 Fang Xue
Fang Xue Jing Liu2†
Jing Liu2† Shuoshuo Li
Shuoshuo Li Jing Zhang
Jing Zhang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 19 February 2025
Sec. Occupational Health and Safety
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1516744
Objective: To investigate burnout, sense of coherence (SOC), and job safety attitudes among nurses in China after the coronavirus disease 2019 (COVID-19) pandemic.
Methods: This cross-sectional study included 302 front-line nurses from Fangcang shelter hospitals (FSHs) in China. Descriptive, univariate, Pearson’s correlation, and multiple linear regression analyses were conducted to analyze factors related to job safety attitudes of nurses toward FSHs.
Results: The incidence of burnout among nurses in FSHs was 65.2%; 57.9% had a low level of SOC, the score for safety attitude was 74.47 (standard deviation = 13.33), and the agreement rate was 51%. Burnout was negatively correlated with SOC (r = −0.399, p < 0.01) and safety attitudes (r = −0.141, p < 0.05), and SOC was positively correlated with safety attitudes (r = 0.428, p < 0.01). Personal accomplishment, depersonalization, changes in working hours, manageability, and marital status explained 33.8% of the variance in work safety attitudes.
Conclusion: This study investigated the levels of burnout, SOC, and safety attitudes among nurses after COVID-19 in Chinese FSHs for the first time, and analyzed the associated factors. The results are valuable for improving the quality of nursing safety as well as patient safety management in FSHs.
The unpredictable behavior of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) and insufficient national responses have contributed to the continued global pandemic of coronavirus disease 2019 (COVID-19). There were more than 633,000,000 confirmed COVID-19 patients and more than 6,596,000 deaths worldwide by November 2022 (1). Global medical and care resources face enormous challenges, and the International Health Regulations Emergency Committee has expressed concerns regarding the heavy workload and associated burnout experienced by healthcare workers worldwide (2). China has adopted active response strategies since the outbreak of COVID-19 in Wuhan. Under the normalized management of the pandemic, China adhered to the general strategy of “external prevention of import, internal prevention of rebound” and the policy of “dynamic COVID-zero” (3), which brought the pandemic under control. The mortality rate and number of severe cases have continued to decline, and Fangcang shelter hospitals (FSHs) have been an important part of the pandemic response.
FSHs are strategies that were implemented for the first time in China to manage COVID-19. These large temporary hospitals expanding and modifying the medical services of existing public facilities in the cities (4). Patients with mild COVID-19 and asymptomatic individuals were treated at FSHs; they not only provide appropriate medical care but also monitor the disease, implement strategic classification, and provide timely transfer of patients with progressive disease to designated hospitals (5), reducing the pressure on traditional hospitals. A certain number of staff members are required to operate an FSH. As the number of infected people has grown rapidly, and there is often a shortage of local medical staff, China has actively mobilized national support through measures such as pulling widespread healthcare staff to help Wuhan, Hong Kong, Shanghai, and other areas. The efforts and dedication of Chinese nurses have been instrumental in the containment of COVID-19 (6).
Nurses are the main forces behind FSHs; they enter these hospitals with protection while working, and live in isolation in a unified living area after work. Although majority of the patients in FSHs have mild cases, nurses also face many challenges such as an increased workload as a result of the large number of patients they have to manage (7), the possibility of infection due to direct contact with confirmed patients (8, 9), and the fear for parents and children due to being away from home (9, 10). Epidemic outbreaks and immense stress have had significant psychological impact on healthcare workers (11). One study (12) found that the proportion of front-line nurses who experienced anxiety, depression, and insomnia was significantly higher during the outbreak and that nurses in FSHs were more likely to experience psychological problems than other front-line nurses during the stable phase of the epidemic. These adverse influences may lead to job burnout among front-line nurses (7, 9). Burnout syndrome is an employee’s emotional response to chronic work stress that manifests as depersonalization and reduced professional efficacy (13). Healthcare workers are at a high risk of burnout (14–16), which is closely related to quality of care and patient safety (11, 14). Sense of coherence (SOC), a core concept of the salutogenic model of health proposed by Antonovsky, is a stable psychological tendency in individuals (17). When people experience stressful events, SOC shapes their overall feelings and perceptions about life, reflecting on their outlook on life and their ability to cope with stress (18). Several studies (19–22) have demonstrated that SOC helps people successfully cope with stressful events. Previous studies (23, 24) have shown that healthcare workers were at a higher risk of psychological problems during SARS and H1N1. When nurses have high levels of SOC, they face difficult situations with a positive mindset, mobilize their resources to cope with stress, and have reduced negative emotions and health risks (25–27). Patient safety has always been a primary goal of global health (28). It is defined as the prevention and avoidance of risk, harm, or adverse events during healthcare delivery (29). Safety culture is the product of the values, attitudes, perceptions, abilities, and behavioral patterns of individuals and groups, which determine the commitment, style, and proficiency of an organization’s health and safety management (30). The safety attitudes of healthcare staff towards patients are an important part of the safety culture of hospitals. As surveys cannot measure all aspects of culture, the safety climate of a healthcare organization should be assessed to determine its strengths and weaknesses (31). The COVID-19 pandemic is not only related to physical health, but also to mental health, sleep problems, depression, burnout and traumatic stress. A systematic evaluation and meta-analysis of 85 studies shows that nurse burnout is negatively correlated with patient safety, patient satisfaction, and nursing quality; Secondly, during the COVID-19 pandemic, the prevalence of nurses’ job burnout was even higher due to hospital overcrowding and understaffing (32).
During the COVID-19 pandemic, the risk to nurses’ mental health increased rapidly. The COVID-19 pandemic is not only related to physical health, but also to mental health, sleep problems, depression, burnout, and traumatic stress. Healthcare workers are at a high risk of burnout, which is closely related to quality of care and patient safety. We conducted a study on the current status and correlation of post-traumatic stress fatigue, coherence, and work safety attitudes among Chinese nurses after COVID-19 in 2019. A literature search revealed that published evidence has focused on determining the level of stress in HCWs in the context of the COVID-19 pandemic. However, there is less research on the relationship between Burnout, Sense of Coherence and Job Safety Attitudes among nurses experiencing frontline work on the outbreak after re-entering the workforce following the New Crown Pneumonia pandemic. Therefore, we were the first to take on the challenge of assessing those factors among nurses. The aim of this study was to investigate the levels of burnout, SOC, and safety attitudes among FSH nurses after the pandemic period of neocoronavirus pneumonia and to analyse the factors related to their attitudes towards safe work. The research results have important reference value for improving the nursing quality and patient safety management of frontline nurses who have experienced FSH during their return to work.
This study used a cross-sectional, descriptive research design and followed the STROBE statement specification for cross-sectional studies (33).
This study was conducted at the Anhui FSH, located on Chongming Island, Shanghai, China. All admitted patients were mildly ill with confirmed COVID-19 and asymptomatic infection, and all nurses providing healthcare services were from the Anhui Province.
In this study, 360 nurses who met these requirements were recruited between May 8 and 15, 2024. Due to the pandemic, the questionnaire was set up online through the Wenjuanxing app1 and distributed through the WeChat platform, which is the most used social networking software in China. All participants anonymously submitted their questionnaires and informed consent forms online. The inclusion criteria were officially registered nurses working in an FSH for 1 month or more who could use their smartphones normally and complete the questionnaire. The exclusion criteria were those who took an overly short time to complete the questionnaire (within 300 s), invalid questionnaires that were not logical, and incomplete or identical responses.
The socio-demographic data collection form was used to collect the personal information from the participants, including gender, age, education status, marital status, if they were an only-child, having children, type of hospital, clinical rank, night shift participation, change in working hours, change in sleep time, experience with the pandemic, experience with negative life events within the last month, and level of concern about the pandemic.
The Maslach Burnout Inventory-Human Services Survey (MBI-HSS) was used to investigate burnout among nurses. The MBI-HSS is applicable to social service workers and is now widely used in burnout studies of healthcare workers (34–37). It has 22 items in three subscales: emotional exhaustion (EE), depersonalization (DP), and personal accomplishment (PA) (38). Each item is evaluated on a 7-point Likert scale ranging from 0 (never) to 6 (every day). The Chinese version of the MBI-HSS was used in the present study. The Cronbach’s α coefficient was previously reported to be 0.737 for the overall scale and 0.858, 0.761, and 0.757 for the subscales, respectively (39). In this study, the total Cronbach’s α coefficient was 0.845, and those of the subscales were 0.894, 0.904, and 0.874, respectively. According to the burnout norms of Chinese nurses (40), the critical value of burnout was determined as follows: EE ≤ 17, DP ≤ 3, and PA ≥ 33 were classified as mild; EE of 18–26, DP of 4–7, and PA of 25–32 were classified as moderate; and EE ≥ 27, DP ≥ 8 and PA ≤ 24 were classified as severe. For the diagnosis of burnout, some studies have used strict criteria to consider high EE, high DP, and low PA (41), while others have used loose criteria to consider high EE with high DP or low PA (42). In this study, with reference to Li’s (43) study on the Chinese population, the diagnostic criteria for burnout were as follows: (1) none: scores on all three subscales were lower than the critical value; (2) mild: scores on one subscale were higher than the critical value; (3) moderate: scores on two subscales were higher than the critical value; and (4) high: scores on all three subscales were higher than the critical value. The most recent version of official manual of MBI recommends not coding burnout as categorical. This study classified coding burnout as categorical mainly based on the odds ratios more interpretable for clinical settings.
