
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Public Health, 12 February 2025
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1517213
This article is part of the Research TopicChallenges in reaching the UNAIDS 95-95-95 targets in Sub-Saharan Africa: Status, innovations, and pathways forwardView all 8 articles
 Yannick F. Ngoume1
Yannick F. Ngoume1 Urmes C. Teagho1
Urmes C. Teagho1 Brice Eselacha2
Brice Eselacha2 Oumarou H. Goni1
Oumarou H. Goni1 Dell-Dylan Kenfack1
Dell-Dylan Kenfack1 Mérimé Tchakoute3
Mérimé Tchakoute3 Georges Nguefack-Tsague4*†
Georges Nguefack-Tsague4*† Marcel Tongo1,5*†
Marcel Tongo1,5*†Introduction: To achieve the UNAIDS 95-95-95 target by 2025, it is of great importance to test and diagnose individuals infected with HIV; especially those residing in communities with limited access to health and in areas with a longstanding HIV epidemic, where the virus has been circulating since the early phase of the pandemic. In this regard, we determined the HIV prevalence in remote communities of the East and South administrative regions of Cameroon where the four cross-species SIV transmissions that gave rise to the four HIV-1 groups likely happened.
Methods: We did this in two different periods: 2012/2013 (Period 1; 4,435 participants enrolled in the East and 2,347 in the South) and 2021/2022 (Period 2; 2,203 participant enrolled in the East and 2,347 in the South) using HIV1/2 rapid assays and standard ELISAs and according to the WHO testing strategy.
Results: During Period 1, the HIV seroprevalence in the East was 6.9%. This prevalence had significantly decreased to 2.7% [Prevalence Difference or PD: 4.1 (3.1; 5.2); p < 0.001] by Period 2. Contrasting with these results, the HIV prevalence in the South during Period 1 was 5.5% and did not significantly change by Period 2 at 5.2% [PD: 0.3 (1.07;1.6); p = 0.67].
Conclusion: Our data suggest that HIV transmission in remote communities of the South administrative region of Cameroon has likely remained uncurbed over the past decade. As a result, this region should be prioritized in efforts to curb the spread of HIV and reduce its prevalence.
The scaling-up of antiretroviral therapy (ART) in Cameroon, as with most countries in Africa, has likely contributed to the decline of the national prevalence of HIV-1. Yet the prevalence of circulating viruses in the country remains heterogeneously distributed within different Cameroonian communities. In 2018, Cameroon’s 2.7% HIV prevalence was amongst the highest in West-Central Africa (1). The Cameroonian HIV epidemic varies greatly across the country with the Adamawa and South administrative regions having the highest estimated prevalence (6 and 6.9% respectively) and the North-West region the lowest (2.1%) (2). According to UNAIDS, there were 14,000 new infections from all ages in the country and prevalence of HIV among young women and men was below 2% (3). In 2020, UNAIDS set a new ambitious target of 95–95–95 to help end the AIDS epidemic, whereby, by 2025, we should have diagnosed, treated and suppressed the viral loads in 95% of people living with HIV. Despite the tremendous gains that this program has achieved, we are still far from ending the epidemic. Diagnostic challenges and inequalities in treatment coverage are the most significant obstacle to achieving this target (4).
There are four groups of HIV-1 (group M, N, O and P), each originated from a cross-species transmission from chimpanzee or gorilla into human; and these events likely happened in locations that encompassed the East and South administrative regions of Cameroon (5). While three of these events resulted in limited spread within humans, one transfer gave rise to HIV-1 group M (HIV-1M) which is today responsible for the global pandemic (5). As a consequence of this, Cameroon has one of the most genetically diverse HIV epidemics in the world. Numerous different subtypes, circulating recombinant forms (CRFs), and unique recombinant forms (URFs) and other difficult to classify genetic variants in both urban and rural areas are found in the country (4). Furthermore, characterising viruses from these two administrative regions in Cameroon, has suggested that contemporary descendants of lineages present in the early phase of the pandemic are still circulating (6–8). This further supports the hypothesis that the epidemic in these two regions is likely among the oldest and most mature globally.
One key element of the strategy to eradicate AIDS is to test and diagnose individuals infected with HIV; especially in key populations and communities with limited access to healthcare systems, such as those residing in the equatorial rain forests of Cameroon where the virus has been circulating since it first jumped into humans during the early 20th century. Besides the low-resolution epidemiological data that has been used to identify wide geographical variations in HIV prevalence in urban settings, the actual seroprevalence of HIV across communities in rural equatorial rain forest regions of Cameroon are still unknown. Such information will be useful in the development of targeted control programs in these areas.
