 Olanrewaju Onigbogi
Olanrewaju Onigbogi Omobola Yetunde Ojo4
Omobola Yetunde Ojo4 Kaija Saranto
Kaija Saranto
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health , 28 January 2025
Sec. Children and Health
Volume 13 - 2025 | https://doi.org/10.3389/fpubh.2025.1392709
Objectives: Increased mobile phone use in Low- and Middle-Income countries (LMIC) has led to suggestions that health interventions using mobile phones can help solve some health problems. Vaccination has been shown to be an effective means of improving health outcomes. However, vaccination coverage in many LMIC has been generally low. The aim of this study was to synthesize evidence concerning the context, mechanisms, and outcome elements of mobile health interventions in improving vaccination coverage among children under 5 years of age in LMIC.
Methods: A search conducted using PubMed, Web of Science, ScienceDirect, CINAHL, Embase, and the Cochrane library led to 27 studies included in the final analysis out of 357 identified articles.
Results: Twenty-one studies were from Africa, four from Asia and two studies were from Latin America and the Caribbean. Short Message Service (SMS) intervention was used exclusively in 21 studies while six studies used a combination of SMS and phone calls, and one intervention was based only on phone calls.
Conclusion: The results from most studies suggest an improved uptake of vaccination with mobile health interventions. However, there is a need for further research to quantify the impact of these interventions and determine the most effective strategies.
Mobile health (mHealth) technologies have been implemented in Low- and Middle-income countries (LMIC) to address public health challenges (1, 2). Many of these technologies were designed to either influence patients’, caregivers’, or health workers’ behavior or impact health outcomes (3–5). The World Health Organization (WHO) Global Observatory for eHealth defines mHealth as a medical and public health practice supported by mobile devices, such as mobile phones, patient monitoring devices, personal digital assistants, and other wireless devices (6).
According to the International Telecommunication Union, the number of mobile users worldwide in year 2021 stood at 7.1 billion and is projected to reach 7.49 billion by 2025 (7, 8). The majority of smartphone users are expected to be in developing countries (9, 10). In addition, mobile phone subscriptions in many LMIC have been shown to expand faster than other infrastructure (11, 12). Moreover, mobile phone access in these countries is greater than 60% because of personal or shared ownership (13). Characteristics such as mobility, instantaneous communication, relative cheap cost, and ability to use for long periods without electric power and in comparison, to other communication infrastructures may be contributing to this expansion (13).
mHealth activities include the use of applications and technologies such as voice, text messaging, also referred to as Short Message Service (SMS), and multimedia message services (14). Therefore, the relative ease of use of mobile phones for SMS has the potential of transforming maternal and child health services, especially in LMIC where investment in health care infrastructure is generally low. mHealth interventions could impact the attainment of the global targets 3.1 and 3.2 of reducing maternal, neonatal and under 5-year mortality under the Sustainable Development Goals 3 (15).
In addition, vaccines are generally believed to set one of the highest standards on ‘return on investment’ in the field of public health because they are highly cost-saving. Vaccination has been proven to be a cost-effective means of improving health outcomes in many parts of the world. A study in the United States (U.S) estimated that every dollar spent on childhood vaccination resulted in a US$3 savings from a payer perspective and a US$10 savings from a societal perspective (16). External factors such as social and political disruptions, disruption of household integrity, school absenteeism, health care utilization and long-term/on-going disability are usually considered in assessing the success of vaccination programs (17–21). Childhood vaccination with the measles antigen is believed to have long-term benefits of preventing all-cause infectious disease by preventing measles-associated immune memory loss and protecting polymicrobial herd immunity (22). Extra attention has been paid to the measles virus in comparison to other viruses responsible for childhood illnesses because of its capacity to cause long-term damage to the immune system, leaving people vulnerable to other infections (22).
Despite the obvious benefits of childhood vaccination, morbidity and mortality from vaccine-preventable diseases continue to challenge the health care systems in LMIC due to limited health infrastructure and a dearth of qualified personnel (23–25). There is an urgent need to address worldwide disparities in health outcomes by exploring innovative means of improving vaccination coverage (26, 27).
The recent increase in reports on the use of mHealth applications to facilitate vaccine uptake has resulted in questions about how effective these approaches are in LMIC (28, 29). Reminders via SMS have been used in some interventions to address memory lapses which is a common reason given for the failure of mothers or care-givers to present their children or wards for vaccination during the next due date (30, 31). mHealth techniques have also been used to exchange health information with caregivers about vaccine dosages and adverse drug reactions. The general belief is that the use of mHealth interventions has the potential to address some of the issues and challenges related to failure of caregivers to take their wards for vaccination (32, 33). However, there are other factors that researchers had observed limit vaccination access in these settings: these include the level of literacy, role of family decision makers, poverty, lack of access roads, and concerns about the safety of the women and children who ought to be vaccinated (33). The possibility of using mHealth interventions to circumvent some of these barriers to vaccination, could lead to improvement in coverage especially in LMIC. Countries that fall into LMIC classification by the World Bank have an average per capita government spending on health of about US$15 in 2018 and received donor financing for vaccines through the Global Alliance for Vaccine (34). In addition, there have been reports of socioeconomic inequalities in child vaccination in these countries (35, 36). Previous reviews, show that systematic reviews and meta-analyses demonstrate trends and design models capable of improving the impact of mHealth interventions on health care outcomes including vaccination (37, 38). These reviews tend to look at the effectiveness of interventions (quantitative) or experiences (qualitative). Furthermore, some vaccination interventions with mixed information delivery modes have been shown to have an enhanced effect on coverage (39, 40). Some other studies have shown an increase in community participation in vaccination among mothers and caregivers by virtue of combining other communication methods with the vaccination process especially if it involves development and pilot testing phases (41–43). However, many of these studies have failed to examine the context under which these programs were undertaken. Some of these studies also failed to define the mechanism adopted for the mHealth intervention, hence the need for a scoping study addressing these gaps identified in literature as its results may be of benefit in improving coverage for new emerging diseases such as COVID-19 and other coronaviruses especially in LMIC (44, 45).
This scoping review therefore had the aim of synthesizing evidence on a general level concerning the context, mechanisms, and outcome elements of mHealth interventions in improving vaccination coverage among children under 5 years of age in LMIC.
This study used a scoping review methodology. Using the framework that had been adopted in similar studies, we did the following: (1) identified the research question; (2) identified relevant studies; (3) selected studies; (4) charted the data; (5) collated, summarized, and reported the results (46–50). For the purpose of this review, LMICs were defined in terms of the World Bank classification of countries on the basis of the Gross Domestic product (51). The review is driven by the primary question: What mHealth interventions have been used to improve vaccination coverage in children 0–5 years in LMIC?
