
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Aging, 02 November 2022
Sec. Interventions in Aging
Volume 3 - 2022 | https://doi.org/10.3389/fragi.2022.845886
 Michel Guillaumin1*
Michel Guillaumin1* Bastien Poirson1
Bastien Poirson1 Aurélie Gerazime2Marc Puyraveau2
Aurélie Gerazime2Marc Puyraveau2 Thomas Tannou1Fréderic Mauny2
Thomas Tannou1Fréderic Mauny2 Éric Toussirot3,4
Éric Toussirot3,4Background: Osteoporosis consists in the reduction of bone mineral density and increased risk of fracture. Age is a risk factor for osteoporosis. Although many treatments are available for osteoporosis, there is limited data regarding their efficacy in older people.
Objective: To evaluate the efficacy of osteoporosis treatments in patients over 75 years old.
Methods: We reviewed all published studies in MEDLINE, Cochrane and EMBASE including patients over 75 years old, treated by osteoporosis drugs, and focused on vertebral fractures or hip fractures.
Results: We identified 4,393 records for review; 4,216 were excluded after title/abstract review. After full text review, 19 records were included in the systematic review. Most studies showed a reduction in vertebral fracture with osteoporosis treatments, but non-significant results were observed for hip fractures. Meta-analysis of 10 studies showed that lack of treatment was significantly associated with an increased risk of vertebral fractures at one (OR = 3.67; 95%CI = 2.50–5.38) and 3 years (OR = 2.19; 95%CI = 1.44–3.34), and for hip fractures at one (OR = 2.14; 95%CI = 1.09–4.22) and 3 years (OR = 1.31, 95%CI = 1.12–1.53).
Conclusion: A reduction in the risk of vertebral fractures with osteoporosis treatments was observed in most of the studies included and meta-analysis showed that lack of treatment was significantly associated with an increased risk of vertebral fractures. Concerning hip fractures, majority of included studies did not show a significant reduction in the occurrence of hip fractures with osteoporotic treatments, but meta-analysis showed an increased risk of hip fractures without osteoporotic treatment. However, most of the data derived from post hoc and preplanned analyses or observational studies.
Osteoporosis is a skeletal systemic disease characterized by a reduction in bone mass and bone mineral density (BMD), deterioration of the bone micro-architecture, and a subsequent increase in the risk of fracture of the spine, hip and other sites (Kanis et al., 2013; Cosman et al., 2014; Black and Rosen, 2016).
Worldwide, osteoporosis causes 8.9 million fractures each year, with one fracture occurring approximately every 3 s (Johnell and Kanis, 2006). By 2025, osteoporosis fractures and costs are projected to grow by >48% to >3 million fractures (Burge et al., 2007).
Fractures are associated with a high mortality rate and have a significant influence on the quality of life of patients with osteoporosis (Cooper et al., 1993; Lips and van Schoor, 2005; Sakamoto et al., 2006), sometimes leading to a need for long-term nursing care and a loss of healthy life expectancy (Tajeu et al., 2014).
Many risk factors have been established for osteoporosis, including age (Hui et al., 1988; Ross, 1996; De Laet et al., 1998; Sanders et al., 1999; Jackson and Mysiw, 2014). The incidence of osteoporotic fractures increases with advancing age: vertebral fractures are the most common, with a prevalence of approximately 20% in women aged 75 years, and 40% in women aged 80 years (Grados et al., 2004). Similarly, the cumulative incidence of hip fractures in women aged 80 years is approximately 30% (Cooper et al., 1992).
Available pharmacological therapies for the treatment of postmenopausal osteoporosis include antiresorptive drugs such as bisphosphonates and denosumab, a fully human monoclonal antibody against the receptor activator of nuclear factor-κB ligand; conversely, the parathyroid hormone analog teriparatide has a bone anabolic mechanism. The reduction of fractures with these treatments has been well demonstrated by large randomized placebo-controlled clinical trials (Black et al., 1996; Cummings et al., 1998; Black et al., 2000; Reginster et al., 2000; McClung et al., 2001; Neer et al., 2001; Black et al., 2007; Lyles et al., 2007; Cummings et al., 2009; Kendler et al., 2018). Recently, a meta-analysis performed by Nayak (Nayak and Greenspan, 2017) showed that osteoporosis treatments reduce the risk of vertebral and possibly non-vertebral fractures in men with osteoporosis.
However, despite the high risk of osteoporotic fractures in the geriatric population, most studies have included a limited number of people aged 75 or over.
The aim of this systematic review and meta-analysis was therefore to review the published literature on the efficacy of osteoporosis treatments in reducing the most common fractures in subjects aged over 75 years. We focused on the two most common and serious types of fractures in older people, namely hip (HF) and vertebral fractures (VF).
This review was conducted in accordance with the Cochrane Handbook for Systematic Reviews (V6.1) (Higgins et al., 2020) and is reported according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analysis) statement (Moher et al., 2015). The PICO method (Population, Intervention, Comparison, Outcome) was used before making the literature search to formalize the objective of the study:
1) Population: patients over 75 years old who were receiving osteoporotic treatment.
2) Intervention: taking a single osteoporosis treatment.
3) Comparison: not taking an osteoporotic treatment.
4) Outcomes: development of an osteoporotic fracture.
We performed an electronic search of Medline, the Cochrane Library and Embase on 3 March 2020, which was also updated on 11 July 2020 and again on 17 August 2020. The search strategy was developed with a research librarian. The keywords used are available in Appendix 1.
We also searched for ongoing clinical trials (in ClinicalTrials.gov) and manually checked bibliography of previously published reviews to identify potentially eligible studies.
The primary outcome was to assess the risk of fractures in subjects older than 75 years who received a single osteoporosis treatment.
We thus included all studies that evaluated the efficacy of osteoporosis treatments in subjects aged over 75 years (at the start of treatment), in terms of the risk of osteoporotic fractures. If the studies did not include only subjects over 75 years, they were only eligible for inclusion if they reported separate data for this age group.
