
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Public Health, 12 February 2025
Sec. Public Health Education and Promotion
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1467571
 Zhendong Gao1
Zhendong Gao1 Chen Soon Chee1*
Chen Soon Chee1* Roxana Dev Omar Dev1
Roxana Dev Omar Dev1 Yutong Liu2*
Yutong Liu2* Jianhong Gao1
Jianhong Gao1 Rui Li1Fangyi Li1Xiaoxiao Liu1
Rui Li1Fangyi Li1Xiaoxiao Liu1 Tao Wang1
Tao Wang1Background: Social capital, as a multidimensional social science concept, plays a crucial role in promoting physical activity. Despite numerous studies exploring the relationship between social capital and physical activity, there is still a lack of systematic understanding of how different dimensions of social capital influence physical activity levels. This study aims to systematically review the literature up to 2024 on the relationship between social capital and physical activity, uncover the role of social capital in promoting physical activity, and identify its multidimensional impacts.
Methods: We used a combination of search terms including “social capital” and “physical activity” to search the Web of Science, PubMed, Scopus, SportDiscus, and PsychINFO databases for English literature published up to March 1, 2024.
Results: We identified 2,021 unique articles and reviewed 115 studies that met our inclusion criteria. These studies evaluated various dimensions of social capital, with key dimensions including social participation (34%), social networks (30%), social cohesion (30%), social trust (29%), overall social network (26%), social support (19%), safety (19%), norms of reciprocity (13%), social control (10%), satisfaction with the environment (8%), collective efficacy (4%), norms for physical activity (3%), and voting (1%). In studies exploring the relationship between social capital and physical activity, the majority of positive results in the hypothesized direction were observed in dimensions such as social cohesion, trust, participation, reciprocity, satisfaction with the environment, and overall social networks. In contrast, dimensions such as voting, collective efficacy, safety, control, and physical activity norms predominantly showed null or negative results. The results for social support were mixed, displaying positive, negative, and null outcomes, while findings for social networks were also predominantly mixed.
Conclusion: This study reveals the significant role of social capital in promoting physical activity, particularly in the dimensions of social cohesion, social trust, social participation, norms of reciprocity, satisfaction with environment, and overall social network. When designing public health interventions in the future, it is crucial to tailor strategies to different populations and contexts to better leverage social capital in promoting physical activity.
In the field of public health, understanding, and promoting physical activity has become a crucial issue (1–3), especially in the context of the global rise in chronic diseases and mental health problems (4–6). Physical activity not only reduces the risk of heart disease, diabetes, and certain cancers but also significantly enhances psychological well-being and overall quality of life (7–9). Despite the well-known benefits of physical activity, activity levels are influenced by various factors, including biological, environmental, psychological, and social factors (10–12). Among these factors, the role of social capital has increasingly garnered the attention of researchers as strategies to promote physical activity continue to be explored in the field of public health (13–15).
Social capital, as a multidimensional social science concept, has become a significant topic of research in public health, psychology, and sociology over the past few decades (16–18). Although the definition and measurement of social capital remain contentious, there is a scholarly consensus on its core elements, which include social networks, social participation, trust, reciprocity, and shared norms (19, 20). Generally, social capital is defined as the resources and advantages individuals or groups derive from their social networks, typically acquired through social interactions, trust relationships, and community participation (19, 21). The key dimensions of social capital involve personal attributes such as the quality and quantity of social networks, social support, and information channels, as well as collective attributes like the degree of mutual trust among community members and shared social norms and values (21, 22).
Social capital can be further subdivided into various operational types or dimensions, including structural and cognitive; bonding, bridging, and linking; strong and weak ties; and horizontal and vertical (20, 23, 24). Cognitive social capital can be understood as individuals' perceptions of interpersonal trust, sharing, and reciprocity (21). Structural social capital refers to the density of social networks or patterns of civic participation (21). Bonding social capital pertains to relationships within homogenous groups, such as those among family members, neighbors, close friends, and colleagues, also known as strong ties (24). Bridging social capital involves connections between individuals or groups across different power structures, such as those linking diverse racial and occupational backgrounds, referred to as weak ties (24). Linking social capital is considered the respect and trust relationships that exist among people interacting across formal or institutionalized power or authority gradients in society (24–26). Among these, bonding and bridging social capital are regarded as horizontal social capital, while linking social capital is seen as vertical social capital (24).
The importance of social capital lies in its inclusion of both individual-level interactions and relationships as well as group or community-level cooperation and cohesion (21). Previous studies have indicated that social capital is considered a protective health factor (27). Some research also suggests that high levels of social capital are associated with numerous positive health outcomes, such as lower mortality rates, better mental health, and reduced crime and violence (17, 20, 28). Although some researchers have pointed out potential “negative effects” of social capital on health outcomes (29) or found its effects to be insignificant (28), there remains substantial evidence linking social capital with self-rated health (22, 30).
In the context of the relationship between social capital and physical activity, qualitative studies have found that social capital is regarded as a key resource for initiating and maintaining physical activity (31). Research indicates that strong social networks and high levels of social participation at the individual level can encourage more active lifestyles, including regular physical activity (32–34). Community-level reciprocity and neighborhood trust norms are associated with higher levels of physical activity among urban adults (15). High social capital has been shown to be associated with regular Moderate-to-Vigorous Physical Activity (MVPA) in boys and with overall physical activity in girls (35). Additionally, social capital can promote physical activity through the dissemination of health information (14). However, it is important to note that the relationship between social capital and physical activity may vary across different populations, influenced by factors such as age, gender, socioeconomic status, and culture (36–38).
To our knowledge, most systematic reviews on the relationship between social capital and health have primarily focused on broad health outcomes and public health interventions (16, 17, 30), and there has not been a systematic review specifically addressing the relationship between social capital and physical activity. Furthermore, scholars have emphasized the need for future research to focus on the multidimensionality and multi-layered perspectives of social capital (16, 17). In light of this, the present study aims to systematically review relevant literature to deeply explore the heterogeneous evidence of the impact of the multiple dimensions of social capital on physical activity, thereby filling the current research gap. By identifying effective social capital-building strategies and their applicability across different social and cultural contexts, we hope to provide new insights for public health practice and policy-making to leverage social capital at the policy level to improve public health outcomes.
Based on previous systematic reviews on related topics (28, 30, 39), we conducted an English literature search in March 2024 using the Web of Science, PubMed, Scopus, SportDiscus, and PsychINFO databases, with a cut-off date of March 1, 2024. These databases were selected for their high credibility and wide recognition in the fields of public health and sports science. We used a combination of search terms including “social capital” and “physical activity.” The specific search strategy is detailed in Table 1. We excluded abstracts, conference proceedings, dissertations, book chapters, and articles published in non-peer-reviewed journals.
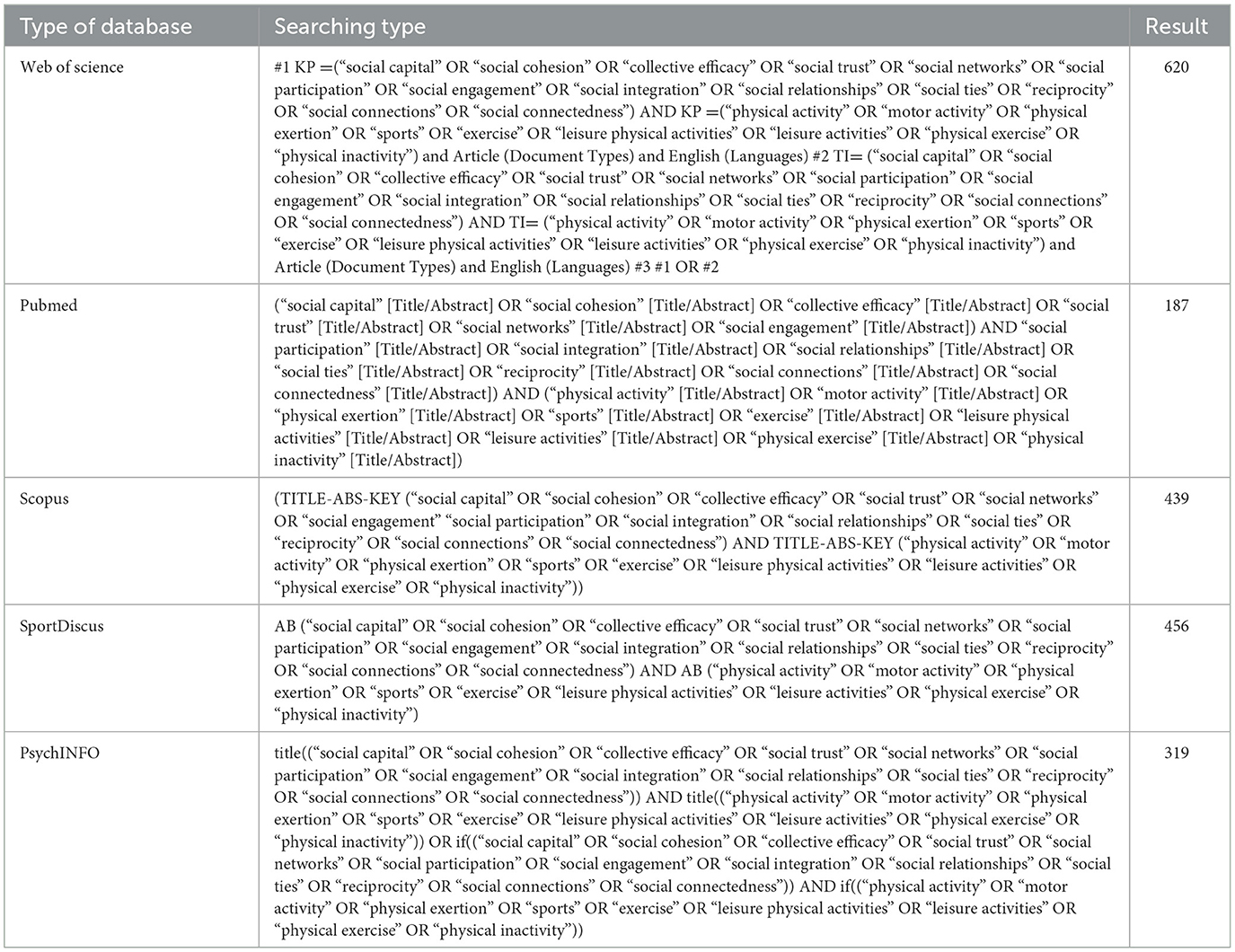
Table 1. Search strategy.
The inclusion criteria were as follows: (1) Studies focusing on the relationship between social capital and physical activity, including observational studies (cross-sectional studies, prospective and retrospective cohort studies, case-control studies) and randomized controlled trials; (2) Studies that conducted formal hypothesis testing on the relationship between measures of social capital and physical activity; (3) Studies that measured physical activity using objective methods or subjective assessments, including but not limited to frequency, duration, and intensity of participation; (4) Studies that included at least one measure of social capital; (5) Studies published in peer-reviewed journals in English up to March 1, 2024.
The exclusion criteria were: (1) Studies that did not provide direct results on the association between measures of social capital and physical activity; (2) Reviews, opinion articles, or theoretical papers; (3) Studies where physical activity outcomes were indirectly obtained or measured through exercise behavior or exercise psychology; (4) Studies that were not available in full text or had incomplete data; (5) Studies that only included measures of social support. We excluded studies focusing solely on social support, as there are numerous reviews on this topic (39–41). We will focus on explaining social capital through the lens of social cohesion, as the search terms for social capital inevitably reveal methods based on social support and social cohesion (16, 30).
