 Zhenbo Tao
Zhenbo Tao Qianqian Xu
Qianqian Xu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 19 February 2025
Sec. Public Health Education and Promotion
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1487400
Background: This study examined the associations between health literacy and smoking behaviors among residents in Ningbo City, Zhejiang Province, China, investigating both the impact of health literacy on smoking prevalence and intensity, and its potential role in smoking cessation interventions.
Methods: This cross-sectional study analyzed data from 2,948 male participants in the 2023 Health Literacy and Tobacco Use Surveillance Survey. We applied logistic regression models and restricted cubic spline analyses to assess the association between health literacy and smoking behaviors, adjusting for demographic characteristics, socioeconomic factors, and self-reported health status.
Results: Our findings indicate that higher levels of health literacy are associated with significantly lower rates of smoking (OR = 0.643, 95%CI = 0.528, 0.783) and daily cigarette consumption (β = −1.938, 95%CI = −3.649, −0.228). Non-smokers with higher health literacy were more likely to discourage others from smoking (OR = 1.464, 95%CI = 1.096, 1.955), underscoring health literacy’s crucial role in smoking prevention and control. A nonlinear relationship between health literacy and smoking behavior was identified.
Conclusion: Health literacy significantly influences smoking behavior, with higher literacy levels associated with reduced smoking prevalence and intensity. These findings support incorporating health literacy enhancement into comprehensive smoking cessation strategies.
Tobacco use remains a critical global public health challenge that threatens both population health and social development. According to the World Health Organization (WHO) report in 2019, approximately 1.14 billion people aged 15 years and older use tobacco products globally, demonstrating the substantial scope of this public health crisis (1). This practice precipitates a multitude of diseases and stands as a principal contributor to premature mortality and disability worldwide. The linkage between smoking and an array of health complications, including cardiovascular diseases, cancer, and respiratory disorders, has been thoroughly substantiated through research (2), elevating the health risks associated with tobacco use to a critical public health dilemma (3). The WHO’s findings reveal that tobacco use is responsible for over 8 million deaths annually, with direct smoking attributing to around 7 million fatalities and secondhand smoke exposure causing 1.3 million deaths (1). China, home to nearly 20% of the global population, is responsible for more than 40% of the world’s total cigarette consumption, leading to over 1 million tobacco-related deaths each year, predominantly among male smokers (4). Research has identified smoking as the leading risk factor for male mortality (5), emphasizing the urgent need for comprehensive strategies to address this public health threat.
In the modern era, health literacy (HL) has gained significant traction as a subject of vital concern, referring to an individual’s ability to obtain, understand, evaluate, and apply health-related information to make informed decisions and actions affecting their health (6). Research underscores that insufficient HL can elevate mortality and hospitalization risks in individuals with chronic conditions (7), and adversely affect daily dietary choices (8). Conversely, enhanced HL is linked to improved health outcomes in children and adolescents (9), a decreased propensity for health-risk behaviors, and fewer negative health consequences (10). Moreover, HL plays a crucial role in heightening awareness about pressing health challenges, including COVID-19 (11). As reported in 2022, the average HL level among Chinese residents was a mere 23.15%, revealing that a staggering majority, over three-quarters of the population, possesses inadequate HL skills (12). This stark reality underscores the urgent need for targeted interventions to bolster HL, aiming to improve public health outcomes and resilience against health threats.
Recent studies have illuminated various risk factors that influence smoking behavior, underscoring the complex interplay between HL and such behaviors. Factors affecting HL, including age, socioeconomic status, education, and occupation, have shown significant overlap with determinants of smoking habits (5, 13). This correlation suggests that populations with lower HL levels frequently exhibit higher rates of smoking. Furthermore, evidence indicates a pronounced link between HL and smoking-related behaviors and outcomes; individuals with greater HL are more inclined toward initiating smoking cessation efforts (14) and exhibit a reduced tendency for relapse following cessation interventions (15). However, the relationship between HL, awareness of smoking hazards, the intensity of smoking habits, and the discouragement of smoking among peers remains underexplored.
This study aims to address these knowledge gaps by examining the relationship between HL and smoking behaviors among residents of Ningbo City, with three specific objectives: (1) to examine the association between HL and smoking patterns, (2) to assess the influence of HL on smoking intensity, and (3) to evaluate HL’s role in promoting smoking prevention through social networks. These findings could inform the development of smoking cessation interventions that integrate HL as a key component of tobacco control strategies.
This manuscript describes a cross-sectional investigation leveraging data from the 2023 Health Literacy and Tobacco Use Surveillance Survey, executed among the populace of Ningbo City, Zhejiang Province. The cohort for this study comprised permanent residents within the age bracket of 15 to 69 years, who had been residing continuously in the designated survey area for a minimum duration of 6 months.
Prior to initiating the survey, comprehensive details concerning the study’s objectives, alongside the voluntary and anonymous nature of participation, were communicated to all prospective respondents. Participants were required to have a thorough understanding of the provided written informed consent information and to have explicitly agreed to partake in the survey beforehand.
The sampling framework of this investigation was anchored in the broader context of the Health Literacy and Tobacco Use Surveillance in Zhejiang Province. The primary aim was to elucidate the prevalence of HL among the provincial residents. To this end, a meticulous sample size determination was employed, guided by the following methodology:
The minimal requisite sample size for each county (district) was ascertained using the formula N = *deff. In 2019, the level of HL in Zhejiang was 29.49%, = 0.2949, the allowable relative error was set to 15%, and the allowable absolute error = 0.2949 * 0.15 = 0.0442, = 1.96, = 1. This calculation suggested a base sample size of 408 for each layer. Considering potential non-responses and invalid questionnaires, the sample size was adjusted to 640 for each county (district). Given Ningbo’s administrative structure comprising 10 counties (districts), the aggregate initial sample size was established at 6400 participants. Notably, the analysis was confined to male smokers due to the negligible representation of female smokers in the sample, with only nine instances reported. Following the exclusion of female participants and invalid questionnaires, the refined sample consisted of 2,948 respondents.
A stratified multi-stage probability sampling method proportional to population size was used in this study. The complete sampling process involved four sequential stages: (1) Ten counties (districts) in Ningbo City were each represented by the selection of four townships. (2) Within each chosen township, two segments were identified for further sampling. (3) A random selection of 120 households was conducted within each segment. (4) Utilizing a Kish grid, one participant was chosen from each household. This structured sampling approach was designed to ensure a representative and statistically robust sample, facilitating an accurate assessment of HL and tobacco use patterns within the targeted population.
