 Haojun Zhang
Haojun Zhang Yunqiu Zhan
Yunqiu Zhan Keqiu Chen
Keqiu Chen
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 15 January 2025
Sec. Health Economics
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1517716
Introduction: Education (EDU) enhances life expectancy (LEF) by improving health literacy and access to healthcare, leading to healthier lifestyles. Urbanization (URB) fosters better healthcare infrastructure and access to essential services, although it must be managed to avoid negative environmental impacts. Green growth (GG) ensures sustainable development, reduces pollution and environmental risks, and contributes to longer, healthier lives. Therefore, this study examines the impact of EDU, URB and GG on LEF in China from 1990 to 2022.
Methods: This study utilizes the unit root, cointegration test, and Auto Regressive distributed lag (ARDL) model, and for robustness analysis, we use the Fully modified ordinary least squares (FMOLS) and Dynamic ordinary least squares (FMOLS) methods.
Results: The results show that education, urbanization and green growth have a positive and significant effect on life expectancy, while C02 emissions negatively affect life expectancy.
Discussion: These findings suggest that more resources should be allocated to public education systems to ensure access to quality education from early childhood through higher education and integrate comprehensive health education into school curricula to raise awareness about healthy lifestyles, nutrition, and disease prevention. Promote intelligent urban planning incorporating green spaces, recreational areas, and safe walkways to encourage physical activity and reduce pollution. The findings significantly contribute to health economics and provide a new avenue of research for the academic community and policymakers.
Health is primarily addressed under SDG 3, which aims to ensure healthy lives and promote well-being for all ages. This goal focuses on reducing maternal and child mortality, combating diseases, and improving healthcare access. Health also supports other SDGs like poverty eradication and quality education by fostering more productive populations. Individuals worldwide require better health facilities, and countries strive to provide their citizens with better health and health-related amenities (1). An essential measure of a country’s health is life expectancy (LEF), which is impacted by social, economic, and environmental factors. Technology, literacy, water, and medical facilities are some of the variables that contribute to the global trend of rising life expectancy (2). The life expectancy at birth estimates how many years a newborn infant would live if the mortality rates at the time of the baby’s birth stayed constant throughout its life (3). Although wealthy countries have improved life expectancy to the desired level, developing countries need help to achieve a fair life expectancy (2). The better modern health system has played a crucial role in the global drop in mortality. However, access to the contemporary health system may differ between rich and poor people (4). Regardless of the state of the economy, all public health systems require consistent financing to maintain essential services such as immunization and screening. In the face of financial constraints, there is also a danger of foregoing cheap preventative care (5, 6). Figure 1 shows the life expectancy trends in China from 1990 to 2022. In 1990, the LEF was approximately 68 years old; it crossed 70 years around 1995, and the milestone of 75 years was reached by 2010. By 2020, it surpassed 78 years, indicating a significant enhancement in public health measures and living conditions. 2020 to 2022 show a gradual increase, with life expectancy rising from 78.072020 to 78.58 in 2022. This reflects ongoing improvements in healthcare and possibly responses to public health challenges. The life expectancy in China has generally increased over the years, rising from 68.005 years in 1990 to 78.58 years in 2022. Over the decades, this indicates improved health, living standards, and medical care.
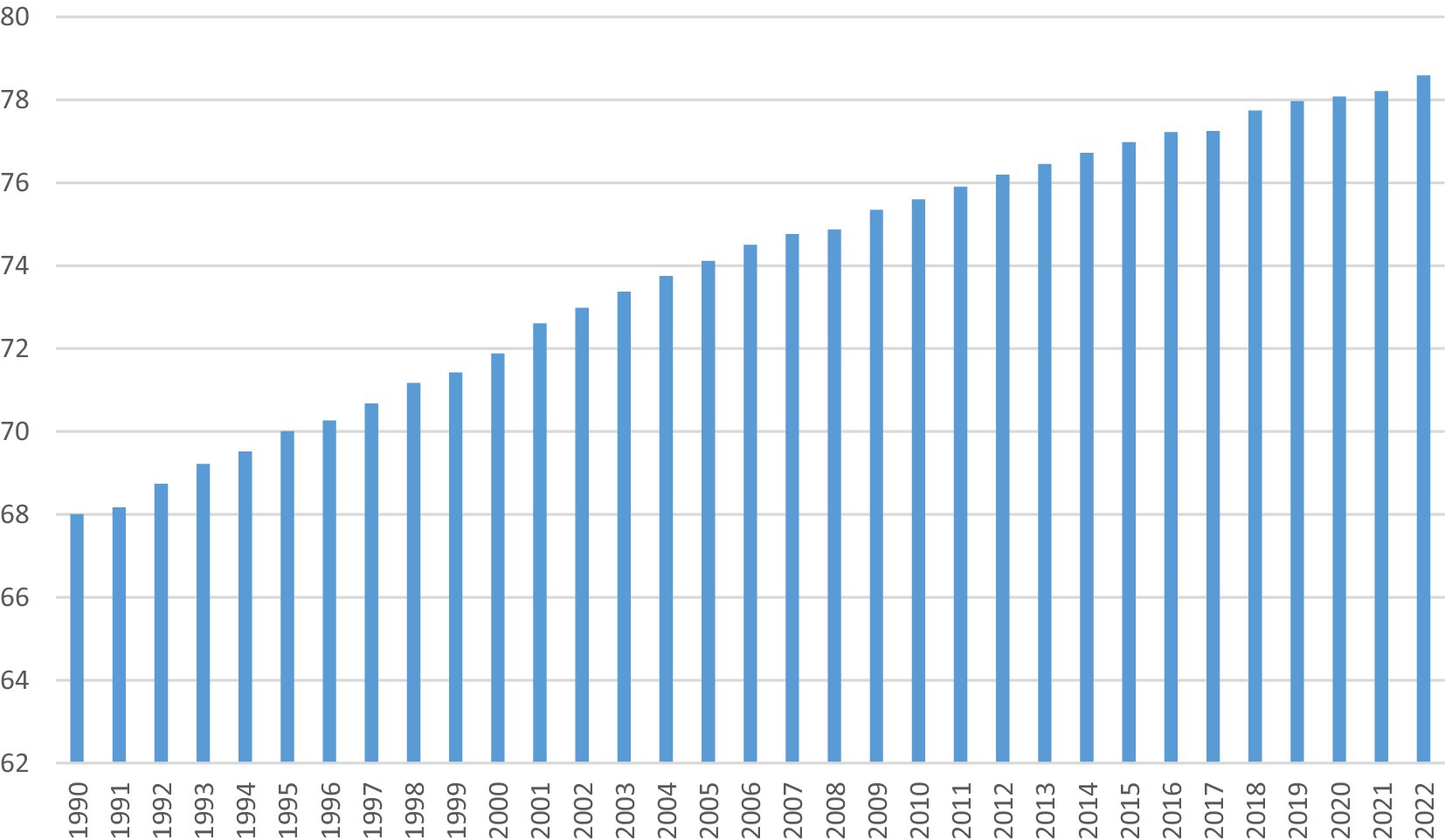
Figure 1. Trends of life expectancy at birth rate in China. Source: WDI.
Educational attainment is a crucial Social determinant of health and a valuable indicator of socioeconomic status (7). The link between increasing education and improved health is well recognized (8, 9). Many studies have found a strong link between education and health outcomes such as life expectancy, healthy aging, cancer, and exposure to risk factors like obesity, substance abuse, and lifestyle factors (10–12). Education directly impacts preventative health by raising awareness of regular health testing, enhancing self-efficacy and confidence, and improving access to health services through increased patience and motivation (13). According to Liu et al. (14) reported that individuals with a greater level of education report better health, maintain a healthier weight, and are less likely to smoke or drink excessively. Parental education has a vital role in reducing child mortality rates; it has been demonstrated that every year of maternal education lowers the risk of under-5 mortality by 3·0%, and every year of paternal education lowers the risk by 1·6% (15, 16). On the contrary, lower education has been linked to increased mortality from all causes, including cardiovascular illnesses, neoplasms, and external causes (17, 18). Several research has linked lower educational attainment or less than high school education to increased all-cause and cardiovascular mortality (7, 19). Health literacy (HL) is one of the most important factors in determining health. Nowadays, HL is a multifaceted idea with a public health viewpoint that characterizes how well people can access, process, and comprehend the fundamental health information they need to make informed decisions about their health (20). Inadequate HL might be a contributing factor to cancer screening inequities and could explain why people are unaware of the significance of getting cancer screening tests (21). Individuals with low HL are more likely to underutilize preventative treatment, increase medical costs by needless hospital stays, and have lower rates of early screenings for diseases like cancer that can be detected early. As a result, these factors increase morbidity and death (22).
Urbanization (URB) refers to human-made settlements with buildings, roads, and infrastructure frequently associated with economic development and improved health due to increased sanitation, education, job opportunities, and access to infrastructure and healthcare facilities. Cities provide more ecological and cultural services, like parks, gardens, and playgrounds. Additionally, sports stadiums and amenities help alleviate stress and promote health (23, 24). Urbanization has increased life expectancy, as city inhabitants earn more and spend more money on their health. The rapid economic advancement and rising urbanization have also expanded access to contemporary, high-tech medical treatment (4). Urbanization has an impact on life expectancy, both positively and negatively. While it frequently leads to increased access to healthcare, education, and higher living standards, unplanned urbanization can also result in environmental degradation, inadequate healthcare infrastructure, and increased exposure to lifestyle-related health risks, potentially lowering life expectancy (2, 25). The rapid and unstructured urbanization process of the 21st century substantially impacts natural and constructed infrastructures, environmental health, and human well-being, emphasizing the role of social dynamics in constructing human society (26–28). Asia and Africa host the world’s largest and fastest-expanding cities. As a result, city living is and will remain the norm for current and future generations globally, with enormous implications for human society, culture, and health (29, 30).