The search process involved a layered evaluation and adhered to the PRISMA guidelines (42) to ensure systematic and transparent literature screening. Initially, the identified literature was downloaded into Endnote X7 after removing duplicates, and studies were selected based on their titles and abstracts. Subsequently, the full texts of the remaining studies were retrieved and assessed for eligibility. If necessary, both abstracts and full texts were screened. The search and selection process was independently conducted by four researchers (ZG, YL, JG, and RL). Any discrepancies regarding the inclusion of specific studies were resolved through consensus meetings. If consensus could not be reached, the final decision on inclusion or exclusion was made by researchers (CC and RO). The basic information of each retrieved article (i.e., author, publication year, and article title) was recorded by the author (ZG) in a Microsoft Excel® spreadsheet to ensure comprehensive tracking and review.
The data extraction process was carried out independently by five reviewers (ZG, YL, JG, RL, and FL) following standardized methods for systematic reviews. In cases of disagreement, the reviewers consulted researchers (CC and RO), and discrepancies were resolved through consensus. Key elements from each study were extracted and summarized in a table, organized chronologically by publication year. For each study, the table included the following: the first author and year of publication, sample information (size, characteristics, and location), study design (cross-sectional, prospective, or experimental), measures of social capital, measures of physical activity, covariates included as control variables, and main statistical results (effect estimates and/or significance of hypothesis testing). Bolded terms in the table indicated statistically significant results.
Additionally, we summarized the distribution of study outcomes, indicating whether the study authors reported “positive” results (significant associations in the hypothesized direction), “negative” results (negative and/or null associations), or “mixed” results (both positive and negative/null associations).
As shown in the PRISMA flow diagram [Figure 1, (42)], the initial search yielded 2,021 published papers. After removing duplicates, 1,778 papers remained. Upon reviewing titles and abstracts, 1,257 papers were further excluded because they did not focus on the relationship between social capital and physical activity (n = 1,056) or were reviews, opinion articles, or theoretical papers (n = 201). Of the remaining 521 papers, 406 were excluded after full-text review for the following reasons: providing measures that included only social support (n = 14), no results exploring the association between social capital and physical activity (n = 356), using non-applicable methods to measure physical activity (n = 33), and not being available in full text (n = 3). Consequently, 115 papers were included in this systematic review.
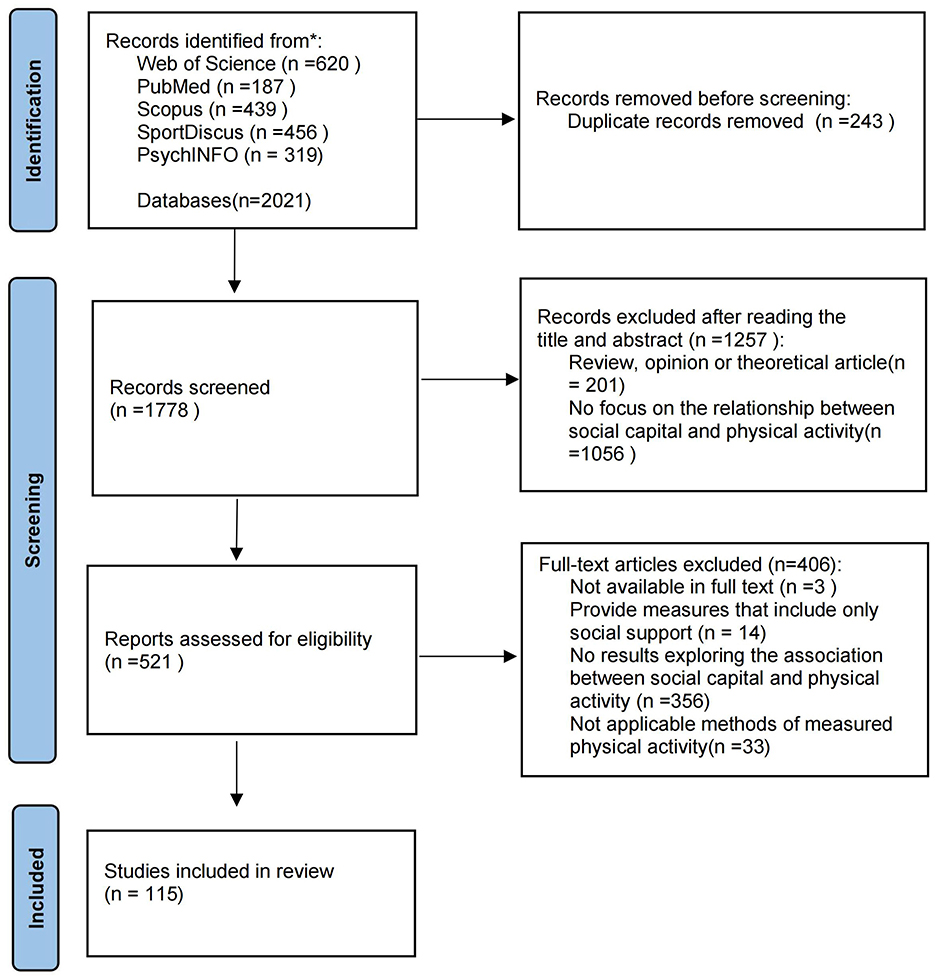
Figure 1. PRISMA flow diagram showing the process of study selection.
This review summarizes the characteristics of the 115 included studies (see Supplementary Material 1 for details). Table 2 provides a summary of these characteristics. Among them, 89 (77%) studies used a cross-sectional design, and 26 (23%) used a longitudinal design. 53 (46%) studies involved samples from the United States, 10 (9%) involved samples from China, and 8 (7%) involved samples from Japan/Canada. Four (3%) studies each involved samples from Brazil/Sweden, and the remaining 28 studies involved samples from 24 different countries. The total sample size of the included studies reached 1,328,785, with 22 (19%) studies having a sample size of over 10,000 and 69 (60%) studies having a sample size of over 1,000. Seventeen (15%) studies used nationally representative data. The sample age range in the included studies was from 6 to 91 years. Twenty-four (21%) studies focused on samples of minors. The majority (79%) of the studies focused on adults, with 40 (44%) studies primarily involving middle-aged and older adults (50 years and above). Covariates controlled at the individual level included age (95%), gender (71%), education level (62%), marital status (30%), and race/ethnicity (27%). Ten percent of the studies included regional-level covariates (neighborhood, school, county). Additionally, 43% of the studies controlled for health-related covariates, and 24% controlled for socioeconomic status-related covariates.
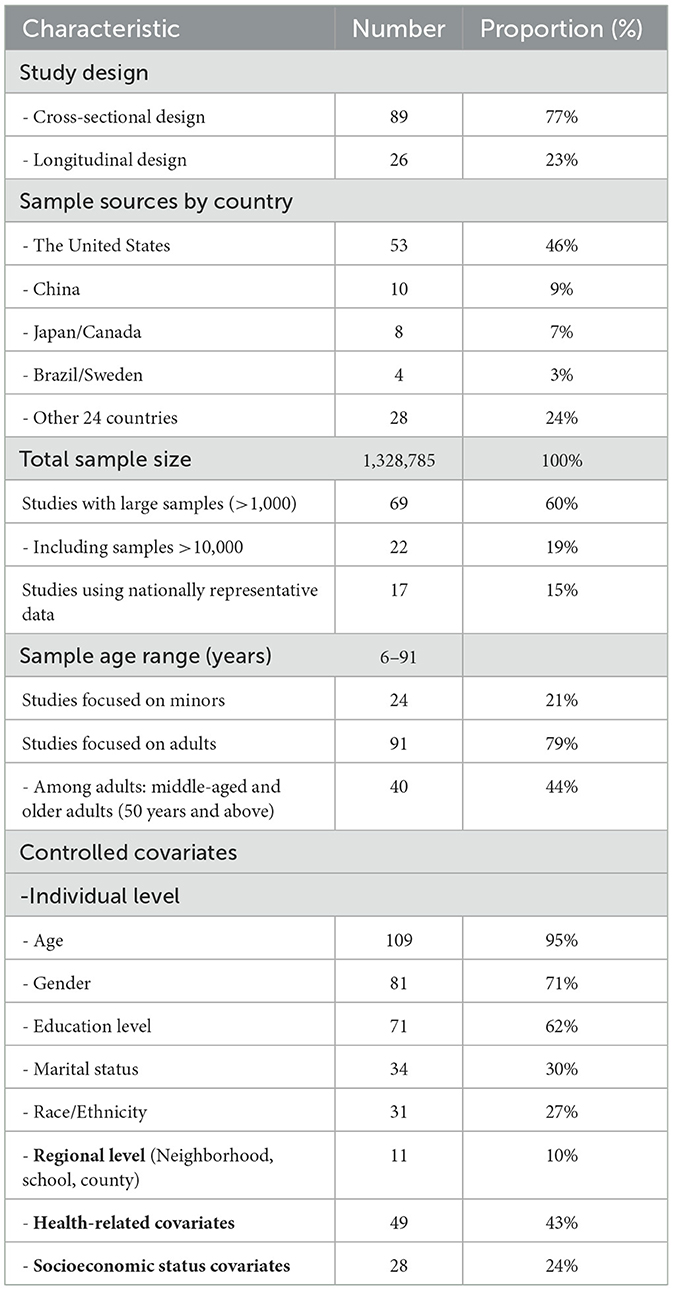
Table 2. Summary of characteristics of the 115 included studies.
Table 3 summarizes the key attributes of the selected studies, including the distribution of social capital domains covered and the main research findings (positive, negative, and mixed). Among the 115 studies, the components measured across the studies varied significantly in frequency. The most commonly assessed components were social participation (34%), social networks (30%), and social cohesion (30%), which appeared in nearly one-third of the studies. In contrast, less frequently assessed components included collective efficacy (4%), norms for physical activity (3%), and voting (1%), highlighting their limited inclusion in the reviewed literature.
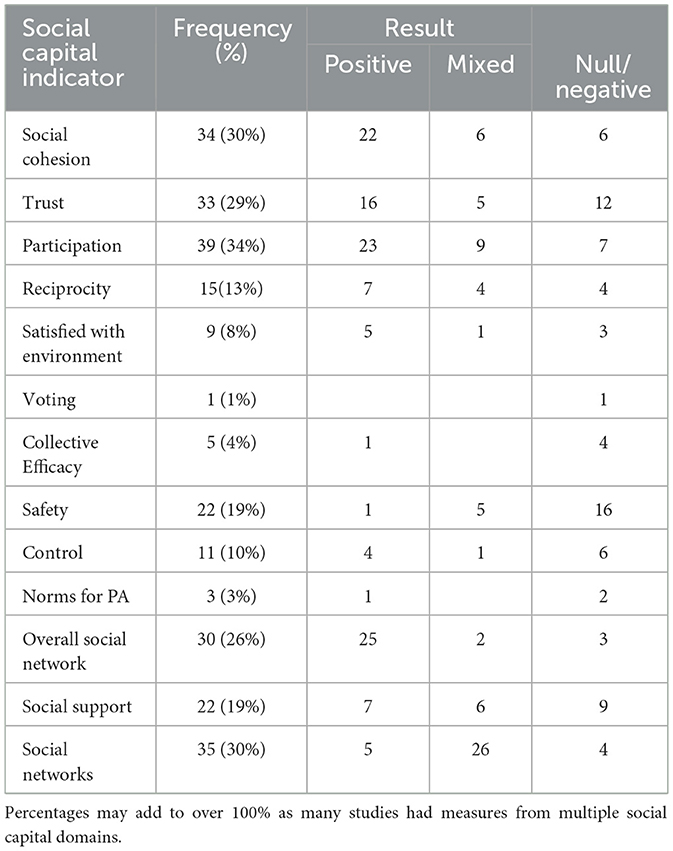
Table 3. Summary of social capital indicators included in the results of the social capital and physical health study (n = 115).