The survey was meticulously conducted utilizing the Health Literacy and Tobacco Use Surveillance questionnaire, a comprehensive instrument partitioned into three distinct sections: personal characteristics, HL and smoking status, officially sanctioned by the Chinese Health Education Center. The reliability of the questionnaire was validated through an overall Cronbach’s alpha and Spearman-Brown coefficient of 0.95 and 0.94, respectively (16), indicating high internal consistency and reliability.
The first section collected demographic and personal information, including sex, age, marital status, educational attainment, profession, annual household income, and self-rated health status. These variables were essential for examining the factors influencing health literacy and smoking behaviors in the study population.
The subsequent section delved into HL, incorporating a variety of question types to assess this multifaceted concept. The HL assessment instrument comprises six core dimensions: scientific perspectives on health, prevention of infectious diseases, prevention of non-communicable diseases, safety and emergency response, basic healthcare services, and health information literacy. The questions were categorized into three formats: true/false (awarding 1 point for each correct response), single-answer multiple choice (with only one correct option, also yielding 1 point per correct answer), and multiple-answer multiple choice (where a correct response necessitated identifying all correct options without any incorrect selections). The aggregate maximum score attainable on this scale was 66 points, with a threshold score of 53 (representing 80% of the total score) delineated as the benchmark for adequate HL. Conversely, scores ranging from 0 to 52 were indicative of insufficient HL levels. The proportion of participants demonstrating sufficient HL relative to the total participant count was utilized to define the HL level (17).
The final part of the questionnaire concentrated on smoking behaviors, including the prevalence and frequency of smoking, alongside awareness regarding the hazards associated with smoking and second-hand smoke exposure. The assessment of knowledge concerning smoking dangers was structured around seven single-answer questions, with a full comprehension of the correct responses equated to an awareness of smoking-related risks. The specifics of these questions and their respective options are detailed in Table 1.
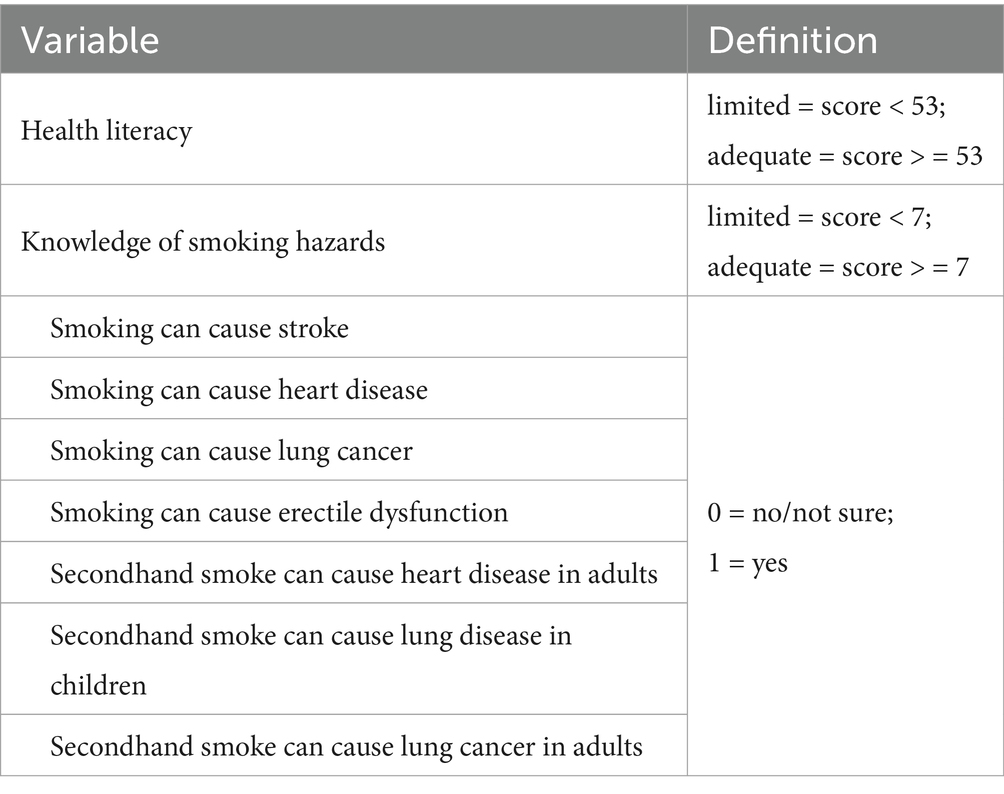
Table 1. Variable detail definition.
The survey was administered by trained investigators who completed standardized training before data collection to ensure consistency and data quality across all survey activities.
Data analysis was conducted using SPSS version 26.0 and R version 4.3.1. Statistical significance was set at a two-tailed p < 0.05. The Kolmogorov–Smirnov test assessed variable normality. For non-normally distributed variables, median values with quartiles were reported and compared using the Mann–Whitney U test. Categorical and ordinal variables were presented as ratios and compared using Pearson chi-square and Mann–Whitney U tests. Multiple logistic regression models were developed to examine relationships between smoking behavior, HL, and other variables, adjusting for covariates. A forest plot visualized the association between smoking habits and HL.
The cohort was bifurcated based on smoking status. Among smokers, a linear regression model was constructed to investigate the correlation between the frequency of weekly smoking and HL. Conversely, for non-smokers, a logistic regression model was devised to examine the linkage between the propensity to discourage smoking and HL. Within each model, key statistics including odds ratios (OR) or regression coefficients (β), 95% confidence intervals (CI), and p-values were systematically reported to elucidate the strength and significance of observed associations.
Lastly, to probe potential non-linear dynamics between smoking behaviors and HL, a restricted cubic spline (RCS) analysis was conducted. This sophisticated statistical technique allows for the exploration of complex relationships that might not be readily apparent or adequately described by linear models, offering nuanced insights into how varying levels of HL might influence smoking habits.
Definitions of HL and tobacco harm knowledge are presented in Table 1. Among 2,948 participants, 1,149 (38.98%) were smokers (Table 2). The prevalence of adequate HL was significantly lower in smokers (25.9%) compared to non-smokers (40.2%, p < 0.05).