The inclusion criteria are identified in relation to the research question with the help of PCC (Population, Concept, and Context) (50). The population of interest is children aged 0–5 years, the concept is the impact of mHealth on vaccination coverage among children 0–5 years, and the context is existence of conventional vaccination schedules in LMIC (Table 1).

Table 1. Inclusion and exclusion criteria.
Medical Subject Headings (MeSH) and non-MeSH terms were used to search selected databases. MeSH tterms used in the search included mHealth, telehealth, mobile Health, eHealth, mobile phone, cellular phone, “cell phone,” “text message,” Africa, Asia, South-East Asia, Sub-Saharan Africa, Far East and Middle East, Latin America, Hispanic and Caribbean Islands, Low- and Middle-Income Countries, LMICs, vaccination, immunization, and inoculation. Pertinent terms were selected after two separate internal discussions and then strung together with Boolean operators ([AND], [OR]). The screening for applicable titles and abstracts was guided by the Joanna Briggs Institute Guidelines (52). Application of inclusion criteria ensured that the content of the included studies was relevant to the aim of the study and the research question. The articles were then assessed for relevance.
The following databases were used in the search: PubMed, Web of Science, ScienceDirect, CINAHL, Embase and Cochrane library. Other sources of information used were University of Eastern Finland library electronic thesis and gray literature online resources. The search was from 1st January 2000 to 31st October 2024. The review was limited to publications in English language only. Details of the search strategy used for each database is outlined in Supplementary Table S1.
Two researchers independently conducted the initial screening of titles and abstracts of articles identified through the search. Reference lists from included studies were used to identify 36 relevant studies which were added to the search. A data extraction was done manually using the following information: the author’s name, year of study, country where the study was conducted, the study design, study population, and outcome of interest. The primary and secondary reviewers used the inclusion criteria to determine eligibility of the studies and subsequently conducted full-text screening of all eligible articles. Articles were selected on a minimum agreement of at least 50% between the two reviewers. The researchers then had agreement meetings to decide on what studies to keep. The reporting of this study process followed the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) (47) (Figure 1). A narrative report was produced to summarize the extracted data. These results were described in relation to the research question and in the context of the overall study purpose.
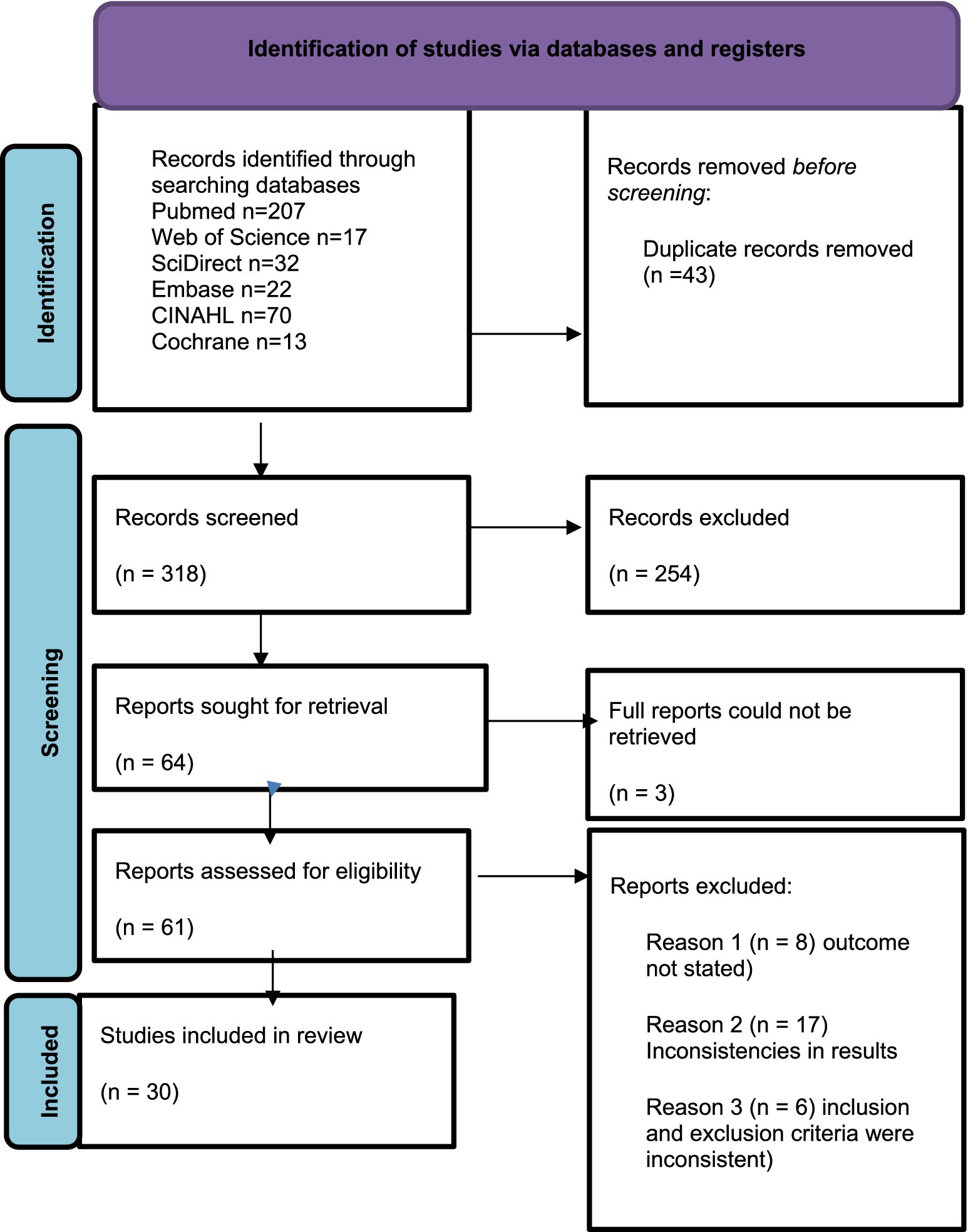
Figure 1. PRISMA flow diagram.
Thirty-one studies were included in the final analysis out of a total of 361 articles initially identified. The most documented mHealth applications in use were one-way text-message and phone reminders to encourage vaccination follow-up appointments (Table 2). There were eight studies from Nigeria, four from Kenya, three from Ethiopia, two from Guatemala, two from Pakistan, while Zimbabwe, Cote D’Ivoire, Tanzania, Philippines, China, India, Burkina Faso and South Africa had one study each reviewed (53–79).