We conducted two health campaigns in 2012/2013 and in 2021/2022, in remote communities of the East and South administrative regions of Cameroon where reservoirs of all the major HIV-1 groups were found (groups M, N, and O in the East and group P in the South; Figure 1). The timepoints were informed by the national policy guidelines. The country implemented the ‘universal test and treat’ policy in 2016, to enhance progress towards the 95-95-95 global targets to end the epidemic by 2030 (9, 10). These campaigns were focused on general health issues (sexually transmitted diseases, high blood pressure, malaria, and food safety) and included voluntary HIV testing. Inclusion criteria comprised individuals with no obvious comorbidities above the age of 18 years willing to know their HIV status (i.e., the exclusion criteria involved any individuals with obvious comorbidities, who were unwilling to know their HIV status and/or who were under the age of 18 years). The health campaign began with a door-to-door awareness phase in each village, done by local health community workers. This phase lasted for about 5 days. Then, a mobile clinic was set up in a public place of the village for the next 2 days. Healthy individuals willing to know their HIV status were enrolled in the study. While the first campaign was entirely anonymous, demographic and behavioral information via a face-to-face interview using a structured questionnaire was collected in the second campaign. During the two campaigns, the procedure included a pre- and post-counseling as required by national Cameroonian guidelines (11). Blood was collected after the pre-counseling for HIV testing. Surveys were conducted in conjunction with local public health personnel who also ensured that individuals diagnosed with HIV were referred to the nearest healthcare centre for access to antiretroviral treatment according to national guidelines and procedures (11). Five ml of blood was drawn from all participants for HIV testing.
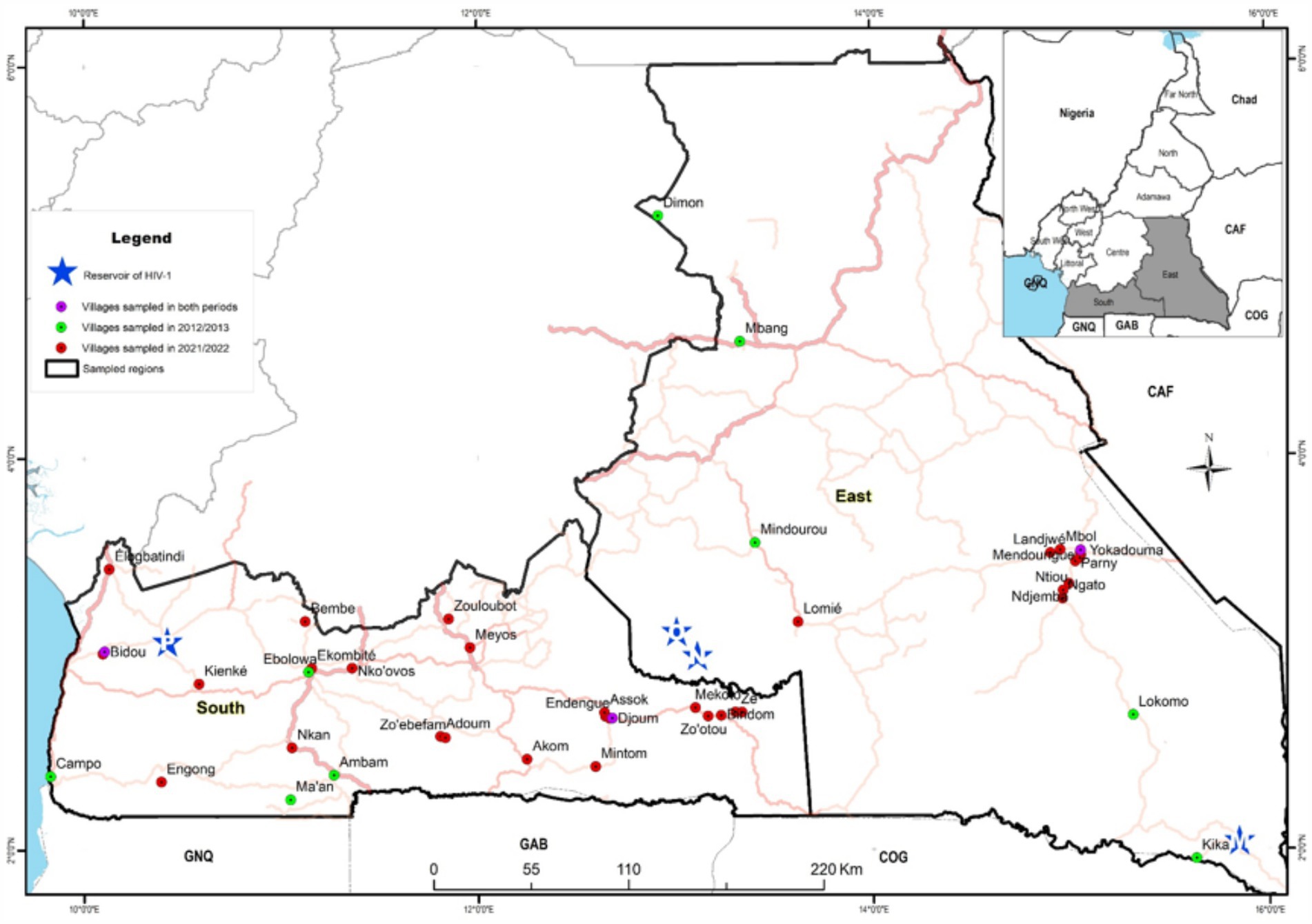
Figure 1. Map of the two equatorial rain forest regions of Cameroon illustrating the sites where samples were collected: red circles represent villages sampled in 2021/2022; green circles represent villages sampled in 2012/2013 and pink circles, villages sampled in the two periods. Blue stars represent the sites where HIV-1 group M (M), group N (N), group O (O) and group P (P) reservoirs were identified.