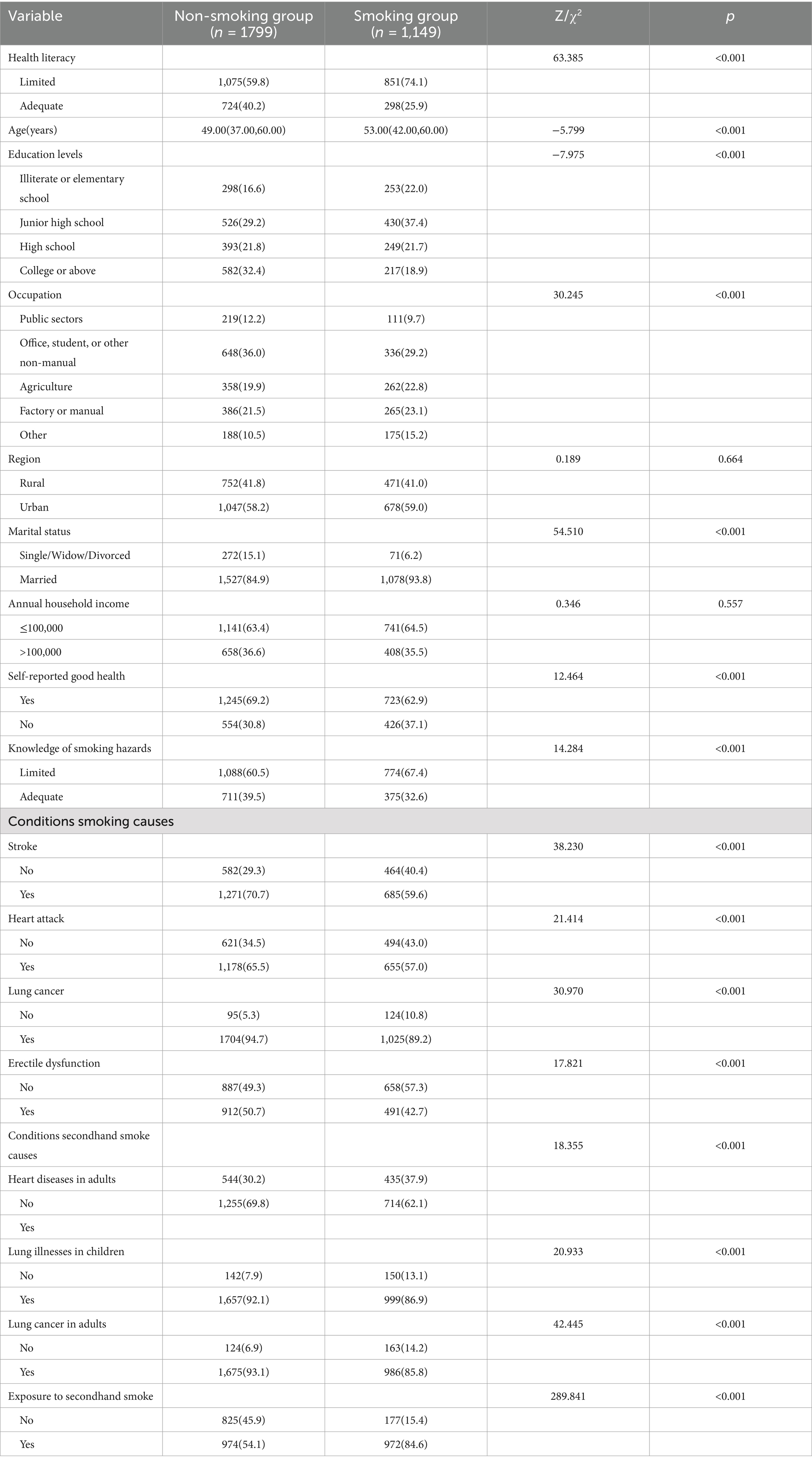
Table 2. Association between smoking status and basic characteristics.
Significant differences between smokers and non-smokers were observed in demographic and socio-economic characteristics. Smokers were generally older and had lower educational attainment. Smoking rates were lower among public sector employees, office workers, and students, but higher among agricultural and manual laborers. A higher proportion of smokers were married, and fewer smokers reported good self-rated health compared to non-smokers (p < 0.05 for all comparisons).
Annual income and urban–rural distribution showed no significant differences between smokers and non-smokers (p > 0.05). However, non-smokers demonstrated better awareness of tobacco-related health risks, including both direct smoking and secondhand smoke exposure (p < 0.05).
Logistic regression analyses of smoking determinants are presented in Table 3 and Figure 1. Three sequential models were constructed: Model 1 (unadjusted), Model 2 (adjusted for sociodemographic factors including age, education level, occupation, urban–rural status, marital status, annual income, and self-rated health), and Model 3 (further adjusted for smoking harm awareness and secondhand smoke exposure).
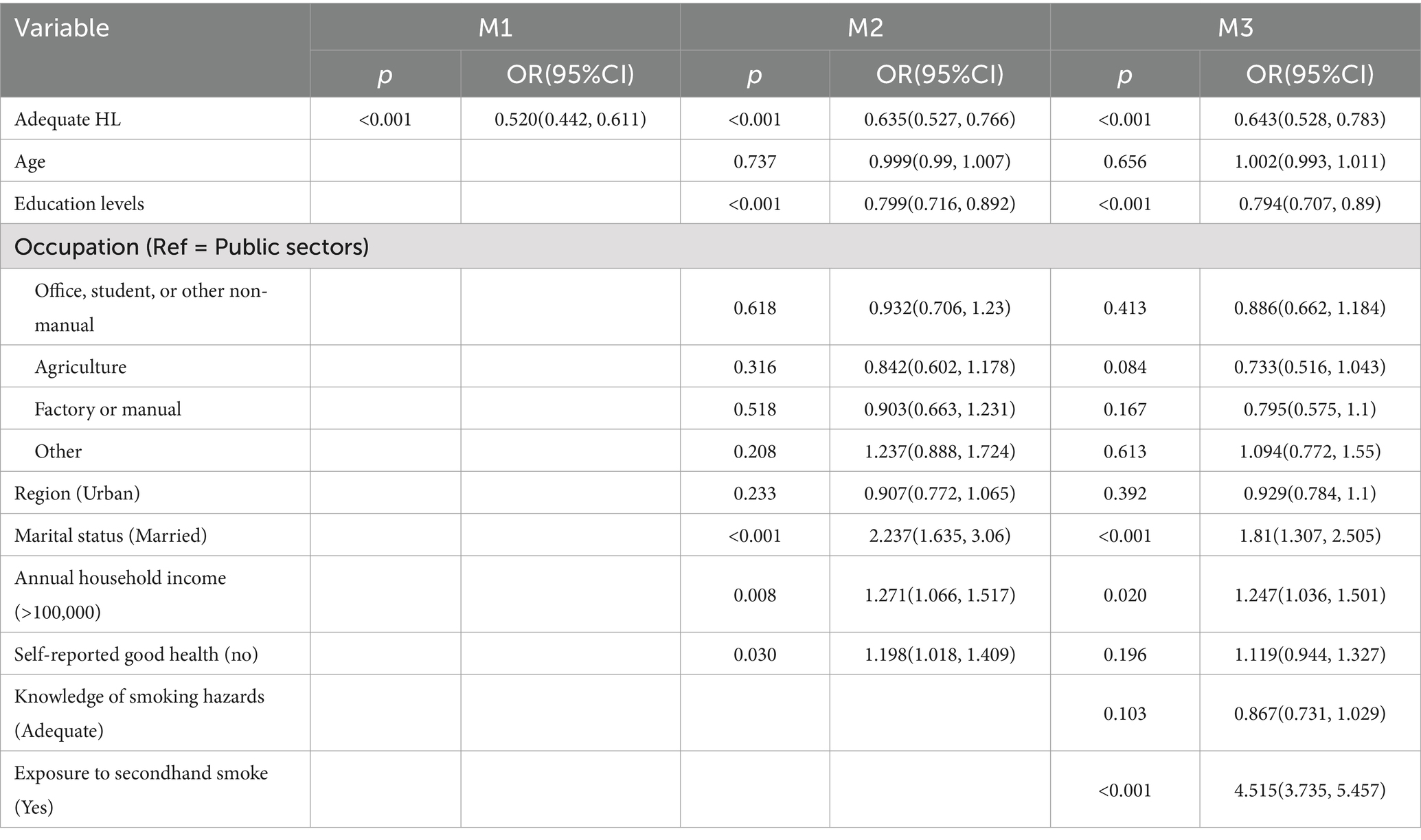
Table 3. Logistic regression analysis of smoking behavior.
