 Yuyuan Zhang
Yuyuan Zhang Ming Zhou1
Ming Zhou1
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 26 February 2025
Sec. Aging and Public Health
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1535987
This article is part of the Research Topic Caregiving for Older Adults within Community Settings View all articles
Objectives: Accessibility is a critical factor in ensuring equitable public services. In urban older adult care systems, resource allocation and service disparities present unique challenges. The classical “5A” theory—availability, accessibility, affordability, adaptability, and acceptability—provides a robust framework for evaluating service delivery. However, its application in urban older adult care, especially in rapidly aging societies like China, remains limited. This study aims to develop and validate a framework to address affordability, resource allocation, and service mismatches in urban older adult care systems.
Methods: A web-based cross-sectional study was performed in 2023. A multi-phase methodology was adopted to construct the framework, grounded in the “5A” theory. Indicators were refined through expert consultations using the Delphi method, involving 20 experts, while the entropy weight method ensured objective indicator weighting. The framework was empirically validated in Xi’an, China, using survey data collected from 438 older adult residents across urban strata. A fuzzy comprehensive evaluation (FCE) method was employed to assess accessibility and identify key service gaps.
Results: This study constructs a comprehensive evaluation framework for basic older adult care services (BECS), structured around 5 primary dimensions, 14 sary indicators, and 37 tertiary indicators. Empirical validation in Xi’an further demonstrates the framework’s scientific rigor and practical applicability. While the framework identifies strong spatial accessibility (3.8815), it also reveals critical gaps in affordability (3.1347) and psychological care (3.0862), confirming its effectiveness in diagnosing systemic disparities and guiding policy interventions.
Conclusion: This study introduces a novel accessibility evaluation framework tailored for basic older adult care services, addressing critical gaps in affordability, psychological care, and service responsiveness. Empirical results validate the framework’s practicality and its alignment with the real-world conditions of urban aging societies. Furthermore, an innovative “Matching-Realization-Satisfaction” improvement pathway is proposed, offering actionable strategies to enhance accessibility and optimize service delivery. This framework serves as a replicable model for advancing equitable older adult care in rapidly aging urban communities.
Population aging remains a persistent global challenge (1). Population aging is not limited to developed countries; developing nations are also facing this demographic trend (2). By 2030, the global population aged 65 and older is expected to reach 994 million, and this figure is projected to rise to 1.6 billion by 2050 (3). Aging has become one of the most significant demographic trends of the 21st century (4) and will shape China’s future demographic structure. According to the United Nations, these shifts highlight the growing urgency of addressing challenges posed by an aging population. By the end of 2023, individuals aged 60 and 65 and above are expected to account for 21.1 and 15.4% of China’s total population, respectively (5). The escalating aging trend poses significant challenges to the nation’s pension service system (6).
In the context of population aging and rapid social and economic transformations, expectations and preferences for living arrangements have undergone significant changes in recent decades, particularly in urban areas. The one-child policy, coupled with the rising participation of women in the workforce, has limited the younger generation’s ability to care for the older adult (7). Consequently, Chinese society has sought alternative sources of older adult care support (8), with basic older adult care services emerging as the cornerstone of the country’s multi-tiered older adult care system (9, 10). The release of Opinions on Promoting the Construction of a BECS System has established a strategic framework emphasizing material assistance and care services as its core components. Specifically, BECS includes essential services such as home-based care, which provides daily living support, healthcare, and in-home medical care; institutional care, which offers comprehensive long-term care and rehabilitation in dedicated facilities; health management, such as regular health check-ups, chronic disease management, and psychological health services; social participation and cultural engagement, which encourage older adult individuals to participate in community activities and foster intergenerational interactions; and policy support, such as financial subsidies and housing assistance tailored to the needs of disadvantaged groups. Despite significant progress in building its basic older adult care system, challenges persist, including urban–rural disparities, unequal resource distribution, and mismatches between service supply and demand (11), particularly in bridging the “last mile.” Despite significant progress, challenges remain in China’s basic older adult care system, such as urban–rural disparities, unequal resource distribution, and mismatches between service supply and demand, especially in addressing the “last mile.”
Accessibility is a key requirement for building a modern Chinese-style public service system (12). Enhancing accessibility has become a critical policy objective for advancing the basic public service system. Accessibility focuses on the endpoints of service delivery, aiming to improve recipients’ sense of access and satisfaction by enhancing the convenience and usability of public services, with greater emphasis on functional value. Ensuring that basic old-age services truly benefit older adult populations, while enhancing accessibility, is a pressing issue at this stage of service development. Despite progress in constructing a basic old-age care system across China, the lack of standardized evaluation metrics and frameworks persists.
We address the theoretical and practical demands of developing BECS by incorporating Western classical accessibility concepts and domestic research paradigms. First, we clarifiy the core elements and dimensions of basic older adult care service accessibility. Second, it employs the Delphi method, entropy weight method, and other approaches to construct and refine the evaluation index system for assessing the accessibility of BECS in urban communities. Representative areas are selected for empirical research to validate the system’s rationality and feasibility. Finally, the evaluation results and current practices are analyzed to pinpoint key areas and priorities for improving the accessibility of basic older adult care services.
We employed a cross-sectional design to evaluate disparities in the accessibility of basic older adult care services (BECS) in urban districts of Xi’an, using a multidimensional framework grounded in the ‘5A’ theory: availability, accessibility, affordability, adaptability, and acceptability. This evaluation follows a systematic approach encompassing four stages: framework construction, indicator optimization, stakeholder empowerment, and application validation, as illustrated in Figure 1.
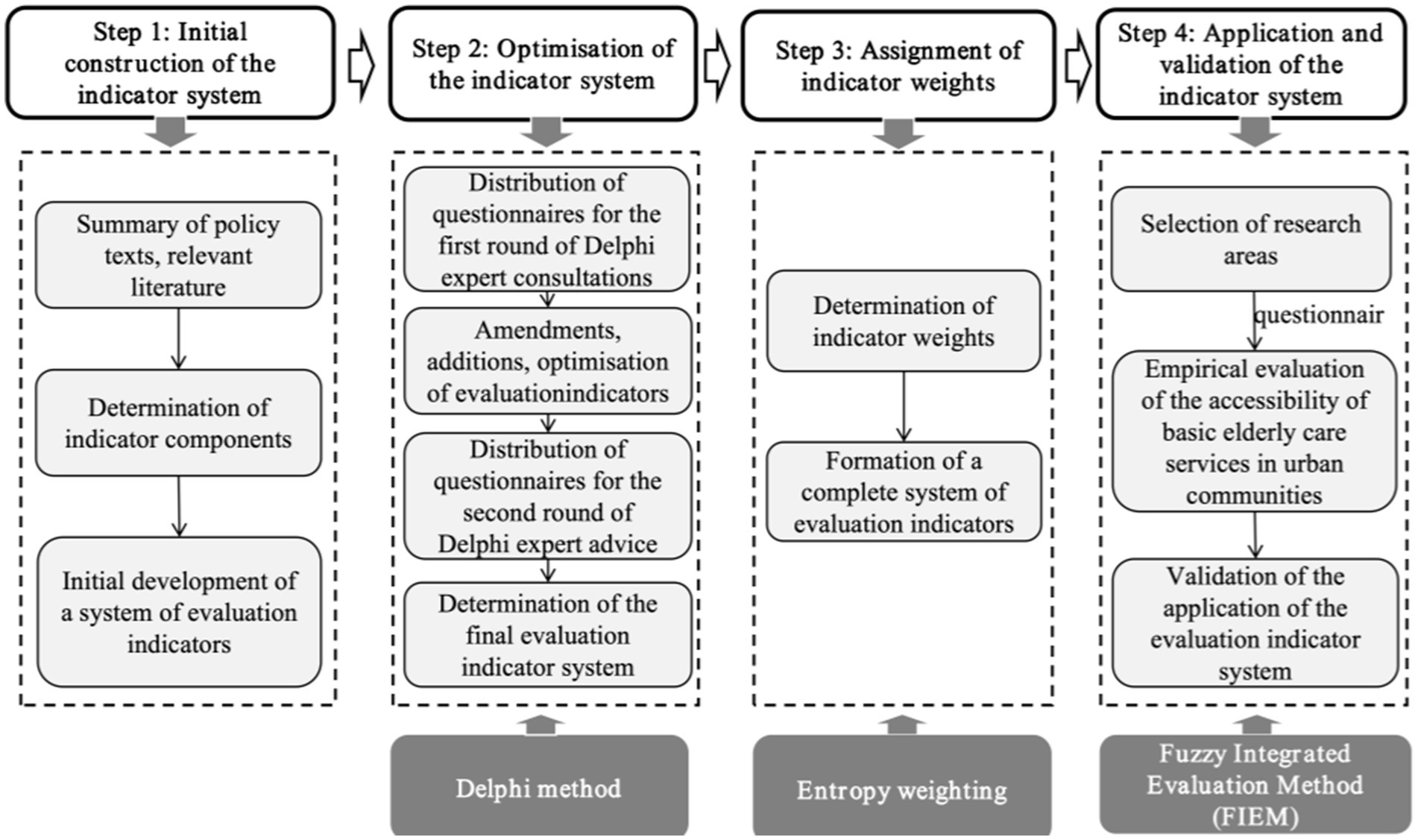
Figure 1. Research framework.
