 Siv T. B. Bjørkedal1,2*
Siv T. B. Bjørkedal1,2* Thomas N. Christensen1,2Rie M. Poulsen1,3
Thomas N. Christensen1,2Rie M. Poulsen1,3 Anne Ranning1,4
Anne Ranning1,4 Anne A. E. Thorup5,6Merete Nordentoft1,6
Anne A. E. Thorup5,6Merete Nordentoft1,6 Anders Bo Bojesen1
Anders Bo Bojesen1 Lene H. Hastrup7,8
Lene H. Hastrup7,8 Marte Ustrup1,2
Marte Ustrup1,2 Lene F. Eplov1,2
Lene F. Eplov1,2- 1Copenhagen Research Center for Mental Health (CORE), Hellerup, Denmark
- 2Copenhagen Research Unit for Recovery, Copenhagen, Denmark
- 3National Board of Social Services in Denmark, Odense, Denmark
- 4Department of Psychology, University of Copenhagen, Copenhagen, Denmark
- 5Research Unit, Child and Adolescent Mental Health Center, Hellerup, Denmark
- 6Department of Clinical Medicine, Faculty of Health Sciences, University of Copenhagen, Copenhagen, Denmark
- 7Psychiatric Research Unit, Psychiatry in Region Zealand, Slagelse, Denmark
- 8Danish Centre for Health Economics (DaCHE), University of Southern Denmark, Odense, Denmark
Introduction: Since 2013, headspace Denmark has been offered in specific areas to adolescents and young adults between 12 and 25 years, to promote youth mental health and wellbeing. Headspace provides free counselling and support, primarily delivered by trained volunteers in the headspace centres and provides information and knowledge about youth mental health, and headspace services, through community engagement. Until now, effectiveness evaluation of the Danish headspace centres has not been conducted.
Methods: Present study consists of (1) an effectiveness evaluation designed as a propensity score matched quasi-experimental trial, where the exposed person (n = 1,500), in this case the young person receiving counselling sessions at headspace, will be matched by using propensity scores to six unexposed individuals. (2) A cost-effectiveness evaluation (3) a process evaluation with predominantly qualitative methods to investigate the implementation of key activities of headspace, their mechanisms of change, and interactions with contextual factors.
Discussion: headspace centres have achieved national endorsement and are implemented in 30 municipalities in Denmark. Thus, there is a need to investigate the effectiveness of the services. Results from the evaluation can also contribute to new knowledge targeted at international youth mental health promotion initiatives. However, this evaluation is limited by selection bias since it is not possible to separate the impact of the intervention from the impact of help-seeking behaviour.
Introduction
Increasing rates of poor mental health among adolescents and young adults is a serious, global public health concern (1, 2). About 62.5% of all mental illnesses have their onset before the age of 25 years (3) and are considered the leading cause of disability in most European countries (4). In Denmark, youth mental health is a pivotal public health challenge (5). According to the Danish Health Authorities, more than 73,000 children and adolescents (corresponding to 63 out of 1,000 youths) are living with a mental illness, which is a 39% increase over the last 10 years (6). Furthermore, national surveys on health and wellbeing in persons up to 24 years of age show that although most young people in Denmark perceive their health to be good, there is an increasing proportion of adolescents and young adults reporting mental health complaints such as high levels of stress and emotional problems (5). There is no doubt that mental health problems pose a threat to young people’s health, wellbeing, and opportunities for thriving and living fulfilling lives. Mental health problems in childhood and adolescent years are also associated with health deterioration, e.g., recurrent illness episodes and functional impairment (5), and obstruction of educational and vocational attainment (7, 8). Thus, poor mental health in youth does not only have adverse consequences for the individual but also for society in terms of loss of productivity and increased expenses to health and social services (1, 9–11).
In Denmark, the health care system is publicly funded, which means that mental health services are available to everyone, free of charge. Despite this, a gap exists between the growing group of young people with mental health complaints and those who receive sufficient support in the mental health system. Barriers for young people to access traditional mental health services include stigma towards mental health problems, long waiting lists for assessment and treatment, and lack of mental health literacy (12, 13). Investments in preventive and mental health promotion initiatives are necessary to help and support young people with mental health complaints before more severe mental health problems develop with the risk of consequently social and/or vocational marginalisation.
To address the above-mentioned challenges and to empower young people with information about mental health, and opportunities for support, the Non-Governmental Organisation, Det Sociale Netværk, has during the previous decade established 30 headspace centres in municipalities in all Danish Regions. The headspace centres provide a low threshold and easily accessible supportive place regarding mental health, to promote mental health and wellbeing in youth between 12 and 25 years. The headspace centres have a “soft entry” to make it as easy as possible for young people to get help to any problem they have, that may affect their mental health and wellbeing. In Denmark, the headspace centres are based on and branded like the Australian headspace model, but contextual adaptations have been made, to meet local needs (14). The headspace centres offer free counselling services (“someone to talk to”) predominantly delivered by trained adult volunteers. The volunteers work in pairs, either with another volunteer, or an employed counsellor in the headspace centre. In contrast to the Australian headspace model, mental health assessment and treatment are not provided. If the counsellor finds that the person may need, for instance, clinical treatment, the person is supported to access these services. This is referred to as bridge building in headspace.
The dissemination of headspace centres in Denmark necessitates evidence-based knowledge on whether headspace is an effective intervention to promote mental health and wellbeing among young people. It also necessitates knowledge on the costs and outcomes of headspace. An evaluation of the impact of headspace in Denmark on young people’s lives and a cost-consequence analysis was conducted by a consulting agency in 2019 (15). Findings showed that 94% of the youth receiving counselling in headspace reported feeling understood and respected. Additionally, the evaluation indicated that counselling sessions improved the wellbeing and life satisfaction of the participants. According to the Cantril’s ladder (16), there was an average of 9% improvement in life satisfaction, while the General Population - Clinical Outcomes in Routine Evaluation (CORE-GP) (17) scale showed an average 7% rise in mental wellbeing. Additionally, the proportion of people who reported feeling lonely reduced by 9% according to the Three-Item Loneliness Scale (18). However, it was emphasised that a major limitation was the lack of a comparable control group, which meant that no firm conclusions could be drawn regarding the effects of headspace. The analysis of cost and returns to society was based on headspace operating costs and scenario-based analyses where the derivative effects for the young people were estimated. Based on the evaluation, it was therefore not possible to draw any conclusion on the cost-effectiveness of headspace due to the short follow-up period, the lack of a control group, and the lack of register-based health care and municipal social care costs (15).
A 2022 national evaluation of headspace in Australia utilised a pre-post treatment comparison design, with regression to mean adjustments, by using the variation in outcomes measured at intake and before the second session. The results showed improvement across all outcomes: wellbeing, functioning and quality of life. In 52% of the young people the improvement was clinically significant in at least one of the outcomes (19). Findings indicated that higher session attendance was associated with greater reductions in distress, as measured by the Kessler Psychological Distress Scale (K10), and improvements in psychosocial functioning, assessed through the Social and Occupational Functioning Assessment Scale (SOFA). For instance, young people who attended two sessions showed minimal change (−0.1 K10; +0.5 SOFA), whereas those attending 3–5 or 6–9 sessions experienced greater improvements (−1.5 and −2.2 K10; +2.7 and +5 SOFA, respectively). The Australian evaluation cannot be directly compared to the Danish evaluation conducted by Rambøll, as the studies measured different outcomes using distinct methodologies. However, the two evaluations suggest that improvements are attainable, in outcomes related to youth mental health. Matthay et al. (20) emphasise that effect sizes vary based on intervention features (intensity, duration, content, and implementers) and mechanisms. Unlike Australia’s primary care-based model, staffed by health professionals and offering treatments such as cognitive behavioural therapy and medical consultations, headspace centres in Denmark operate as a volunteer-driven civic initiative without mental health specialists, making it a lower-intensity, non-medical intervention. Thus, smaller effect sizes than the ones identified in the Australian evaluation may be expected in this evaluation of headspace in Denmark. However, small effect sizes can also be important, from a mental health promotion and prevention perspective (20). Thus, more scientifically based knowledge is needed about if and how the headspace intervention can enhance youth mental health and wellbeing and prevent mental illness. There is also a need for documentation of the cost-effectiveness of the intervention where all relevant costs are measured. This is important to inform policymakers in deciding future investments and implementation of preventive mental health interventions like headspace to ensure that resources are being used properly. Moreover, there is a growing need to investigate the key activities of the Danish headspace intervention and to document how these can be implemented in a local context and how they might create the expected effects on youth mental health and wellbeing.