Since environmental deterioration and climate change (CC) have been considered, green development has drawn much attention. Several institutions are taking the green economy seriously, such as the United Nations Economic and Social Commission for Asia and the Pacific (UNESCAP), the World Bank, and the Organization for Economic Cooperation and Development (OECD). The Intergovernmental Panel on Climate Change has given it priority, which is the cause of the ongoing increase in global temperature and its corresponding impact on the globe (31, 32). The Paris Agreement and the 2030 Sustainable Development Agenda have revitalized efforts to improve the environment in order to solve the problems caused by climate change (33). This implies that all developed or developing nations should adhere to Agenda 2030 for Sustainable Development. The nations that prioritize ecologically friendly economic growth differ significantly from one another. Nonetheless, nations with large GDPs are dedicated to preserving the environment. While green growth stagnates or drops in lower-income nations, it significantly increases in high-GDP ones. Consequently, an increase in ongoing economic activity suggests that complex environmental problems cannot be resolved by all available means (34). Green growth (GG) can increase LEF by promoting sustainable practices that reduce environmental risks. Cleaner air and water, resulting from lower emissions and pollution, can improve public health outcomes. Energy-efficient technologies and green industries reduce exposure to harmful chemicals and pollutants.
Moreover, a healthier natural environment fosters active lifestyles and well-being, contributing to longer, healthier lives. The World Health Organization (35) report “Health in the Green Economy: Co-benefits to Health of Climate Change Mitigation.” Household Energy Sector in Developing Countries highlights the health advantages of mitigating climate change by transforming the household energy sector in developing nations. It focuses on reducing reliance on solid fuels (e.g., wood, coal), which currently contribute to air pollution and respiratory diseases. The report argues that shifting to cleaner energy sources—like electricity and modern biofuels—can improve air quality, reduce disease rates, and benefit the environment by lowering greenhouse gas emissions. It recommends policies promoting affordable, clean technologies, which can simultaneously enhance health outcomes and combat climate change.
China was chosen as the study sample because of its alluring carbon neutralization policies for 2060, which is currently the turning point in the global energy transition because of its ecological civilization, technological innovation, environmental policies, and changes in energy production and consumption mechanisms. To accelerate its energy transition, China has adopted several actions. For instance, China has made significant expenditures in its ability to manufacture green energy in the past several years. Consequently, green energy sources provide 50% of the power produced (36). China has progressively expanded healthcare coverage, including establishing universal health insurance schemes like the New Cooperative Medical Scheme (NCMS) for rural areas and the Urban Resident Basic Medical Insurance (URBMI) for urban populations. The “Healthy China 2030” initiative, which aims to create a healthier China over the next 15 years, was implemented by the Chinese government in October 2016. The program’s objectives include ensuring people’s health is maintained throughout their lives, integrating health into all policies, and enhancing health and health equity. Moreover, it will also increase the national LEF to 79 by 2030. Therefore, the following hypotheses are tested in this empirical study:
H1: Education has a positive effect on life expectancy.
H2: Urbanization has a positive effect on life expectancy.
H3: Green growth has a positive effect on life expectancy.
The study contributes to the existing literature in many ways. For instance, it examines the combined impact of EDU, URB, and GG on life expectancy in China from 1990 to 2022. Previous literature regressed green economy indicators such as renewable energy, green technology and green infrastructure on life expectancy but ignored the GG on LEF. This study is the only study that regressed GG on LEF. Therefore, the study’s outcomes provide a better direction for policy implementation. The rest of the study is organized as follows: Section 2 of the literature review sheds light on the previous studies. Section 3 covers the model, methodology and data. Section 4 illustrates the findings and discussion. Section 5 covers the conclusion and policy recommendation.
Liu et al. (14) investigated the impact of higher education on health in the United Kingdom. They used a quasi-parametric technique for analysis. The result showed that individuals with a greater level of education report better health, maintain a healthier weight, and are less likely to smoke or drink excessively. They suggested that policymakers consider the broader determinants of health and the potential benefits of education in changing health-related behaviors and outcomes.
Iyakaremye and Tripathi (37) examined the impact of education on LEF in Rwanda from 1965 to 2020. They used a vector error correction model (VECM). The findings revealed a significant effect of education on fertility rates, with greater education levels associated with reduced fertility. Furthermore, estimates show an increase in life expectancy across educational levels but less so for the less educated. Gender gaps remain, with male–female life expectancy discrepancies decreasing slower than in prior decades. Increasing prediction intervals indicate increasing uncertainty over time. Balaj et al. (15) conducted a global systematic review and meta-analysis of education’s effects on adult mortality since 1990. The findings indicated that education has a considerable positive effect on reducing all-cause adult mortality, albeit fluctuations in this benefit across time were not statistically significant. Wang et al. (12) used Cox proportional hazard regression to investigate the relationship between education and premature mortality in the Chinese population between 2010 and 2020. They found a strong link between poor education and an increased risk of premature death, with a hazard ratio of 1.93 for individuals with less than elementary education vs. those with higher education levels.
Marlow et al. (38) investigated mortality by education before and during the COVID-19 pandemic in the United States from 2017 to 2020, using data on 7,123,254 deaths, age-standardized-standardized death rates, and mortality rate differences per 100,000 population. Rate ratios comparing the least and most educated were calculated by sex and race/ethnicity. The findings revealed that all-cause mortality rates were around twice as high among those with the most minor education as those with the most education. Disparities in mortality extended dramatically in 2020, with the ratio rising from 2.04 in 2019 to 2.32 in 2020. Notably, unintentional injuries showed the most significant relative rise in mortality inequalities (24.8%).
Addey et al. (39) used Cox regression to investigate the relationship between educational and social inequality and cause-specific death in Mexico City between 1998 and 2004. The findings revealed a considerable inverse relationship between education and premature mortality. Participants with no education had approximately twice the death rate as those with a university education.
Halpern-Manners et al. (40) investigated the effects of education on mortality using linked US Census and administrative mortality data and a twin-difference model. The results revealed strong relationships between education and mortality across all populations, while the estimates were slightly lower among twins and non-twin siblings. This indicates that while education impacts mortality, the effect may be slightly exaggerated without accounting for shared settings. Bijwaard et al. (17) examined the increases in life expectancy related to higher education in men. They analyzed data from the Netherlands using a structural model. The findings revealed significant disparities in life expectancy based on education levels, with higher education being related to longer life expectancy. The study also discusses selection effects, which show that people with greater levels of knowledge have other advantages that help them survive.
The empirical literature examined the EDU-LEF nexus, which reveals consistent evidence of a positive relationship, albeit with variations in magnitude and influencing factors. Studies like Liu et al. (14), Balaj et al. (15), and Halpern-Manners et al. (40) highlight education’s significant role in improving health behaviors, reducing mortality, and increasing LEF across diverse populations. However, differences arise in the degree of impact due to contextual factors. For instance, Iyakaremye and Tripathi (37) emphasize the role of education in reducing fertility and gender gaps in Rwanda, while Marlow et al. (38) and Addey et al. (39) show that the disparities in mortality by EDU are amplified during crises, such as the COVID-19 pandemic. Wang et al. (12) and Bijwaard et al. (17) underscore the heightened risks of premature mortality and reduced LEF among the less educated, often mediated by socioeconomic inequalities. By synthesizing these findings, this study aims to provide a more contextualized understanding of how education shapes life expectancy in China.
Amin et al. (41) used fully modified ordinary least squares to investigate the effects of urbanization and economic growth on life expectancy in ASEAN-5 nations from 1995 to 2020. Life expectancy is the dependent variable, and the independent variables are health expenditure, economic growth, urban population, and CO2 emissions. Their finding of the detrimental impact of urbanization highlights the possible health risks connected with rapid urban development, necessitating careful urban planning. They suggested strategic urban planning to reduce the health risks associated with urbanization, such as investments in healthcare facilities, sanitation, and public health awareness campaigns. Ahmad et al. (1) used a random effect model to examine the impact of URB and income disparity on male and female LEF in South Asian nations between 1997 and 2021. The results demonstrated that urbanization, wealth disparity, and health expenditure significantly impact life expectancy in both males and females. Urbanization and income inequality reduce life expectancy in both circumstances, although health expenditure increases it. Tripathi (4) conducted a state-level analysis of how cities enhanced our health status in India between 1991 and 2011 utilizing static panel data models, specifically fixed-effect and random-effect models. They found that urbanization positively affects life expectancy at birth, with a 10% increase in urbanization resulting in a 3.3% rise in life expectancy. Kadakia and Galea (29) investigated the link between URB and the future of population health. The results revealed that urbanization has resulted in an “urban health advantage” in many locations, with enhanced health services and sanitation contributing to better health outcomes. Michel (27) investigated the relationship between urbanization and aging health outcomes. They discovered a link between urbanization and health outcomes, demonstrating that metropolitan surroundings can have beneficial and harmful effects on the health of older persons. Jiang et al. (42) investigated the impact of urbanization on population health in China from 2007 to 2019 using a threshold regression model. The findings revealed a strong negative association between urbanization and death rates when the logarithm of per capita GDP is less than a threshold value of 10.237. Beyond this threshold, urbanization’s health-promoting effects decline.