Stage 1: Initial Construction of the Indicator System—A systematic review and integration of relevant literature identifies core dimensions and detailed indicators for evaluating BECS in urban communities.
Stage 2: Optimization of the Indicator System—Indicators were developed using a structured literature review and expert consultations conducted through the Delphi method. This iterative process involved experts from gerontology, public health, and social welfare fields. A total of 5 primary dimensions, 14 sary indicators, and 37 tertiary indicators were finalized to comprehensively evaluate accessibility.
Stage 3: Indicator Weight Assignment—Weights are assigned using the entropy weighting method based on field research data, ensuring objectivity and reliability in the optimized indicator system.
Stage 4: Application and Validation of the Indicator System—A typical urban area in Xi’an is selected for empirical research. A Likert five-point scale and the fuzzy comprehensive evaluation method are employed to validate the system’s effectiveness.
Accessibility refers to the actual use of services by individuals in need rather than merely the presence of facilities, indicating the extent to which public service systems are effectively utilized (13). The concept of accessibility, originating in Western healthcare (14), is discussed in academia through two primary perspectives: service utilization and the degree of “fit.” From the “service use” perspective, Andersen defines accessibility as individuals’ actual utilization of health services, emphasizing the factors that either facilitate or hinder service use (15). Conversely, Penchansky and Thomas adopt a “fit” perspective, criticizing Andersen’s exclusion of payment ability and defining accessibility as the degree of alignment between user needs and service systems (16). The matching perspective is widely recognized, forming the basis for classical models such as Katarina’s “4A” framework (17) and Penchansky and Thomas’s five-dimensional framework of accessibility, adaptability, affordability, availability, and acceptability (18). In older adult care, accessibility theory primarily evaluates service quality, often emphasizing the fit between services and user needs (19). Scholars have assessed older adult services through content, geographic and temporal, and economic accessibility. Others have refined these dimensions to construct models focusing on financial, content, and service mode accessibility (20). The “5A” model has also been widely adopted to evaluate older adult service quality comprehensively (21–23). Improving the accessibility of BECS to benefit the older adult population has emerged as a critical issue at the current stage of development.
Following the structural framework of “Definition-Assessment-Application,” we define the accessibility of BECS as the degree of alignment between the needs of older adult individuals and the resources of the basic older adult care system. Specifically, it examines whether older adult individuals can access government- and community-provided care services adequately, conveniently, and efficiently and whether the available resources meet service demands. Considering the development and current practices of BECS in China’s urban communities, we incorporate Penchansky and Thomas’s “5A” analysis framework of health service accessibility. The five key dimensions—availability, accessibility, affordability, adaptability, and acceptability—are adapted to the BECS system. These dimensions are further refined and extended to construct the “5A” conceptual model of accessibility for BECS in urban communities, as illustrated in Figure 2.
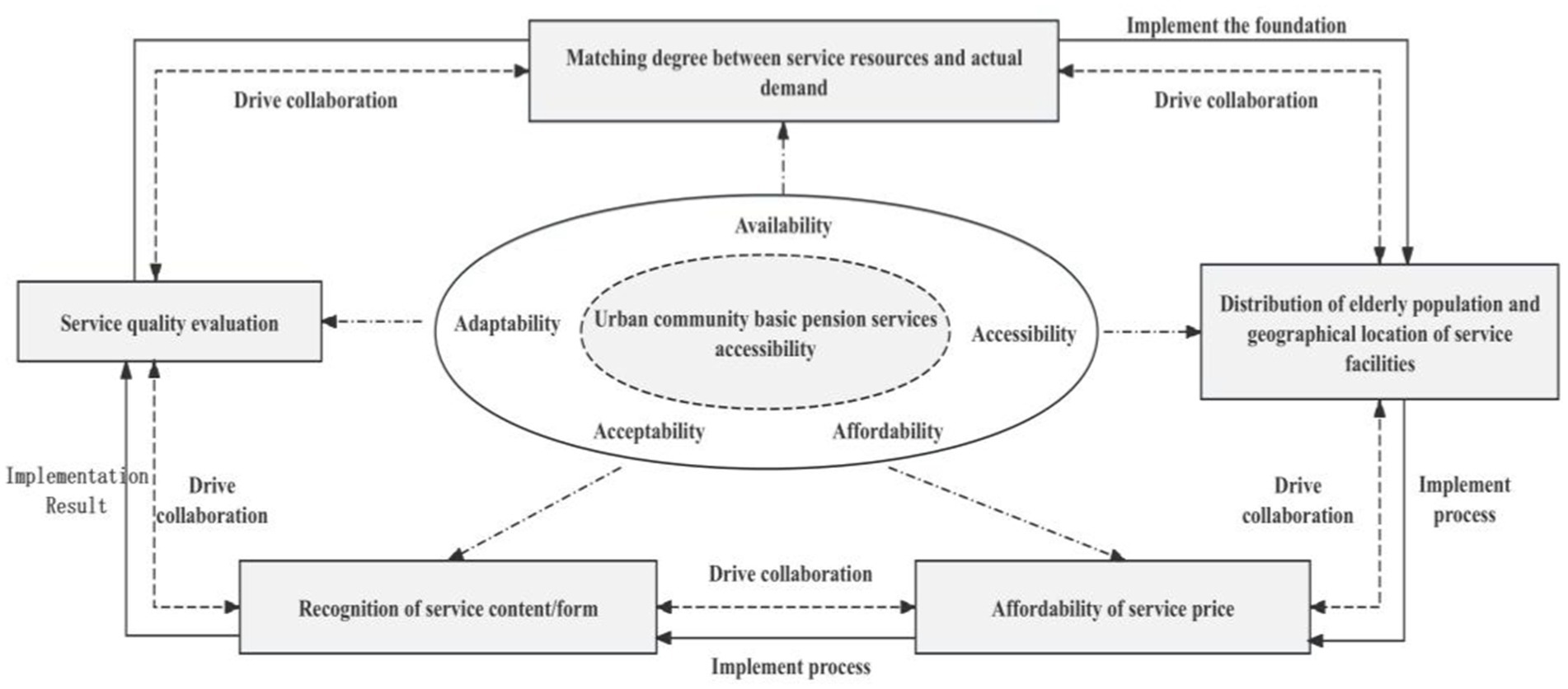
Figure 2. Conceptual model of ‘5A’ accessibility of basic older adult services.
The Delphi Method is a research approach that gathers expert opinions through multiple rounds of structured correspondence to reach a consensus (24). The expert questionnaire in this study consists of two main sections: (1) This section collects basic information about the respondents, including their academic background, knowledge of basic older adult care services, and the rationale for completing the questionnaire. (2) This section asks respondents to rate the importance of indicators on a five-point Likert scale, ranging from 1 (least important) to 5 (most important). The indicator system in the questionnaire is old far based mainly on the accessibility theory and combined with national policy documents (see Supplementary material for details).
Based on the study requirements, 20 experts from relevant fields were invited to participate, as detailed in Table 1. The selection criteria for these experts were: (a) holding professional titles of intermediate level or higher; (b) having a deep understanding of the field with over 10 years of relevant experience; (c) possessing an undergraduate degree or higher academic qualification; (d) demonstrating willingness and availability to engage in this study actively. The co-ordination coefficients and statistical results of the two rounds of expert consultation are detailed in Supplementary material. The co-ordination coefficients for the first and second rounds are 0.328 and 0.332 respectively, and the tests of significance satisfy the statistical requirements, demonstrating the consistency of the expert opinions.