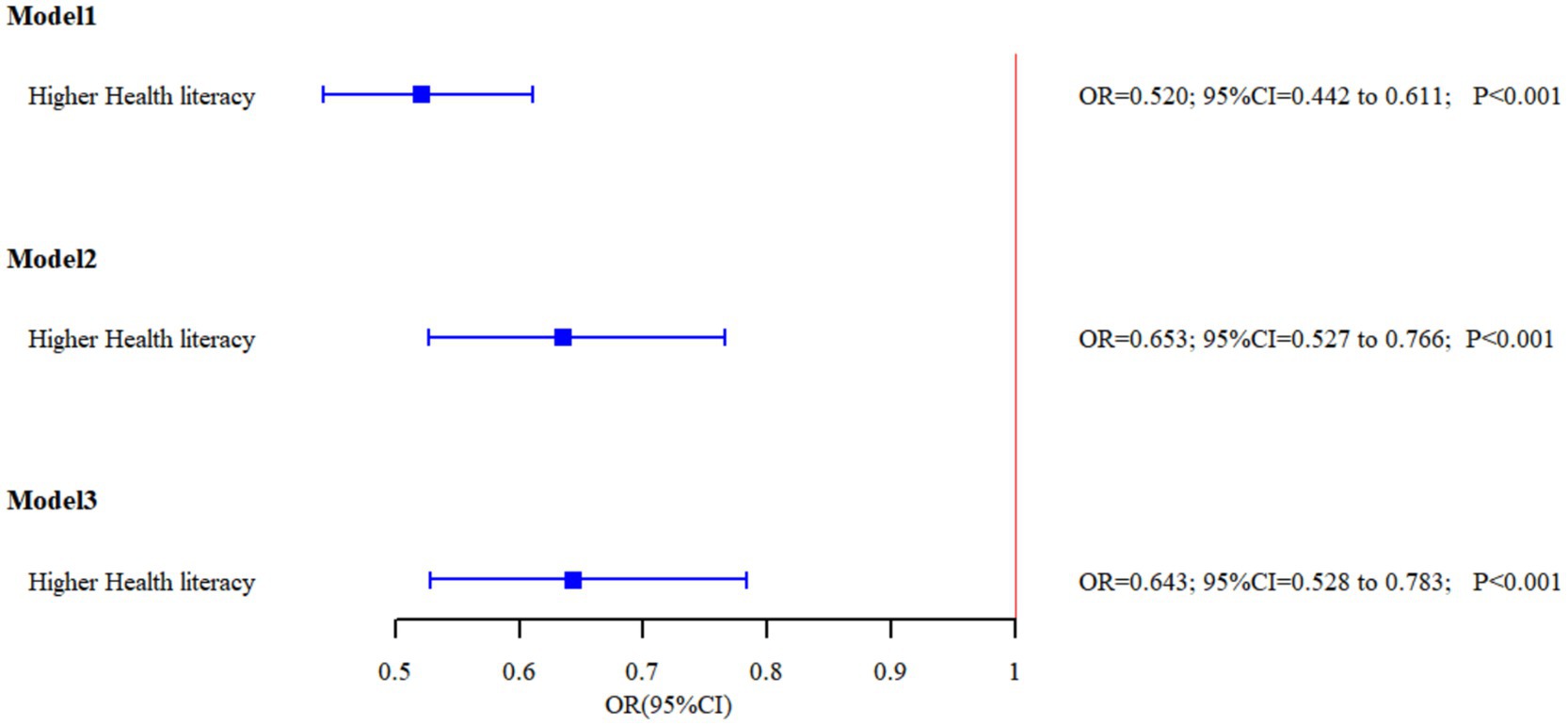
Figure 1. The relationship between HL and smoking behavior in the three models.
Across the three models, possessing HL consistently emerges as a protective factor against smoking, with individuals possessing HL showing lower rates of smoking (OR < 1). In Model 3, individuals with adequate HL exhibited a 35.7% reduction in smoking risk (OR = 0.643, 95%CI = 0.528, 0.783). Higher education levels are associated with lower smoking rates. Married individuals show higher smoking rates. Exposure to secondhand smoke on a regular basis is associated with higher smoking rates (OR = 4.515, 95%CI = 3.735, 5.457), indicating that individuals regularly exposed to secondhand smoke are 4.5 times more likely to be smokers compared to those without such exposure. However, awareness of the harms of smoking did not show a statistically significant impact on smoking behavior.
Table 4 presents the linear regression analysis of daily cigarette consumption among smokers. Adequate HL was consistently associated with lower smoking intensity across all models (β < 0). In the fully adjusted Model 3, adequate HL was associated with smoking approximately two fewer cigarettes per day (β = −1.938, 95%CI = −3.649, −0.228). Age showed a positive association with daily cigarette consumption, while higher education levels were associated with smoking fewer cigarettes. No other variables showed significant associations in the final model.
