Abstract
Introduction:
Adolescents and young adults (AYAs) diagnosed with cancer represent a distinct group with exceptional and unique characteristics. The survival rates for this age group are worse than in children or adults. Cancer care for this population is a challenge, not only for low-income countries but also for the developed world. This review addresses the unique challenges adolescents and young adults (AYAs) diagnosed with cancer in low-income countries face.
Methods:
Two individual authors conducted the literature review to present the global burden of AYAs in resource-limited settings. The articles selected focused on AYA care from Latin America, Asia, and Africa.
Results:
Among the challenges of managing AYAs with cancer are the absence of national and/or hospital cancer registries, and a lack of adequate infrastructure, AYA-dedicated programs, appropriate psycho-social support, fertility preservation, and genetic counseling services. Furthermore, education and training activities specifically dedicated to the care of AYAs diagnosed with cancer are scarce in those countries.
Conclusion:
Implementing a dedicated AYA program in resource-limited settings will be critical in providing patient-centered care bolstered by age-appropriate infrastructure and comprehensive clinical, psycho-social, and allied health support. It will significantly reduce the treatment abandonment rate, diminish the duration of diagnosis delay, and alleviate emotional detachment and disarray.
1. Introduction
Adolescents and young adults (AYA) with cancer are a distinct patient cohort presented with unique characteristics varying from distinctive epidemiology and biology to special clinical-psychosocial challenges (1). These features are present neither in children nor in adults. The age definition for this particular group is still not standard and varies from country to country. According to WHO criteria, this group, aged 15–39, constitutes over 2.9 billion individuals, with nearly 90% residing in low- and middle-income countries (LMICs) (2). During the critical phase of rapid personal and physio-psychological development, the cancer diagnosis introduces intricate psycho-social, fertility, genetic counseling, survivorship, and financial factors that significantly impact overall well-being (3). Unlike pediatric oncology, which adopts a “family-centered” approach, adult oncology tends to be more “patient-centered.” AYAs, however, have characteristics of both age groups, necessitating tailored care strategies. Despite this, an ideal model for AYA care remains uncertain (4, 5).
The global data on AYA cancer care is limited. AYAs face poorer survival rates than children and adults, with limited participation in clinical trials, especially in LMICs where trials are lacking (reported rates ranging from 5%–34% in developed countries) (3, 6). Acute lymphoblastic leukemia (ALL) is an illustrative example, showing the differences between AYA and pediatric patients regarding disease aggressiveness, high-risk characteristics, treatment-related toxicities, and unfavorable prognosis. Survival rates for AYAs with ALL, when treated according to pediatric protocols, are notably lower, around 70%, compared to 90% for children (7). These disparities are exacerbated in developing countries, where data from China and Thailand's cancer registries reveal 5-year survival rates ranging from 9% to 44%, compared to over 75% in developed countries like the USA. However, well-equipped treatment centers in developing nations demonstrate survival rates comparable to those in developed countries (e.g., a 5-year overall survival rate is 72.4% in Jordan), underlining the importance of resource availability (1, 8–10).
Hence, this report aims to give an overview of the burden of AYA cancer care in developing countries, emphasizing the challenges posed by resource limitations. As of the current date, our manuscript represents the first comprehensive review article in the literature addressing the unique challenges encountered in AYA cancer care within LMICs. The following sections of this article will present the specific challenges AYAs face in these regions and explore potential strategies and solutions to bridge the gaps in their care, ultimately striving for a more equitable and effective approach to cancer management for this vulnerable population.