The overall aim of present evaluation is to investigate the potential effects on young individuals in the presence of headspace entities offering easy access and counselling for help-seeking youth, as well as the cost-effectiveness of the intervention. In addition, the aim is to investigate key activities of the headspace intervention utilising a process evaluation and analyse how the key activities can support the intended effects in different local contexts.
headspace Denmark
The headspace intervention can be mapped as a complex intervention since it consists of several flexible components that interact to produce change, involves many types of stakeholders and organisations, and is expected to create multiple outcomes. To accommodate this complexity, the study is guided by the Medical Research Council (MRC) guidelines for evaluation of complex interventions (41). Consequently, the study takes a point of departure in a figurative programme theory for the headspace intervention (see Figure 1). The preliminary programme theory was developed for this study in collaboration with central headspace management and is based on internal documents in the Danish headspace initiative.
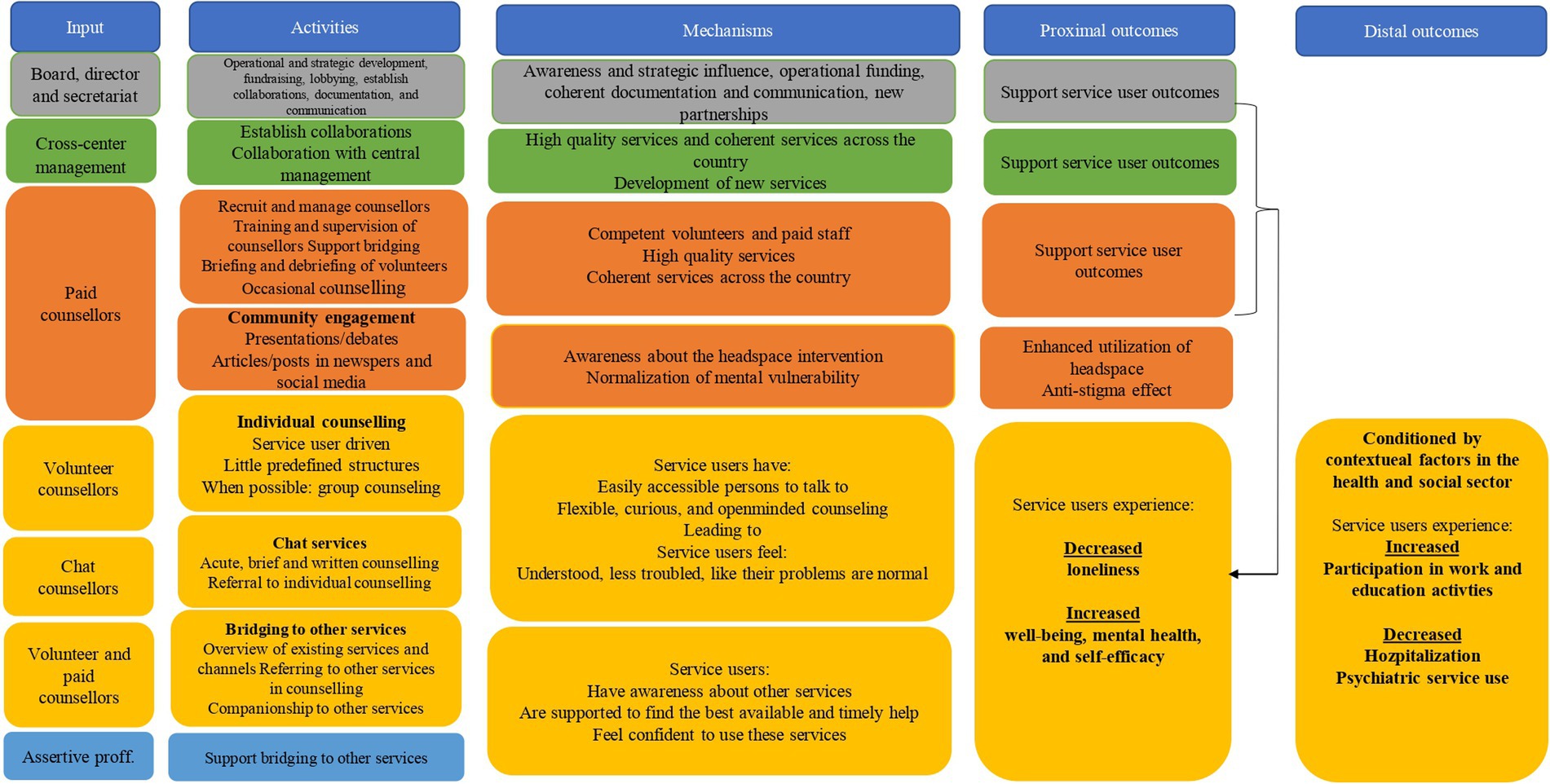
Figure 1. Logic model of the headspace intervention. The figure provides an overview of (1) the activities in headspace; yellow activities are in direct contact with service users, whereas grey, green, orange, and blue activities primarily support the yellow activities, (2) the inputs (personnel) that are necessary to deliver the activities (3) the mechanisms by which the key activities are expected to create the intended outcomes, and (4) the expected proximal and distal outcomes. Yellow outcomes are directly related to service users, while the green and orange outcomes support the yellow proximal outcomes as indicated by the arrow.
headspace centres
headspace Denmark consists of 30 headspace centres and one national chat centre. All centres offer free counselling to young people between 12 and 25 years. The headspace centres are staffed with one cross-centre manager (one manager serves about three headspace centres), two paid counsellors, volunteer counsellors, and two part-time (15 h. per week) assertive professionals employed in the local mental health services and/or social services. The headspace centres are located so they are accessible to young people (for instance close to public transportation). The centres furniture and decorations signal a youth-friendly atmosphere. The headspace centres are open 3 days a week, between 12 and 18 (12 AM to 6 PM) and the chat centre is open between 12 and 22 (12 AM to 10 PM).
Training of counsellors involves an online training program, a weekend course, and on-site training and supervision with experienced counsellors and professionals. The counselling provided to the youth is delivered in an open-minded, curious, and flexible approach, and the counsellors are guided by a person-centred approach that sets the young person’s needs at the centre of their work. Volunteering is a key principle in the headspace organisation, and young people seeking counselling and support are informed that most counsellors are volunteers.
Young people accessing counselling do not need to state their name or personal ID number, so their identity remains anonymous. The headspace centres operate under the motto “Nothing is too big or too small,” meaning that all young people in the targeted age group can access the centres. Should the young person require additional support such as a mental health assessment, specialist treatment or support from social services, the counsellors can offer support and guidance in accessing these services. In addition to counselling and bridging to other services, headspace centres play an active role in providing information about youth mental health, de-tabooing mental health problems among young people, as well as making headspace centres visible and thus accessible through community engagement and collaborations with schools, etc.
Overall study design
The study protocol consists of three studies: an effectiveness evaluation, a cost-effectiveness evaluation, and a process evaluation, to provide a holistic and comprehensive understanding of headspace Denmark, to determine whether the intervention meets it objectives, to investigate the costs of the intervention to the outcomes achieved, and to analyse how the intervention is implemented to improve youth mental health. An overview of the three studies is provided in Figure 2. Appendix 1 shows a timeline of the studies.