The studies varied in their use of social capital measures, including constructs (latent variables composed of indicators) and individual indicators (single items). 10% of the studies used a single measure of social capital (composed of one or more indicators), while 39% used a single social capital indicator only. 51% of the studies used multiple measures and indicators. The median number of indicators per study was 2, with a range of 1 to 6.
The most frequently examined measure of physical activity (PA) was subjective (86%), with 12 studies using objective PA measures. Four studies employed mixed measures. The types of PA included overall physical activity (79%), followed by leisure-time physical activity (17%), and 5 (4%) studies measured other types such as recreational, mixed, and school-based activities.
Among the 115 included studies, the majority of positive results in the hypothesized direction for the association between social capital and physical activity were found in the following indicators: social cohesion, trust, participation, reciprocity, satisfaction with environment, and overall social network (see Table 3). The indicators of voting, collective efficacy, safety, control, and norms for PA predominantly showed null/negative results. The results for social support were similarly distributed among positive, negative, and mixed outcomes, while social networks predominantly showed mixed results. It is worth noting that the included studies examined various aspects of social networks related to physical activity. Some studies focused on specific dimensions, such as family or peer networks, or particular aspects like network size, diversity, and tie strength; these were categorized as social networks. Other studies analyzed the overall characteristics of entire social network, which we classified as overall social network. This classification helps to clarify the variability in the study results, as studies focusing on specific network dimensions may capture more targeted social influences, while studies examining overall network reflect broader structural patterns.
A total of 34 studies examined the relationship between social cohesion and physical activity (38, 43–75). Overall, the studies found a direct positive correlation between social cohesion and physical activity. Specifically, 22 (64.7%) studies showed positive results, 6 (17.6%) studies showed mixed results, and 6 (17.6%) studies showed null or negative results.
The insignificant results were observed in specific subgroups: women/mothers (45, 49, 61), adolescents/high school students (55, 71), residents of high socioeconomic status/developed countries (53, 58, 66), middle-aged and older Chinese people (56, 70), and samples from low-income and socioeconomically disadvantaged populations (46, 60).
A total of 33 studies examined the relationship between social trust and physical activity (15, 35–37, 45, 49, 50, 53, 57, 61, 63, 67, 71, 75–93). Overall, the studies found a direct positive correlation between social trust and physical activity. Specifically, 16 (48.5%) studies showed positive results, 5 (15.2%) studies showed mixed results, and 12 (36.3%) studies showed null or negative results.
The insignificant results were observed in specific subgroups: adults in developed countries (53, 77, 78, 81, 83, 88), middle-aged people in developing countries (84), women/mothers/pregnant women (49, 61, 93), children/high school students (35, 71, 82, 85, 89, 90), and disadvantaged communities (57).
A total of 39 studies examined the relationship between social participation and physical activity (14, 37, 45, 46, 56, 63, 68, 71, 75–77, 79, 83, 84, 86–88, 91, 92, 94–113). Overall, studies found a direct positive correlation between social participation and physical activity. Specifically, 23 (59.0%) studies showed positive results, 9 (23.1%) studies showed mixed results, and 7 (17.9%) studies showed null or negative results.
The insignificant results were observed in specific subgroups: middle-aged and older adults (56, 104–107, 109, 111), adolescents (98, 101), adults in developed countries (77, 79), studies that could not predict longitudinal results (110), and some special samples such as social group members (68, 102), cancer survivors (99), and low-income adults living in public housing (46).
A total of 15 studies examined the relationship between norms of reciprocity and physical activity (15, 35, 46, 57, 67, 78, 80, 82–85, 91, 92, 114, 115). Overall, studies found a direct positive correlation between norms of reciprocity and physical activity. Specifically, 7 (46.6%) studies showed positive results, 4 (26.7%) studies showed mixed results, and 4 (26.7%) studies showed null or negative results.
The insignificant results were observed in specific subgroups: adults in developed countries (78, 83), minors (35, 82, 85), women (45), working-class populations (80), and disadvantaged community adults (57).
Three studies examined the relationship between norms for PA and physical activity (46, 68, 80). Among these, only one study targeting African American church members (68) reported positive results. The other two studies did not find significant results and involved low-income adults living in public housing (46) and working-class populations (80).
A total of 9 studies examined the relationship between community satisfaction with the environment and physical activity (47, 50, 52, 56, 58, 74, 86, 96, 115). Overall, studies found a direct positive correlation between satisfaction with the environment and physical activity. Specifically, 5 (62.5%) studies showed positive results, 1 (11.1%) study showed mixed results, and 3 (37.5%) studies showed null or negative results.
The insignificant results were observed in specific subgroups: adolescents (47), older adults in China (56), and adults in developing countries (58). Adults in developed countries provided mixed results (52).
A total of 30 studies examined the relationship between overall social network and physical activity (14, 15, 38, 45, 46, 53, 57, 60, 67, 77, 80, 83, 86, 87, 91, 92, 94, 97, 98, 106, 108, 116–124). Overall, studies found a direct positive correlation between overall social network and physical activity. Specifically, 25 (83.3%) studies showed positive results, 2 (6.7%) studies showed mixed results, and 3 (10%) studies showed null or negative results.
The insignificant results were observed in specific subgroups: women in developed countries (45), working-class populations (80), and male populations in developing countries (15). Mixed results were observed during the COVID-19 pandemic among older female populations and adults in developed countries (77, 123).
A total of 35 studies examined the relationship between social networks and physical activity (32, 34, 66, 81, 84, 88, 99, 102, 104, 105, 107, 112, 113, 125–145). Overall, the studies found that the relationship between social networks and physical activity was mixed. Specifically, 5 (14.3%) studies showed positive results, 26 (74.3%) studies showed mixed results, and 4 (11.4%) studies showed null or negative results.
The studies that showed only null or negative results were found in specific subgroups: cancer survivors (99), older college students with small sample sizes (135), Latino civic groups (102), and members of the same sociocultural organization (107).
In studies examining the relationship between voting, collective efficacy, safety, and physical activity, the overall relationship was found to be null or negative. Specifically, only one study included voting and provided null/negative results (77). In studies examining collective efficacy (64, 89, 90, 146, 147), only one study reported positive results, which involved an intervention aimed at enhancing collective efficacy among mothers (146).
Regarding studies on safety (37, 43, 45, 47, 49, 51, 52, 58, 62, 73, 78, 80, 84, 85, 93, 105–107, 114, 127, 148, 149), 1 study (4.5%) showed positive results, 5 studies (22.8%) showed mixed results, and 16 studies (72.7%) showed null or negative results.
In studies examining the relationship between social control, social support, and physical activity, the overall relationship was found to be mixed. Regarding studies on social control (14, 35, 37, 60, 61, 71, 73, 89, 90, 108, 146), 4 (36.4%) studies showed positive results, 1 (9.1%) study showed mixed results, and 6 (54.5%) studies showed null or negative results. The insignificant results were observed in women (61), adolescents and children (35, 71, 73, 89, 90,), and socioeconomically disadvantaged populations (60).
In studies on social support (14, 32, 35, 46, 60, 61, 68, 71, 80, 82, 83, 86, 90, 93, 94, 97, 101, 108, 113, 127, 136, 138), 7 (31.8%) studies showed positive results, 6 (27.3%) studies showed mixed results, and 9 (40.9%) studies showed null or negative results.
This study found that social capital plays an important role in promoting physical activity. Our analysis indicates that multiple dimensions of social capital, including social cohesion, social trust, social participation, norms of reciprocity, satisfaction with environment, and overall social network, are significantly associated with physical activity. However, dimensions such as voting, collective efficacy, safety, and norms for physical activity did not show a significant association with physical activity. Additionally, the relationships between social networks, social control, and social support with physical activity yielded mixed results. Due to the varying relationships between different dimensions of social capital and individual characteristics, most studies reported both positive and negative outcomes.
Social cohesion refers to the bonds and sense of solidarity among community members and is a crucial dimension of social capital (150, 151). Strong cohesion within a community can provide emotional support and increase opportunities for physical activity through community events and programs (152, 153). In this study, we found that social cohesion is positively associated with physical activity. This finding aligns with the existing literature and further underscores the critical role of social cohesion in promoting healthy behaviors (30, 154).
Trust is one of the core elements of social capital (155). High levels of trust within a community can enhance residents' sense of safety, indirectly promoting social support and cooperative social interactions, making individuals more willing to engage in outdoor activities and exercise (156–158). Overall, trust is positively associated with physical activity.
Social participation involves individuals' engagement in community activities and social organizations (159). Active participation in community activities not only increases opportunities for physical activity but also helps build more social connections, providing emotional support and social encouragement, thereby enhancing individuals' mental health (160–162). Overall, social participation is significantly associated with physical activity.
Norms of reciprocity refer to the mutual assistance and supportive behaviors among community members (163). In a community with strong norms of reciprocity, residents are more likely to help and encourage each other. This mutual support can provide both emotional support and practical assistance for physical activity (164, 165). Overall, there is a positive association between norms of reciprocity and physical activity.
Satisfaction with the environment refers to residents' overall attitude toward their community environment (166). Studies have shown that a good community environment, including factors like community density, green spaces, sports facilities, and street connectivity, can significantly enhance residents' levels of physical activity (167–169). Our results indicate that satisfaction with the environment is closely related to physical activity levels, with residents of highly satisfying communities being more likely to engage in outdoor activities and exercise.
Overall social network refers to the total sum of an individual's social relationships and connections, which can provide information, support, and motivation (170). In this study, we found that overall social network is significantly positively associated with physical activity. This finding aligns with the existing literature (171–173) and further emphasizes the critical role of overall social networks in promoting healthy behaviors (174, 175).
Although these social capital indicators generally have a positive impact on physical activity, their effects may vary depending on demographic characteristics and social context. For example, women showed insignificant results in indicators such as social cohesion, social trust, norms of reciprocity, and overall social networks. This could be because women, in many cultural contexts, bear more family and caregiving responsibilities, which limit their time and energy (176, 177). Social networks for women often focus more on family and close relationships, which may not directly promote physical activity (130, 178). Additionally, women might rely more on internal family support and trust rather than community-level trust to determine their physical activity behaviors (179).
Minors showed insignificant results in the social capital indicators of social cohesion, social trust, social participation, norms of reciprocity, and satisfaction with the environment. This may be because their physical activity is more influenced by school and family environments rather than the broader community (208). Additionally, some studies on social capital indicators for minors rely on parents' perceptions of family social capital (82, 85), which could affect the results. Parents' perceptions may not fully reflect the actual experiences and interactions of minors, leading to discrepancies in the findings.
Among adults, some insignificant results were observed in the social capital indicators of social cohesion, social trust, social participation, norms of reciprocity, satisfaction with the environment, and overall social networks, particularly among middle-aged and older adults, as well as adults in developed countries. This may be because the influence of social capital is confounded by other variables and external factors, indicating that its impact is not solely dependent on social capital itself (36, 180, 181).
Additionally, certain special populations, such as low-income and socioeconomically disadvantaged groups, specific social groups, and cancer survivors, as well as unpredictable longitudinal results, may reflect the protective potential of social capital. However, the unique challenges faced by these groups might limit its effects (182–184).
The type of social capital indicator can also create differences. For example, the frequency, type, and duration of social participation can influence its relationship with physical activity (102, 105, 106, 111). Moreover, the negative effects of social capital should not be overlooked, such as workplace social capital and social participation among students, which have shown negative associations with physical activity (80, 98).
