
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health , 07 February 2025
Sec. Public Health and Nutrition
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1481002
This article is part of the Research Topic Obesity Across the Life Course View all 4 articles
 Juan R. Ulloque-Badaracco1
Juan R. Ulloque-Badaracco1 Esteban A. Alarcon-Braga1
Esteban A. Alarcon-Braga1 Enrique A. Hernandez-Bustamante2,3
Enrique A. Hernandez-Bustamante2,3 Beatrix M. Von-Koeller-Jones1
Beatrix M. Von-Koeller-Jones1 Miguel Huayta-Cortez1Esduardo Saavedra-Custodio1
Miguel Huayta-Cortez1Esduardo Saavedra-Custodio1 Percy Herrera-Añazco4
Percy Herrera-Añazco4 Vicente A. Benites-Zapata5*
Vicente A. Benites-Zapata5*Background and aims: Childhood and adolescent obesity is a global public health concern. Obesity induces several metabolic disturbances. Several studies have explored the association of vitamin B12, folate, and homocysteine (Hcy) with obesity. This study aimed to synthesize the available evidence regarding the differences in serum levels of vitamin B12, Hcy, and folate among children or adolescents with and without obesity.
Methods: A random-effects meta-analysis using the Sidik-Jonkman method and corrected 95% confidence interval (CI) using the truncated Knapp-Hartung standard errors was used for all meta-analyses. Standardized mean difference (SMD) with the corresponding 95% CI was used as the only effect size. The Cochran’s Q test and the I2 statistic were used to evaluate between-study heterogeneity. Publication bias was assessed using funnel plots and the Egger test.
Results: Twenty studies were included with a combined study population of 7,791 patients. There were no significant differences between children/adolescents with and without obesity with respect to serum vitamin B12 levels (SMD: −0.24; 95% CI: −0.53 to 0.06; p > 0.05, I2 = 74.93%) and folate levels (SMD: −0.12; 95% CI: −0.29 to 0.06; p > 0.05, I2 = 19.6%). However, children/adolescents with obesity had significantly higher Hcy levels compared to counterparts without obesity (SMD: 0.77; 95% CI: 0.39 to 1.14; p < 0.001, I2 = 86.4%).
Conclusion: Children and adolescents with obesity had higher Hcy levels than those without obesity. However, no significant differences were found for vitamin B12 and folate levels. Hcy may play a role in the development of obesity in this population.
According to the World Health Organization (WHO), obesity in children and adolescents aged 5–19 years is defined as a body mass index (BMI) greater than 2 standard deviations above the WHO Growth Reference median (1). Childhood and adolescent obesity is a global public health concern (2, 3). According to research published jointly by UNICEF, WHO, and the World Bank in April 2019, globally, the prevalence of overweight for children under the age of 5 years increased from 4.8% in 1990 to 5.9% in 2018 (4). However, there is considerable heterogeneity regarding the estimates for low-and middle-income United Nations regions. The obesogenic environment has led to a modest global increase in obesity among children, primarily due to a lack of sufficient political will and interventions (4). Fueled by economic growth and lifestyle changes, obesity has emerged as an important health risk due to its long-term complications and earlier onset of chronic illnesses, such as cardiovascular disease, hypertension, and type 2 diabetes mellitus (5, 6).
Due to several metabolic disturbances induced by obesity, studies have explored the association between organic compounds (such as vitamin D and iron) and obesity (7, 8), with special emphasis on the triad of vitamin B12, folate, and homocysteine (Hcy) (9, 10). Hcy is an amino acid that results from the metabolism of methionine to cysteine (11), controlled by mutations on regulating enzymes (9) that use vitamin B12 and folate as cofactors in the remethylation pathway (10). In this context, several studies have identified Hcy as a nontraditional marker of obesity, due to the ability to release mediators of inflammation in patients with obesity and cause endothelial damage (11).
In parallel, the essential vitamins B12 and folate play a pivotal role in numerous physiological processes, including the synthesis of DNA and the production of red blood cells. Children and adolescents with obesity have higher rates of chronic inflammatory diseases, which can interfere with the metabolism of B12 and folate through the release of pro-inflammatory cytokines (12). In consequence, they are more exposed to lifelong use of medications, which would explain the increased risk of B12 and folate deficiency (13).
Some pre-clinical studies have suggested a key role of B12 deficiency in obesity by inducing adipogenesis and cholesterol synthesis (14, 15). In patients with obesity, adipose tissue serves as an active endocrine organ that leads to the release of leptin, adiponectin, and resistin. These adipokines can impact the metabolism of homocysteine and B vitamins, resulting in changes in their levels (16). It is important to highlight that although scientific evidence supports these hypotheses, there is considerable inter-individual variability in this respect (17, 18). Diets that are high in processed foods and low in essential nutrients can lead to deficiencies of B12 and folate (17). Coexisting pathologies, anthropometric parameters, and changes in gut microbiota can also cause disruptions in their absorption and bioavailability (18).
Although diverse studies have identified associations between obesity and the above-mentioned organic compounds, the results are inconclusive (19, 20), especially in relation to their levels in children with obesity. Therefore, there is a lack of consensus in this field of study (21). The objective of this study was to conduct a systematic review and meta-analysis to synthesize the existing evidence on the differences in serum levels of vitamin B12, Hcy, and folate among children or adolescents with and without obesity.
We provided a condensed form of the protocol for systematic reviews, adhering to the International Prospective Register of Systematic Reviews (PROSPERO) [CRD42023402162]. The results are reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines (22).
The PRESS Checklist was used to build the search strategy, which was later adapted for all databases (23). No limitations were imposed in terms of date or language of publication. On February 13, 2023, a simultaneous systematic search was performed across PubMed, Scopus, Embase, LILACS, Ovid-Medline, and Web of Science databases. Furthermore, the reference lists of the included studies and preprint databases were manually screened. The full search strategy is provided in Supplementary Table S1. The research question was based on the Population, Exposure, Comparison, and Outcome (PECO) strategy: Do children and adolescents (P) with obesity (E) have lower levels of vitamin B12, folate, and homocysteine (O) compared to children and adolescents without obesity (C)?
The research question was based on Population (Children and adolescents), Exposure (Obesity), Comparison (no obesity), and Outcome (Vitamin B12, folate, and Hcy) strategy.
Cross-sectional, case–control, or cohort studies that assessed the association between vitamin B12, folate, or Hcy levels with obesity in children/adolescents were eligible for inclusion. The exclusion criteria were as follows: duplicate publications, conference abstracts, scoping reviews, systematic reviews, randomized controlled trial (RCT), and narrative reviews. Among the mentioned, RCT were excluded because they are intervention studies that aim to assess a diseased population; whereas observational studies allow us to study the levels of vitamin B12, folate and Hcy in both healthy and diseased populations.
The articles retrieved from the databases were transferred to a software for data management called Rayyan © (24). After the elimination of duplicates, four authors individually screened the titles and abstracts of all articles against the selection criteria. Subsequently, full texts of the short-listed articles were independently reviewed by two authors. Any article that did not meet the entire set of selection criteria was excluded from the review. For articles with missing information, the authors were contacted. Any conflict of opinion or discrepancy in any of the phases was resolved by consensus.