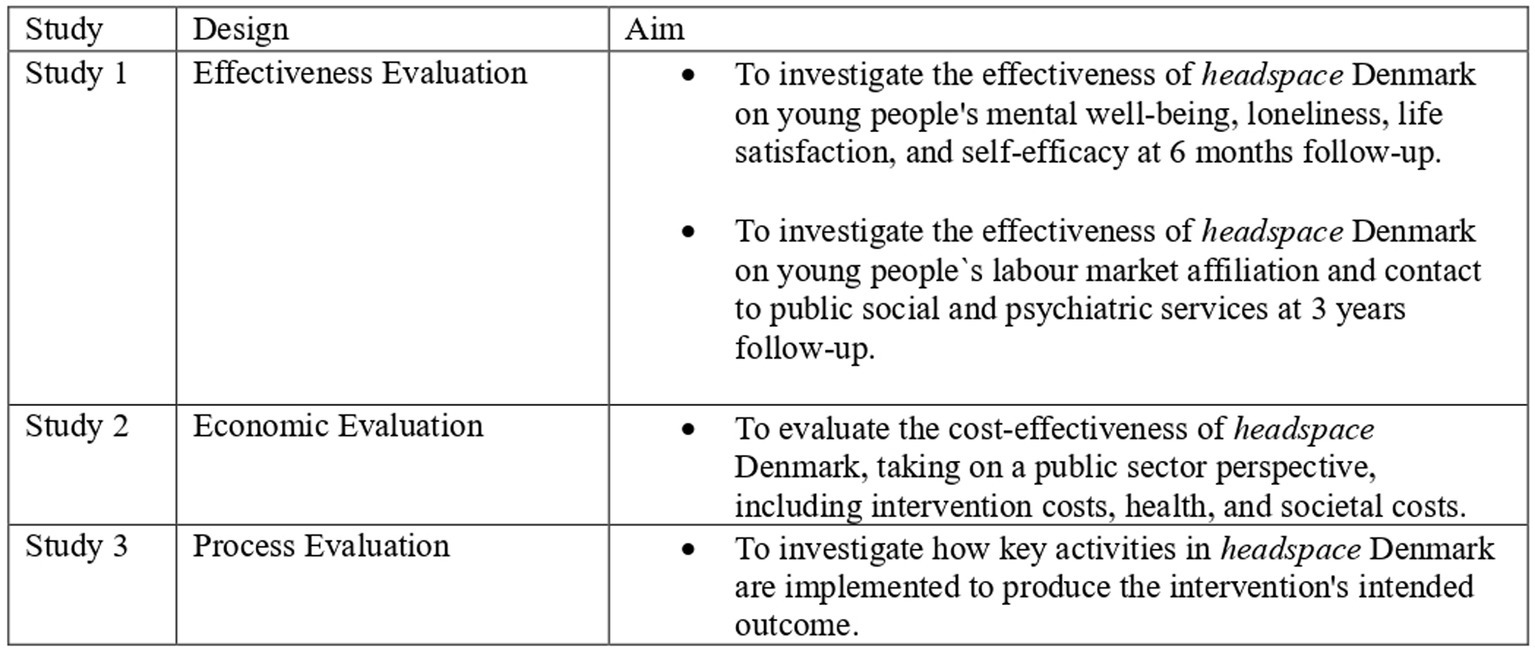
Figure 2. An overview of the three studies comprising the evaluation of headspace Denmark.
Study 1: effectiveness evaluation
Methods
Study design
The evaluation is designed as a propensity score matched quasi-experimental trial, meaning that a young person receiving counselling sessions at headspace will be matched by using propensity scores to six unexposed individuals (controls) based on several background characteristics with potential associations to headspace participation. The study will, by establishing a comparable control group, evaluate the results from the headspace group and measure whether headspace has any effect on mental wellbeing, loneliness, life satisfaction, and self-efficacy at 6 months follow-up, and measure the effects on labour market affiliation, and contact to public social and psychiatric services at 3 years follow-up.
Study sample
In total, 1,500 headspace service users are aimed for being included during the first 15 months of the study. The inclusion criteria for the intervention group are age between 12 and 25, participation in at least one counselling session in one of the physical national headspace centres, and willingness to give informed consent to participate in the study. Since some young people will have had one or more sessions at a headspace centre before the data collection begins, it is required that the first recorded measurement of young people is also their first actual session at a headspace centre. Young people attending the first session in headspace receive oral and written information about the study, from the counsellors. They are informed about the study’s purpose and procedures, including using questionnaires and register data. It is stressed that participation in the study is voluntary, and that declining to participate does not have any negative consequences for them, e.g., their right to receive counselling in headspace. Persons wanting to participate in the study are given a link, where they can log in to provide personal information (e.g., unique personal ID number, contact information), give informed consent and fill out questionnaires. Youth below 15 years are provided with a link to give to their parents/caregivers who need to provide consent before the person can participate in the study.
All included participants will be registered with their unique personal ID number which allows for individual-level linkage of information across nationwide registers provided by Statistics Denmark. Young people who do not want to provide their unique personal ID number cannot participate in the study. As headspace collects basic information on users, a supplementary analysis will be made comparing headspace users accepting registration on unique personal ID with headspace users not accepting to give their personal ID and participate in this evaluation. This comparison includes age, gender, and additional information on social and health-related problems faced by participants.
Procedures for matching the control group
The matching procedure must ensure that the control group is selected on significant prognostic characteristics, related to the young person contacting the headspace centre, which are like a participant in headspace. After 6 and 15 months of the 15 months inclusion period, controls are matched to the included headspace users using propensity score matching. Approximately 10,000 controls in total, living outside of the current headspace catchment area, will be matched. The repeated matching procedure is to ensure that the time lag between the headspace users’ survey response and the matched control can be reduced to 6 months. Table 1 presents an overview of the planned factors and registers in the matching.
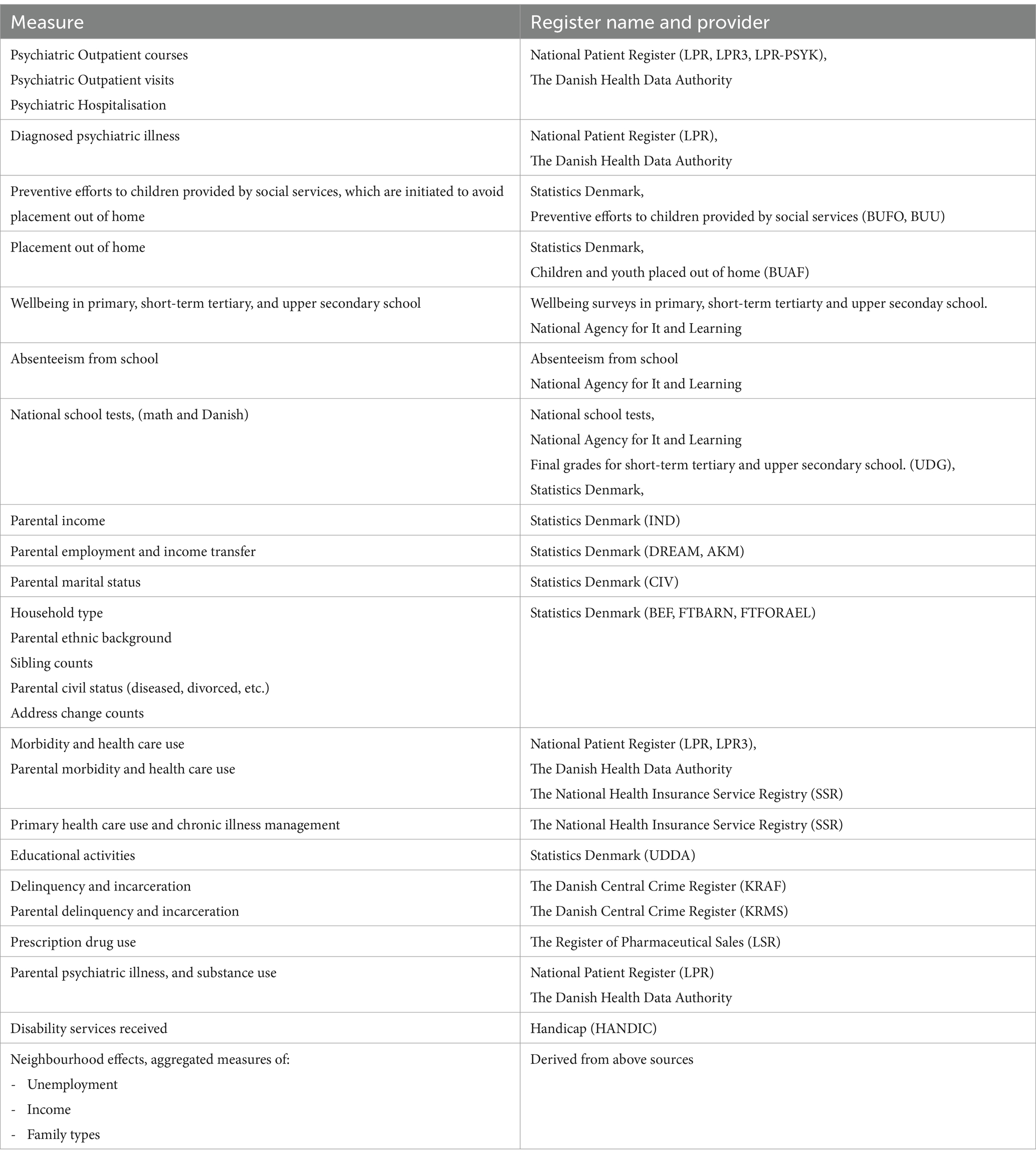
Table 1. Variables planned to be included in the matching procedure.