Sub-group analysis or pooled analysis specifically reporting outcomes in our pre-specified age group were included in this systematic review.
Exclusion criteria for the studies were: meta-analysis/systematic reviews, studies including subjects over 75 years but without independent analysis of this age group, studies with patients receiving two or more osteoporosis treatments, studies without a control group (including case reports, descriptive observational studies, etc.) or with a control group under 75 years or also receiving osteoporotic treatment, and studies not written in English or French.
Two independents reviewers (MG and BP) examined each title and abstract to identify potentially eligible articles. Records deemed eligible, and records that did not contain enough information to confirm their inclusion, underwent full text review. Disagreements were resolved through discussion, and by a third reviewer (AG, MP or FM) if required.
All data were summarized in a spreadsheet recording the first author, year of publication, country, design, sample and mean age of patients, gender, molecule and dose, medical history, type of fracture, and fracture incidence at different times. Another independent reviewer (AG) verified all data extraction.
Authors and industry sponsors were contacted to obtain more information and clarification of subgroup analyses, or additional data on the relevant age group, where necessary.
We excluded studies that were not written in English or French, due to language barrier. In addition, some articles included subjects over 75 years, but the information needed for the systematic review could not be retrieved.
Risk of bias was independently assessed by two reviewers (MG and BP). Studies were judged as either as ‘low risk’, ‘unclear’ or ‘high risk’ according to the Cochrane Handbook for Systematic Reviews of Interventions (Higgins et al., 2011). We considered the methodological quality for each study on the basis of the following categories: selection bias, performance bias, detection bias, potential for attrition bias, potential for reporting bias and other potential bias.
Where suitable statistical summary data were available, we combined selected outcome data in pooled meta-analyses using the Cochrane statistical package RevMan (Cochrane Training, 2022). Odds ratios (ORs) and 95% confidence intervals (CI) were calculated to estimate the fracture rate. Significance was defined as a p < 0.05. We assessed statistical heterogeneity using the I2 test to determine whether fixed effects (I2 < 50%) or random effects (I2 ≥ 50%) modelling should be used.
When two studies included an identical population derived from the same randomized controlled trial (RCT), only one study was included in the meta-analysis.
A first sensitivity analysis was carried out in addition to the OR calculations, calculation of the RRs on all the criteria of the HF and VF subgroups, then the inclusion of the cohorts allows a second sensitivity analysis.
The literature search identified 6,812 records for review, of which 2,419 were excluded because they were duplicates, leaving 4,393 unique records for review. A total of 4,216 were excluded after review of the title/abstract. After full text review, 19 records (Ensrud, 1997; Mcclung et al., 2001; Marcus et al., 2003; Boonen et al., 2004; Boonen et al., 2006; McCloskey et al., 2006; Morin et al., 2007; Eastell et al., 2009; Boonen et al., 2010; Boonen et al., 2011; McClung et al., 2012; Nakano et al., 2014; Bawa et al., 2015; Greenspan et al., 2015; Cosman et al., 2016; Axelsson et al., 2017; Cosman et al., 2017; Bergman et al., 2018; McClung et al., 2018) selected independently by MG and BP (100% concordance) were included in the systematic review and 10 (Ensrud, 1997; Mcclung et al., 2001; Marcus et al., 2003; Boonen et al., 2004; McCloskey et al., 2006; Boonen et al., 2010; Boonen et al., 2011; McClung et al., 2012; Axelsson et al., 2017; Bergman et al., 2018) in the meta-analysis (Table 1). Figure 1 shows a flowchart of the literature search and study selection.

TABLE 1. Summary of included studies.
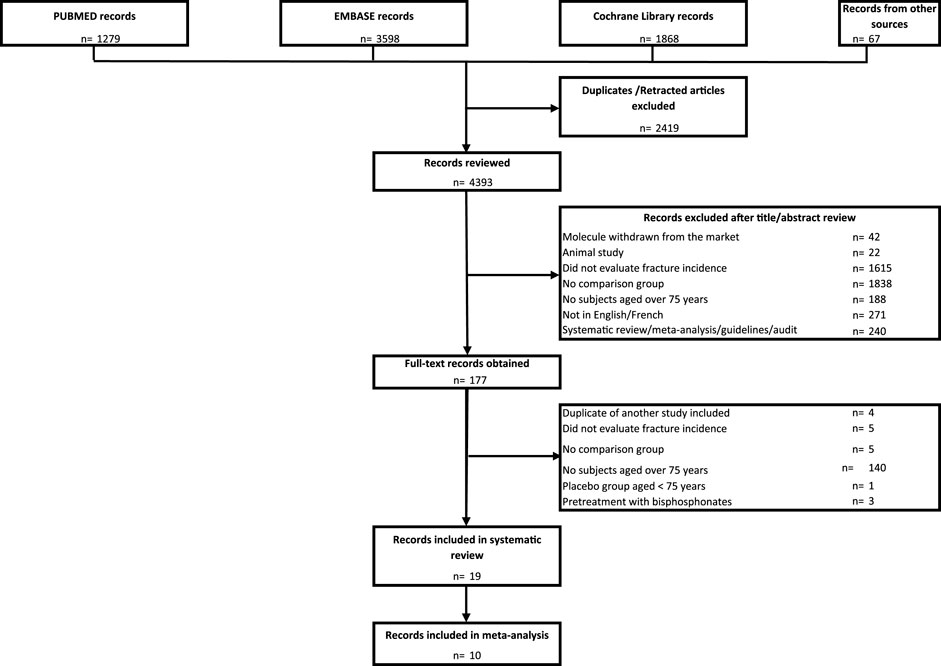
FIGURE 1. PRISMA flow chart.
Risk of bias is summarized for studies included in meta-analysis in Figure 2.