The Sense of Coherence Scale (SOC-13), a 13-item scale developed by Antonovsky, was used to measure the SOC of the nurses (17, 44). The scale contains 13 items across three dimensions: comprehensibility, manageability, and meaningfulness. Comprehensibility is a cognitive dimension that represents feelings about stressful internal and external events; a higher score indicates that people consider stressful events to be reasonable and understandable, and that things they understand are easier to manage. Manageability is a behavioral dimension representing the degree to which people think that internal and external resources are at their disposal; a higher score indicated that people thought they had more resources at their disposal, they were more willing to solve problems that caused stress and find meaning in managing stressful events. Meaningfulness is a motivational dimension, representing the degree to which people think life is meaningful; a higher score indicates that people are more willing to devote energy to solving problems and taking responsibility. The SOC-13 is evaluated on a 7-point Likert scale from 1 (never) to 7 (often), with total scale scores ranging from 13 to 91 and higher scores representing higher levels of SOC. A total scale score of 13–63 represents a low level of SOC, 64–79 represents a moderate level, and 80–91 represents a high level (45). The Chinese version of the SOC-13 was used in this study, with a Cronbach’s alpha coefficient of 0.76 (46, 47). In this study, the overall Cronbach’s alpha coefficient was 0.887.
The Safety Attitude Questionnaire (SAQ) developed by Sexton et al. (30) was used to assess nurses’ perceptions of safety attitudes in their work environments (30). The generic SAQ Short-Form version contains 36 items across six dimensions: teamwork climate, safety climate, perceptions of management, job satisfaction, working conditions, and stress recognition. Each item is evaluated on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). To facilitate interpretation of the scores, the 5-point scale is converted to a 100-point scale (48, 49): scale score for a respondent = [(Mean of the items) − 1] * 25 with ≤ 50 indicating a need for improvement, and ≥ 75 indicating a positive attitude towards safety. A representative response rate of at least 60% is considered a satisfactory level of safety culture (50). The Chinese version of the SAQ (51) was used in this study, with a total Cronbach’s α coefficient of 0.945; the subscales have Cronbach’s α coefficients of 0.785–0.899. The overall Cronbach’s alpha in this study was 0.926, and the Cronbach’s alpha for the subscales were 0.749–0.914.
The study size was calculated according to the formula
SPSS software version 25.0 (SPSS-IBM Corporation, New York, NY, United States) was used for statistical analysis. Descriptive analyses were performed using means, standard deviations, frequencies, and percentages. P-P and Q-Q plots are used to evaluate the normality of data. Univariate analysis uses significance level defined as two-sided p < 0.05 by t-test and analysis of variance. A Pearson’s correlation analysis was performed for the scales and each dimension. Statistically significant factors (p < 0.05) were included as independent variables and SAQ scores were used as dependent variables in a multiple linear regression analysis (stepwise) to analyze the factors that influenced the safety attitudes of nurses toward FSHs. A collinearity diagnosis was made before the analysis to ensure that there was no collinearity between variables.
This study was approved by the Ethics Committee of the First Affiliated Hospital of Bengbu Medical College (approval number: BYYFY-2020KY01). Subjects were informed of the purpose, completion method, and precautions of the questionnaire in advance and the questionnaire was completed online after consent was obtained. The questionnaire was distributed in the WeChat group in the form of a QR code, and only those who voluntarily wished to complete the survey could scan the code and select “agree” to complete the questionnaire. If a participant wanted to terminate the survey at any time process, they could simply exit the interface. All questionnaires were completed anonymously, and the data were stored safely and used only for this study.
All participants were invited to participate in the survey when the QR codes were distributed in the WeChat group. A total of 360 questionnaires were distributed and 302 valid questionnaires were returned (return rate: 83.89%) (Figure 1). The researcher examined each returned questionnaire and excluded invalid questionnaires, including those that did not indicate agreement to participate (n = 27), were completed in an overly short time (n = 16), were illogical (n = 6), or were answered with the same response (n = 9). We set the questionnaire items as mandatory; if the participants missed items, the software automatically reminded them to complete these before they could submit the questionnaire to minimize possible bias in the self-reported results.
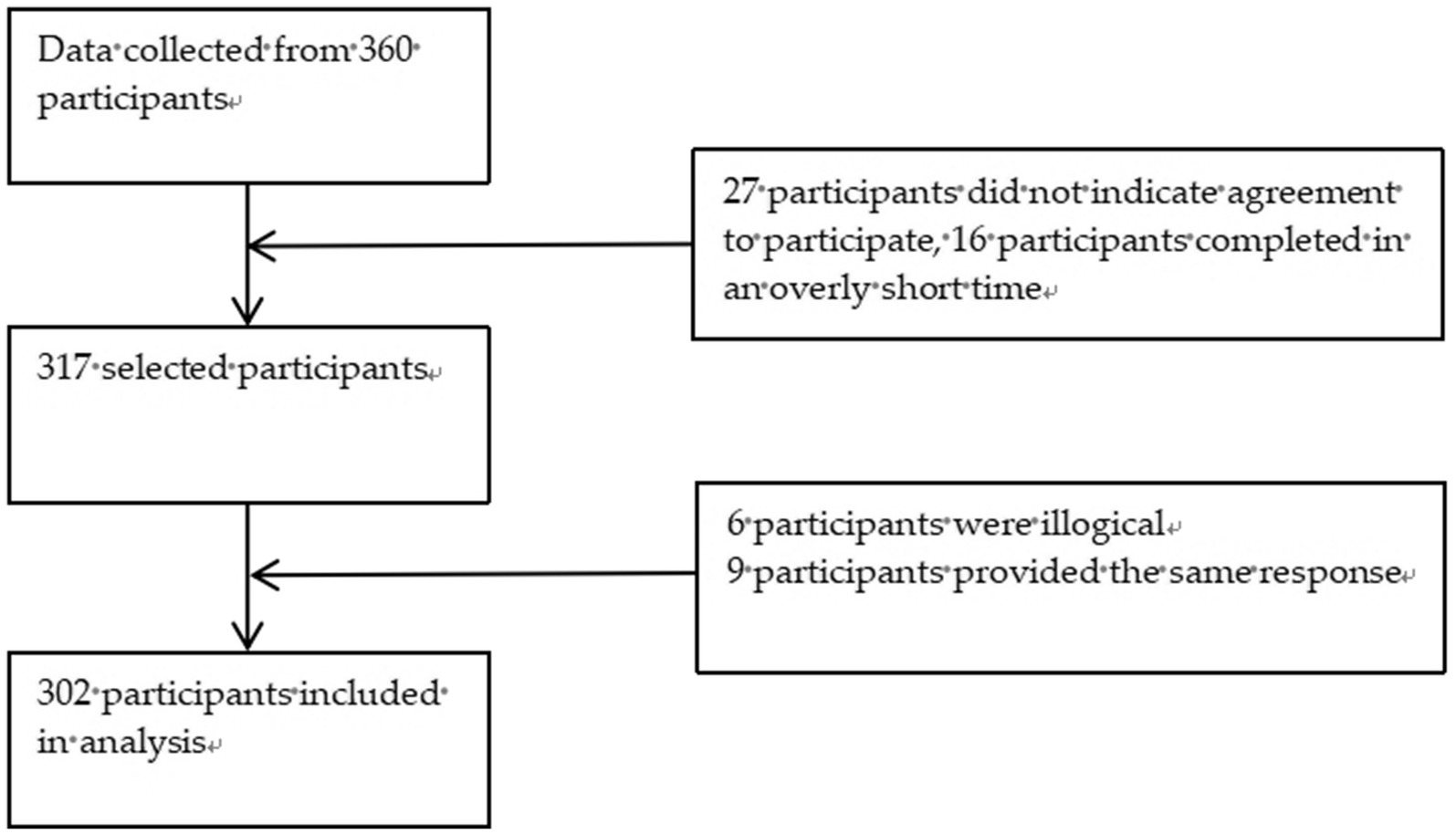
Figure 1. Flow chart for participants’ inclusion.
Of the 302 participants, 89.7% were female, 77.5% had a bachelor’s degree, 63.3% were married, 18.2% were only child, and 61.9% had children. The sociodemographic and work characteristics of the nurses are described in Table 1.
