 Joana Pombo-Lopes1*†
Joana Pombo-Lopes1*† Inês Rodrigues1
Inês Rodrigues1 Joana Costa1
Joana Costa1 Ana Catarina Gomes1
Ana Catarina Gomes1 Jorge Fonseca2,3
Jorge Fonseca2,3 José Grillo-Evangelista1
José Grillo-Evangelista1- 1Clinical Research Unit (CRU), Egas Moniz Center for Interdisciplinary Research (CiiEM), Egas Moniz School of Health & Science, Almada, Portugal
- 2Aging Lab, Egas Moniz School of Health & Science, Egas Moniz Center for Interdisciplinary Research (CiiEM), Almada, Portugal
- 3GENE - Artificial Nutrition Team - Gastroenterology Department - Hospital Garcia de Orta, Almada, Portugal
Introduction: This review aimed to evaluate the perceived barriers, knowledge, and training, of different health care professionals in relation to the oral health of dependent people in nursing homes and access, as well, how this data was evaluated.
Methods: Three electronic databases—PubMed/MEDLINE, Web of Science, and LILACS—were searched independently by two researchers for relevant studies published up to December 2023. Articles were selected according to the established inclusion and exclusion criteria, and a total of 35 studies were included.
Results: Findings from the Nursing Dental Coping Belief Scale studies revealed disparities between training and daily oral health care, with experienced nurses experiencing challenges. Barriers described were categorized and included resident-related issues, organizational challenges, and caregiver-related difficulties. Most caregivers reported inadequate training, often informal or experiential, although they are involved in the hygiene of the older adult, with tooth brushing and denture cleaning being the most common practices. Low oral health literacy coexisted with recognition of the importance of oral health care.
Conclusion: The findings advocate for targeted interventions, standardized training, and improved support systems to improve oral health care for the older adult in diverse health care settings.
1 Introduction
The global shift to an older population continues to be one of the most significant societal changes of the 21st century, with the global population aged 65 years and older projected to exceed 1.5 billion by 2050 (1). As our population continues to age, the burden of chronic non-communicable diseases such as heart disease, cancer and musculoskeletal disorders will continue to increase (2). Oral diseases are no exception, and because they are often neglected, they continue to be a significant burden (3).
Tooth loss increases with age. According to 2017–2020 National Center for Health Statistics data, 13.2% of seniors have no natural teeth (4) Tooth loss can affect overall health and well-being. Edentulous older adults commonly experience compromised nutritional status, impaired speech function, and social discomfort, potentially leading to social isolation Seniors who have lost all of their teeth typically experience poor nutrition, difficulty speaking, and embarrassment, which can contribute to isolation (5). Nursing home residents, in particular, exhibit high rates of preventable or treatable oral/dental problems, including dental caries, gingivitis, periodontal disease, and gingival or oral discomfort and pain (6–9). The need to improve oral health care in nursing homes becomes even more urgent when we consider that the consequences of poor oral health are associated with an increased risk of malnutrition, aspiration pneumonia, respiratory disease, diabetes, and cardiovascular disease (10–12).
Health care professionals, such as nurses and aides, serve as the primary health care providers in nursing homes. Not only do they spend a considerable amount of time with the older adult, but they also have a significant impact on their health care (13). Although nurses recognize the importance of promoting oral health in frail older adults (14–16), the literature highlights the inadequacy of oral health education and training for health care professionals (17, 18). Unfortunately, dental health in older adults is often overlooked and remains an understudied area of research despite its importance in maintaining well-being, overall health, and quality of life (19, 20).
While there are scientific papers on oral health in nursing homes and institutionalized older adults, there are no systematic reviews on caregivers’ perceptions. This systematic review aims to evaluate caregivers’ perceptions of oral health care for dependent nursing home residents. The objectives were to summarize the methods used to assess barriers/difficulties, knowledge, training, available equipment, and perceptions of health care professionals regarding oral health care for dependent nursing home residents.