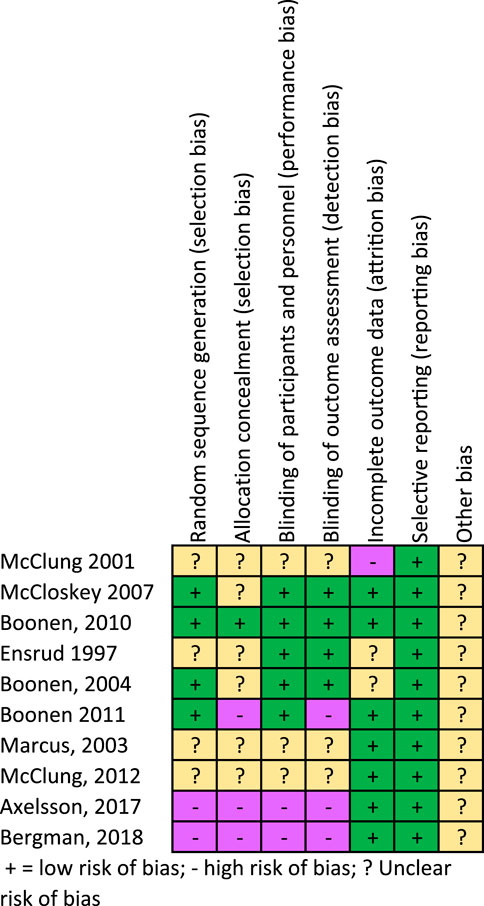
FIGURE 2. Risk of bias summary.
Table 1 summarizes the key characteristics of the selected studies in systematic review and meta-analysis.
The included studies had a number of different designs, including four randomized controlled trials (RCTs) (Mcclung et al., 2001; McCloskey et al., 2006; Greenspan et al., 2015; Cosman et al., 2016), eight post-hoc analyses (Ensrud, 1997; Marcus et al., 2003; Boonen et al., 2004; Boonen et al., 2010; Boonen et al., 2011; McClung et al., 2012; Nakano et al., 2014; McClung et al., 2018), one pre-planned and post-hoc analysis (Eastell et al., 2009), two pre-specified subgroup analyses (Boonen et al., 2006; Cosman et al., 2017), one prospective cohort study (Axelsson et al., 2017) and three retrospective cohort studies (Morin et al., 2007; Bawa et al., 2015; Bergman et al., 2018).
The molecules studied were alendronate, risedronate, zoledronic acid, clodronic acid, etidronate, denosumab, romosozumab, teriparatide, abaloparatide (Table 1). Two retrospective cohorts also studied raloxifene, hormone replacement therapy and calcitonin (Morin et al., 2007; Bawa et al., 2015) but these treatments are not approved for osteoporosis treatment in older people.
Studies were conducted in North America, Europe, Australia, China, or Japan. Included studies were published between 1997 and 2018 and study duration ranged from one to 3 years except for one study lasting 7 years (Axelsson et al., 2017). The majority of studies included only women with postmenopausal osteoporosis (Ensrud, 1997; Mcclung et al., 2001; Marcus et al., 2003; Boonen et al., 2004; Boonen et al., 2006; McCloskey et al., 2006; Eastell et al., 2009; Boonen et al., 2011; McClung et al., 2012; Greenspan et al., 2015; Cosman et al., 2016; Cosman et al., 2017; McClung et al., 2018), and did not include men or patients with secondary causes of osteoporosis. Osteoporosis fractures were detected radiographically in most studies, except for one in which fractures were detected by dual energy x-ray absorptiometry (DXA) (Greenspan et al., 2015). Fracture incidence was the primary endpoint for all studies, except the study by Greenspan, where fracture was a secondary endpoint (Greenspan et al., 2015).
Thirteen studies evaluated the incidence of VF with osteoporosis treatment (Ensrud, 1997; Marcus et al., 2003; Boonen et al., 2004; Boonen et al., 2006; Eastell et al., 2009; Boonen et al., 2010; McClung et al., 2012; Nakano et al., 2014; Bawa et al., 2015; Greenspan et al., 2015; Cosman et al., 2016; Cosman et al., 2017; McClung et al., 2018). There were only two RCTs, including one with a subgroup of subjects over 75 years, but data concerning this age-group were not given (Cosman et al., 2016), while the second involved subjects over 65 years living in nursing homes, with a mean age of 85 years. The incidence of VF was a secondary outcome in this study, and was not significantly lower in the zoledronic acid group than in the placebo group (OR = 0.76; 95%CI = 0.25–2.28; p = 0.62) (Greenspan et al., 2015). One retrospective cohort performed stratification by age and observed a significant reduction in 3-year VF incidence in the subgroup over 80 years (OR = 0.57; 95%CI = 0.42–0.78; p < 0.01) (Bawa et al., 2015). All other studies were post hoc or prespecified subgroup analyses from RCTs versus placebo and concerned subjects over 75 years (Ensrud, 1997; Marcus et al., 2003; Boonen et al., 2004; Boonen et al., 2006; Eastell et al., 2009; Boonen et al., 2010; McClung et al., 2012; Nakano et al., 2014; Cosman et al., 2017; McClung et al., 2018). Among these studies, two did not show significant results (Cosman et al., 2017; McClung et al., 2018). These two studies were derived from the same RCT and concerned abaloparatide (Miller et al., 2016). The remaining studies showed a significant decrease in the incidence of new vertebral fractures in the treatment group.
