
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 07 April 2025
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1560131
This article is part of the Research TopicDevelopment and Application of New Diagnostic Methods in Clinical Diagnosis of Virus-Related DiseasesView all articles
 Yasmin Garad1Andreea A. Manea1Negin Pak1Lames Danok1Stefan Baral1,2Tom Dykstra3Danielle Kasperavicius1Sharon E. Straus1,4
Yasmin Garad1Andreea A. Manea1Negin Pak1Lames Danok1Stefan Baral1,2Tom Dykstra3Danielle Kasperavicius1Sharon E. Straus1,4 Christine Fahim1,5*
Christine Fahim1,5*Introduction: Point of care multiplex rapid antigen testing (RAT) is a tool that can be used to mitigate and respond to facility-based infectious disease outbreaks. However, little is known about how to optimally implement this testing in congregate living settings (CLSs), including long term care homes (LTCHs), retirement homes (RHs), and shelters serving people experiencing homelessness. Our objective was to explore the barriers and facilitators to implementing a new device for multiplex RAT for COVID-19 and influenza across CLSs in the Greater Toronto Area, Canada.
Materials and methods: Using key informant interviews, we assessed barriers and facilitators to implementing multiplex RAT across CLSs. Qualitative coding using the framework approach was used to identify themes. We used the Theoretical Domains Framework (TDF) and the Consolidated Framework for Implementation Research (CFIR) to identify individual and contextual-level barriers and facilitators to implementation. Identified barriers were then mapped to implementation strategies using theoretically-rooted frameworks and tools.
Results: We completed 45 interviews with staff at CLSs (8 LTCHs, 4 RHs, 12 shelters) between January 2022 and March 2023. Four barriers to RAT implementation in CLSs emerged including: limited material resources for implementation; insufficient staff capacity to perform RAT testing; complexity of RAT implementation; and reluctance among staff to adopt a new testing process. Five facilitators to implementation were described including: training and implementation support for staff at the CLSs; site-level implementation champions; access to materials to support testing; perceived advantages of simultaneous testing for COVID-19 and influenza; and the usability and functionality of the RAT testing device. Twenty implementation strategies were identified through implementation strategy mapping.
Discussion: Multiplex RAT options can empower CLS staff to promptly identify and respond to viral respiratory outbreaks. The use of evidence-based implementation strategies can enhance the effectiveness of using multiplex RAT to control outbreaks in CLSs.
Congregate living settings (CLSs) including long-term care homes (LTCHs), retirement homes (RHs) and shelters serving people experiencing homelessness represent high-risk settings for SARS-CoV-2 transmission in Canada (1–3). Crowding, frailty and pre-existing medical conditions put residents of CLSs at higher risk of COVID-19 and influenza infection and death, compared to the general population (4, 5). Despite relatively low influenza burden in 2020–2021 in Canada, concerns were raised that CLSs would experience a resurgence of influenza cases in subsequent years, alongside COVID-19 (6). Reasons for this concern included limited recent infection-derived influenza immunity due to large scale public health interventions adopted during the COVID-19 pandemic (6, 7). This concern was realized when influenza rose to epidemic levels in Canada between April 2022–June 2022 (8). CLSs have historically been prone to influenza outbreaks, which highlights the importance of multiplex rapid antigen testing (RAT) as a critical tool for managing both influenza and COVID-19 (9).
Delayed implementation of screening and infection prevention and control (IPAC) measures for SARS-CoV-2 in CLSs in Ontario posed challenges to early detection and management of outbreaks during the COVID-19 pandemic (1). Further, influenza and COVID-19 symptoms are similar, but IPAC strategies vary. For instance, there is more emphasis on social distancing/quarantining for COVID-19 (e.g., limiting visitors, mask mandates, remote services and telehealth, isolation protocols, etc.) because COVID-19 spreads more easily than influenza (10, 11) and can lead to more severe illness and complications for some individuals (12). Thus, the ability to discern infections in real time is critical to implementing timely programs and policies to mitigate outbreaks (13) and enabling targeted treatments for COVID-19 and influenza. Multiplex testing simplifies operations by identifying multiple pathogens from a single sample, supporting tailored responses (14).
A multiplex RAT platform for both COVID-19 and influenza A and B offers a practical tool for infection prevention and control in CLSs by efficiently providing multiple results from a single sample. Multiplex RAT may enable early identification of respiratory infections in residents and staff and allow for the timely application of outbreak prevention strategies (e.g., isolation of affected individuals) (13, 15). However, little is known about how to optimally implement, scale up, and sustain these tests in CLSs (16–18).
We aimed to explore the barriers and facilitators of multiplex RAT for COVID-19 and influenza using test kits from Quidel Corporation, San Diego, California, along with their Sofia® 2 Analyzer across several Ontario CLSs. In a recent systematic review that assessed 49 different types of RATs for COVID-19, the Sofia® Flu + SARS Antigen Fluorescent Immunoassay (FIA) (hereafter Sofia RAT) was one of seven tests that met the World Health Organization’s performance standards for sensitivity, and one of twelve that met these standards for specificity (19). Implementation of multiplex RAT for COVID-19 and influenza using the Sofia RAT took place between December 2021 and March 2023 as part of an initiative to improve IPAC practices across CLSs in the Greater Toronto Area, Ontario, Canada. Once barriers and facilitators were identified, they were mapped to corresponding, theoretically rooted implementation strategies that could be used to support and sustain multiplex RAT implementation in CLSs.
We conducted a qualitative study using the framework approach (20) to assess the perceived barriers and facilitators of implementing the Sofia RAT with the Sofia 2 Analyzer across CLSs in the Greater Toronto Area, Ontario, Canada (population 6,372,000). The Sofia RAT uses immunofluorescence technology to simultaneously detect nucleocapsid protein from influenza A, influenza B and SARS-CoV-2.It is paired with the Sofia 2 Analyzer, which is a small bench top analyzer that uses an ultraviolet LED energy source to automatically read each test in 15 minutes (21, 22). The Sofia 2 Analyzer also allows for the electronic storage of data on test results, which can be exported.
Retirement homes, shelters, and long-term care homes in the Greater Toronto Area that had the highest resident capacity were prioritized for study recruitment. Due to the limited number of analyzers available for implementation, the maximum number of LTCHs and RHs that could participate simultaneously was twelve. With the support of a mobile health team, implementation across a larger number of shelters was possible. Implementation took place across six RHs, twelve shelters and seven LTCHs, in the Greater Toronto Area. Testing was open to staff but was focused mainly on residents, as staff who were symptomatic or were exposed to COVID-19 typically completed self-testing at home.
Data collection and analysis for this study were guided by the 2022 Consolidated Framework for Implementation Research (CFIR) (23–25) and the Theoretical Domains Framework (TDF) (26, 27). The CFIR is a meta-framework that is used to guide the identification of factors that may influence the implementation and effectiveness of an intervention (23, 24). It includes several constructs that have been associated with effective implementation, organized across five domains. Similarly, the TDF is a framework used to assess factors that influence individual behavior change (28). The TDF can be used alongside the Capability, Opportunity, Motivation-Behavior (COM-B) model, a theory that suggests that behavior is impacted by an individual’s capabilities, opportunities and motivations to change; these factors can interact with contextual factors to determine uptake of interventions (29). We used the TDF and the CFIR to identify individual-level and contextual-level barriers and facilitators to change, respectively. We then used implementation tools to identify theoretically-linked strategies that could be used to mitigate barriers and leverage facilitators to change (30, 31).