2. Methods
A comprehensive search was conducted using the PubMed and Cochrane databases, targeting articles published before January 2022. Two independent authors (SH and RP) executed the search to ensure a thorough exploration of the topic. The search strategy included key terms “AYA,” “adolescents and young adults, “cancer “oncology, “LMICs,” “resource-limited,” and “developing countries.” In addition to the primary search strategy, supplementary articles were included in the research if they met the inclusion criteria and were found either in the references of the identified articles or were previously familiar to the authors due to their relevance. Further pertinent articles were included in the research if they were cited in the references of the identified articles or were already familiar to the authors. Articles were screened at the title, abstract, or full-text level. Only English-written articles were included. Given the limited availability of published data from developing countries on AYA cancer care, this narrative review adopts a broad scope. Despite our efforts, it is important to note that we also conducted a manual search, including each country classified as a LMIC according to the World Bank classification. This manual search aimed to identify any additional relevant articles in LMICs. However, we found a very limited number of articles that met our inclusion criteria. The limited number of search results indicates that our initial search did not yield a large pool of relevant information. This could be due to the specificity of our search query or the niche nature of the topic we're researching. Instead, we can focus on summarizing the key elements of our approach and the main findings or sources we discovered.
3. Being an AYA with cancer in LMICs: situation and challenges
3.1. Epidemiology