In the initial survey, serologic screening for HIV infection was conducted on-site using two point-of-care rapid tests that detect HIV antibodies (IgG, IgM, and IgA). The Abbott Determine HIV-1/2 rapid assay (Abbott, Wiesbaden, Germany) was used to pre-screen samples, with non-reactive results considered HIV-negative. Reactive samples (potentially HIV-positive) were then retested using the INSTI HIV-1/HIV-2 antibody test (BioLytical Laboratories, Richmond, Canada). Samples that tested positive on both assays were classified as HIV-positive. Discordant results (reactive on the first test but non-reactive on the second) were retested, and if the result remained the same, the participant was deemed “indeterminate” and advised to retest at a local health center after 1 month, while refraining from any risky behaviour. Data from participants with indeterminate results were excluded from further analysis (Figure 2).
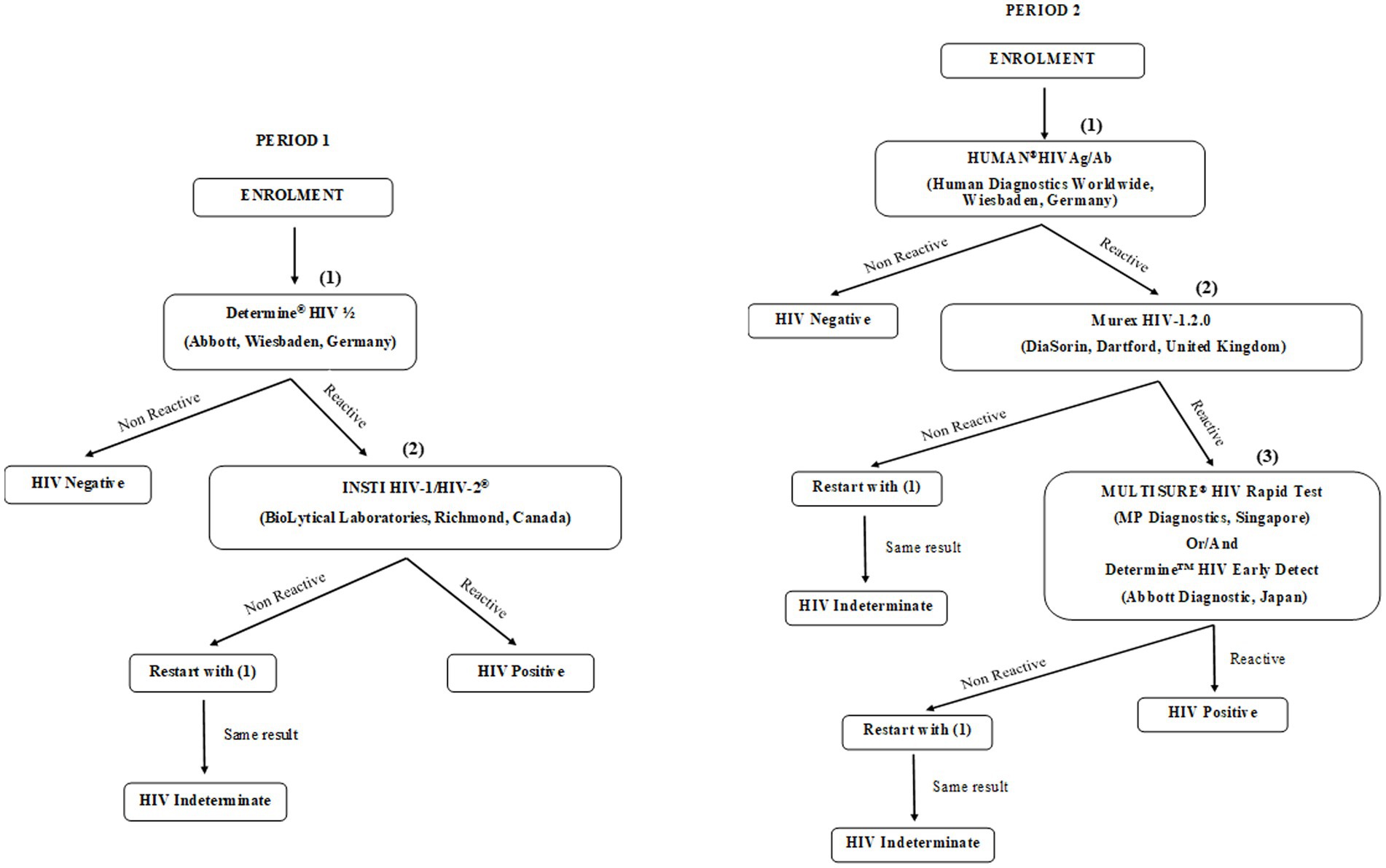
Figure 2. Flow diagram detailing the HIV testing strategy.