Purposive and snowball sampling were used to recruit interview participants across the 25 CLSs participating in the multiplex RAT implementation project (32, 33). Purposive sampling ensured the inclusion of individuals directly involved in implementation, such as site leadership and frontline staff, to capture diverse perspectives on adoption, sustainability, and scale-up. Efforts were also made to recruit participants from CLSs at different stages of implementation. Snowball sampling further expanded recruitment by identifying additional staff with relevant experience who may not have been initially identified.
Individuals involved in implementation at these CLSs were identified through leadership at each site and invited to participate in this study. All individuals identified were then contacted via email for interview recruitment (n = 57). Once potential participants confirmed interest, an interview was scheduled and informed consent was obtained. Participants were compensated using $20 CAD gift cards upon study completion.
The population of Ontario, Canada is 15.8 million people (34). There are approximately 1439 RH, 157 shelters and 627 LTCHs in the province, of which 64.5, 37.4 and 33.8%, respectively, are found in the Greater Toronto Area (35–40). Multiplex RAT implementation across the 25 participating CLSs was launched on a rolling basis between December 2021 and March 2023 (representing the COVID-19 Omicron variant waves in the province) (41).
Semi-structured interview guides were rooted in the CFIR (23–25) and the TDF (26, 27) (see Appendix A). To capture barriers and facilitators throughout the implementation period, we conducted interviews at different stages of implementation. Interviews conducted at earlier stages of implementation examined existing workflows and identified barriers and facilitators to adoption, informing the co-creation of an implementation strategy with CLS staff. Interviews conducted at later stages of implementation, explored factors influencing the sustainability and scale-up of rapid testing in CLSs. Some individuals participated in both baseline and follow-up interviews to provide insights into changes over time. Interviews were conducted with staff at CLSs at various stages of implementation, ranging from 1 to 15 months post-implementation.
Interviews were conducted remotely over the phone or through a secure videoconferencing software (Zoom; audio setting only) by members of the research team [YG, OO, MB, AM]. Interviews lasted 30 to 60 min and were offered in English. Only interviewees and researchers were present at the interviews. The interviews were audiotaped and then transcribed verbatim using NVivo 12 (42). The research team [AM, MB, NP, LD] de-identified the transcripts and reviewed them for accuracy.
Demographic data were collected using an electronic survey that was circulated via email after the interviews (see Appendix B). In addition to demographic characteristics (e.g., age, gender), participants were asked about the type of CLS they worked at (LTCH, RH, or shelter), their role, and their level of involvement in the implementation of RAT using the Sofia 2 Analyzer (see Appendix B).
In keeping with the framework method (20), both inductive and deductive coding were used to categorize individual and contextual implementation barriers and facilitators (23–25, 28). Research staff (NP, LD) developed a codebook guided by the frameworks. Coding was conducted using NVivo 12 (42). Research staff double coded a 10% sample of transcripts until a kappa of 0.6 (moderate) agreement was reached, after which the remaining transcripts were independently coded (NP), and reviewed by a second reviewer (LD). The data were coded to identify emergent themes, and the codebook was iteratively revised as needed to accommodate additional themes (NP, LD). Themes were then categorized using the CFIR and the TDF domains by one coder (YG). Differences over time were assessed by comparing interview responses related to each theme at different point in implementation.
To identify corresponding implementation strategies, one coder (YG) mapped CFIR domains using the CFIR-Expert Recommendations for Implementing Change (ERIC) Barrier Buster tool and TDF domains were mapped to strategies identified using the SELECT tool (30, 31). The CFIR Barrier Buster tool generates a list of ERIC implementation strategies, prioritized by highest to lowest cumulative percentage of endorsement across all selected CFIR barriers. Implementation strategies with a cumulative percentage greater than 50% were chosen and combined with implementation strategies generated through the SELECT tool, which leverages Michie’s COM-B model to map TDF domains to COM-B intervention functions and intervention strategies corresponding to these functions.
Demographic data were analyzed using descriptive frequencies by a research coordinator (YG). We report our methods and findings in accordance with the consolidated criteria for reporting qualitative studies (COREQ, Supplementary file 1) (43). This study was approved by the St. Michael’s Hospital evaluation/quality improvement project approval process, ReQuIST (Review of Quality Improvement Studies) (ReQuIST Number: 166).
Interviews were conducted by research staff from the Knowledge Translation Program at St. Michael’s Hospital in Toronto, Ontario, Canada (YG, OO, MB, AM). Interviewers held a Bachelor’s or Master’s level degree and were experienced in qualitative methodology. All interviewers were women of diverse racial backgrounds who worked as research assistants or research coordinators. An interview guide with predefined questions and prompts was developed to reduce the risk of bias while interviewing and during analysis (see Appendix A). Additionally, the research staff engaged in self-reflection exercises to recognize and mitigate the risk of bias (44). Research staff had previously established relationships with some of the interview participants through collaboration on research projects. While these pre-existing relationships facilitated trust, they may have influenced participant responses and interactions during the interview process.
Twenty-four out of 25 intervention sites (96%) agreed to participate in this study. A total of 57 individuals were invited for interviews, of whom 39 participated (response rate = 68%). These participants collectively participated in 46 interviews conducted between January 12 2022 and March 31 2023. The remaining 18 individuals either left their organization, were unavailable due to competing priorities, or did not respond to scheduling attempts.
Participants represented a range of ages, professions, and other demographic characteristics. Ten percent of participants worked in LTCHs, 41% worked in RHs and 49% worked in shelter settings (see Table 1). The majority of interview participants were women (n = 24, 61.5%) and college/university educated (n = 34, 87.2%; see Table 1). Participants were evenly distributed between age groups: 15.4% (n = 6) were aged 18–30, 20.5% (n = 8) were aged 31–40, 28.2% (n = 11) were aged 41–50 and 17.9% (n = 7) were over the age of 50. The sample included individuals from diverse racial backgrounds, with approximately half identifying as racialized (n = 19, 48.7%). Individuals who identified as Black/LatinX represented 15% of the participant population (n = 6), and 33.3% (n = 13) of participants identified as South Asian, East Asian or Southeast Asian. Additionally, 51.3% were foreign-born Canadian citizens or Permanent Residents (n = 20). Participants held a wide range of roles, including nurses, IPAC practitioners, directors, managers, quality improvement staff, personal support workers and physicians. Most participants worked full time (n = 29, 74.4%) and had been working in their role for at least 4 years (n = 17, 43.6%). Most respondents reported that they were moderately or highly involved in RAT implementation at their site (n = 24, 61.5%).