2 Methods
2.1 Protocol and registration
All authors drafted the protocol, registered it with the National Institute for Health Research PROSPERO (http://www.crd.york.ac.uk/PROSPERO, ID number: CRD42024497782), and reported it according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) checklist (Supplementary Table S1).
2.2 Focused questions and eligibility criteria
We developed a protocol to answer the following PICO question: “What are the perceptions of health care professionals regarding oral health care for dependent nursing home residents?.” The respective statements were as follows:
• P (Participants): Health care professionals caring for dependent older adults in long-term care facilities.
• I (Intervention): No intervention was applied, as the focus was on health care professionals’ perceptions and practices.
• C (Control): The presence or absence of a control group was not a limitation.
• (Outcome): The outcome was the assessment of the perceptions, barriers, difficulties, knowledge, training, and available equipment for performing oral health care, as reported by health care professionals.
Cross-sectional observational studies were eligible for inclusion if they addressed the perceptions, difficulties, activities performed, and knowledge of health care professionals providing oral health care to dependent adults in long-term care facilities. Exclusion criteria were as follows: 1. duplicate studies; 2. abstracts, commentaries, reviews, letters to the editor, consensus, opinions, case studies, and case series; 3. unpublished information; 4. absence of the data being studied; 5. data obtained through a non-structured interview with non-comparable results; 6. population being family members as informal caregivers; and 7. articles written in languages other than English, Spanish, Portuguese, or French. There were no restrictions on the year of publication.
2.3 Data search strategy and study selection
We searched PubMed through PubMed/MEDLINE, Web of Science, and LILACS for all relevant articles published until December 2023. The following search terms were used: (1) (care home OR nursing home OR residential OR caregiver* OR care facilities); (2) (elder* OR senior* OR old OR aged OR geriatric); (3) (oral health OR oral care OR oral knowledge OR health care). Two independent reviewers (J.P.L. and I.R.) performed the search and included studies. Two independent reviewers independently assessed the titles and/or abstracts of the retrieved studies in duplicate (J.P.L. and I.R.), and disagreements were resolved by discussion with a third author (J.C.). For measurement reproducibility, inter-examiner reliability following full-text assessment was calculated using the kappa statistic.
2.4 Risk of bias assessment
The methodological quality of the eligible studies was assessed using the Newcastle-Ottawa Scale (NOS) (21), which was adapted for cross-sectional studies (Appendix 1). This adapted version of NOS evaluates three major domains for potential sources of bias: (1) selection bias (methods of participant selection), (2) comparability bias (methods of controlling for confounding variables), and (3) outcome bias (methods of assessing outcomes). Each of the seven items on the scale is assigned a star, with a maximum of one star per item. In this review, both selection bias and outcome bias were of particular concern due to the reliance on self-reported data, which can introduce a range of biases, such as recall bias or social desirability bias. Therefore, we assessed whether studies adequately controlled for such biases by using validated tools, objective measures, or triangulation of data sources where possible. The risk of bias assessment was conducted by two researchers (J.P.L. and I.R.), with any disagreements resolved by consulting a third researcher (J.C.). If a study was deemed to have a high risk of bias in any domain, we noted this in the quality assessment summary and took it into account when interpreting the findings.
2.5 Data extraction process and data items
Data extraction was performed independently by two reviewers (J.P.L. and I.R.), with discrepancies resolved through discussion with a third reviewer (J.C.). The following information was extracted from each eligible study: first author’s name, year of publication, country and location of sampling, sample size (male/female), mean age and mean years of experience, oral health perceptions of health care professionals, type of assessment, and study funding. For nurse perceptions, some specific information was collected from the studies for comparison: knowledge of dental terms/oral health; previous training to provide oral health care, type of training and perceived need for additional training; oral health care activities performed and availability of supplies to perform such care; access to oral health care by an oral health professional, perceived barriers/difficulties; and importance placed on oral health/relationship of oral health to systemic health.
