 Sélim Benjamin Guessoum1,2,3*
Sélim Benjamin Guessoum1,2,3* Laelia Benoit3,4
Laelia Benoit3,4 Isaiah Thomas4
Isaiah Thomas4 Jasmina Mallet5,6Jordan Sibeoni7,8Cyril Hanin9
Jasmina Mallet5,6Jordan Sibeoni7,8Cyril Hanin9 Marie Rose Moro1,2,3
Marie Rose Moro1,2,3
- 1Université Paris Cité, PCPP, Paris, France
- 2Department of Child and Adolescent Psychiatry, AP-HP, Cochin University Hospital, Paris, France
- 3Université Paris-Saclay, Inserm U1018, CESP, Team DevPsy, Villejuif, France
- 4Yale School of Medicine, Child Study Center, New Haven, CT, United States
- 5Université Paris Cité, Inserm U1266, Institute of Psychiatry and Neuroscience of Paris, Paris, France
- 6Department of Psychiatry, AP-HP, Louis Mourier University Hospital, Colombes, France
- 7Centre Hospitalier d’Argenteuil, Department of Child and Adolescent Psychiatry, Argenteuil, France
- 8Université Paris Cité, Inserm U1153, ECSTRRA Team, Paris, France
- 9Centre de Référence des Maladies Rares à Expression Psychiatrique & PSYDEV Team, Department of Child and Adolescent Psychiatry, Pitié-Salpêtrière University Hospital, AP-HP, Sorbonne University, Paris, France
Child and adolescent psychiatry has been based on numerous fields of research and theories, including neuroscience, physiology, psychology (developmental, psychodynamic, systemic, cognitive-behavioral, etc.), anthropology, sociology, and education sciences. Integrating transdisciplinary knowledge in multi-level models is an ongoing challenge for the future that is not immediately applicable in clinical practice and research. Articulating, i.e., to connect, to be jointed, (psycho)biological and (psycho)social approaches in child and adolescent psychiatry is a daily challenge for clinicians and researchers. Research is often limited to specific fields whereas real-life clinical practice needs a pluralistic approach. Research designs, tools, and clinical training need to provide knowledge applicable to the necessarily pluralistic daily clinical practice. This article provides some perspectives on how to articulate biological and social approaches, from research to clinical practice, and discusses the concept of pluralistic approaches, multimodal interventions, and how to provide articulated mental health care and training. Suggestions to better articulate biological and social approaches are provided: (I) State that the research object can be approached from different theoretical, research and clinical angles and explain the one chosen; (II) Propose synthesis articles that articulate biological and social knowledge; (III) Design biological studies that take into account social factors, and design social studies that take into account biological factors; (IV) Design transcultural tools; (V) Build pluralistic interventions, i.e., therapeutic modalities and mental health care settings that articulate biological and social approaches; (VII) Develop training in pluralistic articulated care.
Introduction
Child and adolescent psychiatry (CAP) aims to treat disorders of thinking, feeling, and/or behavior affecting children, adolescents, and their families. Articulating biological and social approaches is necessary to grapple with the complexities of patients and mental disorders. As examples of this tension between biological and social approaches, one can cite the three following: (1) Possession by spirits in an adolescent from a Islamic culture could be a culturally meaningful non-psychotic syndrome or a psychotic disorder or both could be interrelated with one another; such complexities can lead to misdiagnosis; (2) Anorexia nervosa has clear neurobiological correlates, including a strong genetic component, but family therapy, which focuses on environmental, familial, and social factors, is an evidence-based treatment (1–3); (3) Autism spectrum disorder has been progressively explained through in-depth knowledge at the genomic, molecular, cellular, and neural-circuit levels, yet interventions focus on improving interactions and communication between patients and their families(4, 5). Further examples are detailed in Table 1.
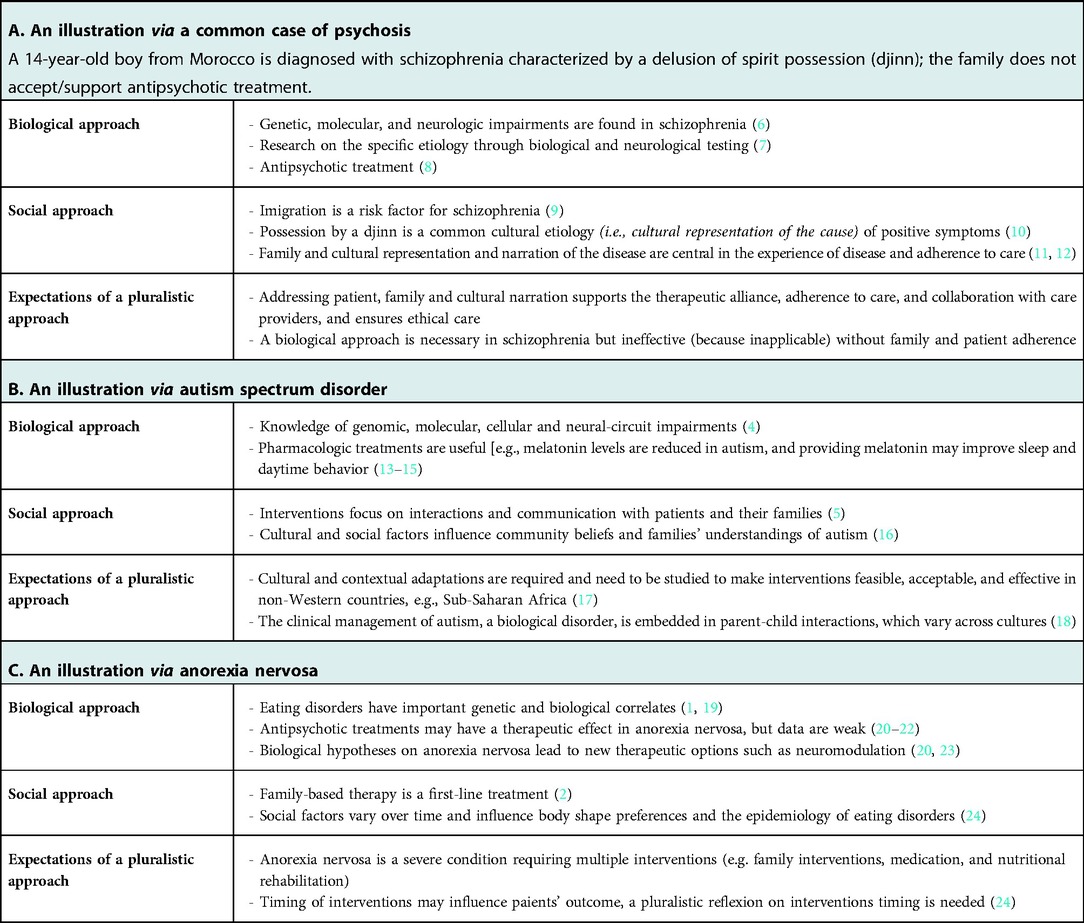
Table 1. Examples.