The selection process was depicted using the PRISMA flowchart. A standardized data collection sheet developed in Google Sheets© was used for data extraction. Data pertaining to the following variables were independently extracted by two authors: first author, study location, publication date, study design, sample size, age and sex distribution of the study population, definition of obesity, number of patients with obesity, vitamin B12 levels in patients with and without obesity, folate levels in patients with and without obesity, Hcy levels in patients with and without obesity, and assay technique. Obesity was defined based on the parameters established by each author of the included articles. The definitions of obesity are presented in Supplementary Table S2.
The risk of bias was evaluated independently by two authors. For cohort and case–control studies, the Newcastle-Ottawa Scale (NOS) was employed, while an adaptation of the NOS for cross-sectional studies (NOS-CS) was used for cross-sectional studies. The NOS assesses the methodological quality (risk of bias) of a study based on three main aspects: the selection of study groups, the comparability of the groups, and the assessment of outcomes or exposures. The NOS consists of eight items (seven items if it is the NOS-CS), with each item scored up to one star, except for comparability, which can be scored up to two stars. A score of ≥7 stars was regarded as a low risk of bias (high methodological quality), while a score of <7 stars was deemed a high risk of bias (low methodological quality). The effect of potential publication bias on the results of the meta-analysis was evaluated using funnel plots, the Egger test, and the trim-and-fill method (25). For funnel plots, the minimum number of studies required was 10.
Statistical analysis was performed using STATA 17.0©. Standardized mean difference (SMD) with the corresponding 95% confidence interval (CI) was used as the only effect size. Median values and their interquartile ranges were converted into mean and the corresponding standard deviation (SD) using Hozo’s method (26). For variables with the standard errors (SE) reported, SD was determined using the following equation: SE × √ (sample size). In addition, the natural logarithm of the odds ratio (lnOR) and its standard error were transformed into SMD and its 95% CI using Chinn’s method (27). A random-effects meta-analysis was performed using the Sidik-Jonkman method and corrected 95%CI using the truncated Knapp-Hartung standard error (28, 29). The Cochran’s Q test and the I2 statistic were employed to evaluate between-study heterogeneity; high heterogeneity was defined as I2 ≥ 60% and a p-value <0.05. Subgroup analyses were performed by study design and assay method. A sensitivity analysis was conducted according to risk of bias and obesity definition.
The systematic literature search yielded 1,524 records; after the elimination of duplicates, 682 records remained. After the screening of titles/abstracts, 132 articles were selected for full-text review. Finally, only 20 records complied with all the selection criteria and were included in this systematic review (30–49). The selection process is summarized in the PRISMA flow diagram (Figure 1).
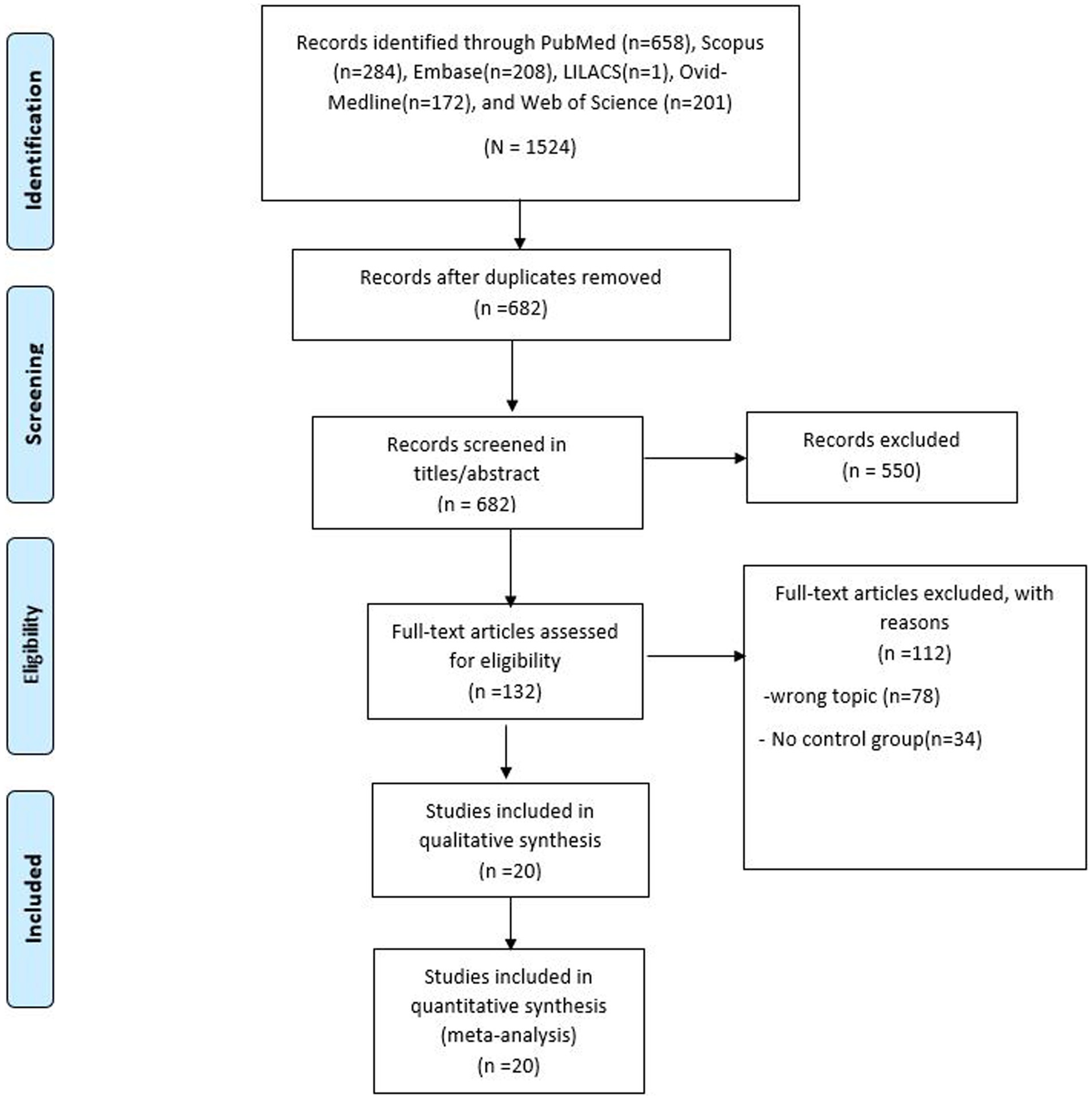
Figure 1. PRISMA flow diagram.