Voting behavior is often considered a form of social participation (185). However, in this study, we found no significant association between studies involving voting behavior and physical activity. This may be because voting behavior itself does not directly involve physical activity, nor does it directly provide social support or enhance community interaction. Voting behavior mainly reflects citizens' willingness to participate politically rather than their daily health behaviors or physical activity levels (186). This could also be one of the reasons why there are fewer studies investigating the relationship between voting behavior and physical activity.
Collective efficacy refers to the ability of community members to work together to solve problems and achieve common goals (187). In this study, the association between collective efficacy and physical activity was not significant. This may be because collective efficacy more accurately reflects a community's ability to address social issues and provide public services rather than directly involving individual health behaviors (188, 189). Although communities with high collective efficacy may have better public resources and a safer environment (190, 191), this does not necessarily translate into individual physical activity behaviors.
Safety is often considered an important factor influencing physical activity (192, 193), but our study found no significant association between safety and physical activity. This is consistent with previous review findings (194). The lack of significant results may be due to varying measurement standards among the included studies, as broad crime indicators and PA measures might limit our ability to interpret the results. Additionally, while a safe community environment can provide the basic assurance for physical activity, merely feeling safe may not be sufficient to motivate individuals to increase their physical activity. Crime itself might not affect a person's PA behavior unless they feel threatened by crime or fear it (193).
Norms for physical activity refer to the community's expectations and promotion of physical activity (195). However, our study found no significant association between norms for physical activity and actual physical activity. This may be due to the limited number of studies involved, which focused on specific groups such as low-income adults (46) and working-class populations (80). Individuals' physical activity behavior may be more influenced by personal motivation, time management, and lifestyle (196, 197), rather than solely by community norms. Even if there are positive norms for physical activity within a community, the impact of these norms on individual behavior may be limited without the necessary facilities and support (198).
Social networks refer to individuals' social relationships and connections, including family, friends, colleagues, and neighborhood ties. These networks can be measured by various characteristics, such as size, density, relationship quality, and composition (199). Our findings show that the relationship between social networks and physical activity is mixed. This is consistent with previous studies (200–202). The mixed results highlight that strong social networks can promote physical activity through multiple pathways (170). However, the effects of social networks may vary across different populations and social contexts, potentially leading to ineffectiveness in certain groups, such as cancer survivors (99), older college students with small sample sizes (135), Latino civic groups (102), and members of the same sociocultural organization (107).
Social control refers to the ability of community members to influence and regulate individual behaviors through formal or informal means (203). In the included studies, social control provided mixed results. However, insignificant results were observed in specific groups such as women (61), adolescents and children (35, 71, 73, 89, 90), and socioeconomically disadvantaged populations (60). This may stem from the dual nature of social control's impact on individual behavior, encompassing both positive and negative influences (204, 205). Its effects vary depending on the implementation method and community context.
Social support refers to the emotional, informational, and practical assistance individuals receive from others, and it is considered an important factor in promoting physical activity (206). Our results show mixed findings regarding the relationship between social support and physical activity. This is likely due to the limitations of our search strategy and inclusion criteria. Numerous existing reviews have already established the relationship between social support and physical activity (39–41).
This study has several limitations. First, we only included literature published in English, which may have led to the exclusion of important studies in other languages. Second, most of the included studies used a cross-sectional design. While this design can reveal associations between variables, it cannot establish causality. Third, as a multidimensional concept, social capital has been measured using different methods and indicators across studies. This inconsistency can lead to heterogeneous results and limit the comparability of findings across studies. This is a common issue in social capital and health research, where the lack of consensus on the definition and measurement of social capital restricts researchers' ability to aggregate and quantitatively analyze results (30, 207). In our study, we combined unified social capital indicators with specific social capital indicators, which may have increased heterogeneity and potential confounding effects, thus limiting the robustness of our findings. Fourth, we adopted broad inclusion criteria for physical activity measures, and the studies primarily relied on subjective assessments of physical activity levels, which could result in reporting bias and measurement errors. Fifth, although the sample populations in the included studies are increasingly diverse, they are predominantly from developed countries, which limits the generalizability of the results and their applicability to different cultural contexts.
Based on the limitations discussed in this paper, future research should focus on: (1) adopting more longitudinal designs to better understand the long-term effects and causal mechanisms of social capital on physical activity; (2) striving for standardization and consistency in social capital measurement methods to improve the comparability of results and the ability to conduct comprehensive analyses; (3) using objective assessment tools to reduce potential biases and improve accuracy; (4) expanding the sample range to include more studies from developing countries and diverse cultural backgrounds to provide a more comprehensive understanding; (5) increasing focus on specific populations (such as minors, older adults, and socioeconomically disadvantaged groups) is needed, as there are fewer studies on these groups and the results are inconsistent. Future research should explore the role and impact of social capital in these populations in greater depth; (6) exploring the negative effects of social capital, as some studies have highlighted its potential adverse impacts. Future research should investigate these negative effects to fully understand their influence on physical activity and health; (7) developing and evaluating interventions aimed at promoting physical activity by enhancing social capital, and testing the underlying mechanisms and mediating effects, as most studies assume specific pathways but rarely test potential mechanisms.
This study systematically reviewed the literature on the relationship between social capital and physical activity up to 2024, revealing the significant role of social capital in promoting physical activity. Our review of studies meeting our inclusion criteria found substantial evidence of associations between multiple dimensions of social capital—such as social cohesion, social trust, social participation, norms of reciprocity, satisfaction with environment, and overall social network—and physical activity. Few studies found significant associations between physical activity and the dimensions of voting, collective efficacy, safety, and norms for physical activity. In contrast, the dimensions of social networks, social control, and social support showed more support for an association with physical activity, but the results were mixed. Most studies yielded both positive and null results. These findings highlight the protective role of social capital in physical activity, indicating a strong influence of individual characteristics and cultural backgrounds. In the future, public health interventions should be tailored to different populations and contexts to better leverage social capital in promoting physical activity.
ZG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. CC: Conceptualization, Data curation, Formal analysis, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing. RO: Conceptualization, Data curation, Formal analysis, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing. YL: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Writing – original draft, Writing – review & editing. JG: Data curation, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing. RL: Data curation, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing. FL: Data curation, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing. XL: Data curation, Formal analysis, Project administration, Validation, Writing – original draft, Writing – review & editing. TW: Data curation, Formal analysis, Project administration, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1467571/full#supplementary-material
1. Memon AR, To QG, Vandelanotte C. Vigorously cited: a bibliometric analysis of the 500 most cited physical activity articles. J Phys Activity Health. (2021) 18:904–19. doi: 10.1123/jpah.2020-0744
2. Varela AR, Cruz GIN, Hallal P, Blumenberg C, da Silva SG, Salvo D, et al. Global, regional, and national trends and patterns in physical activity research since 1950: a systematic review. Int J Behav Nutr Phys Activ. (2021) 18:5. doi: 10.1186/s12966-021-01100-3
3. Sabe M, Chen C, Sentissi O, Deenik J, Vancampfort D, Firth J, et al. Thirty years of research on physical activity, mental health, and wellbeing: a scientometric analysis of hotspots and trends. Front Public Health. (2022) 10:943435. doi: 10.3389/fpubh.2022.943435
4. Ai X, Yang J, Lin Z, Wan X. Mental health and the role of physical activity during the COVID-19 pandemic. Front Psychol. (2021) 12:759987. doi: 10.3389/fpsyg.2021.759987
5. Liu Y, Zhang H, Xu R. The impact of technology on promoting physical activities and mental health: a gender-based study. BMC Psychol. (2023) 11:298. doi: 10.1186/s40359-023-01348-3
6. Mahindru A, Patil P, Agrawal V. Role of physical activity on mental health and well-being: a review. Cureus. (2023) 15:e33475. doi: 10.7759/cureus.33475
7. Warburton DER, Nicol CW, Bredin SSD. Health benefits of physical activity: the evidence. CMAJ. (2006) 174:801–809. doi: 10.1503/cmaj.051351
8. Anderson E, Durstine JL. Physical activity, exercise, and chronic diseases: a brief review. Sports Med Health Sci. (2019) 1:3–10. doi: 10.1016/j.smhs.2019.08.006
9. Misiag W, Piszczyk A, Szymańska-Chabowska A, Chabowski M. Physical activity and cancer care—a review. Cancers. (2022) 14:4154. doi: 10.3390/cancers14174154