According to the Global Burden of Diseases, Injuries and Risk Factors Study Adolescent Young Adult Cancer Collaborators, approximately 1.19 million individuals aged 15–39 years were diagnosed with cancer worldwide in 2019. It is noteworthy that countries with low to middle Socio-demographic Index (SDI), representing the social and economic development of the country, reported the highest age-standardized mortality rates (14.2 per 100,000 person-years) compared to countries with higher SDI (9.2 per 100,000 person-years). This data underscores the critical need to address the unique challenges AYAs face with cancer, particularly in LMICs, where socioeconomic factors can significantly impact diagnosis and treatment (Table 1) (11).
Table 1
| Age-standardized incidence rate per 1,00,000 | Age-standardized mortality rate per 1,00,000 | |
|---|---|---|
| Global | 39.7 | 13.2 |
| High SDI quintile | 59.6 | 9.2 |
| High-middle SDI quintile | 53.2 | 13.4 |
| Middle SDI quintile | 38.3 | 13.6 |
| Low-middle SDI quintile | 29.4 | 14.2 |
| Low SDI quintile | 25.0 | 13.3 |
Mortality rates of AYAs with cancer globally and by SDI quintile in 2019 (11).
Based on the GLOBOCAN 2020 report, Asia recorded the highest estimated number of new cases among AYAs diagnosed with cancer as well as the highest number of AYA cancer-related deaths, accounting for approximately 54.9% and 59.5%, respectively (Figures 1, 2).
Figure 1
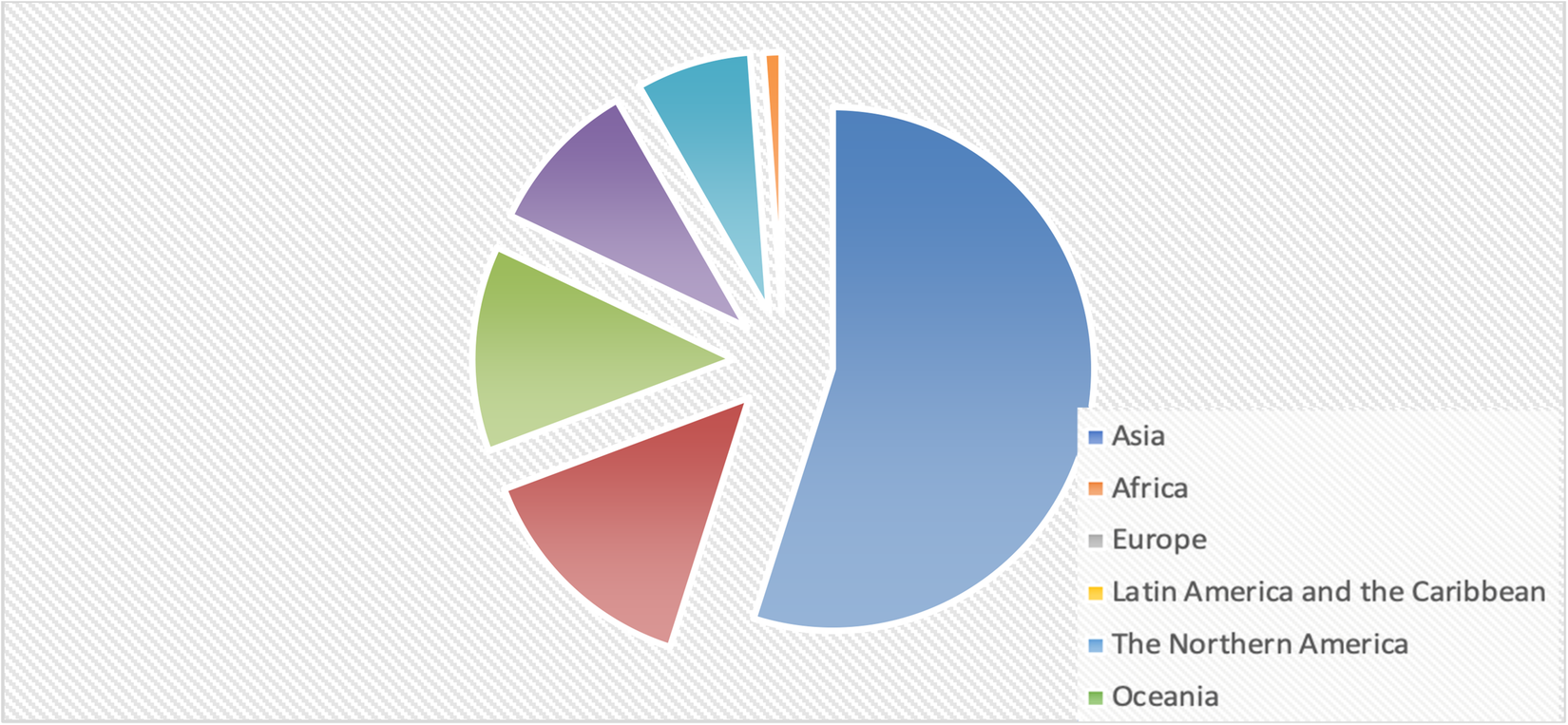
Estimated number of new cases, both sexes, ages 15–39, estimated number of deaths among individuals with cancer, both sexes, ages 15–39 (12). Legend: Asia, 688.089 (54.9%); Africa, 180.621 (14.4%); Europe, 159.300 (12.7%); Latin America and the Caribbean, 121.602 (9.7%); Northern America, 89.392 (7.1%); Oceania, 14.408 (1.1%).
Figure 2

Estimated number of deaths, both sexes, ages 15–39, estimated number of deaths among individuals with cancer, both sexes, ages 15–39 (11). Legend: Asia, 229,973 (59.5%); Africa, 86.557 (22.4%); Europe, 23.671 (6.1%); Latin America and the Caribbean, 34.557 (8.9%); Northern America, 10.103 (2.6%); Oceania, 1,659 (0.43%).