The characteristics of the included studies are summarized in Table 1. A total of 20 studies (5 case–control, 14 cross-sectional, and one cohort study) that assessed the association of vitamin B12, folate, and Hcy levels with obesity in children and adolescents were included. These studies were conducted between 2004 and 2022 in various countries: Turkey (6 studies), India (3 studies), Spain (2 studies), Israel (2 studies), United States (1 study), South Korea (1 study), Egypt (1 study), China (1 study), Brazil (1 study), Romania (1 study), and Tunisia (1 study). The combined total study population in the 20 studies was 7,791. Only 12 studies (n = 4,066) reported the number of male (n = 1834) and female (n = 2,232) participants included.
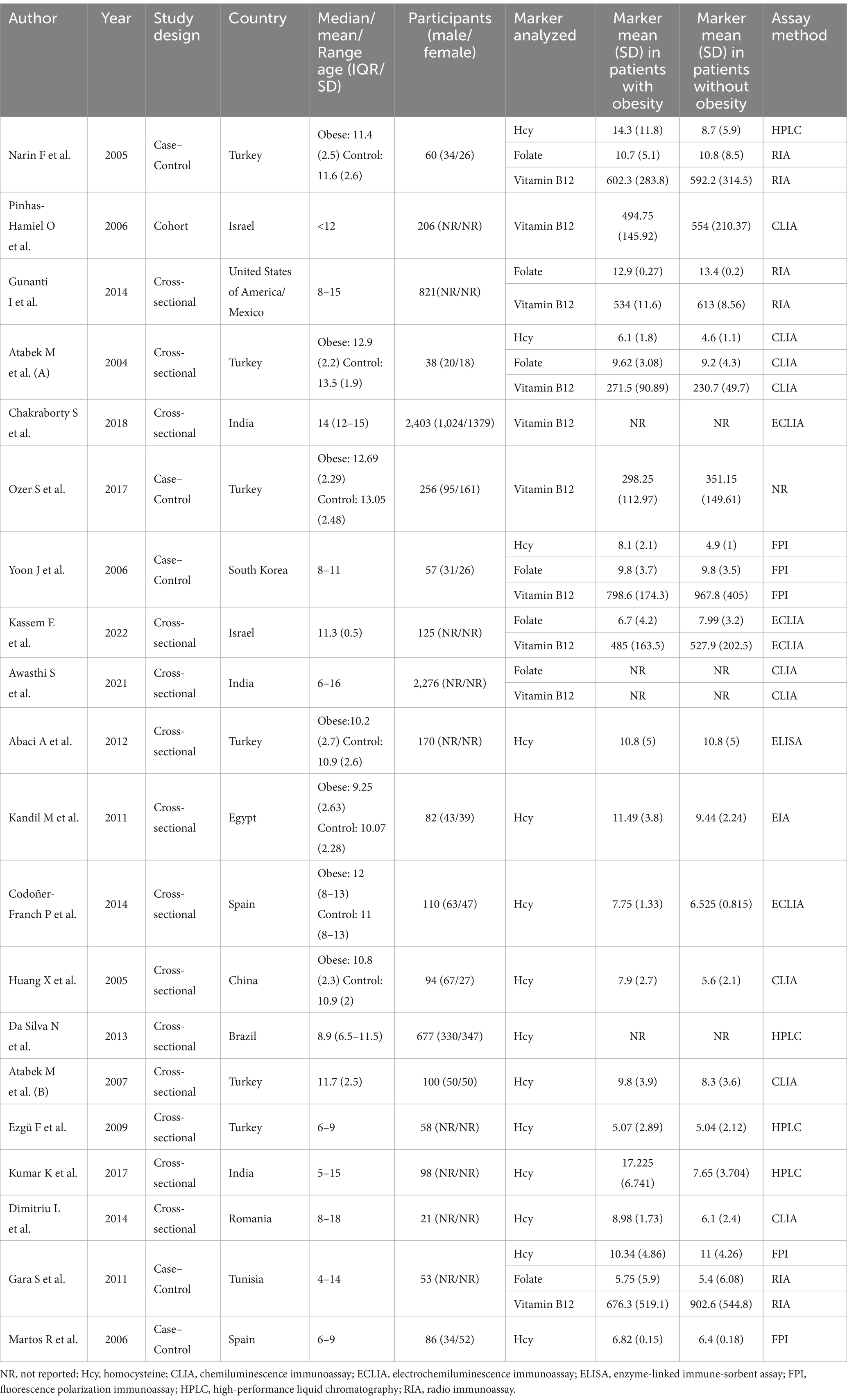
Table 1. Characteristics of the included studies.
The methods used to measure Hcy, vitamin B12, and folate levels were Chemiluminescence Immunoassay (CLIA), Electrochemiluminescence Immunoassay (ECLIA), Enzyme-linked Immunosorbent Assay (ELISA), Fluorescence Polarization Immunoassay (FPI), High-Performance Liquid Chromatography (HPLC), Radioimmunoassay (RIA), and Enzyme immunoassays (EIA).
The risk of bias assessment of the included studies using the NOS and the NOS-CS revealed that 3 studies had a high risk of bias (low methodological quality) while the remaining 17 articles had a low risk of bias (high methodological quality; Supplementary Table S3).
These differences were evaluated in 10 studies (n = 6,295). No significant difference was observed in the vitamin B12 levels between children/adolescents with and without obesity (SMD: −0.26; 95% CI: −0.52 to 0.00; p > 0.05, I2 = 75.15%; Figure 2). Subgroup analyses performed according to study design (Supplementary Figure S1), assay method (Supplementary Figure S2), and continents (Supplementary Figure S3) revealed no significant differences in these subgroups. No high heterogeneity (I2 ≥ 60%) was found in the subgroups that evaluated B12 using RIA or in case–control studies. In the sensitivity analysis according to risk of bias (Supplementary Figure S4), the lack of significant difference and high heterogeneity was maintained (SMD: −0.26; 95% CI: −0.59 to 0.07; p > 0.05, I2 = 73.97%).