We recognize that this review relied on self-reported data (e.g., surveys or interviews) to assess health care professionals’ perceptions and practices. While self-reported data are commonly used in research of this nature, they introduce a potential source of bias, such as social desirability bias, where respondents may report behaviors or attitudes, they believe are more socially acceptable or expected. Additionally, recall bias may influence the accuracy of self-reports, particularly when participants are asked to reflect on past experiences or behaviors. These limitations were considered when assessing the overall quality of the studies, and we critically discuss their potential impact on the findings in the subsequent sections.
For data analysis, standard spreadsheet software (Microsoft Excel for Mac, version 16.50. Microsoft, Redmond, WA, United States) was used to extract data. Frequencies and percentages were used to describe categorical variables, while continuous variables were reported as mean ± standard deviation (SD) and range.
3 Results
3.1 Study selection
The online search strategy identified 2,091 potentially relevant publications. After removing duplicates, 1,455 articles were assessed for eligibility criteria and 1,359 were excluded after title and/or abstract review. Of the 96 articles assessed for eligibility through full paper review, one could not be retrieved and 60 were excluded, with reasons for exclusion detailed in Supplementary Table S1. As a result, a final number of 35 observational studies were included for qualitative synthesis. The PRISMA plot is shown in Figure 1. The inter-observer reliability of the full-text screening was considered substantial (kappa score = 0.614, 95% CI: 0.471–0.757) (22).