10. John JM, Haug V, Thiel A. Physical activity behavior from a transdisciplinary biopsychosocial perspective: a scoping review. Sports Med Open. (2020) 6:49. doi: 10.1186/s40798-020-00279-2
11. Noh W, Kim KY. Review of ecological approach factors affecting physical activity among older people. West J Nurs Res. (2022) 44:799–808. doi: 10.1177/01939459211017530
12. Wang Y, Steenbergen B, van der Krabben E, Kooij HJ, Raaphorst K, Hoekman R. The impact of the built environment and social environment on physical activity: a scoping review. Int J Environ Res Public Health. (2023) 20:6189. doi: 10.3390/ijerph20126189
13. McNeill LH, Kreuter MW, Subramanian SV. Social environment and physical activity: a review of concepts and evidence. Soc Sci Med. (2006) 63:1011–22. doi: 10.1016/j.socscimed.2006.03.012
14. Chen W, Zhang C, Cui Z, Wang J, Zhao J, Wang J, et al. The impact of social capital on physical activity and nutrition in China: the mediating effect of health literacy. BMC Public Health. (2019) 19:1713. doi: 10.1186/s12889-019-8037-x
15. Aliyas Z. Social capital and physical activity level in an urban adult population. Am J Health Educ. (2020) 51:40–9. doi: 10.1080/19325037.2019.1691092
16. Villalonga-Olives E, Wind TR, Kawachi I. Social capital interventions in public health: a systematic review. Soc Sci Med. (2018) 212:203–18. doi: 10.1016/j.socscimed.2018.07.022
17. Ehsan A, Klaas HS, Bastianen A, Spini D. Social capital and health: a systematic review of systematic reviews. Population Health. (2019) 8:100425. doi: 10.1016/j.ssmph.2019.100425
18. Carradore M. Academic research output on social capital: a bibliometric and visualization analysis. Int J Sociol Soc Policy. (2022) 42:113–34. doi: 10.1108/IJSSP-11-2022-0281
19. Bhandari H, Yasunobu K. What is social capital? A comprehensive review of the concept. Asian J Soc Sci. (2009) 37:480–510. doi: 10.1163/156853109X436847
20. Murayama H, Fujiwara Y, Kawachi I. Social capital and health: a review of prospective multilevel studies. J Epidemiol. (2012) 22:179–87. doi: 10.2188/jea.JE20110128
21. Villalonga-Olives E, Kawachi I. The measurement of social capital. Gaceta Sanitaria. (2015) 29:62–4. doi: 10.1016/j.gaceta.2014.09.006
22. Kawachi I, Subramanian SV, Kim, D. Social capital and health. in Social Capital and Health, New York, NY: Springer (2008). p. 1–26. doi: 10.1007/978-0-387-71311-3_1
23. Harpham T, Grant E, Thomas E. Measuring social capital within health surveys: key issues. Health Policy Plan. (2002) 17:106–11. doi: 10.1093/heapol/17.1.106
24. Islam MK, Merlo J, Kawachi I, Lindström M, Gerdtham U. Social capital and health: does egalitarianism matter? A literature review. Int J Equity Health. (2006) 5:3. doi: 10.1186/1475-9276-5-3
25. Szreter S, Woolcock M. Health by association? Social capital, social theory, and the political economy of public health. Int J Epidemiol. (2004) 33:650–67. doi: 10.1093/ije/dyh013
26. Poortinga W. Community resilience and health: the role of bonding, bridging, and linking aspects of social capital. Health Place. (2012) 18:286–95. doi: 10.1016/j.healthplace.2011.09.017
27. Coll-Planas L, Nyqvist F, Puig T, Urrútia G, Solà I, Monteserín R. Social capital interventions targeting older people and their impact on health: a systematic review. J Epidemiol Commun Health. (2017) 71:663–672. doi: 10.1136/jech-2016-208131
28. Xue X, Reed WR, Menclova A. Social capital and health: a meta-analysis. J Health Econ. (2020) 72:102317. doi: 10.1016/j.jhealeco.2020.102317
29. Villalonga-Olives E, Kawachi I. The dark side of social capital: a systematic review of the negative health effects of social capital. Soc Sci Med. (2017) 194:105–27. doi: 10.1016/j.socscimed.2017.10.020
30. Rodgers J, Valuev AV, Hswen Y, Subramanian SV. Social Capital and Physical Health: An Updated Review of the Literature for 2007–2018′. Soc Sci Med. (2019) 236:112360. doi: 10.1016/j.socscimed.2019.112360
31. Wiltshire G, Stevinson C. Exploring the role of social capital in community-based physical activity: qualitative insights from parkrun. Qualit Res Sport, Exer Health. (2018) 10:47–62. doi: 10.1080/2159676X.2017.1376347
32. Flórez KR, Richardson AS, Ghosh-Dastidar M, Troxel W, DeSantis A, Colabianchi N, et al. The power of social networks and social support in promotion of physical activity and body mass index among African American adults. SSM - Populat Health. (2018) 4:327. doi: 10.1016/j.ssmph.2018.03.004
33. Luo M, Ding D, Bauman A, Negin J, Phongsavan P. Social engagement pattern, health behaviors and subjective well-being of older adults: an international perspective using WHO-SAGE survey data. BMC Public Health. (2020) 20:99. doi: 10.1186/s12889-019-7841-7
34. Du T, Li Y. Effects of social networks in promoting young adults' physical activity among different sociodemographic groups. Behav Sci. (2022) 12:345. doi: 10.3390/bs12090345
35. Novak D, Doubova SV, Kawachi I. Social capital and physical activity among croatian high school students. Public Health. (2016) 135:48–55. doi: 10.1016/j.puhe.2016.02.002
36. Lindström M. Social capital, desire to increase physical activity and leisure-time physical activity: a population-based study. Public Health. (2011) 125:442–7. doi: 10.1016/j.puhe.2011.01.015
37. Kim JR, Jeong B, Park KS, Kang YS. Association of social capital at the individual level with physical activity in communities with high mortality in Korea. Health Promot Int. (2017) 32:850–9. doi: 10.1093/heapro/daw017
38. Fu C, Wang C, Yang F, Cui D, Wang Q, Mao Z. Association between social capital and physical activity among community-dwelling elderly in Wuhan, China. Int J Gerontol. (2018) 12:155–9. doi: 10.1016/j.ijge.2017.10.001
39. Mendonça G, Cheng LA, Mélo EN, de Farias Júnior JC. Physical activity and social support in adolescents: a systematic review. Health Educ Res. (2014) 29:822–39. doi: 10.1093/her/cyu017
40. Lindsay Smith G, Banting L, Eime R, O'Sullivan G, van Uffelen JGZ. The association between social support and physical activity in older adults: a systematic review. Int J Behav Nutr Phys Activity. (2017) 14:56. doi: 10.1186/s12966-017-0509-8
41. Scarapicchia TMF, Amireault S, Faulkner G, Sabiston CM. Social support and physical activity participation among healthy adults: a systematic review of prospective studies. Int Rev Sport Exerc Psychol. (2017) 10:50–83. doi: 10.1080/1750984X.2016.1183222
42. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. (2021) 88:105906. doi: 10.1016/j.ijsu.2021.105906
43. Fisher KJ, Li F, Michael Y, Cleveland M. Neighborhood-level influences on physical activity among older adults: a multilevel analysis. J Aging Phys Act. (2004) 12:45–63. doi: 10.1123/japa.12.1.45
44. Cradock AL, Kawachi I, Colditz GA, Gortmaker SL, Buka SL. Neighborhood social cohesion and youth participation in physical activity in Chicago. Soc Sci Med. (2009) 68:427–35. doi: 10.1016/j.socscimed.2008.10.028
45. Ball K, Cleland VJ, Timperio AF, Salmon J, Giles-Corti B, Crawford DA. Love thy neighbour? Associations of social capital and crime with physical activity amongst women. Soc Sci Med. (2010) 71:807–14. doi: 10.1016/j.socscimed.2010.04.041
46. Shelton RC, McNeill LH, Puleo E, Wolin KY, Emmons KM, Bennett GG. The association between social factors and physical activity among low-income adults living in public housing. Am J Public Health. (2011) 101:2102–10. doi: 10.2105/AJPH.2010.196030
47. Utter J, Denny S, Robinson E, Ameratunga S, Milfont TL. Social and physical contexts of schools and neighborhoods: associations with physical activity among young people in New Zealand. Am J Public Health. (2011) 101:1690–5. doi: 10.2105/AJPH.TEST.2011.300171
48. Kaczynski AT, Glover TD. Talking the talk, walking the walk: examining the effect of neighbourhood walkability and social connectedness on physical activity. J Public Health. (2012) 34:382–9. doi: 10.1093/pubmed/fds011
49. Strong LL, Reitzel LR, Wetter DW, McNeill LH. Associations of perceived neighborhood physical and social environments with physical activity and television viewing in African-American men and women. Am J Health Promot. (2013) 27:401–9. doi: 10.4278/ajhp.120306-QUAN-127
50. Button B, Trites S, Janssen I. Relations between the school physical environment and school social capital with student physical activity levels. BMC Public Health. (2013) 13:1191. doi: 10.1186/1471-2458-13-1191
51. Pabayo R, Molnar BE, Cradock A, Ichiro K. The relationship between neighborhood socioeconomic characteristics and physical inactivity among adolescents living in Boston, Massachusetts. Am J Public Health. (2014) 104:e142–9. doi: 10.2105/AJPH.2014.302109
52. Jongeneel-Grimen B, Droomers MHAM, van Oers Stronks K, Kunst AE. The relationship between physical activity and the living environment: a multi-level analyses focusing on changes over time in environmental factors. Health Place. (2014) 26:149–160. doi: 10.1016/j.healthplace.2013.12.003
53. Moore S, Stewart S, Teixeira A. Decomposing social capital inequalities in health. J Epidemiol Commun Health. (2014) 68:233–8. doi: 10.1136/jech-2013-202996
54. Prins RG, Beenackers MA, Boog MC, Van Lenthe FJ, Brug J, Oenerna A. Neighbourhood social capital as a moderator between individual cognitions and sports behaviour among dutch adolescents. Soc Sci Med. (2014) 105:9–15. doi: 10.1016/j.socscimed.2013.12.031
55. Pabayo R, Janosz M, Bisset S, Kawachi I. School social fragmentation, economic deprivation and social cohesion and adolescent physical inactivity: a longitudinal study. PLoS ONE. (2014) 9:e99154. doi: 10.1371/journal.pone.0099154
56. Gao J, Fu H, Li J, Jia Y. Association between social and built environments and leisure-time physical activity among chinese older adults - a multilevel analysis energy balance-related behaviours. BMC Public Health. (2015) 15:3. doi: 10.1186/s12889-015-2684-3
57. Marlier M, Van Dyck D, Cardon G, De Bourdeaudhuij I, Babiak K, Willem A. Interrelation of sport participation, physical activity, social capital and mental health in disadvantaged communities: a SEM-analysis. PLoS ONE. (2015) 10:e0140196. doi: 10.1371/journal.pone.0140196
58. Andrade ACS, Peixoto SV, Friche AAL, Goston JL, César CC, Xavier CC, et al. Social context of neighborhood and socioeconomic status on leisure-time physical activity in a brazilian urban center: the BH health study. Cad Saude Publica. (2015) 31:S136–47. doi: 10.1590/0102-311X00069514
59. Yi SS, Trinh-Shevrin C, Yen IH, Kwon SC. Racial/ethnic differences in associations between neighborhood social cohesion and meeting physical activity guidelines, United States, 2013-2014′. Prevent Chron Dis. (2016) 13:160261. doi: 10.5888/pcd13.160261
60. Kamimura A, Tabler J, Nourian MM, Assasnik N, Wright L, Ashby J. Prevention and management of hypertension and diabetes using social capital and physical activity among socioeconomically disadvantaged populations. Family Commun Health. (2017) 40:205–11. doi: 10.1097/FCH.0000000000000156
61. Dlugonski D, Das BM, Martin TR, Palmer A. Collective efficacy, physical activity, and health outcomes among mothers. Family Commun Health. (2017) 40:316–23. doi: 10.1097/FCH.0000000000000162
62. Yuma-Guerrero P, Cubbin JC, von Sternberg K. Neighborhood social cohesion as a mediator of neighborhood conditions on mothers' engagement in physical activity: results from the geographic research on wellbeing study. Health Educ Behav. (2017) 44:845–856. doi: 10.1177/1090198116687537