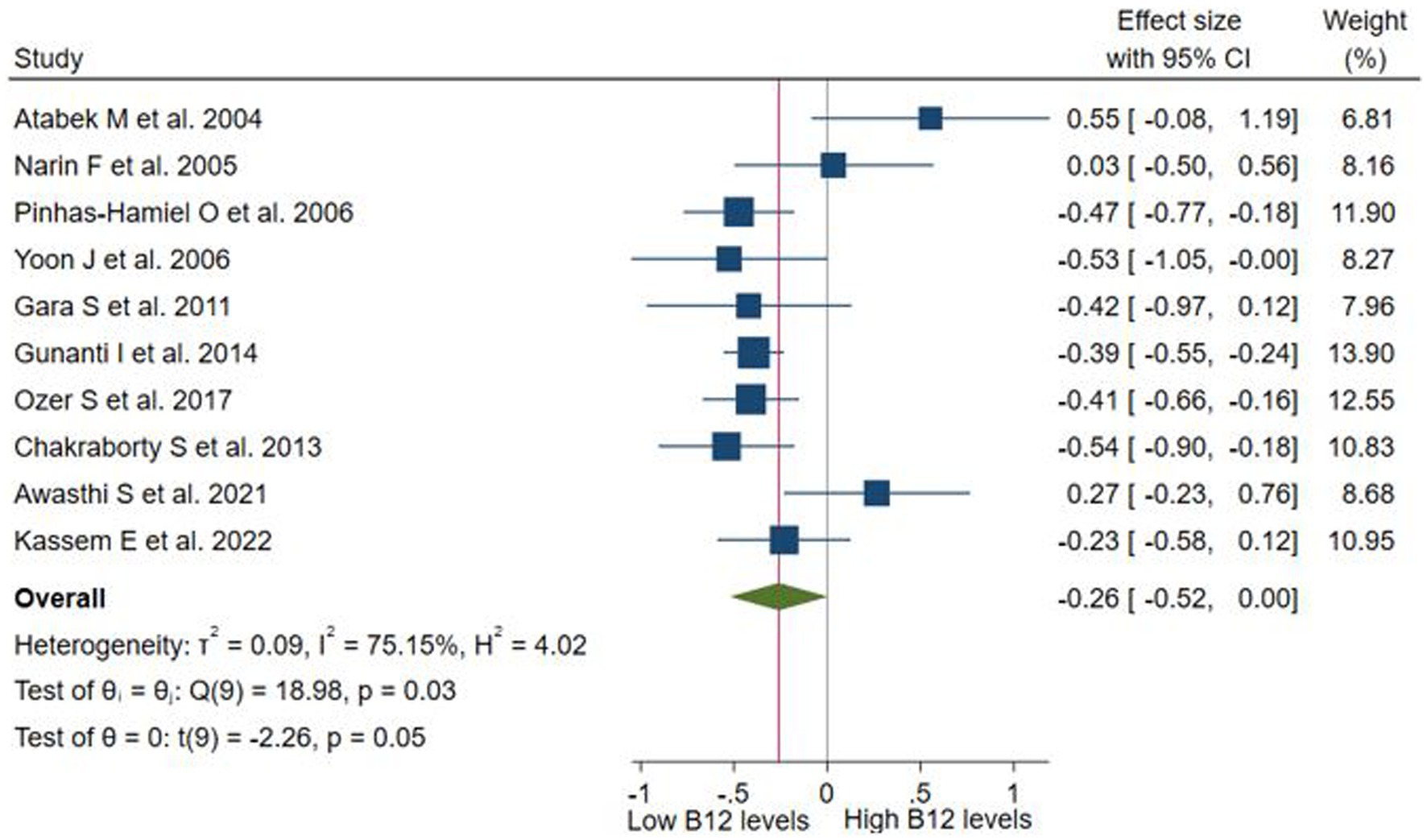
Figure 2. Differences in serum levels of vitamin B12 among children or adolescents with and without obesity.
The funnel plot (Supplementary Figure S5) and the Egger test (p < 0.1) indicated potential publication bias, which was corrected by the trim-and-fill method (SMD = −0.42, 95% CI −0.69 to −0.14; Supplementary Figure S6).
These differences were evaluated in 07 studies (n = 3,430). No significant difference was observed in the folate levels between children/adolescents with and without obesity (SMD: −0.12; 95% CI: −0.29 to 0.06; p > 0.05, I2 = 19.6%; Figure 3). Subgroup analyses performed according to study design (Supplementary Figure S7), assay method (Supplementary Figure S8), and continents (Supplementary Figure S9) revealed no significant differences in these subgroups. No high heterogeneity (I2 ≥ 60%) was found in the subgroups that evaluated folate using RIA, as well as in case–control studies, cross-sectional studies, and studies conducted in Asia. In the sensitivity analysis according to risk of bias (Supplementary Figure S10), the lack of significant difference was maintained (SMD: −0.13; 95% CI: −0.42 to 0.15; p > 0.05, I2 = 21.97%). The Egger test indicated no significant publication bias (p = 0.48).

Figure 3. Differences in serum levels of folate among children or adolescents with and without obesity.
These differences were evaluated in 14 studies (n = 1704). Children and adolescents with obesity had significantly higher Hcy levels than those without obesity (SMD: 0.77; 95% CI: 0.39 to 1.14; p < 0.001, I2 = 86.4%; Figure 4). Subgroup analyses were performed according to study design (Supplementary Figure S11), assay method (Supplementary Figure S12), and continents (Supplementary Figure S13). Significant differences were only observed in the subgroups that evaluated Hcy with CLIA, cross-sectional studies, and studies conducted in Asia. The only subgroup that did not exhibit high heterogeneity was the one that evaluated Hcy using CLIA. The sensitivity analysis according to risk of bias (Supplementary Figure S14) maintained a significant difference and high heterogeneity (SMD: 0.86; 95% CI: 0.44 to 1.27; p < 0.001, I2 = 85.5%). Similarly, in the sensitivity analysis according to the definition of obesity (Supplementary Figure S15), the significant difference and high heterogeneity were maintained (SMD: 0.65; 95% CI: 0.19 to 1.12; p < 0.05, I2 = 87.58%), despite the exclusion of studies that did not report the definition for obesity (42, 46, 47), as well as the study (49) that defined obesity as a BMI > 90th percentile, due to the risk of including overweight participants. The funnel plot (Supplementary Figure S16) and the Egger test revealed no significant publication bias (p = 0.13).