Propensity scores are estimated using regularised logistic regression (11), or a low-depth random forest with headspace participation as a binary outcome. The matching will be done using the probability score and an optimal matching algorithm that will select the six closest matches with a caliper threshold at or below 0.25 on the log (odds) transformation of the propensity score. No replacements will be used. Missing values in predictors are handled by adding missingness indicator categories to categorical data and by replacing missing data with model-based imputations or slicing numerical variables in quantiles and then adding a categorical indicator of missingness. Matching will be carried out in two repeated batches with no overlap or cross-sample replacement. When all baseline data is collected, the matching is reiterated for the whole pool of cases and controls to ensure optimal balance on all matching parameters, at the cost of a smaller control group. The matching parameters will include all self-reported outcomes (e.g., wellbeing, loneliness) and register-based outcomes (e.g., number of hospitalizations or outpatient contacts). The statistical power obtained for numerical outcomes is above 0.98 for Cohen’s D at 0.15, even in the case of a reduction of controls to a 2:1 ratio in the final matching.
Data collection and outcome measures
Outcome measures at 6 months follow-up
The 6 months follow-up will be based on survey data. Both the headspace group and the matched control group will be requested via a personal digital e-mail system, to answer an online questionnaire at baseline, which is the first contact with headspace, and at the 6 months follow-up. The questionnaires sent to the control group will be administered by Statistics Denmark. There will be a 6 months’ time difference between the headspace group and control group’s answers to the same questionnaires because the matching cannot take place until enough headspace participants are included in the study. The outcome measures are mental wellbeing, loneliness, life satisfaction and general self-efficacy, measured on the validated psychometric scales: The WHO Five Wellbeing Index (WHO-5) (21), Three-Item Loneliness Scale (18), Cantril’s ladder (16), EuroQol-5 Domain (EQ-5D-5L) (22), and general self-efficacy scale (23). A description of the outcome measures can be found in Appendix 2.
Outcome measures for 3 years follow-up
At the 3 years follow-up the following effect of headspace will be analysed using register-based data on the following outcomes:
1. Weeks in competitive employment or education in the follow-up period; The Employment Ministry’s longitudinal database (DREAM register data) (24).
2. Hours of work in the follow-up period; The Employment Ministry’s longitudinal database (DREAM register data) (24).
3. Type of education in the follow-up period; Statistics Denmark, highest completed education (UDDA).
4. The proportion receiving cash benefits or early retirement pension at follow-up: the Employment Ministry’s longitudinal database (DREAM register data) (24).
5. Number of admissions in a psychiatric hospital in the follow-up period; National Patient Register (LPR) (25).
6. Number of outpatient visits in psychiatric treatment in the follow-up period; National Patient Register (LPR) (25).
7. The number of social services received according to Danish Social Service Law. This includes personal social support §85, provided social activities §104 and housing for people with mental illness §83 and §85 (Statistic Denmark, Handicap services).
8. Days of school absence in the follow-up period; National Agency for It and Learning.
9. Wellbeing in primary, short-term tertiary and upper secondary school in the follow-up period; Wellbeing surveys in primary, short-term tertiarty and upper secondary school. National Agency for It and Learning.
10. Test scores from the National School tests (Danish and Math) in the follow-up period; National school tests, National Agency for It and Learning.
11. Exam grades in Primary School in the follow-up period; Final grades for short-term tertiary and upper secondary school (UDG), Statistics Denmark.
Data analysis
Sample size
A very conservative estimate of 1,900 participants with complete data at both baseline and follow-up (400 in headspace and 1,500 among controls), will provide 90% power to detect standardised mean differences of 0.18 in a two-sided t-test. This corresponds to 0.22 points on the WHO-5 Wellbeing Index, 1.16 points on the General Self-Efficacy scale and 0.36 points on Cantril’s Ladder. However, the statistical power might be degraded for analyses relying on multiple imputation because of the expected substantial proportion of missing data. The registry-based outcomes measured at 3 years of follow-up are unaffected by missingness and will have an expected 10,000 controls and 1,500 cases. This will provide statistical power sufficient for detecting small effect sizes, e.g., 83% power for detecting a 12.5 vs. 10% difference on a binary outcome.
Baseline characteristics for the two groups will be reported using means and standard deviations for numeric variables and count (n) with percentages for categorical variables. Mean difference from baseline to follow-up will be presented for both the headspace and the control group for all the included outcome measures. For normally distributed continuous outcomes a linear regression will be conducted to test the differences between the two groups. For non-normally distributed outcomes a proportional odds model will be used. The analyses for differences between groups will be adjusted for any baseline differences exceeding a predefined threshold. Moreover, subgroup analyses will be conducted where all analyses will be stratified for age (≥18 years). Missingness will affect the survey measures recorded at baseline and follow-up. Missing data will be handled using multiple imputations, possibly in combination with inverse probability weighting of observations (26). Imputation variables will be included from the complete (or near-complete) and co-occurring registry-based data observations as well as from all survey data collected up to the timepoint of the measure being imputed. A detailed statistical analysis plan (SAP) is also published and available at: https://archive.org/details/osf-registrations-9kzfd-v1.
Study 2: economic evaluation
The aim of the economic evaluation is to evaluate the cost-effectiveness of headspace, compared with a matched control group. The evaluation takes on a health care perspective when considering the costs of headspace, including intervention and health care costs. The study uses the same cohort as in the effectiveness evaluation, described above.
Outcome
Outcome for the cost-effectiveness analysis will be weeks in competitive employment or education during follow-up.
Costs
The total costs of individuals in contact with headspace including intervention costs will be estimated and compared with the costs of individuals in the control group. Non-parametric bootstrapped t-test analysis will be used to estimate the statistical significance of the cost difference between headspace participants and controls. Mean costs and p-values will be reported to show a statistically significant difference between the groups. Intervention costs will be estimated by using information on operating costs from the headspace centres.
Register data
All data will be drawn from Danish national registers. The study will include information on health care services (somatic and psychiatric inpatient and outpatient care, including emergency services and diagnosis related groups (DRG), general practitioners, dentists and other medical specialists, medical prescriptions) and social services. Differences in utilisation of health care will be reported in natural units and costs, while differences in utilisation of social services will be reported in natural units. All elements included in the analyses are described in more detail in Table 2.