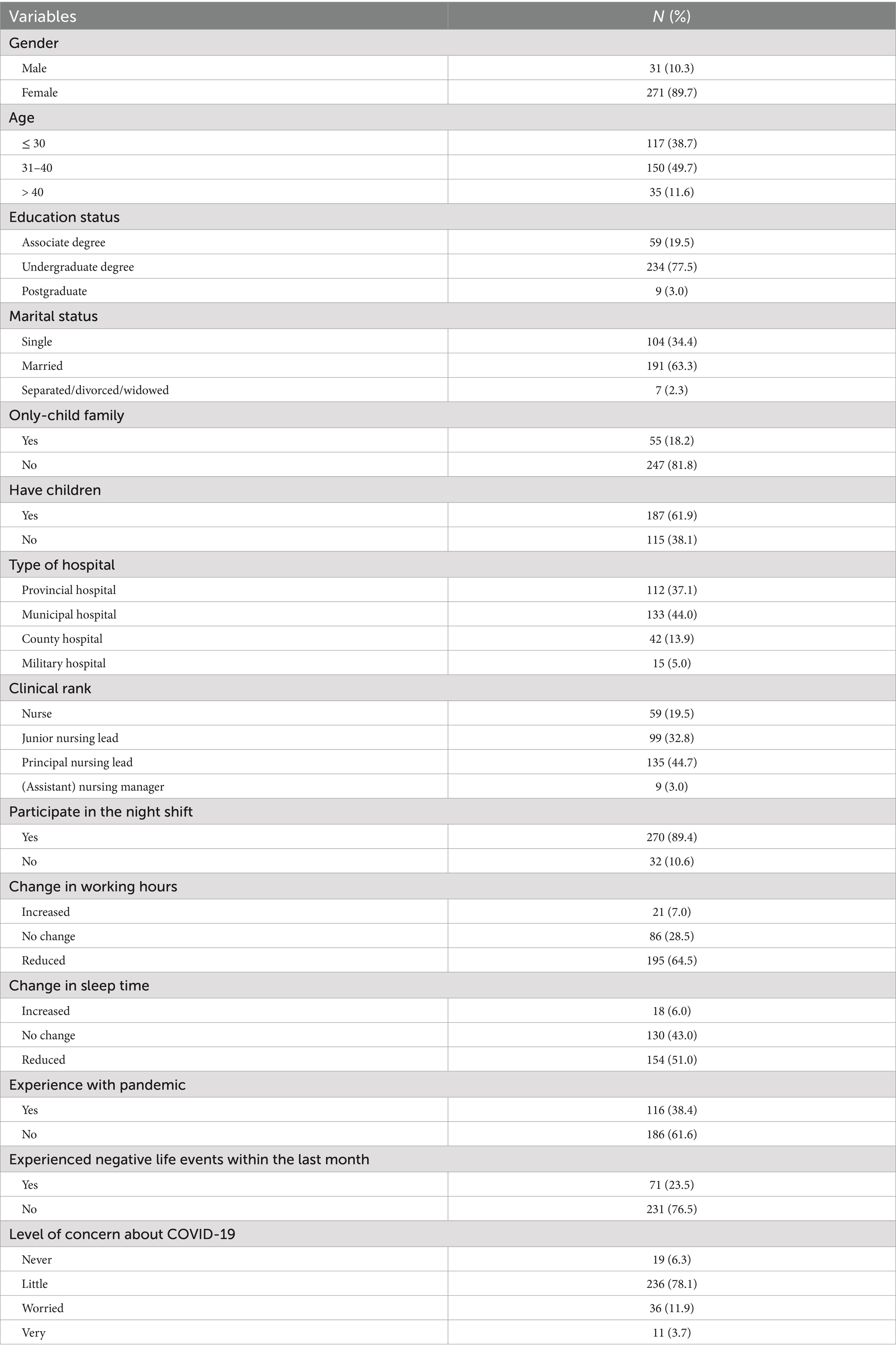
Table 1. Sociodemographic and work characteristics variables (N = 302).
The average score of burnout among nurses in FSHs was 65.41 [standard deviation (SD) = 15.92], with an incidence of 65.2% (Table 2). The SOC score was 61.13 (SD = 13.00), with 57.9% at a low level. Table 3 shows that the average job safety attitude score of nurses was 74.47 (SD = 13.33), with a percentage agreement rate of 51.0%.
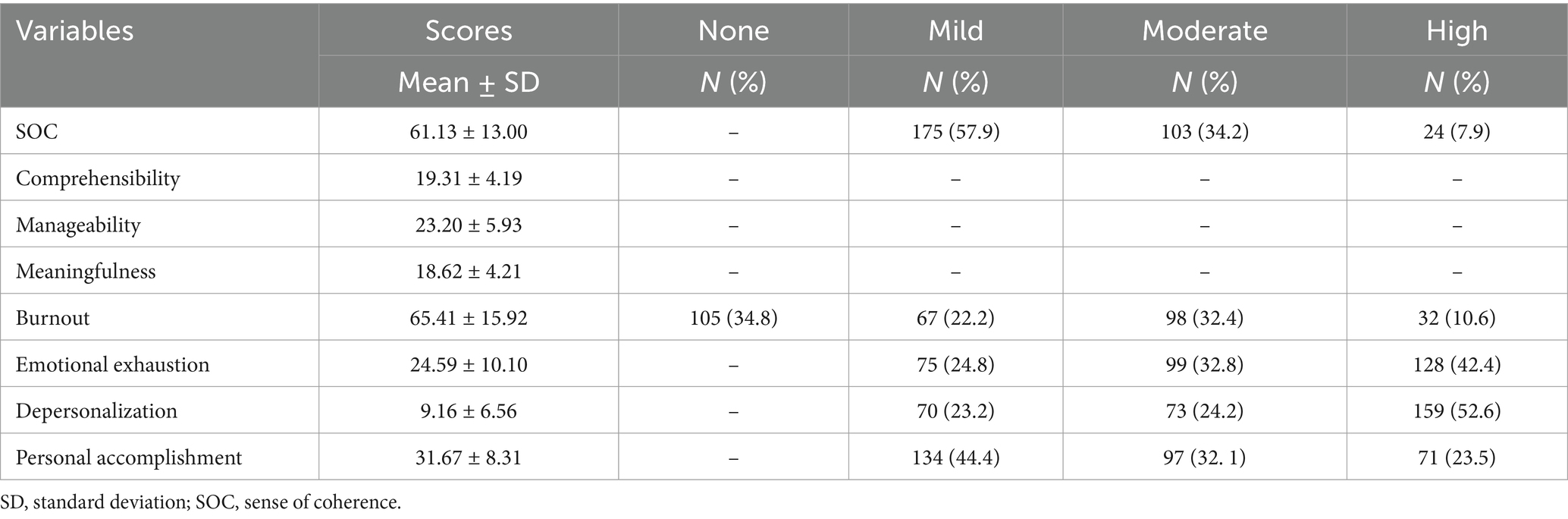
Table 2. Burnout and SOC scores of nurses in Fangcang shelter hospitals (N = 302).
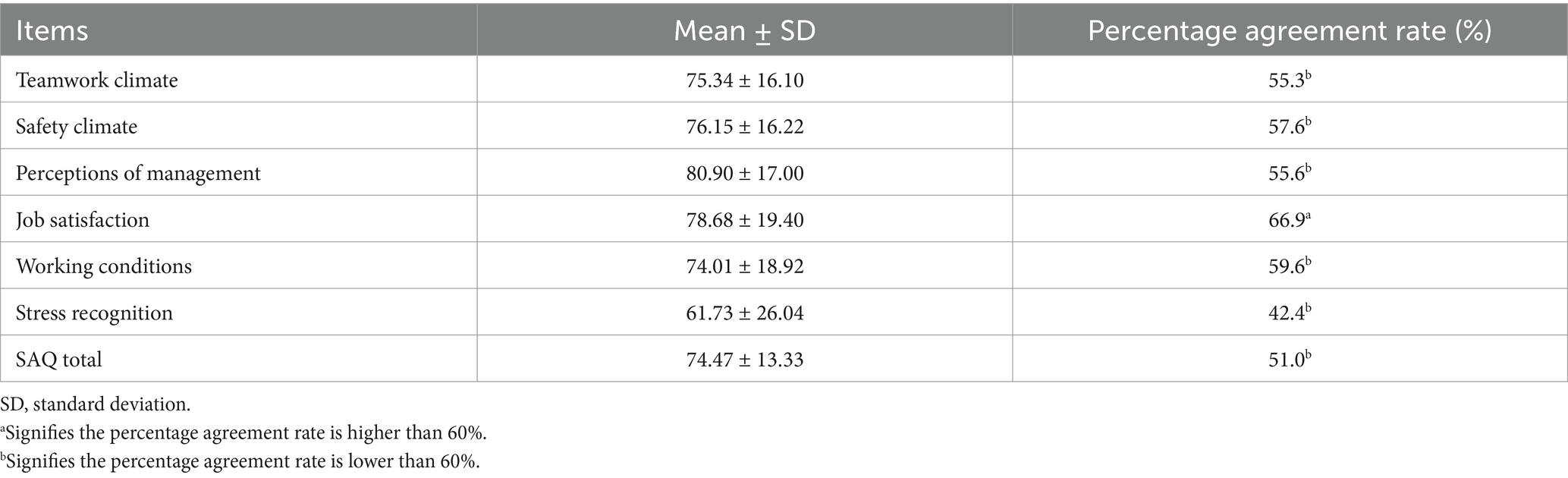
Table 3. SAQ scores of nurses in Fangcang shelter hospitals (N = 302).