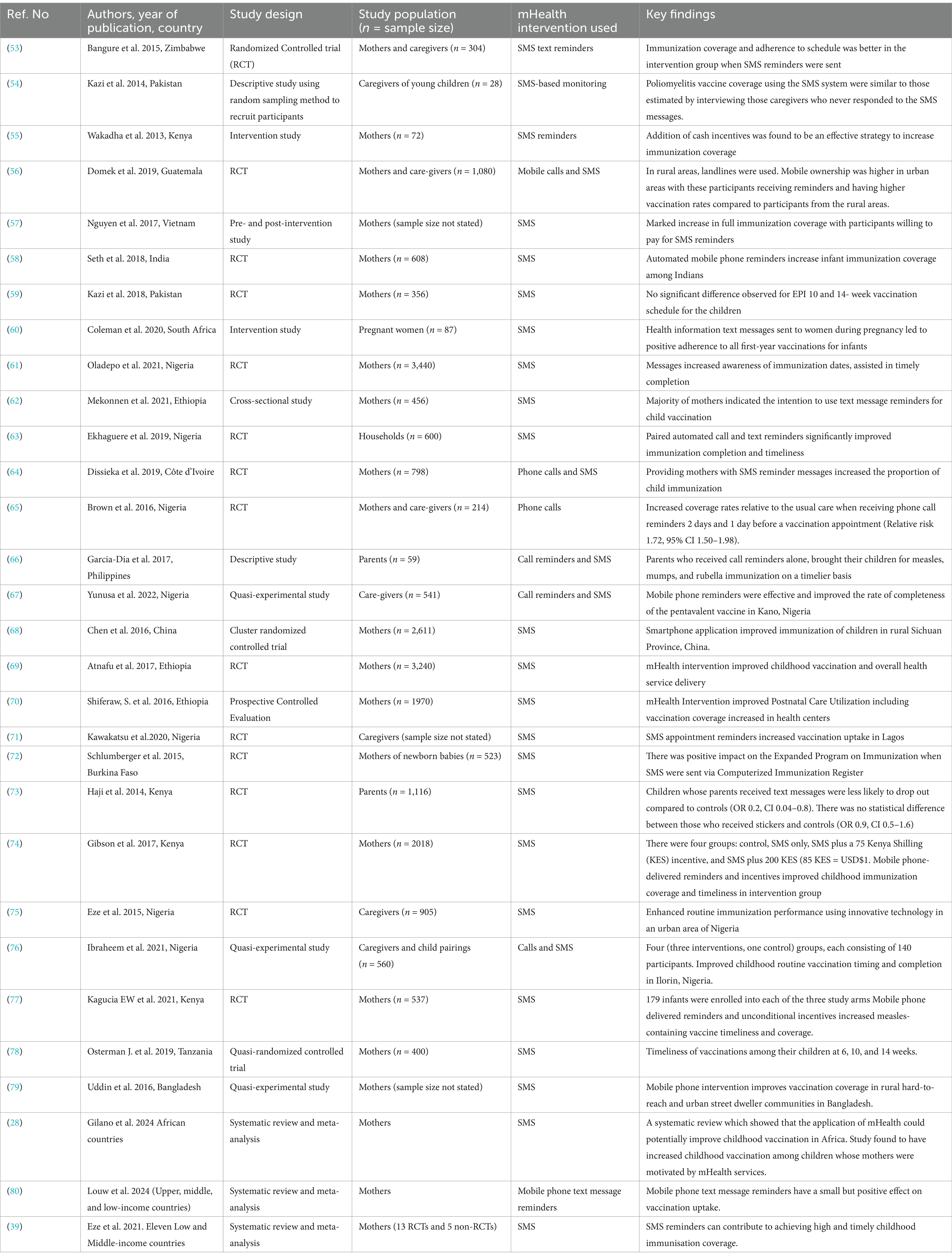
Table 2. Summary of reviewed studies (table order according to intervention method used).
The most commonly used mHealth intervention was SMS without a phone monitoring component which was used to determine the vaccination rate or improve coverage in 19 studies (54, 57–63, 68–74, 76–79). Four studies used a combination of SMS and phone calls to achieve similar objectives among participants (56, 64, 67, 75). In one study, the researchers interviewed caregivers by sending SMS in order to determine the poliomyelitis vaccine coverage by vaccinators during Supplemental Immunization Activities (53). A Nigerian study used only mobile telephone calls to determine the coverage of vaccination among participants (65). Most participants were a combination of mothers and care-givers as observed in 24 studies. Only two studies were designed with both parents as participants (66, 73) and one study focused on households (63). Moreover, results of the effect of mHealth on vaccination outcomes from studies conducted in countries classified by the World Bank as lower middle-income countries (Nigeria, Tanzania, Kenya, Côte d’Ivoire, Philippines, Pakistan) were identical to those obtained from South Africa, Guatemala, China, Vietnam, India which are classified as upper-middle income countries. Furthermore, countries classified as low-income countries such as Zimbabwe, Burkina-Faso and Ethiopia did not have markedly different results despite the variety of study methodology adopted by the researchers.
There were 18 randomized controlled trials (RCT), three quasi-experimental, and three intervention studies. In addition, there were two cross-sectional/descriptive studies and one prospective controlled evaluation study. The total participants in the studies ranged 28 (54) to 3,440 (61). Four studies each were conducted in years 2017 and 2019 while Year 2015, 2016, 2018, and 2021 each contributed three studies.
Most of the RCT studies reported the use of phone calls or SMS reminders to increase vaccination coverage (53–63). Three of these studies (two in Kenya and one in Nigeria) included monetary incentives to increase coverage among participants (58, 65, 72). Twenty-one of the studies were conducted on SMS vaccine reminders in Africa, out of which 18 revealed either an increase in vaccination coverage, decrease in dropout rates, increase in completion rate, or a decrease in delayed vaccination (53–60, 62–79). Six studies focused on SMS reminder systems as an intervention, with no reminder system as the control. However, four studies added other forms of intervention alongside SMS reminders (59–65). A Zimbabwean RCT showed that immunization coverage and adherence to immunization schedule was higher among those in the SMS intervention group in comparison with the control group. SMS reminders were sent to parents (n = 152) when their baby was 6, 10, and 14 weeks old, in addition to routine health education. The control group received health education alone (n = 152). At all three time points, the percentage of children fully vaccinated with the relevant dose of polio, pentavalent, and pneumococcal vaccines was significantly higher in the intervention group compared to the control group (p < 0.001), and the delay in receiving the vaccinations was significantly less in the intervention group compared to the control group (p < 0.001) (59). Another RCT conducted in Nigeria identified increased coverage rates relative to usual care when receiving phone call reminders 2 days and 1 day before a vaccination appointment (relative risk 1.72, 95% CI 1.50–1.98) (67). A similar RCT by Osterman et al. in Tanzania found that SMS reminders increased the odds of vaccination uptake in both urban and rural areas; odds ratio (OR) 2.3 (95% CI 1.1–5.5) and OR 3.6 (95% CI 1.5–8.9), respectively (78). Chen et al. (2016) in another RCT recruited village doctors to assess the effectiveness of a smartphone application on improving vaccination coverage in China with the primary outcome as full vaccination coverage and the secondary outcome as coverage. The study found that smartphone applications improved immunization of the children (68).