63. Bartshe M, Coughenour C, Pharr J. Perceived walkability, social capital, and self-reported physical activity in las vegas college students. Sustainability. (2018) 10:3023. doi: 10.3390/su10093023
64. Rodrigues DE, César CC, Kawachi I, Xavier CC, Caiaffa WT, Proietti FA. The influence of neighborhood social capital on leisure-time physical activity: a population-based study in Brazil. J Urban Health-Bull New York Acad Med. (2018) 95:727–38. doi: 10.1007/s11524-018-0293-z
65. Vancampfort D, Stubbs B, Veronese N, Mugisha J, Swinnen N, Koyanagi A. Correlates of physical activity among depressed older people in six low-income and middle-income countries: a community-based cross-sectional study. Int J Geriatr Psychiatry. (2018) 33:e314–22. doi: 10.1002/gps.4796
66. Yamamoto M, Jo H. Perceived neighborhood walkability and physical exercise: an examination of casual communication in a social process. Health Place. (2018) 51:28–35. doi: 10.1016/j.healthplace.2018.02.006
67. Quinn TD, Wu F, Mody D, Bushover B, Mendez DD, Schiff M, et al. Associations between neighborhood social cohesion and physical activity in the united states, national health interview survey, 2017′. Prevent Chronic Dis. (2019) 16. doi: 10.5888/pcd16.190085
68. Heredia N, Nguyen N, McNeill LH. The importance of the social environment in achieving high levels of physical activity and fruit and vegetable intake in African American church members. Am J Health Promot. (2020) 34:886–93. doi: 10.1177/0890117120925361
69. Kim J, Kim J, Han A. Leisure time physical activity mediates the relationship between neighborhood social cohesion and mental health among older adults. J Appl Gerontol. (2020) 39:292–300. doi: 10.1177/0733464819859199
70. Feng Z, Cramm JM, Nieboer AP. Associations of social cohesion and socioeconomic status with health behaviours among middle-aged and older Chinese people. Int J Environ Res Public Health. (2021) 18:4894. doi: 10.3390/ijerph18094894
71. Mieziene B, Emeljanovas A, Tilindiene I, Tumynaite L, Trinkuniene L, Kawachi I. The direct and indirect relationships of environmental, interpersonal and personal factors with high school students physical activity: an ecological approach. Int J Environ Res Public Health. (2021) 18:1–16. doi: 10.3390/ijerph18030874
72. Wang ML, Narcisse MR, Alatorre S, Kozak AT, McElfish PA. Neighborhood social cohesion and physical activity and obesity outcomes among native hawaiian and pacific islander individuals. Obesity. (2022) 30:249–56. doi: 10.1002/oby.23298
73. Ganzar LA, Salvo D, Burford K, Zhang Y, Kohl HW, Hoelscher DM. Longitudinal changes in objectively-measured physical activity and sedentary time among school-age children in central Texas, US during the COVID-19 pandemic. Int J Behav Nutr Phys Act. (2022) 19:11. doi: 10.1186/s12966-022-01299-9
74. Cheng GJ, Nicklett EJ. Racial and ethnic differences in the relationship between neighborhood environment and physical activity among middle-aged and older adults. J Aging Health. (2022) 34:1163–77. doi: 10.1177/08982643221103359
75. Bartshe M, Coughenour C, Stephen H. The relationship between tree canopy and social capital on physical activity in college students. J Am College Health. (2023) 71:1705–14. doi: 10.1080/07448481.2021.1947299
76. Greiner KA, Li C, Kawachi I, Hunt DC, Ahluwalia JS. The relationships of social participation and community ratings to health and health behaviors in areas with high and low population density. Soc Sci Med. (2004) 59:2303–12. doi: 10.1016/j.socscimed.2004.03.023
77. Kim D, Subramanian SV, Gortmaker SL, Kawachi I. US state- and county-level social capital in relation to obesity and physical inactivity: a multilevel, multivariable analysis. Soc Sci Med. (2006) 63:1045–59. doi: 10.1016/j.socscimed.2006.02.017
78. Wen M, Browning CR, Cagney KA. Neighbourhood deprivation, social capital and regular exercise during adulthood: a multilevel study in Chicago. Urban Stud. (2007) 44:2651–71. doi: 10.1080/00420980701558418
79. Ueshima K, Fujiwara T, Takao S, Suzuki E, Iwase T, Doi H, et al. Does social capital promote physical activity? A population-based study in Japan. PLoS ONE. (2010) 5:e12135. doi: 10.1371/journal.pone.0012135
80. McNeill LH, Stoddard A, Bennett GG, Wolin KY, Sorensen GG. Influence of individual and social contextual factors on changes in leisure-time physical activity in working-class populations: results of the healthy directions-small businesses study. Cancer Causes Control. (2012) 23:1475–87. doi: 10.1007/s10552-012-0021-z
81. Legh-Jones H, Moore S. Network social capital, social participation, and physical inactivity in an urban adult population. Soc Sci Med. (2012) 74:1362–7. doi: 10.1016/j.socscimed.2012.01.005
82. Davison KK, Nishi A, Kranz S, Wyckoff L, May JJ, Earle-Richardson GB, et al. Associations among social capital, parenting for active lifestyles, and youth physical activity in rural families living in upstate New York. Soc Sci Med. (2012) 75:1488–96. doi: 10.1016/j.socscimed.2012.06.002
83. Nieminen T, Prättälä R, Martelin T, Härkänen T, Hyyppä MT, Alanen E, et al. Social capital, health behaviours and health: a population-based associational Study. BMC Public Health. (2013) 13:614. doi: 10.1186/1471-2458-13-613
84. Loch MR, Souza RK, Mesas AE, Martinez-Gómez D, Rodríguez-Artalejo F. Relationship between social capital indicators and lifestyle in Brazilian adults. Cadernos de Saúde Pública. (2015) 31:1636–47. doi: 10.1590/0102-311X00132614
85. Muthuri SK, Wachira LM, Onywera VO, Tremblay MS. Associations between parental perceptions of the neighborhood environment and childhood physical activity: results from ISCOLE-Kenya. J Phys Activity Health. (2016) 13:333–43. doi: 10.1123/jpah.2014-0595
86. Fang J, Wang JW, Li J, Li H, Shao C. The correlates of social capital and adherence to healthy lifestyle in patients with coronary heart disease. Patient Prefer Adherence. (2017) 11:1701–7. doi: 10.2147/PPA.S140787
87. Xue X, Cheng M. Social capital and health in china: exploring the mediating role of lifestyle. BMC Public Health. (2017) 17:6. doi: 10.1186/s12889-017-4883-6
88. Josey MJ, Moore S. The influence of social networks and the built environment on physical inactivity: a longitudinal study of urban-dwelling adults. Health Place. (2018) 54:62–8. doi: 10.1016/j.healthplace.2018.08.016
89. Yildizer G, Bilgin E, Korur EN, Novak D, Demirhan G. The association of various social capital indicators and physical activity participation among Turkish adolescents. J Sport Health Sci. (2018) 7:27–33. doi: 10.1016/j.jshs.2017.10.008
90. Yildizer G, Yilmaz I, Novak D. Social capital and physical activity participation among Turkish adolescents in urban centres: a preliminary study. South African J Res Sport Phys Educ Recreat. (2019) 41:117–29.
91. Jun HJ, Park S. The effect of cross-level interaction between community factors and social capital among individuals on physical activity: considering gender difference. Int J Environ Res Public Health. (2019) 16:495. doi: 10.3390/ijerph16030495
92. Liang H, Yue Z, Liu E, Xiang N. How does social capital affect individual health among the elderly in rural China?— Mediating effect analysis of physical exercise and positive attitude. PLoS ONE. (2020) 15:18. doi: 10.1371/journal.pone.0231318
93. Sugiyama S, Momma H, Yamada A, Huang C, Tatsuta N, Sakurai K, et al. Social capital and physical activity among japanese pregnant women: adjunct study of japan environment and children's study in Miyagi prefecture. Tohoku J Exper Med. (2023) 259:307–18. doi: 10.1620/tjem.2023.J004
94. Lindström M, Hanson BS, Östergren PO. Socioeconomic differences in leisure-time physical activity: the role of social participation and social capital in shaping health related behaviour. Soc Sci Med. (2001) 52:441–451. doi: 10.1016/S0277-9536(00)00153-2
95. Lindström M, Moghaddassi M, Merlo J. Social capital and leisure time physical activity: a population based multilevel analysis in Malmö, Sweden. J Epidemiol Commun Health. (2003) 57:23–8. doi: 10.1136/jech.57.1.23
96. Zlot AI, Librett J, Buchner D, Schmid T. Environmental, transportation, social, and time barriers to physical activity. J Phys Activity Health. (2006) 3:15–21. doi: 10.1123/jpah.3.1.15
97. Mummery WK, Lauder W, Schofield G, Caperchione C. Associations between physical inactivity and a measure of social capital in a sample of Queensland adults. J Sci Med Sport. (2008) 11:308–15. doi: 10.1016/j.jsams.2007.06.002
98. Logstein B, Blekesaune A, Almås R. Physical activity among Norwegian adolescents a multilevel analysis of how place of residence is associated with health behaviour: the young-HUNT study. Int J Equity Health. (2013) 12:56. doi: 10.1186/1475-9276-12-56
99. Kim BH, Wallington SF, Makambi KH, Adams-Campbell LL. Social networks and physical activity behaviors among cancer survivors: data from the 2005 health information national trends survey. J Health Commun. (2015) 20:656–62. doi: 10.1080/10810730.2015.1018576
100. Johnson-Lawrence V, Schulz AJ, Zenk SN, Israel BA, Wineman J, Marans RW, et al. Joint associations of residential density and neighborhood involvement with physical activity among a multiethnic sample of urban adults. Health Educ Behav. (2015) 42:510–7. doi: 10.1177/1090198114564500
101. Babey SH, Wolstein J, Diamant AL. Adolescent physical activity: role of school support, role models, and social participation in racial and income disparities. Environ Behav. (2016) 48:172–91. doi: 10.1177/0013916515609086
102. Becky M, Gonzalez P, Gallo L, Ji M. Latino civic group participation, social networks, physical activity. Am J Health Behav. (2016) 40:437–45. doi: 10.5993/AJHB.40.4.5
103. Kikuchi H, Inoue S, Fukushima N, Takamiya T, Odagiri Y, Ohya Y, et al. Social participation among older adults not engaged in full- or part-time work is associated with more physical activity and less sedentary time. Geriatr Gerontol Int. (2017) 17:1921–7. doi: 10.1111/ggi.12995
104. Ho EC, Hawkley L, Dale W, Waite L, Huisingh-Scheetz M. Social capital predicts accelerometry-measured physical activity among older adults in the US: a cross-sectional study in the national social life, health, aging project. BMC Public Health. (2018) 18. doi: 10.1186/s12889-018-5664-6
105. Davis CMA, Sentell TL, de Souza Barbosa JF, Ylli A, Curcio C, Pirkle CM. Meeting physical activity guidelines by walking in older adults from three middle-income countries: a cross-sectional analysis from the international mobility in aging study. J Aging Phys Act. (2020) 28:333–42. doi: 10.1123/japa.2018-0463
106. Ward M, Gibney S, O'Callaghan D, Shannon S. Age-friendly environments, active lives? Associations between the local physical and social environment and physical activity among adults aged 55 and older in Ireland. J Aging Phys Act. (2020) 28:140–48. doi: 10.1123/japa.2019-0012
107. Boen F, Pelssers J, Scheerder J, Vanbeselaere N, Vos S, Hurkmans E, et al. Does social capital benefit older adults' health and well-being? the mediating role of physical activity. J Aging Health. (2020) 32:688–97. doi: 10.1177/0898264319848638
108. Zhao J, Ma Y, Tanimoto T, Ozaki A, Chen WL, Wang JY, et al. Effects of physical activity and stress on the relationship between social capital and quality of life among breast cancer survivors. Sci Rep. (2020) 10:5. doi: 10.1038/s41598-020-74706-5
109. Sasaki S, Sato A, Tanabe Y, Matsuoka S, Adachi A, Kayano T, et al. Associations between socioeconomic status, social participation, and physical activity in older people during the COVID-19 pandemic: a cross-sectional study in a northern Japanese city. Int J Environ Res Public Health. (2021) 18:1477. doi: 10.3390/ijerph18041477