The univariate analysis showed that participating in the night shift (p = 0.003) and experiencing negative life events within the last month (p = 0.003) were associated with burnout (Table 4). Age (p = 0.023), marital status (p = 0.018), having children (p = 0.011), type of hospital (p = 0.016), clinical rank (p = 0.032), participation in night shifts (p < 0.001), changes in sleep time (p < 0.001), negative life events within the last month (p < 0.001), and level of concern about the pandemic (p = 0.001) were all related to SOC. Age (p = 0.002), educational status (p = 0.006), marital status (p = 0.011), having children (p = 0.012), type of hospital (p = 0.006), clinical rank (p = 0.003), change in working hours (p = 0.006), experience with the pandemic (p = 0.043), and negative life events within the last month (p = 0.001) were related to safety attitudes.
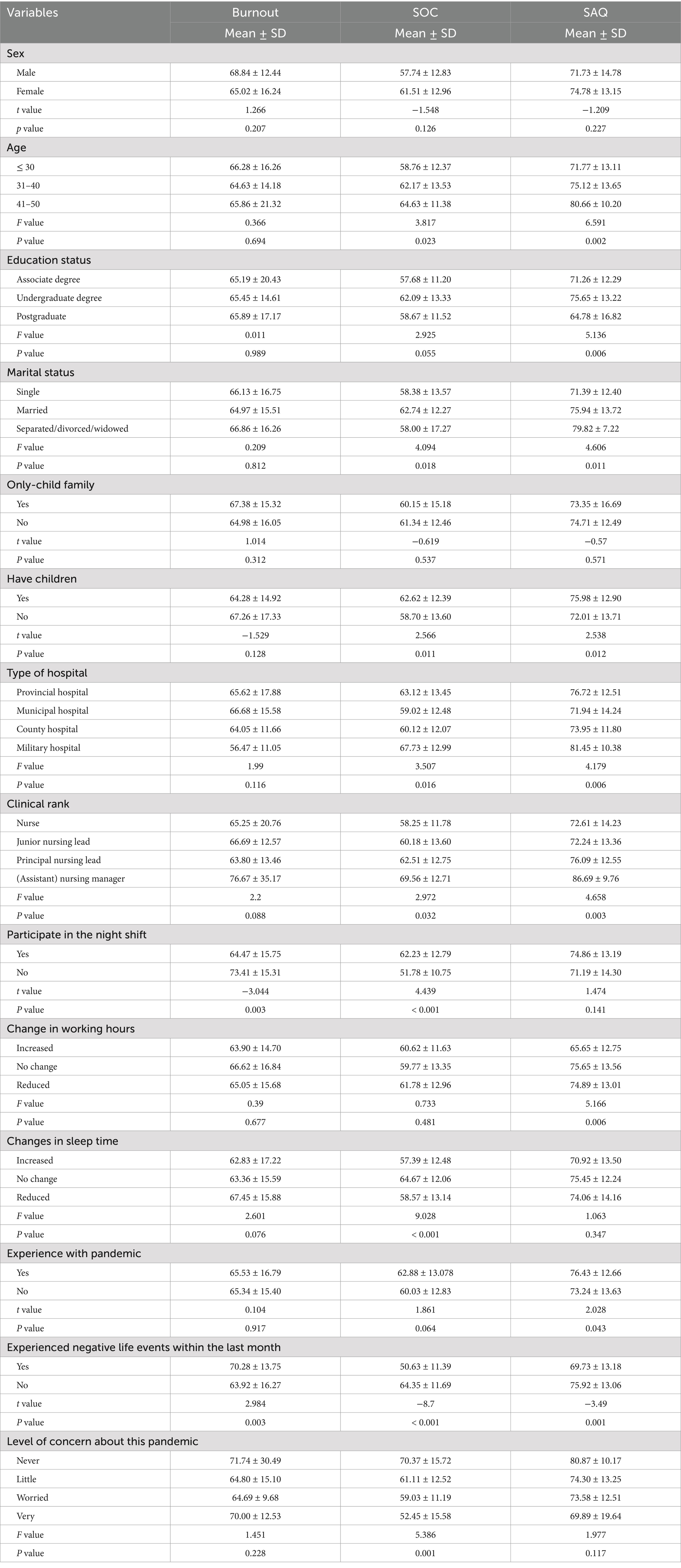
Table 4. Burnout, SOC, and SAQ scores of nurses with different characteristics (N = 302).
There was a significant negative correlation between burnout and SOC (r = −0.399, p < 0.01), a negative correlation between burnout and safety attitude (r = −0.141, p < 0.05), and a significant positive correlation between SOC and safety attitude (r = 0.428, p < 0.01) (Table 5).
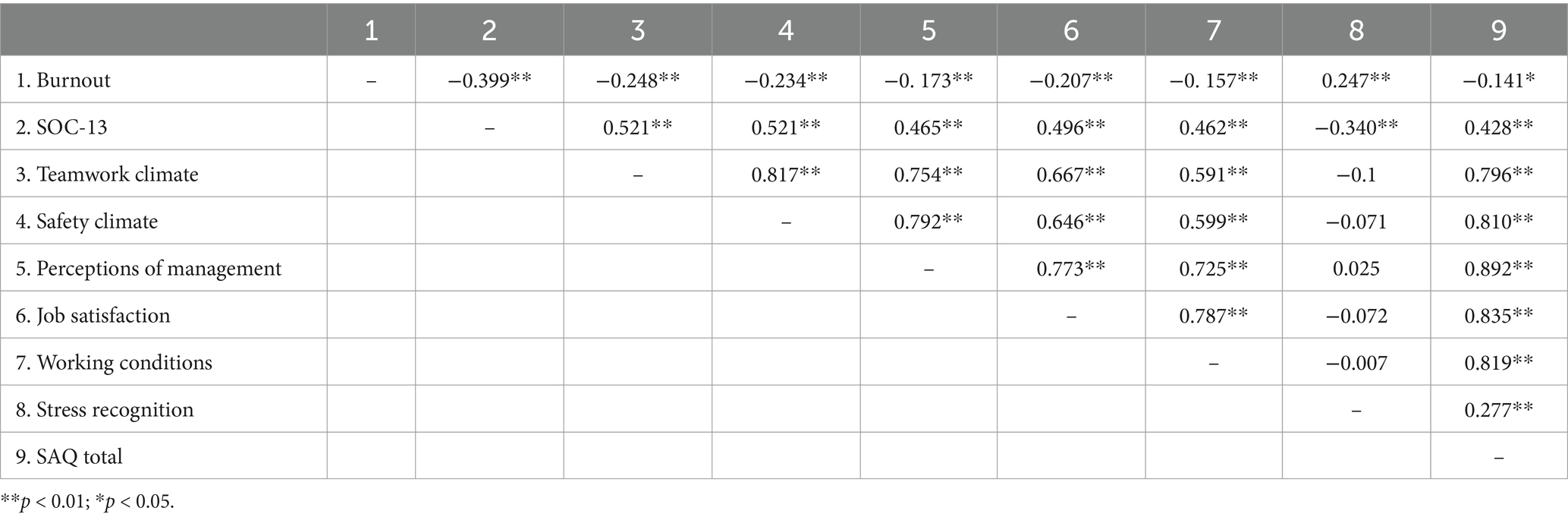
Table 5. Correlation coefficients between burnout, SOC, and SAQ (r).
The SAQ of nurses in FSHs was taken as the dependent variable for a stepwise multiple linear regression, with burnout, SOC, and sociodemographic variables with significant relationships with safety attitude as independent variables. The model created from the results explained 33.8% of the variance in work-safety attitudes, which was statistically significant (F = 31.674, p < 0.001). In order of importance, personal accomplishment (β = 0.343; p < 0.001), depersonalization (β = −0.212; p < 0.001), manageability (β = 0. 159; p = 0.005), change in working hours (β = −0. 151; p = 0.002) and marital status (β = 0.097; p = 0.046) predicted safety attitudes and were statistically significant. Personal accomplishment, manageability, and marital status positively predicted safety attitudes, whereas depersonalization and changes in working hours negatively predicted safety attitudes (Table 6).