Child and adolescent psychiatry has been based on numerous fields of research and theories, including neuroscience, genetics, physiology, psychology (developmental, psychodynamic, systemic, cognitive-behavioral, etc.), anthropology, sociology, and education sciences. Over the past 70 years, we have witnessed the demise of “big” theories in CAP purporting to offer overarching explanations and in its place the development of specialized research fields that provide strategies for tackling particular questions (25). Leon Eisenberg, a prominent U.S. child psychiatrist and pioneer in autism and ADHD research, criticized knowledge silos in CAP as leading to ineffective and even harmful interventions. In a dramatic but meaningful formulation, Eisenberg described the shift from overly psychoanalytic to overly biological psychiatry during the second half of the 20th century as a switch from “brainless” to “mindless” psychiatry (26). Various fields in CAP are evolving simultaneously, with distinct theories, concepts, representations, and interventions. In this article, we schematize the diversity of approaches into (psycho)biological approaches vs. (psycho)social approaches. Biological approaches refer to the conception of psychiatry as a medical science based on biology, physiology and neuroscience. This perspective posits that biology grounds medical practice and that other sciences can contribute but cannot displace biology from its central role (27). Biological approaches have brought important changes to CAP, such as the vast body of research on the use of stimulants to treat ADHD (25). Nevertheless, social approaches, such as sociology and anthropology, are critical in CAP: These approaches are grounded in the concept that humans are fundamentally social beings, and that social factors are key determinants of health (28). Thus, in the context of CAP, the child is not only an individual and must be viewed within a larger familial, social, and cultural context (29).
Evidence-based medicine (EBM) has influenced research methods in the last few decades, promoting quantitative research, which tends to exclude cultural factors, and thus minority groups, in order to obtain homogeneous study populations. Consequently, there is scarce transcultural data in CAP (30, 31). This lack of research knowledge and the need for updated and integrative diagnostic and interventional models remains a challenge in the field. A pluralistic approach argues that multiple independent methods are necessary in the understanding and treatment of mental illness and that no single method is sufficient (32).
There are numerous obstacles that impede the implementation of a pluralistic approach in CAP: the difficulty of identifying and treating diseases in CAP; objects in CAP are multiple and heterogeneous [e.g., Kleinman's developments on the personal and social meanings disease, illness, and sickness (33, 34)]; the divide between biologically oriented child psychiatrists and other types of child psychiatrists (35); the lack of unifying theories and the pragmatic oversimplification for the sake of practice and training (36). Integrative transdisciplinary models in research are promising, but they are not immediately applicable to clinical practice [e.g., translational social neuroscience (37); cultural neuroscience (38); neurophenomenology (39)]. In our opinion, significant gaps persist between biological and social approaches, and between theory, research, and clinical practice. The objective of this article is to provide practical perspectives on how to articulate (i.e., to connect, to be jointed) biological and social approaches in CAP.
Definitions: pluralistic articulated approach
Biological and social approaches have not only different theories and concepts (self, disorders, emotions, etc.), but also different methodologies. Biological research is more often quantitative and nomothetic, i.e., it provides standardized, generalizable knowledge on disorders. Social research is often qualitative and idiographic, i.e., it provides in-depth knowledge on the experience of patients (40, 41), though numerous nomothetic studies also exist in the social sciences. Nomothetic methods do not take into account the personal and subjective factors involved in patients' disorders. In contrast, idiographic methods, based on the patient and his or her particular features, can help identify the social experience of mental disorders.
We provide brief definitions of some important concepts in the Supplementary materials, and we highlight three of them here: pluralistic, complementary and integrative. A pluralistic approach states that multiple independent methods are necessary in the understanding and treatment of mental illness and that no single method is sufficient (32). In pluralistic approaches, the conceptual differences are assumed to understand mental and brain phenomena (32). Care providers can combine actions from different fields and theories, wondering which ones are relevant in a given case (rather than applying a little of each for every disorder). Complementary frames of reference (complémentarisme) is a concept historically based on George Devereux's French school of transcultural psychiatry: it argues for the necessary non-simultaneous use of several methods (at the time, anthropology and psychoanalysis) (42). Integrative psychiatry aims at providing a synthetic approach to the distinct psychiatry fields (41). In this article, we use the term pluralistic approach to refer to the use of multiple independent methods, articulated rationally and non-simultaneously but with possible overlap, in accordance with both evidence-based and patient-centered medicine.
There are essentially two options: (1) To assume a pluralistic approach with separated concepts and research methods, or (2) To build models whose theories encompass the traditionally separated fields. With the first option, one can study a single theme with two or more methods via distinct research protocols. For example, one can perform, on the one hand, biological studies on adolescent depression and, on the other hand, social research on this topic (43, 44). The objects, methods, and theories would be distinct between these methods. As another example, within a single team, in adult psychiatry, we performed, on the one hand, a quantitative epidemiological study and, on the other hand, a qualitative psychological study on care providers' mental health during the COVID-19 pandemic (45, 46). The second option, integrating typically separate fields, requires a wider and deeper theoretical foundation. Achieving this goal would be, in our opinion, the most ambitious and important transformation for the future of psychiatry (47). Like biological processes, social factors influence the brain's development and functioning. For example, children in situations of severe social isolation demonstrate abnormal brain development and language impairments (48). Proposing sociobiological models could constitute the future of CAP (49). Until then, clinicians and researchers still require perspectives to grapple with the coexistence of social and biological approaches.