Another RCT conducted in year 2017 among 3,242 Ethiopians indicated that SMS interventions resulted in an increase in utilization of maternal health care services with no significant impact on childhood immunization (70). An RCT using 3,440 Nigerian women revealed that messages increased awareness of immunization dates and assisted in timely completion of vaccination (71). In addition, Ekhaguere et al. in another RCT conducted in Nigeria discovered that pairing automated call and text reminders significantly improved immunization completion and timeliness (63). An RCT conducted in Côte d’Ivoire concluded that voice or SMS reminders provided to mothers with SMS reminder messages increased the proportion of child immunizations (75), while a similar one discovered that delivery of automated mobile phone reminders increased infant immunization coverage (78). Kazi et al. in a Pakistani RCT concluded that although SMS interventions were generally observed to be successful, there was not a significant difference observed between 10 and 14 week scheduled visits (59). However, Domek et al. in a RCT conducted in Guatemala found that SMS messages were more beneficial to most women in urban areas because of high mobile phone ownership (56).
Although they were fewer in number, non-RCT studies also indicated favorable vaccination uptake results. Non-RCT studies included cross-sectional and quasi-experimental studies. For example, a random sampling with SMS-based monitoring of child immunization to ask the caregivers whether their children received vaccines concluded that SMS was an effective strategy to monitor coverage following mass immunization (53). Moreover, Nguyen et al. (2017) reported in a pre- and post-intervention using SMS that texts could increase measles immunization rates and that respondents were willing to pay for the messages (57). Furthermore, a cross-sectional study of 456 women in Northwest Ethiopia found that the majority of mothers had the intention to use text message reminders for child vaccination (62). Garcia-Dia et al. in a descriptive study using call reminders in the Philippines found out that parents who received call reminders alone brought their children for measles, mumps, and rubella immunization on a timelier basis (66). Nguyen et al. (2017) had a similar observation in study conducted among Vietnamese mothers in which an increase in full immunization coverage was observed with participants willing to pay for SMS reminders (57). Coleman et al. also observed a similar trend in South Africa despite conducting the intervention among pregnant women. The researchers observed that health information text messages sent to the women during pregnancy led to positive adherence to all first-year vaccinations for infants (60).
Quasi-experimental studies also indicated a similar trend in the results. Yunusa et al. in their study conducted in Kano, Nigeria found out that mobile phone reminders were effective and improved the rate of completeness of the pentavalent vaccine (67). A similar observation was made in Ilorin, also in Nigeria where caregivers and mothers were put in three intervention and, one control groups, each consisting of 140 participants and researchers observed an improved childhood routine vaccination timing and completion (76). An identical observation was made by Uddin et al. (2016) where mobile phone intervention was found to have improved vaccination coverage in rural hard-to-reach and urban street dweller communities in Bangladesh (79).
Three studies involved systematic reviews and meta-analysis conducted in multiple countries in Asia, Africa and the Americas (28, 39, 80). All the studies reported positive changes in the vaccinated coverage and output of vaccination programs in low -and middle-income countries. The lowest effect was recorded in the meta-analysis of randomized controlled trials of caregivers of children, adolescents, or adults. The researchers concluded that Mobile phone text message reminders had a small positive effect which had no bearing on the intervention characteristics, country setting, country economic status, and vaccination type (80). The most prominent effect was found in a systematic review of 13 RCTs and 5 non-RCTs in which pooled estimates showed that SMS reminders significantly improved childhood immunization coverage. In addition, subgroup analysis showed that SMS reminders were effective in increasing childhood immunization coverage in lower middle-income and low-income countries than in upper middle-income countries (p < 0.001) and sending more than two SMS reminders significantly improved timely receipt of childhood vaccines than one or two SMS reminders (39). The individual studies met the criteria used in the systematic reviews to be included, ensuring the review accurately represented the relevant research landscape. In addition, the reviews assessed the quality of each study highlighting discrepancies in quality ratings. All three systematic review studies highlighted consistency or potential differences in comparing the specific outcomes measured in the individual studies to the primary outcomes analyzed in the reviews. Two of the studies involved meta-analysis and another used a risk-bias tool as the statistical method for the analysis. Finally, there was some homogeneity between the results in the systematic reviews studies with individual reviews showing consistent findings and overall conclusions.
The aim of this review was to synthesize evidence concerning the context, mechanisms, and outcome elements of mHealth interventions in improving vaccination coverage among children under 5 years of age in LMIC. The review indicated a generally growing interest by researchers in how mHealth methods could be used to increase vaccination coverage. This is evidenced by a steady increase in number of reviewed articles from 2015 until 2021. This observed interest may be associated with the overall increase in mobile telephone coverage during this time period as reported in previous studies (9–13).
This review included studies conducted in LMIC which have wide socioeconomic inequalities in child vaccination coverage (34, 35). It was impossible to disaggregate data obtained from participants who belonged to the higher socio-economic classes in comparison to those obtained from the lower socio-economic classes in these countries because these categorizations were not available from the reported studies. Therefore, our review was not able to demonstrate a link between mHealth and vaccination either directly or indirectly. Studies with some disaggregation bearing in mind the socio-economic inequalities in LMIC and how it might have affected the vaccination coverage recorded would be helpful for subsequent scoping reviews.
The sample of reviewed studies had more studies from Africa (21) in comparison with four from Asia and two from Latin America and the Caribbean with no studies from Oceania or Europe. The distribution of the studies in this review was not directly proportional to the numerical distribution of LMIC according to the World Bank with 54 countries in Africa, 34 in Asia, 24 in Latin America and the Caribbean, 11 in Europe, and 8 countries in Oceania (51). This observation may be as due to the increased interest of researchers in working on the subject in African countries because of the general perception of poorer health outcomes on the continent.