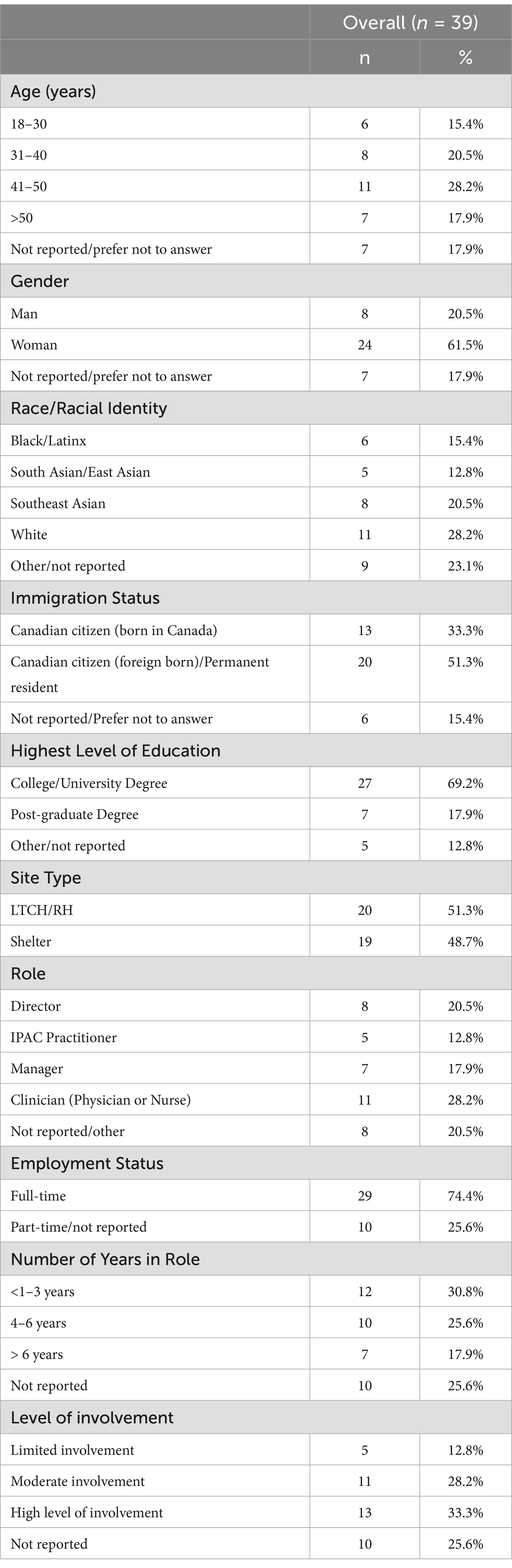
Table 1. Demographic characteristics.
We observed four main barriers and five facilitators to RAT implementation in the CLSs. Barriers and facilitators identified at baseline continued to persist for the study period (see Tables 2, 3 for summary of themes and participant quotes). Barriers to implementation included limited material resources for implementation (e.g., more devices were needed at some sites due to a high volume of residents), lack of staff capacity (e.g., staff shortage, lack of trained staff), complexity of implementation, reluctance among staff to adopt a new testing process, and preferred alternatives to the Sofia RAT (see Table 2).
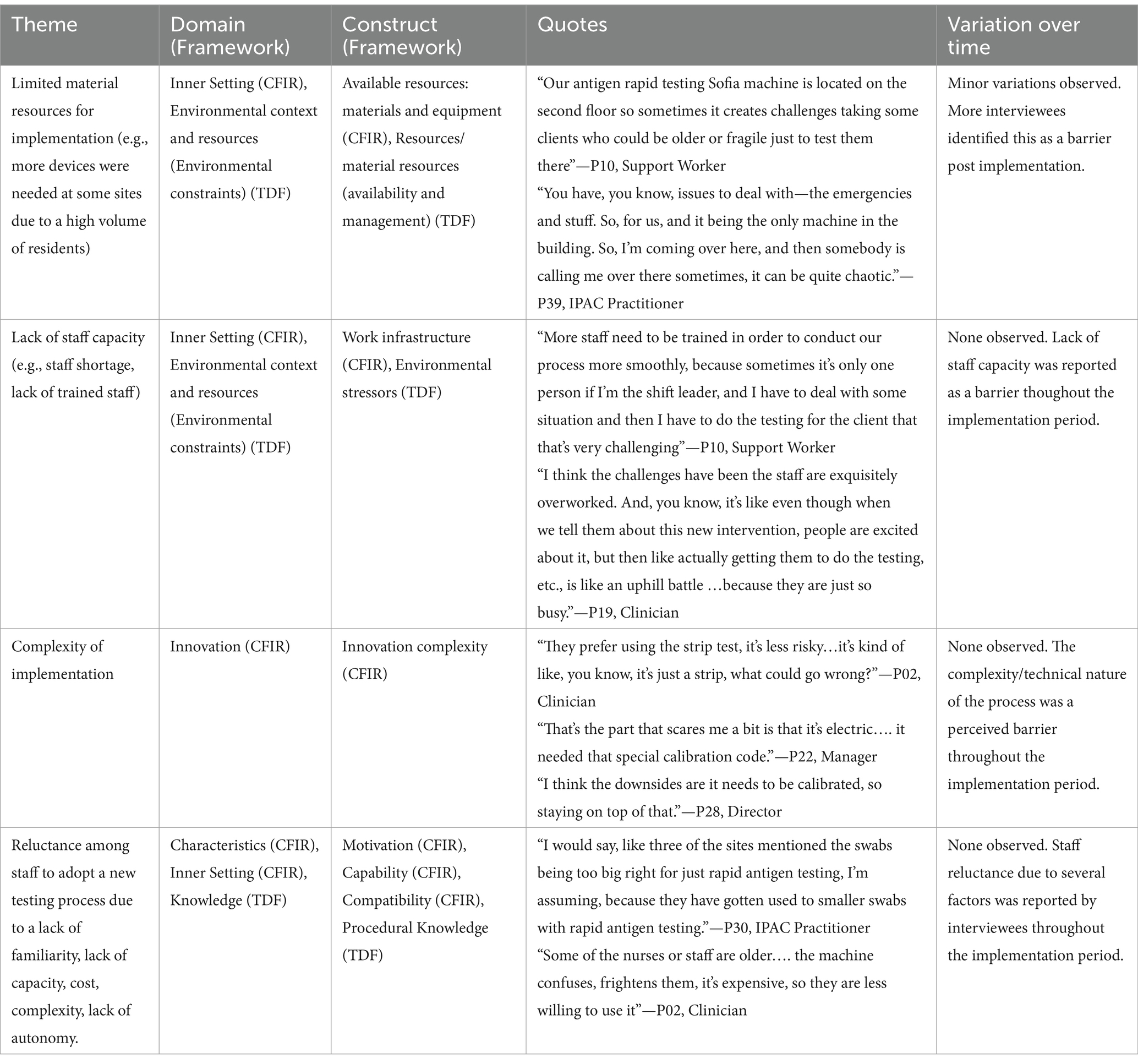
Table 2. Barriers to multiplex RAT implementation.