Research: articulating biological and social approaches from clinical description to research
The articulation of social and biological approaches should be carried out starting from the clinical description phase. Otherwise, if psychiatrists follow a standard descriptive criteriologic approach, only a part of the patients' experience—the objective, standardized, generalizable and observable aspects—will be reported and thus shape the research perspectives. Additionally, the expression of mental distress varies within populations and across cultures, depending on social and biological factors, and is also characterized by distinct cultural presentations that demand a social assessment by psychiatrists [e.g., hikikomori syndrome in adolescents (50)].
Collecting and synthesizing both sociocultural knowledge and neurobiological knowledge on a subject is not an obvious approach, but we argue that it should be more widely utilized. We applied this synthetic approach to study clinical lycanthropy, a syndrome in which patients have the delusional belief that he or she is turning into a wolf (51, 52). We conducted a systematic review of medical publications and linked together biological and cultural knowledge (53). The reader thus witnesses the clear necessity of both approaches: clinical lycanthropy is related to neuropsychiatric disorders, but it occurs in a particular environmental and cultural context. Consequently, we hope that any reader on this topic will have a representation of clinical lycanthropy that integrates both approaches. Next steps consist of offering multilevel perspectives that include the brain and its environment (47).
We offer the following suggestions:
• [I] All available sociocultural and biological data should be included in clinical descriptions and case reports. Psychiatrists should exhibit the same precision in describing both the biological (neurological) and social features of disease as early psychiatrists did in their meticulous clinical observations;
• [II] Biological studies should consider the social context, and social studies should consider the biological context;
• [III] Scientific syntheses (e.g., reviews) should gather both biological and social data.
Tools: build tools that meet the needs of pluralism
Pertinent validated tools (e.g., questionnaires and scales), designed for research or clinical practice, are keystones to articulating biological and social approaches. Instruments are scarce in CAP, and their use is complicated by the dynamic aspect of development and the necessary adaptation of instruments to the age and developmental stage of each patient. Standard rating scales can reflect a nomothetic representation of the measured variables, whereas transcultural validity includes an idiographic perspective.
The tools available to us shape research designs and clinicians’ representations, notably by capturing some cultural forms of mental health experiences, while rendering others invisible. In standard evidence-based and nomothetic CAP approaches, there is a lack of culturally appropriate and transculturally valid instruments (54, 55). Some Western-derived scales distort or miss some culturally specific dimensions of mental distress, inducing a form of experience measure fallacy, or an error in measuring the experience of patients by superimposing Western experiences of mental distress (as a parallel to Kleinman's category fallacy, referring the application of a nosological category developed for a particular cultural group to the members of another culture for whom it lacks coherence and validity has not been established) (56–58). A Western scale in adult psychiatry would miss a culturally meaningful form of dysphoria that the Afghan symptom checklist does capture: jigar khun, literally “liver blood,” is an extreme and persistent dysphoria that includes grief following interpersonal loss but that may also be a reaction to any deeply disappointing or painful experience (59).
As an example in CAP, several tools for autism spectrum disorder showed lower psychometric properties among immigrant minority groups, non-native speakers, and other cultural minorities from non-Western countries, attesting to a worldwide scarcity of validated and culturally attuned screening and diagnostic tools (17, 60). For example, the Autism Diagnostic Interview-Revised (ADI-R) in a Spanish-speaking population in the U.S. showed lower sensitivity and specificity rates than in the original validation that included only native English speakers (61). The Spanish version of ADI-R may be less valid when the parent and child's Spanish language proficiencies differ; if the parent speaks mostly Spanish and the child speaks mostly English with peers and at school, the ADI-R verbal communication questions may be less valid.
Efforts have been made to make ICD-11 culturally sensitive; however ICD-11, as a nomothetic nosography, is not intended to provide support for individual evaluation (62). The cultural formulation interview of DSM-5 includes interesting idiographic questions on cultural definitions of the problem, and some authors have suggested developing a supplementary module specifically for young children (63, 64). More tools are needed to assess other factors such as interactional aspects within a particular cultural context. The matter is complicated further by the changes that inevitably occur in culture over time, resulting in the need for regular reassessments and revisions of these instruments.
Some researchers have designed culturally pertinent scales: Phan et al. designed an adult psychiatric scale that is derived from Vietnamese idioms and cultural understandings of psychiatric and emotional distress identified in Vietnamese literature and using ethnographic methods (57). Another option is to propose transcultural validations and adaptations of existing scales [e.g., cross-cultural validation of the Positive and Negative Syndrome Scale (65)]. A third option is to intentionally develop tools, from their conception, to be applicable across cultures, such as: the PSYca, a tool designed to screen for psychological difficulties among children aged 6–36 months (66), and the ELAL scale, an instrument designed to assess language skills in any minority language and consequently better diagnose language disorders across various populations (65). Kohrt et al. propose criteria to evaluate the cross-cultural validity of CAP instruments, such as the incorporation of mention of local idioms employed, the structure of response sets, and comparisons with other measurable phenomena (67). Within a health justice framework, it is our ethical responsibility as child psychiatrists to develop tools that are adaptable to the needs of different patient populations.
Clinical practice: provide pluralistic articulated interventions
In clinical practice, it remains a challenge to implement this plurality of approaches and develop different narratives of a patient's condition that can coexist. Articulating pluralistic care in clinical practice can be promoted through the following axes:
• [I] train clinicians in pluralistic care;
• [II] ensure that these interventions are accessible to patients;
• [III] develop competency in determining the temporal sequence of care: which intervention is prioritized and/or can facilitate other interventions (e.g., family intervention is sometimes necessary before a patient can accept medical treatment, or vice versa);
• [IV] encourage diverse care teams with psychiatrists trained in distinct approaches (for complex patients).
For example, the management of eating disorders requires a pluralistic approach as well as a transdisciplinary care team (68, 69). Autism spectrum disorder is another example of a disorder that is explained with a biological approach, treated with interactional and behavioral treatments, and influenced by important cultural and social factors (16) (see Table 1). Some authors have proposed integrative frameworks that encompass developmental, multidimensional, eco-systemic, and multifactorial approaches and are associated with pluralistic interventions (70).