3.2. Latin America
With an estimated population of around 660 million people, Latin America and the Caribbean have witnessed significant economic and social growth over the past decades. However, despite these advancements, the region grapples with persistent issues of inequality and poverty. Encouragingly, as reported by the Pan American Health Organization (PAHO), there have been substantial improvements in the survival rates of children and adolescents with cancer, currently standing at 55% in Latin America and the Caribbean (Table 2) (12). Obtaining comprehensive cancer incidence data for adolescents and young adults (AYAs) in Latin America remains a challenge due to the absence of national registries. In response to this gap, Nomellini et al. undertook an epidemiological descriptive study with the primary objective of providing incidence rates for the most prevalent cancer types within this distinct age group across the Latin American region. By meticulously extracting and analyzing data from 24 population-based cancer registries spanning the years from 1998 to 2007, the study uncovered a total of 22,990 newly diagnosed cancer cases among AYAs in the region (13). Moreover, Curado et al. presented a comprehensive analysis of mortality rates of AYAs with leukemia in 12 countries in Latin America over the period of 1980 to 2004. Leukemia represents the predominant cancer-related cause of death among AYAs in this region. Moreover, a single-center study from Northeast Mexico reported that patients of this age group diagnosed with AML had lower 5-year OS in comparison to what is observed in the developed world (22% vs. 50%–60%) (9). Among potential explanations for this disparity were Hispanic ethnicity, low socioeconomic status, delayed diagnosis, and limited access to innovative therapeutic approaches (14). The study showed that mortality patterns in Latin America have declined over the specified period, however, they are still high when compared with the results reported from the developed world (15). In Brazil, the majority of AYAs with cancer were treated by medical oncologists (68%) and were subsequently referred to adult medical wards (2). However, a comprehensive meta-analysis conducted in 2012 showed that AYAs treated according to pediatric protocols had superior outcomes than those treated with adult protocols (16). Another report from Brazil evaluated the diagnosis and treatment delay among AYAs with bone tumors. Their findings revealed that patients aged 20–29 years had the longest delays, because of difficulties in histopathological diagnosis, lack of beds in medical oncology wards, and increasing patient autonomy. In Mexico in this age group cancer is the major cause of death, suppressed solely by traumas, with an estimated survival of 56% from the time of diagnosis vs. 80% reported from the developed world (17). One of the studies that included 63 Mexican adolescents with cancer, showed that out of 41 patients who were hospitalized and required palliative care, only 3 of them received it. Hence, there is limited access to palliative care as well (18). To date, there is a notable absence of reports addressing the care and diagnostic challenges associated with AYA programs and AYA-specific approaches in the context of Latin America. This gap in research underscores the need for further investigation into this important area of healthcare in the region.
Table 2
| Population | Age-standardized incidence rate (ASR) World per 1,00,000 | Age-standardized morality rate (ASR) World per 1,00,000 |
|---|---|---|
| Asia | 34.7 | 11.7 |
| Europe | 59.2 | 8.5 |
| Northern America | 64.7 | 12.4 |
| Latin America and the Caribbean | 43.6 | 16.7 |
| Africa | 34.9 | 7.3 |
| Oceania | 84.9 | 9.9 |
Estimated number of new cases and deaths in 2020, all cancers, both sexes, ages 15–39 (12).
3.3. Asia
Similar to the Latin American and Caribbean regions, the Asian region faces comparable challenges in the management of AYAs diagnosed with cancer. In 2016 the European Society for Medical Oncology (ESMO) and the European Society for Paediatric Oncology (SIOPE) surveyed to understand the situation of the challenges among healthcare professionals in Asia. The survey aimed to evaluate the access to specialized services in AYA patients with cancer and showed significant insufficiency in access to and quality of specialized AYA-focused cancer care across Asian countries. The absence of adequate infrastructure, AYA-dedicated services, and AYA-oriented education and training presents considerable challenges, leading to treatment non-compliance and patient abandonment, especially in rural areas. However, the majority of professionals were able to refer patients to specific psychosocial assistance (19). In Asian countries, AYA patients represent a growing percentage of the overall population, in contrast to European countries (Figure 1). In the case of Bangladesh and Jordan, the AYA age group comprises about 44% of the total population (10, 20). According to the population-based study conducted by the University of Hong Kong, the incidence of AYA patients with cancer is relatively lower in countries with low socio-demographic indexes. One of the reasonable explanations for this is the fact that in these countries potential misdiagnosis or unreported cases are higher compared to developed countries (21). The Chinese population-based study reported that the incidence of cancer in adolescents and young adults in China was found to be lower than the rates reported in the International incidence of childhood cancer. Additionally, China's childhood cancer incidence was also lower than that of other Asian countries, including South Korea, Japan, and Thailand (22). A descriptive analysis conducted in India, based on data from 28 population-based cancer registries, showed that the majority of head and neck cancers, and bone and CNS tumors diagnosed in the region had distant metastasis and/or locoregional disease. These rates were lower compared to studies conducted in other countries within the Asian region. Nonetheless, the study highlights the significance of timely diagnosis, prompt treatment initiation, treatment adherence, and regular follow-up for this age group (23). A registry-based retrospective study conducted in Jordan showed an increase in the incidence of different types of cancer among adolescents and young adults between the time interval of 2000 and 2017. The estimated annual percentage change was 2.6%. Another study from Jordan described a 72.4% 5-year overall survival rate among adolescents and young adults diagnosed with cancer (10, 24).