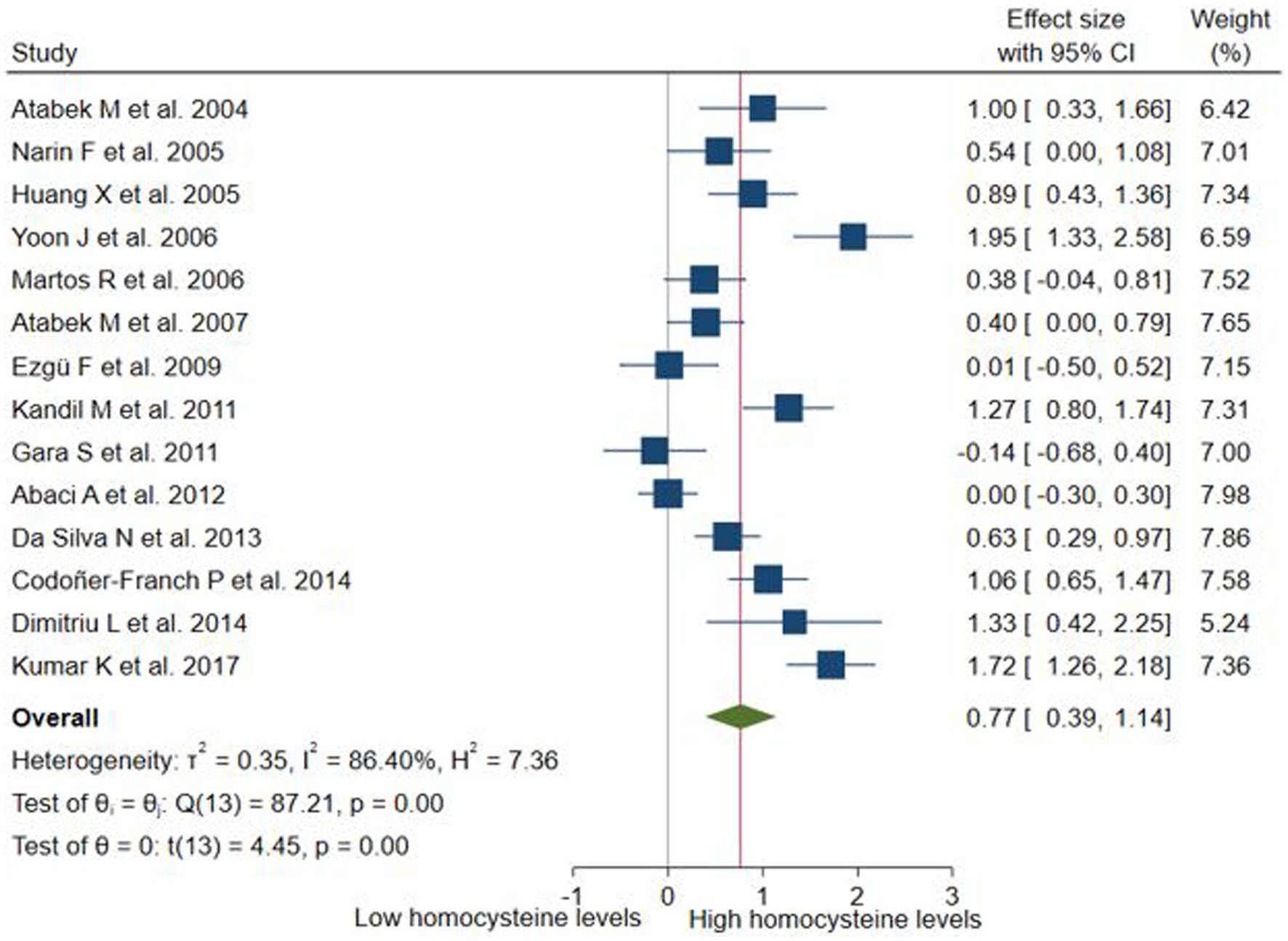
Figure 4. Differences in serum levels of homocysteine among children or adolescents with and without obesity.
The key finding of this study was that children and adolescents with obesity had higher Hcy levels than their counterparts without obesity. This difference was sustained in the sensitivity and some subgroup analyses. Of note, there were no significant differences in vitamin B12 and folate levels among children or adolescents with and without obesity. The associations between obesity with folate, and homocysteine did not demonstrate publication bias. However, the association between vitamin B12 and obesity did show publication bias, which, when corrected using the trim-and-fill method, revealed a significant difference.
A previous systematic review has shown an association between Hcy levels and obesity in children and adolescents (21). However, to the best of our knowledge, there are no systematic reviews on the differences between their levels in children and adolescents with and without obesity. Another systematic review found that adult patients with obesity had significantly higher levels of Hcy compared to their counterparts without obesity, using standardized mean difference as a measure of effect size (9).
Hcy is a naturally occurring amino acid in the human body, formed during the metabolism of methionine to cysteine (50), derived from dietary proteins. Variations in its levels are widely known to affect various chronic conditions, particularly cardiovascular disorders (51, 52). Even though the relationship between high Hcy levels and obesity is multifaceted, significant correlations have been identified by researchers with several potential underlying mechanisms. First, due to poor eating habits and reduced nutrient absorption (53), individuals with obesity are more prone to deficiencies of vitamins that participate in Hcy metabolism, such as B6, B12, and folate. These vitamins act as cofactors during the remethylating pathway of Hcy (54), contributing to elevated Hcy levels in the context of poor-quality food intake. Second, due to the inadequate diet, individuals with obesity often display alterations in gut microbiota (55). Certain gut bacteria interfere with the body’s ability to metabolize Hcy, thus elevating circulating levels (56). Third, obesity is associated with impaired insulin sensitivity (57), a condition where cells become unresponsive to insulin. Even though the relationship is not entirely clear, some studies suggest that insulin resistance can affect the regulation of Hcy metabolism (58), and therefore also contribute to hyperhomocysteinemia. Lastly, inflammation plays a key role in Hcy levels in subjects with obesity (59). The chronic release of pro-inflammatory cytokines (60, 61), combined with obesity-related alterations in gut microbiota (62), contribute both to systemic inflammation and the production of metabolites that affect the body’s ability to break down Hcy, potentially elevating its circulating levels.
Nevertheless, there is considerable heterogeneity regarding the differences in serum Hcy among children or adolescents with and without obesity. This may be attributable to the differences in population characteristics, geographical variability, confounding factors, and statistical approaches. Indeed, a study has shown the differential geographical distribution of the risk variants in the folate/Hcy metabolic pathway relative to ethnic background in Mexico (63).
Our study does not attempt to explain the reasons for the lack of differences in the levels of vitamin B12 and folate in children and adolescents with and without obesity. However, it is possible to propose some hypotheses related to the complex relationship between these vitamins and obesity. For example, the relationship between folate and obesity is not straightforward; low folate levels have been linked in certain studies to an increased risk of obesity or weight gain because folate deficiency may change how energy is metabolized, resulting in a gradual weight increase (64). As for vitamin B12, there are indirect mechanisms by which it may be linked to weight management (31). On one hand, the metabolism of proteins, lipids, and carbohydrates depends heavily on vitamin B12 (65). It has been argued that increasing B12 levels may enhance energy metabolism; however, there is little empirical evidence that B12 supplementation alone can cause considerable weight loss (66). On the other hand, studies have also implied that B12 plays a role in appetite-regulating hormones and its deficiency can lead to anemia and exhaustion, thus indirectly affecting physical activity levels and obesity (14). Likewise, although our study only evaluated differences in vitamin B12 and folate levels, the primary studies that were part of the analysis did not evaluate dietary habits. This is important because some studies have suggested a greater need for folic acid and vitamin B supplementation in certain areas of the world (63). Similarly, recent advances in the field of nutrigenetics have highlighted the impact of genetic variations on individuals’ responses to dietary intake. In the case of vitamin B-complex, special reference has been made to the widely studied variant in the 5,10-methylenetetrahydrofolate reductase (MTHFR) gene (66).
Serum folate and total Hcy levels are influenced by folate intake and genetic polymorphisms in the MTHFR gene such as C677T (67). The prevalence of the MTHFR 677TT genotype varies across ethnic groups and regions, with a frequency of approximately 15% in Japanese populations (67). These differences may also explain our findings because individuals with the TT genotype have significantly higher serum Hcy levels and lower serum folate levels than those with the CT and TT genotypes (67).
This study has some limitations. First, differences with respect to the study population (e.g., age, sex, ethnicity, and underlying health conditions) and study characteristics might have led to substantial heterogeneity across the included studies. However, subgroup and sensitivity analyses were performed to explore potential sources of heterogeneity. Second, the pooled estimates were based on crude measures of effect size, which may have potentially been affected by non-controlled confounders. Third, although there is at least one included study per continent, the generalizability of our findings is limited. Fourth, the sensitivity and specificity of optimal cut-off levels of the biomarkers assessed have not been reported. Further studies should establish these cut-off levels to evaluate the prognostic value of these biomarkers in children and adolescents with obesity. Nonetheless, our study has several strengths. Multiple databases were searched, allowing a comprehensive synthesis of the available literature. A substantial number of participants were included, which ensured adequate statistical power.
