med. (2015) 45(15):3269–79. doi: 10.1017/S0033291715001270
38. Koome F, Hocking C, Sutton D. Why routines matter: the nature and meaning of family routines in the context of adolescent mental illness. J Occup Sci. (2012) 19:312–25. doi: 10.1080/14427591.2012.718245
39. Law M, Steinwender S, Leclair L. Occupation, health and well-being. Canadian Journal of Occupational Therapy. (1998) 65(2):81–91. doi: 10.1177/000841749806500204
40. Widnall E, Winstone L, Mars B, Haworth CM, Kidger J. Young people’s mental health during the COVID-19 pandemic. University of Bristol: Bristol, UK (2020) Available at: https://sphr.nihr.ac.uk/research/young-peoples-mental-health-during-the-covid-19-pandemic/
41. Soneson E, Puntis S, Chapman N, Mansfield KL, Jones PB, Fazel M. Happier during lockdown: a descriptive analysis of self-reported wellbeing in 17,000 UK school students during COVID-19 lockdown. Eur Child Adolesc Psychiatry. (2023) 32:1131–46. doi: 10.1007/s00787-021-01934-z
42. Oliver C, Vincent C, Pavlopoulou G. The experiences of autistic young people & their parents of lockdown & the reopening of schools (education & Covid19 series). London: British Educational Research Association (2021) Available at: https://www.bera.ac.uk/publication/the-experiences-of-autistic-young-people-theirparents-of-lockdown-the-reopening-of-schools
43. Olino TM, Michelini G, Mennies RJ, Kotov R, Klein DN. Does maternal psychopathology bias reports of offspring symptoms? A study using moderated non-linear factor analysis. J Child Psychol Psychiatr. (2021) 62:1195–201. doi: 10.1111/jcpp.13394
44. Mackenbach JD, Ringoot AP, van der Ende J, Verhulst FC, Jaddoe VW, Hofman A, et al. Exploring the relation of harsh parental discipline with child emotional and behavioral problems by using multiple informants. The generation R study. PLoS One. (2014) 9(8):e104793. doi: 10.1371/journal.pone.0104793
45. Costantini I, Sallis H, Tilling K, Major-Smith D, Pearson RM, Kounali D-Z. Childhood trajectories of internalising and externalising problems associated with a polygenic risk score for neuroticism in a UK birth cohort study. JCPP Advances. (2023) 3(1):e12141. doi: 10.1002/jcv2.12141
Keywords: routine, child behavioural difficulties, child emotional difficulties, parental anxiety, COVID-19
Citation: Lees V, Hay R, Bould H, Kwong ASF, Major-Smith D, Kounali D and Pearson RM (2023) The impact of routines on emotional and behavioural difficulties in children and on parental anxiety during COVID-19. Front. Child Adolesc. Psychiatry 2:1114850. doi: 10.3389/frcha.2023.1114850
Received: 3 December 2022; Accepted: 2 November 2023;
Published: 13 December 2023.
Edited by:
Emanuela Del Giudice, Sapienza University of Rome, ItalyReviewed by:
Valerio Manippa, University of Bari Aldo Moro, Italy© 2023 Lees, Hay, Bould, Kwong, Major-Smith, Kounali and Pearson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rebecca M. Pearson Ui5QZWFyc29uQG1tdS5hYy51aw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.