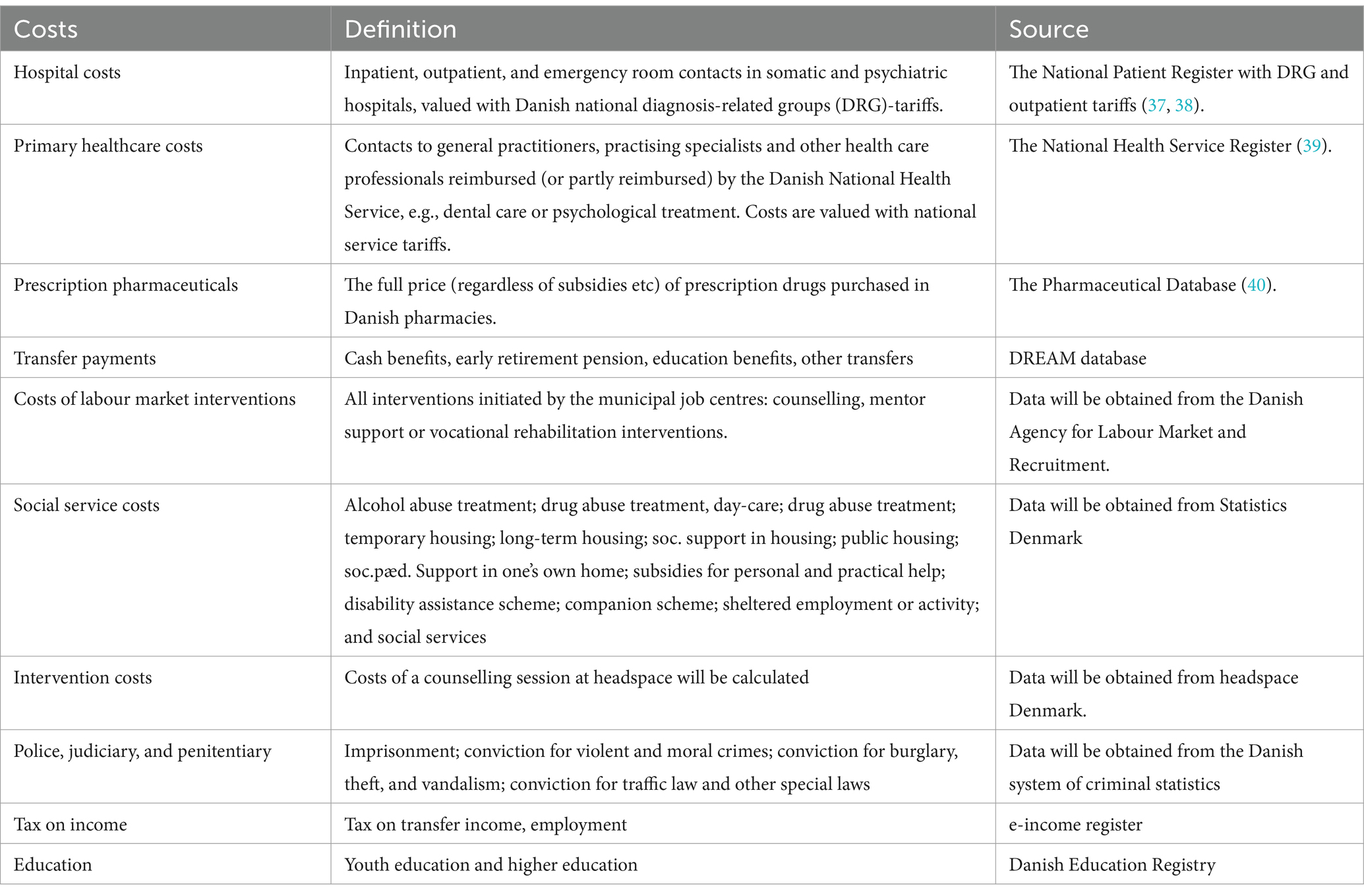
Table 2. Components included in the economic evaluation.
Cost-effectiveness analyses
The time horizon of the evaluation will be 3 years from the first contact to headspace. To evaluate cost-effectiveness, the incremental cost-effect ratio (ICER) will be estimated (27). The ICER represents the cost differences between the headspace group and the control group divided with differences in outcome measured by labour market contact/educational attainment. Nonparametric bootstrapping will be used to estimate confidence intervals of the mean differences of the groups. Predicted ICERs will be depicted on cost-effectiveness planes to show uncertainty therein. A cost-effectiveness acceptability curve will be generated to assess the probability of headspace being cost-effective when the decision-maker is willing to incur additional costs for an extra point increase in outcome up to a given threshold.
Study 3: process evaluation
The aim of the process evaluation is to investigate the implementation, context, and mechanisms of impact of the key activities in the headspace intervention. The focus of the study is the four key activities of headspace: (1) individual counselling with headspace volunteers, (2) bridging to established social and health services, (3) chat services (counselling and referral to individual counselling) and (4) community engagement where counsellors engage in community activities to obtain visibility regarding headspace and possibly also reduce stigma towards mental vulnerability. In line with the MRC guidelines (28), and as recommended by Moore et al. (29), the study will address the three aspects of the headspace intervention, implementation, mechanisms of change and context, through a multi-stakeholder perspective (Table 3).
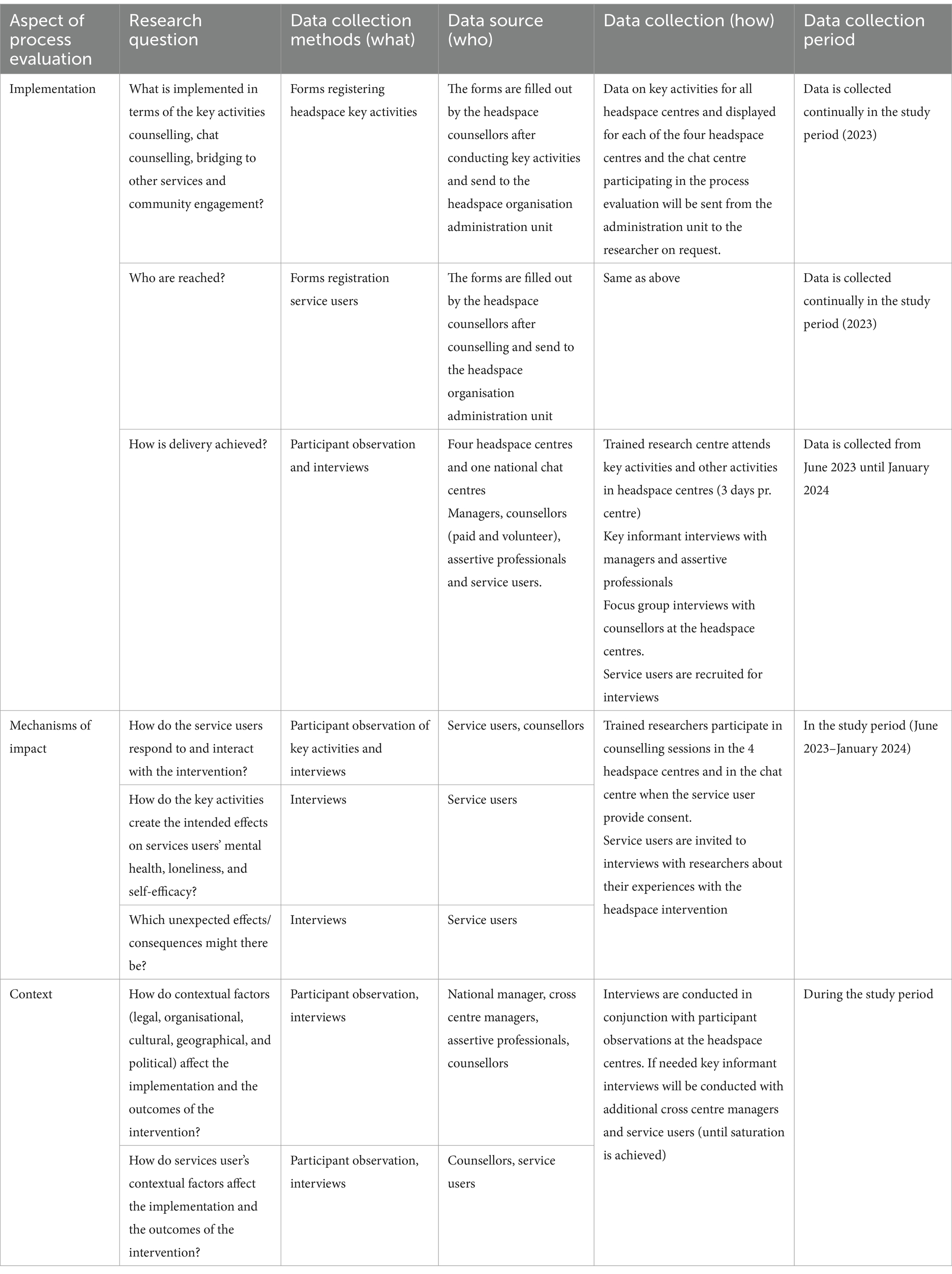
Table 3. Overview of research questions and data collection methods in the process evaluation of the headspace intervention.