In the second campaign, blood samples were transported to a specialized HIV-testing laboratory, where they were tested for HIV antibodies. Four different tests were conducted: two ELISA tests, the HUMAN®HIVAg/Ab (HUMAN Diagnostics Worldwide, Wiesbaden, Germany) and the Murex HIV-1.2.0 ELISA (DiaSorin, Dartford, United Kingdom), along with two rapid tests, the Determine™ HIV Early Detect (Abbott Diagnostic Medical Co. Ltd., Matsudo, Japan) and the MULTISURE® HIV Rapid Test (MP Diagnostics, Asia Pacific, Singapore). Plasma samples that were reactive in at least three of the tests were classified as HIV-positive. During Period 1, screening for HIV antibodies resulted in 378 “indeterminate” cases, while in Period 2, there were 41 “indeterminate” results. These indeterminate cases were excluded from further analysis (Figure 2).
Data were analysed using STATA version 18. Frequencies and percentages (%) were used to describe qualitative variables. Pearson’s Chi-square test was used to establish relationships between qualitative variables. Associations were further quantified using unadjusted prevalence ratio (PR) and prevalence difference (PD) for univariable (bivariate) analysis and adjusted prevalence ratio (aPR) and adjusted prevalence difference (aPD) for multiple Poisson regression analysis (with interactions) with 95% confidence interval (CI), as recommended by Barros and Hirakata (12). Variables used for adjustment included administrative region and its interaction with the sampling period. Variables with p-values less than 0.05 were considered statistically significant.
The study was approved by the National Ethics Committee of the Cameroonian Ministry of Health (N° 2022/12/1510/CE/CNERSH/SP).
We visited six villages in 2012/2013 (Period 1) both in the East and South administrative regions of Cameroon; during this period, 4,425 participants were enrolled in the East, and 2,347 participants in the South. In the second health campaign performed in 2021/2022 (Period 2), we visited 11 villages in the East and 22 in the South, respectively, enrolling 2,203 and 2,062 participants. Only three villages were visited during both surveys: Djoum and Bidou in the South region and Yokadouma Rural in the East. Villages were selected based on the known acceptability of campaigns to their inhabitants and the availability of local staff.
While no socio-demographic data were available during Period 1, a total of 3,510 (1,687 in the East and 1,823 in the South) participants disclosed their sex information during Period 2; among them, 38% were female and 62% male. Across the region, these proportions were similar. The mean age was 36 years; greater in the South (40 years) than in the East (32 years). Table 1 summarises other socio-demographic data including marital status, education level, history of HIV testing and sexually transmitted diseases; overall these data were similar between the two regions.
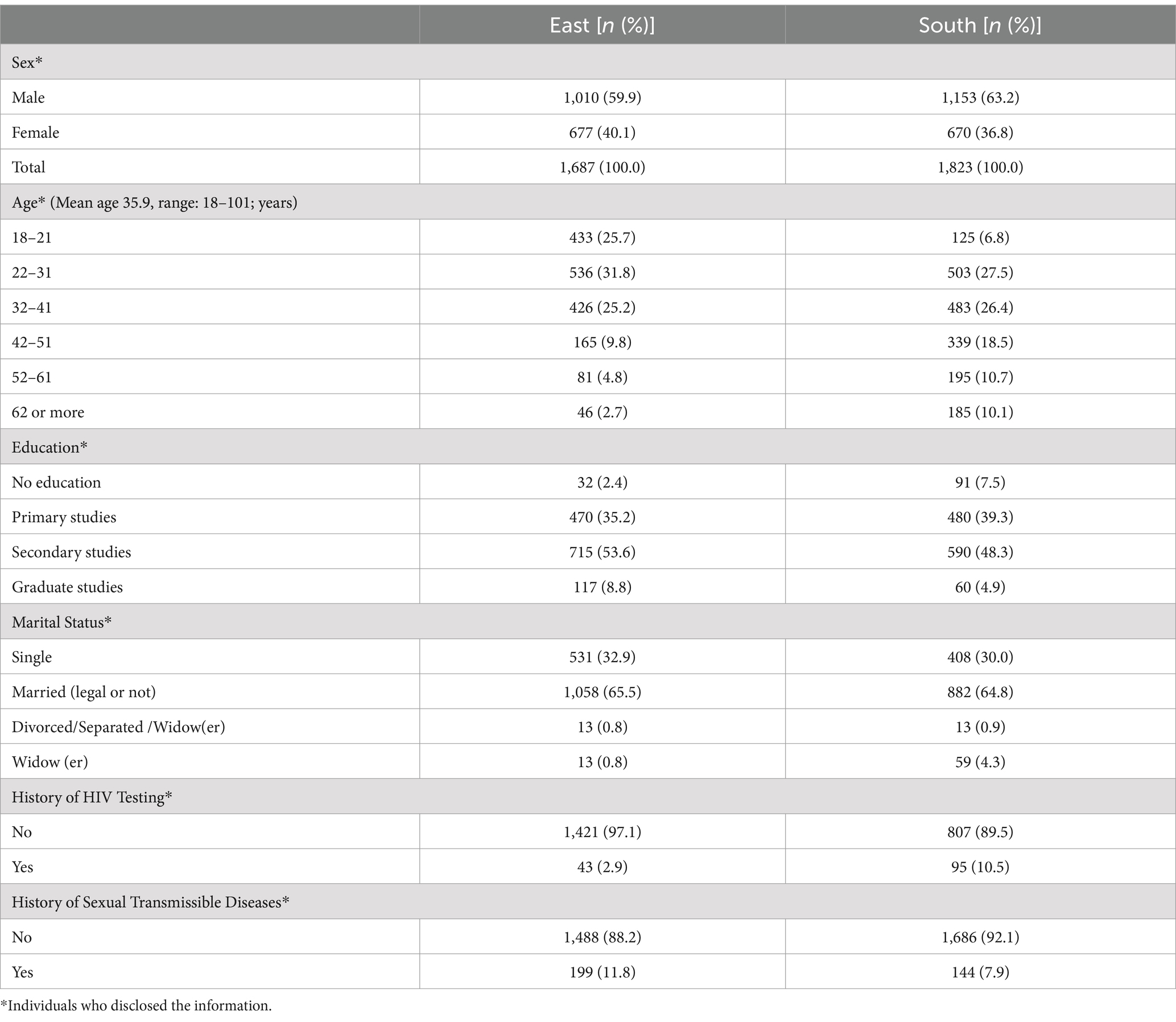
Table 1. Characteristics of study individuals.