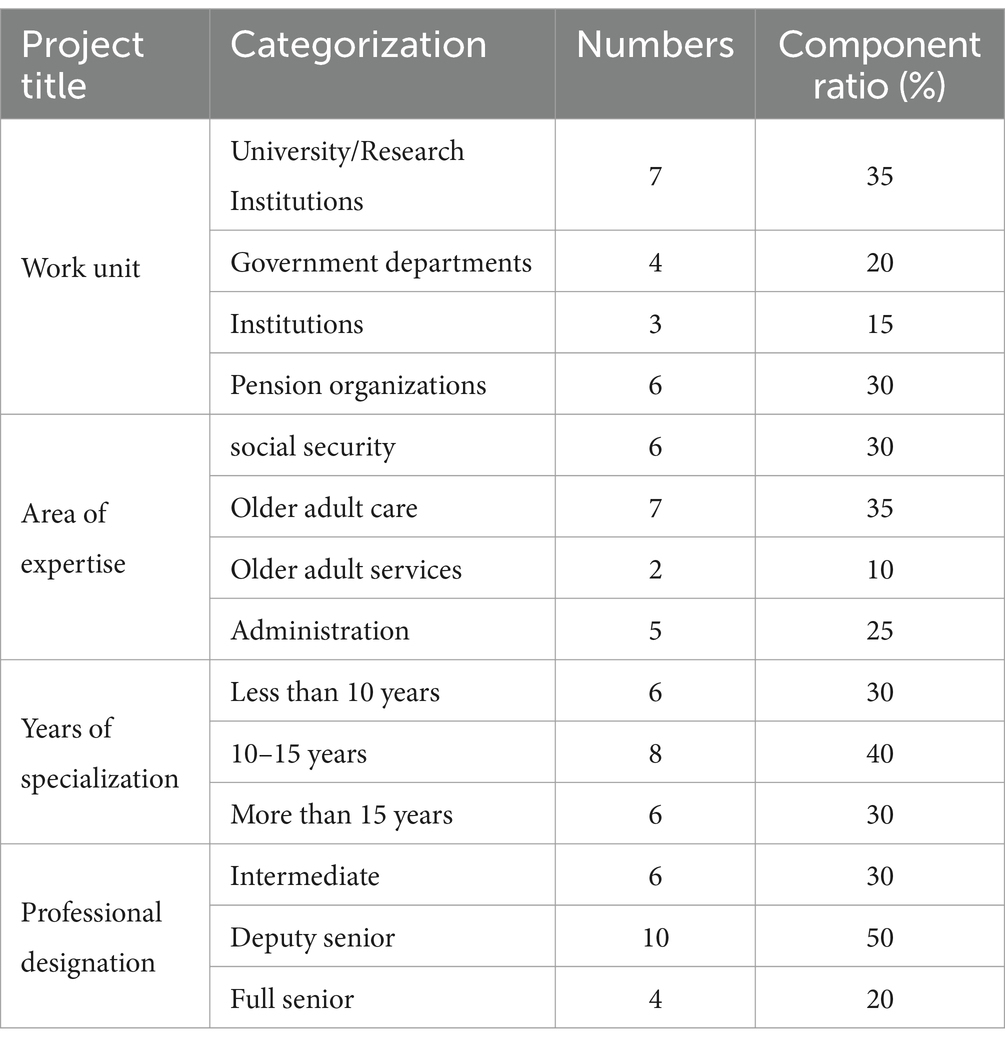
Table 1. Basic information on experts.
The accessibility of BECS in urban communities is often assessed based on the subjective perceptions of the older adult. However, traditional subjective weighting methods have inherent limitations. Therefore, we employ the entropy weight method as an objective approach to assign weights for analysis (25). The detailed process of weight calculation is as follows:
(a) Data normalization.
Assuming that there are n evaluation objects and m evaluation indicators, the value of the jth indicator of the ith evaluation object is denoted as xij. Through data normalization, the differences arising from different scales of the indicators are eliminated in order to make the values of the indicators have the same scale and magnitude, so as to achieve the homogeneity of the values.
For positive indicators:
For negative indicators:
(b) Calculation of the weight of the ith evaluation object under the jth evaluation indicator:
(c) Calculate the entropy value of the jth indicator:
(d) Calculate the information entropy redundancy (utility value):
(e) Calculation of the weights of the indicators:
Following the outlined process, the weights of the second-level indicators are calculated as the sum of the corresponding third-level indicator weights. Similarly, the weights of the first-level indicators are derived by aggregating the weights of the second-level indicators. The calculation of these weights is based on Equations 1–7, which detail the normalization and weighting procedures. The specific weight results, which will be presented later in Table 5, outline the accessibility evaluation indicator system and its associated weights for basic older adult services in urban communities. These results are detailed in the Results section (Section 3.2).
The fuzzy comprehensive evaluation method applies fuzzy mathematical theory to address evaluation factors with ambiguous boundaries and challenges in quantification (26). The fuzzy comprehensive evaluation (FCE) method was employed to integrate both qualitative and quantitative data for each dimension. This approach accommodates uncertainty and subjectivity inherent in survey responses, synthesizing scores to generate an overall accessibility evaluation. In addition to the structured Likert-scale questions providing quantitative inputs, qualitative data were also incorporated into the FCE analysis. Examples of qualitative data include: (1) Open-ended survey questions: Participants provided detailed feedback on their satisfaction with cultural activities, emotional support services, and accessibility of community facilities. These responses supplemented quantitative ratings and offered insights into unmet needs. (2) Field observations: During visits to community service centers, researchers documented observations related to facility usability, inclusiveness of service environments, and staff responsiveness, which informed the evaluation of adaptability and acceptability dimensions. (3) Caregiver narratives: For participants unable to complete the survey independently, caregivers contributed qualitative insights regarding the challenges and effectiveness of home-based care services.
The FCE process was employed to assess the accessibility of Xi’an’s central city through the following steps:
(1) Construct the evaluation factor set. Denote the set of indicators for this evaluation of the accessibility of BECS in urban communities by U, U = {u1, u2, …, um}.
2. Construct the evaluation set. The evaluation set is the result synthesized by the respondents’ scores on the evaluation of the accessibility of basic older adult care services. The evaluation ratings are described by V = {V1, V2, …, V5}, where V1 means very satisfied, V2 means satisfied, V3 means average, V4 means dissatisfied, and V5 means very dissatisfied.
(3) Determining the degree of affiliation. The number of samples corresponding to the evaluation levels of the 37 tertiary indicators can be obtained according to the scoring situation, divided by the total number of the corresponding, that is, to obtain the degree of affiliation corresponding to each level.
(4) Construct the weight set. The weight of each indicator has been calculated according to the entropy weight method.
(5) Compound operation of fuzzy matrix, through the synthetic operation of weight set W and evaluation result V, in order to precise the overall judgment vector of each indicator, and get the evaluation result corresponding to each indicator.
Xi’an, the capital of Shaanxi Province, was chosen as the study site due to its unique demographic profile and its significance in addressing aging-related challenges in urban China. As of 2023, Xi’an has a population of approximately 13.08 million, with 15.5% aged 60 or older and 12.6% aged 65 or older (27), classifying it as a deeply aging society. The city has faced aging-related issues, such as an imbalance between the supply and demand for older adult care services, earlier than many other Chinese cities. Its advanced efforts in developing older adult care infrastructure and services make Xi’an an ideal location to test the feasibility and applicability of the proposed evaluation framework.
We focused on the central urban areas of Xi’an, including Xincheng, Beilin, Lianhu, Baqiao, Weiyang, and Yanta districts, as the sample region. A combination of stratified and random sampling was employed to ensure a diverse and representative sample across different urban strata. Eligible participants were required to meet the following criteria: (1) aged 60 years or older and (2) had previously received basic older adult care services.
Data collection was primarily conducted at community older adult service centers through face-to-face interviews and paper questionnaires, complemented by surveys in other community locations, such as activity centers and nearby parks. For participants with limited mobility or reduced self-care ability, caregivers or family members were permitted to complete the questionnaire on their behalf. This stratified sampling approach, combined with the targeted distribution of questionnaires, ensured the validity and authenticity of the responses while reflecting the diverse conditions of older adult residents in urban areas.