Study participants and data collection methods
The process evaluation will predominantly deploy a qualitative research methodology, as it is suitable for investigating how the headspace intervention is implemented to produce its intended outcomes and how interactions, dynamics, and contextual factors influence implantation (29). This will be done by investigating the stakeholders’ interactions, experiences, and perspectives on the process. The stakeholders in this study are identified as the service users, the implementers, and the management of headspace Denmark. Thus, study participants are young people using headspace counselling, the counsellors (paid counsellors and volunteers) the assertive professionals, and the cross-centre management.
To explore and capture the complexity and nuances of how the intervention is delivered, the data collection will take place in four headspace centres in Denmark, and in the national chat enter and utilise a combination of data collection methods: semi-structured interviews (individual and focus group) and participant observations.
Implementation
Implementation can be defined as “the process through which interventions are delivered” (29). The delivery of the four key activities (counselling, chat counselling, bridging to other services, community engagement) in headspace is described through semi-structured interviews (individual and focus group) and observations of the stakeholders in the intervention: volunteer counsellors, paid counsellors, chat counsellors, assertive professionals, and managers (both cross-centre management and the national headspace CEO). Factors that support or impede the implementation of these four activities (e.g., training, knowledge sharing) are investigated. Participant observations will be used to gain a more in-depth understanding of how the activities are practised and how that adds nuances to the described experiences from the interviews (30). The implementation of key activities will also be described through interviews with service users and descriptions of their experiences in the headspace intervention. In addition to investigating the intervention delivery processes, the headspace intervention’s reach and dose will be described quantitatively with register data from the headspace centres.
Mechanisms of impact
Mechanisms of impact are defined as “the intermediate mechanisms through which intervention activities produce intended (or unintended) effects” for the individual service user (29). This study will describe possible mechanisms by which the key activities might create effects on service users’ loneliness, wellbeing, self-efficacy, and mental health (see Figure 1). The study will emphasise the perspectives of the service users and investigate their (possible) progression after engaging with headspace. If feasible, service users will be interviewed twice. The first interview is expected to take place right after the first counselling session. Previous evaluations have shown that service users engage in 2.7 counselling sessions on average (15). Follow-up interviews are expected to be conducted after the last counselling session and on average 4 months after the first session. This relatively short follow-up time (compared to study 1) will ensure that experiences regarding headspace are not too far away in memory and thus provide longitudinal information about the life course of each service user and their experienced benefits (or negative experiences from interacting with headspace personnel).
Context
Context is broadly understood as “factors external to the intervention which may influence its implementation, or whether its mechanisms of impact act as intended” (29). Contextual factors that might be relevant for the delivery and function of the headspace intervention can both be related to the context of the service user, the political and geographical context, the organisational context, the socio-economic context, legal and cultural context (31). Some variation in the way the headspace intervention works in different municipalities with different demographical and organisational settings is expected. To be able to address how these contextual factors might influence the implementation and functioning of the intervention, we will apply a sampling strategy with a high variation (for instance centres located in urban vs. rural areas) between cases (32). By understanding how the intervention possibly works differently or is implemented differently in different municipal contexts can give clues for how context affects implementation and mechanisms of impact (31).
Data analysis and integration
The quantitative data will be analysed, using descriptive statistics to provide information on the reach and dose of delivery of the headspace intervention. The data will be presented for all headspace centres in Denmark and the four headspace centres and the national chat centre participating in the process evaluation. The qualitative data is recorded digitally and transcribed ad verbatim, using NVivo software. The transcripts will be analysed thematically, using both a deductive approach with the preliminary programme theory as a point of the departure and an inductive approach for allowing unforeseen information and emerging themes to come forward. The findings of the process evaluation will not be reported to the centres continuously or used for quality improvement purposes, as the effectiveness evaluation attempts to evaluate the headspace intervention under “natural” circumstances. Thus, this process evaluation can be characterised as summative.
Ethics statement
The evaluation will be conducted in accordance with the present protocol, the Helsinki Declaration in its latest form, good clinical practise guidelines, and national and EU legislation on data management. The effectiveness evaluation, the cost-effectiveness evaluation and the process evaluation are not expected to pose any known adverse effects. For all studies, informed consent will be utilised in accordance with Danish and European legislation, and all service users who participate in the survey of questionnaires, observations and/or interviews will be secured anonymity (Privacy no. P-2022-602). Since the evaluation is not a biomedical study and because the intervention is conducted at the headspace centres, the protocol does not require acceptance from the Ethics Committee in the Capital Region of Denmark (Case number of correspondence with the Ethics Committee: 21061429).
Discussion
This paper presents the study protocol for three studies: an effectiveness, cost-effectiveness, and process evaluation of the headspace intervention in Denmark. Because the headspace model has achieved national endorsement and is fully implemented in 30 municipalities throughout Denmark there is an urgent need for scientific knowledge about the effectiveness of the intervention. The evaluation will contribute with new, important knowledge that not only will benefit headspace Denmark, but also contributes with new knowledge and documentation targeted to international mental health promotion initiatives, primary and lower secondary schools, educational institutions, and municipal social initiatives.
Overall, the three studies presented in this paper will bring new knowledge about the potential contribution and impact of headspace Denmark as a preventive intervention and contribute with new and useful knowledge about the possibly derived effects of counselling sessions in headspace. The large number of participants, as well as the establishment of a matched control group and long-term follow-up, makes it possible to provide more reliable and accurate estimates compared with previous studies.
The economic evaluation will contribute new knowledge about the cost-effectiveness of headspace Denmark, which can be used for a more nuanced societal prioritisation of resources allocated to vulnerable young people. Finally, the process evaluation will thoroughly describe the key activities of the Danish headspace intervention and document how these can be implemented in a local context and how they might create the expected effects on youth mental health and wellbeing. This valuable information can in a future perspective be used to further qualify the Danish headspace model.
Methodological challenges
Despite a comprehensive study design, some methodological challenges exist. The main limitation of this study is the design—that the effectiveness evaluation of the Danish headspace model is not performed as a randomised controlled trial, as it was not practically possible. The second most important limitation is difficulties in identifying a control group. We have tried to solve that by matching on failure to thrive, but we cannot identify the most important variable: help-seeking behaviour. Therefore, there is a risk that participants in the control group might have a better prognosis because they do not feel quite as bad (even though they have the same wellbeing and other match factors). There may also be a risk that participants in the headspace group have a better prognosis because they were able to seek and find help. There is also a risk that young people in the control group seek help from headspace centres after taking part in the study. Although the members of the control group live outside the catchment areas of the headspace centres, there might be a chance that some individuals contact the centres or the national chat centre during the study period. This introduces a risk of contamination, as both groups will be exposed to the intervention investigated. Young people in the control group who need help can use available social and health services, and mental health support offered in their community, but no signposting to specific organisations/services is provided in the material sent to the participants.