Torres et al. (43) investigated the impact of URB on variations in LEF in Scotland from 1861 to 1910. They used a new decomposition method that divides changes in life expectancy into two major components: changes in mortality and population composition. The findings indicated the occurrence of an “urban penalty,” in which urban regions have higher death rates. Furthermore, an “urbanization penalty” is established, indicating the negative impact of population movement from rural to urban areas on overall survival rates. Ali and Audi (2) used ARDL to examine the association between life expectancy, urbanization, and economic misery in MENA countries between 2001 and 2016. They revealed that urbanization has a considerable and beneficial impact on LEF.
The empirical literature on URB and LEF revealed positive and negative impacts. Studies like Amin et al. (41), Ahmad et al. (1), and Torres et al. (43) highlight adverse effects due to health risks, income inequality, and inadequate planning, while Tripathi (4), Kadakia and Galea (29), and Ali and Audi (2) emphasize positive outcomes such as improved infrastructure and urban health advantages. Jiang et al. (42) reveal a threshold effect, where urbanization’s health benefits diminish beyond certain economic levels. These differences often arise from variations in geography, periods, and socio-economic conditions. This study contributes by making these findings and providing an in-depth understanding of how URB affects LEF in China.
Very limited literature is available on the nexus between green growth and LEF; researchers mostly examine the association between green growth indicators and LEF. Such as Karimi Alavijeh et al. (44) analyzed the nexus between renewable energy (RE) and LEF in G-7 economies from 2000 to 2019. They applied the method of moment-quantile regression (MMQR). The findings showed that while increasing carbon dioxide emissions lowers LEF across all quantiles (5th to 95th), renewable energy, health spending, and urbanization enhance life expectancy across all quantiles (5th to 95th). Mihoub et al. (45) examined the relationship between green energy, sustainable development, and the health system in Saudi Arabia from 1990 to 2022 using machine learning. Overall, the findings of machine learning models indicate a strong impact of digital connectivity on health spending by internet users, with scores of 0.673 and 0.86.
Further, economic growth also influences health costs but to a lesser extent, with scores of 0.145 and 0.082. Mobile user penetration and CO2e have moderate to low importance, suggesting nuanced interactions with health expenditure. Patent applications and logistics performance show minimal impact, indicating a limited direct influence on health costs within this study. Similarly, the share of renewable energy is negligible, reflecting its minimal impact on the analyzed data. Finally, regression analyses using ridge and lasso models confirmed similar trends, further validating these findings. Jiang et al. (23) looked at how green technology and digitalization have affected the health of the BRICS nations between 1993 and 2019. The study empirically investigated country-specific analysis using the ARDL estimation technique. They found that, except in Brazil, digitalization has raised life expectancy over the long term in the BRICS countries. In China and Russia, green technology tends to increase life expectancy over the long term, but its short-term effects on health outcomes are negligible. In the short and long term, life expectancy increases in most BRICS nations due to GDP and health spending. Zhou et al. (46) examined the association between public health events and green economy efficiency in 30 Chinese provinces from 2011 to 2019 by utilizing the four-stage SBM-DEA model and a panel model to construct green economic efficiency indicators. First, it is discovered that public health events significantly impair the effectiveness of the green economy. Second, the influence of public health events on green economic efficiency is significantly moderated by environmental legislation. Third, when environmental regulations become more stringent, the effect of public health events on green economic efficiency shifts from impeding to promoting it. Bowen and Lynch (47) analyzed the public health benefits of green infrastructure. They endorse the effectiveness of using green infrastructure as a climate change adaptation tactic. Green infrastructure may enhance water management, control climate change, and lower air pollution.
Most studies have analyzed EDU, URB, or green growth independently or in limited combinations. There is little research that comprehensively examines their joint impact on LEF, particularly in China, where rapid URB, educational advancements, and green growth policies are intertwined. While some studies, like Zhou et al. (46) and Jiang et al. (23), focus on China, they primarily address green growth and its efficiency or the effects of digitalization and green technology. These studies do not explore how green growth interacts with education and urbanization to shape life expectancy. Therefore, this study fills the gap in the existing literature to examine the impact of education, urbanization, and GG on life expectancy in China.
The main purpose of this study to analyze the impact of education, urbanization and GG on life expectancy in China from 1990 to 2022. The model use in this study emerged from the previous literature.
In Equation 1, LEF, EDU, URB, GG, and CO2e denote the life expectancy, education, urbanization, green growth, and CO2 emissions, respectively. Where t represents a time series data from (1990 to 2022), LEF is dependent variable, and independent variables are EDU, URB, GG, and CO2e. We add CO2e as a control variable. If EDU and GG role plays in the functioning of the rising the LEF, and will be positive. Regarding the empirical literature, URB is positive or negative, will be positive or negative. It is expected that CO2e will be negative effect on LEF, will be negative.
In this study, we first test the unit root. Testing for a unit root is important because it helps determine whether a time series is stationary or non-stationary. Non-stationary data with a unit root can lead to spurious regression results, where relationships between variables may appear significant even when they are not. In this we employs the Augmented Dickey-Fuller (ADF), and Phillips-Perron (PP) unit root test. The ADF test developed by Dickey and Fuller (48) and PP test is developed by Phillips and Perron, (49). Equation 2 serves as the foundation for the ADF test.
Where in Equation 2, is the first difference, is a drift term, is a deterministic time trend, represents the lagged level of the series, includes the lagged differences of the dependent variable, is the white noise error term, the super script p is the number of lagged difference terms. The null hypothesis (H0): implies that there is a unit root (non-stationary series), while the alternative hypothesis (H1): suggests stationarity (50). The key feature of the PP test is that it uses non-parametric methods to correct the t-statistic of the coefficient for serial correlation and Heteroscedasticity in the residuals without adding lagged difference terms like in the ADF test.
After the unit root test, we employs the cointegation technique such as (JJ) Johansen and Juselius, (51) cointegation test. Testing the cointegration is important because it helps to identify long-run relationships between non-stationary time series variables. If variables are cointegrated, it means they share a common trend and move together over time, even if individually they are non-stationary. Without testing for cointegration, there is risk obtaining spurious results in regression analysis. Co-integration tests, like the JJ cointegation and ARDL bounds tests, ensure that models capture meaningful long-term relationships. Co-integrated variables can be modeled together, improving the accuracy of predictions and policy implications. The JJ approach is ideal for multivariate time series to detect long-run equilibrium relationships. After the cointegration, we thirdly employs the Autoregressive Distributed Lag (ARDL) model, it estimates the both short-run and long-run relationships between variables, in particularly useful when the variables are of mixed order of integration, i.e., when some variables are I(0) or I(1). The ARDL model can be specified as in Equation 3:
Where difference operator is denoted by delta. The null hypothesis of no long-run relationship existing between the variables (). If -value < lower bound, then accept and the variables are not co-integrated, if -value > upper bound, then reject and the variables are co-integrated, if, but if -value lower bound and upper bound, then the decision is inconclusive. The (ECM) error correction model for the estimation of the short run relationships are specified as in Equation 4:
A negative and significant coefficient implies that any short term disequilibrium between the dependent and explanatory variables will converge back to the long-run equilibrium relationship (52).
After the ARDL estimation, we will test ARDL Diagnostic test, and lastly we further employ the fully modified OLS (FMOLS) and dynamic OLS (DOLS) for the robustness analysis. Both are econometric techniques used to estimate long-run relationships in cointegrated systems. Both methods correct for potential issues like endogeneity and serial correlation that can arise when dealing with non-stationary time series data. FMOLS is a non-parametric correction approach to address serial correlation and endogeneity. While DOLS explicitly adds leads and lags of first differences to deal with the same issues [see, (53, 54); Table 6].
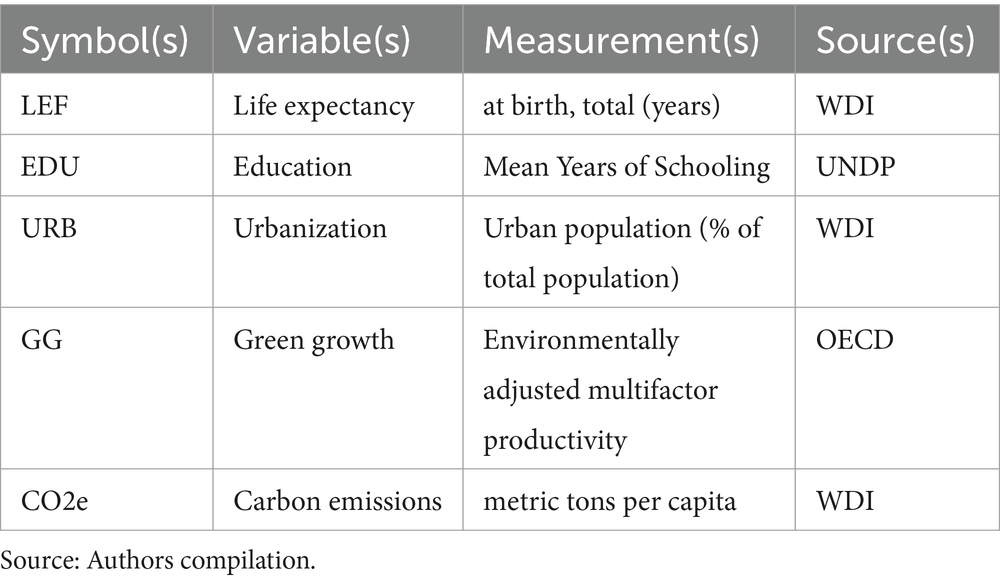
Table 1. Variable measurement.