3.3.1. Armenia
In Armenia, where we, the co-authors of the current review practice medicine, still there is no specialized AYA department. Hence, this group of patients is treated by a variety of specialists and their special characteristics are often overlooked. Similar to other developing countries, this population has not historically been a major focus of cancer control programs and research development. All children (<18 years) with cancer and blood disorders in Armenia receive their diagnosis and chemotherapy at the Pediatric Cancer and Blood Disorders Center, which is part of the Hematology Center named after Prof. R.H. Yeolyan under the Ministry of Health. It was established in 2019 as a result of merging all existing pediatric hematology and oncology units. Hence, pediatric cancer care is centralized in Armenia. Nevertheless, all patients ≥18 years old are treated by adult oncologists in different hospitals based on distinct protocols, where they face such problems as the generation gap and rigid hospitalization rules, and in most cases, no distinction is made between them and older patients. We performed a retrospective analysis of AYA patients (aged 15–25) treated at the Hematology Center from 2019 to 2021 among a cohort of 110 patients. Although all patients received psychosocial support, at the time of the survey there was no designated program and consistent evaluation for AYA-specific needs. In total, 11 patients (10%) sought diagnosis or treatment abroad due to unavailability within Armenia. The median diagnostic delay for solid tumors was 90 days, while that for hematological malignancies was 9 days. Virtual tumor boards featuring international experts were convened for 53 cases, with 34 paraffin blocks being sent overseas, resulting in 13 final diagnoses being amended. Treatment discontinuation was reported in 10 (9%) cases, with disbelief in the efficacy of treatment being the primary factor. This rate is commensurate with findings from other developing nations. The AYA-dedicated program with the active involvement of allied health professionals, including fertility preservation experts, sexual health counselors, genetic specialists, and the psychosocial team, will be crucial in the management of AYAs in Armenia (25). Currently, the new program is already approved by the Ministry of Health and it is planned to open an AYA program at the Hematology Center.
3.4. Africa
A Global Burden of Disease study initiated in 2019 showed that the highest age-standardized incidence rate of AYAs with cancer was observed in Western Europe, whereas the lowest rates were observed in sub-Saharan Africa (age-standardized incidence rate per 100,000 population 70 vs. 25). The main reason for the low cancer incidence rate in this region is primarily due to the lack of sufficient data and the absence of cancer registries (26). The survival rate of AYAs diagnosed with breast cancer in Nigeria between the period of 2009–2016 is significantly lower compared to the developed world. Several factors can cause this, including limited disease awareness, inadequate health-seeking behavior, insufficient educational attainment among females, and a suboptimal health system. Throughout the study period, the proportion of AYAs diagnosed with breast cancer among all breast cancer cases accounts for 30.58%, which is notably higher when compared with the data from the USA (5.6%). The explanation of this might be attributed to various factors such as environmental, genetic, ethnic, and lifestyle influences, necessitating additional investigation (27). Another multi-institutional, retrospective study conducted in Africa focused on AYAs diagnosed with brain tumors between 2010 and 2019. The study showed that approximately 40% of cases experienced delays in diagnosis due to insufficient access to imaging studies. The median duration between the symptoms and presentation to the hospital was 9 months, whereas, in developed countries, it was around 1 month. Moreover, they reported that because of disbelief in disease and cultural factors, many people deny the existence of these tumors. Among the limitations of the study were missing data from some medical records, and the absence of a centralized review of the radiological and histological findings (28, 29).
4. Limitations
It is important to mention that our search results revealed a significant limitation in the available literature referring to the AYA population within the context of the selected countries. Despite our comprehensive search across various databases, we found a scarcity of articles originating from these countries. One explanation for this could be the lack of awareness and emphasis on the unique healthcare needs of AYA individuals with cancer. In many regions, AYA patients may not receive the attention they require within the broader healthcare landscape, leading to limited research initiatives and publications. Addressing this gap in the literature is crucial, as AYA individuals face a distinct set of health challenges and transitional issues that require specialized attention.