Nine studies (Mcclung et al., 2001; McCloskey et al., 2006; Morin et al., 2007; Eastell et al., 2009; Boonen et al., 2010; Boonen et al., 2011; Bawa et al., 2015; Axelsson et al., 2017; Bergman et al., 2018) evaluated the incidence of HF with osteoporosis treatment. There were two RCTs (Mcclung et al., 2001; McCloskey et al., 2006), including one study that included women older than 80 years (Mcclung et al., 2001). In that study, at 3 years, there was no significant reduction in the risk of HF (RR = 0.8; 95%CI = 0.6–1.2; p = 0.35). The second study was a single center study in elderly community-dwelling women older than 75 years (McCloskey et al., 2006). The particularity of this study is that subjects did not necessarily have osteoporosis or an underlying fracture. No significant reduction in the incidence of HF was observed after 1 year (RR = 1.31; 95%CI = 0.6–1.2) or after 3 years (RR = 0.49; 95%CI = 0.23–1.06). Among the three post hoc analyses, one study found significant results (Boonen et al., 2011), while the two others did not (Eastell et al., 2009; Boonen et al., 2010). A prospective cohort study by Axelsson showed that alendronate was associated with a reduced risk of HF (HR per year = 0.91; 95%CI = 0.85–0.97; p < 0.01) (Axelsson et al., 2017). The three retrospective cohorts selected did not report a significant reduction in HF among patients receiving treatment (Morin et al., 2007; Bawa et al., 2015; Bergman et al., 2018).
Ten studies (Ensrud, 1997; Mcclung et al., 2001; Marcus et al., 2003; Boonen et al., 2004; McCloskey et al., 2006; Boonen et al., 2010; Boonen et al., 2011; McClung et al., 2012; Axelsson et al., 2017; Bergman et al., 2018) reported sufficient data for separate meta-analysis for the following drugs: alendronate, risedronate, zoledronic acid, denosumab and clodronate for VF; and alendronate, risedronate, zoledronic acid, denosumab and teriparatide for HF.
At 1 year, analysis of data from three studies (Marcus et al., 2003; Boonen et al., 2004; Boonen et al., 2010) demonstrated that lack of treatment was associated with an increased risk of VF (OR = 3.67; 95%CI = 2.50–5.38; p < 0.00001). There was no evidence of statistical heterogeneity across studies (I2 = 7%) (Figure 3).

FIGURE 3. Meta-analysis of vertebral fractures.
At 3 years, analysis of data from four studies (Ensrud, 1997; Boonen et al., 2004; Boonen et al., 2010; McClung et al., 2012) showed that lack of treatment was also associated with an increased risk of VF (OR = 2.19; 95%CI = 1.44–3.34; p = 0.0003). There was evidence of high heterogeneity (I2 = 78%), so a random effect was performed (Figure 3).
At 1 year, analysis of six studies (Mcclung et al., 2001; McCloskey et al., 2006; Boonen et al., 2010; Boonen et al., 2011; Axelsson et al., 2017; Bergman et al., 2018) showed an increase in the incidence of HF (OR 2.14; 95%CI = 1.09–4.22; p = 0.03) in untreated subjects. A random effects meta-analysis was performed because of high heterogeneity (I2 = 92%) (Figure 4).
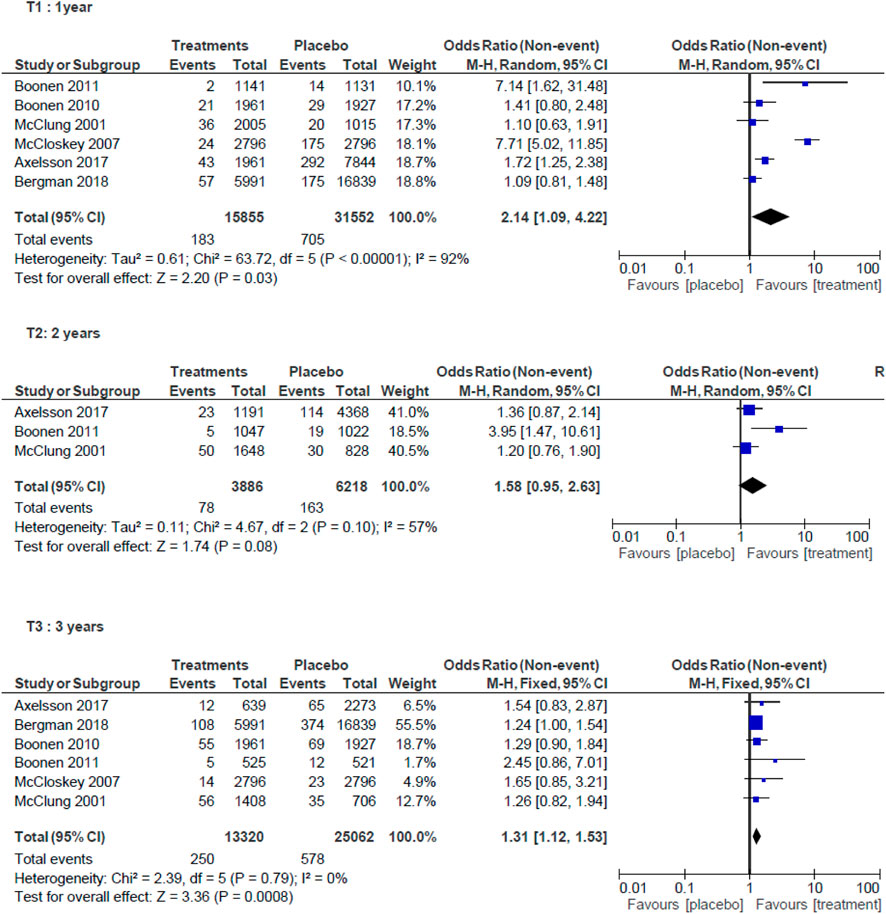
FIGURE 4. Meta-analysis of hip fractures.
At 2 years, analysis of three studies (Mcclung et al., 2001; Boonen et al., 2011; Axelsson et al., 2017) found that lack of treatment was not associated with an increased risk of HF (OR = 1.58; 95%CI = 0.95–2.63; p = 0.08). Random effects meta-analysis was performed (I2 = 57%) (Figure 4).