The multivariate Poisson model (Table 2) using period, region, and their interactions showed that, in terms of HIV prevalence, there was a significant interaction between geographical region and sampling period (adjusted Prevalence Ratio or aPR: 2.4 (1.6; 3.5); p < 0.001 and adjusted Prevalence Difference or aPD: 0.88 (0.5;1.3); p < 0.001). In addition, HIV prevalence showed significant (p < 0.001) disparities by region (aPR: 0.5 (0.38; 0.71); p < 0.001 and aDR: −0.7 (−1.0; −0.3); p < 0.001). This significant interaction implies that results should not be combined and must be presented per region.
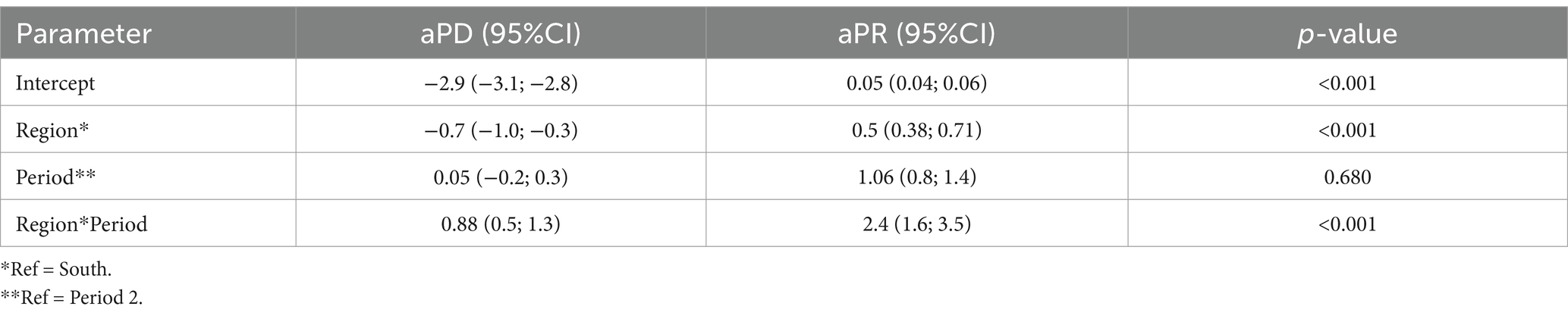
Table 2. adjusted Prevalence Ratio (aPR) and adjusted Prevalence Difference (aPD) for multiple Poisson regression analysis (with interactions).
The stratified analysis (Table 3) reveals a decrease in HIV prevalence in the East between the two study periods, while the prevalence remained unchanged in the South. Specifically, during Period 1, 290 out of 4,223 samples from the East tested HIV-positive, resulting in a seroprevalence of 6.9%. This prevalence had significantly decreased to 2.7% [Prevalence Difference or PD: 4.1 (3.1; 5.2); p < 0.001] by Period 2 (Figure 3; Table 3). In contrast, 120 out of 2,171 samples from the South tested HIV-positive during Period 1, resulting in a prevalence of 5.5%. This prevalence remained relatively unchanged by Period 2, with a slight decrease to 5.2% [PD: 0.3 (1.07; 1.6); p = 0.67] (Figure 3; Table 3). Trends of HIV prevalence in the three communities that were visited during both the Period 1 and Period 2 campaigns revealed that the prevalence remained unchanged in Bidou (South) at 3.7% for both periods; while non significantly decreased in Djoum (South) from 5.3 to 4.0% (p = 0.34). A significant decline of the prevalence was observed in Yokadouma Rural (East) from 7.6% in Period 1 to 2.2% in Period 2 (p < 0.001).