4.1. Future developments and take-home messages
The cancer care of adolescents and young adults represents a challenge globally, with particular difficulties observed in low and middle-income countries. Transitions between distinct stages of life are a continuous and changing journey for each individual, impacted by geographic, social, economic, and individual physiological variables, as well as life events. Differences in healthcare systems, lack of dedicated age-specific infrastructure, and cultural and social factors create significant disparities in the management of AYAs diagnosed with cancer worldwide. In contrast to the sufficient data reported by high-income countries, there is a scarcity of published data dedicated to this vulnerable age group from developing countries. The delayed diagnosis, unequal access to treatment in specialized cancers, misdiagnosis, high abandonment rate, and care with non-disease specific and standardized treatment protocols are the unmet needs that should be addressed. Equally alarming is the fact that there is a lack of awareness among healthcare professionals and patients regarding research initiatives focused on AYAs, especially in developing countries. Moreover, the ESMO/SIOPE/SIOP Asia survey was conducted to evaluate the accessibility of training opportunities tailored to AYA patients, with a focus on healthcare professionals as the survey's target audience and showed that only 12% of the healthcare professionals had access to such training opportunities (19). In the developing world, where the main healthcare challenges often revolve around critical issues such as malnutrition, infection disease control, and disbelief in medicine, addressing the specific healthcare needs of AYAs can indeed be a secondary priority. Raising awareness among patients and physicians is a crucial step towards improving the overall outcomes and quality of life for AYA cancer patients globally. It is essential to enhance the training and research efforts in the management and care of AYAs diagnosed with cancer, as it is a lynchpin of the development of a sustainable infrastructure, high-quality services, and adequate care that can cater to the specific needs of this special age group. In order to have the best care model it is extremely important the collaboration of pediatric and adult oncologists. The European Society for Medical Oncology (ESMO) has long been dedicated to enhancing cancer care and education for people. Together with the European Society for Paediatric Oncology (SIOPE), they launched the joint Cancer in AYA Working Group (WG) in 2015 to focus on the unique requirements of AYA with cancer. This working group is one of the platforms to address the unmet needs. A multifaceted approach is necessary to bridge the gap in AYA patient care, with the ultimate goal of establishing a new field, AYA oncology (3). In conclusion, addressing the above-mentioned challenges and issues through concerted efforts and collaboration via prioritizing the needs of AYAs diagnosed with cancer will be crucial for the continued development and enhancement of cancer care in LMICs. The lack of research emphasizes the importance of conducting further in-depth studies in this critical area of healthcare within the regions.
Statements
Author contributions
SH: Resources, Visualization, Writing – original draft. JH: Methodology, Writing – review & editing. LS: Validation, Writing – review & editing. LH: Writing – review & editing. LK: Writing – review & editing. AK: Writing – review & editing. NM: Writing – review & editing. SA: Writing – review & editing. AM: Writing – review & editing. SD: Writing – review & editing. GT: Resources, Supervision, Writing – review & editing. SB: Writing – review & editing. RP: Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1.
BarrRDFerrariARiesLWhelanJBleyerWA. Cancer in adolescents and young adults. JAMA Pediatr. (2016) 170(5):495. 10.1001/jamapediatrics.2015.4689
2.
MartinsHTGBalmantNVde Paula SilvaNSantosMdOReisRdSde CamargoB. Who cares for adolescents and young adults with cancer in Brazil?J Pediatr (Rio J). (2018) 94(4):440–5. 10.1016/j.jped.2017.07.008
3.
FerrariAStarkDPeccatoriFAFernLLaurenceVGasparNet alAdolescents and young adults (AYA) with cancer: a position paper from the AYA working group of the European society for medical oncology (ESMO) and the European society for paediatric oncology (SIOPE). ESMO Open. (2021) 6(2):100096. 10.1016/j.esmoop.2021.100096
4.