As an illustration of a pluralistic intervention, we carried out a study on a specific mental health care program for unaccompanied immigrant minors: Multimodal Co-Therapy for Unaccompanied Minors (MUCTUM) (Guessoum et al., under review). This monthly consultation brings together a standard biological approach (including pharmacological treatment), an institutional approach (aiming to improve caseworker-youth relationships and communication as well as solving stressful daily life problems), transcultural psychiatry (providing an interpreter who speaks the patient's native language and acts as a bond with the patient's native country, cultural affiliations, family, and culturally meaningful care), and a narrative approach (narration of the youth's story, immigration, and trauma). MUCTUM aims to provide a pluralistic approach through the use of two therapists with different backgrounds (a psychiatrist and a psychologist), further enriched by the participation of an interpreter and the youth's caseworker. MUCTUM is consistent with the idea that pluralism requires close collaboration among psychiatrists, psychologists, and social workers (32). In this study, we hypothesize that following a hierarchy of needs, through a patient-centered and problem-solving approach, could be one axis by which to articulate these interventions. We also hypothesize that a pluralistic approach could be provided through interventions in a single consultation with several care providers with both biological and cultural backgrounds. Implementation research for such approaches is much needed in CAP (71).
Training: pluralistic competency
Suggestions for training in pluralistic competency:
• [I] Provide a basic pluralistic theoretical training (introduction to biological and social approaches and how to articulate them in clinical practice) early on in medical school;
• [II] Make sure residents complete internships in both biological psychiatry-oriented and social psychiatry-oriented services;
• [III] Train faculty members in basic clinical and teaching skills for both approaches and promote dialogue among faculty members from different fields;
• [IV] Develop and teach interventions that articulate biological and social approaches;
• [V] Provide a model curriculum for pluralistic articulated training.
Training in social approaches is provided at several universities, such as (trans)cultural competency and structural competency (72, 73). McGill University's medical school curriculum provides training grounded in basic social science perspectives (74). Cultural competency notably includes an awareness of the impact of the clinician's own ethnocultural identity on patients, knowledge of the language and cultural background of groups seen in clinical practice and their interactions with mental health issues and treatment, and skills for working with particular groups (75). Structural competency training relies on developing a capacity to identify how social, economic, and political conditions produce health inequalities and can shape symptoms and diseases (72, 76). After identifying such factors, the clinician would then mobilize to address the inequities in the clinician-patient dynamic or in the patient's life. Transcultural competency developed in France (77), describes the ability of clinicians to provide culturally appropriate care, allowing the co-existence of medical and patients' cultural narratives and treatments. Training in transcultural psychiatry in Université Paris Cité in France is embedded in the early curriculum and provided in later programs for care providers and cultural mediation (73, 78). Training also occurs through mentoring during consultations, lecture courses, role-playing, or use of senior resident-assisted consultations.
Pluralistic competency would call for basic skills in both biological and social approaches, which enables one to identify the most suitable approach for a given patient and refer patients to specialists when necessary, e.g., having basic skills in transcultural psychiatry allows any clinician to seek for a cultural etiology of the disease and evaluate its importance in the patient's and their family's narration of the disorder and the need for specialized transcultural therapy if available. Another central aspect is dialogue, self-esteem, and collaborative work among care providers from different disciplines to achieve a pluralistic approach, including multidisciplinary staff meetings.
Discussion
This article discusses the articulation and implementation of a pluralistic approach. There is still a lack of appropriate tools, pluralistic syntheses, integrative knowledge, and training for professionals in these approaches. More biological studies should be conducted in non-Western countries to obtain results applicable in these settings and address the population homogeneity needed in many biological studies. Distinct avenues for cross-cultural perspectives allow for the comparison of data from disparate item sets and response formats, such as mega-analyses of aggregated heterogeneous data from many individuals (79).
Promoting the implementation of pluralistic care in psychiatry requires assessing its financial cost. Evidence exists for the economic and social value of specific interventions in CAP (80), e.g., proposing specialized transcultural care, in addition to standard approaches, may be cost-effective for health systems (81).
From an ethical standpoint, the driving force behind such research should be improving the quality of health care, not economic factors only (25, 82, 83). Promoting pluralistic research that includes social factors is necessary to provide just and equitable health care (84). This includes ethically justified exclusion criteria (82). Promoting such approaches requires that they be available and accessible to both patients and professionals, and supporting free online access to diverse tools may be a simple contribution.
Articulating biological and social approaches in CAP in clinical practice and research is an ongoing challenge. As a conclusion, we provide highlights in Table 2.
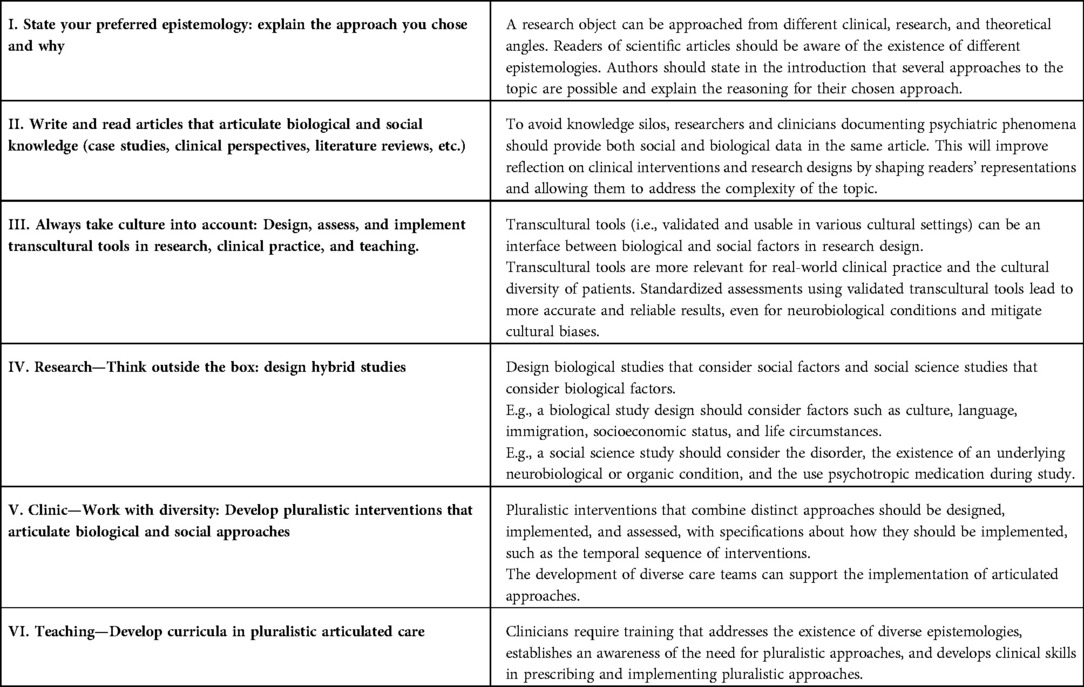
Table 2. Take-home messages for articulating biological and social approaches in child and adolescent psychiatry.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Author contributions
SBG conceived the first draft of the article. SBG, LB and IT took the lead in writing the manuscript, in consultation with MRM, CH, JM and JS. All authors provided critical feedback and helped shape the manuscript. All authors contributed to the article and approved the submitted version.