110. Herbolsheimer F, Ungar N, Portegijs E, Dallmeier D, Schaap L, Smith TB, et al. Neighborhood environment, social participation, and physical activity in older adults with lower limb osteoarthritis: a mediation analysis. Health Place. (2021) 68:7. doi: 10.1016/j.healthplace.2021.102513
111. Nemoto Y, Sato S, Kitabatake Y, Nakamura M, Takeda N, Maruo K, et al. Longitudinal associations of social group engagement with physical activity among Japanese older adults. Arch Gerontol Geriatr. (2021) 92:104092. doi: 10.1016/j.archger.2020.104259
112. Otaki N, Yokoro M, Yano M, Imamura T, Akita M, Tanino N, et al. Social contact impacts physical activity and sedentary behavior among older adults in japan due to COVID-19. BMC Geriatr. (2022) 22:491. doi: 10.1186/s12877-022-03188-z
113. Zimmer C, McDonough MH. Social support and physical activity in older adults: identifying predictors using data from the Canadian longitudinal study on aging. J Aging Phys Act. (2022) 30:136–47. doi: 10.1123/japa.2020-0393
114. Dwyer LA, Patel M, Nebeling LC, Oh AY. Independent associations and interactions of perceived neighborhood and psychosocial constructs on adults' physical activity. J Phys Activity Health. (2018) 15:361–8. doi: 10.1123/jpah.2017-0202
115. Wang RY, Chen HS, Liu Y, Lu Y, Yao Y. Neighborhood social reciprocity and mental health among older adults in china: the mediating effects of physical activity, social interaction, and volunteering. BMC Public Health. (2019) 19:1036. doi: 10.1186/s12889-019-7385-x
116. Unger JB, Johnson CA. Social relationships and physical-activity in health club members. Am J Health Promot. (1995) 9:340–3. doi: 10.4278/0890-1171-9.5.340
117. Azar D, Naughton GA, Joseph CW. Physical activity and social connectedness in single-parent families. Leisure Stud. (2009) 28:349–58. doi: 10.1080/02614360903046656
118. Lightner J, Irwin BC, Chrisman M. Changes in social integration predict changes in physical activity: a 25-year prospective study. J Phys Activity Health. (2018) 15:531–6. doi: 10.1123/jpah.2017-0009
119. Pérez LM, Castellano-Tejedor C, Cesari M, Soto-Bagaria L, Ars J, Zambom-Ferraresi F, et al. Depressive symptoms, fatigue and social relationships influenced physical activity in frail older community-dwellers during the spanish lockdown due to the COVID-19 pandemic. Int J Environ Res Public Health. (2021) 18:808. doi: 10.3390/ijerph18020808
120. Yamashita R, Sato S, Akase R, Doi T, Tsuzuku S, Yokoi T, et al. Effects of social network incentives and financial incentives on physical activity and social capital among older women: a randomized controlled trial. BMC Public Health. (2021) 21:188. doi: 10.1186/s12889-021-10175-3
121. Liu Y, Lachman ME. A group-based walking study to enhance physical activity among older adults: the role of social engagement. Res Aging. (2021) 43:368–77. doi: 10.1177/0164027520963613
122. Wieland ML, Njeru JW, Asiedu GB, Zeratsky KA, Clark MM, Goetze R, et al. Pilot social network weight loss intervention with two immigrant populations during the COVID-19 pandemic. Am J Health Promot. (2022) 36:458–71. doi: 10.1177/08901171211053450
123. Crandall CJ, Larson J, Cene CW, Bellettiere J, Laddu D, Jackson RD, et al. Relationship of social connectedness with decreasing physical activity during the COVID-19 pandemic among older women participating in the women's health initiative study. J Gerontol. (2022) 77:S22–30. doi: 10.1093/gerona/glac108
124. Xie H, Salinas-Mosombite D, Spear SE. Residential mobility and adolescents' physical activity: the mediating role of neighborhood social ties. J Hum Behav Soc Environ. (2024) 34:221–33. doi: 10.1080/10911359.2023.2219706
125. Voorhees CC, Murray D, Welk G, Birnbaum A, Ribisl KM, Johnson CC, et al. The role of peer social network factors and physical activity in adolescent girls. Am J Health Behav. (2005) 29:183–90. doi: 10.5993/AJHB.29.2.9
126. Peláez S, Lavoie KL, Gordon JL, Arsenault A, Bacon SL. Social networks and exercise in coronary heart disease patients. J Cardiopulm Rehabil Prev. (2010) 30:324–8. doi: 10.1097/HCR.0b013e3181d8dd12
127. Yu G, Renton A, Schmidt E, Tobi P, Bertotti M, Watts P, et al. A multilevel analysis of the association between social networks and support on leisure time physical activity: evidence from 40 disadvantaged areas in London. Health Place. (2011) 17:1023–9. doi: 10.1016/j.healthplace.2011.07.002
128. Shiovitz-Ezra S, Litwin H. Social network type and health-related behaviors: evidence from an american national survey. Soc Sci Med. (2012) 75:901–4. doi: 10.1016/j.socscimed.2012.04.031
129. Gesell SB, Tesdahl E, Ruchman E. The distribution of physical activity in an after-school friendship network. Pediatrics. (2012) 129:1064–71. doi: 10.1542/peds.2011-2567
130. Larsen B, Strong D, Linke S. The association between family and friend integration and physical activity: results from the NHIS. Int J Behav Med. (2014) 21:529–36. doi: 10.1007/s12529-013-9318-x
131. Marquez B, Elder JP, Arredondo EM, Madanat H, Ji M, Ayala GX. Social network characteristics associated with health promoting behaviors among latinos. Health Psychol. (2014) 33:544–53. doi: 10.1037/hea0000092
132. Shin HS, Valente TW, Riggs NR, Huh J, Spruijt-Metz D, Chou CP, et al. The interaction of social networks and child obesity prevention program effects: the pathways trial. Obesity. (2014) 22:1520–6. doi: 10.1002/oby.20731
133. Kennedy-Hendricks A, Schwartz H, Thornton RJ, Griffin BA, Green HDJr, Kennedy DP, et al. Intergenerational social networks and health behaviors among children living in public housing. Am J Public Health. (2015) 105:2291–7. doi: 10.2105/AJPH.2015.302663
134. Calogiuri G. Natural environments and childhood experiences promoting physical activity, examining the mediational effects of feelings about nature and social networks. Int J Environ Res Public Health. (2016) 13:439. doi: 10.3390/ijerph13040439
135. Harmon BE, Forthofer M, Bantum EO, Nigg CR. Perceived influence and college students' diet and physical activity behaviors: an examination of ego-centric social networks. BMC Public Health. (2016) 16:473. doi: 10.1186/s12889-016-3166-y
136. Clarke CL, Sniehotta FF, Vadiveloo T, Argo IS, Donnan PT, McMurdo MET, et al. Factors associated with change in objectively measured physical activity in older people - data from the physical activity cohort scotland study. BMC Geriatr. (2017) 17:578. doi: 10.1186/s12877-017-0578-1
137. Haynie DL, Whichard C, Kreager DA, Schaefer DR, Wakefield S. Social networks and health in a prison unit. J Health Soc Behav. (2018) 59:318–34. doi: 10.1177/0022146518790935
138. Marquez B, Norman G, Fowler J, Gans K, Marcus B. Egocentric networks and physical activity outcomes in latinas. PLoS ONE. (2018) 13:e0199139. doi: 10.1371/journal.pone.0199139
139. Seino S, Kitamura A, Nishi M, Tomine Y, Tanaka I, Taniguchi Y, et al. Individual- and community-level neighbor relationships and physical activity among older japanese adults living in a metropolitan area: a cross-sectional multilevel analysis. Int J Behav Nutr Phys Act. (2018) 15:11. doi: 10.1186/s12966-018-0679-z
140. Fingerman KL, Huo M, Charles ST, Umberson DJ. Variety is the spice of late life: social integration and daily activity. J Gerontol. (2020) 75:377–88. doi: 10.1093/geronb/gbz007
141. Thanawala MS, Siddique J, Schneider JA, Kanaya AM, Cooper AJ, Dave SS, et al. Association of social networks and physical activity in south asians: the mediators of atherosclerosis in south Asians living in America cohort study. J Phys Activity Health. (2020) 17:149–55. doi: 10.1123/jpah.2019-0099
142. Montgomery SC, Donnelly M, Badham J, Kee F, Dunne L, Hunter RF. A multi-method exploration into the social networks of young teenagers and their physical activity behavior. BMC Public Health. (2021) 21:77. doi: 10.1186/s12889-020-10081-0
143. Cho SMJ, Lee H, Shim JS, Youm Y, Jung SJ, Kim DJ, et al. Association between social network structure and physical activity in middle-aged Korean adults. Soc Sci Med. (2021) 282. doi: 10.1016/j.socscimed.2021.114112
144. Wray B, Grimes A, Eighmy K, Lightner J. The relationship between social integration and physical activity, diet, and sleep among youths: cross-sectional survey study. JMIR Pediatr Parent. (2022) 5:40354. doi: 10.2196/40354
145. Prochnow T, Park JH, Patterson MS. Intramural sports social networks and implications for college student physical activity, sense of community, and retention. J Am College Health. (2023) 2:1–7. doi: 10.1080/07448481.2023.2239367
146. Dlugonski D, Das BM, Martin TR. Impact of a standard versus collective-efficacy enhanced intervention to increase physical activity among mothers. Psychol Health. (2020) 35:239–53. doi: 10.1080/08870446.2019.1626397
147. Kronaizl SG, Koss KJ. Perceived neighbourhood collective efficacy and adolescent health determinants: investigating outdoor play as a mediator. Child Care Health Dev. (2023) 49:933–40. doi: 10.1111/cch.13103
148. Ruijsbroek A, Droomers M, Groenewegen PP, Hardyns W, Stronks K. Social safety, self-rated general health and physical activity: changes in area crime, area safety feelings and the role of social cohesion. Health and Place. (2015) 31:39–45. doi: 10.1016/j.healthplace.2014.10.008
149. Akosile CO, Ngwu NP, Okonkwo UP, Onwuakagba IU, Okoye EC. Neighborhood safety, fall indices, physical activity level and social participation restrictions from a population of community-dwelling older adults in Nsukka, Enugu State, Nigeria. BMC Geriatr. (2023) 23:358. doi: 10.1186/s12877-023-04059-x
150. Manca AR. Social cohesion. In: Alex Michalos C., editor. Encyclopedia of Quality of Life and Well-Being Research. Dordrecht: Springer Netherlands (2014). p. 6026–28. doi: 10.1007/978-94-007-0753-5_2739
151. Miller HN, Thornton CP, Rodney T, Thorpe RJ, Allen J. Social cohesion in health. ANS. (2020) 43:375–90. doi: 10.1097/ANS.0000000000000327
152. Cramm JM, van Dijk HM, Nieboer AP. The importance of neighborhood social cohesion and social capital for the well being of older adults in the community. Gerontologist. (2013) 53:142–52. doi: 10.1093/geront/gns052
153. Jennings V, Bamkole O. The relationship between social cohesion and urban green space: an avenue for health promotion. Int J Environ Res Public Health. (2019) 16:452. doi: 10.3390/ijerph16030452
154. Chuang Y, Chuang K, Yang T. Social cohesion matters in health. Int J Equity Health. (2013) 12:87. doi: 10.1186/1475-9276-12-87
155. Six B, van Zimmeren E, Popa F, Frison C. Trust and social capital in the design and evolution of institutions for collective action. Int J Commons. (2015) 9:151–76. doi: 10.18352/bmgn-lchr.435
156. Di Napoli I, Dolce P, Arcidiacono C. Community trust: a social indicator related to community engagement. Soc Indic Res. (2019) 145:551–79. doi: 10.1007/s11205-019-02114-y
157. Lansing AE, Romero NJ, Siantz E, Silva V, Center K, Casteel D, et al. Building trust: leadership reflections on community empowerment and engagement in a large urban initiative. BMC Public Health. (2023) 23:1252. doi: 10.1186/s12889-023-15860-z
158. Zwart R, Hines R. Community wellness and social support as motivation for participation in outdoor adventure recreation. J Outdoor Recreat Educ Leader. (2022) 14:11139. doi: 10.18666/JOREL-2022-V14-I1-11139
159. Levasseur M, Richard L, Gauvin L, Raymond E. Inventory and analysis of definitions of social participation found in the aging literature: proposed taxonomy of social activities. Soc Sci Med. (2010) 71:2141–9. doi: 10.1016/j.socscimed.2010.09.041