FerrariAThomasDFranklinARKHayes-LattinBMMascarinMvan der GraafWet alStarting an adolescent and young adult program: some success stories and some obstacles to overcome. J Clin Oncol. (2010) 28(32):4850–7. 10.1200/JCO.2009.23.8097
5.
SironiGBarrRDFerrariA. Models of care—there is more than one way to deliver. Cancer J. (2018) 24(6):315–20. 10.1097/PPO.0000000000000338
6.
TramaAStarkDBozovic-SpasojevicIGasparNPeccatoriFTossAet alCancer burden in adolescents and young adults in Europe. ESMO Open. (2023) 8(1):100744. 10.1016/j.esmoop.2022.100744
7.
MountziosGBielackSSMehraN. ESMO Handbook of cancer in adolescents and young adults. Lugano, Switzerland: European Society for Medical Oncology (2022).
8.
ChenJGChenHZZhuJYangYLZhangYHHuangPXet alCancer survival in patients from a hospital-based cancer registry, China. J Cancer. (2018) 9(5):851–60. 10.7150/jca.23039
9.
BerkmanAMLivingstonJAMerrimanKHildebrandtMWangJDibajSet alLong-term survival among 5-year survivors of adolescent and young adult cancer. Cancer. (2020) 126(16):3708–18. 10.1002/cncr.33003
10.
Razeq HABarbarMAbu HejlehTMansourA. Cancer care for adolescents and young adults in Jordan. East Mediterr Health J. (2018) 24(07):687–95. 10.26719/2018.24.7.687
11.
GBD 2019 Adolescent Young Adult Cancer Collaborators. The global burden of adolescent and young adult cancer in 2019: a systematic analysis for the global burden of disease study 2019. Lancet Oncol. (2022) 23(1):27–52. 10.1016/S1470-2045(21)00581-7
12.
Pan American Health Organization. 55% of children and adolescents with cancer recover in Latin America and the Caribbean. 2022. Available at:https://www.paho.org/en/news/15-2-2022-55-children-and-adolescents-cancer-recover-latin-america-and-caribbean.
13.
NomelliniPFCuradoMPOliveiraMd. Cancer incidence in adolescents and young adults in 24 selected populations of Latin America. J Adolesc Young Adult Oncol. (2018) 7(2):164–73. 10.1089/jayao.2017.0088
14.
Jaime-PérezJCPadilla-MedinaJRFernándezLTHerrera-GarzaJLGutiérrez-AguirreCHTarín-ArzagaLet alOutcomes of adolescents and young adults with acute myeloid leukemia treated in a single Latin American center. Clin Lymphoma Myeloma Leuk. (2018) 18(4):286–92. 10.1016/j.clml.2018.02.002
15.
CuradoMPPontesTGuerra-YiMECancelaMdC. Leukemia mortality trends among children, adolescents, and young adults in Latin America. Rev Panam Salud Publica. (2011) 29(2):96–102. 10.1590/s1020-49892011000200004
16.
RamRWolachOVidalLGafter-GviliAShpilbergORaananiP. Adolescents and young adults with acute lymphoblastic leukemia have a better outcome when treated with pediatric-inspired regimens: systematic review and meta-analysis. Am J Hematol. (2012) 87(5):472–8. 10.1002/ajh.23149
17.
LeungAWKLoongHHFTseTLiCK. Management of malignancies developing in AYA. Clin Pediatr Hematol Oncol. (2021) 28(1):1–13. 10.15264/cpho.2021.28.1.1
18.
Cicero-OnetoCEMata-ValderramaGValdez-MartínezE. La mortalidad en adolescentes con cáncer: características clinicoepidemiológicas de muerte y aspectos éticos emergentes. Gaceta de México. (2018) 154(1):8–15. 10.24875/GMM.17002698
19.