Another interesting point for consideration is the possibility for interventions with mixed information delivery modes to have an enhanced effect. This trend has been seen in previous studies (39, 40). In this review, interventions that combined texting and phone calls all reported improved results which agrees with the possibility of an enhanced effect proposed by previous studies (39, 40). In addition, although little was reported about the processes of development of the mHealth messages, there is potential to increase community participation and overall interest in vaccination among mothers and care-givers during the development process especially if it involves development and pilot testing phases (41–43). The small sample sizes of some of the studies and the inclusion criteria of ownership and use of mobile phones by many of them may have introduced a sampling bias in these studies and would have to be considered when adopting these mHealth methods on a population scale (53, 55, 66).
Furthermore, the quality of the studies in this review ranged from RCT to quasi-experimental, and intervention studies as well as cross-sectional/descriptive studies. The quality of these studies and the rigor in their methodologies had some impact on the conclusions by the authors. Although the conclusion of a positive effect of mHealth interventions on vaccination outcomes were made by both RCT and non-RCT studies, the RCT studies had more assertive conclusions.
Overall, SMS reminders for vaccination appointments were found to increase vaccination uptake and reduce delays in receiving vaccinations with a direct association in all but two of the studies. In certain instances, monetary incentives proved beneficial as mothers who received an incentive reported mostly positive experiences with receiving SMS reminders about vaccination appointments (64, 65).However, in contrast, a study from Pakistan found no significant difference in the response rates to SMS messages about vaccinations, even when a financial inducement was introduced (59).
We observed that education and behavioral change because of mHealth interventions was the most represented domain, to which 21 of the reviewed papers related (56–73). Mobile technology makes it easier to contact individuals and offers a useful tool to deliver education and improve health-seeking behavior or health-related lifestyle decisions. However, there was no qualitative study in the review to explore other factors that may have been responsible for any observed change.
Although the review was not conducted to compare external factors related to success of vaccination programs, our findings indicated some level of success irrespective of economic status and the study setting. The impact of this study is that it could inform policymakers and practitioners in LMIC that adopting the use of mHealth may be a low hanging fruit in improving vaccination coverage in their countries.
One of the major strengths of this study was our search strategy, which had a wide timeframe, included 5 databases, and involved a variety of countries, populations, and study designs. However, our search did not include all databases and was restricted to studies conducted between 1st January 2000 and 31st October 2024. Although this search period was adopted because of reports of an increase in mobile phone use based on previous studies (9–13), we concede that it may have resulted in exclusion of some important studies. Moreover, our selection criteria included only studies which were published in the English language. This might have resulted in absence of potentially relevant studies conducted in other languages such as French and Spanish which are widely spoken in LMIC. During the review, a total of 254 studies were excluded which is an indication for greater refining of search strategies in future reviews. Furthermore, given the regular changes to vaccination data, our findings may not be generalizable a few years down the line.
This scoping review identified and described several studies used to demonstrate a relationship between mHealth and vaccination coverage outcomes. The review shows that mHealth technologies in combination with other interventions have been used to increase vaccination uptake in LMIC. The review also identified that the results of most studies broadly suggest an improved uptake of vaccinations with mHealth especially mobile phone–based interventions. However, there is a need for further research to adequately quantify the impact of these interventions and determine the most effective strategies to increase vaccination outcomes.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author/s.
OO: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing. OYO: Data curation, Investigation, Methodology, Software, Writing – original draft, Writing – review & editing. U-MK: Conceptualization, Formal analysis, Methodology, Supervision, Writing – original draft, Writing – review & editing. KS: Conceptualization, Methodology, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The study was conducted with funding from the authors. There were no external funding sources.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2025.1392709/full#supplementary-material
1. Abreu, FDL, Bissaco, MAS, Silva, AP, Boschi, SRMS, Scardovelli, TA, Santos, M, et al. The use and impact of mHealth by community health workers in developing and least developed countries: a systematic review. Res Biomed Eng. (2021) 37:563–82. doi: 10.1007/s42600-021-00154-3
2. Bastawrous, A, and Armstrong, MJ. Mobile health use in low- and high-income countries: an overview of the peer-reviewed literature. J R Soc Med. (2013) 106:130–42. doi: 10.1177/0141076812472620
3. Meyer, AJ, Babirye, D, Armstrong-Hough, M, Mark, D, Ayakaka, I, Katamba, A, et al. Text messages sent to household tuberculosis contacts in Kampala, Uganda: process evaluation. JMIR Mhealth Uhealth. (2018) 6:e10239. doi: 10.2196/10239
4. Ringi, T, Dobson, R, Herman, J, Taire, M, Nosa, V, Whitaker, R, et al. Takore i te Kai Ava'ava (quit smoking), a mCessation program adapted for the Cook Islands: indicators of potential for tobacco control. Asia Pac J Public Health. (2021) 33:714–20. doi: 10.1177/10105395211036267
5. Piette, JD, List, J, Rana, GK, Townsend, W, Striplin, D, and Heisler, M. Mobile health devices as tools for worldwide cardiovascular risk reduction and disease management. Circulation. (2015) 132:2012–27. doi: 10.1161/CIRCULATIONAHA.114.008723
6. World Health Organization. mHealth: New horizons for health through mobile technologies. Geneva, Switzerland: World Health Organization (2011).
7. International Telecommunications Union. The World in 2010: ICT facts and figures. Geneva, International Telecommunications Union (2010). Available at: http://www.itu.int/ITU-D/ict/material/FactsFigures2010.pdf (Accessed May 13, 2022).
8. Statistica. Forecast number of mobile users worldwide from 2020 to 2025. Available at: https://www.statista.com/statistics/218984/number-of-global-mobile-users-since-2010/ (Accessed October 14, 2022).
9. Odea, SS. (2020). Global unique mobile subscribers from 2010–2025, by region (millions). Available at: https://www.statista.com/statistics/740154/worldwide-unique-mobile-subscribers-by-region/ (Accessed February 27, 2022).
10. Sam, S. Towards an empowerment framework for evaluating mobile phone use and impact in developing countries. Telematics Inform. (2017) 34:359–69. doi: 10.1016/j.tele.2016.06.003
11. Betjeman, TJ, Soghoian, SE, and Foran, MP. mHealth in sub-Saharan Africa. Int J Telemed Appl. (2013) 2013:482324:1–7. doi: 10.1155/2013/482324
12. Burki, T. Developing countries in the digital revolution. Lancet. (2018) 391:417. doi: 10.1016/S0140-6736(18)30191-0
13. Silver, L. Digital connectivity growing rapidly in emerging economies. Available at: https://www.pewresearch.org/global/2019/02/05/digital-connectivity-growing-rapidly-in-emerging-economies/ (Accessed June 24, 2023).