At 3 years, analysis of six studies (Mcclung et al., 2001; McCloskey et al., 2006; Boonen et al., 2010; Boonen et al., 2011; Axelsson et al., 2017; Bergman et al., 2018) showed an increase in the incidence of HF (OR = 1.31; 95%CI = 1.12–1.53; p = 0.0008) in untreated subjects. Fixed effect meta-analysis was performed (I2 = 0%) (Figure 4).
Results of sensitivity analysis were similar to the results of the study, across all criteria of the HF and VF subgroups.
To the best of our knowledge, this is the first systematic review and meta-analysis to examine the effectiveness of osteoporosis treatments specifically in older people. Concerning VF, most of the studies selected for systematic review showed significant results concerning fracture reduction with osteoporotic treatment (10 of 13), contrary to HF (2 of 7). This could be explained by the fact that some studies concerning HF included patients with prevalent HF, but without confirmation of established osteoporosis (McCloskey et al., 2006; Morin et al., 2007; Bawa et al., 2015; Axelsson et al., 2017; Bergman et al., 2018).
Results of the meta-analysis showed that osteoporosis treatments are associated with a reduction in the risk of VF and HF in people aged over 75 years. This is consistent with previously published reviews (Schneider, 2008; Inderjeeth et al., 2009; Vandenbroucke et al., 2017). Only the analysis of HF at 2 years found that lack of treatment was not associated with an increased risk of HF. This can be explained by the low number of studies available for analysis (3) compared to the one and 3 year analysis each comprising six studies.
In our analysis, we considered osteoporosis treatments as a whole for the treatment category in the meta-analysis because data were insufficient to envisage a separate analysis for each molecule. However, there is wide heterogeneity among the different treatments. Indeed, indication, dosage, frequency, route of administration and mechanism of action are not the same. Some drugs, such as bisphosphonates, are only antiresorptive drugs, contrary to teriparatide or abaloparatide, which are bone-forming agents, with a different mode of action. Among the bisphosphonates, some need to be taken orally every week, like alendronate, while others must be injected intravenously every year, like zoledronic acid. All these factors could influence medication adherence and consequently, efficacy, especially in older populations (Hughes, 2004).
We focused our analysis on the two most common and serious types of fractures in older people, namely VF and HF. There were not enough data to analyze other types of fracture. We chose to separate the results, because VF are often atraumatic, while HF are often due to moderate trauma, such as a fall. Indeed, in older subjects, falls are probably the strongest single risk factor in over 90% of HF (Järvinen et al., 2008). This may explain the lower efficacy of osteoporosis treatments against HF. Vitamin D supplementation was also not systematic or was insufficient in some studies, whereas it has been proven that ≥800 IU of vitamin D daily has a favorable effect in the prevention of HF in older people (Bischoff-Ferrari et al., 2012).
Medication adherence (MA) is defined as the extent to which prescribed medications are taken according to the dosage and frequency recommended by the provider (Cramer et al., 2008). It is estimated that between 30 and 50% of people do not take their medications as prescribed (Sabaté, 2003) It is therefore essential to offer multidisciplinary care to improve patient compliance and allow better effectiveness of anti-osteoporosis treatments. A list of recommendations has been issued to promote this (De Vincentis et al., 2021).
In this study, we evaluated the efficacy of osteoporosis treatments, but not safety. There were only six studies in our selection that evaluated the adverse effects specifically in older people (Boonen et al., 2004; Boonen et al., 2006; Boonen et al., 2010; Boonen et al., 2011; Greenspan et al., 2015; Axelsson et al., 2017); four of these were post hoc studies and therefore, their selection criteria did not enable the inclusion of older patients with multiple comorbidities and multiple medications.
Furthermore, patients over 75 years of age represented a small proportion of the overall sample in each study. In Europe and the United States of America, the annual risk of VF increases with age, from 0.4 to 0.6% in women aged 50–54 years to 1.2–1.3% between 65 and 69 years and to 2.9–3.8% after 85 years (O’Neill et al., 2009). Yet only one RCT included exclusively frail elderly women and did not observe a reduction in VF (Greenspan et al., 2015). Clinical trials will need to include more older people than previously, and should actively seek to include patients with extensive comorbidities in order to better assess the effectiveness of osteoporotic treatments in this age group.
This review has strengths and limitations that should be taken into account when interpreting the results. The strengths were that we used the well-established PRISMA process and the studies were rigorously identified via a double search by two independents reviewers, with the support of experienced methodologists (MP and FM) and a biostatistician (AG) to ensure the right search terms and high quality databases were used. We also improved the validity of the search by using the broadest possible search terms and considering all potential studies that covered the research topic. Despite this detailed approach, we identified only 19 publications for inclusion. Some relevant papers may have been missed due to the search strategy, the choice of databases, inconsistent search terminology, indexing problems or the filters used. In addition, we did not include gray or theoretical literature or papers that were not published in English or French.
In conclusion, a reduction in the risk of VF with osteoporosis treatments was observed in most of the studies included and meta-analysis showed that lack of treatment was significantly associated with an increased risk of VF. Concerning HF, majority of included studies did not show a significant reduction in the occurrence of HF with osteoporotic treatments, but meta-analysis showed an increased risk of HF without osteoporotic treatment. Nevertheless, data are sparse concerning this age group, and most studies included were post hoc analyses or observational studies. Additional RCTs are thus needed to confirm the efficacy of osteoporosis treatments in reducing the risk of HF or VF in persons aged 75 years and older.
The original contributions presented in the study are included in the article/Supplementary Materials, further inquiries can be directed to the corresponding author.
MG and BP examined each title and abstract to identify potentially eligible articles. Disagreements were resolved through discussion, and by AG, MP or FM if required. ET supervised the entire work.