A potential pitfall in the effectiveness evaluation pertains to selection bias and the dynamics of outcomes before participation in the study (33). Young people’s mental health and wellbeing may be volatile with emotional ups and downs rather than persistent with the same levels of wellbeing over time, for instance shown in a study by Tegner Anker et al. (34). Youth would primarily seek help at “mental downturns,” that is at times with high level of emotional distress, there will be a regression to the mean, that might be difficult to identify in the control, thus posing a risk that natural improvements will be interpreted as effectiveness of the headspace intervention. While analysing the data, differences between the groups on all baseline outcomes will be tested for statistical significance. The analyses for differences between groups will be adjusted for any baseline differences with a p-value below 0.05.
Participants in the headspace group and the control group are matched on individual-level characteristics only. At the beginning of the data collection period, there were headspace centres in 22 out of the 100 municipalities of Denmark, meaning that it was not hard to identify controls. There were headspace centres is the four largest cities of Denmark (Copenhagen, Aarhus, Odense, and Aalborg) but not in some of the other larger cities such as Silkeborg or Kolding. There could be unobserved municipality-level factors potentially affecting the treatment effect estimates, e.g., related to urban density or distance to urban centres. We have, however, seen no substantial problems for the matching algorithm to identify comparable controls on the observed factors. We would also, from a pragmatic point of view, expect important municipality-level differences to be captured by the range of individual-level matching factors used (e.g., social status).
A limitation in the effectiveness evaluation may be that not all the register-based data will be completely updated at the time of matching. However, historical data such as national school tests, and wellbeing at primary school is expected to be prognostic and relevant to use in the matching. Moreover, many but not all the registers are updated in real-time such as the National Patient Register, which is available from The Danish Health Data Authority after a few days. Moreover, the matching procedure will be repeated before conducting the 3 years effect analyses, where all data will be updated at the time of matching. A limitation in using surveys as data collection methods is that respondents constitute a sample of the population rather than the whole population of headspace service users. As headspace collects basic information on service users, a supplementary analysis will be performed, comparing headspace users accepting registration on unique personal ID with headspace users not accepting to give their personal ID and participate in this evaluation. The comparison includes age, gender and additional information on social and health-related problems faced by participants. The process evaluation must consider, the flexibility of the headspace intervention. Key principles in the headspace model necessitate a person-centred approach where the consultation is guided by what is on the mind of the young person seeking support. Also, the counsellors are encouraged to take ownership in the local headspace centres and initiatives to develop local services. Although the sampling strategy is based on maximal variations with respect to factors such as urban/rural locations, new/old centres and high/low community engagement, there might be other important factors not considered in the selection of centres that affect how the headspace intervention is implemented and works, thus comprising the external validity of the findings.
Also, the evaluation’s limitation pertains to potential bias in the volunteer-based counselling model offered in the headspace centres, which may affect issues related to the outcomes and implementation. The young people seeking counselling in headspace may be characterised by distinct features (e.g., related to motivations, and skills) compared to the whole population of youth with mental health problems. Moreover, the young people who participate in the studies might be different from the group of service users in headspace. They may already have positive attitudes and expectations towards counselling. This potential selection bias might lead to an overestimation of the effectiveness of the counselling offered in headspace (35). Another limitation of the volunteer-based counselling model is that the counsellors posit varying levels of skills and competencies, which may lead to inconsistent quality of counselling. Although training is provided to the counsellors before and during their involvement in headspace, there is a risk that the effectiveness of the counselling model depends on the counsellors` experiences rather than the model itself. To ensure that the headspace intervention is implemented as intended and strengthen the quality of the counselling services provided in headspace centres, a fidelity scale will be developed based on the findings from the process evaluation (36).
Ethics statement
Since the evaluation is not a biomedical study and because the intervention is conducted at the headspace centres, the protocol does not require acceptance from the Ethics Committee in the Capital Region of Denmark (Case number of correspondence with the Ethics Committee: 21061429). The evaluation of headspace will be conducted in accordance with the Helsinki Declaration, and informed consent will be used for all research in compliance with Danish and European law. Anonymity will be guaranteed to all service users who take part in surveys using questionnaires, observations, and/or interviews.
Author contributions
SB: Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. TC: Conceptualization, Funding acquisition, Methodology, Writing – original draft, Writing – review & editing. RP: Conceptualization, Funding acquisition, Methodology, Writing – review & editing. AR: Conceptualization, Funding acquisition, Writing – review & editing. AT: Conceptualization, Funding acquisition, Writing – review & editing. MN: Conceptualization, Funding acquisition, Writing – review & editing. AB: Methodology, Writing – review & editing. LH: Methodology, Writing – review & editing. MU: Formal analysis, Investigation, Methodology, Writing – review & editing. LE: Conceptualization, Formal analysis, Funding acquisition, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was supported by the Trygfonden (Grant no. 153506) and Det Sociale Netvaerk.
Acknowledgments
The authors want to thank the headspace personnel, volunteers and paid counsellors, managers, central management, and service users, as well as research coordinators and research assistants for their involvement in the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1491756/full#supplementary-material
References
1. McGorry, PD, Mei, C, Dalal, N, Alvarez-Jimenez, M, Blakemore, SJ, Browne, V, et al. The lancet psychiatry commission on youth mental health. Lancet Psychiatry. (2024) 11:731–74. doi: 10.1016/S2215-0366(24)00163-9
2. Fusar-Poli, P, Correll, CU, Arango, C, Berk, M, Patel, V, and Ioannidis, JPA. Preventive psychiatry: a blueprint for improving the mental health of young people. World Psychiatry. (2021) 20:200–21. doi: 10.1002/wps.20869
3. Solmi, M, Radua, J, Olivola, M, Croce, E, Soardo, L, Salazar de Pablo, G, et al. Age at onset of mental disorders worldwide: large-scale meta-analysis of 192 epidemiological studies. Mol Psychiatry. (2022) 27:281–95. doi: 10.1038/s41380-021-01161-7
4. Castelpietra, G, Knudsen, AKS, Agardh, EE, Armocida, B, Beghi, M, Iburg, KM, et al. The burden of mental disorders, substance use disorders and self-harm among young people in Europe, 1990–2019: findings from the global burden of disease study 2019. Lancet Reg Health-Eur. (2022) 16:100341. doi: 10.1016/j.lanepe.2022.100341
5. Jeppesen, P. Mental Sundhed Og Sygdom Hos Børn Og Unge i Alderen 10–24 År: Forekomst, Udvikling Og Forebyggelsesmuligheder. Toronto: Vidensråd for Forebyggelse (2020).