To determine the sample size, we applied the formula for large sample populations proposed by Wu (28):
where the significant level α is 0.05 (28) and the confidence level used for interval estimation is 1-α = 0.95, at which point the quantile k = 1.96, and according to this formula, the calculation yields n ≥ 384.
To account for potential non-responses and ensure a robust sample size, a total of 438 questionnaires were distributed. Among these, 430 valid responses were recovered, resulting in a response rate of 98.17%. Missing data accounted for less than 5% of the total dataset, primarily due to incomplete demographic information. These missing values were addressed using multiple imputation to ensure data integrity without biasing the analysis. The respondents’ basic information is detailed in Table 2.
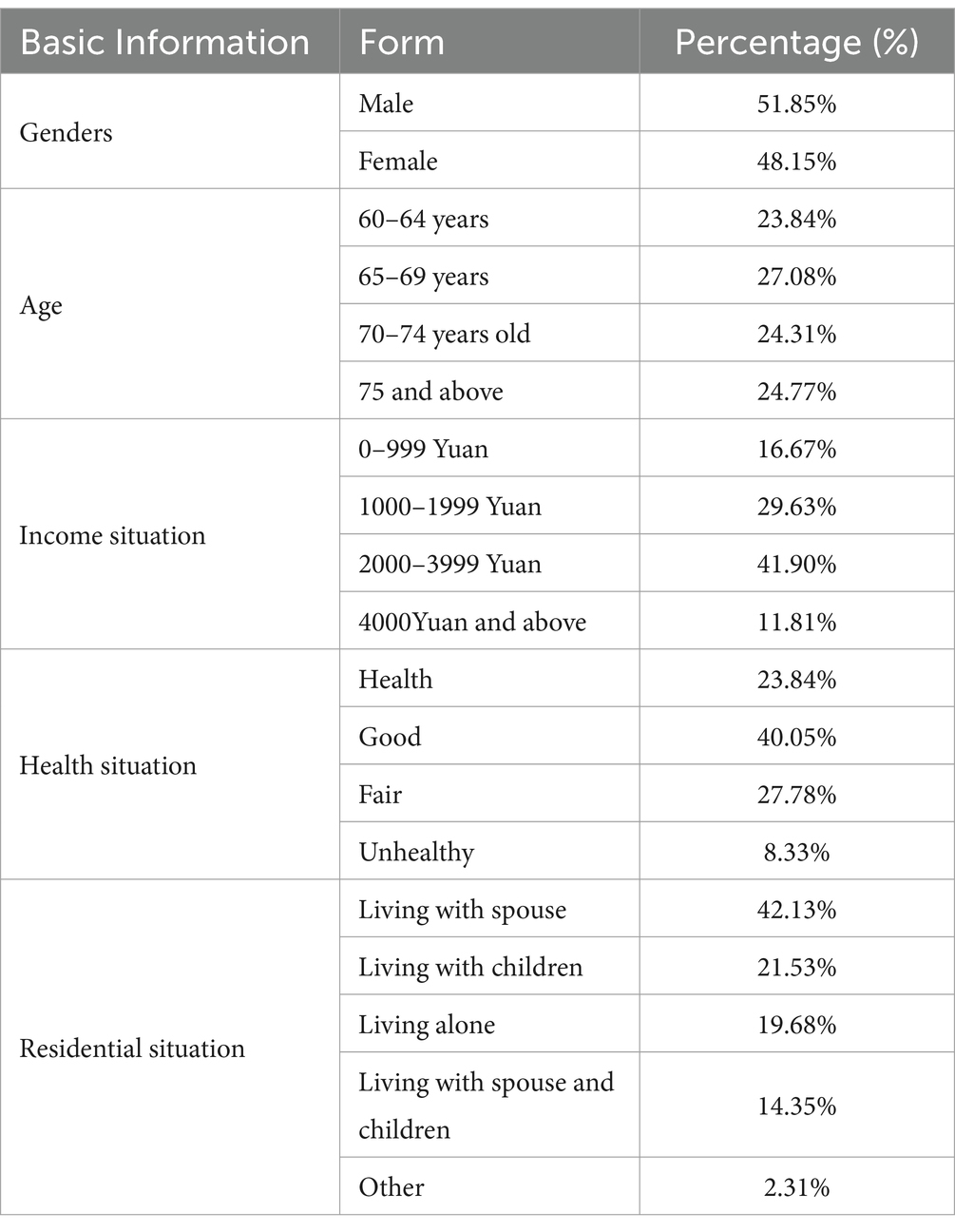
Table 2. Basic information of survey respondents.
Expert authority degree coefficient (Cr) ≥ 0.70 is acceptable coefficient (29), expert authority coefficient (Cr) = (Ca + Cs) / 2, Ca is the basis of expert judgment. The Cr value ranges from 0 to 1, with higher values indicating greater expert authority. The quantitative results for expert authority are presented in Table 3.
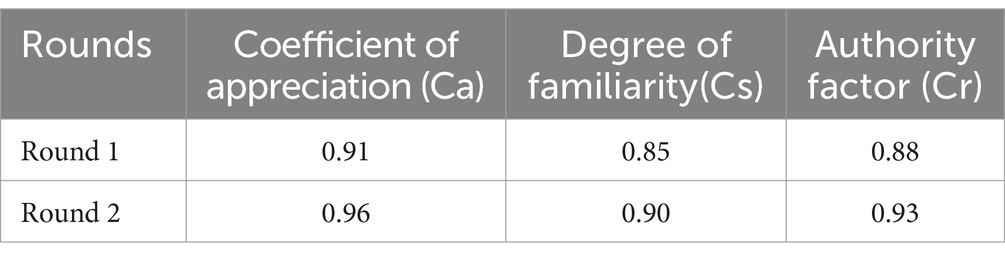
Table 3. Degree of authority of experts.
The consistency of the evaluation indicators is assessed using Kendall’s WWW harmony coefficient, which ranges from 0 to 1. Higher WWW values indicate greater consistency among expert opinions. As shown in Table 4, the significance test for the harmony coefficient yielded a p-value below the threshold of 0.05, confirming its statistical significance. Therefore, the expert evaluations demonstrated consistency and satisfied the criteria for indicator screening.
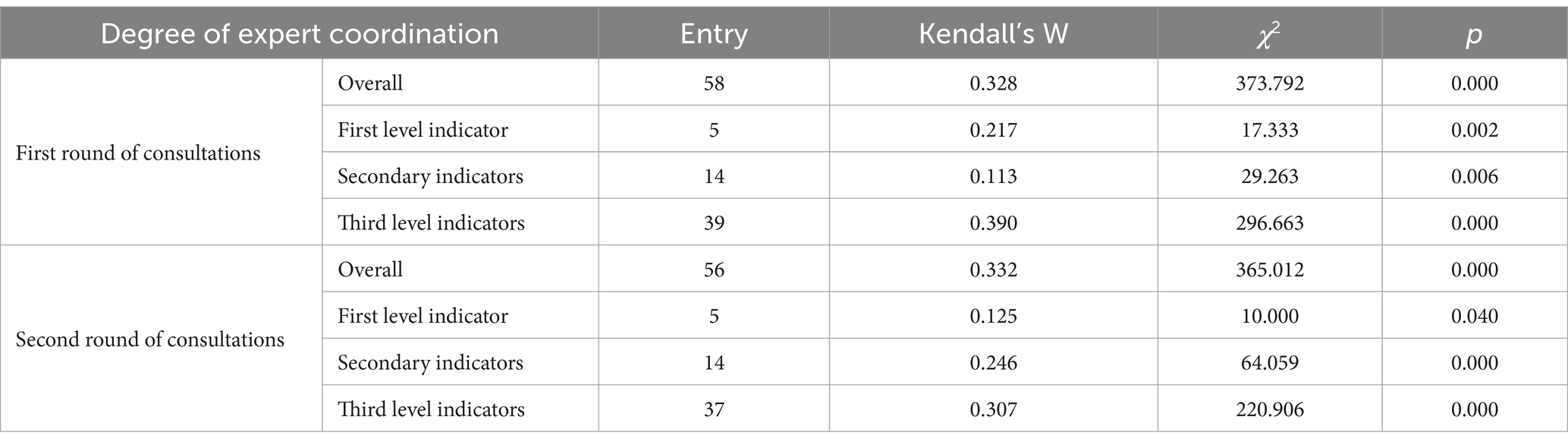
Table 4. Degree of coordination between the two rounds of consultancies.