The authors thank Prof. Bernard Cortet CHRU Lille, France for his critical review of the manuscript. Thanks to Fiona Ecarnot, (EA3920, University of Franche-Comté, Besançon, France), for her help in editing the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Axelsson, K. F., Wallander, M., Johansson, H., LunDh, D., and LorentzonM., (2017). Hip fracture risk and safety with alendronate treatment in the oldest-old. J. Intern. Med. 282, 546–559. doi:10.1111/joim.12678
Bawa, H. S., Weick, J., and Dirschl, D. R. (2015). Anti-osteoporotic therapy after fragility fracture lowers rate of subsequent fracture: Analysis of a large population sample. J. Bone Jt. Surg. Am. 97, 1555–1562. doi:10.2106/JBJS.N.01275
Bergman, J., Nordström, A., Nordström, P., and Nordstrom, A. (2018). Bisphosphonate use after clinical fracture and risk of new fracture. Osteoporos. Int. 29, 937–945. doi:10.1007/s00198-017-4367-7
Bischoff-Ferrari, H. A., Willett, W. C., Orav, E. J., Oray, E. J., Lips, P., Meunier, P. J., et al. (2012). A pooled analysis of vitamin D dose requirements for fracture prevention. N. Engl. J. Med. 367, 40–49. doi:10.1056/NEJMoa1109617
Black, D. M., Cummings, S. R., Karpf, D. B., Cauley, J. A., Thompson, D. E., Nevitt, M. C., et al. (1996). Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Fracture Intervention Trial Research Group. Lancet 348, 1535–1541. doi:10.1016/s0140-6736(96)07088-2
Black, D. M., Delmas, P. D., Eastell, R., Reid, I. R., Boonen, S., Cauley, J. A., et al. (2007). Once-yearly zoledronic acid for treatment of postmenopausal osteoporosis. N. Engl. J. Med. 14, 1809–1822. doi:10.1056/NEJMoa067312
Black, D. M., and Rosen, C. J. (2016). Clinical practice. Postmenopausal osteoporosis. N. Engl. J. Med. 374, 254–262. doi:10.1056/NEJMcp1513724
Black, D. M., Thompson, D. E., Bauer, D. C., Ensrud, K., Musliner, T., Hochberg, M. C., et al. (2000). Fracture risk reduction with alendronate in women with osteoporosis: The fracture intervention trial. FIT research group. J. Clin. Endocrinol. Metab. 85, 4118–4124. doi:10.1210/jcem.85.11.6953
Boonen, S., Adachi, J. D., Man, Z., Cummings, S. R., Lippuner, K., Torring, O., et al. (2011). Treatment with denosumab reduces the incidence of new vertebral and hip fractures in postmenopausal women at high risk. J. Clin. Endocrinol. Metab. 96, 1727–1736. doi:10.1210/jc.2010-2784
Boonen, S., Black, D. M., Colón-Emeric, C. S., Eastell, R., Magaziner, J. S., Eriksen, E. F., et al. (2010). Efficacy and safety of a once-yearly intravenous zoledronic acid 5 mg for fracture prevention in elderly postmenopausal women with osteoporosis aged 75 and older: Zol in elderly postmenopausal women with osteoporosis. J. Am. Geriatr. Soc. 58, 292–299. doi:10.1111/j.1532-5415.2009.02673.x
Boonen, S., Marin, F., Mellstrom, D., Xie, L., Desaiah, D., Krege, J. H., et al. (2006). Safety and efficacy of teriparatide in elderly women with established osteoporosis: Bone anabolic therapy from a geriatric perspective. J. Am. Geriatr. Soc. 54, 782–789. doi:10.1111/j.1532-5415.2006.00695.x
Boonen, S., McClung, M. R., Eastell, R., El-Hajj Fuleihan, G., Barton, I. P., and Delmas, P. (2004). Safety and efficacy of risedronate in reducing fracture risk in osteoporotic women aged 80 and older: Implications for the use of antiresorptive agents in the old and oldest old. J. Am. Geriatr. Soc. 52, 1832–1839. doi:10.1111/j.1532-5415.2004.52506.x
Burge, R., Dawson-Hughes, B., Solomon, D. H., Wong, J. B., King, A., and Tosteson, A. (2007). Incidence and economic burden of osteoporosis-related fractures in the United States, 2005-2025. J. Bone Min. Res. 22, 465–475. doi:10.1359/jbmr.061113
Cooper, C., Atkinson, E. J., Jacobsen, S. J., O'Fallon, W. M., and Melton, L. J. (1993). Population-based study of survival after osteoporotic fractures. Am. J. Epidemiol. 137, 1001–1005. doi:10.1093/oxfordjournals.aje.a116756
Cooper, C., Campion, G., and Melton, L. J. (1992). Hip fractures in the elderly: A world-wide projection. Osteoporos. Int. 2, 285–289. doi:10.1007/BF01623184
Cosman, F., Crittenden, D. B., Adachi, J. D., Binkley, N., Czerwinski, E., Ferrari, S., et al. (2016). Romosozumab treatment in postmenopausal women with osteoporosis. N. Engl. J. Med. 375, 1532–1543. doi:10.1056/NEJMoa1607948
Cosman, F., de Beur, S. J., LeBoff, M. S., Lewiecki, E. M., Tanner, B., Randall, S., et al. (2014). Clinician’s guide to prevention and treatment of osteoporosis. Osteoporos. Int. 25, 2359–2381. doi:10.1007/s00198-014-2794-2
Cosman, F., Hattersley, G., Hu, M., Williams, G. C., Fitzpatrick, L. A., and Black, D. M. (2017). Effects of abaloparatide-SC on fractures and bone mineral density in subgroups of postmenopausal women with osteoporosis and varying baseline risk factors: ABALOPARATIDE-SC effects on fractures in postmenopausal women. J. Bone Min. Res. 32, 17–23. doi:10.1002/jbmr.2991
Cramer, J. A., Roy, A., Burrell, A., Fairchild, C. J., Fuldeore, M. J., Ollendorf, D. A., et al. (2008). Medication compliance and persistence: Terminology and definitions. Value Health 11, 44–47. doi:10.1111/j.1524-4733.2007.00213.x