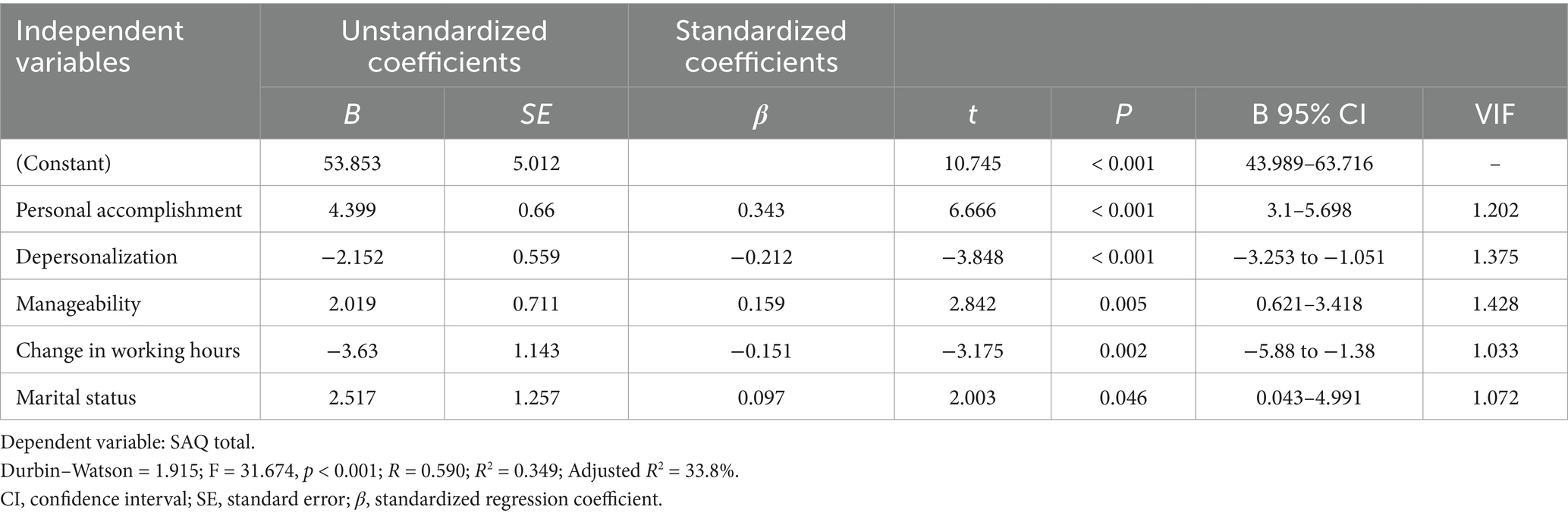
Table 6. Multiple linear regression on nurses’ safety attitude in Fangcang shelter hospitals (N = 302).
With the extension of working hours, people who experience job burnout become emotionally exhausted, their sense of identity with regard to their own abilities and professional skills declines, and their attitudes towards work and patients become negative and indifferent (7). In this study, 42.4% of respondents reported high EE, 52.6% reported high DP, and 44.4% reported low PA. These results indicate that FSH nurses are at a high risk of burnout. Due to the special characteristics of FSHs, nurses leave their familiar working environments and live in isolation from their families, relatives, and friends, which reduces their social activities and increases their feelings of isolation (9). In our study, nurses reported higher DP, which may be related to this isolation.
In addition, while working in FSHs, nurses must shoulder excessive workloads, make direct contact with confirmed COVID-19 patients, and be concerned about becoming infected with COVID-19. During the round of the pandemic occurring when this study was conducted, the majority of patients were infected with the SARS-CoV-2 Omicron variant. This variant has characteristics of rapid transmission, the ability to escape defenses of the immune system, poor immunity to the COVID-19 vaccine, and a high risk of reinfection (52), making it more difficult to control Because of this, nurses often encountered more severe challenges during this period. These stressful events associated with COVID-19 is related to the negative emotions among nurses in FSHs (7–9), such as anxiety and depression, and may exhaust nurses’ positive emotional reserves, leading to burnout.
In our study, the SOC score for FSH nurses was higher than that of nurses in hospitals of Anhui Province (53); the “manageability” dimension having the highest score. During the 2 years since the COVID-19 pandemic, China has been exploring localized epidemic prevention policies (4, 54, 55). Every year, Chinese hospitals simulate an outbreak and conduct training on epidemic protection strategies. The Chinese government and community provide human, financial, and material support to FSHs during their operations. The high score on the “manageability” dimension may be related to the fact that daily emergency drills and good social support led nurses to believe that internal and external resources were at their disposal and that the COVID-19 outbreak was manageable, helping them find meaning in their work at the hospital. In the face of difficult and stressful events, SOC can protect individuals from damage. Kikuchi et al. (56) found a negative correlation between SOC and shiftwork, job rank, and overtime. Interestingly, in our study, burnout was higher and SOC lower among those not working night shifts. This may be because most night shift participants were front-line nurses who were mainly responsible for the care of asymptomatic and mildly infected patients; their working frequency was regular and they had sufficient protective materials and social support. Additionally, most of those who did not participate in the night shift were administrative staff responsible for the safe operation of the FSH; they needed to arrive earlier than others, participate in the design, planning, and coordination of the FSH, and undertake the training and assessment of incoming staff to ensure that the infection rate in the hospital remained low. After the opening of FSHs, it is necessary to provide good human resource management, staff and patient safety management, life care, and coordination of materials and equipment. Consequently, these factors are related to the psychological stress and burnout of managers (57, 58).
The SAQ agreement rate was below international standards (60%) (51). Job satisfaction scores were the highest among the six subscales and results were higher than those reported by nurses in general tertiary hospitals in China (59), Poland (49), Australia (60), and Malaysia (61). Job satisfaction reflects nurses’ positive evaluations of their workplaces. FSHs have become a part of a regular initiative to combat the COVID-19 pandemic in China. Although hospital conditions are not as good as those in formal hospitals, working staff still express high satisfaction with support from various sources.
The teamwork climate reflects the quality of relationships among team members as well as the collaborative climate (31). The nurses in FSHs were redeployed by the government, and although they came from different units, they were able to maintain a good teamwork climate during the fight against COVID-19. The safety climate represents the culture of safety at a particular point and measures the perceptions of healthcare personnel regarding a healthcare organization’s systems and policies for patient safety. The safety climate score of nurses in FSHs was high, likely related to the fact that managers took a series of measures to ensure the normal operation of the hospital and protect staff from infection, including optimizing the workflow, systematic knowledge training, scientific setup of shifts, establishing a collaborative model, focusing on key populations, paying attention to psychological issues, dividing management into zones, strengthening the supervision of infection control, verifying the implementation of the system, and regularly opening the clinic for staff nucleic acid testing (62). In our study, perceptions of management were positive, indicating that nurses were receptive to relevant decisions regarding staff, patients, and organizational management. Several studies (49, 61, 63, 64) have shown that nurses’ reported results on safety climates and perceptions of hospital management were lower than those found in this study. This indicates that the safety management measures adopted by the FSH managers are active.
As FSHs are innovative models, managers must solve many problems to identify the best solutions. Chinese managers usually prefer to solve problems through brainstorming, empowerment, and democracy, which means that solutions to many problems rely on the wisdom of most employees. This is conducive to finding a balance between employees and conflicts during the problem-solving process. Managers work with staff to examine safety hazards and obtain adequate resources and support, which can influence staff to develop positive attitudes towards patients (65). A study by Rasool et al. (66) indicated that occupational stress is related to safety and productivity. The stress recognition scores reported by nurses in this study were lower than those of in Sweden (64), Australia (60), Brazil (67), and tertiary hospitals in China (59). According to the conservation of resources theory, when people’s resources are depleted, they enter a defensive mode to protect themselves, usually becoming aggressive or behaving irrationally (68). During the pandemic, nurses were overworked and under stress, and had no time to reflect on their mental health (69). In situations of poor stress recognition, when nurses’ positive emotions are exhausted, it can have a detrimental related to patient safety. Therefore, better education and training on stress recognition are important to improve the safety climate of FSHs.
During a pandemic, the psychological health of healthcare workers is of great importance to society. High levels of stress and negative mood can exacerbate burnout among healthcare workers. High burnout is associated with a decreased quality of care and increased patient-related adverse events (70). SOC is an important factor in the management of stress and burnout, and also has a relationship with job satisfaction (25–27, 71). Pachi et al. (72) identified SOC as a negative moderator of the burnout-depression relationship, consistent with our findings. SOC can be improved by improving nurses’ social support, reducing burnout (73). Despite the severe challenges faced by countries worldwide from COVID-19, FSH managers have provided a series of measures to alleviate the tremendous stress and negative emotions of front-line nurses, such as adequate protective equipment, appropriate working hours, regular rest and sleep, standard disease protection measures, regulations and disposal procedures appropriate for FSHs, food and daily necessities, and psychological counsellors.