In summary, children and adolescents with obesity had higher Hcy levels than their counterparts without obesity. However, no statistically significant differences were found for vitamin B12 and folate levels. These findings highlight the potential role of Hcy in the development of obesity in this population. Although further research is required to elucidate the underlying mechanisms and establish causality, these findings underscore the importance of early detection and targeted interventions to address elevated Hcy levels as a potential risk factor for obesity in the pediatric population. Future studies should explore the interaction between Hcy, nutritional status, and obesity to improve our understanding and inform preventive strategies in the context of childhood and adolescent obesity.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
JU-B: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. EA-B: Data curation, Methodology, Writing – original draft. EH-B: Methodology, Writing – original draft. BV-K-J: Data curation, Writing – original draft. MH-C: Data curation, Writing – original draft. ES-C: Data curation, Formal analysis, Writing – original draft. PH-A: Formal analysis, Writing – original draft, Writing – review & editing. VB-Z: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1481002/full#supplementary-material
1. World Health Organization (WHO). (2021). Obesity and overweight. Available at: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
2. Smith, JD, Fu, E, and Kobayashi, MA. Prevention and management of childhood obesity and its psychological and health comorbidities. Annu Rev Clin Psychol. (2020) 16:351–78. doi: 10.1146/annurev-clinpsy-100219-060201
3. Zhang, X, Liu, J, Ni, Y, Yi, C, Fang, Y, Ning, Q, et al. Global prevalence of overweight and obesity in children and adolescents: A systematic review and Meta-analysis. JAMA Pediatr. (2024) 178:800–13. doi: 10.1001/jamapediatrics.2024.1576
4. Sorić, M, Bovet, P, Miranda, JJ, Bhutta, Z, and Stevens, GA. The epidemiological burden of obesity in childhood: a worldwide epidemic requiring urgent action. BMC Med. (2019) 17:212. doi: 10.1186/s12916-019-1449-8
5. Ulloque-Badaracco, JR, Al-Kassab-Córdova, A, Alarcon-Braga, EA, Hernandez-Bustamante, EA, Huayta-Cortez, MA, Cabrera-Guzmán, JC, et al. Association of vitamin B12, folate, and homocysteine with COVID-19 severity and mortality: A systematic review and meta-analysis. SAGE Open Med. (2024) 12:20503121241253957. doi: 10.1177/20503121241253957
7. Haghighat, N, Sohrabi, Z, Bagheri, R, Akbarzadeh, M, Esmaeilnezhad, Z, Ashtary-Larky, D, et al. A systematic review and Meta-analysis of vitamin D status of patients with severe obesity in various regions worldwide. Obes Facts. (2023) 16:519–39. doi: 10.1159/000533828
8. Tan, X, Tan, PY, Gong, YY, and Moore, JB. Overnutrition is a risk factor for iron, but not for zinc or vitamin A deficiency in children and young people: a systematic review and meta-analysis. BMJ glob. Health. (2024) 9:e015135. doi: 10.1136/bmjgh-2024-015135
9. Wang, J, You, D, Wang, H, Yang, Y, Zhang, D, Lv, J, et al. Association between homocysteine and obesity: a meta-analysis. J Evid Based Med. (2021) 14:208–17. doi: 10.1111/jebm.12412
10. Froese, DS, Fowler, B, and Baumgartner, MR. Vitamin B12, folate, and the methionine remethylation cycle-biochemistry, pathways, and regulation. J Inherit Metab Dis. (2019) 42:673–85. doi: 10.1002/jimd.12009
11. Yuan, D, Chu, J, Lin, H, Zhu, G, Qian, J, Yu, Y, et al. Mechanism of homocysteine-mediated endothelial injury and its consequences for atherosclerosis. Front Cardiovasc Med. (2023) 9:1109445. doi: 10.3389/fcvm.2022.1109445
12. Benites-Zapata, VA, Ignacio-Cconchoy, FL, Ulloque-Badaracco, JR, Hernandez-Bustamante, EA, and Alarcón-Braga, EA. Vitamin B12 levels in thyroid disorders: a systematic review and meta-analysis. Front Endocrinol. (2023) 14:1070592. doi: 10.3389/fendo.2023.1070592
13. Wiebe, N, Field, CJ, and Tonelli, M. A systematic review of the vitamin B12, folate and homocysteine triad across body mass index. Obes Rev. (2018) 19:1608–18. doi: 10.1111/obr.12724
14. Boachie, J, Adaikalakoteswari, A, Samavat, J, and Saravanan, P. Low vitamin B12 and lipid metabolism: evidence from pre-clinical and clinical studies. Nutrients. (2020) 12:1925. doi: 10.3390/nu12071925
15. Fu, L, Cheng, H, Gao, L, Zhao, X, and Mi, J. Genetically proxied vitamin B12 and homocysteine in relation to life course adiposity and body composition. Diabetes Metab Syndr. (2023) 17:102883. doi: 10.1016/j.dsx.2023.102883
16. Harshman, SG, Wons, O, Rogers, MS, Izquierdo, AM, Holmes, TM, Pulumo, RL, et al. A diet high in processed foods, Total carbohydrates and added sugars, and low in vegetables and protein is characteristic of youth with avoidant/restrictive food intake disorder. Nutrients. (2019) 11:2013. doi: 10.3390/nu11092013
17. Diethelm, K, Jankovic, N, Moreno, LA, Huybrechts, I, de, S, de, T, et al. Food intake of European adolescents in the light of different food-based dietary guidelines: results of the HELENA (healthy lifestyle in Europe by nutrition in adolescence) study. Public Health Nutr. (2012) 15:386–98. doi: 10.1017/S1368980011001935
18. Liu, BN, Liu, XT, Liang, ZH, and Wang, JH. Gut microbiota in obesity. World J Gastroenterol. (2021) 27:3837–50. doi: 10.3748/wjg.v27.i25.3837
19. Grundy, SM, Cleeman, JI, Daniels, SR, Donato, KA, Eckel, RH, Franklin, BA, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute scientific statement: executive summary. Crit Pathw Cardiol. (2005) 4:198–203. doi: 10.1097/00132577-200512000-00018
20. Semiz, S, Rota, S, Özdemir, O, Özdemir, A, and Kaptanoğlu, B. Are C-reactive protein and homocysteine cardiovascular risk factors in obese children and adolescents? Pediatr Int. (2008) 50:419–23. doi: 10.1111/j.1442-200X.2008.02615.x