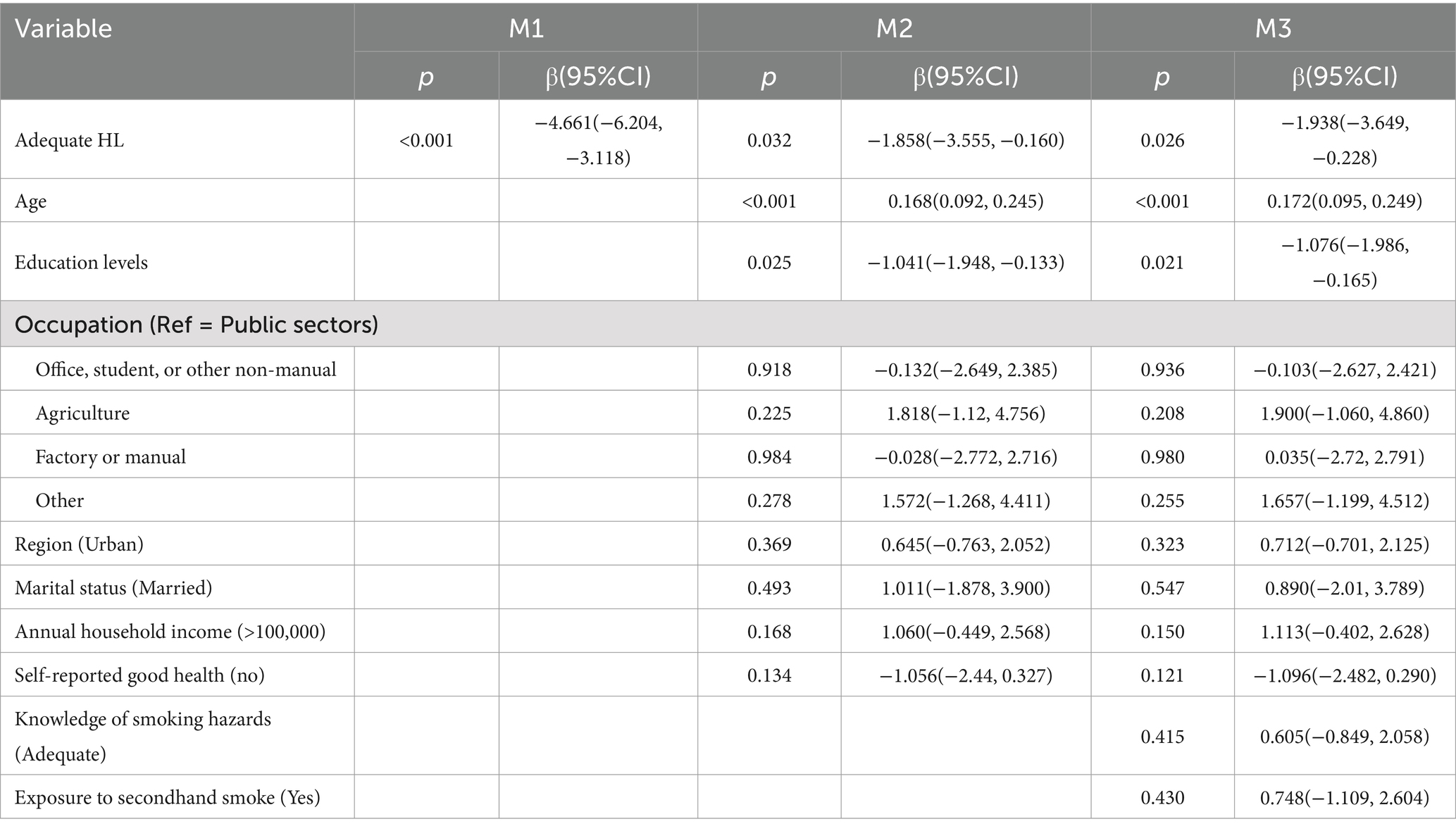
Table 4. Linear regression analysis of smoking severity.
The factors influencing non-smokers’ likelihood to discourage others from smoking were examined using logistic regression (Table 5). Adequate HL was consistently associated with a greater likelihood of discouraging smoking across all models. In the fully adjusted Model 3, individuals with adequate HL were 46.4% more likely to discourage others from smoking (OR = 1.464, 95%CI = 1.096, 1.955). Conversely, individuals who encounter secondhand smoke in their daily lives were less inclined to discourage smoking in others (OR = 0.527, 95%CI = 0.409, 0.680), indicating a potential desensitization or resignation to the prevalence of smoking behaviors. Other variables, such as age, educational level, and occupation, did not demonstrate statistical significance in Model 3.
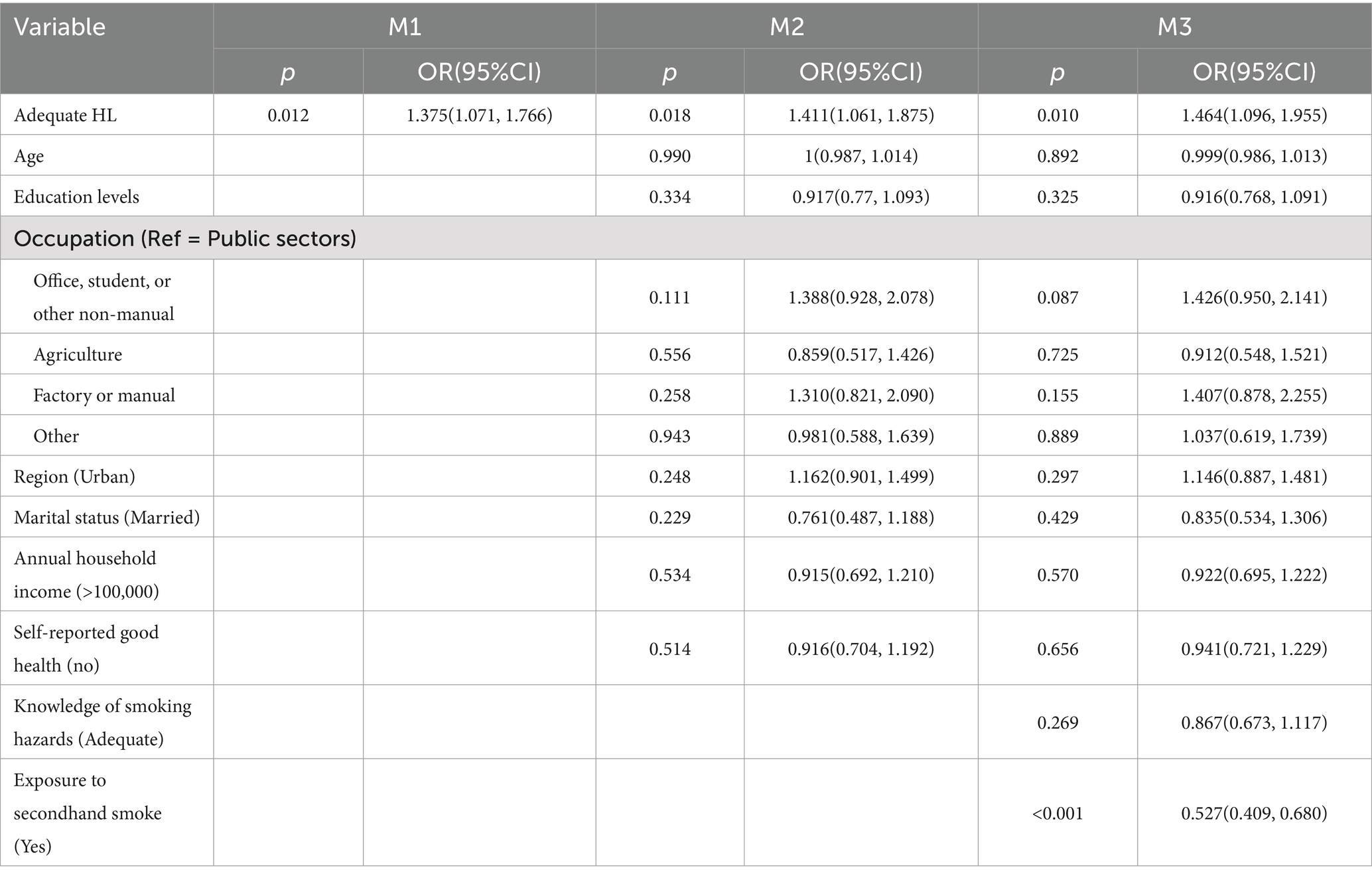
Table 5. Logistic regression analysis of dissuading others from smoking.