Acknowledgments
To Hajar Chokairi, Tania Sanchez and Thomas Bazeille, for their kind help by critical comments on the manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frcha.2022.1065932/full#supplementary-material.
References
1. Gorwood P, Blanchet-Collet C, Chartrel N, Duclos J, Dechelotte P, Hanachi M, et al. New insights in anorexia nervosa. Front Neurosci. (2016) 10:256. doi: 10.3389/fnins.2016.00256
2. Lock J, Le Grange D. Family-based treatment: where are we and where should we be going to improve recovery in child and adolescent eating disorders. Int J Eat Disord. (2019) 52(4):481–7. doi: 10.1002/eat.22980
3. de Jorge Martínez C, Rukh G, Williams MJ, Gaudio S, Brooks S, Schiöth HB. Genetics of anorexia nervosa: an overview of genome-wide association studies and emerging biological links. J Genet Genomics. (2022) 49(1):1–12. doi: 10.1016/j.jgg.2021.09.005
4. Willsey HR, Willsey AJ, Wang B, State MW. Genomics, convergent neuroscience and progress in understanding autism spectrum disorder. Nat Rev Neurosci. (2022) 23(6):323–41. doi: 10.1038/s41583-022-00576-7
5. Fuentes J, Hervás A, Howlin P, (ESCAP ASD Working Party). ESCAP Practice guidance for autism: a summary of evidence-based recommendations for diagnosis and treatment. Eur Child Adolesc Psychiatry. (2021) 30(6):961–84. doi: 10.1007/s00787-020-01587-4
6. Lakhan SE, Vieira KF. Schizophrenia pathophysiology: are we any closer to a complete model? Ann Gen Psychiatry. (2009) 8:12. doi: 10.1186/1744-859X-8-12
7. Kurukgy JL, Bourgin J, Benoit JP, Guessoum SB, Benoit L. Implementing organicity investigations in early psychosis: spreading expertise. PLoS One. (2021) 16(6):e0252610. doi: 10.1371/journal.pone.0252610
8. Driver DI, Thomas S, Gogtay N, Rapoport JL. Childhood-onset schizophrenia and early-onset schizophrenia spectrum disorders: an update. Child Adolesc Psychiatr Clin N Am. (2020) 29(1):71–90. doi: 10.1016/j.chc.2019.08.017
9. Chen L, Selvendra A, Stewart A, Castle D. Risk factors in early and late onset schizophrenia. Compr Psychiatry. (2018) 80:155–62. doi: 10.1016/j.comppsych.2017.09.009
10. Lim A, Hoek HW, Ghane S, Deen M, Blom JD. The attribution of mental health problems to jinn: an explorative study in a transcultural psychiatric outpatient clinic. Front Psychiatry. (2018) 9:89. doi: 10.3389/fpsyt.2018.00089
11. Rodolico A, Bighelli I, Avanzato C, Concerto C, Cutrufelli P, Mineo L, et al. Family interventions for relapse prevention in schizophrenia: a systematic review and network meta-analysis. Lancet Psychiatry. (2022) 9(3):211–21. doi: 10.1016/S2215-0366(21)00437-5
12. Tranulis C, Goff D, Henderson DC, Freudenreich O. Becoming adherent to antipsychotics: a qualitative study of treatment-experienced schizophrenia patients. Psychiatr Serv. (2011) 62(8):888–92. doi: 10.1176/ps.62.8.pss6208_0888
13. Tordjman S, Anderson GM, Pichard N, Charbuy H, Touitou Y. Nocturnal excretion of 6-sulphatoxymelatonin in children and adolescents with autistic disorder. Biol Psychiatry. (2005) 57(2):134–8. doi: 10.1016/j.biopsych.2004.11.003
14. Reading R. Melatonin in autism spectrum disorders: a systematic review and meta-analysis. Child Care Health Dev. (2012) 38(2):301–2. doi: 10.1111/j.1365-2214.2011.01363_4.x
15. Schroder CM, Malow BA, Maras A, Melmed RD, Findling RL, Breddy J, et al. Pediatric prolonged-release melatonin for sleep in children with autism spectrum disorder: impact on child behavior and caregiver’s quality of life. J Autism Dev Disord. (2019) 49(8):3218–30. doi: 10.1007/s10803-019-04046-5
16. Kang-Yi CD, Grinker RR, Beidas R, Agha A, Russell R, Shah SB, et al. Influence of community-level cultural beliefs about autism on families’ and professionals’ care for children. Transcult Psychiatry. (2018) 55(5):623–47. doi: 10.1177/1363461518779831
17. de Leeuw A, Happé F, Hoekstra RA. A conceptual framework for understanding the cultural and contextual factors on autism across the globe. Autism Res. (2020) 13(7):1029–50. doi: 10.1002/aur.2276
18. Sotgiu I, Galati D, Manzano M, Gandione M, Gómez K, Romero Y, et al. Parental attitudes, attachment styles, social networks, and psychological processes in autism spectrum disorders: a cross-cultural perspective. J Genet Psychol. (2011) 172(4):353–75. doi: 10.1080/00221325.2010.544342
19. Bourne L, Bryant-Waugh R, Cook J, Mandy W. Avoidant/restrictive food intake disorder: a systematic scoping review of the current literature. Psychiatry Res. (2020) 288:112961. doi: 10.1016/j.psychres.2020.112961
20. Muratore AF, Attia E. Current therapeutic approaches to anorexia nervosa: state of the art. Clin Ther. (2021) 43(1):85–94. doi: 10.1016/j.clinthera.2020.11.006