LiCKDalviRYonemoriKAriffinHLyuCJFaridMet alCare of adolescents and young adults with cancer in Asia: results of an ESMO/SIOPE/SIOP Asia survey. ESMO Open. (2019) 4(3):e000467. 10.1136/esmoopen-2018-000467
20.
HasanMRaheemESultanaTAHossainMS. Pattern of hematological malignancies in adolescents and young adults in Bangladesh. Cancer Epidemiol. (2017) 51:109–12. 10.1016/j.canep.2017.11.001
21.
ZhangZWangJSongNShiLDuJ. The global, regional, and national burden of stomach cancer among adolescents and young adults in 204 countries and territories, 1990–2019: a population-based study. Front Public Health. (2023) 11:1079248. 10.3389/fpubh.2023.1079248
22.
SunKZhengRZhangSZengHWangSChenRet alPatterns and trends of cancer incidence in children and adolescents in China, 2011–2015: a population-based cancer registry study. Cancer Med. (2021) 10(13):4575–86. 10.1002/cam4.4014
23.
MathurPNathA. Adolescent and young adult cancers in India-findings from the national cancer registry programme. Cancer Epidemiol. (2022) 78:102124. 10.1016/j.canep.2022.102124
24.
AmarinJZMansourRNimriOFAl-HussainiM. Incidence of cancer in adolescents and young adults in Jordan, 2000-2017. JCO Glob Oncol. (2021) 7:934–46. 10.1200/GO.21.00007
25.
PapyanRHovsepyanSSargsyanLVagharshakyanLVoskanyanABardakhchyanSet alPatterns of unmet needs of adolescents and young adults (AYA) in the developing world: beyond the walls. JCO. (2023) 41(16_suppl):e18612–e18612. 10.1200/JCO.2023.41.16_suppl.e18612
26.
WenYFChenMXYinGLinRZhongYJDongQQet alThe global, regional, and national burden of cancer among adolescents and young adults in 204 countries and territories, 1990–2019: a population-based study. J Hematol Oncol. (2021) 14(1):89. 10.1186/s13045-021-01093-3
27.
NtekimAOluwasanuMOdukoyaO. Breast cancer in adolescents and young adults less than 40 years of age in Nigeria: a retrospective analysis. Int J Breast Cancer. (2022) 2022:9943247. 10.1155/2022/9943247
28.
BalogunJABankoleOBOkereOUcheEOBalogunFMShilongDJet alEpidemiology of brain tumors among adolescents and young adults in Nigeria. J Clin Neurosci. (2022) 96:50–5. 10.1016/j.jocn.2021.12.019
29.
Zumel-MarneAKundiMCastaño-VinyalsGAlguacilJPetridouETGeorgakisMKet alClinical presentation of young people (10–24 years old) with brain tumors: results from the international MOBI-Kids study. J Neurooncol. (2020) 147(2):427–40. 10.1007/s11060-020-03437-4
Summary
Keywords
adolescents, young adults, cancer, limited resources, developing countries
Citation
Hovsepyan S, Hoveyan J, Sargsyan L, Hakobyan L, Krmoyan L, Kamalyan A, Manukyan N, Atoyan S, Muradyan A, Danelyan S, Tamamyan G, Bardakhchyan S and Papyan R (2023) The unique challenges of AYA cancer care in resource-limited settings. Front. Adolesc. Med. 1:1279778. doi: 10.3389/fradm.2023.1279778
Received
23 August 2023
Accepted
12 October 2023
Published
16 November 2023
Volume
1 - 2023
Edited by
Michael James Burke, Medical College of Wisconsin, United States
Reviewed by
Stefan Essig, University of Lucerne, Switzerland Mariana Kruger, Stellenbosch University, South Africa
Updates
Copyright
© 2023 Hovsepyan, Hoveyan, Sargsyan, Hakobyan, Krmoyan, Kamalyan, Manukyan, Atoyan, Muradyan, Danelyan, Tamamyan, Bardakhchyan and Papyan.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shushan Hovsepyan shushhovsepyan96@gmail.com Ruzanna Papyan ruzannapapyan92@gmail.com
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.