As shown in Figure 2, utilizing restricted cubic spline analysis, a nonlinear relationship between HL and smoking behavior was identified (p = 0.004). The inflection point was determined to be at a score of 47.83, it shows that the when HL is raised to this threshold, smoking behavior changes more.
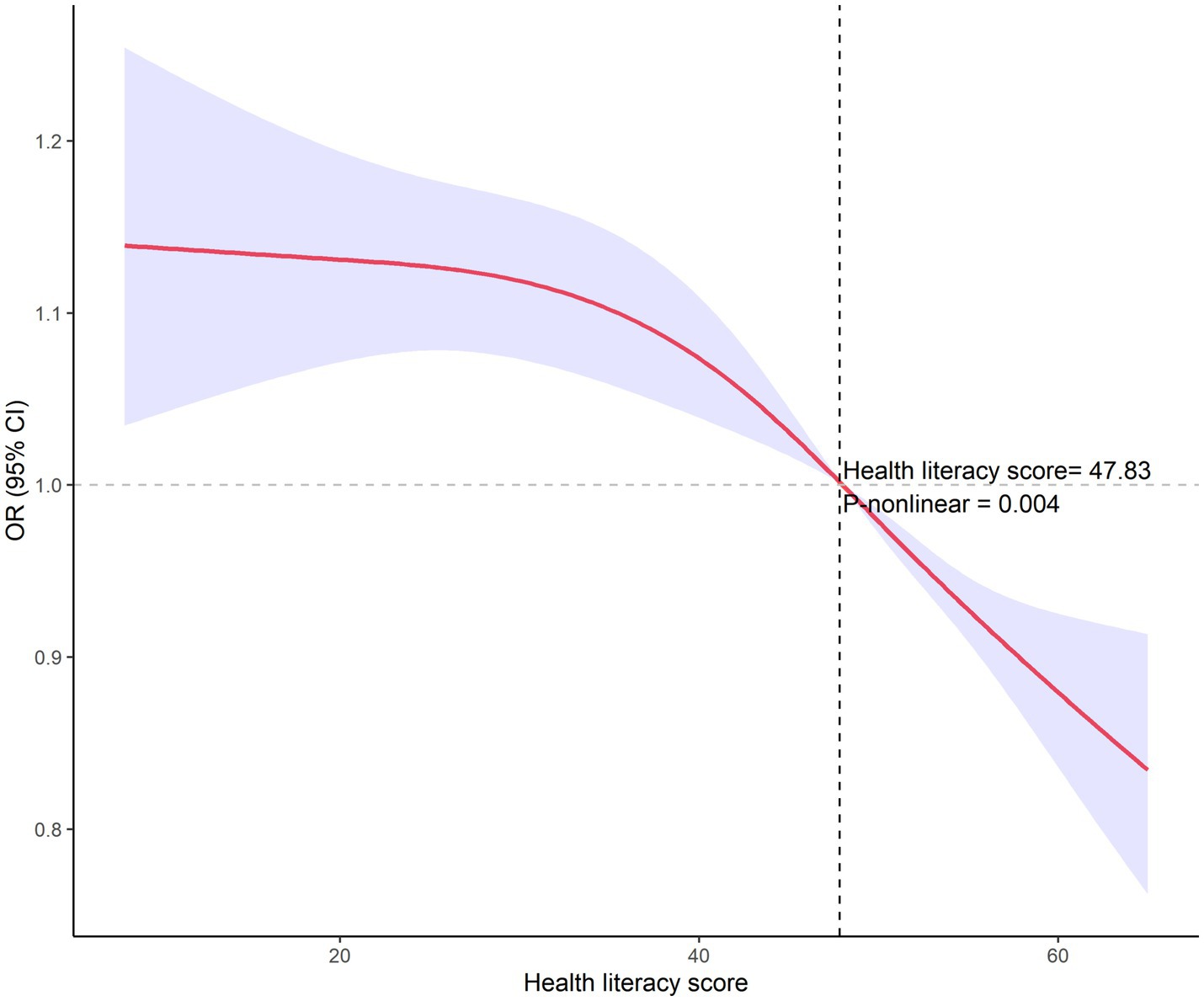
Figure 2. RCS analysis of health literacy and smoking behavior.
This study, conducted among the permanent residents of Ningbo City, examines the relationship between HL and smoking behavior, including the severity of such habits. Analyzing data from 2,948 participants, the study results in Table 2 showed that individuals with higher levels of HL exhibit significantly lower smoking rates compared to those with lower HL. After covariate-adjusted multifactor logistic regression, the results are still robust (Table 3; Figure 1). This observation aligns with previous research outcomes (12). HL levels influence both smoking awareness and behavior. Individuals with higher HL demonstrate better understanding of smoking’s health risks and greater tendency toward health-promoting behaviors, including smoking cessation and avoidance of smoking environments. In contrast, those with lower HL may have limited understanding of smoking risks, increasing their vulnerability to smoking culture influences. These findings emphasize the importance of enhancing population-level HL for effective smoking prevention and control.
Further analysis revealed additional dimensions of HL’s influence on smoking behavior. Among smokers, higher HL was associated with lower daily cigarette consumption (Table 4), demonstrating that HL affects not only smoking initiation but also smoking intensity. Moreover, non-smokers with higher HL levels showed greater likelihood of discouraging others from smoking (Table 5), suggesting HL’s role in promoting smoking prevention through social networks. The restricted cubic spline analysis revealed a significant nonlinear relationship between HL and smoking behavior, with an inflection point at a score of 47.83 (Figure 2). The analysis demonstrated that the protective effect against smoking was most pronounced at HL scores above this threshold, with progressively decreasing odds of smoking as HL levels increased. This nonlinear relationship provides valuable insights for public health interventions, suggesting that efforts to improve population HL levels could yield substantial benefits for smoking control.