Tan et al. (58) noted that shifts lasting ≥8 h were associated with higher burnout scores, while healthcare workers who voluntarily redeployed to field support had lower burnout levels. In this study, increased working hours were associated with lower safety attitude scores; however, no significant differences were observed in burnout or SOC scores. This may be due to the characteristics of Chinese hospitals, the uneven distribution of medical resources, the high number of patients attending provincial and municipal hospitals, high workloads, and long working hours, which have become the norm for nurses. Although there were many patients and a high workload in the FSHs, the managers set the working time at the hospital to 6 h. The reduction in total working hours and the voluntary acceptance of redeployment may equalize the difference in burnout scores caused by changes in working hours.
Consistent with the study by Moazez et al., marital status influenced perceptions of safety attitudes (74); however, the results of Magalhaes et al. (75) showed that safety attitudes were not related to marital status. We believe that marriage is a reflection of personal responsibility and that married nurses may assume more family responsibility, receive more family support, value the importance of work, and invest in it more than unmarried and divorced individuals do.
Liu et al. (70) concluded that high burnout and low job satisfaction were associated with decreased quality of care and increased patient-related adverse events. The results of a systematic evaluation and meta-analysis of 85 studies demonstrated that nurse burnout was associated with lower health care quality and safety and lower patient satisfaction (32). Multiple supportive factors allow nurses in FSHs to perceive COVID-19 as manageable and understandable and to find meaning in their work. Diverse rewards, especially nonfinancial ones, can promote nursing excellence and help ensure a high level of quality care and patient safety (76). In our study, we found that personal accomplishment and manageability positively predicted safety attitudes, while depersonalization negatively predicted them. This is easy to understand because nurses in FSHs consider it meaningful to accept a unified deployment, support Shanghai healthcare, and fight the pandemic. Additionally, global attention toward nurses is increasing, and their social status is constantly improving. The Chinese health department recognizes the contributions of nurses in FSHs and awards excellent anti-pandemic nurses, which enhances their professional identity and personal achievement. High personal accomplishment and low depersonalization reduce burnout and are strongly associated with high SAQ agreement rates (58).
This study was the first to investigate the levels of burnout, SOC, and safety attitudes among nurses after COVID-19 in Chinese FSHs, analyzing the associated factors. The research results have important reference value for improving the nursing quality and patient safety management of frontline nurses who have experienced FSH during their return to work. This study suggests that managers should consider the importance of recognising stress, working conditions and teamworking climate in FSHs, and take effective measures to improve nurses’ safety attitudes, such as improving personal accomplishments and SOC, and reducing the degree of depersonalization and working time. A supportive work safety environment plays an important role in reducing job burnout and improving SOC (77). This study also showed that the Chinese version of the SAQ has good consistency within the FSHs and provides baseline data for future studies on patient safety in FSHs. More studies can be combined and analyzed in the future to effectively improve healthcare job safety attitudes and patient safety.
Occupational stress is a key factor that has a negative impact on safety and productivity. Chinese managers usually prefer to solve problems through brainstorming, empowerment, and democracy, which means that the resolution of many problems depends on the wisdom of the majority of employees. This helps to find a balance between employees and conflicts in the process of problem-solving. Management personnel and employees jointly inspect safety hazards and obtain sufficient resources and support, which can influence employees to form a positive attitude towards patients and improve the quality of nursing safety. The management has taken a series of measures to create a good team cooperation atmosphere, optimize work processes, systematize stress recognition education and knowledge training, scientifically set up shifts, establish collaboration models, focus on key populations, thereby improving the work safety environment and strengthening patient safety practices. Consistency plays a crucial role in nursing practice, especially in the quality of interaction between nursing and patients. The interaction between nurses and patients is not only related to the psychological health and quality of life of patients, but is also closely related to the professional satisfaction and work engagement of nurses. Future research will explore the intrinsic mechanisms of nurse consistency and patient interaction quality, providing theoretical support for improving nursing practice.
This study had some limitations. The data sources were all from the Anhui Fangcang shelter hospital in Shanghai, meaning that the results were not representative of nurses in all FSHs. Although the research subjects strictly follow the inclusion and exclusion criteria, there may be a phenomenon of low levels of burnout among some survey subjects, resulting in certain sample selection biases. In addition, survey subjects may have various measurement errors of self-reports, such as recall and social expectation biases, which may limit the generalizability of research results. This study is a cross-sectional design, and there may be related causal confusion and reverse causal relationships. In future studies, managers should obtain informed consent to conduct studies using more FSHs. Future cohort studies could be conducted with continuous attention to the psychological status and work safety attitudes of healthcare workers in FSHs to more accurately analyze associated factors.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the Ethics Committee of the First Affiliated Hospital of Bengbu Medical College (approval number: BYYFY-2020KY01). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
FX: Conceptualization, Methodology, Writing – original draft. JL: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft. TZ: Data curation, Investigation, Supervision, Writing – review & editing. XiL: Data curation, Investigation, Methodology, Writing – review & editing. CL: Data curation, Investigation, Supervision, Writing – original draft. XuL: Data curation, Investigation, Software, Validation, Writing – original draft. SL: Conceptualization, Formal analysis, Investigation, Methodology, Writing – review & editing. PY: Investigation, Writing – review & editing. JZ: Project administration, Resources, Supervision, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. WHO. WHO coronavirus (COVID-19) dashboard. Available at: https://covid19.who.int/ (Accessed November 21, 2022).
2. Statement on the Thirteenth Meeting of the International Health Regulations (2005) Emergency committee regarding the coronavirus disease (COVID-19) pandemic. Available at: https://www.who.int/news/item/18-10-2022-statement-on-the-thirteenth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(covid-19)-pandemic (Accessed November 21, 2022).
3. NHC. Transcript of press conference under the Joint Prevention and Control Mechanism of the State Council on 8 July 2022. Available at: http://www.nhc.gov.cn/xcs/s3574/202207/0cfdc8703b224992bca1adbaae26f4aa.shtml (Accessed July 13, 2022).
4. Chen, S, Zhang, Z, Yang, J, Wang, J, Zhai, X, Bärnighausen, T, et al. Fangcang shelter hospitals: a novel concept for responding to public health emergencies. Lancet. (2020) 395:1305–14. doi: 10.1016/S0140-6736(20)30744-3
5. NHC. Notice on the issuance of diagnosis and treatment protocol for COVID-19 pneumonia (trial ninth edition). Available at: http://www.nhc.gov.cn/yzygj/s7653p/202203/b74ade1ba4494583805a3d2e40093d88.shtml (Accessed November 18, 2022).