Cummings, S. R., Black, D. M., Thompson, D. E., Applegate, W. B., BarrEtt-Connor, E., Musliner, T. A., et al. (1998). Effect of alendronate on risk of fracture in women with low bone density but without vertebral FracturesResults from the fracture intervention trial. JAMA 280, 2077–2082. doi:10.1001/jama.280.24.2077
Cummings, S. R., Martin, J. S., McClung, M. R., Siris, E. S., Eastell, R., Reid, I. R., et al. (2009). Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N. Engl. J. Med. Overseas. Ed. 361, 756–765. doi:10.1056/nejmoa0809493
De Laet, C. E., Van Hout, B. A., Burger, H., Weel, A. E., HofmAn, A., and Pols, H. A. (1998). Hip fracture prediction in elderly men and women: Validation in the rotterdam study. J. Bone Min. Res. 13, 1587–1593. doi:10.1359/jbmr.1998.13.10.1587
De Vincentis, A., Behr, A. U., Bellelli, G., Bravi, M., Castaldo, A., Galluzzo, L., et al. (2021). Orthogeriatric co-management for the care of older subjects with hip fracture: Recommendations from an Italian intersociety consensus. Aging Clin. Exp. Res. 33, 2405–2443. doi:10.1007/s40520-021-01898-9
Eastell, R., Black, D. M., Boonen, S., Adami, S., Felsenberg, D., Lippuner, K., et al. (2009). Effect of once-yearly zoledronic acid five milligrams on fracture risk and change in femoral neck bone mineral density. J. Clin. Endocrinol. Metab. 94, 3215–3225. doi:10.1210/jc.2008-2765
Ensrud, K. E. (1997). Trreatment with alendronate prevents fractures in women at highest risk: Results from the fracture intervention trial. Arch. Intern. Med. 157, 2617. doi:10.1001/archinte.1997.00440430099012
Grados, F., Marcelli, C., Dargent-Molina, P., Roux, C., Vergnol, J. F., Meunier, P. J., et al. (2004). Prevalence of vertebral fractures in French women older than 75 years from the EPIDOS study. Bone 34, 362–367. doi:10.1016/j.bone.2003.11.008
Greenspan, S. L., Perera, S., Ferchak, M. A., Nace, D. A., and Resnick, N. M. (2015). Efficacy and safety of single-dose zoledronic acid for osteoporosis in frail elderly women: A randomized clinical trial. JAMA Intern. Med. 175, 913–921. doi:10.1001/jamainternmed.2015.0747
Higgins, J. P. T., Altman, D. G., Gotzsche, P. C., Juni, P., Moher, D., Oxman, A. D., et al. (2011). The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 343, d5928. doi:10.1136/bmj.d5928
Higgins, J. P. T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M. J., et al. (2020). Data From: Cochrane Handbook for systematic reviews of Interventions. version 6.1. Cochrane, Available from www.training.cochrane.org/handbook.
Hughes, C. M. (2004). Medication non-adherence in the elderly: How big is the problem? Drugs Aging 21, 793–811. doi:10.2165/00002512-200421120-00004
Hui, S. L., Slemenda, C. W., and Johnston, C. C. (1988). Age and bone mass as predictors of fracture in a prospective study. J. Clin. Invest. 81, 1804–1809. doi:10.1172/JCI113523
Inderjeeth, C. A., Foo, A. C. H., Lai, M. M. Y., and Glendenning, P. (2009). Efficacy and safety of pharmacological agents in managing osteoporosis in the old old: Review of the evidence. Bone 44, 744–751. doi:10.1016/j.bone.2008.12.003
Jackson, R. D., and Mysiw, W. J. (2014). Insights into the epidemiology of postmenopausal osteoporosis: The women’s health initiative. Semin. Reprod. Med. 32, 454–462. doi:10.1055/s-0034-1384629
Järvinen, T. L. N., Sievänen, H., Khan, K. M., Heinonen, A., and Kannus, P. (2008). Shifting the focus in fracture prevention from osteoporosis to falls. BMJ 336, 124–126. doi:10.1136/bmj.39428.470752.AD
Johnell, O., and Kanis, J. A. (2006). An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos. Int. 17, 1726–1733. doi:10.1007/s00198-006-0172-4
Kanis, J. A., McCloskey, E. V., Johansson, H., and Reginster, J. Y. (2013). European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporos. Int. 24, 23–44. doi:10.1007/s00198-018-4704-5
Kendler, D. L., Marin, F., Zerbini, C. A. F., Russo, L. A., Greenspan, S. L., Zikan, V., et al. (2018). Effects of teriparatide and risedronate on new fractures in post-menopausal women with severe osteoporosis (VERO): A multicentre, double-blind, double-dummy, randomised controlled trial. Lancet 391, 230–240. doi:10.1016/S0140-6736(17)32137-2
Lips, P., and van Schoor, N. M. (2005). Quality of life in patients with osteoporosis. Osteoporos. Int. 16, 447–455. doi:10.1007/s00198-004-1762-7
Lyles, K. W., Colón-Emeric, C. S., Magaziner, J. S., Adachi, J. D., Pieper, C. F., Mautalen, C., et al. (2007). Zoledronic acid and clinical fractures and mortality after hip fracture. N. Engl. J. Med. 357, 1799–1809. doi:10.1056/NEJMoa074941
Marcus, R., Wang, O., Satterwhite, J., and Mitlak, B. (2003). The skeletal response to teriparatide is largely independent of age, initial bone mineral density, and prevalent vertebral fractures in postmenopausal women with osteoporosis. J. Bone Min. Res. 18, 18–23. doi:10.1359/jbmr.2003.18.1.18