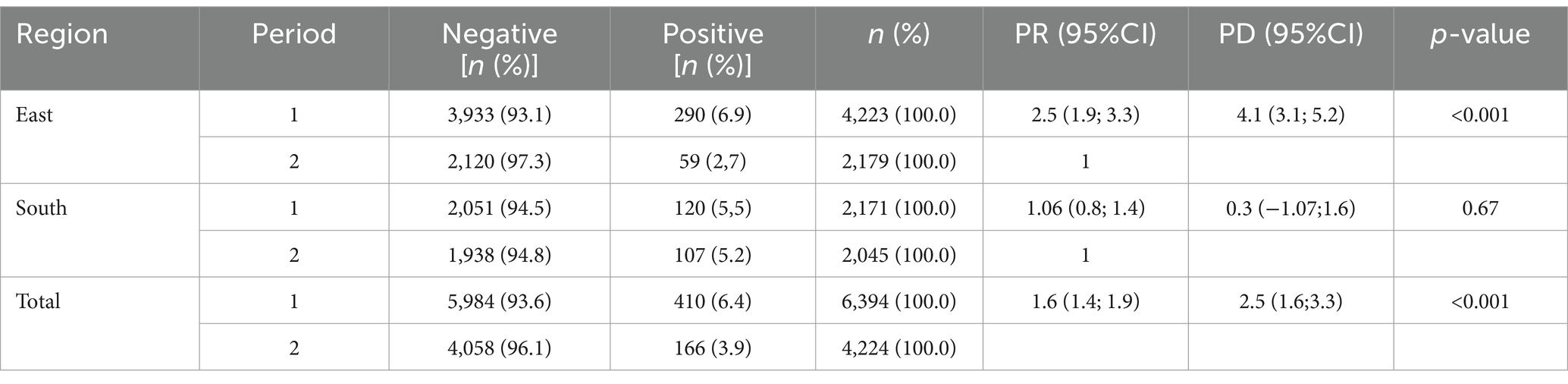
Table 3. Stratified HIV prevalence per region and sampling period.
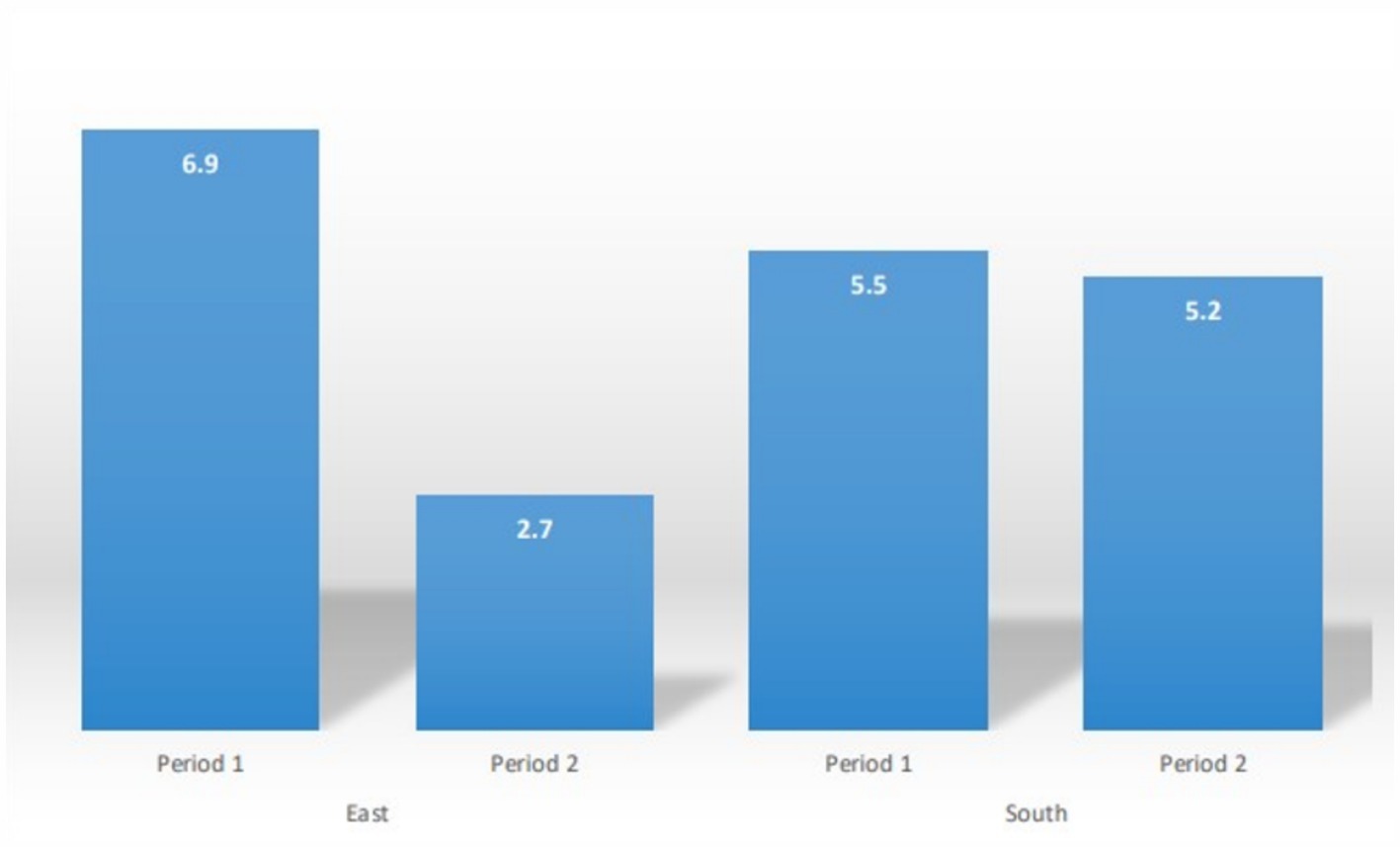
Figure 3. HIV Prevalence (%) per period and by region.