Following two rounds of Delphi expert consultation, a final evaluation indicator system for assessing the accessibility of BECS in urban communities was established. The system comprises 5 first-level indicators, 14 second-level indicators, and 37 third-level indicators, as detailed in Table 5. According to the weighting order presented in Table 5, affordability ranks highest, followed by availability, adaptability, acceptability, and accessibility. Among the 14 second-level indicators, resource provision emerges as the core element with the highest weight (0.0943), underscoring the critical role of abundant resources in ensuring access to older adult care services. Facility provision (0.077) and facility layout (0.0616) rank next, emphasizing the significance of sufficient older adult beds and diverse programs in meeting the varied needs of the older adult population. The prices of life care services (0.0820) and spiritual comfort services (0.0859) carry comparable weights, reflecting the older adult’s dual focus on quality of life and emotional well-being.
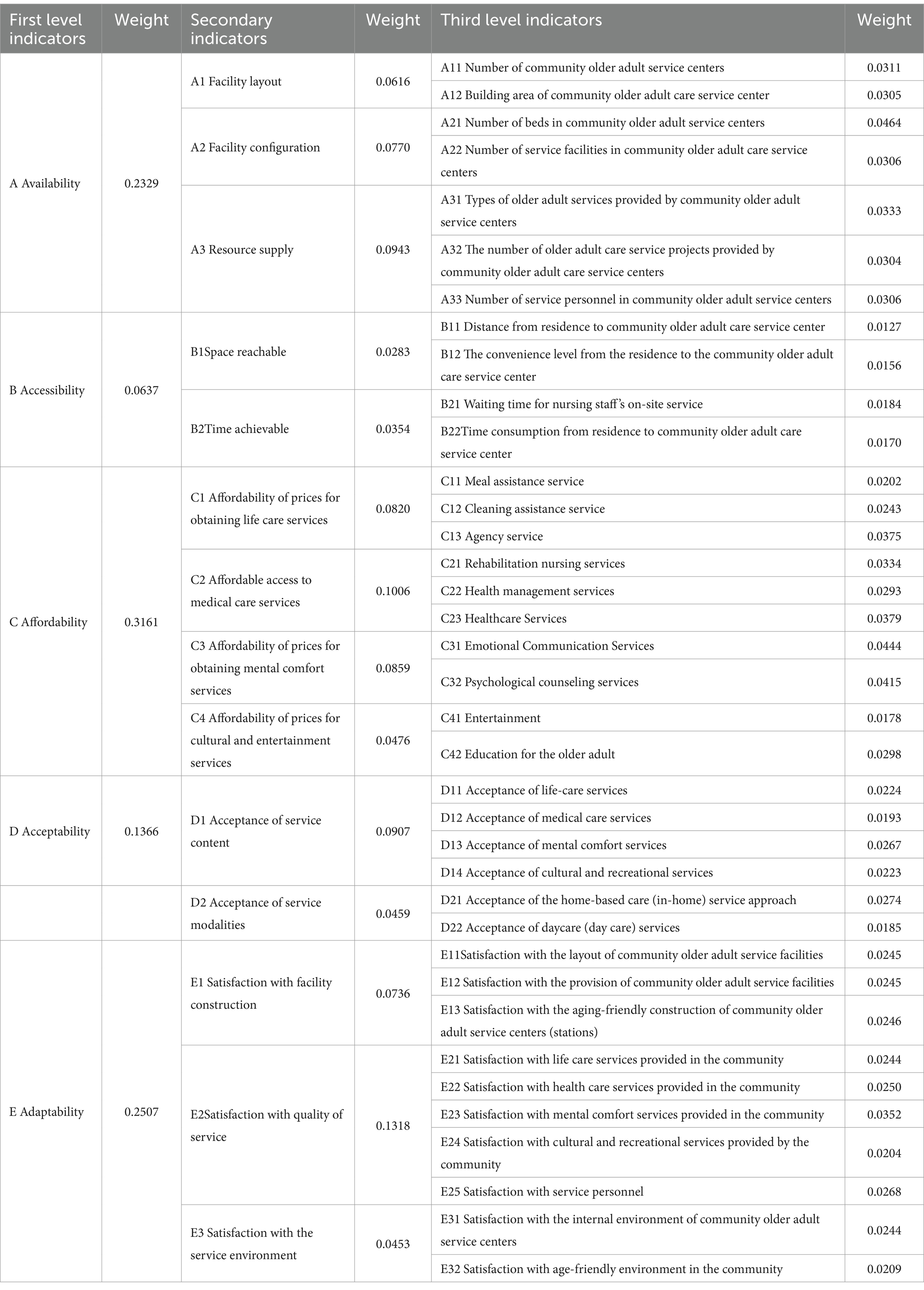
Table 5. Evaluation indicator system for accessibility of basic older adult services in urban communities and its weights.
The primary, secondary, and tertiary indicators, along with the comprehensive evaluation results, were determined by de-fuzzifying the evaluation result set, as detailed in Table 6. Using the final calculated PPP value for de-fuzzification as an example, the comprehensive evaluation score for the accessibility of basic community older adult care services in Xi’an’s urban center is:
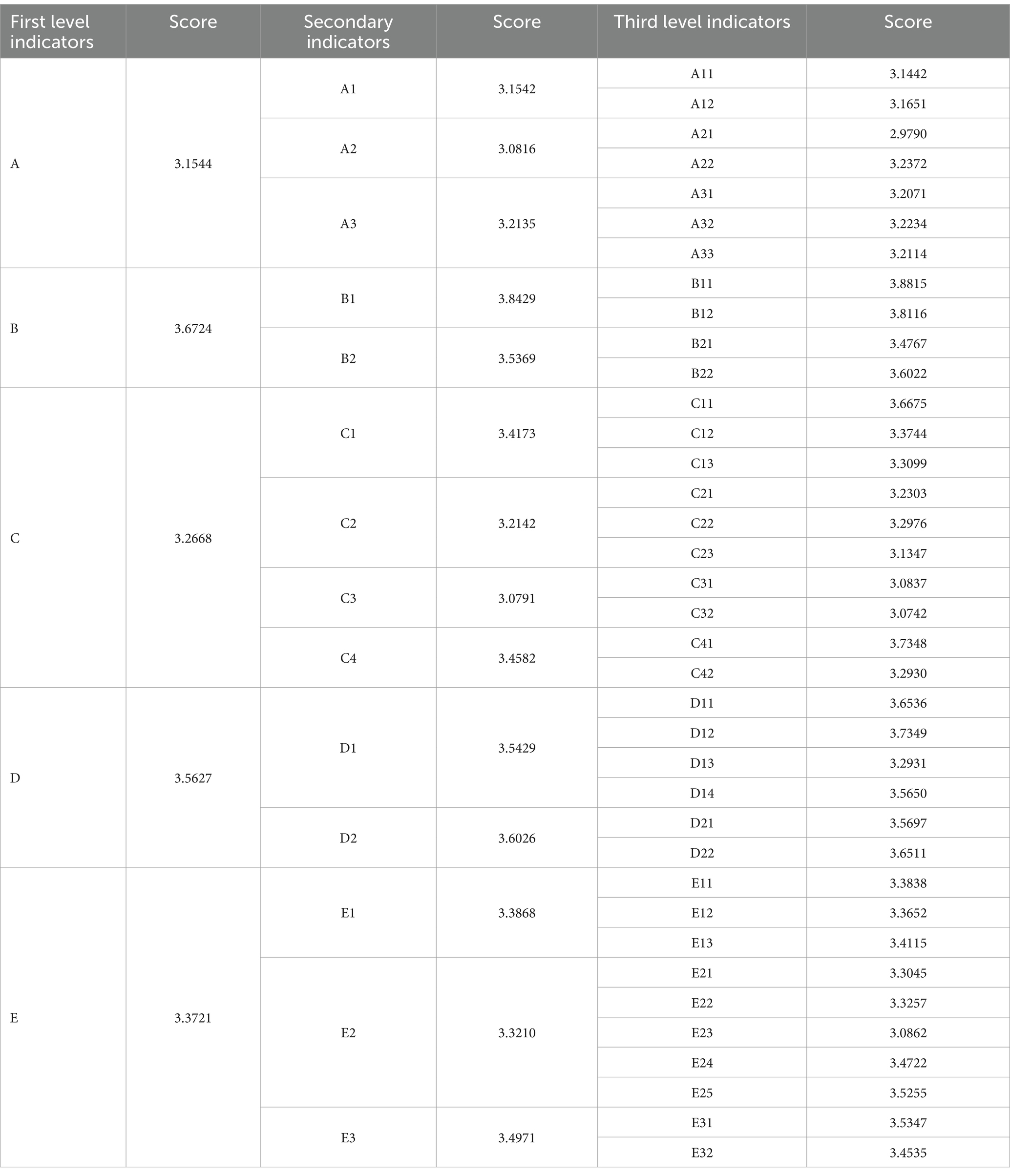
Table 6. Evaluation results of the accessibility of basic community-based older adult care services in the six urban districts of Xi’an City.