Beyond the relationship between HL and smoking, our analysis revealed significant demographic differences between smokers and non-smokers, particularly regarding age and education. Higher smoking rates among older individuals suggest generational variations in health behavior perceptions and responses to different life stage pressures. In alignment with the bulk of existing research, individuals with higher educational attainment exhibit a lower risk of smoking, a risk that escalates with age (18, 19). Those with a higher level of education have easier access to information about the harms of tobacco and are more likely to engage in and practice smoking cessation behaviors, demonstrating a propensity toward healthier lifestyles (20). Conversely, individuals with lower educational levels may exhibit a weaker response to health promotion, possess less knowledge about the health risks associated with smoking, and have fewer opportunities to access smoking cessation services. This scenario potentially leads to a higher incidence of smoking and, subsequently, a greater dependency on tobacco (21).
Our study revealed important connections between health awareness, risk perception, and smoking behavior. Participants who demonstrated better understanding of smoking risks and reported positive self-assessed health status were less likely to smoke, highlighting the crucial role of health cognition in behavioral choices.
However, significant misconceptions about smoking risks persist in the population. For example, only 55.61% of current smokers correctly identified that low-tar cigarettes are not less harmful than regular cigarettes. This finding suggests that tobacco industry marketing strategies continue to influence public understanding of smoking risks (4).
The relationship between health cognition and smoking behavior appears to operate through multiple pathways. Individuals with positive health self-assessment tend to adopt healthier lifestyles overall, including avoiding smoking. This may reflect both heightened health consciousness and sociopsychological factors, as these individuals often maintain their healthy behaviors to align with their self-image and societal health standards.
These findings emphasize the importance of comprehensive health education in smoking prevention. Strengthening public understanding of smoking risks, particularly regarding chronic disease associations, could effectively reduce smoking rates. Moreover, improving health literacy through both educational and economic interventions may enhance individuals’ capacity to access, understand, and act upon health information, thereby promoting healthier lifestyle choices.
The link between marital status and smoking behavior may highlight the relationship between social support and individual choices regarding behavior. The increased smoking rates among married individuals could relate to life stress, a spouse’s smoking habits, or broader socio-cultural factors (22). Those who are cohabiting or married tend to bear more societal and familial responsibilities, leading to a higher risk of smoking. This observation underscores the potential efficacy of family and community-level interventions, such as enhancing support for healthy lifestyles within families and encouraging partners to quit smoking together.
Occupationally, the prevalence of smoking is comparatively lower among those working in the public sector, office environments, students, or other non-manual labor roles, while individuals engaged in agriculture, factory work, or manual labor have significantly higher smoking rates. Several factors could drive this disparity. Firstly, occupation types often correlate with an individual’s education level and socio-economic status. Typically, higher education and socio-economic status are associated with healthier lifestyle choices, likely due to easier access to health-related information, including the risks of smoking, thus reducing the occurrence of smoking behaviors. Secondly, the work environment itself may directly impact smoking habits. For example, agriculture and manual labor are often associated with higher job stress and physical fatigue, where individuals might use smoking as a stress relief method. Moreover, these sectors might lack health promotion policies and smoking control measures, such as less stringent enforcement of workplace smoking bans compared to office settings.
Our findings reveal that individuals exposed to secondhand smoke in their daily lives are at a high risk of current smoking (OR = 4.515, 95%CI = 3.735, 5.457). Exposure to secondhand smoke could lead to smoking due to imitation or social needs (23). Both domestic environments and public spaces should be key venues for promoting smoke-free and smoking control initiatives. Particularly, adolescents, susceptible to external influences, may easily mimic others’ smoking behaviors (24). It is recommended to establish smoke-free homes on top of banning smoking in public places to reduce youth exposure to tobacco and lower the overall smoking rates in the population (25).
This study also has some limitations. Due to its cross-sectional design, establishing causal relationships is challenging. Moreover, as data collection relied on self-reporting, there may be some degree of information bias. Future research could consider employing a longitudinal design to ascertain the causal relationship between HL and smoking behavior, and attempt to use more objective measurement methods, such as blood nicotine levels, to minimize the potential for reporting bias.
This study underscores the potential value of enhancing HL to reduce smoking behavior. These findings provide strong scientific support for the design and implementation of public health strategies and health education interventions. Notably, the nonlinear relationship between HL and smoking behavior identified in this research offers new insights for crafting more precise and effective strategies for smoking control. Furthermore, considering the influence of education level, occupational type, and social support, these strategies should integrate socio-economic factors to design comprehensive and targeted health promotion plans.