The current analysis highlights differences in HIV infection trends over the decade from 2012 to 2022 in remote communities across two administrative regions of the equatorial rainforest in Cameroon, a country where HIV-1M has likely been circulating since the onset of the global HIV-1M pandemic. Our findings reveal a significant decline in HIV prevalence in the East, from 6.9 to 2.7%, over this period. In contrast, no similar decline was observed in the South, where the prevalence remained stable at around 5%.
Previous studies have also examined HIV prevalence in remote areas of the equatorial forest in Cameroon. In 2000, Nyambi and colleagues conducted a survey in locations including both the East and South regions of the country (13). They reported an HIV prevalence of 4.5% in the South and 6.9% in the East, which closely aligns with the data we obtained during Period 1. In a similar study, Edoul and collaborators investigated the prevalence of circulating HIV in three remote villages of Cameroon including two in the East and one in the South during the years 2011–2013 (14). They found that HIV was circulating at a prevalence of 9% in Moloundou/Mambele and 7% in Messok in the East (that gave an average of 8%); and 5.4% in Bipindi in the South (14). The main observation from these data and the present work is that, HIV prevalence in the South region of Cameroon has been stable over time at around 5%. While it is difficult to determine why the prevalence stays high within communities in the South despite widespread ARV used, several factors can be speculated.
The South administrative region of Cameroon has one of the best road networks in the country, connecting it more thoroughly to both other parts of the country, and neighbouring countries (Gabon, Equatorial Guinea and Republic of Congo) than do the road networks of the East administrative region. The higher connectivity of the South relative to the East is expected to favour a greater degree of mixing of human populations and more migration in the South than in the East: a factor which might contribute to lower barriers to HIV-1 spread in the South than in the East (15).
Another potentially important difference between the two regions is the availability and quality of health services for the management of HIV/AIDS. Specifically when the national AIDS control committee assessed health facilities throughout Cameroon in 2018, health facilities in the South ranked lower on average than those anywhere else in the country (15). Factors assessed that were directly relevant to reducing the prevalence of HIV were the accessibility of HIV testing and counselling, the intensity of efforts directed towards prevention of mother-to-child-transmissions, care and support of people living with HIV, and the provision of laboratory and medication management.
We acknowledge that our study has many limitations, including its restriction to two of the five regions of the equatorial rain forest in the country and all have old and mature HIV epidemics. In addition, the lack of individual socio-epidemiological data especially during Period 1 limits the possible impacts that these data may have had on the observed difference in prevalence and in formulating specific recommendations that might help to significantly reduce HIV prevalence in the studied regions.
In conclusion, our data indicate that HIV-transmission in remote communities of the South administrative region of Cameroon has likely not been curbed over the past decade. The connectivity of this region both to other parts of Cameroon and neighbouring African countries should make this region a priority with respect to containing the spread of HIV and lowering its prevalence. To achieve this though, urgent focused intervention to bolster the quality of HIV-focused healthcare in this region will likely be required; more specifically local authorities should implement and scale-up innovative approaches to HIV testing and provide better linkage to prevention tools and treatment.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by National Ethics Committee of the Cameroonian Ministry of Health (N° 2022/12/1510/CE/CNERSH/SP). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
YN: Data curation, Formal analysis, Investigation, Methodology, Writing – original draft. UT: Methodology, Formal analysis, Writing – review & editing. BE: Formal analysis, Writing – review & editing. OG: Writing – review & editing, Formal analysis. D-DK: Formal analysis, Writing – review & editing. MTc: Supervision, Investigation, Writing – review & editing. GN-T: Conceptualization, Data curation, Formal analysis, Supervision, Writing – original draft. MTo: Conceptualization, Supervision, Writing – original draft, Funding acquisition, Investigation, Methodology, Project administration.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was supported by the Sub-Saharan African Network for TB/HIV Research Excellence (SANTHE) which is funded by the Science for Africa Foundation to the Developing Excellence in Leadership, Training and Science in Africa (DELTAS Africa) programme (Del-22-007) with support from the Wellcome Trust and the UK Foreign, Commonwealth & Development Office. The latter is part of the EDCPT2 programme supported by the European Union; the Bill & Melinda Gates Foundation (INV-033558); and Gilead Sciences Inc., (19275). All content contained within is that of the authors and does not necessarily reflect positions or policies of any SANTHE funder. For the purpose of open access, the author has applied a CC BY public copyright licence to any Author Accepted Manuscript version arising from this submission.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewers KAF and AK declared a shared affiliation with the author MT to the handling editor at the time of review.