6. Catton, H. Global challenges in health and health care for nurses and midwives everywhere. Int Nurs Rev. (2020) 67:4–6. doi: 10.1111/inr.12578
7. Murat, M, Köse, S, and Savaşer, S. Determination of stress, depression and burnout levels of front-line nurses during the COVID-19 pandemic. Int J Ment Health Nurs. (2021) 30:533–43. doi: 10.1111/inm.12818
8. Tan, R, Yu, T, Luo, K, Teng, F, Liu, Y, Luo, J, et al. Experiences of clinical first-line nurses treating patients with COVID-19: a qualitative study. J Nurs Manag. (2020) 28:1381–90. doi: 10.1111/jonm.13095
9. Zhang, Y, Wang, C, Pan, W, Zheng, J, Gao, J, Huang, X, et al. Stress, burnout, and coping strategies of frontline nurses during the COVID-19 epidemic in Wuhan and Shanghai, China. Front Psychiatry. (2020) 11:565520. doi: 10.3389/fpsyt.2020.565520
10. Sun, N, Wei, L, Shi, S, Jiao, D, Song, R, Ma, L, et al. A qualitative study on the psychological experience of caregivers of COVID-19 patients. Am J Infect Control. (2020) 48:592–8. doi: 10.1016/j.ajic.2020.03.018
11. Denning, M, Goh, ET, Tan, B, Kanneganti, A, Almonte, M, Scott, A, et al. Determinants of burnout and other aspects of psychological well-being in healthcare workers during the Covid-19 pandemic: a multinational cross-sectional study. PLoS One. (2021) 16:e0238666. doi: 10.1371/journal.pone.0238666
12. Cai, Z, Cui, Q, Liu, Z, Li, J, Gong, X, Liu, J, et al. Nurses endured high risks of psychological problems under the epidemic of COVID-19 in a longitudinal study in Wuhan China. J Psychiatr Res. (2020) 131:132–7. doi: 10.1016/j.jpsychires.2020.09.007
13. Maslach, C, and Jackson, SE. The measurement of experienced burnout. J Organ Behav. (1981) 2:99–113. doi: 10.1002/job.4030020205
14. Kakemam, E, Chegini, Z, Rouhi, A, Ahmadi, F, and Majidi, S. Burnout and its relationship to self-reported quality of patient care and adverse events during COVID-19: a cross-sectional online survey among nurses. J Nurs Manag. (2021) 29:1974–82. doi: 10.1111/jonm.13359
15. Zhang, YY, Han, WL, Qin, W, Yin, HX, Zhang, CF, Kong, C, et al. Extent of compassion satisfaction, compassion fatigue and burnout in nursing: a meta-analysis. J Nurs Manag. (2018) 26:810–9. doi: 10.1111/jonm.12589
16. Luo, G, Xiao, N, and Chen, XL. A meta-analysis of detection rate of Chinese nurses’ job burnout. Occup Health. (2022) 38:1854–9. doi: 10.13329/j.cnki.zyyjk.2022.0367
17. Antonovsky, A. The structure and properties of the sense of coherence scale. Soc Sci Med. (1993) 36:725–33. doi: 10.1016/0277-9536(93)90033-z
18. Geyer, S. Some conceptual considerations on the sense of coherence. Soc Sci Med. (1997) 44:1771–9. doi: 10.1016/s0277-9536(96)00286-9
19. Masanotti, GM, Paolucci, S, Abbafati, E, Serratore, C, and Caricato, M. Sense of coherence in nurses: a systematic review. Int J Environ Res Public Health. (2020) 17:1861. doi: 10.3390/ijerph17061861
20. Nowicki, GJ, Ślusarska, B, Tucholska, K, Naylor, K, Chrzan-Rodak, A, and Niedorys, B. The severity of traumatic stress associated with COVID-19 pandemic, perception of support, sense of security, and sense of meaning in life among nurses: research protocol and preliminary results from Poland. Int J Environ Res Public Health. (2020) 17:6491. doi: 10.3390/ijerph17186491
21. Ramberg, J, Låftman, SB, Nilbrink, J, Olsson, G, and Toivanen, S. Job strain and sense of coherence: associations with stress-related outcomes among teachers. Scand J Public Health. (2022) 50:565–74. doi: 10.1177/14034948211011812
22. Coutinho, VM, Araújo, GL, Lyra, MCA, Rosenblatt, A, and Heimer, MV. Sense of coherence and quality of life in adolescents with heart disease. Rev Paul Pediatr. (2022) 40:e2021104. doi: 10.1590/1984-0462/2022/40/2021104IN
23. Tam, CW, Pang, EP, Lam, LC, and Chiu, HF. Severe acute respiratory syndrome (SARS) in Hong Kong in 2003: stress and psychological impact among frontline healthcare workers. Psychol Med. (2004) 34:1197–204. doi: 10.1017/s0033291704002247
24. Fitzgerald, G, Aitken, P, Shaban, RZ, Patrick, J, Arbon, P, McCarthy, S, et al. Pandemic (H1N1) influenza 2009 and Australian emergency departments: implications for policy, practice and pandemic preparedness. Emerg Med Australas. (2012) 24:159–65. doi: 10.1111/j.1742-6723.2011.01519.x
25. Betke, K, Basińska, MA, and Andruszkiewicz, A. Sense of coherence and strategies for coping with stress among nurses. BMC Nurs. (2021) 20:107. doi: 10.1186/s12912-021-00631-1
26. Schmuck, J, Hiebel, N, Rabe, M, Schneider, J, Erim, Y, Morawa, E, et al. Sense of coherence, social support and religiosity as resources for medical personnel during the COVID-19 pandemic: a web-based survey among 4324 health care workers within the German network university medicine. PLoS One. (2021) 16:e0255211. doi: 10.1371/journal.pone.0255211
27. Malagon-Aguilera, MC, Suñer-Soler, R, Bonmatí-Tomas, A, Bosch-Farré, C, Gelabert-Vilella, S, and Juvinyà-Canal, D. Relationship between sense of coherence, health and work engagement among nurses. J Nurs Manag. (2019) 27:1620–30. doi: 10.1111/jonm.12848
28. WHO. Consensus statement: role of policy-makers and health care leaders in implementation of the global patient safety action plan 2021–2030. Available at: https://www.who.int/publications/i/item/WHO-UHL-IHS-PSF-2022.3 (Accessed November 18, 2022).
29. WHO. Patient safety. Available at: https://www.who.int/news-room/fact-sheets/detail/patient-safety (Accessed November 18, 2022).
30. Sexton, JB, Helmreich, RL, Neilands, TB, Rowan, K, Vella, K, Boyden, J, et al. The safety attitudes questionnaire: psychometric properties, benchmarking data, and emerging research. BMC Health Serv Res. (2006) 6:44. doi: 10.1186/1472-6963-6-44
31. Alves, DFB, Lorenzini, E, and Kolankiewicz, ACB. Patient safety climate in a Brazilian general hospital. Int J Risk SafMed. (2020) 31:97–106. doi: 10.3233/JRS-191024
32. Li, LZ, Yang, P, Singer, SJ, Pfeffer, J, Mathur, MB, and Shanafelt, T. Nurse burnout and patient safety, satisfaction, and quality of care: a systematic review and meta-analysis. JAMA Netw Open. (2024) 7:e2443059. doi: 10.1001/jamanetworkopen.2024.43059
33. von Elm, E, Altman, DG, Egger, M, Pocock, SJ, Gøtzsche, PC, and Vandenbroucke, JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg. (2014) 12:1495–9. doi: 10.1016/j.ijsu.2014.07.013
34. Zhao, X, Liu, S, Chen, Y, Zhang, Q, and Wang, Y. Influential factors of burnout among village doctors in China: a cross-sectional study. Int J Environ Res Public Health. (2021) 18:2013. doi: 10.3390/ijerph18042013
35. Cabezón, M, Agurto, M, Estefó, M, Oliveros, X, Ojeda, D, Cisternas, P, et al. Burnout syndrome in healthcare workers during COVID-19 pandemic. Rev Med Chile. (2021) 149:1589–93. doi: 10.4067/S0034-98872021001101589
36. Pang, Y, He, Y, Chen, Z, Han, X, Leng, J, and Tang, L. The perceptions of burnout and related influencing factors in Chinese physicians and nurses working in a cancer hospital. Psychooncology. (2021) 30:1525–34. doi: 10.1002/pon.5709
37. Shahin, MA, Al-Dubai, SAR, Abdoh, DS, Alahmadi, AS, Ali, AK, and Hifnawy, T. Burnout among nurses working in the primary health care centers in Saudi Arabia, a multicenter study. AIMS Public Health. (2020) 7:844–53. doi: 10.3934/publichealth.2020065
38. Christina, M, Jackson, S, and Leiter, M. Burnout inventory manual. 3rd ed. Palo Alto, CA: Consulting Psychologists Press (1996).
40. Ye, ZH, Luo, H, and Jiang, AL. Diagnostic standard and norms of Maslach burnout inventory for nurses in Hangzhou. Chin J Nurs. (2008) 3:207–9.
41. Gan, Y, Jiang, H, Li, L, Yang, Y, Wang, C, Liu, J, et al. Prevalence of burnout and associated factors among general practitioners in Hubei, China: a cross-sectional study. BMC Public Health. (2019) 19:1607. doi: 10.1186/s12889-019-7755-4
42. Li, H, Zuo, M, Gelb, AW, Zhang, B, Zhao, X, Yao, D, et al. Chinese anesthesiologists have high burnout and low job satisfaction: a cross-sectional survey. Anesth Analg. (2018) 126:1004–12. doi: 10.1213/ANE.0000000000002776
43. Li, YX. Study on job burnout across three occupational samples: An integrity perspective. Doctoral dissertation, East China Normal University, Shanghai (2005).
44. Mittelmark, MB, Bauer, GF, Vaandrager, L, Pelikan, JM, Sagy, S, Eriksson, M, et al. eds. The handbook of salutogenesis. 2nd ed. Cham (CH): Springer (2022).
45. Eriksson, M, Lindström, B, and Lilja, J. A sense of coherence and health. Salutogenesis in a societal context: Aland, a special case? J Epidemiol Community Health. (2007) 61:684–8. doi: 10.1136/jech.2006.047498
46. Bao, LP, and Liu, JS. The reliability and validity of Chinese version of SOC-13. Chin J Clin Psych. (2005) 4:24–6.
47. Bao, LP, Liu, JS, and Zhou, Y. Reliability and validity of sense of Coherence-13(SOC-13). Chin Ment Health J. (2006) 5:299–301.