This research demonstrates that (1) residents with higher levels of HL have significantly lower smoking rates compared to those with lower HL, and (2) smokers with higher HL consume fewer cigarettes daily. (3) Additionally, non-smokers with higher HL are more inclined to discourage others from smoking, highlighting the crucial role of HL in preventing and controlling smoking behavior. (4) The study also reveals a nonlinear relationship between HL and smoking behavior through RCS analysis. (5) Moreover, the findings indicate significant differences between smokers and non-smokers across various dimensions, including age, education level, occupational category, marital status, and awareness of health.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
ZT: Writing – original draft, Writing – review & editing. QX: Writing – original draft. YZ: Writing – review & editing. QJ: Writing – review & editing. LC: Writing – review & editing. SD: Writing – original draft. SZ: Writing – original draft. YD: Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by funding from the Zhejiang Province Key Medical Discipline, Ningbo Public Welfare Science and Technology Program Project, and Zhejiang Science and Technology Plan for Disease Prevention and Control (grants no. 07-013, 2023S027, 2023S196, and 2025JK262).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. GBD 2019 Tobacco Collaborators. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990-2019: a systematic analysis from the global burden of disease study 2019. Lancet. (2021) 397:2337–60. doi: 10.1016/S0140-6736(21)01169-7
2. Aghapour, M, Raee, P, Moghaddam, SJ, Hiemstra, PS, and Heijink, IH. Airway epithelial barrier dysfunction in chronic obstructive pulmonary disease: role of cigarette smoke exposure. Am J Respir Cell Mol Biol. (2018) 58:157–69. doi: 10.1165/rcmb.2017-0200TR
3. GBD 2015 Tobacco Collaborators. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990-2015: a systematic analysis from the global burden of disease study 2015. Lancet. (2017) 389:1885–906. doi: 10.1016/S0140-6736(17)30819-X
4. Chen, Z, Peto, R, Zhou, M, Iona, A, Smith, M, Yang, L, et al. Contrasting male and female trends in tobacco-attributed mortality in China: evidence from successive Nationwide prospective cohort studies. Lancet. (2015) 386:1447–56. doi: 10.1016/S0140-6736(15)00340-2
5. Uysal, N, Ceylan, E, and Koç, A. Health literacy level and influencing factors in university students. Health Soc Care Community. (2020) 28:505–11. doi: 10.1111/hsc.12883
6. Nutbeam, D, and Lloyd, JE. Understanding and responding to health literacy as a social determinant of health. Annu Rev Public Health. (2021) 42:159–73. doi: 10.1146/annurev-publhealth-090419-102529
7. Fabbri, M, Murad, MH, Wennberg, AM, Turcano, P, Erwin, PJ, Alahdab, F, et al. Health literacy and outcomes among patients with heart failure: a systematic review and Meta-analysis. JACC Heart Fail. (2020) 8:451–60. doi: 10.1016/j.jchf.2019.11.007
8. Zoellner, JM, Hedrick, VE, You, W, Chen, Y, Davy, BM, Porter, KJ, et al. Effects of a behavioral and health literacy intervention to reduce sugar-sweetened beverages: a randomized-controlled trial. Int J Behav Nutr Phys Act. (2016) 13:38. doi: 10.1186/s12966-016-0362-1
9. Ceylan, D, Akan-Çelen, FN, Özkan, S, and Aycan, Z. Promoting adolescent health: health literacy, self-efficacy and internet use. Turk J Pediatr. (2022) 64:110–21. doi: 10.24953/turkjped.2021.1264
10. Prihanto, JB, Nurhayati, F, Wahjuni, ES, Matsuyama, R, Tsunematsu, M, and Kakehashi, M. Health literacy and health behavior: associated factors in Surabaya high school students, Indonesia. Int J Environ Res Public Health. (2021) 18:8111. doi: 10.3390/ijerph18158111
11. Tao, Z, Xu, Q, Zhu, Y, Mei, Q, Feng, H, Jin, Q, et al. Relationship between health literacy and Covid-19 knowledge: a cross-sectional study. Front Public Health. (2023) 11:1058029. doi: 10.3389/fpubh.2023.1058029
12. Sun, S, Yu, H, Ling, J, Yao, D, Chen, H, and Liu, G. The influence of health literacy and knowledge about smoking hazards on the intention to quit smoking and its intensity: an empirical study based on the data of China's health literacy investigation. BMC Public Health. (2023) 23:2355. doi: 10.1186/s12889-023-17292-1
13. Zhao, Y, Sheng, Y, Zhou, J, Wang, H, Chilufya, MM, Liu, X, et al. Influencing factors of Residents' environmental health literacy in Shaanxi Province, China: a cross-sectional study. BMC Public Health. (2022) 22:114. doi: 10.1186/s12889-022-12561-x
14. Fawns-Ritchie, C, Starr, JM, and Deary, IJ. Health literacy, cognitive ability and smoking: a cross-sectional analysis of the English longitudinal study of ageing. BMJ Open. (2018) 8:e023929. doi: 10.1136/bmjopen-2018-023929
15. Stewart, DW, Cano, MA, Correa-Fernández, V, Spears, CA, Li, Y, Waters, AJ, et al. Lower health literacy predicts smoking relapse among racially/ethnically diverse smokers with low socioeconomic status. BMC Public Health. (2014) 14:716. doi: 10.1186/1471-2458-14-716
16. Shen, M, Hu, M, Liu, S, Chang, Y, and Sun, Z. Assessment of the Chinese resident health literacy scale in a population-based sample in South China. BMC Public Health. (2015) 15:637. doi: 10.1186/s12889-015-1958-0
17. Rong, H, Cheng, X, Garcia, JM, Zhang, L, Lu, L, Fang, J, et al. Survey of health literacy level and related influencing factors in military college students in Chongqing, China: a cross-sectional analysis. PLoS One. (2017) 12:e0177776. doi: 10.1371/journal.pone.0177776
18. Shariful Islam, M, AlWajeah, H, Rabbani, MG, Ferdous, M, Mahfuza, NS, Konka, D, et al. Prevalence of and factors associated with tobacco smoking in the Gambia: a National Cross-Sectional Study. BMJ Open. (2022) 12:e057607. doi: 10.1136/bmjopen-2021-057607
19. Cao, P, Jeon, J, Tam, J, Fleischer, NL, Levy, DT, Holford, TR, et al. Smoking disparities by level of educational attainment and birth cohort in the U.S. Am J Prev Med. (2023) 64:S22–31. doi: 10.1016/j.amepre.2022.06.021
20. Li, C, Wang, LM, Huang, ZJ, Zhao, ZP, Zhang, M, and Zhang, X. Survey of degree of passive smoking exposure and related risk awareness in adults in China, 2013. Zhonghua Liu Xing Bing Xue Za Zhi. (2017) 38:572–6. doi: 10.3760/cma.j.issn.0254-6450.2017.05.003
21. El-Khoury Lesueur, F, Bolze, C, and Melchior, M. Factors associated with successful vs. unsuccessful smoking cessation: data from a nationally representative study. Addict Behav. (2018) 80:110–5. doi: 10.1016/j.addbeh.2018.01.016
22. Ramsey, MW, Chen-Sankey, JC, Reese-Smith, J, and Choi, K. Association between marital status and cigarette smoking: variation by race and ethnicity. Prev Med. (2019) 119:48–51. doi: 10.1016/j.ypmed.2018.12.010
23. Simon, C, and Mendez, D. The importance of peer imitation on smoking initiation over time: a dynamical systems approach. Health Care Manag Sci. (2022) 25:222–36. doi: 10.1007/s10729-021-09583-z
24. Fithria, F, Adlim, M, Jannah, SR, and Tahlil, T. Indonesian Adolescents' perspectives on smoking habits: a qualitative study. BMC Public Health. (2021) 21:82. doi: 10.1186/s12889-020-10090-z
Keywords: health literacy, smoking behavior, nonlinear relationship, socio-economic factors, tobacco use
Citation: Tao Z, Xu Q, Zhu Y, Jin Q, Chen L, Ding S, Zhao S and Dong Y (2025) The impact of health literacy on smoking patterns among male residents: insights from Ningbo City. Front. Public Health. 13:1487400. doi: 10.3389/fpubh.2025.1487400
Edited by:
Santi Martini, Airlangga University, IndonesiaReviewed by:
Xuehai Zhang, Zhejiang Center for Disease Control and Prevention (Zhejiang CDC), ChinaCopyright © 2025 Tao, Xu, Zhu, Jin, Chen, Ding, Zhao and Dong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ying Dong, NDY0NTY2NDhAcXEuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.