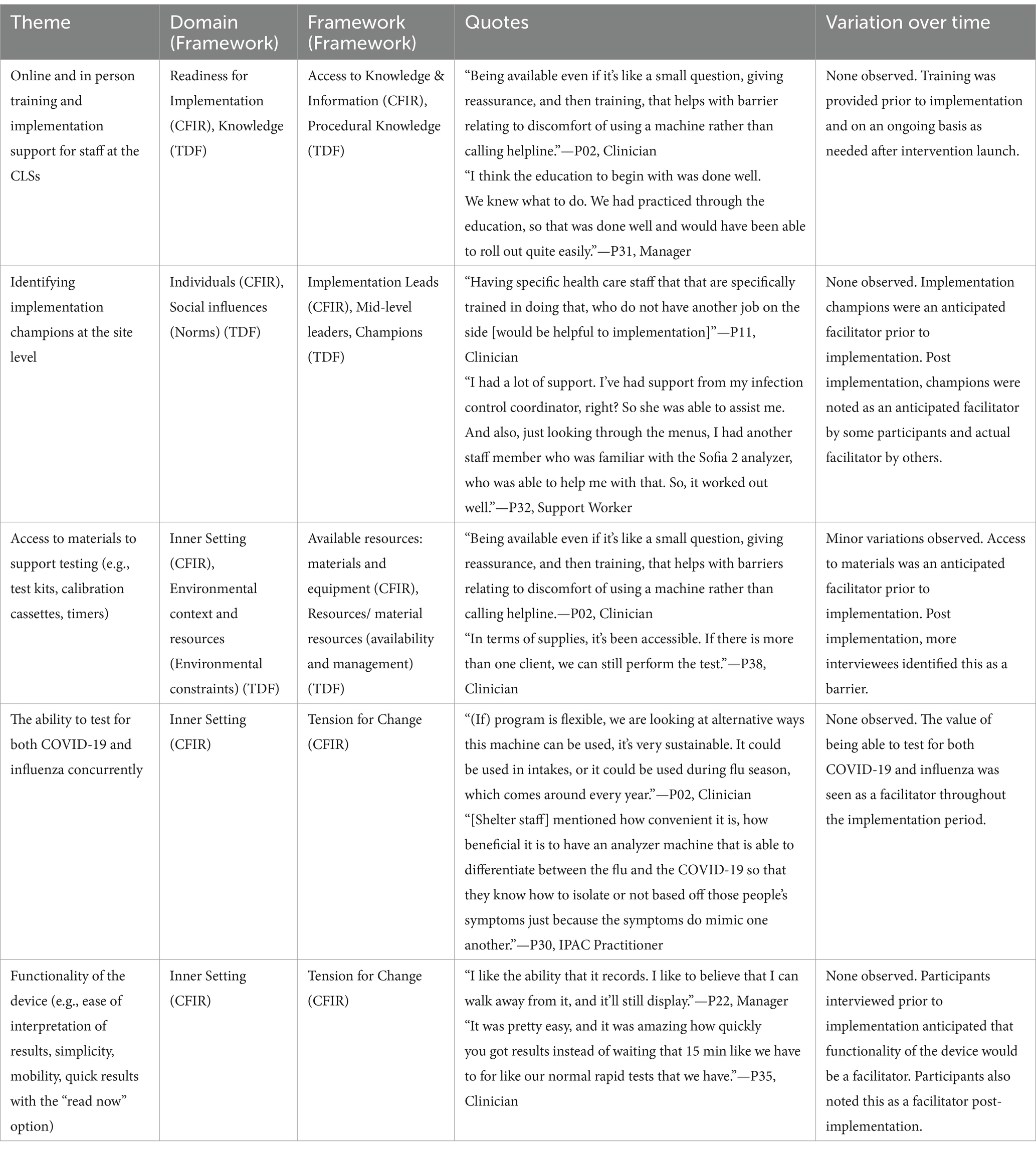
Table 3. Facilitators to multiplex rapid antigen testing implementation.
Facilitators to implementation included online and in-person training and implementation support for staff at the CLSs, implementation champions at the site level, access to materials to support testing, and the benefit of being able to test for both COVID-19 and influenza. CLS staff also found the device to be very functional (see Table 3). Several participants expressed that their site wanted to continue to use the multiplex Sofia RAT beyond the scope of the project, due to its ability to detect multiple pathogens.
Limited access to material resources was a barrier expressed by several participants. Each site that participated in implementation was provided with one Sofia 2 Analyzer. For sites that were large and/or had multiple floors, having access to only one analyzer created longer testing wait times. It also created a barrier for residents with mobility challenges. Although the analyzer was mobile, having access to only one meant that the machine was often assigned to a specific location at large CLSs. This increased the burden for site staff that attempted to test patients in one location while managing care needs in other areas of the building.
Many interview participants noted a lack of staff capacity as a barrier to the implementation of the multiplex Sofia RAT. Participants noted that staff were overworked and that some sites had high rates of staff turnover. During the implementation period, some sites decided to train only a few of their staff to use the Sophia RAT. This led to a barrier when the trained staff members were not on site or were busy with other tasks. Also, some trained staff felt that their workloads had increased as a result of the RAT testing.
Many interview participants mentioned that they found the administration of multiplex RAT using the Sofia 2 Analyzer to be technical and complex. Some were uncomfortable with the use of the technology, while others felt that the need to calibrate the machine every 30 days created a barrier that other rapid testing options (e.g., the BTNX Rapid Response® COVID-19 Antigen Rapid Test) did not pose. Additionally, the calibration process required the insertion of a small cassette that was often misplaced, which impacted staff’s ability to calibrate the machine.
Factors that influenced reluctance among staff to adopt this new testing process included the complexity of the machine as well as the swab size. Some participants noted that the swabs were thicker than what they were accustomed to from other rapid tests, which was uncomfortable for residents. Additionally, the complexity of the testing process acted as a deterrent to continuing the use of the Sofia RAT despite initial interest.
Training resources in the form of modules and demonstrations (online and in-person) were provided to site staff. The implementation team (YG, AM, OO) was also available to respond to questions or provide onsite support as needed. Many participants found these resources to be beneficial to implementation.
Some interview participants expressed that having an individual trained and tasked to perform multiplex Sofia RAT testing was beneficial. Similarly, having a well-trained individual who was able to assist others onsite to use the Sofia 2 analyzer helped to facilitate implementation.
Some sites felt that they had enough materials to implement the multiplex Sofia RAT while others had higher levels of need, including the need for more analyzers to carry out testing efficiently when testing residents on multiple floors. Shelters more commonly reported a need for more resources. Despite a preference for more materials to allow for optimal implementation (e.g., shorter wait times), shelters were able to continue with testing. Retirement homes typically did not report the need for more resources. In addition to resources for testing, the availability of space to conduct testing and access to implementation were seen as facilitators for these staff.
Many participants expressed that the ability to concurrently test for both COVID-19 and influenza facilitated implementation due to the need to differentiate between respiratory illnesses in CLSs. This guided use of most appropriate IPAC measures and mitigated the risk of COVID-19 or influenza spread. Some participants believed that the the Sofia RAT would be especially useful during annual influenza seasons.
Some staff found the analyzer to be user friendly and easy to interpret. Additionally, some individuals reported that RAT using the Sofia 2 Analyzer led to quick results (due to the “read now” mode), and its ability to keep an electronic record of all test results was also seen as beneficial.
Barriers and facilitators were mapped to CFIR and TDF constructs (see Tables 2, 3). These constructs were mapped to 34 ERIC implementation strategies using the CFIR-ERIC Barrier Buster tool and 19 implementation strategies identified across 5 intervention functions (education, training, persuasion, enablement, environmental restructuring) using the SELECT tool. Duplicate strategies identified via both the CFIR-ERIC and the SELECT tool were merged, resulting in 44 unique strategies. These implementation strategies were then further refined based priorities and recommendations for strategies, as identified through interviews. This resulted in 20 identified implementation strategies (see Table 4).