This study examines the impact of education, urbanization, and green growth on LEF in China from 1990 to 2022. The data has been obtained from the World Development Indicators (WDI), United Nation Development Program (UNDP) and Organization for Economic Cooperation and Development (OECD) websites. Table 1 shows the Variable measurement.
Table 2 displays the descriptive statistics, the mean value of LEF, EDU, URB, GG and CO2e are 73.887, 6.366, 44.237, 4.886 and 4.827, respectively. The median value of LEF, EDU, URB, GG and CO2e are 74.504, 6.407, 43.868, 4.474 and 4.910, respectively. The standard deviation of LEF, EDU, URB, GG and CO2e are 3.290, 1.166, 11.731, 1.414 and 2.221, respectively. The null hypothesis (H0) of the Jarque-Bera test assumes the variable is normally distributed. A higher p-value (> 0.10) suggests failure to reject H0 (i.e., the variable is likely normal). A low p-value (≤ 0.10) indicates a departure from normality. The variables LEF, EDU, URB and CO2e are normally distributed except, GG.
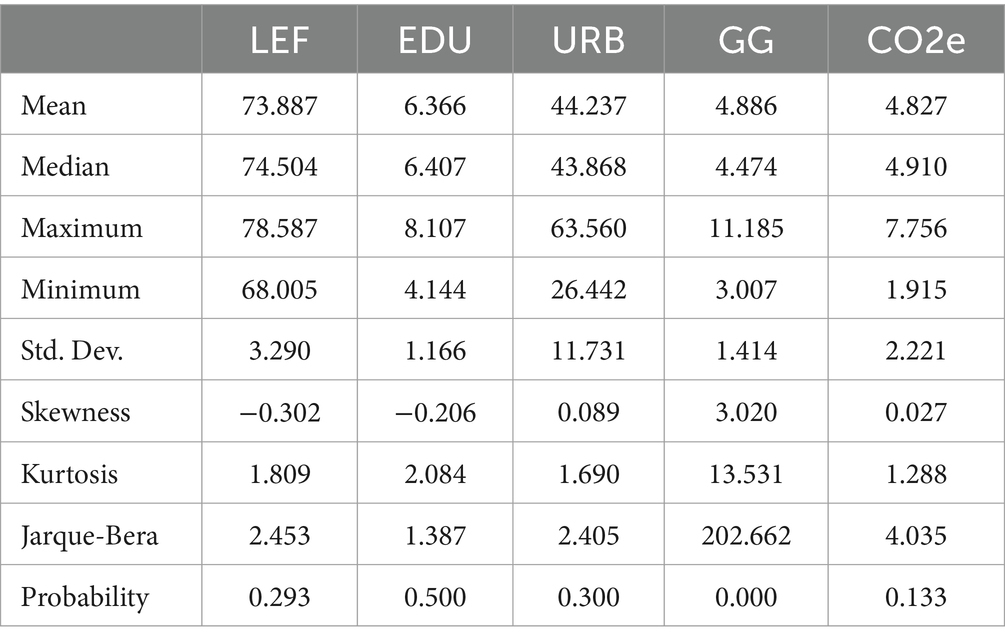
Table 2. Descriptive statistics.
Table 3 presents the outcomes of the ADF and PP unit root test. The outcomes of ADF reported that with constant LEF and GG are stationary at level, URB and GG are stationary at level with constant & trend, while EDU and CO2e are non-stationary at level. After the first difference all variables becomes stationary. The results of PP reported that LEF and GG are stationary at level, while all variables becomes stationary after first difference. So we concluded that there are mixed order of the data stationary. So we will used the ARDL methods. Table 4, shows the results of Johansen cointegration and ARDL bound test. The Johansen cointegration test, Trace statistics confirms the 4 cointegated equation, while Max-Eigen statistics confirms the 3 cointegated equation. Table 4 also shows the assessed value of the ARDL bound test, the F statistic is greater than the 8.560 > 5.53, so the data confirms that there is cointegration among the variables.
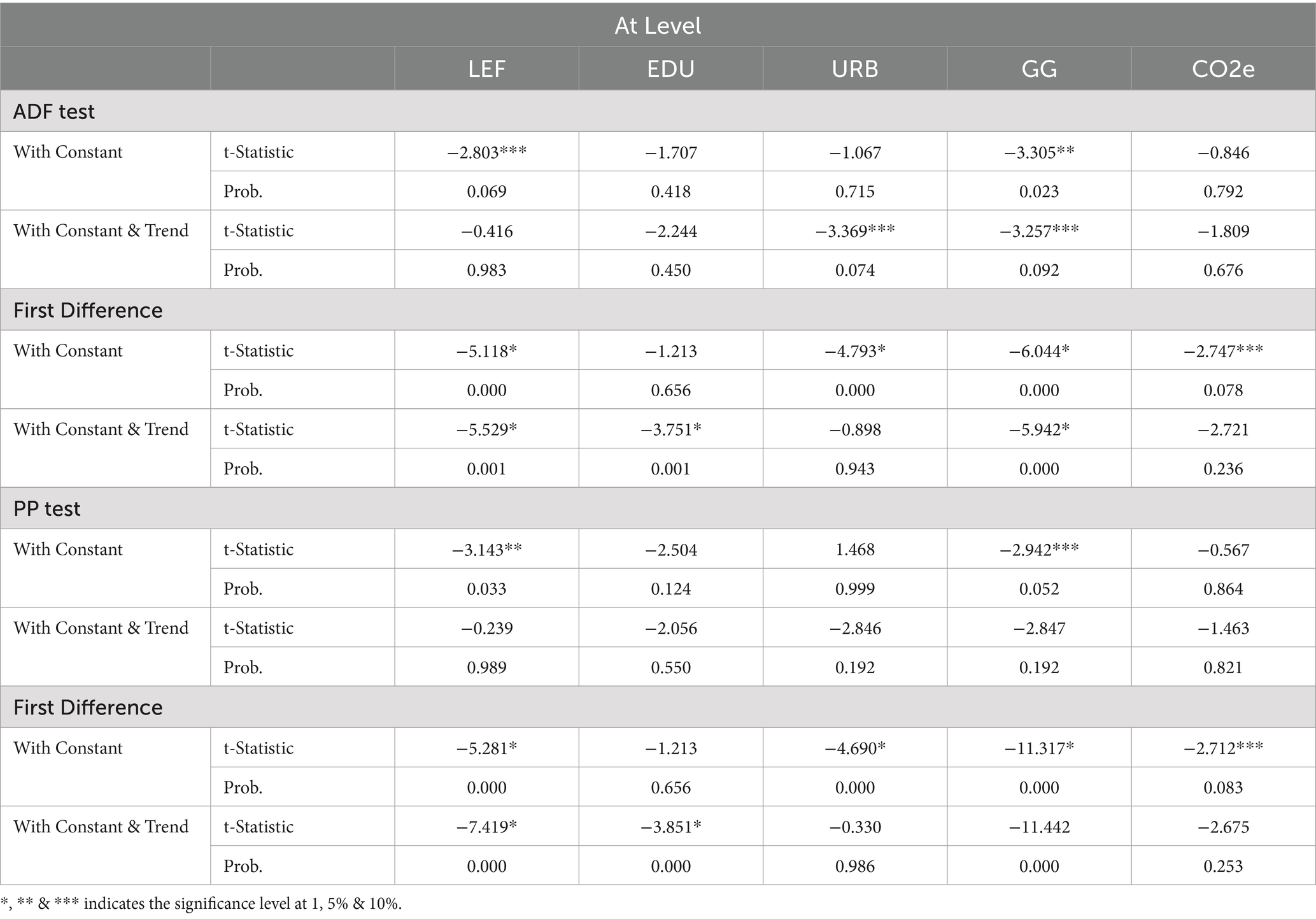
Table 3. Unit root test.