7. Rodwell, L, Romaniuk, H, Nilsen, W, Carlin, JB, Lee, KJ, and Patton, GC. Adolescent mental health and behavioural predictors of being NEET: a prospective study of young adults not in employment, education, or training. Psychol Med. (2018) 48:861–71. doi: 10.1017/S0033291717002434
8. Gariépy, G, Danna, SM, Hawke, L, Henderson, J, and Iyer, SN. The mental health of young people who are not in education, employment, or training: a systematic review and meta-analysis. Soc Psychiatry Psychiatr Epidemiol. (2022) 57:1107–21. doi: 10.1007/s00127-021-02212-8
9. Dalsgaard, S, McGrath, J, Østergaard, SD, Wray, NR, Pedersen, CB, Mortensen, PB, et al. Association of Mental Disorder in childhood and adolescence with subsequent educational achievement. JAMA Psychiatry. (2020) 77:797–805. doi: 10.1001/jamapsychiatry.2020.0217
10. Kessler, RC. The costs of depression. Psychiatr Clin North Am. (2012) 35:1–14. doi: 10.1016/j.psc.2011.11.005
11. Philipson, A, Alaie, I, Ssegonja, R, Imberg, H, Copeland, W, Möller, M, et al. Adolescent depression and subsequent earnings across early to middle adulthood: a 25-year longitudinal cohort study. Epidemiol Psychiatr Sci. (2020) 29:e123. doi: 10.1017/S2045796020000360
12. Radez, J, Reardon, T, Creswell, C, Lawrence, PJ, Evdoka-Burton, G, and Waite, P. Why do children and adolescents (not) seek and access professional help for their mental health problems? A systematic review of quantitative and qualitative studies. Eur Child Adolesc Psychiatry. (2021) 30:183–211. doi: 10.1007/s00787-019-01469-4
13. Westberg, KH, Nyholm, M, Nygren, JM, and Svedberg, P. Mental health problems among young people—a scoping review of help-seeking. Int J Environ Res Public Health. (2022) 19:1430. doi: 10.3390/ijerph19031430
14. McGorry, PD, Mei, C, Chanen, A, Hodges, C, Alvarez-Jimenez, M, and Killackey, E. Designing and scaling up integrated youth mental health care. World Psychiatry. (2022) 21:61–76. doi: 10.1002/wps.20938
15. Rambøll Management Consulting. Evaluering Af Headspace. Virkninger for Den Enkelte Og for Samfundet. Hannemanns Allé, København S: Rambøll. (2019).
16. Levin, KA, and Currie, C. Reliability and validity of an adapted version of the Cantril ladder for use with adolescent samples. Soc Indic Res. (2014) 119:1047–63. doi: 10.1007/s11205-013-0507-4
17. Evans, C, Connell, J, Audin, K, Sinclair, A, and Barkham, M. Rationale and development of a general population well-being measure: psychometric status of the GP-CORE in a student sample. Br J Guid Couns. (2005) 33:153–73. doi: 10.1080/03069880500132581
18. Hughes, ME, Waite, LJ, Hawkley, LC, and Cacioppo, JT. A short scale for measuring loneliness in large surveys. Res Aging. (2004) 26:655–72. doi: 10.1177/0164027504268574
19. Rickwood, D, McEachran, J, Saw, A, Telford, N, Trethowan, J, and McGorry, P. Sixteen years of innovation in youth mental healthcare: outcomes for young people attending Australia’s headspace Centre services. PLoS One. (2023) 18:e0282040. doi: 10.1371/journal.pone.0282040
20. Matthay, EC, Hagan, E, Gottlieb, LM, Tan, ML, Vlahov, D, Adler, N, et al. Powering population health research: considerations for plausible and actionable effect sizes. SSM-Popul Health. (2021) 14:100789. doi: 10.1016/j.ssmph.2021.100789
21. Topp, CW, Østergaard, SD, Søndergaard, S, and Bech, P. The WHO-5 well-being index: a systematic review of the literature. Psychother Psychosom. (2015) 84:167–76. doi: 10.1159/000376585
22. Jensen, MB, Jensen, CE, Gudex, C, Pedersen, KM, Sørensen, SS, and Ehlers, LH. Danish population health measured by the EQ-5D-5L. Scand J Public Health. (2023) 51:241–9. doi: 10.1177/14034948211058060
23. Scholz, U, Doña, BG, Sud, S, and Schwarzer, R. Is general self-efficacy a universal construct? Psychometric findings from 25 countries. Eur J Psychol Assess. (2002) 18:242–51. doi: 10.1027//1015-5759.18.3.242
24. Burr, H, Pedersen, J, and Hansen, J. Work environment as predictor of long-term sickness absence: linkage of self-reported DWECS data with the DREAM register. Scand J Public Health. (2011) 39:147–52. doi: 10.1177/1403494811401480
25. Andersen, TF, Madsen, M, Jørgensen, J, Mellemkjoer, L, and Olsen, JH. The Danish National Hospital Register. A valuable source of data for modern health sciences. Dan Med Bull. (1999) 46:263–8.
26. Seaman, SR, White, IR, Copas, AJ, and Li, L. Combining multiple imputation and inverse-probability weighting. Biometrics. (2012) 68:129–37. doi: 10.1111/j.1541-0420.2011.01666.x
27. Glick, HA, Doshi, JA, Sonnad, SS, and Polsky, D. Economic evaluation in clinical trials. Oxford: OUP Oxford (2014).
28. Skivington, K, Matthews, L, Simpson, SA, Craig, P, Baird, J, Blazeby, JM, et al. Framework for the development and evaluation of complex interventions: gap analysis, workshop and consultation-informed update. Health Technol Assess Winch Engl. (2021) 25:1–132. doi: 10.3310/hta25570
29. Moore, GF, Audrey, S, Barker, M, Bond, L, Bonell, C, Hardeman, W, et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ. (2015) 350:h1258. doi: 10.1136/bmj.h1258
31. Craig, P, Di Ruggiero, E, Frolich, KL, Mykhalovskiy, E, White, M, Campbell, R, et al. Taking account of context in population health intervention research: Guidance for producers, users and funders of research. NIHR J. Libr. (2018). doi: 10.3310/CIHR-NIHR-01
32. Malterud, K, Siersma, VD, and Guassora, AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. (2016) 26:1753–60. doi: 10.1177/1049732315617444
33. Heckman, JJ, and Smith, JA. The pre-programme earnings dip and the determinants of participation in a social Programme. Implications for simple Programme evaluation strategies. Econ J. (1999) 109:313–48.
34. Tegner Anker, AS, Hald Andersen, S, and Andersen, H. Within-Individual Variability in Well Being among Late Adolescents. Ny Kongensgade, Copenhagen, Denmark: The ROCKWOOL Foundation Research Unit. (2024).
35. Tripepi, G, Jager, KJ, Dekker, FW, and Zoccali, C. Selection bias and information bias in clinical research. Nephron Clin Pract. (2010) 115:c94–9. doi: 10.1159/000312871
37. Ankjær-Jensen, A, Rosling, P, and Bilde, L. Variable prospective financing in the Danish hospital sector and the development of a Danish case-mix system. Health Care Manag Sci. (2006) 9:259–68. doi: 10.1007/s10729-006-9093-1
38. Lynge, E, Sandegaard, JL, and Rebolj, M. The Danish national patient register. Scand J Public Health. (2011) 39:30–3. doi: 10.1177/1403494811401482
39. Sahl Andersen, J, De Fine Olivarius, N, and Krasnik, A. The Danish national health service register. Scand J Public Health. (2011) 39:34–7. doi: 10.1177/1403494810394718
40. Wallach Kildemoes, H, Toft Sørensen, H, and Hallas, J. The Danish national prescription registry. Scand J Public Health. (2011) 39:38–41. doi: 10.1177/1403494810394717
Keywords: youth mental health, volunteerism, complex intervention, civic society, anti-stigma
Citation: Bjørkedal STB, Christensen TN, Poulsen RM, Ranning A, Thorup AAE, Nordentoft M, Bojesen AB, Hastrup LH, Ustrup M and Eplov LF (2025) Study protocol: an effectiveness, cost-effectiveness, and process evaluation of headspace Denmark. Front. Public Health. 13:1491756. doi: 10.3389/fpubh.2025.1491756
Edited by:
Renato de Filippis, University Magna Graecia of Catanzaro, ItalyReviewed by:
Patrick Köck, Clinic and Care Center Barmelweid, SwitzerlandRhiannon Packer, Cardiff Metropolitan University, United Kingdom
Jacob Nielsen Arendt, Rockwool Foundation, Denmark
Copyright © 2025 Bjørkedal, Christensen, Poulsen, Ranning, Thorup, Nordentoft, Bojesen, Hastrup, Ustrup and Eplov. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Siv T. B. Bjørkedal, c2l2LXRoZXJlc2UuYm9nZXZpay5iam9lcmtlZGFsQHJlZ2lvbmguZGs=