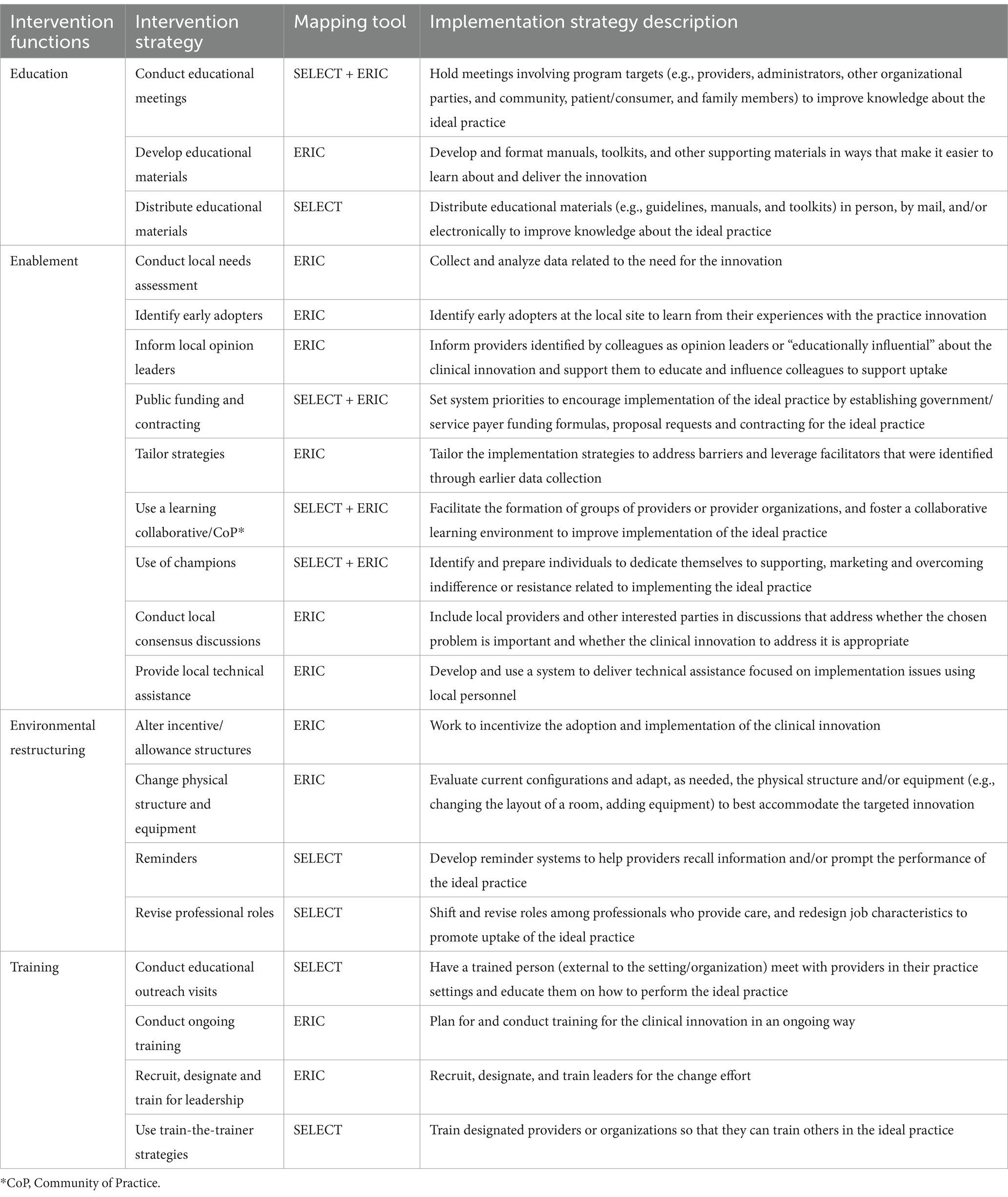
Table 4. Intervention strategies mapped to identified barriers.
We identified four barriers and five facilitators to implementation of the multiplex Sofia RAT for COVID-19 and influenza across 25 CLSs. Individual-level barriers included a lack of staff capacity and materials needed for testing, and complexity of the testing process. System-level barriers included limited material resources. Implementation facilitators included provider training, the assignment of implementation champions, the ability to test for both COVID-19 and influenza simultaneously, and functionality of the test. Participants in our study also noted the benefit of quick results, which enabled CLSs staff to administer timely treatment and implement IPAC measures promptly to mitigate the spread of disease (45).
Our identified barriers are similar to previous studies that assessed the implementation of RAT for infectious diseases in other settings (46–51). Notably, our study assessed one specific test, the Sofia 2 Analyzer, which was perceived to be user-friendly. It is important that other tests be evaluated for usability, given that ease of use is an important contributor to uptake and implementation of RAT testing (52–57). Our participants also noted the importance of dual point care testing, which has been found to save time, reduce patient burden, and lead to cost-savings (50, 58–60). Additionally, the ability to conduct testing onsite for multiple infectious diseases reduces obstacles experienced by individuals living in CLSs, such as access challenges due to a lack of mobility or limited funds (e.g., inability to travel to healthcare facilities) (53, 61, 62).
There is a paucity in the literature regarding solutions to identified barriers in the context of rapid antigen testing implementation. However, there is some evidence that suggests that workforce capacity can be improved by automating some administrative tasks (e.g., documenting results), training programs for staff, modifying procedures and task shifting (63–66). These adjustments can also reduce staff burnout which can in turn enhance staff capacity (63, 67). Research also indicates that staff training and integrating the implementation of complex tools into existing workflows can support their successful adoption in healthcare settings (68). Lastly, to mitigate the risk of limited material resources, policy interventions, including digital infrastructure to track the utilization of products, strategic stockpiling, and supply stewardship when needed, may be beneficial (69–71).
We mapped our findings using theoretically-rooted frameworks to identify 20 implementation strategies that can be considered to mitigate barriers and leverage facilitators for the routine implementation of the Sofia 2 Analyzer in CLSs. CLSs considering RAT implementation should further refine this list of strategies, based on their perceived barriers, facilitators and context, and should consider elements of feasibility, acceptability, and cost in their selection (72).
Limited staff capacity in the context of the COVID-19 pandemic made it challenging to obtain a representative sample of interviews from each site involved in this study, thus potentially introducing a sampling bias in our findings. Additionally, it is possible that barriers and facilitators evolved over time, in particular as pandemic pressures eased; resource constraints limited our ability to conduct multiple interviews over a prolonged period to assess such temporal changes. Finally, we did not interview CLS residents due to access limitations related to IPAC measures, and may have missed important considerations from this perspective.
This study was conducted in the Greater Toronto Area, where CLSs operate within a publicly funded healthcare system and serve a high-density population. These conditions may not be generalizable to regions with different population demographics, healthcare funding models, mandates, or cultural attitudes toward rapid testing. Future research should examine barriers and facilitators to the implementation of point-of-care multiplex rapid testing in rural areas, different healthcare system infrastructures, and diverse geographical and cultural contexts to assess the transferability of these findings.
The use of site leadership to identify interviewees may have also introduced sampling bias. Additionally, pre-existing professional relationships between some research staff and participants may have influenced responses due to familiarity or social desirability bias. Self-reflection exercises were conducted to mitigate this risk and trust and relationship building were central to gaining access to these CLSs to facilitate this study.