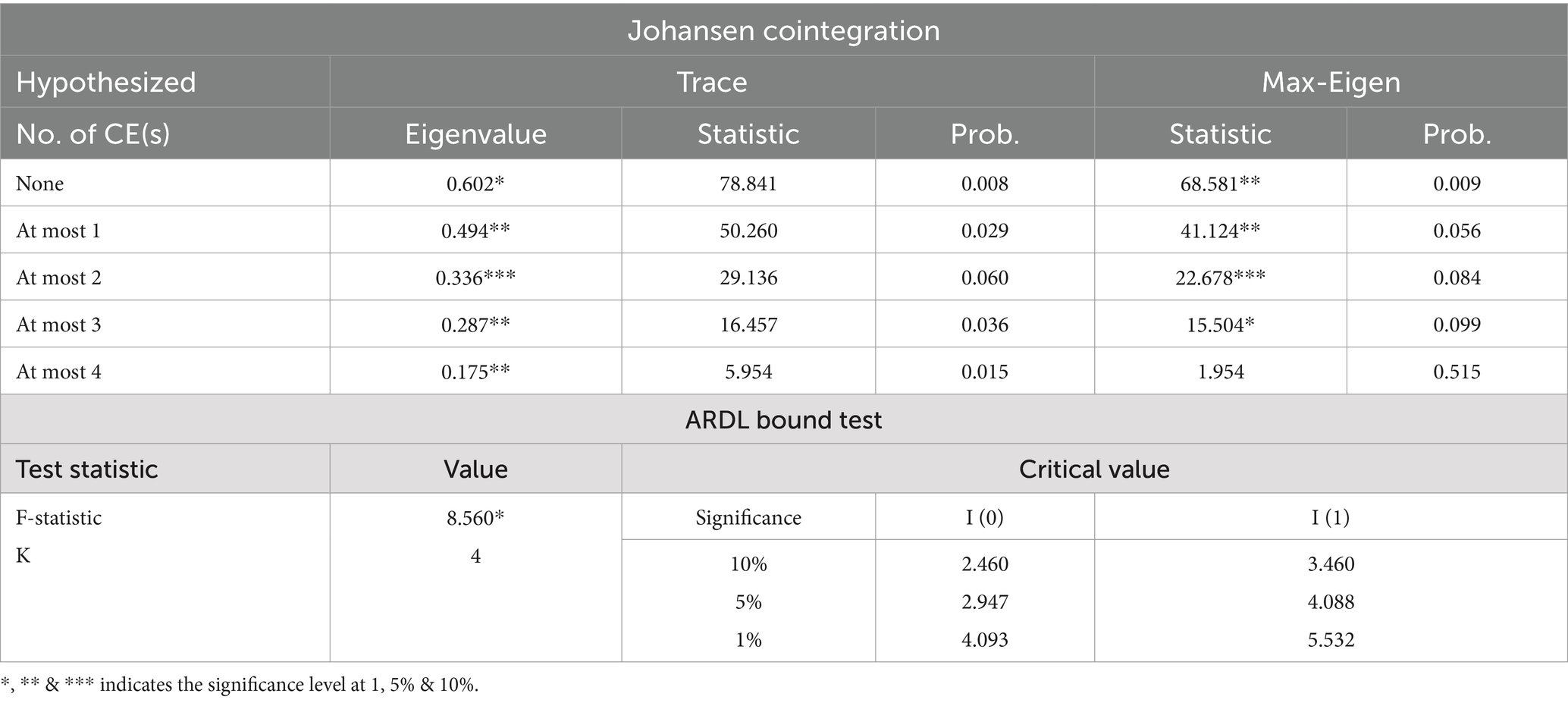
Table 4. Cointegration test.
Table 5 illustrates the results of the ARDL test. In the long run, the coefficient of EDU is positive, indicating that a 1% increase in EDU will surge the LEF by 0.151% at a 1% significance level in China from 1990 to 2022. It rejects the null hypothesis of no nexus between EDU and LEF.
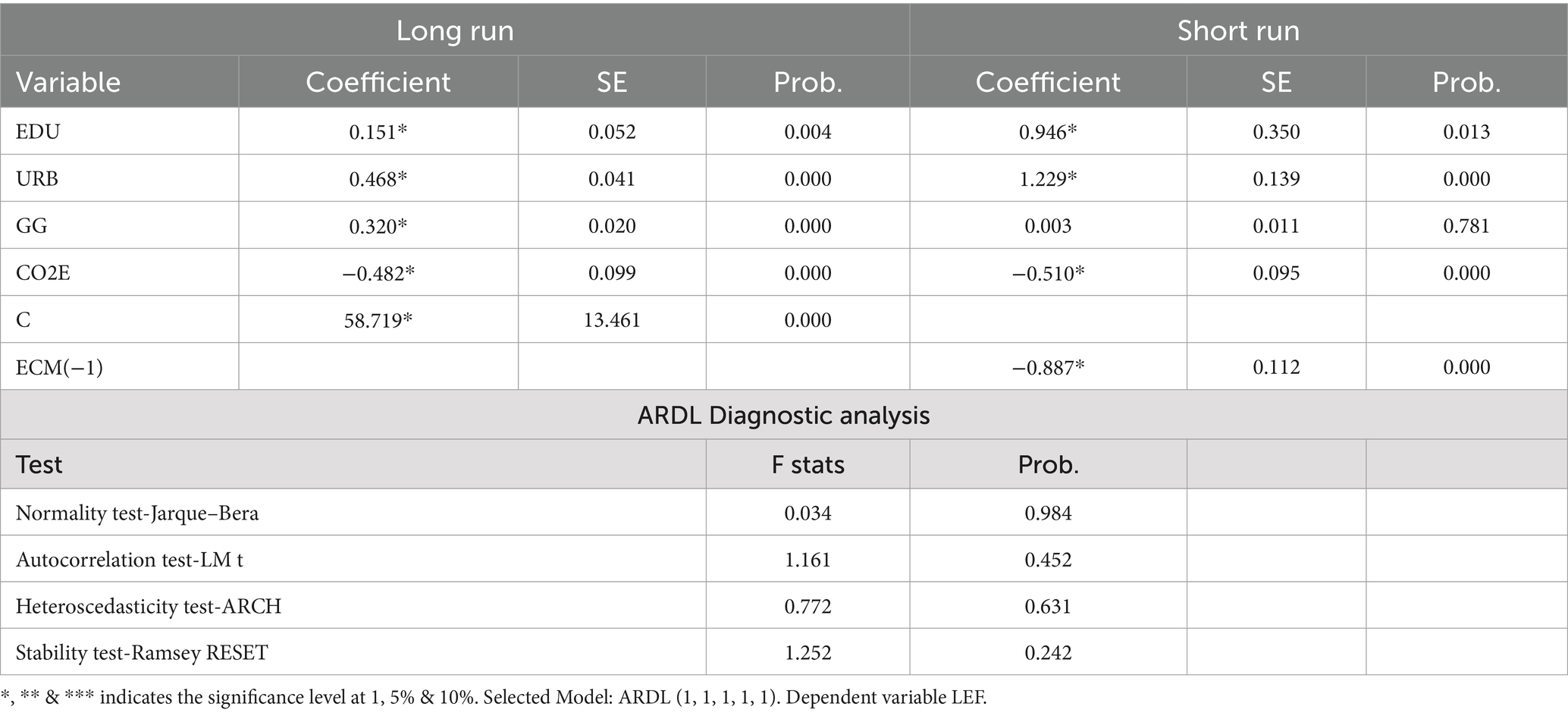
Table 5. ARDL estimates.
The coefficient of URB is positive, showing that a 1% increase in urbanization leads to a surge in LEF by 0.468%. The coefficient of GG is positive, showing that a 1% increase in green growth leads to a surge in LEF by 0.320%. The coefficient of CO2e is −0.482, showing that a 1% increase in CO2e leads to reduced LEF by 0.482%. Table 5 also shows the short-run ARDL estimates. EDU, URB, and GG positively affect LEF, while CO2e negatively affects LEF China from 1990 to 2022. The error correction mechanism (ECM) coefficient is negative −0.887 and significant. It indicates the 88.7% rate at which the dependent variable returns to equilibrium following a deviation.
As shown in Table 5, ARDL diagnostic analyses examine the LEF models. Diagnostic tests indicated that Autocorrelation and Heteroscedasticity were not issues in the ARDL model. The Ramsey RESET and the Jarque–Bera statistic accepted the stable model and normal distribution of residual of the ARDL model. The CUSUM (Cumulative Sum) and CUSUMsq (Cumulative Sum of Squares) tests are shows in Figures 2, 3. Both tests are diagnostic tools used to assess the stability of model parameters over time, particularly in time series analysis, such as in ARDL models. The reliability of policy replication based on the sample period outcomes depends on parameter stability. Since the red line falls within the critical boundaries (represented by blue lines at the 5% significance level), Figures 2, 3 indicate that the LEF models (both short-run and long-run) are well-specified. This demonstrates that the model parameters are robust and produce consistent results. For the robustness analysis we used the FMOLS and DOLS estimators for time series data also used by Azam et al. (55), Khan et al. (56) and Khan et al. (57). The robustness analysis of both FMOLS and DOLS tests confirms the same finding regarding the ARDL long-run estimates, but their magnitude and significance levels differ. According to the findings, the EDU, URB, and GG have a positive effect on LEF, while CO2e has a negative effect on LEF (Table 6).