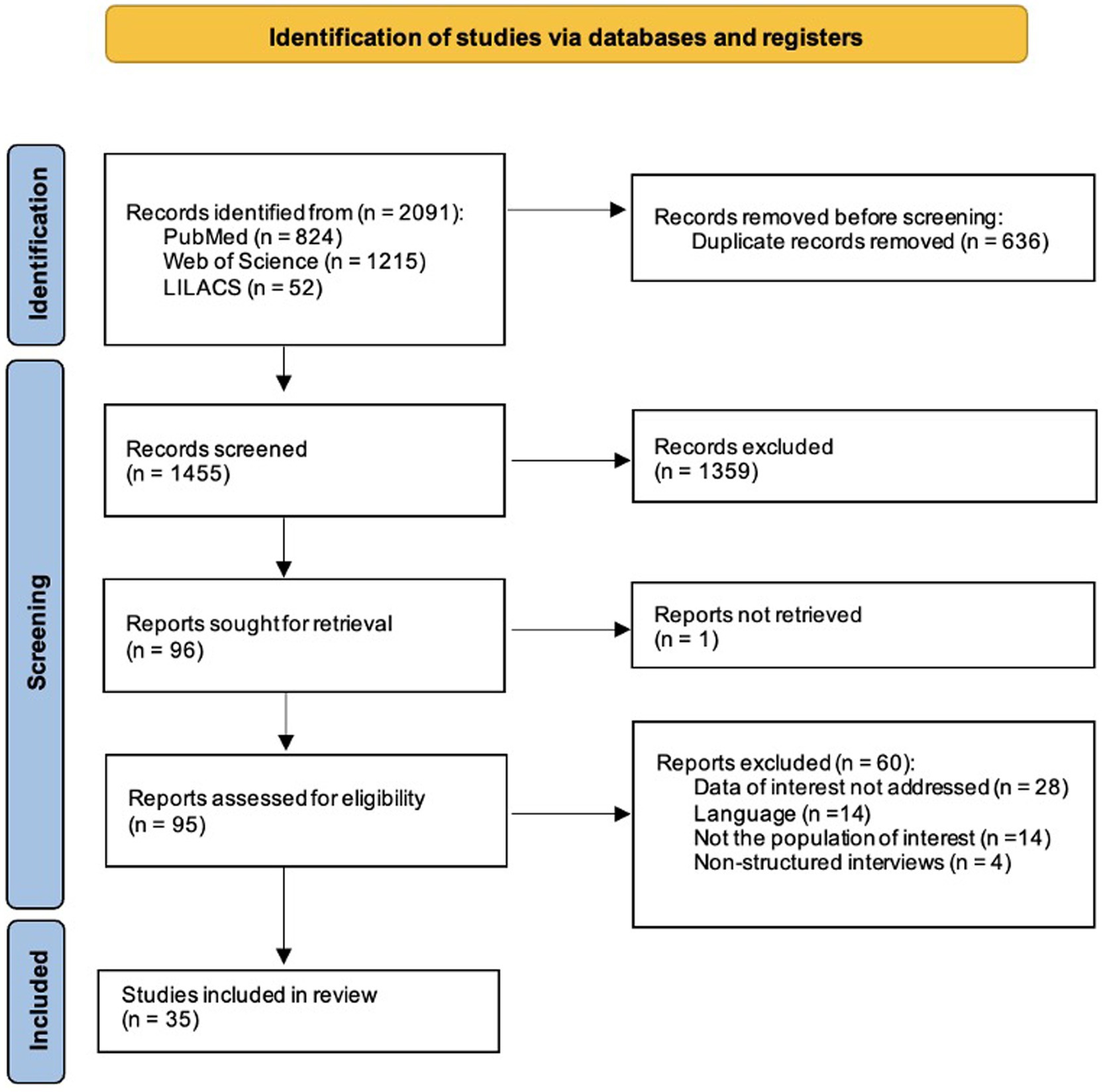
Figure 1. Prisma Flowchart.
3.2 Studies characteristics
A total of 6,179 participants, 4,219 women, and 554 men (1,406 did not report gender), from all 35 included studies were included in this systematic review (Table 1). The calculated percentage of 88.4% of female participants corroborates the literature, where most caregivers were female. The sample included personnel directly involved in providing oral health care to residents of health facilities: mostly nurses, assistant nurses, qualified aides, non-qualified aides, and some articles categorized them only as caregivers or careers (23–37). Others included diverse populations such as occupational therapists, speech therapists, social workers, physiotherapists, nursing students, dental nurses, and dental hygienists (15, 16, 38).
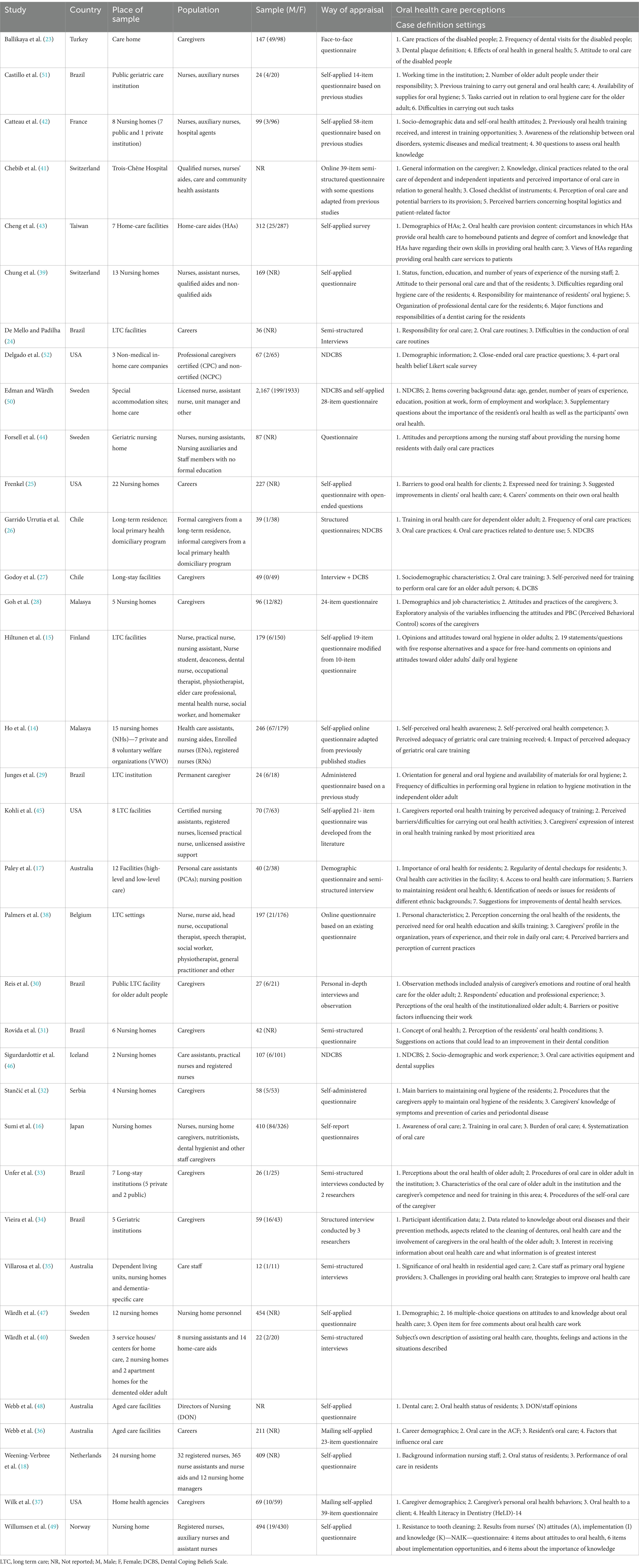
Table 1. Characteristics of the included studies.
Of the 35 articles included, 9 articles (about 17%) were published before 2010 (16, 17, 24, 25, 39, 40), with the oldest article published in 1999. All the remaining articles were published after 2010, and about 43% of them were published after 2015. The latest article was published in 2023.
Most of the studies were conducted in care facilities for the older adult, with the exception of one study developed in a hospital setting (41).