The empirical analysis in Xian’s central urban area underscores the importance of affordability, availability, and adaptability in ensuring equitable older adult care. These findings are critical for policymakers and healthcare providers, emphasizing key areas for prioritizing resource allocation and service improvements. A systematic assessment of the accessibility of community-based older adult care services in Xi’an’s central urban districts (Baqiao, Weiyang, Yanta, Xincheng, Beilin, and Lianhu) was conducted using the fuzzy comprehensive evaluation method, with results presented in Figure 3. We result indicate that the overall accessibility score of Xi’an’s six central urban districts is 3.3330, falling within the “average” range to “good.” This reflects an overall efficient provision of public service facilities, adequately meeting the basic daily needs of most older adult residents.
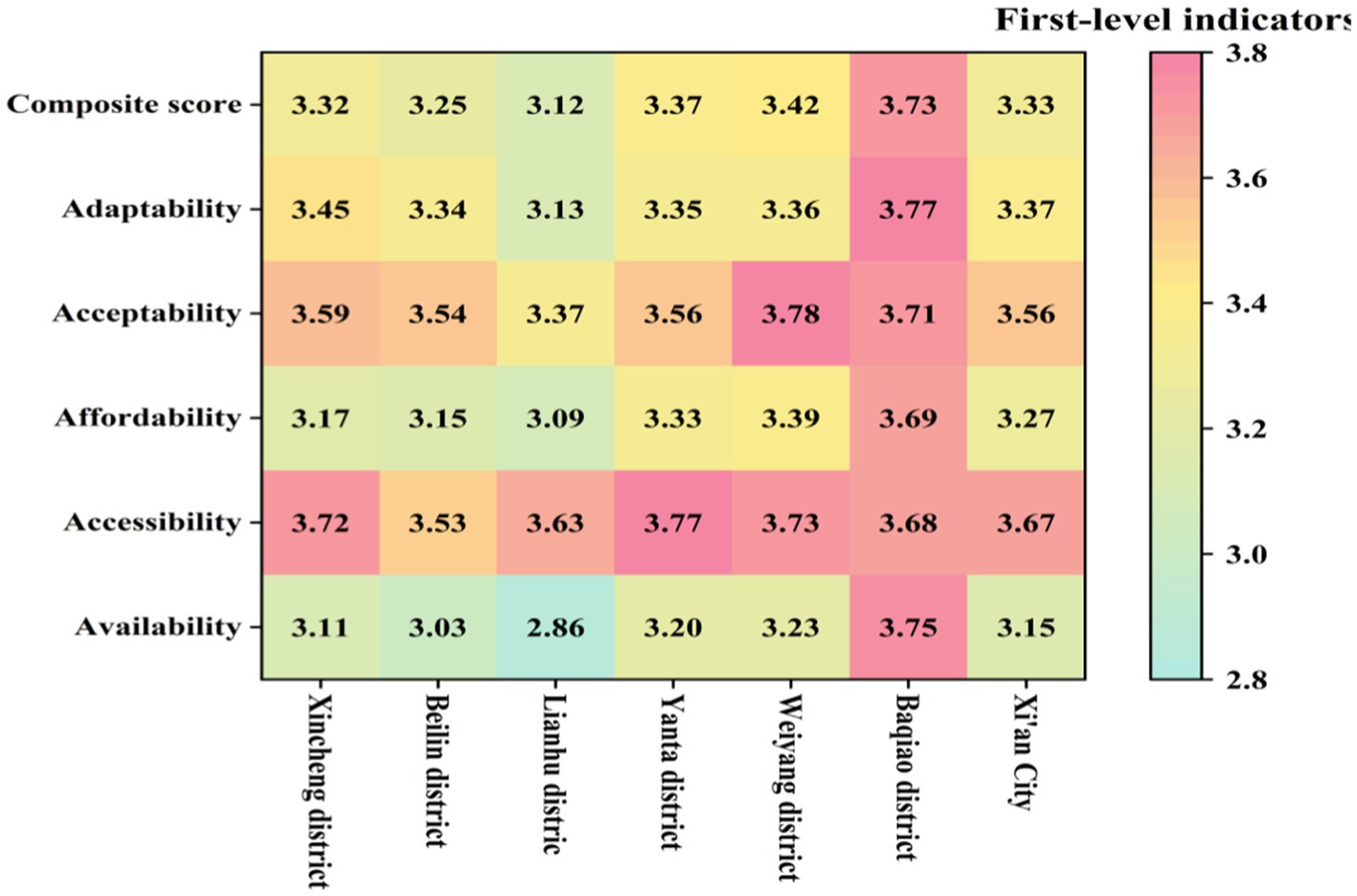
Figure 3. Hot map of accessibility evaluation results for BECS in urban communities.
The data reveal a structural imbalance between resource supply and growing demand, highlighting an availability dilemma (30). The availability score is 3.1544, with facility layout and equipment scoring 3.1542 and 3.0816, respectively, suggesting that the infrastructure generally meets the basic needs of the older adult. However, the score for the number of beds is relatively low (3.2135), revealing a structural shortfall in resource capacity. This result reflects a lag in facility investment and planning relative to the surge in service demand caused by accelerated aging.
Accessibility is challenged by both spatial optimization and service responsiveness (31). The overall accessibility score is 3.6724, with spatial accessibility scoring a relatively high 3.8429, suggesting that the central city’s service facility layout is reasonable. However, the time accessibility score is relatively low (3.5369), with waiting times for door-to-door services scoring only 3.4767, indicating significant room for improvement in service responsiveness. This disparity between spatial and temporal accessibility highlights the tension between facility centralization and service personalization. While centralized facility layouts provide spatial convenience, they limit the flexibility of service responsiveness, particularly in addressing personalized and urgent needs.
Affordability faces a dual imbalance in economic costs (32). The affordability score is 3.2668, with meal assistance services scoring the highest (3.6675) and healthcare services the lowest (3.1347). The high cost of healthcare services imposes a financial burden on low-income older adult groups, exposing a gap between basic living and healthcare needs. This finding underscores insufficient policy support and the limitations of the social security system in addressing high-cost healthcare services.
Acceptability faces challenges related to neglecting psychological needs and insufficient cultural adaptation. The acceptability score is 3.5627, with medical services scoring the highest (3.7349) and psychological comfort services the lowest (3.2931). The low score reflects insufficient psychological support services and unmet emotional and spiritual care needs among the older adult. This issue indicates an overemphasis on material needs in the older adult service system, with insufficient attention and resources allocated to soft needs such as emotional care and social participation.
Adaptability faces challenges due to the absence of a dynamic adjustment mechanism. The adaptability score is 3.3721, with high satisfaction in cultural and recreational services (3.4722) and the lowest satisfaction in spiritual comfort services (3.0862). The low satisfaction score highlights inadequate psychological support services and the absence of a dynamic adjustment mechanism to address the increasingly complex needs of the older adult. The mismatch between service supply and demand has resulted in a disconnect between service quality and the actual needs of the older adult.
These results underscore the systemic challenges in resource allocation and service capacity, necessitating policy interventions tailored to affordability and psychological care deficiencies.