Multiplex RAT options can empower CLSs to promptly identify and respond to viral respiratory outbreaks. Implementing evidence-based strategies can further improve the effectiveness of RAT in controlling and responding to outbreaks.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The requirement of ethics approval was waived by ReQuIST (Review of Quality Improvement Studies; ReQuIST Number: 166) at Unity Health Toronto. The study was conducted in accordance with local legislation and institutional requirements. The institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin. Recorded, verbal informed consent was obtained from all participants.
YG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Writing – original draft, Writing – review & editing. AM: Data curation, Project administration, Writing – review & editing. NP: Data curation, Formal analysis, Project administration, Writing – review & editing. LD: Formal analysis, Writing – review & editing. SB: Conceptualization, Writing – review & editing. TD: Writing – review & editing. DK: Conceptualization, Writing – review & editing. SS: Conceptualization, Funding acquisition, Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing. CF: Conceptualization, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by Health Canada (Arrangement # 2122-HQ-000078). The funders provided equipment for testing, but had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The authors thank all of the study participants for their engagement in this study. The authors also thank Olu Odole-Akinyemi and Meryl Bloom for their contributions to data collection.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1560131/full#supplementary-material
1. Liu, M, Maxwell, CJ, Armstrong, P, Schwandt, M, Moser, A, McGregor, MJ, et al. COVID-19 in long-term care homes in Ontario and British Columbia. CMAJ. (2020) 192:E1540–6. doi: 10.1503/cmaj.201860
2. Estabrooks, CA, Ewa, V, Keefe, J, and Straus, SE. The predictable crisis of covid-19 in Canada's long term care homes. BMJ. (2023) 382:e075148. doi: 10.1136/bmj-2023-075148
3. Brown, KA, Jones, A, Daneman, N, Chan, AK, Schwartz, KL, Garber, GE, et al. Association between nursing home crowding and COVID-19 infection and mortality in Ontario, Canada. JAMA Intern Med. (2021) 181:229–36. doi: 10.1001/jamainternmed.2020.6466
4. Leece, P, Whelan, M, Costa, AP, Daneman, N, Johnstone, J, McGeer, A, et al. Nursing home crowding and its association with outbreak-associated respiratory infection in Ontario, Canada before the COVID-19 pandemic (2014-19): a retrospective cohort study. Lancet Healthy Longev. (2023) 4:e107–14. doi: 10.1016/S2666-7568(23)00018-1
5. Boyer, J, Konig, E, and Friedl, H. Sustained increase in very low influenza vaccination coverage in residents and healthcare Workers of Long-Term Care Facilities in Austria after educational interventions. Vaccines (Basel). (2023) 11:1066. doi: 10.3390/vaccines11061066
6. Ali, ST, Lau, YC, Shan, S, Ryu, S, du, Z, Wang, L, et al. Prediction of upcoming global infection burden of influenza seasons after relaxation of public health and social measures during the COVID-19 pandemic: a modelling study. Lancet Glob Health. (2022) 10:e1612–22. doi: 10.1016/S2214-109X(22)00358-8
7. Groves, HE, Papenburg, J, Mehta, K, Bettinger, JA, Sadarangani, M, Halperin, SA, et al. The effect of the COVID-19 pandemic on influenza-related hospitalization, intensive care admission and mortality in children in Canada: a population-based study. Lancet Reg Health Am. (2022) 7:100132. doi: 10.1016/j.lana.2021.100132
8. Nwosu, A, Lee, L, Schmidt, K, Buckrell, S, Sevenhuysen, C, and Bancej, C. National influenza annual report, Canada, 2020-2021, in the global context. Can Commun Dis Rep. (2021) 47:405–13. doi: 10.14745/ccdr.v47i10a02
9. Finnie, TJ, Hall, IM, and Leach, S. Behaviour and control of influenza in institutions and small societies. J R Soc Med. (2012) 105:66–73. doi: 10.1258/jrsm.2012.110249
10. Nasrullah, A, Gangu, K, Garg, I, Javed, A, Shuja, H, Chourasia, P, et al. Trends in hospitalization and mortality for influenza and other respiratory viruses during the COVID-19 pandemic in the United States. Vaccines (Basel). (2023) 11:412. doi: 10.3390/vaccines11020412
11. Chotpitayasunondh, T, Fischer, TK, Heraud, JM, Hurt, AC, Monto, AS, Osterhaus, A, et al. Influenza and COVID-19: what does co-existence mean? Influenza Other Respir Viruses. (2021) 15:407–12. doi: 10.1111/irv.12824
12. Chen, Z, Peng, Y, Wu, X, Pang, B, Yang, F, Zheng, W, et al. Comorbidities and complications of COVID-19 associated with disease severity, progression, and mortality in China with centralized isolation and hospitalization: a systematic review and meta-analysis. Front Public Health. (2022) 10:923485. doi: 10.3389/fpubh.2022.923485
13. Buckle, P, Micocci, M, Tulloch, J, Kierkegaard, P, Parvulescu, P, Thompson, C, et al. COVID-19 point-of-care testing in care homes: what are the lessons for policy and practice? Age Ageing. (2021) 50:1442–4. doi: 10.1093/ageing/afab101
14. Stockl, KM, Tucker, J, Beaubrun, A, Certa, JM, Becker, L, and Chase, JG. Real-world use of multiplex point-of-care molecular testing or laboratory-based molecular testing for influenza-like illness in a 2021 to 2022 US outpatient sample. PLoS One. (2024) 19:e0313660. doi: 10.1371/journal.pone.0313660
15. Crozier, A, Rajan, S, Buchan, I, and McKee, M. Put to the test: use of rapid testing technologies for covid-19. BMJ. (2021) 372:n208. doi: 10.1136/bmj.n208
16. Mitton, C SN, Lakzadeh, P, and Kim, D. Rapid diagnostic testing for COVID-19 in a fully vaccinated population. Report prepared for the SPOR Evidence Alliance and COVID-END (2021). Available at: https://sporevidencealliance.ca/wp-content/uploads/2021/06/Rapid-Diagnostic-Testing-COVID-19-in-fully-vaccinated_Final-Report_2021.06.18.pdf (Accessed February 9, 2024.)
17. Sim, M, At-home COVID-19 testing: A rapid scoping review. (2021). Available at: https://sporevidencealliance.ca/wp-content/uploads/2021/05/At-home-COVID-19-testing_Full-Report_2021.02.12.pdf (Accessed August 11, 2021).
18. Sim, M, Barriers to COVID-19 testing and testing hesitancy: A rapid scoping review. (2021). Available at: https://sporevidencealliance.ca/wp-content/uploads/2021/05/Barriers-to-COVID-19-testing-and-Testing-Hesitancy_Full-Report_2021.02.03.pdf.