Several issues were considered in the case definition setting. Some studies addressed more than one issue: 29 studies searched barriers or difficulties felt when performing oral health care activities (14–18, 23–25, 28–33, 35–49), 13 studies assessed the perceived importance of oral health care (28, 30, 31, 34, 35, 41, 42, 50, 14–18), 19 accessed oral health knowledge (14, 18, 23, 28, 30–37, 40, 42, 46–49, 51), 20 studies emphasized previous training received (14–16, 18, 23, 26–28, 32, 35, 39–43, 46–48, 51, 52), and 24 the perceived need for training (14–18, 23, 25, 27, 30, 32–38, 40, 42, 45–50). The other 14 studies mentioned the access to oral health care by an oral health professional (14–18, 24, 30, 31, 35–37, 39, 40, 42, 48), 22 studies explored the oral health care activities performed (14, 18, 23, 24, 26, 29–37, 40, 41, 43, 46–49, 52), and 7 studies evaluate if supplies to perform such oral health care activities were available (18, 25, 29, 30, 32, 33, 46).
The methods used to collect data on oral health care provided by caregivers varied between studies and some applied more than one. Questionnaires were used in 24 studies (14–16, 18, 23, 25, 26, 28, 29, 31, 32, 36–39, 41, 42, 44, 45, 47–49, 51), semi-structured interviews in 8 studies (17, 24, 27, 30, 33–35, 40), and a more systematic data collection approach using the NDCBS in 5 studies (26, 27, 46, 50, 52).
Furthermore, studies were conducted in 17 countries worldwide: Turkey (23), Brazil (24, 29–31, 33, 34, 51), France (42), Switzerland (39, 41), Taiwan (43), USA (25, 37, 45, 52, 53), Sweden (40, 44, 47, 50), Chile (26, 27), Malaysia (14, 28), Finland (15), Australia (17, 35, 36, 48), Iceland (46), Serbia (32), Japan (16), Netherlands (18), Norway (49) and Belgium (38). Of note, no studies were performed in Africa.