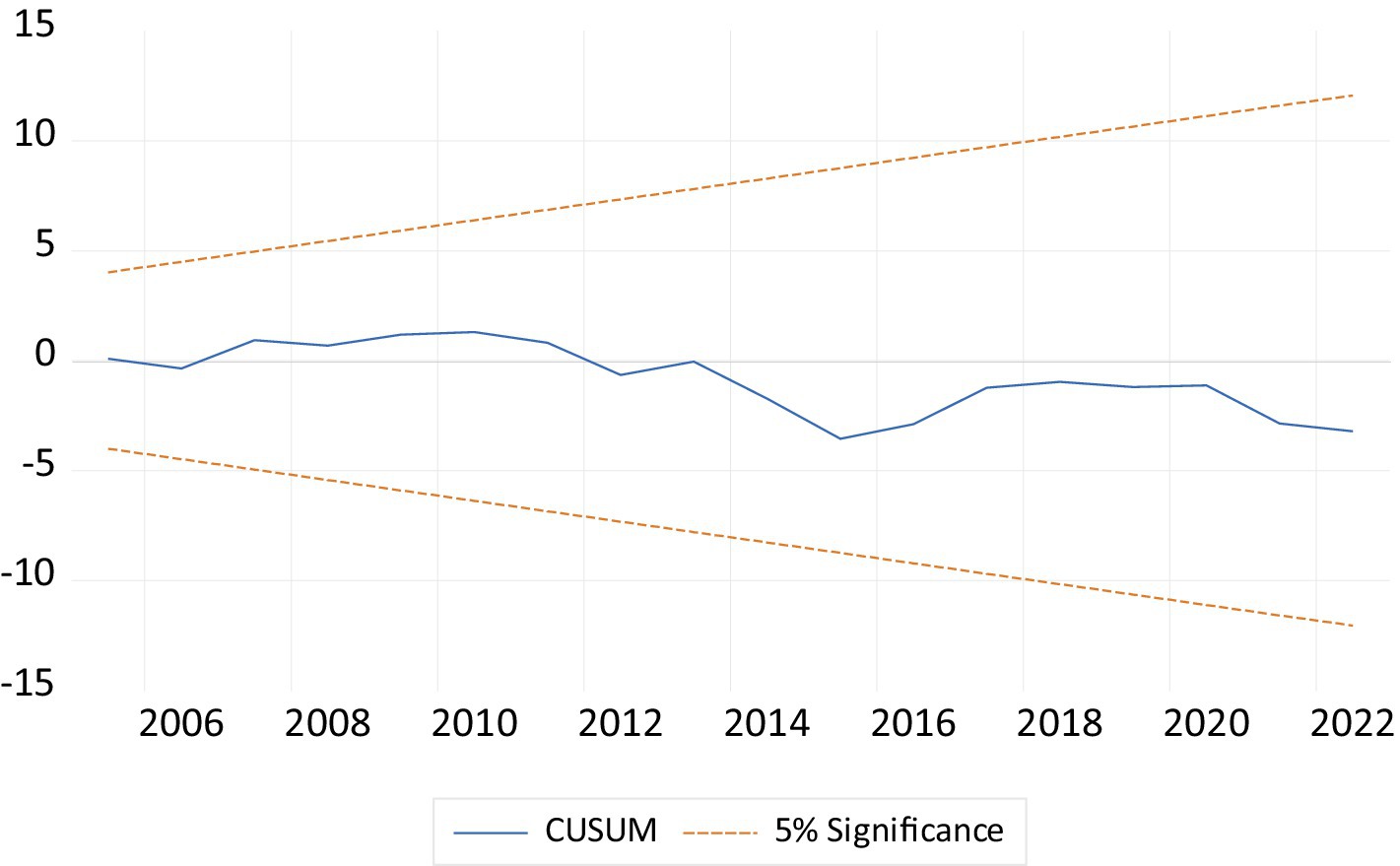
Figure 2. The cumulative sum of the recursive residual plot.
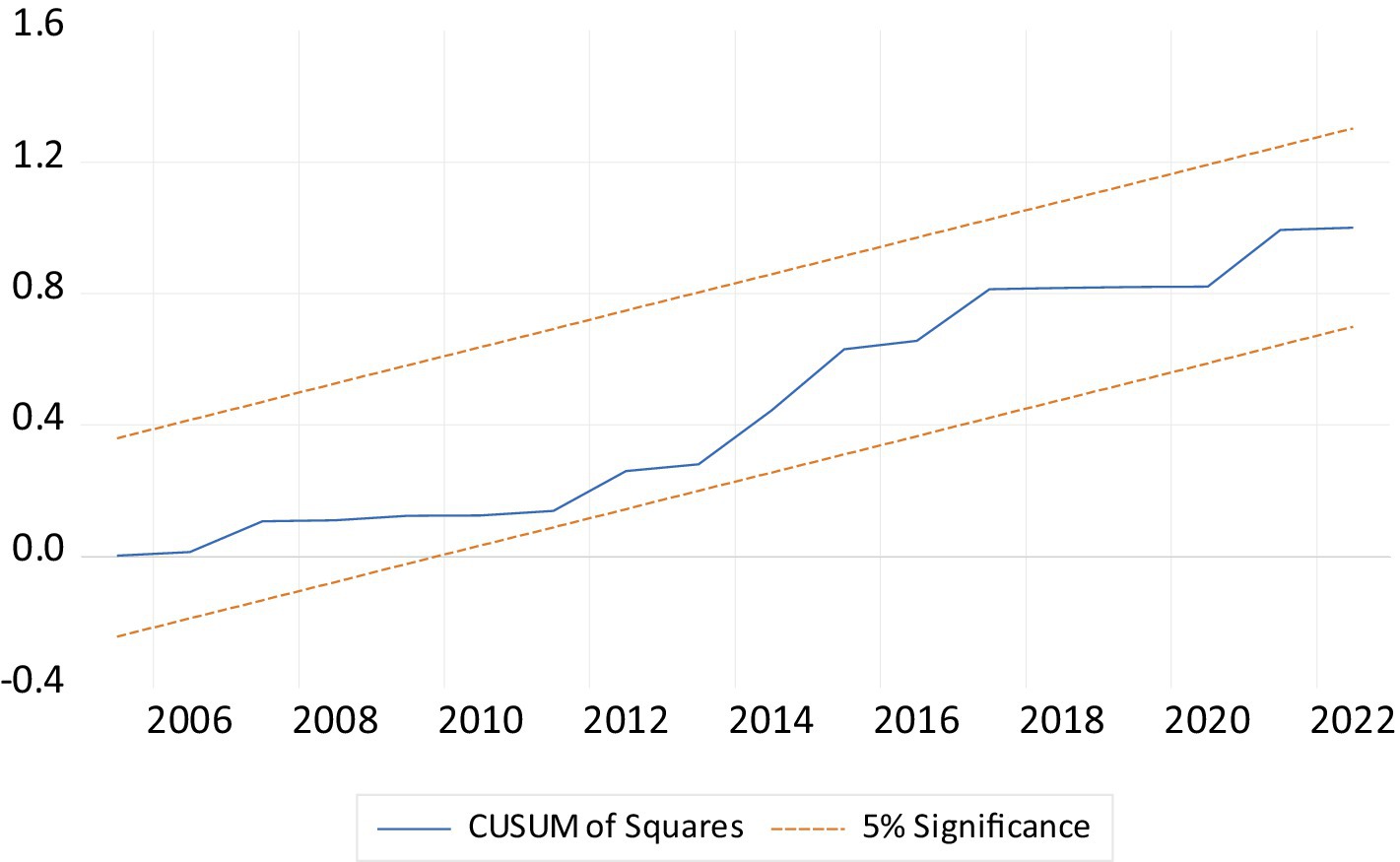
Figure 3. The cumulative sum of the square of the recursive residual plot.
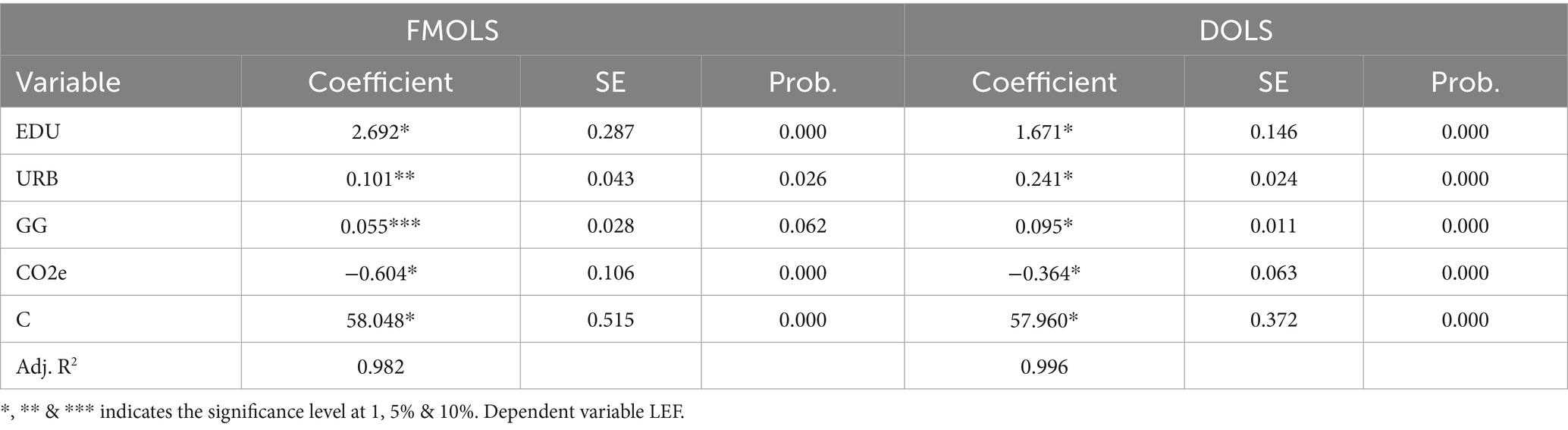
Table 6. Robustness analysis.
In the long run, the coefficient of Education is positive effect on LEF. Education increases LEF by promoting healthier lifestyles, better access to healthcare, and improved health literacy. Educated individuals are more likely to understand health risks, adopt preventative measures, and make informed diet, exercise, and medical care decisions. Moreover, EDU can lead to better economic opportunities, reducing poverty-related health risks and improving access to clean water, sanitation, and nutritious food. The results are consistent with the lines of Liu et al. (14), Iyakaremye and Tripathi (37), and Bijwaard et al. (17). Liu et al. (14) showed that individuals with a greater level of education report better health, maintain a healthier weight, and are less likely to smoke or drink excessively. Iyakaremye and Tripathi (37) revealed a significant effect of education on fertility rates, with greater education levels associated with reduced fertility. Furthermore, estimates show an increase in life expectancy across educational levels but less so for the less educated. Bijwaard et al. (17) revealed significant disparities in life expectancy based on education levels, with higher education related to longer life expectancy. The study also discusses selection effects, which show that people with greater levels of knowledge have other advantages that help them survive.