19. Dinnes, J, Sharma, P, and Berhane, S. Rapid, point-of-care antigen tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Syst Rev. (2022) 2022:CD013705. doi: 10.1002/14651858.CD013705.pub3
20. Gale, NK, Heath, G, Cameron, E, Rashid, S, and Redwood, S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. (2013) 13:117. doi: 10.1186/1471-2288-13-117
21. Bornemann, L, Kaup, O, Kleideiter, J, Panning, M, Ruprecht, B, and Wehmeier, M. Real-life evaluation of the Sofia SARS-CoV-2 antigen assay in a large tertiary care hospital. J Clin Virol. (2021) 140:104854. doi: 10.1016/j.jcv.2021.104854
22. QuidelOrtho Corporation. Sofia® 2 fluorescent immunoassay analyzer. QuidelOrtho Corporation. (2023).
23. Damschroder, LJ, Aron, DC, Keith, RE, Kirsh, SR, Alexander, JA, and Lowery, JC. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. (2009) 4:50. doi: 10.1186/1748-5908-4-50
24. Damschroder, LJ, Reardon, CM, Widerquist, MAO, and Lowery, J. The updated consolidated framework for implementation research based on user feedback. Implement Sci. (2022) 17:75. doi: 10.1186/s13012-022-01245-0
25. Rodrigues, IB, Fahim, C, Garad, Y, Presseau, J, Hoens, AM, Braimoh, J, et al. Developing the intersectionality supplemented consolidated framework for implementation research (CFIR) and tools for intersectionality considerations. BMC Med Res Methodol. (2023) 23:262. doi: 10.1186/s12874-023-02083-4
26. Cane, J, O'Connor, D, and Michie, S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement Sci. (2012) 7:37. doi: 10.1186/1748-5908-7-37
27. Birken, SA, Powell, BJ, Presseau, J, Kirk, MA, Lorencatto, F, Gould, NJ, et al. Combined use of the consolidated framework for implementation research (CFIR) and the theoretical domains framework (TDF): a systematic review. Implement Sci. (2017) 12:2. doi: 10.1186/s13012-016-0534-z
28. Michie, S, Johnston, M, Abraham, C, Lawton, R, Parker, D, Walker, A, et al. Making psychological theory useful for implementing evidence based practice: a consensus approach. Qual Saf Health Care. (2005) 14:26–33. doi: 10.1136/qshc.2004.011155
29. Michie, S, van Stralen, MM, and West, R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. (2011) 6:42. doi: 10.1186/1748-5908-6-42
30. Powell, BJ, Waltz, TJ, Chinman, MJ, Damschroder, LJ, Smith, JL, Matthieu, MM, et al. A refined compilation of implementation strategies: results from the expert recommendations for implementing change (ERIC) project. Implement Sci. (2015) 10:21. doi: 10.1186/s13012-015-0209-1
31. Knowledge Translation Program. The Select tool. (2019). Available at: https://knowledgetranslation.net/wp-content/uploads/2023/03/SelectToolHardCopyKTP.pdf. (Accessed February 9, 2024).
32. Palinkas, LA, Horwitz, SM, Green, CA, Wisdom, JP, Duan, N, and Hoagwood, K. Purposeful sampling for qualitative data collection and analysis in mixed method implementation research. Admin Pol Ment Health. (2015) 42:533–44. doi: 10.1007/s10488-013-0528-y
33. Johnson, TP. Snowball sampling: Introduction In: The Encyclopedia of Biostatistics. US: John Wiley & Sons, Ltd (2014)
35. Canadian Institute for Health Research. Long-term care homes in Canada: How many and who owns them? (2021). Available at: https://www.cihi.ca/en/long-term-care-homes-in-canada-how-many-and-who-owns-them#:~:text=Ontario%20has%20a%20total%20of,not%2Dfor%2Dprofit%20organizations (Accessed February 9, 2024).
36. Manis, DR, Poss, JW, Jones, A, Rochon, PA, Bronskill, SE, Campitelli, MA, et al. Rates of health services use among residents of retirement homes in Ontario: a population-based cohort study. CMAJ. (2022) 194:E730–8. doi: 10.1503/cmaj.211883
37. Government of Canada. Shelter capacity report 2021. (2021). Available at: https://secure.infc.gc.ca/homelessness-sans-abri/reports-rapports/shelter-cap-hebergement-2021-eng.html (Accessed February 9, 2024).
38. Retirement Homes Regulatory Authority. (2025). Retirement Home Database. Available at: https://www.rhra.ca/en/retirement-home-database/ (Accessed March 20, 2025).
39. Curtis, E, Jones, R, Tipene-Leach, D, Walker, C, Loring, B, Paine, SJ, et al. Why cultural safety rather than cultural competency is required to achieve health equity: a literature review and recommended definition. Int J Equity Health. (2019) 18:174. doi: 10.1186/s12939-019-1082-3
40. City of Toronto. (2025) About City-operated services. Available at: https://www.toronto.ca/community-people/community-partners/emergency-shelter-operators/about-torontos-shelter-system/see-our-shelters/#:~:text=Through%20Shelter%2C%20Support%20and%20Housing,programs%20mostly%20used%20by%20families (Accessed February 9, 2024).
41. Murphy, TJ, Swail, H, Jain, J, Anderson, M, Awadalla, P, Behl, L, et al. The evolution of SARS-CoV-2 seroprevalence in Canada: a time-series study, 2020-2023. CMAJ. (2023) 195:E1030–7. doi: 10.1503/cmaj.230249
43. Tong, A, Sainsbury, P, and Craig, J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. (2007) 19:349–57. doi: 10.1093/intqhc/mzm042
44. Knowledge Translation Program. Intersectionality & Knowledge Translation (KT) reflection workbook. (2019). Available at: https://knowledgetranslation.net/wp-content/uploads/2020/08/Intersectionality_KT_Reflection_Workbook_20200317_FD.pdf (Accessed February 9, 2024).