3.3 Methodological quality of the included studies
The methodological quality of the studies varied significantly, with most studies falling into the fair (31.4%, n = 11) or high (28.6%, n = 10) quality categories, and 7 studies rated as low quality (Table 2). None of the included studies described and calculated the non-response rate (item 3). Studies mostly failed to identify confounding factors and to perform a subgroup or multivariable analysis taking them into account (51.4%, n = 18) (item 5) and to use a validated screening/measurement tool (88.6%, n = 31) (item 4). This presents a concern regarding the reliability and generalizability of the findings.
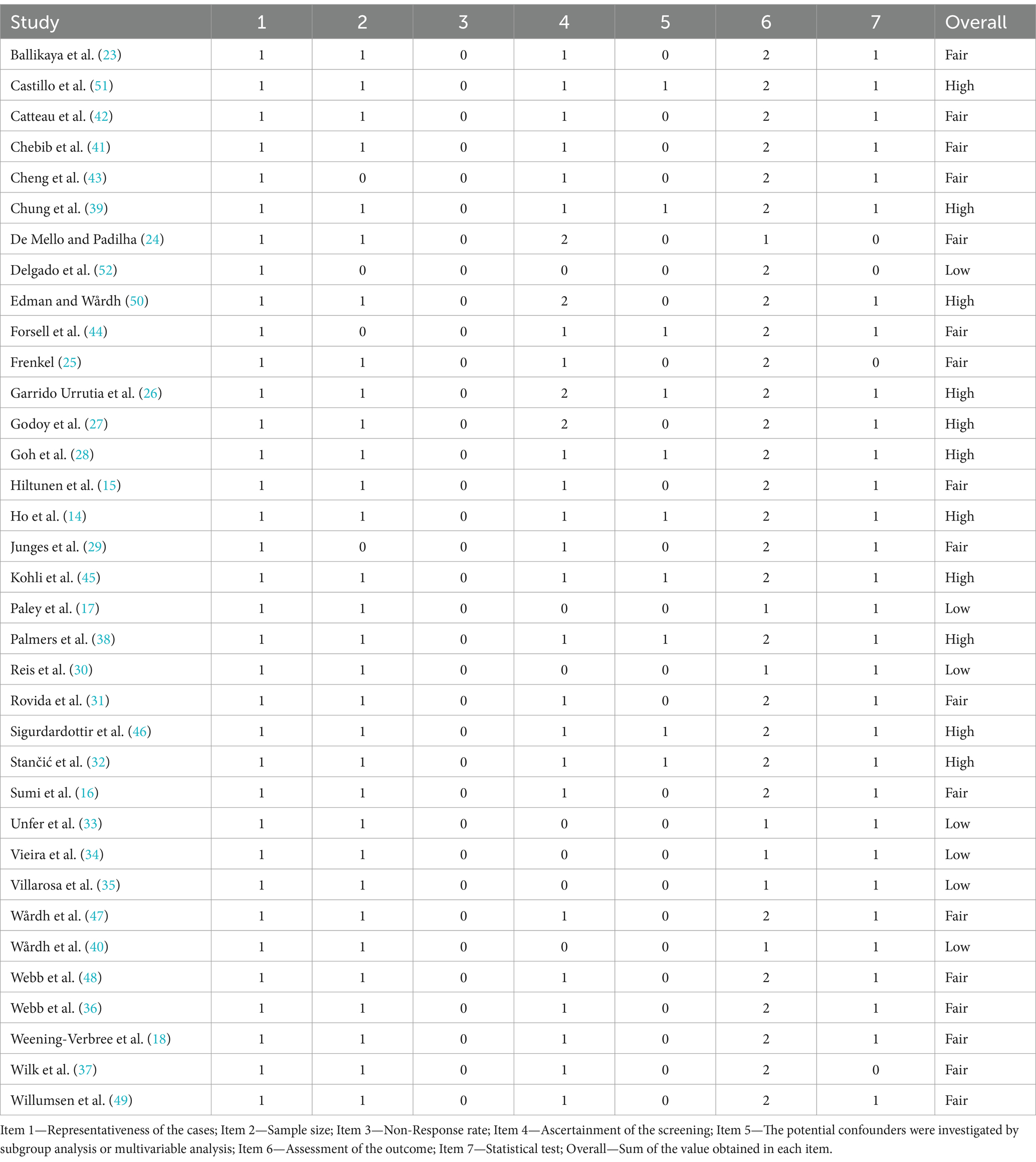
Table 2. Results from the methodological appraisal using Newcastle-Ottawa Quality Assessment Scale adapted for cross sectional studies.