The urbanization is positive effect on LEF, urbanization increases LEF by improving access to healthcare, clean water, and sanitation infrastructure. Urban areas often provide better medical services, disease prevention programs, and emergency care. URB promotes higher education levels, contributing to healthier lifestyles and better health awareness. Moreover, economic opportunities in cities often lead to improved living conditions, nutrition, and overall well-being, helping reduce mortality rates and extend LEF. The finding is consistent with the findings of Tripathi (4) and contradicts Amin et al. (41) and Ahmad et al. (1). Tripathi (4) reported that urbanization has a positive effect on LEF. Amin et al. (41) found that a detrimental impact of urbanization highlights the possible health risks connected with rapid urban development in ASEAN-5 nations, necessitating careful urban planning. Ahmad et al. (1) reported that urbanization and income inequality reduce life expectancy in South Asian countries.
The green growth is also positive effect on LEF, Green growth boosts LEF by promoting sustainable development that reduces environmental pollution and improves public health. Green growth minimizes health risks such as respiratory and cardiovascular diseases by transitioning to cleaner energy, reducing emissions, and enhancing air and water quality. The finding is consistent with Jiang et al. (23) and Karimi Alavijeh et al. (44). Jiang et al. (23) reported that green technology increases life expectancy. Karimi Alavijeh et al. (44) found that renewable energy has raised the LEF.
The CO2e coefficient is negative effect on LEF, the reason of the negative sign in that CO2e reduces LEF by contributing to air pollution, increasing respiratory and cardiovascular disease risk. Long-term exposure to high levels of CO2e and associated pollutants can worsen public health, leading to higher mortality rates. Additionally, climate change driven by CO2e exacerbates extreme weather events, food insecurity, and the spread of diseases, further negatively impacting LEF. The finding is consistent with the findings of Azam et al. (55) and Uddin et al. (58). Both reported that CO2e reduces the LEF in Pakistan and South Asia.
This study empirically examined the impact of education, urbanization, and green growth on LEF in China from 1990 to 2022 using the ARDL approach to co-integration analysis. The findings showed that urbanization, education, and green growth have a positive effect on LEF, while CO2e has a negative effect on LEF in China.
This study recommends some suggestions for policymakers for health and social well-being through increased life expectancy in China: first, increase funding for public health facilities, ensuring they are accessible, affordable, and equipped to handle a diverse range of health issues. Second, Promote thoughtful urban planning incorporating green spaces, recreational areas, and safe walkways to encourage physical activity and reduce pollution. Third, stricter industrial emissions and vehicle pollution regulations should be enforced to improve air quality, thereby protecting residents’ respiratory health. Fourth, more resources should be allocated to public education systems to ensure access to quality education from early childhood through higher education. Fifth, Promote programs that provide free or subsidized early childhood education to lay a strong foundation for lifelong learning. Sixth, comprehensive health education should be integrated into school curricula to raise awareness about healthy lifestyles, nutrition, and disease prevention. Seventh, Create initiatives that foster parental involvement in education, as engaged parents can positively influence their children’s academic performance and health. Eight, Support policies that incentivize the transition to renewable energy sources, such as solar, wind, and hydroelectric power, to reduce pollution and greenhouse gas emissions and improve health. Ninth, invest in developing and maintaining urban green spaces, parks, and community gardens to improve public health and encourage outdoor activities.
Lastly, several limitations identified in this study will inform future investigations. Future research will use these variables to assess developed, emerging, and developing nations, as we only considered the Chinese economy. Only we utilized some variables and ignored the numerous macroeconomic, demographic, social, and health variables that influence LEF. We did not employ asymmetric analysis or quintile regression and structural break; future research will be used to extend the current study by using this technique.
Data used in this study for empirical examination have been obtained from the World Development Indicators, UNDP, and OECD, given in Table 1. Further inquiries can be directed to the corresponding author.
HZ: Conceptualization, Investigation, Writing – original draft, Writing – review & editing. YZ: Formal analysis, Methodology, Writing – original draft, Data curation, Validation, Writing – review & editing. KC: Formal analysis, Resources, Validation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was funded by “Research on the influence of high-quality population development on the level of new quality productivity in Chengdu”: Z2024PD03 Chengdu Population and Development Research base; “Research on the Impact of Social Capital on Fertility Intention of Women of Childbearing Age”: SXJYZ2401 Sichuan Center for Sociology and Sex Education.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ahmad, N, Raid, M, Alzyadat, J, and Alhawal, H. Impact of urbanization and income inequality on life expectancy of male and female in south Asian countries: a moderating role of health expenditures. Human Soc Sci Commun. (2023) 10:1–9. doi: 10.1057/s41599-023-02005-1
2. Ali, A., and Audi, M. (2019). Economic misery, urbanization and life expectancy in MENA nations: An empirical analysis.
3. Nkalu, CN, and Edeme, RK. Environmental hazards and life expectancy in Africa: evidence from GARCH model. SAGE Open. (2019) 9:2158244019830500. doi: 10.1177/2158244019830500
4. Tripathi, S. Do cities improve our health status? A state-level analysis in India. Regional Econ Develop Res. (2022) 3:89–101. doi: 10.37256/redr.3220221417
5. Liang, LL, and Tussing, AD. The cyclicality of government health expenditure and its effects on population health. Health Policy. (2019) 123:96–103. doi: 10.1016/j.healthpol.2018.11.004
6. World Health Organization (WHO). The financial crisis and global health: Report of a high-level consultation. Geneva, Switzerland: World Health Organization (2009, 2009).
7. Khan, N, Javed, Z, Acquah, I, Hagan, K, Khan, M, Valero-Elizondo, J, et al. Low educational attainment is associated with higher all-cause and cardiovascular mortality in the United States adult population. BMC Public Health. (2023) 23:900. doi: 10.1186/s12889-023-15621-y
8. Grossman, M. Education and nonmarket outcomes. Handbook Econ Educ. (2006) 1:577–633. doi: 10.1016/S1574-0692(06)01010-5
9. Ross, CE, and Mirowsky, J. Why education is the key to socioeconomic differentials in health. Handbook of medical sociology. (2010) 6:33–51. doi: 10.2307/j.ctv16h2n9s.6
10. Mao, Y, Hu, J, Ugnat, AM, Semenciw, R, and Fincham, S. Socioeconomic status and lung cancer risk in Canada. Int J Epidemiol. (2001) 30:809–17. doi: 10.1093/ije/30.4.809
11. Puka, K, Buckley, C, Mulia, N, Lasserre, AM, Rehm, J, and Probst, C. Educational attainment and lifestyle risk factors associated with all-cause mortality in the US. JAMA health forum. (2022) 3:e220401–1. doi: 10.1001/jamahealthforum.2022.0401
12. Wang, J, Zhao, Z, Yang, J, Ng, M, and Zhou, M. The association between education and premature mortality in the Chinese population: a 10-year cohort study. Lancet Regional Health–Western Pacific. (2024) 47:101085.
13. Sabates, R, and Feinstein, L. Education, training and the take-up of preventative health care [wider benefits of learning research report no. 12]. London: Centre for Research on the Wider Benefits of Learning, Institute of Education, University of London (2004).