21. de Oliveira Leite, L, Pitangueira, CD, Ferreira Damascena, N, and Ribas de Farias Costa, P. Homocysteine levels and cardiovascular risk factors in children and adolescents: systematic review and meta-analysis. Nutr Rev. (2021) 79:1067–78. doi: 10.1093/nutrit/nuaa116
22. Liberati, A, Altman, DG, Tetzlaff, J, Mulrow, C, Gotzsche, P, Ioannidis, JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. (2009) 339:b2700. doi: 10.1136/bmj.b2700
23. McGowan, J, Sampson, M, Salzwedel, DM, Cogo, E, Foerster, V, and Lefebvre, C. PRESS peer review of electronic search strategies: 2015 guideline statement. J Clin Epidemiol. (2016) 75:40–6. doi: 10.1016/j.jclinepi.2016.01.021
24. Ouzzani, M, Hammady, H, Fedorowicz, Z, and Elmagarmid, A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. (2016) 5:210. doi: 10.1186/s13643-016-0384-4
25. Duval, S, and Tweedie, R. A nonparametric “trim and fill” method of accounting for publication bias in meta-analysis. J Am Stat Assoc. (2000) 95:89–98. doi: 10.1080/01621459.2000.10473905
26. Hozo, SP, Djulbegovic, B, and Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. (2005) 5:13. doi: 10.1186/1471-2288-5-13
27. Chinn, S. A simple method for converting an odds ratio to effect size for use in meta-analysis. Stat Med. (2000) 19:3127–31. doi: 10.1002/1097-0258(20001130)19:22<3127::aid-sim784>3.0.co;2-m
28. Felsch, M, Beckmann, L, Bender, R, Kuss, O, Skipka, G, and Mathes, T. Performance of several types of beta-binomial models in comparison to standard approaches for meta-analyses with very few studies. BMC Med Res Methodol. (2022) 22:319. doi: 10.1186/s12874-022-01779-3
29. van Aert, RCM, and Jackson, D. A new justification of the Hartung-Knapp method for random-effects meta-analysis based on weighted least squares regression. Res Synth Methods. (2019) 10:515–27. doi: 10.1002/jrsm.1356
30. Narin, F, Atabek, ME, Karakukcu, M, Narin, N, Kurtoglu, S, Gumus, H, et al. The association of plasma homocysteine levels with serum leptin and apolipoprotein B levels in childhood obesity. Ann Saudi Med. (2005) 25:209–14. doi: 10.5144/0256-4947.2005.209
31. Pinhas-Hamiel, O, Doron-Panush, N, Reichman, B, Nitzan-Kaluski, D, Shalitin, S, and Geva-Lerner, L. Obese children and adolescents: a risk group for low vitamin B12 concentration. Arch Pediatr Adolesc Med. (2006) 160:933–6. doi: 10.1001/archpedi.160.9.933
32. Gunanti, IR, Marks, GC, Al-Mamun, A, and Long, KZ. Low serum vitamin B-12 and folate concentrations and low thiamin and riboflavin intakes are inversely associated with greater adiposity in Mexican American children. J Nutr. (2014) 144:2027–33. doi: 10.3945/jn.114.201202
33. Atabek, ME, Bağcı, Z, Pirgon, Ö, and Erkul, İ. Plasma total homocysteine levels in childhood obesity. Turk J Endocrinol Metab. (2004) 3:107–11. Available at: https://endocrinolrespract.org/en/plasma-total-homocysteine-levels-in-childhood-obesity-131062
34. Chakraborty, S, Chopra, M, Mani, K, Giri, AK, Banerjee, P, Sahni, NS, et al. Prevalence of vitamin B12 deficiency in healthy Indian school-going adolescents from rural and urban localities and its relationship with various anthropometric indices: a cross-sectional study. J Hum Nutr Diet. (2018) 31:513–22. doi: 10.1111/jhn.12541
35. Ozer, S, Sonmezgoz, E, and Demir, O. Negative correlation among vitamin B12 levels, obesity severity and metabolic syndrome in obese children: a case control study. J Pak Med Assoc. (2017) 67:1648–53. Available at: https://www.archive.jpma.org.pk/article-details/8425
36. Park, JY, and Hong, YM. Homocysteine, insulin, vitamin B12 and folic acid levels in obese children. Korean J Pediatr. (2006) 49:475–81. doi: 10.3345/kjp.2006.49.5.475
37. Kassem, E, Na’amnih, W, Shapira, M, Ornoy, A, and Muhsen, K. Comparison between school-age children with and without obesity in nutritional and inflammation biomarkers. J Clin Med. (2022) 11:6973. doi: 10.3390/jcm11236973
38. Awasthi, S, Kumar, D, Mahdi, AA, Agarwal, GG, Pandey, AK, Parveen, H, et al. Prevalence of specific micronutrient deficiencies in urban school going children and adolescence of India: a multicenter cross-sectional study. PLoS One. (2022) 17:e0267003. doi: 10.1371/journal.pone.0267003
39. Abaci, A, Akelma, AZ, Özdemir, O, Hizli, Ş, Razi, CH, and Akin, KO. Relation of total homocysteine level with metabolic and anthropometric variables in obese children and adolescents. Turk J Med Sci. (2012) 42:69–76. doi: 10.3906/sag-1011-1252
40. Kandil, ME, Anwar, GM, Fatouh, A, Salama, N, Ahmed, A, Elabd, E, et al. Relation between serum homocysteine and carotid intima-media thickness in obese Egyptian children. J Clin Basic Cardiol. (2010) 13:8–11. Available at: https://www.kup.at/mobile/summary/9733.html
41. Codoñer-Franch, P, Tavárez-Alonso, S, Porcar-Almela, M, Navarro-Solera, M, Arilla-Codoñer, Á, and Alonso-Iglesias, E. Plasma resistin levels are associated with homocysteine, endothelial activation, and nitrosative stress in obese youths. Clin Biochem. (2014) 47:44–8. doi: 10.1016/j.clinbiochem.2013.10.021
42. Huang, XM, Zhang, YY, Yu, ZS, Zhu, WH, Fu, JF, He, J, et al. Early arterial atherosclerosis and level of plasma homocysteine in simply obese children. Zhonghua Er Ke Za Zhi. (2005) 43:192–5. doi: 10.3760/cma.j.issn.0578-1310.2005.03.110
43. da Silva, NP, de Souza, FIS, Pendezza, AI, Fonseca, FLA, Hix, S, Oliveira, AC, et al. Homocysteine and cysteine levels in prepubertal children: association with waist circumference and lipid profile. Nutrition. (2013) 29:166–71. doi: 10.1016/j.nut.2012.05.015
44. Atabek, ME, Pirgon, O, and Kivrak, AS. Evidence for association between insulin resistance and premature carotid atherosclerosis in childhood obesity. Pediatr Res. (2007) 61:345–9. doi: 10.1203/pdr.0b013e318030d206
45. Ezgü, F, Tümer, L, Ozbay, F, Hasanoglu, A, Biberoğlu, G, and Aybay, C. Homocysteine, fibrinogen and anti-ox-LDL antibody levels as markers of atherosclerosis in prepubertal obese children. J Pediatr Endocrinol Metab. (2009) 22:915–20. doi: 10.1515/jpem.2009.22.10.915