The heterogeneity of the studies was also evident, as different data collection methods were used, including questionnaires (24 studies), semi-structured interviews (8 studies), and the Nursing Dental Coping Belief Scale (NDCBS) (5 studies). This methodological diversity complicates direct comparisons between studies and highlights the potential for bias introduced by the lack of standardization in measurement tools. Furthermore, the study populations varied widely, including different categories of health care professionals (e.g., nurses, aides, dental professionals) across various countries, settings (nursing homes vs. hospitals), and types of training (formal vs. informal). This variation in study design and execution calls for caution in interpreting the aggregated results and underscores the need for more standardized approaches in future research.
3.4 Synthesis of evidence
3.4.1 Nursing dental coping belief scale
The Nursing Dental Coping Belief Scale (NDCBS), originally validated in the U.S. for male veterans (54), was adapted for use with health care professionals in nursing settings (55). The aim was to create an oral health care priority index that could be used in both hospital wards and specialized facilities. The instrument consists of a 28-item questionnaire covering four dimensions: internal locus of control (IL), external locus of control (EL), self-efficacy (SE), and oral health care beliefs (OHCB). Lower scores represent an individual’s positive DCB and strong belief in their ability and competence to influence oral health behaviors. Four of the included studies (26, 27, 46, 52) used the NDCBS. The scale measures four dimensions: internal locus of control, external locus of control, self-efficacy, and beliefs about oral health care. Studies using the NDCBS have found that nurses’ beliefs about their ability to influence oral health behavior were often overly optimistic, with many overestimating their knowledge and skills. However, their actual practice did not always support this self-assessment bias (26, 52). In some studies, nurses with more formal training showed better beliefs about their competence (27, 46). In constrast, while other studies showed that more extended work experience was paradoxically associated with poorer dental coping beliefs (46). The inconsistency of these findings points to the heterogeneity of carers’ perceptions, which personal attitudes, educational background, and workplace dynamics may influence.
3.4.2 Perceived oral care barriers
The barriers or difficulties experienced by caregivers in providing oral health care to residents, which were mentioned in 29 of the included studies (14–18, 23–25, 28–33, 35–49), were categorized into 3 groups: barriers related to the residents themselves, barriers related to the organization, and barriers related to the caregiver (Table 3).