14. Anderson-Lewis, C, Darville, G, Mercado, RE, Howell, S, and Di Maggio, S. mHealth technology use and implications in historically underserved and minority populations in the United States: systematic literature review. JMIR Mhealth Uhealth. (2018) 6:e128. doi: 10.2196/mhealth.8383
15. Linde, DS, Korsholm, M, Katanga, J, Rasch, V, Lundh, A, and Andersen, MS. One-way SMS and healthcare outcomes in Africa: systematic review of randomised trials with meta-analysis. PLoS One. (2019) 14:e0217485. doi: 10.1371/journal.pone.0217485
16. WHO. World health statistics 2017: Monitoring health for the SDGs. Sustainable development goals. Geneva: WHO (2017).
17. Gessner, BD, Kaslow, D, Louis, J, Neuzil, K, O’Brien, KL, Picot, V, et al. Estimating the full public health value of vaccination. Vaccine. (2017) 35:6255–63. doi: 10.1016/j.vaccine.2017.09.048
18. Gouglas, D, Thanh, T, Henderson, K, Kaloudis, A, Danielsen, T, Hammersland, N, et al. Estimating the cost of vaccine development against epidemic infectious diseases: a cost minimisation study. Lancet Glob Health. (2018) 6:e1386–96. doi: 10.1016/S2214-109X(18)30346-2
19. Manzoli, L, Schioppa, F, Boccia, A, and Villari, P. The efficacy of influenza vaccine for healthy children: a meta-analysis evaluating potential sources of variation in efficacy estimates including study quality. Pediatr Infect Dis J. (2007) 26:97–106. doi: 10.1097/01.inf.0000253053.01151.bd
20. Marchant, A, Sadarangani, M, Garand, M, Dauby, N, Verhasselt, V, Pereira, L, et al. Maternal immunization: collaborating with mother nature. Lancet Infect Dis. (2017) 17:e197–208. doi: 10.1016/S1473-3099(17)30229-3
21. Mina, MJ, Kula, T, Leng, Y, Li, M, de Vries, RD, Knip, M, et al. Measles virus infection diminishes preexisting antibodies that offer protection from other pathogens. Science. (2019) 366:599–606. doi: 10.1126/science.aay6485
22. Mina, MJ, Metcalf, CJ, de Swart, RL, Osterhaus, AD, and Grenfell, BT. Long-term measles-induced immunomodulation increases overall childhood infectious disease mortality. Science. (2015) 348:694–9. doi: 10.1126/science.aaa3662
23. Mbonigaba, E, Nderu, D, Chen, S, Denkinger, C, Gelseltzer, P, McHahon, S, et al. Childhood vaccine uptake in Africa: threats, challenges, and opportunities. J Glob Health Rep. (2021) 5:e2021080. doi: 10.29392/001c.26312
24. Kazungu, JS, and Adetifa, IMO. Crude childhood vaccination coverage in West Africa: trends and predictors of completeness. Wellcome Open Res. (2017) 2:12. doi: 10.12688/wellcomeopenres.10690.1
25. Li, AJ, Tabu, C, Shendale, S, Okoth, PO, Sergon, K, Maree, E, et al. Qualitative insights into reasons for missed opportunities for vaccination in Kenyan health facilities. PLoS One. (2020) 15:e0230783. doi: 10.1371/journal.pone.0230783
26. Abdullahi, MF, Stewart Williams, J, Sahlèn, KG, Bile, K, and Kinsman, J. Factors contributing to the uptake of childhood vaccination in Galkayo District, Puntland, Somalia. Glob Health Action. (2020) 13:543. doi: 10.1080/16549716.2020.1803543
27. Adedokun, ST, Uthman, OA, Adekanmbi, VT, and Wiysonge, CS. Incomplete childhood immunization in Nigeria: a multilevel analysis of individual and contextual factors. BMC Public Health. (2017) 17:236. doi: 10.1186/s12889-017-4137-7
28. Gilano, G, Sako, S, Molla, B, Dekker, A, and Fijten, R. The effect of mHealth on childhood vaccination in Africa: a systematic review and meta-analysis. PLoS One. (2024) 19:e0294442. doi: 10.1371/journal.pone.0294442
29. Gibson, DG, Kagucia, EW, Ochieng, B, Hariharan, N, Obor, D, Moulton, LH, et al. The mobile solutions for immunization (M-SIMU) trial: a protocol for a cluster randomized controlled trial that assesses the impact of mobile phone delivered reminders and travel subsidies to improve childhood immunization coverage rates and timeliness in western Kenya. JMIR Res Protoc. (2016) 5:e72. doi: 10.2196/resprot.5030
30. Mekonnen, ZA, Gelaye, KA, Were, MC, Gashu, KD, and Tilahun, BC. Effect of mobile text message reminders on routine childhood vaccination: a systematic review and meta-analysis. Syst Rev. (2019) 8:154. doi: 10.1186/s13643-019-1054-0
31. Rahman, MO, Yamaji, N, Nagamatsu, Y, and Ota, E. Effects of mHealth interventions on improving antenatal care visits and skilled delivery Care in low- and Middle-Income Countries: systematic review and Meta-analysis. J Med Internet Res. (2022) 24:e34061. doi: 10.2196/34061
32. Gibson, DG, Kagucia, EW, Were, J, Obor, D, Hayford, K, and Ochieng, B. Text message reminders and unconditional monetary incentives to improve measles vaccination in western Kenya: study protocol for the mobile and scalable innovations for measles immunization randomized controlled trial. JMIR Res Protoc. (2019) 8:e13221. doi: 10.2196/13221
33. Schwebel, FJ, and Larimer, ME. Using text message reminders in health care services: a narrative literature review. Internet Interv. (2018) 13:82–104. doi: 10.1016/j.invent.2018.06.002
34. Saxenian, H, Hecht, R, Kaddar, M, Schmitt, S, Ryckman, T, and Cornejo, S. Overcoming challenges to sustainable immunization financing: early experiences from GAVI graduating countries. Health Policy Plan. (2015) 30:197–205. doi: 10.1093/heapol/czu003
35. Hajizadeh, M. Socioeconomic inequalities in child vaccination in low/middle-income countries: what accounts for the differences? J Epidemiol Community Health. (2018) 72:719–25. doi: 10.1136/jech-2017-210296
36. Restrepo-Méndez, MC, Barros, AJD, Wong, KLM, Johnson, HL, Pariyo, G, França, GV, et al. Inequalities in full immunization coverage: trends in low- and middle-income countries. Bull World Health Organ. (2016) 94:794–805A. doi: 10.2471/BLT.15.162172