21. Attia E, Steinglass JE, Walsh BT, Wang Y, Wu P, Schreyer C, et al. Olanzapine versus placebo in adult outpatients with anorexia nervosa: a randomized clinical trial. Am J Psychiatry. (2019) 176(6):449–56. doi: 10.1176/appi.ajp.2018.18101125
22. Blanchet C, Guillaume S, Bat-Pitault F, Carles ME, Clarke J, Dodin V, et al. Medication in AN: a multidisciplinary overview of meta-analyses and systematic reviews. J Clin Med Res. (2019) 8(2):278. doi: 10.3390/jcm8020278
23. Gallop L, Flynn M, Campbell IC, Schmidt U. Neuromodulation and eating disorders. Curr Psychiatry Rep. (2022) 24(1):61–9. doi: 10.1007/s11920-022-01321-8
24. Stern JM. Transcultural aspects of eating disorders and body image disturbance‡. Nord J Psychiatry. (2018) 72(sup1):S23–6. doi: 10.1080/08039488.2018.1525642
25. Rutter M, Stevenson J. Developments in child and adolescent psychiatry over the last 50 years. In: Rutter’s child and adolescent psychiatry. Oxford, UK: Blackwell Publishing Ltd. (2009). pp. 1–17. Available from: https://onlinelibrary.wiley.com/doi/10.1002/9781444300895.ch1
26. Eisenberg L. Mindlessness and brainlessness in psychiatry. Br J Psychiatry. (1986) 148:497–508. doi: 10.1192/bjp.148.5.497
27. Guze SB. Biological psychiatry: is there any other kind? Psychol Med. (1989) 19(2):315–23. doi: 10.1017/S0033291700012356
28. Kirmayer L. Toward an ecosocial psychiatry. World Soc Psychiatry. (2019) 1(1):30. doi: 10.4103/WSP.WSP_9_19
29. Hirschberg JC. The basic functions of a child psychiatrist in any setting. J Am Acad Child Psychiatry. (1966) 5(2):360–6. doi: 10.1016/S0002-7138(09)62063-X
30. Martin R, Moro MR, Benoit L. Is early management of psychosis designed for migrants? Improving transcultural variable collection when measuring duration of untreated psychosis. Early Interv Psychiatry. (2019) 13(3):347–57. doi: 10.1111/eip.12701
31. Deriu V, Moro MR, Benoit L. Early intervention for everyone? A review of cross-cultural issues and their treatment in ultra-high-risk (UHR) cohorts. Early Interv Psychiatry. (2018) 12(5):796–810. doi: 10.1111/eip.12671
32. Nassir Ghaemi S. The concepts of psychiatry: A pluralistic approach to the mind and mental illness. Baltimore: JHU Press (2004). 368 p. Available from: https://play.google.com/store/books/details?id=Q69zDCED9ssC
33. Kleinman A. The illness narratives: suffering, healing, and the human condition: [excerpt]. Acad Med. (2017) 92(10):1406. doi: 10.1097/ACM.0000000000001864
34. Young A. The anthropologies of illness and sickness. Annu Rev Anthropol. (1982) 11:257–85. doi: 10.1146/annurev.an.11.100182.001353
35. Rey JM, Assumpção FB, Bernad CA, Çuhadaroğlu FC, Evans B, Fung D, et al. History of child and adolescent psychiatry. In: Rey JM, editors. IACAPAP e-Textbook of Child and Adolescent Mental Health. Geneva: International Association for Child and Adolescent Psychiatry and Allied Professions (2015).
36. Lantéri-Laura G. Principales théories dans la psychiatrie contemporaine. EMC - Psychiatrie. (2004) 1(2):128–49. doi: 10.1016/j.emcps.2004.02.002
37. Ford CL, Young LJ. Translational opportunities for circuit-based social neuroscience: advancing 21st century psychiatry. Curr Opin Neurobiol. (2021) 68:1–8. doi: 10.1016/j.conb.2020.11.007
38. Chiao JY. Cultural neuroscience: a once and future discipline. Prog Brain Res. (2009) 178:287–304. doi: 10.1016/S0079-6123(09)17821-4
39. Nelson B, Lavoie S, Gawęda Ł, Li E, Sass LA, Koren D, et al. The neurophenomenology of early psychosis: an integrative empirical study. Conscious Cogn. (2020) 77:102845. doi: 10.1016/j.concog.2019.102845
40. Amir D, McAuliffe K. Cross-cultural, developmental psychology: integrating approaches and key insights. Evol Hum Behav. (2020) 41(5):430–44. doi: 10.1016/j.evolhumbehav.2020.06.006
41. Oulis P. Toward a unified methodological framework for the science and practice of integrative psychiatry. Philos Psychiatr Psychol. (2013) [cited 2021 Sep 14] 20(2):113–26. doi: 10.1353/ppp.2013.0019
43. Zajkowska Z, Walsh A, Zonca V, Gullett N, Pedersen GA, Kieling C, et al. A systematic review of the association between biological markers and environmental stress risk factors for adolescent depression. J Psychiatr Res. (2021) 138:163–75. doi: 10.1016/j.jpsychires.2021.04.003
44. Rose-Clarke K, Hassan E, Bk P, Magar J, Devakumar D, Luitel NP, et al. A cross-cultural interpersonal model of adolescent depression: a qualitative study in rural Nepal. Soc Sci Med. (2021) 270:113623. doi: 10.1016/j.socscimed.2020.113623
45. Marvaldi M, Mallet J, Dubertret C, Moro MR, Guessoum SB. Anxiety, depression, trauma-related, and sleep disorders among healthcare workers duirng the COVID-19 pandemic: a systematic review and meta-analysis. Neurosci Biobehav Rev. (2021) 126:252–64.