160. Wanchai A, Phrompayak D. Social participation types and benefits on health outcomes for elder people: a systematic review. Ageing Int. (2019) 44:9338. doi: 10.1007/s12126-018-9338-6
161. Chen J, Zeng Y, Fang Y. Effects of social participation patterns and living arrangement on mental health of Chinese older adults: a latent class analysis. Front Public Health. (2022) 10:915541. doi: 10.3389/fpubh.2022.915541
162. Tcymbal A, Abu-Omar K, Hartung V, Bußkamp A, Comito C, Rossmann C, et al. Interventions simultaneously promoting social participation and physical activity in community living older adults: a systematic review. Front Public Health. (2022) 10:1048496. doi: 10.3389/fpubh.2022.1048496
163. Gouldner AW. The norm of reciprocity: a preliminary statement. Am Sociol Rev. (1960) 25:161. doi: 10.2307/2092623
164. Sánchez-Franco MJ, Roldán J. The influence of familiarity, trust and norms of reciprocity on an experienced sense of community: an empirical analysis based on social online services. Behav Inf Technol. (2015) 34:92–412. doi: 10.1080/0144929X.2014.959455
165. Ngai SS, Cheung CK, Mo J, Chau SY, Yu EN, Wang L, et al. Mediating effects of emotional support reception and provision on the relationship between group interaction and psychological well-being: a study of young patients. Int J Environ Res Public Health. (2021) 18:12110. doi: 10.3390/ijerph182212110
166. Adriaanse CCM. Measuring residential satisfaction: a residential environmental satisfaction scale (RESS). J Hous Built Environ. (2007) 22:287–304. doi: 10.1007/s10901-007-9082-9
167. Sugiyama T, Leslie E, Giles-Corti B, Owen N. Physical activity for recreation or exercise on neighbourhood streets: associations with perceived environmental attributes. Health Place. (2009) 15:1058–63. doi: 10.1016/j.healthplace.2009.05.001
168. Zhang Y, van Dijk T, Wagenaar C. How the built environment promotes residents' physical activity: the importance of a holistic people-centered perspective. Int J Environ Res Public Health. (2022) 19:5595. doi: 10.3390/ijerph19095595
169. Zeng E, Dong Y, Yan L, Lin A. Perceived safety in the neighborhood: exploring the role of built environment, social factors, physical activity and multiple pathways of influence. Buildings. (2023) 13:2. doi: 10.3390/buildings13010002
170. Berkman LF, Glass T, Brissette I, Seeman TE. From social integration to health: durkheim in the new millennium. Soc Sci Med. (2000) 51:843–57. doi: 10.1016/S0277-9536(00)00065-4
171. Latkin CA, Knowlton AR. Social network assessments and interventions for health behavior change: a critical review. Behav Med. (2015) 41:90–7. doi: 10.1080/08964289.2015.1034645
172. van Woudenberg TJ, Simoski B, Fernandes de Mello Araújo E, Bevelander KE, Burk WJ, Smit CR, et al. Identifying influence agents that promote physical activity through the simulation of social network interventions: agent-based modeling study. J Med Internet Res. (2019) 21:e12914. doi: 10.2196/12914
173. Van Woudenberg TJ, Bevelander KE, Burk WJ, Smit CR, Buijs L, Buijzen M. Testing a social network intervention using vlogs to promote physical activity among adolescents: a randomized controlled trial. Front Psychol. (2020) 10:2913. doi: 10.3389/fpsyg.2019.02913
174. Pescosolido B, Levy J. The role of social networks in health, illness, disease and healing: the accepting present, the forgotten past, and the dangerous potential for a complacent future. Adv Med Sociol. (2001) 8:3–25. doi: 10.1016/S1057-6290(02)80019-5
175. Smith KP, Christakis NA. Social networks and health. Annu Rev Sociol. (2008) 34:405–29. doi: 10.1146/annurev.soc.34.040507.134601
176. Samtleben C, Müller K. Care and careers: gender (in)equality in unpaid care, housework and employment. Res Soc Stratif Mobil. (2022) 77:100659. doi: 10.1016/j.rssm.2021.100659
177. Miao X, Han J, Wang S, Han B. Impacts of family care for children and the elderly on women's employment: evidence from rural China. Front Psychol. (2023) 14:1208749. doi: 10.3389/fpsyg.2023.1208749
178. Henderson K, Ainsworth B. The connections between social support and women's physical activity involvement: the cultural activity participation study. Women Sport Phys Activ J. (2000) 9:27–53. doi: 10.1123/wspaj.9.2.27
179. Segar M, Taber JM, Patrick H, Thai CL, Oh A. Rethinking physical activity communication: using focus groups to understand women's goals, values, and beliefs to improve public health. BMC Public Health. (2017) 17:462. doi: 10.1186/s12889-017-4361-1
180. Eriksson U, Arvidsson D, Sundquist K. Availability of exercise facilities and physical activity in 2,037 adults: cross-sectional results from the swedish neighborhood and physical activity (SNAP) study. BMC Public Health. (2012) 12:607. doi: 10.1186/1471-2458-12-607
181. Lin L, Liu Q, Xiao X, Luo Q. Perceived constraints on active recreational sport participation among residents in urban China. Int J Environ Res Public Health. (2022) 19:14884. doi: 10.3390/ijerph192214884
182. Kaljee ML, Chen X. Social capital and risk and protective behaviors: a global health perspective. Adolesc Health Med Ther. (2011) 2:113–22. doi: 10.2147/AHMT.S26560
183. Santini ZI, Jose PE, Koyanagi A, Meilstrup C, Nielsen L, Madsen KR, et al. Formal social participation protects physical health through enhanced mental health: a longitudinal mediation analysis using three consecutive waves of the survey of health, ageing and retirement in Europe (SHARE). Soc Sci Med. (2020) 251:112906. doi: 10.1016/j.socscimed.2020.112906
184. Snel E, Engbersen G, de Boom J, van Bochove M. (2022). Social capital as protection against the mental health impact of the COVID-19 pandemic. Front Sociol. 7:728541. doi: 10.3389/fsoc.2022.728541
185. Becker R. Voting behavior as social action: habits, norms, values, and rationality in electoral participation. Ration Soc. (2023) 35:81–109. doi: 10.1177/10434631221142733
186. Kulachai W, Lerdtomornsakul U, Homyamyen P. Factors influencing voting decision: a comprehensive literature review. Soc Sci. (2023) 12:469. doi: 10.3390/socsci12090469
187. Hipp JR. Collective efficacy: how is it conceptualized, how is it measured, and does it really matter for understanding perceived neighborhood crime and disorder? J Crim Justice. (2016) 49:32–44. doi: 10.1016/j.jcrimjus.2016.02.016
188. Carroll J, Reese D. Community collective efficacy: structure and consequences of perceived capacities in the blacksburg electronic village. In: 36th Annual Hawaii International Conference on System Sciences. (2003). doi: 10.1109/HICSS.2003.1174585
189. Drakulich KM. Social capital and collective efficacy. In: G. Bruinsma and D. Weisburd, editors. Encyclopedia of Criminology and Criminal Justice, New York, NY: Springer (2014). p. 4891–99. doi: 10.1007/978-1-4614-5690-2_428
190. Sampson R. Neighbourhood and community: collective efficacy and community safety. New Econ. (2004) 11:106–13. doi: 10.1111/j.1468-0041.2004.00346.x
191. Prince DM, Hohl B, Hunter BA, Thompson AB, Matlin SL, Hausman AJ, et al. Collective efficacy as a key context in neighborhood support for urban youth. Am J Community Psychol. (2019) 63:179–89. doi: 10.1002/ajcp.12311
192. Bennett GG, McNeill LH, Wolin KY, Duncan DT, Puleo E, Emmons KM. Safe to walk? Neighborhood safety and physical activity among public housing residents. PLoS Med. (2007) 4:e306. doi: 10.1371/journal.pmed.0040306
193. Rees-Punia E, Hathaway ED, Gay JL. Crime, perceived safety, and physical activity: a meta-analysis. Prevent Med. (2018) 111:307–13. doi: 10.1016/j.ypmed.2017.11.017
194. da Silva IC, Payne VL, Hino AA, Varela AR, Reis RS, Ekelund U, et al. Physical activity and safety from crime among adults: a systematic review. J Phys Activity Health. (2016) 13:663–70. doi: 10.1123/jpah.2015-0156
195. Bicchieri C, Muldoon R. Social norms. In: Z. N. Edward, U. Nodelman., editors. The Stanford Encyclopedia of Philosophy, Stanford University (2014).
196. Deliens T, Deforche B, De Bourdeaudhuij I, Clarys P. Determinants of physical activity and sedentary behaviour in university students: a qualitative study using focus group discussions. BMC Public Health. (2015) 15:201. doi: 10.1186/s12889-015-1553-4
197. Kekäläinen T, Tammelin TH, Hagger MS, Lintunen T, Hyvärinen M, Kujala UM, et al. Personality, motivational, and social cognition predictors of leisure-time physical activity. Psychol Sport Exerc. (2022) 60:102135. doi: 10.1016/j.psychsport.2022.102135
198. Kim J, Dunn E, Rellinger K, Robertson-Wilson J, Eys M. Social norms and physical activity in american and Canadian contexts: a scoping review. Int Rev Sport Exerc Psychol. (2017) 12:1–23. doi: 10.1080/1750984X.2017.1354229
199. Li N, Huang Q, Ge X, He M, Cui S, Huang P, et al. A review of the research progress of social network structure. Complexity. (2021) 2021:e6692210. doi: 10.1155/2021/6692210
200. Macdonald-Wallis K, Jago R, Sterne JAC. Social network analysis of childhood and youth physical activity: a systematic review. Am J Prev Med. (2012) 43:636–42. doi: 10.1016/j.amepre.2012.08.021
201. Prochnow T, Delgado H, Patterson MS, Umstattd Meyer MR. Social network analysis in child and adolescent physical activity research: a systematic literature review. J Phys Activity Health. (2020) 17:250–60. doi: 10.1123/jpah.2019-0350
202. Prochnow T, Patterson MS. Assessing social network influences on adult physical activity using social network analysis: a systematic review. Am J Health Promot. (2022) 36:537–58. doi: 10.1177/08901171211060701
203. Kurlychek MC. Social control. In: G. Bruinsma and D. Weisburd, editors. Encyclopedia of Criminology and Criminal Justice, New York, NY: Springer (2014). p. 4899–4908. doi: 10.1007/978-1-4614-5690-2_360
204. Knoll N, Burkert S, Scholz U, Roigas J, Gralla O. The dual-effects model of social control revisited: relationship satisfaction as a moderator. Anxiety Stress Coping. (2012) 25:291–307. doi: 10.1080/10615806.2011.584188
205. Scholz U, Stadler G, Berli C, Lüscher J, Knoll N. How do people experience and respond to social control from their partner? Three daily diary studies. Front Psychol. (2021) 11:613546. doi: 10.3389/fpsyg.2020.613546
206. Smith GSE, Moyle W, Burton NW. The relationship between social support for physical activity and physical activity across nine years in adults aged 60–65 years at baseline. Int J Environ Res Public Health. (2023) 20:4531. doi: 10.3390/ijerph20054531
207. Choi M, Mesa-Frias M, Nuesch E, Hargreaves J, Prieto-Merino D, Bowling A, et al. Social capital, mortality, cardiovascular events and cancer: a systematic review of prospective studies. Int J Epidemiol. (2014) 43:1895–1920. doi: 10.1093/ije/dyu212
Keywords: social capital, physical activity, public health, social cohesion, social trust, social participation, norms of reciprocity, social networks
Citation: Gao Z, Chee CS, Omar Dev RD, Liu Y, Gao J, Li R, Li F, Liu X and Wang T (2025) Social capital and physical activity: a literature review up to March 2024. Front. Public Health 13:1467571. doi: 10.3389/fpubh.2025.1467571
Received: 20 July 2024; Accepted: 27 January 2025;
Published: 12 February 2025.
Edited by:
Daniela Stackeová, College of Physical Education and Sport Palestra, CzechiaReviewed by:
John R. Tower, Victoria University, AustraliaCopyright © 2025 Gao, Chee, Omar Dev, Liu, Gao, Li, Li, Liu and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chen Soon Chee, Y3NjaGVlQHVwbS5lZHUubXk=; Yutong Liu, bGl1eXV0b25nQGx6dS5lZHUuY24=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.