37. Oliver-Williams, C, Brown, E, Devereux, S, Fairhead, C, and Holeman, I. Using Mobile phones to improve vaccination uptake in 21 low- and middle-income countries: systematic review. JMIR Mhealth Uhealth. (2017) 5:e148. doi: 10.2196/mhealth.7792
38. Ilozumba, O, Schmidt, P, Ket, JCF, and Jaspers, M. Can mHealth interventions contribute to increased HPV vaccination uptake? A systematic review. Prev Med Rep. (2020) 28:101289. doi: 10.1016/j.pmedr.2020.101289
39. Eze, P, Lawani, LO, and Acharya, Y. Short message service (SMS) reminders for childhood immunisation in low-income and middle-income countries: a systematic review and meta-analysis. BMJ Glob Health. (2021) 6:e005035. doi: 10.1136/bmjgh-2021-005035
40. Jacobson Vann, JC, Jacobson, RM, Coyne-Beasley, T, Asafu-Adjei, JK, and Szilagyi, PG. Patient reminder and recall interventions to improve immunization rates. Cochrane Database Syst Rev. (2018) 1:CD003941. doi: 10.1002/14651858.CD003941.pub3
41. Goldman, RD, Yan, TD, Seiler, M, Parra Cotanda, C, Brown, JC, Klein, EJ, et al. Caregiver willingness to vaccinate their children against COVID-19: cross sectional survey. Vaccine. (2020) 38:7668–73. doi: 10.1016/j.vaccine.2020.09.084
42. Pramanik, S, Ghosh, A, Nanda, RB, De Rouw, M, Forth, P, and Albert, S. Impact evaluation of a community engagement intervention in improving childhood immunization coverage: a cluster randomized controlled trial in Assam, India. BMC Public Health. (2018) 18:1–3. doi: 10.1186/s12889-018-5458-x
43. Goldstein, S, MacDonald, NE, and Guirguis, S. Health communication and vaccine hesitancy. Vaccine. (2015) 143:4212–4. doi: 10.1016/j.vaccine.2015.04.042
44. McCulloh, RJ, Darden, PM, Snowden, J, Ounpraseuth, S, Lee, J, Clarke, M, et al. Improving pediatric COVID-19 vaccine uptake using an mHealth tool (MoVeUp): study protocol for a randomized, controlled trial. Trials. (2022) 23:911. doi: 10.1186/s13063-022-06819-3
45. Elsebaie, EH, Fathy, MA, Khalifa, AK, El-Deen, M, Alnagdy, M, Elsaidi, M, et al. How can mobile health technology improve usage and delivery of the covid-19 vaccine in low-and middle-income countries? Open Access Maced J Med Sci. (2022) 10:437–43. doi: 10.3889/oamjms.2022.8323
46. Grimshaw, J. A guide to knowledge synthesis: a knowledge synthesis chapter. Available at: https://cihr-irsc.gc.ca/e/41382.html (Accessed March 27, 2022).
47. Tricco, AC, Lillie, E, Zarin, W, O'Brien, KK, Colquhoun, H, Levac, D, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. (2018) 169:467–73. doi: 10.7326/M18-0850
48. Arksey, H, and O’Malley, L. Scoping studies: towards a methodological framework. Int J Soc Res Method. (2005) 8:19–32. doi: 10.1080/1364557032000119616
49. Peters, MD, Godfrey, CM, Khalil, H, McInerney, P, Parker, D, and Soares, CB. Guidance for conducting systematic scoping reviews. Int J Evid Based Healthc. (2015) 13:141–6. doi: 10.1097/XEB.0000000000000050
50. Peters, MD, Marnie, C, Tricco, AC, Pollock, D, Munn, Z, Alexander, L, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. (2020) 18:2119–26. doi: 10.11124/JBIES-20-00167
51. World Bank. World Bank Country and Lending Groups, Country Classification. Available at: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (Accessed March 29, 2021).
52. Aromataris, E, and Munn, Z. JBI manual for evidence synthesis. JBI (2020). Available at: https://synthesismanual.jbi.global. (Accessed 24 December 24).
53. Bangure, D, Chirundu, D, Gombe, N, Marufu, T, Mandozana, G, Tshimanga, M, et al. Effectiveness of short message services reminder on childhood immunization programme in Kadoma, Zimbabwe - a randomized controlled trial, 2013. BMC Public Health. (2015) 15:137. doi: 10.1186/s12889-015-1470-6
54. Kazi, AM, Murtaza, A, Khoja, S, Zaidi, AK, and Ali, SA. Monitoring polio supplementary immunization activities using an automated short text messaging system in Karachi. Pak Bull World Health Organ. (2014) 92:220–5. doi: 10.2471/BLT.13.122564
55. Wakadha, H, Chandir, S, Were, EV, Rubin, A, Obor, D, Levine, OS, et al. The feasibility of using mobile phone-based SMS reminders and conditional cash transfers to improve timely immunization in rural Kenya. Vaccine. (2013) 31:987–93. doi: 10.1016/j.vaccine.2012.11.093
56. Domek, GJ, Contreras-Roldan, IL, O'Leary, ST, Bull, S, Furniss, A, Kempe, A, et al. SMS text message reminders to improve infant vaccination coverage in Guatemala: a pilot randomized controlled trial. Vaccine. (2016) 34:2437–43. doi: 10.1016/j.vaccine.2016.03.065
57. Nguyen, NT, Vu, MH, Dao, SD, Tran, HT, and Nguyen, TXC. Digital immunization registry: evidence for the impact of mHealth on enhancing the immunization system and improving immunization coverage for children under one year old in Vietnam. Mhealth. (2017) 3:26. doi: 10.21037/mhealth.2017.06.03
58. Seth, R, Akinboyo, I, Chhabra, A, Qaiyum, Y, Shet, A, Gupte, N, et al. Mobile phone incentives for childhood immunizations in rural India. Pediatrics. (2018) 141:e20173455. doi: 10.1542/peds.2017-3455
59. Kazi, AM, Ali, M, Zubair, K, Kalimuddin, H, Kazi, AN, Iqbal, SP, et al. Effect of Mobile phone text message reminders on routine immunization uptake in Pakistan: randomized controlled trial. JMIR Public Health Surveill. (2018) 4:e20. doi: 10.2196/publichealth.7026
60. Coleman, J, Black, V, Thorson, AE, and Eriksen, J. Evaluating the effect of maternal mHealth text messages on uptake of maternal and child health care services in South Africa: a multicentre cohort intervention study. Reprod Health. (2020) 17:160. doi: 10.1186/s12978-020-01017-3
61. Oladepo, O, Dipeolu, IO, and Oladunni, O. Outcome of reminder text messages intervention on completion of routine immunization in rural areas. Niger Health Promot Int. (2021) 36:765–73. doi: 10.1093/heapro/daaa092