46. Kumar, KJ, Saldanha, K, Sushma, K, Murthy, DS, and Vishwanath, P. A prospective study of homocysteine and its relation to body mass index and lipid profile in school children. Indian Pediatr. (2017) 54:935–7. doi: 10.1007/s13312-017-1185-0
47. Dimitriu, L, and Dimitriu, AG. PO-0018 plasma homocysteine in overweight and obese school children. Arch Dis Child. (2014) 99:A256.4–A257. doi: 10.1136/archdischild-2014-307384.698
48. Gara, S, Ochi, H, Chango, A, Najjar, L, Feki, M, B’Chir, F, et al. C677t polymorphism of MTHFR and G80A polymorphism of RFC genes and their relation with homocysteine levels in obese Tunisian children. Tunis Med. (2011) 89:565–8. Available at: https://latunisiemedicale.com/index.php/tunismed/article/view/1741
49. Martos, R, Valle, M, Morales, R, Cañete, R, Gavilan, MI, and Sánchez-Margalet, V. Hyperhomocysteinemia correlates with insulin resistance and low-grade systemic inflammation in obese prepubertal children. Metabolism. (2006) 55:72–7. doi: 10.1016/j.metabol.2005.07.008
50. Finkelstein, JD, and Martin, JJ. Homocysteine. Int J Biochem Cell Biol. (2000) 32:385–9. doi: 10.1016/s1357-2725(99)00138-7
51. Ulloque-Badaracco, JR, al-kassab-Córdova, A, Hernández-Bustamante, EA, Alarcón-Braga, EA, Cabrera-Guzmán, JC, Horruitiner-Mendoza, AA, et al. Homocysteine, vitamin B12, and folate circulating levels in women with and without polycystic ovary syndrome: A systematic review and meta-analysis. Women's Health (Lond). (2024) 20:17455057241279039. doi: 10.1177/17455057241279039
52. Osganian, SK, Stampfer, MJ, Spiegelman, D, Rimm, E, Cutler, JA, Feldman, HA, et al. Distribution of and factors associated with serum homocysteine levels in children: child and adolescent trial for cardiovascular health. JAMA. (1999) 281:1189–96. doi: 10.1001/jama.281.13.1189
53. Roblin, L. Childhood obesity: food, nutrient, and eating-habit trends and influences. Appl Physiol Nutr Metab. (2007) 32:635–45. doi: 10.1139/H07-046
54. Mason, JB, and Miller, JW. The effects of vitamins B12, B6, and folate on blood homocysteine levels. Ann N Y Acad Sci. (1992) 669:197–203. doi: 10.1111/j.1749-6632.1992.tb17100.x
55. Cho, KY. Association of gut microbiota with obesity in children and adolescents. Clin Exp Pediatr. (2023) 66:148–54. doi: 10.3345/cep.2021.01837
56. Festi, D, Schiumerini, R, Eusebi, LH, Marasco, G, Taddia, M, and Colecchia, A. Gut microbiota and metabolic syndrome. World J Gastroenterol. (2014) 20:16079–94. doi: 10.3748/wjg.v20.i43.16079
57. Ala, OA, Akintunde, AA, Ikem, RT, Kolawole, BA, Ala, OO, and Adedeji, TA. Association between insulin resistance and total plasma homocysteine levels in type 2 diabetes mellitus patients in south West Nigeria. Diabetes Metab Syndr. (2017) 11:S803–9. doi: 10.1016/j.dsx.2017.06.002
58. Arnoni, CP, Lima, C, Cristovam, PC, Maquigussa, E, Vidotti, DB, and Boim, MA. Regulation of glucose uptake in mesangial cells stimulated by high glucose: role of angiotensin II and insulin. Exp Biol Med (Maywood). (2009) 234:1095–101. doi: 10.3181/0902-RM-50
59. Kabil, O, and Banerjee, R. Enzymology of H2S biogenesis, decay and signaling. Antioxid Redox Signal. (2014) 20:770–82. doi: 10.1089/ars.2013.5339
60. Wang, CY, Chen, ZW, Zhang, T, Liu, J, Chen, SH, Liu, SY, et al. Elevated plasma homocysteine level is associated with ischemic stroke in Chinese hypertensive patients. Eur J Intern Med. (2014) 25:538–44. doi: 10.1016/j.ejim.2014.04.011
61. Ulloque-Badaracco, JR, Hernandez-Bustamante, EA, Alarcon-Braga, EA, al-kassab-Córdova, A, Cabrera-Guzmán, JC, Herrera-Añazco, P, et al. Vitamin B12, folate, and homocysteine in metabolic syndrome: a systematic review and meta-analysis. Front Endocrinol. (2023) 14:1221259. doi: 10.3389/fendo.2023.1221259
62. Weber, GJ, Pushpakumar, S, Tyagi, SC, and Sen, U. Homocysteine and hydrogen sulfide in epigenetic, metabolic and microbiota related renovascular hypertension. Pharmacol Res. (2016) 113:300–12. doi: 10.1016/j.phrs.2016.09.002
63. Binia, A, Contreras, AV, Canizales-Quinteros, S, Alonzo, VA, Tejero, ME, and Silva-Zolezzi, I. Geographical and ethnic distribution of single nucleotide polymorphisms within genes of the folate/homocysteine pathway metabolism. Genes Nutr. (2014) 9:421. doi: 10.1007/s12263-014-0421-7
64. Köse, S, Sözlü, S, Bölükbaşi, H, Ünsal, N, and Gezmen-Karadağ, M. Obesity is associated with folate metabolism. Int J Vitam Nutr Res. (2020) 90:353–64. doi: 10.1024/0300-9831/a000602
65. Ho, M, Halim, JH, Gow, ML, El-Haddad, N, Marzulli, T, Baur, LA, et al. Vitamin B12 in obese adolescents with clinical features of insulin resistance. Nutrients. (2014) 6:5611–8. doi: 10.3390/nu6125611
66. Niforou, A, Konstantinidou, V, and Naska, A. Genetic variants shaping inter-individual differences in response to dietary intakes-A narrative review of the case of vitamins. Front Nutr. (2020) 7:558598. doi: 10.3389/fnut.2020.558598
Keywords: obesity, vitamin B12, folate, homocysteine, meta-analysis
Citation: Ulloque-Badaracco JR, Alarcon-Braga EA, Hernandez-Bustamante EA, Von-Koeller-Jones BM, Huayta-Cortez M, Saavedra-Custodio E, Herrera-Añazco P and Benites-Zapata VA (2025) Vitamin B12, folate, and homocysteine levels in children and adolescents with obesity: a systematic review and meta-analysis. Front. Public Health. 13:1481002. doi: 10.3389/fpubh.2025.1481002
Edited by:
Anagha Killedar, The University of Sydney, AustraliaReviewed by:
Rosaura Leis, University of Santiago de Compostela, SpainCopyright © 2025 Ulloque-Badaracco, Alarcon-Braga, Hernandez-Bustamante, Von-Koeller-Jones, Huayta-Cortez, Saavedra-Custodio, Herrera-Añazco and Benites-Zapata. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vicente A. Benites-Zapata, dmJlbml0ZXNAdXNpbC5lZHUucGU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.