McCloskey, E. V., Beneton, M., Charlesworth, D., Kayan, K., deTakats, D., Dey, A., et al. (2006). Clodronate reduces the incidence of fractures in community-dwelling elderly women unselected for osteoporosis: Results of a double-blind, placebo-controlled randomized study. J. Bone Min. Res. 22, 135–141. doi:10.1359/jbmr.061008
McClung, M. R., Boonen, S., Törring, O., Roux, C., Rizzoli, R., Bone, H. G., et al. (2012). Effect of denosumab treatment on the risk of fractures in subgroups of women with postmenopausal osteoporosis. J. Bone Min. Res. 27, 211–218. doi:10.1002/jbmr.536
McClung, M. R., Geusens, P., Miller, P. D., Zippel, H., Bensen, W. G., Roux, C., et al. (2001). Effect of risedronate on the risk of hip fracture in elderly women. Hip Intervention Program Study Group. N. Engl. J. Med. 344, 333–340. doi:10.1056/NEJM200102013440503
McClung, M. R., Harvey, N. C., Fitzpatrick, L. A., Miller, P. D., Hattersley, G., Wang, Y., et al. (2018). Effects of abaloparatide on bone mineral density and risk of fracture in postmenopausal women aged 80 years or older with osteoporosis. Menopause 25, 767–771. doi:10.1097/GME.0000000000001080
Miller, P. D., Hattersley, G., Riis, B. J., Williams, G. C., Lau, E., Russo, L. A., et al. (2016). Effect of abaloparatide vs placebo on new vertebral fractures in postmenopausal women with osteoporosis: A randomized clinical trial. JAMA 316, 722–733. doi:10.1001/jama.2016.11136
Moher, D., Shamseer, L., Clarke, M., Ghersi, D., Liberati, A., Petticrew, M., et al. (2015). Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 4, 1. doi:10.1186/2046-4053-4-1
Morin, S., Rahme, E., Behlouli, H., Tenenhouse, A., Goltzman, D., and PiLote, L. (2007). Effectiveness of antiresorptive agents in the prevention of recurrent hip fractures. Osteoporos. Int. 18, 1625–1632. doi:10.1007/s00198-007-0421-1
Nakano, T., Shiraki, M., Sugimoto, T., Kishimoto, H., Ito, M., Fukunaga, M., et al. (2014). Once-weekly teriparatide reduces the risk of vertebral fracture in patients with various fracture risks: Subgroup analysis of the teriparatide once-weekly efficacy research (TOWER) trial. J. Bone Min. Metab. 32, 441–446. doi:10.1007/s00774-013-0505-2
Nayak, S., and Greenspan, S. L. (2017). Osteoporosis treatment efficacy for men: A systematic review and meta-analysis. J. Am. Geriatr. Soc. 65, 490–495. doi:10.1111/jgs.14668
Neer, R. M., Arnaud, C. D., Zanchetta, J. R., Prince, R., Gaich, G. A., Reginster, J. Y., et al. (2001). Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N. Engl. J. Med. Overseas. Ed. 8, 1434–1441. doi:10.1056/nejm200105103441904
O’Neill, T. W., Felsenberg, D., Varlow, J., Cooper, C., Kanis, J. A., and Silman, A. J. (2009). The prevalence of vertebral deformity in European men and women: The European vertebral osteoporosis study. J. Bone Min. Res. 11, 1010–1018. doi:10.1002/jbmr.5650110719
Reginster, J., Minne, H. W., Sorensen, O. H., HooperM., , Roux, C., Brandi, M. L., et al. (2000). Randomized trial of the effects of risedronate on vertebral fractures in women with established postmenopausal osteoporosis. Vertebral Efficacy with Risedronate Therapy (VERT) Study Group. Osteoporos. Int. 11, 83–91. doi:10.1007/s001980050010
Ross, P. D. (1996). Osteoporosis. Frequency, consequences, and risk factors. Arch. Intern. Med. 156, 1399–1411. doi:10.1001/archinte.156.13.1399
Sabaté, E. (2003). Adherence to long-term therapies: Evidence for action. Geneva: World Health Organization.
Sakamoto, K., Nakamura, T., Hagino, H., Endo, N., Mori, S., Muto, Y., et al. (2006). Report on the Japanese Orthopaedic Association’s 3-year project observing hip fractures at fixed-point hospitals. J. Orthop. Sci. 11, 127–134. doi:10.1007/s00776-005-0998-1
Sanders, K. M., Seeman, E., Ugoni, A. M., Pasco, J. A., Martin, T. J., Skoric, B., et al. (1999). Age- and gender-specific rate of fractures in Australia: A population-based study. Osteoporos. Int. 10, 240–247. doi:10.1007/s001980050222
Schneider, D. L. (2008). Management of osteoporosis in geriatric populations. Curr. Osteoporos. Rep. 6, 100–107. doi:10.1007/s11914-008-0018-4
Tajeu, G. S., Delzell, E., Smith, W., Arora, T., Curtis, J. R., Saag, K. G., et al. (2014). Death, debility, and destitution following hip fracture. J. Gerontol. A Biol. Sci. Med. Sci. 69, 346–353. doi:10.1093/gerona/glt105
Keywords: osteoporosis treatments, osteoporosis, fractures, older people, systematic review
Citation: Guillaumin M, Poirson B, Gerazime A, Puyraveau M, Tannou T, Mauny F and Toussirot É (2022) Fractures reduction with osteoporotic treatments in patients over 75-year-old: A systematic review and meta-analysis. Front. Aging 3:845886. doi: 10.3389/fragi.2022.845886
Received: 30 December 2021; Accepted: 13 October 2022;
Published: 02 November 2022.
Edited by:
Rita Cassia Menegati Dornelles, São Paulo State University, BrazilReviewed by:
Giovanni Iolascon, University of Campania Luigi Vanvitelli, ItalyCopyright © 2022 Guillaumin, Poirson, Gerazime, Puyraveau, Tannou, Mauny and Toussirot. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michel Guillaumin, bWljaGVsLmd1aWxsYXVtaW45MkBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.