62. Mekonnen, ZA, Gelaye, KA, Were, MC, and Tilahun, B. Acceptability, barriers and facilitators of mobile text message reminder system implementation in improving child vaccination: a qualitative study in Northwest Ethiopia. J Multidiscip Healthc. (2021) 14:605–16. doi: 10.2147/JMDH.S298167
63. Ekhaguere, OA, Oluwafemi, RO, Badejoko, B, Oyeneyin, LO, Butali, A, Lowenthal, ED, et al. Automated phone call and text reminders for childhood immunisations (PRIMM): a randomised controlled trial in Nigeria. BMJ Glob Health. (2019) 4:e001232. doi: 10.1136/bmjgh-2018-001232
64. Dissieka, R, Soohoo, M, Janmohamed, A, and Doledec, D. Providing mothers with mobile phone message reminders increases childhood immunization and vitamin a supplementation coverage in Côte d'Ivoire: a randomized controlled trial. J Public Health Afr. (2019) 10:1032. doi: 10.4081/jphia.2019.1032
65. Brown, VB, Oluwatosin, OA, Akinyemi, JO, and Adeyemo, AA. Effects of community health nurse-led intervention on childhood routine immunization completion in primary health care centers in Ibadan. Nigeria J Community Health. (2016) 41:265–73. doi: 10.1007/s10900-015-0092-3
66. Garcia-Dia, MJ, Fitzpatrick, JJ, Madigan, EA, and Peabody, JW. Using text reminder to improve childhood immunization adherence in the Philippines. Comput Inform Nurs. (2017) 35:212–8. doi: 10.1097/CIN.0000000000000307
67. Yunusa, U, Ibrahim, AH, Ladan, MA, and Gomaa, HEM. Effect of mobile phone text message and call reminders in the completeness of pentavalent vaccines in Kano state, Nigeria. J Pediatr Nurs. (2022) 6:e77–83. doi: 10.1016/j.pedn.2021.12.026
68. Chen, L, Du, X, Zhang, L, van Velthoven, MH, Wu, Q, Yang, R, et al. Effectiveness of a smartphone app on improving immunization of children in rural Sichuan Province, China: a cluster randomized controlled trial. BMC Public Health. (2016) 16:909. doi: 10.1186/s12889-016-3549-0
69. Atnafu, A, Otto, K, and Herbst, CH. The role of mHealth intervention on maternal and child health service delivery: findings from a randomized controlled field trial in rural Ethiopia. Mhealth. (2017) 3:39. doi: 10.21037/mhealth.2017.08.04
70. Shiferaw, S, Spigt, M, Tekie, M, Abdullah, M, Fantahun, M, and Dinant, GJ. The effects of a locally developed mhealth intervention on delivery and postnatal care utilization; a prospective controlled evaluation among health centres in Ethiopia. PLoS One. (2016) 11:e0158600. doi: 10.1371/journal.pone.0158600
71. Kawakatsu, Y, Oyeniyi Adesina, A, Kadoi, N, and Aiga, H. Cost-effectiveness of SMS appointment reminders in increasing vaccination uptake in Lagos, Nigeria: a multi-centered randomized controlled trial. Vaccine. (2020) 38:6600-6608. doi: 10.1016/j.vaccine.2020.07.075
72. Schlumberger, M, Bamoko, A, Yameoogo, TM, Rouvet, F, Ouedraogo, R, Traoré, B, et al. Positive impact on the expanded program on immunization when sending call-back sms through a computerized immunization register, Bobo Dioulasso (Burkina Faso). Bull Soc Pathol Exot. (2015) 108:349–54. doi: 10.1007/s13149-015-0455-4
73. Haji, A, Lowther, S, Ngan’ga, Z, Gura, Z, Tabu, C, Sandhu, H, et al. Reducing routine vaccination dropout rates: evaluating two interventions in three Kenyan districts, 2014. BMC Public Health. (2016) 16:152. doi: 10.1186/s12889-016-2823-5
74. Gibson, DG, Ochieng, B, Kagucia, EW, Were, J, Hayford, K, Moulton, LH, et al. Mobile phone-delivered reminders and incentives to improve childhood immunization coverage and timeliness in Kenya (M-SIMU): a cluster randomised controlled trial. Lancet Glob Health. (2017) 5:e428–38. doi: 10.1016/S2214-109X(17)30072-4
75. Eze, G, and Adeleye, O. Enhancing routine immunization performance using innovative technology in an urban area of Nigeria. West Afr J Med. (2015) 34:3–10.
76. Ibraheem, R, Akintola, M, Abdulkadir, M, Ameen, H, Bolarinwa, O, and Adeboye, M. Effects of call reminders, short message services (sms) reminders, and sms immunization facts on childhood routine vaccination timing and completion in Ilorin. Niger Afr Health Sci. (2021) 21:951–9. doi: 10.4314/ahs.v21i2.57
77. Kagucia, EW, Ochieng, B, Were, J, Hayford, K, Obor, D, O'Brien, KL, et al. Impact of mobile phone delivered reminders and unconditional incentives on measles-containing vaccine timeliness and coverage: a randomised controlled trial in western Kenya. BMJ Glob Health. (2021) 6:e003357. doi: 10.1136/bmjgh-2020-003357
78. Ostermann, J, Vasudevan, L, Baumgartner, JN, Ngadaya, E, and Mfinanga, SG. Do mobile phone-based reminders and conditional financial transfers improve the timeliness of childhood vaccinations in Tanzania? Study protocol for a quasi-randomized controlled trial. Trials. (2019) 20:397. doi: 10.1186/s13063-019-3430-4
79. Uddin, MJ, Shamsuzzaman, M, Horng, L, Labrique, A, Vasudevan, L, Zeller, K, et al. Use of mobile phones for improving vaccination coverage among children living in rural hard-to-reach areas and urban streets of Bangladesh. Vaccine. (2016) 34:276–83. doi: 10.1016/j.vaccine.2015.11.024
Keywords: Low- and Middle-Income countries, mHealth, scoping review, vaccination, under five, children
Citation: Onigbogi O, Ojo OY, Kinnunen U-M and Saranto K (2025) Mobile health interventions on vaccination coverage among children under 5 years of age in Low and Middle-Income countries; a scoping review. Front. Public Health. 13:1392709. doi: 10.3389/fpubh.2025.1392709
Edited by:
Md Shafiur Rahman, Kanagawa University of Human Services, JapanReviewed by:
Md Rashedul Islam, Hitotsubashi University, JapanCopyright © 2025 Onigbogi, Ojo, Kinnunen and Saranto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Olanrewaju Onigbogi, bGFucmVvbmlnYm9naUB5YWhvby5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.