We developed a comprehensive indicator system to assess the accessibility of basic older adult care services (BECS) in urban communities, structured around five dimensions: availability, accessibility, affordability, adaptability, and acceptability. Using Xi’an City as a case study, the framework highlights critical disparities in service provision. For instance, affordability received a score of 3.1347, indicating significant financial barriers for older adult residents, while spiritual comfort services scored 3.0862, revealing substantial gaps in emotional and psychological care. Conversely, spatial accessibility achieved a high score of 3.8815, reflecting effective infrastructure planning and facility distribution. However, delays in caregiver home visits, with a score of 3.4767, indicate persistent gaps in responsiveness and personalized care. These results underscore the multidimensional challenges facing urban older adult care systems and provide actionable insights for addressing them.
A distinguishing feature of this study is its focus on the unique characteristics of BECS, emphasizing universal coverage and equity. BECS prioritize economically disadvantaged and health-compromised populations, contrasting with general older adult care frameworks that often target affluent groups with premium or personalized services. The results validate this distinction, as affordability and availability emerge as key dimensions requiring targeted interventions. The low affordability score of 3.1347 highlights the urgent need for financial subsidies, particularly for low-income older adult populations. The framework’s emphasis on equity and inclusivity makes it a practical tool for guiding public welfare policy.
As a deeply aging city, Xi’an faces systemic constraints such as resource imbalances and insufficient service capacity. While investments in infrastructure have enhanced spatial accessibility, affordability and psychological care deficiencies remain significant barriers. For example, while investments in infrastructure have enhanced spatial accessibility (score: 3.8815), persistent affordability challenges and gaps in psychological care (score: 3.0862) underscore the need for targeted investments. Addressing these challenges requires a multi-pronged strategy.
Based on these findings, We adopt a “demand–supply matching, service realization, and satisfaction enhancement” framework to examine strategies for improving the accessibility of BECS in urban communities (Figure 4). Effective demand–supply alignment requires a dynamic, data-driven approach to monitor demographic trends and forecast resource needs. Transitioning from reactive to proactive service models involves leveraging intelligent platforms to enable real-time resource allocation and optimize service delivery. Service realization depends on integrated funding mechanisms and age-friendly environments. A unified funding framework ensures efficient resource utilization, while investments in accessible infrastructure, including barrier-free facilities and digital adaptations, address the diverse needs of older adult populations. Enhancing satisfaction is critical for fostering continuous improvement, supported by comprehensive oversight mechanisms and innovative service delivery approaches. Comprehensive monitoring frameworks—incorporating governmental, non-governmental, and public stakeholders—facilitate accountability, while feedback systems inform actionable improvements. Innovative models, such as ‘Internet + Older adult Care’ and mutual assistance initiatives like ‘time banking,’ expand service options and enhance the well-being of older adults. Collectively, these strategies offer a holistic and adaptable blueprint for advancing the accessibility and equity of urban older adult care services.
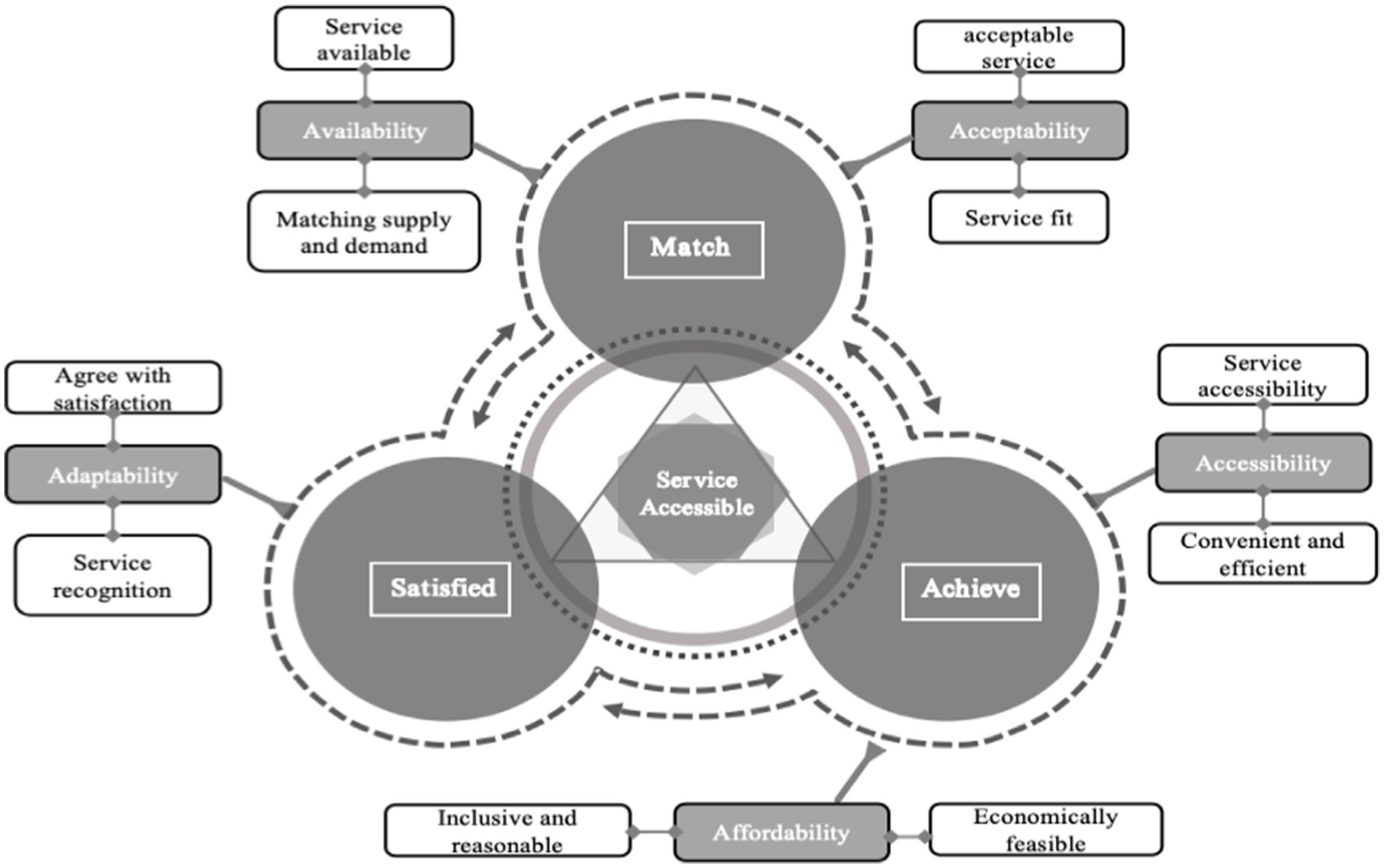
Figure 4. Pathway for improving the accessibility of BECS in urban communities.
The validation in Xi’an confirms the framework’s effectiveness in assessing and enhancing the accessibility of basic older adult care services. While spatial accessibility is strong (3.8815), affordability and psychological care remain key challenges, requiring targeted policy actions. To improve affordability, expanding financial support, such as subsidies for low-income older adult individuals and creating a long-term care security system, is essential. To address service adaptability, digital platforms like “Internet + Older adult Care” should be developed to integrate home-based care, telemedicine, and community mental health services, improving resource allocation and service efficiency. Strengthening home and community care, through home adaptations and family doctor services, will enhance the synergy between family and professional care.
In the long term, building a robust basic older adult care system must support equitable public services. By reducing accessibility and affordability gaps, governments can facilitate the transition from basic care to higher-quality, personalized services, promoting fairness and improving the well-being of older adult individuals in urban environments.
This study has certain limitations. First, the empirical analysis is confined to Xi’an City, which may restrict the generalizability of the findings. Future research should expand to additional cities or regions and conduct comparative analyses to validate the framework’s broader applicability. Second, the study primarily uses quantitative methods, lacking an in-depth exploration of the older adult’s subjective experiences and emotional needs. Future research could address this gap by incorporating qualitative methods to capture the psychological experiences and satisfaction evaluations of older adult individuals. Lastly, with the accelerating integration of artificial intelligence and digital platforms into older adult care, future research should explore their applications in service delivery and accessibility assessments, providing insights for developing older adult care systems in the new era.
This study introduces a novel framework for evaluating the accessibility of basic older adult care services (BECS), addressing critical dimensions such as availability, affordability, adaptability, and acceptability. Grounded in the “5A” theory, the framework was empirically validated in Xi’an, China, and revealed significant disparities in affordability and psychological care services, alongside strong performance in spatial accessibility. These findings underscore the urgent need for targeted policy interventions to address resource imbalances.