The author(s) declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Statistique/INS IN de la, ICF (2020). République du Cameroun Enquête Démographique et de Santé 2018. Published online February 1, 2020. Available at: https://dhsprogram.com/publications/publication-FR360-DHS-Final-Reports.cfm (Accessed October 11, 2024).
2. Bissek, ACZK (2020). Cameroon population-based HIV impact assessment CAMPHIA 2017-2018. Available at: https://stacks.cdc.gov/view/cdc/120052 (Accessed October 11, 2024).
3. GPC (2023). The state of HIV prevention in Cameroon – poster. Available at: https://hivpreventioncoalition.unaids.org/en/resources/state-hiv-prevention-cameroon-poster (Accessed January 10, 2025).
4. Frescura, L, Godfrey-Faussett, P, Ali Feizzadeh, A, El-Sadr, W, Syarif, O, Ghys, PD, et al. Achieving the 95 95 95 targets for all: a pathway to ending AIDS. PLoS One. (2022) 17:e0272405. doi: 10.1371/journal.pone.0272405
5. Sharp, PM, and Hahn, BH. Origins of HIV and the AIDS pandemic. Cold Spring Harb Perspect Med. (2011) 1:a006841. doi: 10.1101/cshperspect.a006841
6. Jk, C, Nd, W, Jn, T, et al. HIV-1 recombinants with multiple parental strains in low-prevalence, remote regions of Cameroon: evolutionary relics? Retrovirology. (2010) 7:7. doi: 10.1186/1742-4690-7-39
7. Tongo, M, Dorfman, JR, Abrahams, MR, Mpoudi-Ngole, E, Burgers, WA, and Martin, DP. Near full-length HIV type 1M genomic sequences from Cameroon. Evol Med Public Health. (2015) 2015:254–65. doi: 10.1093/emph/eov022
8. Tongo, M, Martin, DP, and Dorfman, JR. Elucidation of early evolution of HIV-1 group M in the Congo Basin using computational methods. Genes (Basel). (2021) 12:517. doi: 10.3390/genes12040517
9. Drupal (2015). Plan d’Acceleration de la Thérapie ARV au Cameroun (2016-2018). Available at: https://www.childrenandaids.org/Cameroon_Plan-Acceleration-Therapie-ARV_2015 (Accessed January 9, 2025).
10. GPC. (2021). Plan stratégique national de lutte contre le VIH/sida et les IST du Cameroun de 2021-2023. Available at: https://hivpreventioncoalition.unaids.org/fr/resources/cameroon-national-strategic-plan-fight-against-hivaids-and-stis-2021-2023 (Accessed November 21, 2024).
11. Directives_version-finale-05-aout-2021_Cameroon.pdf. (2021). Available at: https://www.differentiatedservicedelivery.org/wp-content/uploads/Directives_version-finale-05-aout-2021_Cameroon.pdf (Accessed January 16, 2025).
12. Barros, AJ, and Hirakata, VN. Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol. (2003) 3:21. doi: 10.1186/1471-2288-3-21
13. Nyambi, P, Zekeng, L, Kenfack, H, Tongo, M, Nanfack, A, Nkombe, I, et al. HIV infection in rural villages of Cameroon. J Acquir Immune Defic Syndr. (1999) 31:506–13. doi: 10.1097/00126334-200212150-00008
14. Edoul, G, Chia, JE, Vidal, N, Guichet, E, Montavon, C, Delaporte, E, et al. High HIV burden and recent transmission chains in rural forest areas in southern Cameroon, where ancestors of HIV-1 have been identified in ape populations. Infect Genet Evol. (2020) 84:104358. doi: 10.1016/j.meegid.2020.104358
15. Bulletin_Epidémiologique_VIH_N°5.pdf (2018). Available at: https://www.childrenandaids.org/sites/default/files/2017-05/Cameroon_National-Integrated-HIV-Guidelines2014.pdf (Accessed January 9, 2025).
Keywords: HIV prevalence, Cameroon, HIV diagnosis, HIV diversity, HIV infection
Citation: Ngoume YF, Teagho UC, Eselacha B, Goni OH, Kenfack D-D, Tchakoute M, Nguefack-Tsague G and Tongo M (2025) Differences in HIV infection trends in two regions of Cameroon with a longstanding HIV epidemic: insights from 2012 and 2022. Front. Public Health. 13:1517213. doi: 10.3389/fpubh.2025.1517213
Edited by:
Olivier Mukuku, Institut Supérieur des Techniques Médicales de Lubumbashi, Democratic Republic of CongoReviewed by:
Kerri-Lee Ann Francois, University of KwaZulu-Natal, South AfricaCopyright © 2025 Ngoume, Teagho, Eselacha, Goni, Kenfack, Tchakoute, Nguefack-Tsague and Tongo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Georges Nguefack-Tsague, bmd1ZWZhY2t0c2FndWVAZ21haWwuY29t; Marcel Tongo, bWFyY2VsLnRvbmdvQGdtYWlsLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.