45. Teoh, TK, Powell, J, Kelly, J, McDonnell, C, Whelan, R, O'Connell, NH, et al. Outcomes of point-of-care testing for influenza in the emergency department of a tertiary referral hospital in Ireland. J Hosp Infect. (2021) 110:45–51. doi: 10.1016/j.jhin.2021.01.004
46. Bagchi, AD, and Davis, T. Clinician barriers and facilitators to routine HIV testing: a systematic review of the literature. J Int Assoc Provid AIDS Care. (2020) 19:2325958220936014. doi: 10.1177/2325958220936014
47. Hardy, V, Thompson, M, Alto, W, Keppel, GA, Hornecker, J, Linares, A, et al. Exploring the barriers and facilitators to use of point of care tests in family medicine clinics in the United States. BMC Fam Pract. (2016) 17:149. doi: 10.1186/s12875-016-0549-1
48. Martin, K, Wenlock, R, Roper, T, Butler, C, and Vera, JH. Facilitators and barriers to point-of-care testing for sexually transmitted infections in low- and middle-income countries: a scoping review. BMC Infect Dis. (2022) 22:561. doi: 10.1186/s12879-022-07534-9
49. Shehata, N, Austin, T, Ha, S, and Timmerman, K. Barriers to and facilitators of hepatitis C virus screening and testing: a scoping review. Can Commun Dis Rep. (2018) 44:166–72. doi: 10.14745/ccdr.v44i78a03
50. Garcia, PJ, Carcamo, CP, and Chiappe, M. Rapid syphilis tests as catalysts for health systems strengthening: a case study from Peru. PLoS One. (2013) 8:e66905. doi: 10.1371/journal.pone.0066905
51. Santos, WJ, Graham, ID, Lalonde, M, Demery Varin, M, and Squires, JE. The effectiveness of champions in implementing innovations in health care: a systematic review. Implement Sci Commun. (2022) 3:80. doi: 10.1186/s43058-022-00315-0
52. Ansbro, EM, Gill, MM, Reynolds, J, Shelley, KD, Strasser, S, Sripipatana, T, et al. Introduction of syphilis point-of-care tests, from pilot study to National Programme Implementation in Zambia: a qualitative study of healthcare Workers' perspectives on testing, training and quality assurance. PLoS One. (2015) 10:e0127728. doi: 10.1371/journal.pone.0127728
53. Young, N, Achieng, F, Desai, M, Phillips-Howard, P, Hill, J, Aol, G, et al. Integrated point-of-care testing (POCT) for HIV, syphilis, malaria and anaemia at antenatal facilities in western Kenya: a qualitative study exploring end-users' perspectives of appropriateness, acceptability and feasibility. BMC Health Serv Res. (2019) 19:74. doi: 10.1186/s12913-018-3844-9
54. Kasaro, MP, Bosomprah, S, Taylor, MM, Sindano, N, Phiri, C, Tambatamba, B, et al. Field performance evaluation of dual rapid HIV and syphilis tests in three antenatal care clinics in Zambia. Int J STD AIDS. (2019) 30:323–8. doi: 10.1177/0956462418800872
55. Marks, M, Esau, T, Asugeni, R, Harrington, R, Diau, J, Toloka, H, et al. Point-of-care tests for syphilis and yaws in a low-income setting - a qualitative study of healthcare worker and patient experiences. PLoS Negl Trop Dis. (2018) 12:e0006360. doi: 10.1371/journal.pntd.0006360
56. Benzaken, AS, Sabido, M, Galban, EG, Pedroza, V, Vasquez, F, Araujo, A, et al. Field evaluation of the performance and testing costs of a rapid point-of-care test for syphilis in a red-light district of Manaus, Brazil. Sex Transm Infect. (2008) 84:297–302. doi: 10.1136/sti.2007.029462
57. Ruffinen, CZ, Sabido, M, and Diaz-Bermudez, XP. Point-of-care screening for syphilis and HIV in the borderlands: challenges in implementation in the Brazilian Amazon. BMC Health Serv Res. (2015) 15:495. doi: 10.1186/s12913-015-1155-y
58. Maddox, BLP, Wright, SS, Namadingo, H, Bowen, VB, Chipungu, GA, and Kamb, ML. Assessing stakeholder perceptions of the acceptability and feasibility of national scale-up for a dual HIV/syphilis rapid diagnostic test in Malawi. Sex Transm Infect. (2017) 93:S59–64. doi: 10.1136/sextrans-2016-053062
59. Dassah, ET, Adu-Sarkodie, Y, and Mayaud, P. Rollout of rapid point of care tests for antenatal syphilis screening in Ghana: healthcare provider perspectives and experiences. BMC Health Serv Res. (2018) 18:130. doi: 10.1186/s12913-018-2935-y
60. Flores, EC, Lluque, ME, Chiappe, M, Lino, R, and Bayer, AM. Operations research study to implement HIV and syphilis point-of-care tests and assess client perceptions in a marginalised area of Lima, Peru. Int J STD AIDS. (2015) 26:723–8. doi: 10.1177/0956462414552696
61. Bristow, CC, Lee, SJ, Severe, L, William Pape, J, Javanbakht, M, Scott Comulada, W, et al. Attributes of diagnostic tests to increase uptake of dual testing for syphilis and HIV in Port-Au-Prince, Haiti. Int J STD AIDS. (2017) 28:259–64. doi: 10.1177/0956462416642340
62. Withers, K, Bristow, C, Nguyen, M, Stafylis, C, Giang, LM, and Klausner, JD. A field evaluation of a rapid dual immunoassay for human immunodeficiency virus and syphilis antibodies, Hanoi, Vietnam. Int J STD AIDS. (2019) 30:173–80. doi: 10.1177/0956462418802685
63. Das, S, Grant, L, and Fernandes, G. Task shifting healthcare services in the post-COVID world: a scoping review. PLOS Glob Public Health. (2023) 3:e0001712. doi: 10.1371/journal.pgph.0001712
64. Cavalcante de Oliveira, AP, Galante, ML, Maia, LS, Craveiro, I, da Silva, AP, Fronteira, I, et al. Implementation of policy and management interventions to improve health and care workforce capacity to address the COVID-19 pandemic response: a systematic review. Hum Resour Health. (2023) 21:80. doi: 10.1186/s12960-023-00856-y
65. Matovu, JK, Wanyenze, RK, Mawemuko, S, Okui, O, Bazeyo, W, and Serwadda, D. Strengthening health workforce capacity through work-based training. BMC Int Health Hum Rights. (2013) 13:8. doi: 10.1186/1472-698X-13-8
66. Siow, WT, Liew, MF, Shrestha, BR, Muchtar, F, and See, KC. Managing COVID-19 in resource-limited settings: critical care considerations. Crit Care. (2020) 24:167. doi: 10.1186/s13054-020-02890-x
67. Lu, Y, Liu, Q, Yan, H, Gao, S, and Liu, T. Job burnout and its impact on work ability in biosafety laboratory staff during the COVID-19 epidemic in Xinjiang. BMC Psychiatry. (2021) 21:543. doi: 10.1186/s12888-021-03555-x
68. Marwaha, JS, Landman, AB, Brat, GA, Dunn, T, and Gordon, WJ. Deploying digital health tools within large, complex health systems: key considerations for adoption and implementation. NPJ Digit Med. (2022) 5:13. doi: 10.1038/s41746-022-00557-1
69. Hempel, S, Burke, R, Hochman, M, Thompson, G, Brothers, A, Shin, J, et al. Allocation of scarce resources in a pandemic: rapid systematic review update of strategies for policymakers. J Clin Epidemiol. (2021) 139:255–63. doi: 10.1016/j.jclinepi.2021.04.021
70. Snowdon, AW, and Wright, A. Supply chain capacity to respond to the COVID-19 pandemic in Ontario: challenges faced by a health system in transition. Healthc Manage Forum. (2022) 35:53–61. doi: 10.1177/08404704211057664
71. Maluleke, K, Musekiwa, A, Kgarosi, K, Gregor, EM, Dlangalala, T, Nkambule, S, et al. A scoping review of supply chain Management Systems for Point of care diagnostic services: Optimising COVID-19 testing capacity in resource-limited settings. Diagnostics (Basel). (2021) 11:2299. doi: 10.3390/diagnostics11122299
Keywords: SARS-CoV-2, influenza A and B, rapid antigen testing, congregate living settings, implementation strategies, barriers and facilitators
Citation: Garad Y, Manea AA, Pak N, Danok L, Baral S, Dykstra T, Kasperavicius D, Straus SE and Fahim C (2025) An evaluation of barriers and facilitators to implementing multiplex rapid antigen testing for SARS-CoV-2 and influenza A and B in congregate living settings. Front. Public Health. 13:1560131. doi: 10.3389/fpubh.2025.1560131
Edited by:
Xin Ye, The First Affiliated Hospital of Xi’an Jiaotong University, ChinaReviewed by:
Io Cheong, Shanghai Jiao Tong University, ChinaCopyright © 2025 Garad, Manea, Pak, Danok, Baral, Dykstra, Kasperavicius, Straus and Fahim. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christine Fahim, Q2hyaXN0aW5lLkZhaGltQHVuaXR5aGVhbHRoLnRv
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.