48. Zhao, C, Chang, Q, Zhang, X, Wu, Q, Wu, N, He, J, et al. Evaluation of safety attitudes of hospitals and the effects of demographic factors on safety attitudes: a psychometric validation of the safety attitudes and safety climate questionnaire. BMC Health Serv Res. (2019) 19:836. doi: 10.1186/s12913-019-4682-0
49. Malinowska-Lipień, I, Micek, A, Gabryś, T, Kózka, M, Gajda, K, Gniadek, A, et al. Nurses and physicians attitudes towards factors related to hospitalized patient safety. PLoS One. (2021) 16:e0260926. doi: 10.1371/journal.pone.0260926
50. Sexton, JB, Paine, LA, Manfuso, J, Holzmueller, CG, Martinez, EA, Moore, D, et al. A check-up for safety culture in "my patient care area". Jt Comm J Qual Patient Saf. (2007) 33:699–703, 645. doi: 10.1016/s1553-7250(07)33081-x
51. Cui, Y, Xi, X, Zhang, J, Feng, J, Deng, X, Li, A, et al. The safety attitudes questionnaire in Chinese: psychometric properties and benchmarking data of the safety culture in Beijing hospitals. BMC Health Serv Res. (2017) 17:590. doi: 10.1186/s12913-017-2543-2
52. Zhou, H, Møhlenberg, M, Thakor, JC, Tuli, HS, Wang, P, Assaraf, YG, et al. Sensitivity to vaccines, therapeutic antibodies, and viral entry inhibitors and advances to counter the SARS-CoV-2 omicron variant. Clin Microbiol Rev. (2022) 35:e0001422. doi: 10.1128/cmr.00014-22
53. Ding, H, Song, GQ, Zhu, Y, and Zhang, HL. Correlation analysis of presenteeismin and the sense of coherence on nurse in tertiary hospitals from Anhui Province. J Nurs Adm. (2021) 21:463–7. doi: 10.3969/j.issn.1671-315x.2021.07.002
54. Hu, B, Chen, W, Yue, T, and Jiang, G. Study on the localization of Fangcang shelter hospitals during pandemic outbreaks. Front Public Health. (2022) 10:876558. doi: 10.3389/fpubh.2022.876558
55. NHC. Notice on the issuance of design guidelines for Fangcang shelter hospitals (trial). Available at: http://www.nhc.gov.cn/guihuaxxs/s7824/202208/1f16df5c140b4ad587381184ce51c317.shtml (Accessed August 12, 2022).
56. Kikuchi, Y, Nakaya, M, Ikeda, M, Okuzumi, S, Takeda, M, and Nishi, M. Sense of coherence and personality traits related to depressive state. Psychiatry J. (2014) 2014:738923. doi: 10.1155/2014/738923
57. Gu, Y, Zhu, Y, and Xu, G. Factors associated with mental health outcomes among health care workers in the Fangcang shelter hospital in China. Int J Soc Psychiatry. (2022) 68:64–72. doi: 10.1177/0020764020975805
58. Tan, BYQ, Kanneganti, A, Lim, LJH, Tan, M, Chua, YX, Tan, L, et al. Burnout and associated factors among health care workers in Singapore during the COVID-19 pandemic. J Am Med Dir Assoc. (2020) 21:1751–1758.e5. doi: 10.1016/j.jamda.2020.09.035
59. Li, Y, Zhao, Y, Hao, Y, Jiao, M, Ma, H, Teng, B, et al. Perceptions of patient safety culture among healthcare employees in tertiary hospitals of Heilongjiang province in northern China: a cross-sectional study. Int J Qual Health Care. (2018) 30:618–23. doi: 10.1093/intqhc/mzy084
60. Connell, CJ, Cooper, S, and Endacott, R. Measuring the safety climate in an Australian emergency department. Int Emerg Nurs. (2021) 58:101048. doi: 10.1016/j.ienj.2021.101048
61. Krishnasamy, K, Tan, MP, and Zakaria, MI. Interdisciplinary differences in patient safety culture within a teaching hospital in Southeast Asia. Int J Clin Pract. (2021) 75:e14333. doi: 10.1111/ijcp.14333
62. Qi, XL, Gan, ZH, Tong, ZH, Xia, WM, Ni, J, Yu, LC, et al. Treatment practice of COVID-19 outbreak at Shanghai Fangcang shelter hospital. J Med Postgrad. (2022) 35:868–71. doi: 10.16571/j.cnki.1008-8199.2022.08.014
63. Ningrum, EH, Evans, S, Soh, SE, and Ernest, A. Perception of safety climate among Indonesian nurses: a cross-sectional survey. J Public Health Res. (2021) 10:2182. doi: 10.4081/jphr.2021.2182
64. Milton, J, Chaboyer, W, Åberg, ND, Erichsen, AA, and Oxelmark, L. Safety attitudes and working climate after organizational change in a major emergency department in Sweden. Int EmergNurs. (2020) 53:100830. doi: 10.1016/j.ienj.2020.100830
65. Sexton, JB, Berenholtz, SM, Goeschel, CA, Watson, SR, Holzmueller, CG, Thompson, DA, et al. Assessing and improving safety climate in a large cohort of intensive care units. Crit Care Med. (2011) 39:934–9. doi: 10.1097/CCM.0b013e318206d26c
66. Rasool, SF, Wang, M, Zhang, Y, and Samma, M. Sustainable work performance: the roles of workplace violence and occupational stress. Int J Environ Res Public Health. (2020) 17:912. doi: 10.3390/ijerph17030912
67. Carvalho, PA, Amorim, FF, Casulari, LA, and Gottems, LBD. Safety culture in the perception of public-hospital health professionals. Rev Saude Publica. (2021) 55:56. doi: 10.11606/s1518-8787.2021055002838
68. Hobfoll, SE, Halbesleben, J, Neveu, JP, and Westman, M. Conservation of resources in the organizational context: the reality of resources and their consequences. Annu Rev Organ Psych Organ Behav. (2018) 5:103–28. doi: 10.1146/annurev-orgpsych-032117-104640
69. Chen, HY, Lu, L, Ko, YM, Chueh, JW, Hsiao, SY, Wang, PC, et al. Post-pandemic patient safety culture: a case from a large metropolitan hospital group in Taiwan. Int J Environ Res Public Health. (2021) 18:4537. doi: 10.3390/ijerph18094537
70. Liu, J, Zheng, J, Liu, K, Liu, X, Wu, Y, Wang, J, et al. Workplace violence against nurses, job satisfaction, burnout, and patient safety in Chinese hospitals. Nurs Outlook. (2019) 67:558–66. doi: 10.1016/j.outlook.2019.04.006
71. Colomer-Pérez, N, Paredes-Carbonell, JJ, Sarabia-Cobo, C, Useche, SA, and Gea-Caballero, V. Self-care and sense of coherence: a salutogenic model for health and care in nursing education. Int J Environ Res Public Health. (2022) 19:9482. doi: 10.3390/ijerph19159482
72. Pachi, A, Sikaras, C, Ilias, I, Panagiotou, A, Zyga, S, Tsironi, M, et al. Burnout, depression and sense of coherence in nurses during the pandemic crisis. Healthcare (Basel). (2022) 10:134. doi: 10.3390/healthcare10010134
73. Zhan, T, Li, H, and Ding, X. Can social support enhance sense of coherence and perceived professional benefits among Chinese registered nurses? A mediation model. J Nurs Manag. (2020) 28:488–94. doi: 10.1111/jonm.12931
74. Moazez, M, Miri, S, Foroughameri, G, and Farokhzadian, J. Nurses' perceptions of systems thinking and safe nursing care: a cross-sectional study. J Nurs Manag. (2020) 28:822–30. doi: 10.1111/jonm.13000
75. Magalhães, FHL, Pereira, ICA, Luiz, RB, Barbosa, MH, and Ferreira, MBG. Patient safety atmosphere in a teaching hospital. Clima de segurança do paciente em um hospital de ensino. Rev Gaucha Enferm. (2019) 40:e20180272. doi: 10.1590/1983-1447.2019.20180272
76. Seitovirta, J, Lehtimäki, AV, Vehviläinen-Julkunen, K, Mitronen, L, and Kvist, T. Registered nurses' perceptions of rewarding and its significance. J Nurs Manag. (2018) 26:457–66. doi: 10.1111/jonm.12571
Keywords: COVID-19, nurse, burnout, sense of coherence, safety attitude
Citation: Xue F, Liu J, Zhou T, Li X, Liu C, Li X, Li S, Ye P and Zhang J (2025) The relationship between burnout, sense of coherence and job safety attitudes among nurses after coronavirus disease 2019 in China: a cross-sectional survey. Front. Public Health. 13:1516744. doi: 10.3389/fpubh.2025.1516744
Edited by:
Sonia Regina Pasian, University of São Paulo, BrazilReviewed by:
Lambert Zixin Li, Stanford University, United StatesCopyright © 2025 Xue, Liu, Zhou, Li, Liu, Li, Li, Ye and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jing Zhang, MDcwMDAwN0BiYm1jLmVkdS5jbg==
†These authors have contributed equally to this work
‡ORCID: Jing Zhang, orcid.org/0000-0002-5496-1574
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.