The proposed “Matching-Realization-Satisfaction” pathway provides targeted strategies, including demand–supply alignment and innovative service models, to enhance BECS accessibility. By leveraging dynamic demand–supply alignment, integrated funding mechanisms, and innovative service delivery models.
Despite its contributions, this study is limited by its focus on Xi’an City and its primary use of quantitative methods, which may not fully capture subjective experiences. Future research should expand the framework’s application to diverse urban contexts and incorporate qualitative approaches to capture the subjective experiences of older adult individuals. Additionally, exploring the integration of artificial intelligence and digital platforms in service delivery could further enhance the framework’s adaptability in the digital age.
This study advances the theoretical and practical understanding of older adult care accessibility, providing a scalable and adaptable framework to inform policy development and service optimization. By addressing the complex challenges of affordability, psychological care, and responsiveness, it contributes to building equitable and sustainable older adult care systems globally.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Participants provided their written informed consent to participate in this study in accordance with the national legislation and the institutional requirements.
YZ: Conceptualization, Data curation, Methodology, Resources, Writing – original draft, Writing – review & editing. MZ: Writing – review & editing. JH: Investigation, Resources, Validation, Writing – review & editing. RW: Conceptualization, Investigation, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1535987/full#supplementary-material
1. Bengtson, VL. Is the “contract across generations” changing? Effects of population aging on obligations and expectations across age groups In: VL Bengtson and WA Achenbaum, editors. The changing contract across generations. New York: Routledge (2024). 3–23.
2. Zhang, B, Ma, Q, and Fang, Y. Experiences of developed countries in promoting healthy aging and their implications for China. Med Soc. (2024) 37:1–6. doi: 10.13723/j.yxysh.2024.07.001
3. Zhu, Y, Zhu, Q, Ma, Y, Chen, S, Meng, H, and Zubair, M. Identify travel and health factors influencing well-being of the older adults–a case study in China. Front Public Health. (2023) 11:1213499. doi: 10.3389/fpubh.2023.1213499
4. Bar-Tur, L. Fostering well-being in the elderly: translating theories on positive aging to practical approaches. Front Med. (2021) 8:517226. doi: 10.3389/fmed.2021.517226
5. National Bureau of Statistics of China. (2024). Statistical Communiqué of the people’s republic of China on the 2023 National Economic and social development [EB/OL]. Available at: https://www.gov.cn/lianbo/bumen/202402/content_6934935.htm (Accessed April 15, 2024).
6. Pan, L, Sun, J, and Zhou, R. Research on the construction of age-friendly communities based on the fuzzy comprehensive evaluation model: evidence from communities in Hefei, China. Risk Manag Healthc Policy. (2021) 14:3841–52. doi: 10.2147/RMHP.S324109
7. Jing, T, Zhao, X, Xing, H, Bao, C, and Zhan, L. The influence of strong social ties on the choice of long-term care model for middle-aged and older adults in China. Front Public Health. (2023) 11:1112422. doi: 10.3389/fpubh.2023.1112422
8. Wang, J, Zhang, L, Wang, S, and Zhang, L. Living arrangements, health lifestyles, and health outcomes among Chinese oldest-old[J]. Front Public Health. (2023) 11:1235768. doi: 10.3389/fpubh.2023.1235768
9. Hu, J, Zhang, Y, Wang, L, and Shi, V. An evaluation index system of basic elderly care services based on the perspective of accessibility. Int J Environ Res Public Health. (2022) 19:4256. doi: 10.3390/ijerph19074256
10. Du, P. China's aging society for 20 years: Achievements, challenges, and prospects. Beijing, China: People’s Publishing House (2021).
11. Guo, Y. From “providing for the aged” to “caring well for the aged”: the construction and improvement of the basic elderly care service system. People’s Forum. (2024) 16:70–2.
12. Sun, H. Enhancing balance and accessibility: building a socialist modernized public service system. Theor Explor. (2023) 2:111–8. doi: 10.16354/j.cnki.23-1013/d.2023.02.014
13. Yang, B, and Li, W. Accessibility differences in community elderly care services: an empirical analysis based on the integrated framework of “institution-network-culture. Chin Pub Adm. (2024) 40:54–64. doi: 10.19735/j.issn.1006-0863.2024.02.06
14. Dai, J. Research on the concept, measurement, and influencing factors of accessibility: a literature review. Study Pract. (2017) 4:86–94. doi: 10.19624/j.cnki.cn42-1005/c.2017.04.011
15. Andersen, R. A behavioral model of families’ use of health services. Chicago: Center for Health Administration Studies, University of Chicago (1968).
16. Penchansky, R, and Thomas, JW. The concept of access: definition and relationship to consumer satisfaction. Med Care. (1981) 19:127–40. doi: 10.1097/00005650-198102000-00001
17. Tomasevski, K. (2022), Preliminary report of the special rap⁃porteur on the right to education [EB/OL]. Available at: http://daccess-dds-ny.un.org/doc/UNDOC/GEN/G99/101/34/PDF/G9910134.pdf?OpenElement. (Accessed March 21, 2024).
18. Thomas, JW, and Penchansky, R. Relating satisfaction with access to utilization of services. Med Care. (1984) 22:553–68. doi: 10.1097/00005650-198406000-00006
19. Wang, Z, Yong, L, and Wang, L. Evaluation of the accessibility of community services for home-based elderly care: based on a survey in Suzhou. Popul Develop. (2016) 22:90–9.
20. Wang, F, and Bai, W. Research on the accessibility of basic elderly Care Services in Rural Areas: based on survey data from 17 prefecture-level cities in Shandong Province. Popul Econ. (2017) 4:54–62.
21. Wang, Z, He, B, and Yong, L. The analysis framework and empirical exploration of the equalization of home care community services in China: based on the research of Beijing, Nanjing and Xianyang. Sci Decis Mak. (2020) 7:49–69.
22. Han, X, and Xu, Y. Construction and empirical testing of an accessibility evaluation index system for home-based elderly Care Services in Changchun Driven by data. Chin J Gerontol. (2023) 43:4058–62.
23. Yong, L, Wang, Z, and Zhang, D. Accessibility of home-based elderly care community services: conceptual model, index system, and comprehensive evaluation. Popul Econ. (2018) 4:1–11.
24. Lund, BD. Review of the Delphi method in library and information science research. J Doc. (2020) 76:929–60. doi: 10.1108/JD-09-2019-0178
25. Zhu, Y, Tian, D, and Yan, F. Effectiveness of entropy weight method in decision-making. Math Probl Eng. (2020) 2020:1–5. doi: 10.1155/2020/3564835
26. Zhu, L. Research and application of AHP-fuzzy comprehensive evaluation model. Evol Intel. (2022) 15:2403–9. doi: 10.1007/s12065-020-00415-7
27. Xi’an Municipal Bureau of Statistics. (2024). Municipal Bureau of Statistics. Available at: http://xalgb.gov.cn/info/1004/15290.htm (Accessed June 02, 2024).
28. Wu, M. Questionnaire statistical analysis practice. Chongqing: Chongqing University Press (2010).
29. Skulmoski, GJ, Hartman, FT, and Krahn, J. The Delphi method for graduate research. J Inf Technol Educ Res. (2007) 6:001–21. doi: 10.28945/199
30. Bloom, DE, Canning, D, and Lubet, A. Global population aging: facts, challenges, solutions & perspectives. Daedalus. (2015) 144:80–92. doi: 10.1162/DAED_a_00332
31. Wu, HC, and Tseng, MH. Evaluating disparities in elderly community care resources: using a geographic accessibility and inequality index. Int J Environ Res Public Health. (2018) 15:1353. doi: 10.3390/ijerph15071353
Keywords: accessibility, basic older adult care, urban community, evaluation framework, service equity
Citation: Zhang Y, Zhou M, Hu J and Wang R (2025) Bridging accessibility gaps in urban community-based basic older adult care: a comprehensive framework validated in Xi’an, China. Front. Public Health. 13:1535987. doi: 10.3389/fpubh.2025.1535987
Edited by:
Matthew Lee Smith, Texas A&M University, United StatesReviewed by:
Sarah Dys, Portland State University, United StatesCopyright © 2025 Zhang, Zhou, Hu and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yuyuan Zhang, emhhbmd5dXl1YW55eUAxNjMuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.