46. Guessoum SB, Marvaldi M, Thomas I, Lachal J, Carretier E, Moro MR, et al. The experience of anaesthesiology care providers in temporary intensive care units during the COVID-19 pandemic in France: a qualitative study. Anaesth Crit Care Pain Med. (2022) 41(3):101061. doi: 10.1016/j.accpm.2022.101061
47. Kirmayer LJ, Worthman CM, Kitayama S, Lemelson R, Cummings CA. Culture, mind, and brain: emerging concepts, models, and applications. Cambridge University Press (2020). 683 p. Available from: https://play.google.com/store/books/details?id=XxH9DwAAQBAJ
48. Kirmayer LJ, Crafa D. What kind of science for psychiatry? Front Hum Neurosci. (2014) 8:435. doi: 10.3389/fnhum.2014.00435
49. Baptista A, Cohen D, Jacquet PO, Chambon V. The cognitive, ecological, and developmental origins of self-disturbance in borderline personality disorder. Front Psychiatry. (2021) 12:707091. doi: 10.3389/fpsyt.2021.707091
50. Kato TA, Tateno M, Shinfuku N, Fujisawa D, Teo AR, Sartorius N, et al. Does the “hikikomori” syndrome of social withdrawal exist outside Japan? A preliminary international investigation.. Soc Psychiatry Psychiatr Epidemiol. (2012) 47(7):1061–75. doi: 10.1007/s00127-011-0411-7
51. Guessoum SB, Mallet J, Todo F, Benoit JP, Moro MR. First reported case of clinical lycanthropy in a 12-year-old adolescent: from culture-bound syndromes to internet-mediated delusions? Psychiatry Clin Neurosci. (2021) 75(2):70–1. doi: 10.1111/pcn.13177
52. Guessoum SB, Mallet J, Moro MR. The neurobiological hypotheses on clinical lycanthropy. Psychiatry Res. (2020) 293:113405. doi: 10.1016/j.psychres.2020.113405
53. Guessoum SB, Benoit L, Minassian S, Mallet J, Moro MR. Clinical lycanthropy, neurobiology, culture: a systematic review. Front Psychiatry. (2021) 12:718101. doi: 10.3389/fpsyt.2021.718101
54. Kaiser BN, Ticao C, Anoje C, Minto J, Boglosa J, Kohrt BA. Adapting culturally appropriate mental health screening tools for use among conflict-affected and other vulnerable adolescents in Nigeria. Glob Ment Health (Camb). (2019) 6:e10. doi: 10.1017/gmh.2019.8
55. Guessoum SB, Rezzoug D, Touhami F, Bennabi-Bensekhar M, Taieb O, Baubet T, et al. Transcultural and familial factors in bilingualism and language transmission: a qualitative study of maternal representations of French-Maghrebi Arabic bilingual children. Transcult Psychiatry. (2021) 58(6):13634615211011846. doi: 10.1177/13634615211011846
56. Kleinman AM. Depression, somatization and the “new cross-cultural psychiatry.”. Soc Sci Med. (1977) 11(1):3–10. doi: 10.1016/0037-7856(77)90138-X
57. Phan T, Steel Z, Silove D. An ethnographically derived measure of anxiety, depression and somatization: the Phan Vietnamese Psychiatric Scale. Transcult Psychiatry. (2004) 41(2):200–32. doi: 10.1177/1363461504043565
58. Kleinman A. Anthropology and psychiatry. The role of culture in cross-cultural research on illness. Br J Psychiatry. (1987) 151:447–54. doi: 10.1192/bjp.151.4.447
59. Rasmussen A, Ventevogel P, Sancilio A, Eggerman M, Panter-Brick C. Comparing the validity of the self reporting questionnaire and the Afghan symptom checklist: dysphoria, aggression, and gender in transcultural assessment of mental health. BMC Psychiatry. (2014) 14:206. doi: 10.1186/1471-244X-14-206
60. Perera H, Wijewardena K, Aluthwelage R. Screening of 18-24-month-old children for autism in a semi-urban community in Sri Lanka. J Trop Pediatr. (2009) 55(6):402–5. doi: 10.1093/tropej/fmp031
61. Vanegas SB, Magaña S, Morales M, McNamara E. Clinical validity of the ADI-R in a US-based latino population. J Autism Dev Disord. (2016) 46(5):1623–35. doi: 10.1007/s10803-015-2690-4
62. Sharan P, Hans G. Cultural issues related to ICD-11 mental, behavioural and neurodevelopmental disorders. Consortium Psychiatricum. (2021) 2(2):7–15. doi: 10.17816/CP67
63. American Psychiatric Association DS. Diagnostic and statistical manual of mental disorders: DSM-5. (2013). Available from: https://www.amberton.edu/media/Syllabi/Fall%202021/Graduate/CSL6798_E1.pdf
64. La Roche MJ, Bloom JB. Examining the effectiveness of the Cultural Formulation Interview with young children: a clinical illustration. Transcult Psychiatry. (2020) 57(4):515–24. doi: 10.1177/1363461518780605
65. Khan A, Yavorsky C, Liechti S, Opler M, Rothman B, DiClemente G, et al. A rasch model to test the cross-cultural validity in the positive and negative syndrome scale (PANSS) across six geo-cultural groups. BMC Psychol. (2013) 1(1):5. doi: 10.1186/2050-7283-1-5
66. Nackers F, Roederer T, Marquer C, Ashaba S, Maling S, Mwanga-Amumpaire J, et al. A screening tool for psychological difficulties in children aged 6 to 36 months: cross-cultural validation in Kenya, Cambodia and Uganda. BMC Pediatr. (2019) 19(1):108. doi: 10.1186/s12887-019-1461-3
67. Kohrt BA, Jordans MJD, Tol WA, Luitel NP, Maharjan SM, Upadhaya N. Validation of cross-cultural child mental health and psychosocial research instruments: adapting the Depression Self-Rating Scale and Child PTSD Symptom Scale in Nepal. BMC Psychiatry. (2011) 11(1):127. doi: 10.1186/1471-244X-11-127