14. Liu, B, Ji, S, and Zhu, Z. Does higher education matter for health in the UK? SSM-Population Health. (2024) 25:101642. doi: 10.1016/j.ssmph.2024.101642
15. Balaj, M, Henson, CA, Aronsson, A, Aravkin, A, Beck, K, Degail, C, et al. Effects of education on adult mortality: A global systematic review and meta-analysis. Lancet Public Health. (2024) 9:e155–65. doi: 10.1016/S2468-2667(23)00306-7
16. Balaj, M, York, HW, Sripada, K, Besnier, E, Vonen, HD, Aravkin, A, et al. Parental education and inequalities in child mortality: a global systematic review and meta-analysis. Lancet. (2021) 398:608–20. doi: 10.1016/S0140-6736(21)00534-1
17. Bijwaard, GE, van Poppel, F, Ekamper, P, and Lumey, LH. Gains in life expectancy associated with higher education in men. PLoS One. (2015) 10:e0141200. doi: 10.1371/journal.pone.0141200
18. Huisman, M, Kunst, AE, Bopp, M, Borgan, JK, Borrell, C, Costa, G, et al. Educational inequalities in cause-specific mortality in middle-aged and older men and women in eight western European populations. Lancet. (2005) 365:493–500. doi: 10.1016/S0140-6736(05)17867-2
19. Byhoff, E, Hamati, MC, Power, R, Burgard, SA, and Chopra, V. Increasing educational attainment and mortality reduction: a systematic review and taxonomy. BMC Public Health. (2017) 17:1–9. doi: 10.1186/s12889-017-4754-1
20. Giusti, M, Nardi, C, Bonaccorsi, G, Lorini, C, and Persiani, N. Organizational health literacy as a supportive tool for the effective implementation of the 2013/59/EURATOM directive in Italy. Annali dell'Istituto superiore di sanita. (2024) 60:145–53. doi: 10.4415/ANN_24_02_09
21. Zanobini, P, Bonaccorsi, G, Giusti, M, Minardi, V, Possenti, V, Masocco, M, et al. Health literacy and breast cancer screening adherence: results from the population of Tuscany, Italy. Health Promot Int. (2023) 38:daad177. doi: 10.1093/heapro/daad177
22. Elkin, N. The relationship between health literacy and healthy lifestyle behaviors: a meta-analysis. Medicine. (2024) 103:e40260. doi: 10.1097/MD.0000000000040260
23. Jiang, C, Chang, H, and Shahzad, I. Digital economy and health: does green technology matter in BRICS economies? Front Public Health. (2022) 9:827915. doi: 10.3389/fpubh.2021.827915
24. Kabisch, N, van den Bosch, M, and Lafortezza, R. The health benefits of nature-based solutions to urbanization challenges for children and the elderly–a systematic review. Environ Res. (2017) 159:362–73. doi: 10.1016/j.envres.2017.08.004
25. Zhang, L, Yang, L, Zohner, CM, Crowther, TW, Li, M, Shen, F, et al. Direct and indirect impacts of urbanization on vegetation growth across the world’s cities. Sci Adv. (2022) 8:eabo0095. doi: 10.1126/sciadv.abo0095
26. Li, X, Song, J, Lin, T, Dixon, J, Zhang, G, and Ye, H. Urbanization and health in China, thinking at the national, local and individual levels. Environ Health. (2016) 15:113–23. doi: 10.1186/s12940-016-0104-5
27. Michel, JP. Urbanization and ageing health outcomes. J Nutr Health Aging. (2020) 24:463–5. doi: 10.1007/s12603-020-1360-1
28. Okkels, N, Kristiansen, CB, Munk-Jørgensen, P, and Sartorius, N. Urban mental health: challenges and perspectives. Curr Opin Psychiatry. (2018) 31:258–64. doi: 10.1097/YCO.0000000000000413
29. Kadakia, KT, and Galea, S. Urbanization and the future of population health. Milbank Q. (2023) 101:153–75. doi: 10.1111/1468-0009.12624
30. United Nations Department of Economic and Social Affairs (UNDESA) (2018). Data query: urban and rural populations 2018. Available at: https://population.un.org/wup/DataQuery/ (Accessed October 15, 2024).
31. Intergovernmental Panel on Climate Change (IPCC). Climate change 2014: Synthesis report. Contribution of working groups I, II, and III to the fifth assessment report of the intergovernmental panel on climate change. Geneva, Switzerland: IPCC (2014).
32. Kasecker, TP, Ramos-Neto, MB, da Silva, JMC, and Scarano, FR. Ecosystem-based adaptation to climate change: defining hotspot municipalities for policy design and implementation in Brazil. Mitig Adapt Strateg Glob Chang. (2018) 23:981–93. doi: 10.1007/s11027-017-9768-6
33. Organisation for Economic Co-operation and Development (OECD). (2020). Towards green growth: Monitoring progress. Retrieved from https://www.oecd-ilibrary.org/environment/towards-green-growth-monitoring-progress_9789264111356-en (Accessed October 15, 2024).
34. Hussain, Z, Mehmood, B, Khan, MK, and Tsimisaraka, RSM. Green growth, green technology, and environmental health: evidence from high-GDP countries. Front Public Health. (2022) 9:816697. doi: 10.3389/fpubh.2021.816697
35. World Health Organization. (2010). Health in the green economy: co-benefits to health of climate change mitigation - household energy sector in developing countries. Available at: https://www.who.int/publications/m/item/health-in-the-green-economy-co-benefits-to-health-of-climate-change-mitigation---household-energy-sector-in-developing-countries (Accessed October 12, 2024).
36. IEA (2021). China has a clear pathway to build a more sustainable, secure and inclusive energy future. Available at https://www.iea.org/news/china-has-a-clear-pathway-to-build-a-more-sustainable-secure-and-inclusive-energy-future (Accessed October 13, 2024).
37. Iyakaremye, A, and Tripathi, A. Assessing the impact of education on life expectancy in Rwanda. Int J Econ. (2024) 9:65–73. doi: 10.47604/ijecon.2555
38. Marlow, EC, Jemal, A, Thomson, B, Wiese, D, Zhao, J, Siegel, RL, et al. Mortality by education before and during the COVID-19 pandemic, US, 2017–2020. Am J Prev Med. (2023) 64:105–16. doi: 10.1016/j.amepre.2022.08.015
39. Addey, T, Alegre-Díaz, J, Bragg, F, Trichia, E, Wade, R, Santacruz-Benitez, R, et al. Educational and social inequalities and cause-specific mortality in Mexico City: a prospective study. Lancet Public Health. (2023) 8:e670–9. doi: 10.1016/S2468-2667(23)00153-6
40. Halpern-Manners, A, Helgertz, J, Warren, JR, and Roberts, E. The effects of education on mortality: evidence from linked US census and administrative mortality data. Demography. (2020) 57:1513–41. doi: 10.1007/s13524-020-00892-6
41. Amin, NAM, Shaari, MSS, Sulong, A, and Masnan, F. The impacts of urbanization and economic growth on LIFE expectancy in the ASEAN-5 countries. Asian People J (APJ). (2024) 7:126–37. doi: 10.37231/apj.2024.7.1.605
42. Jiang, TB, Deng, ZW, Zhi, YP, Cheng, H, and Gao, Q. The effect of urbanization on population health: evidence from China. Front Public Health. (2021) 9:706982. doi: 10.3389/fpubh.2021.706982
43. Torres, C, Canudas-Romo, V, and Oeppen, J. The contribution of urbanization to changes in life expectancy in Scotland, 1861–1910. Popul Stud. (2019) 73:387–404. doi: 10.1080/00324728.2018.1549746
44. Karimi Alavijeh, N, Ahmadi Shadmehri, MT, Dehdar, F, Zangoei, S, and Nazeer, N. The role of renewable energy on life expectancy: evidence from method of moments quantile regression based on G-7 countries data. Int J Energy Sector Manag. (2024) 18:767–88. doi: 10.1108/IJESM-11-2022-0001
45. Mihoub, A, Kahia, M, and Alswailim, M. Measuring the impact of technological innovation, green energy, and sustainable development on the health system performance and human well-being: evidence from a machine learning-based approach. AIMS Environ Sci. (2024) 11:703–22. doi: 10.3934/environsci.2024035
46. Zhou, J, Yuan, Y, Fu, Z, and Zhong, K. The impact of public health events on green economy efficiency in the context of environmental regulation. Front Public Health. (2022) 10:996139. doi: 10.3389/fpubh.2022.996139
47. Bowen, KJ, and Lynch, Y. The public health benefits of green infrastructure: the potential of economic framing for enhanced decision-making. Curr Opin Environ Sustain. (2017) 25:90–5. doi: 10.1016/j.cosust.2017.08.003
48. Dickey, DA, and Fuller, WA. Distribution of the estimators for autoregressive time series with a unit root. J Am Stat Assoc. (1979) 74:427–31. doi: 10.1080/01621459.1979.10482531
49. Phillips, PCB, and Perron, P. Testing for a unit root in time series regression. Biometrika. (1988) 75:335–46. doi: 10.1093/biomet/75.2.335
51. Johansen, S, and Juselius, K. Maximum likelihood estimation and inference on cointegration—with appucations to the demand for money. Oxf Bull Econ Stat. (1990) 52:169–210. doi: 10.1111/j.1468-0084.1990.mp52002003.x
52. Iheanacho, E. The impact of financial development on economic growth in Nigeria: an ARDL analysis. Dent Econ. (2016) 4:26. doi: 10.3390/economies4040026
53. Phillips, PC, and Hansen, BE. Statistical inference in instrumental variables regression with I (1) processes. Rev Econ Stud. (1990) 57:99–125. doi: 10.2307/2297545
54. Stock, JH, and Watson, MW. A simple estimator of cointegrating vectors in higher order integrated systems. Econometrica. (1993) 61:783–820. doi: 10.2307/2951763
55. Azam, M, Uddin, I, and Saqib, N. The determinants of life expectancy and environmental degradation in Pakistan: evidence from ARDL bounds test approach. Environ Sci Pollut Res. (2023) 30:2233–46. doi: 10.1007/s11356-022-22338-9
56. Khan, F, Uddin, I, Don, YB, and Awan, AM. Does women's education play a role in sustainable environment in Pakistan? A quantitative approach. Environ Dev Sustain. (2024):1–19. doi: 10.1007/s10668-024-05479-4
57. Khan, MA, Uddin, I, and Othman, NS. Factors determining water stress: Do environmental distress, energy consumption and industrialization matter? Environ Dev Sustain. (2024):1–25. doi: 10.1007/s10668-024-04653-y
Keywords: education, urbanization, green growth, life expectancy, China
Citation: Zhang H, Zhan Y and Chen K (2025) Do education, urbanization, and green growth promote life expectancy? Front. Public Health. 12:1517716. doi: 10.3389/fpubh.2024.1517716
Edited by:
Yilmaz Bayar, Bandirma Onyedi Eylül University, TürkiyeReviewed by:
Martina Giusti, University of Florence, ItalyCopyright © 2025 Zhang, Zhan and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yunqiu Zhan, emhhbnl1bnFpdTA2ODhAb3V0bG9vay5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.