68. Rezakhany C, Guessoum SB, Moro MR, Blanchet C. Severe nondiabetic plantar mal perforant in an adolescent girl with anorexia nervosa. Eat Weight Disord. (2022) 27(3):1229–33. doi: 10.1007/s40519-021-01255-9
69. Collet CB. Acute metabolic acidosis in an adolescent with anorexia nervosa: a transdisciplinary approach. J Nutrit Health Food Sci. (2016) 4(3):1–4. doi: 10.15226/jnhfs.2016.00168
70. Cohen D, Hanin C, Benarous X. Debate: developmental and integrative approaches in child and adolescent psychiatry inpatient facilities: the case of a tertiary university hospital in Paris. Child Adolesc Ment Health. (2021) 26(2):171–3. doi: 10.1111/camh.12461
71. Proctor EK, Landsverk J, Aarons G, Chambers D, Glisson C, Mittman B. Implementation research in mental health services: an emerging science with conceptual, methodological, and training challenges. Adm Policy Ment Health. (2009) 36(1):24–34. doi: 10.1007/s10488-008-0197-4
72. Hansen H, Braslow J, Rohrbaugh RM. From cultural to structural competency-training psychiatry residents to act on social determinants of health and institutional racism. JAMA Psychiatry. (2018) 75(2):117–8. doi: 10.1001/jamapsychiatry.2017.3894
73. Ogrizek A, Moro MR, Bouznah S, Lachal J. Perspective changes through transcultural mediation training: a qualitative study of trainees, instructors, and experts. Transcult Psychiatry. (2022) 59(2):154–64. doi: 10.1177/13634615211062967
74. Kirmayer LJ, Rousseau C, Guzder J, Jarvis GE. Training clinicians in cultural psychiatry: a Canadian perspective. Acad Psychiatry. (2008) 32(4):313–9. doi: 10.1176/appi.ap.32.4.313
75. Kirmayer LJ, Fung K, Rousseau C, Lo HT, Menzies P, Guzder J, et al. Guidelines for training in cultural psychiatry. Can J Psychiatry. (2021) 66(2):195–246. doi: 10.1177/0706743720907505
76. Metzl JM, Hansen H. Structural competency and psychiatry. JAMA Psychiatry. (2018) 75(2):115–6. doi: 10.1001/jamapsychiatry.2017.3891
77. Moro MR, de La Noë Q. Manuel de psychiatrie transculturelle: Travail clinique, travail social. Pensée sauvage (2004).
78. Radjack R, Touhami F, Woestelandt L, Minassian S, Mouchenik Y, Lachal J, et al. Cultural competence of professionals working with unaccompanied minors: addressing empathy by a shared narrative. Front Psychiatry. (2020) 11:528. doi: 10.3389/fpsyt.2020.00528
79. Mansolf M, Vreeker A, Reise SP, Freimer NB, Glahn DC, Gur RE, et al. Extensions of multiple-group item response theory alignment: application to psychiatric phenotypes in an international genomics consortium. Educ Psychol Meas. (2020) 80(5):870–909. doi: 10.1177/0013164419897307
80. Skokauskas N, Lavelle TA, Munir K, Sampaio F, Nystrand C, McCrone P, et al. The cost of child and adolescent mental health services. Lancet Psychiatry. (2018) 5(4):299–300. doi: 10.1016/S2215-0366(18)30089-0
81. Lachal J, Escaich M, Bouznah S, Rousselle C, De Lonlay P, Canoui P, et al. Transcultural mediation programme in a paediatric hospital in France: qualitative and quantitative study of participants’ experience and impact on hospital costs. BMJ Open. (2019) 9(11):e032498. doi: 10.1136/bmjopen-2019-032498
82. Dakić T. Mental health burden and unmet needs for treatment: a call for justice. Br J Psychiatry. (2020) 216(5):241–2. doi: 10.1192/bjp.2019.254
83. Dumit J. The infernal alternatives of corporate pharmaceutical research: abandoning psychiatry. Med Anthropol. (2018) 37(1):59–74. doi: 10.1080/01459740.2017.1360877
84. Moro MR, Radjack R. Vers une équité en santé mentale pour les enfants de migrants: propositions transculturelles. Bull de L’Acad Natl de Méd. (2022) 206(6):766–74. doi: 10.1016/j.banm.2022.01.026
86. Idiographic. [cited 2021 Sep 16]. Available from: http://methods.sagepub.com/reference/the-sage-dictionary-of-social-research-methods/n96.xml
87. Collet C. La transdisciplinarité dans le champ des troubles des conduites alimentaires: un modèle innovant pour le soin et la recherche. (2019) [cited2022 Jun 30]; Available from: http://www.theses.fr/s176778
88. Guessoum S. Approche dimensionnelle des symptômes négatifs: revue de la physiopathologie et étude clinique transnosographique dans les premiers épisodes psychiatriques. (2019). 246 p. Available from: https://play.google.com/store/books/details?id=mp8cyAEACAAJ
Keywords: child and adolescent psychiatry, transcultural psychiatry, biological psychiatry, social psychiatry, pluralistic, integrative, complementary, research design
Citation: Guessoum SB, Benoit L, Thomas I, Mallet J, Sibeoni J, Hanin C and Moro MR (2022) Articulating biological and social approaches in child and adolescent psychiatry. Front. Child Adolesc. Psychiatry 1:1065932. doi: 10.3389/frcha.2022.1065932
Received: 10 October 2022; Accepted: 5 December 2022;
Published: 21 December 2022.
Edited by:
Peter Parry, The University of Queensland, AustraliaReviewed by:
Simone Pisano, University of Naples Federico II, Italy© 2022 Guessoum, Benoit, Thomas, Mallet, Sibeoni, Hanin and Moro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sélim Benjamin Guessoum c2VsaW0uZ3Vlc3NvdW1AZ21haWwuY29t
Specialty Section: This article was submitted to Child Mental Health and Interventions, a section of the journal Frontiers in Child and Adolescent Psychiatry