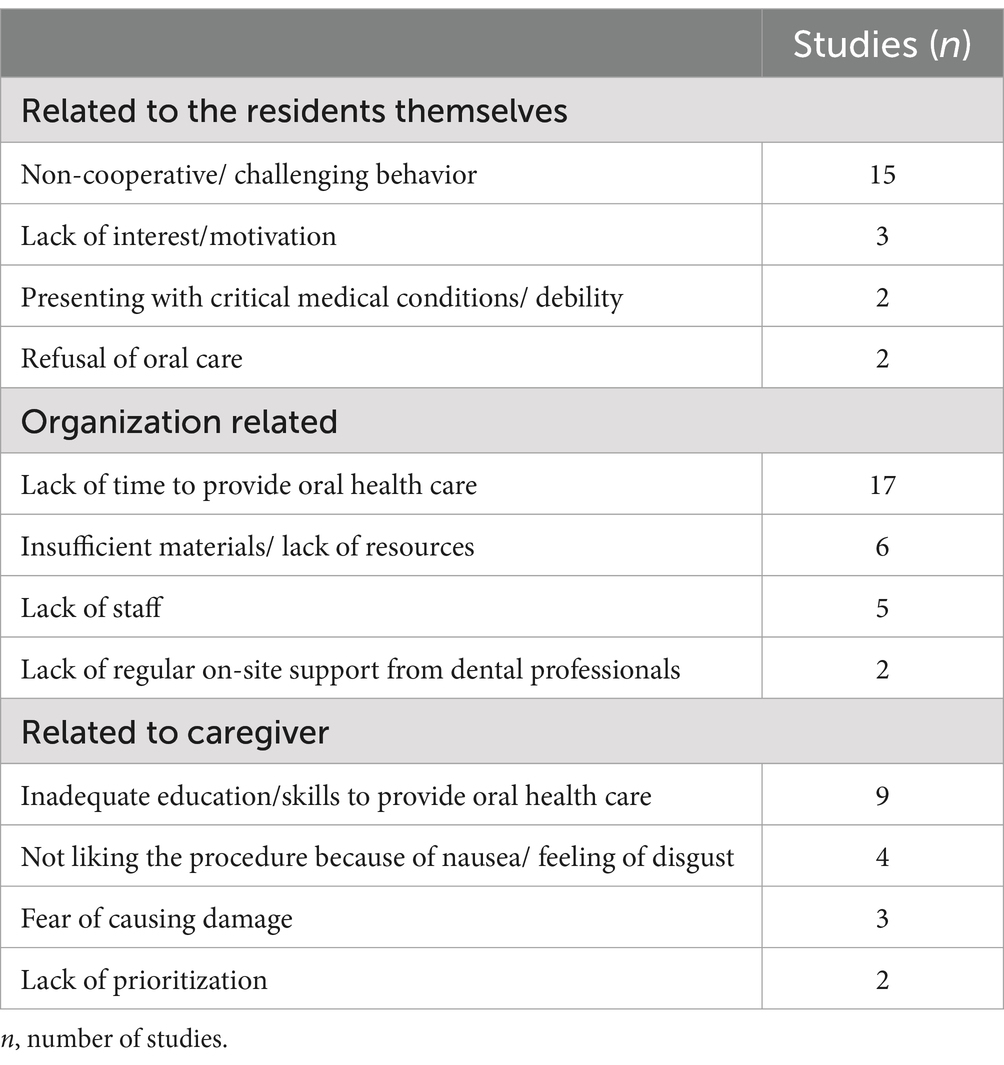
Table 3. Barriers/difficulties perceived by the caregivers and mentioned in the included studies (n total = 29 studies).
In terms of barriers related to the residents themselves, lack of cooperation was the most frequently reported, in 15 studies (14, 18, 24, 25, 28–30, 32, 35, 39, 41, 44, 45, 47, 48). Negative attitudes, bad moods, cursing, and even physical violence are some of the challenging behaviors exhibited by the residents and reported by caregivers. Other barriers include residents’ lack of interest or motivation (32, 41, 44), residents’ critical illness or debility (30, 41), and residents’ refusal of oral health care (41, 45).
Most caregivers report that they do not have time to provide oral hygiene to the residents (15, 18, 24, 25, 28, 29, 32, 33, 38–43, 45–47). Lack of oral hygiene materials (18, 28, 32, 38, 41, 48), lack of staff (33, 38, 41, 42, 47), and lack of regular on-site support from dental health professionals (14, 35) are also reported as organizational barriers. Caregivers also report not having adequate training or skills to provide oral health care (28, 31, 35, 37–40, 46, 48). In addition, motives such as disgust or lack of association with the procedure (15, 23, 25, 39), fear of causing harm (25, 28, 44), or lack of prioritization (18, 35) have also been reported as caregiver-related difficulties in providing oral health care.
The variability in the nature and extent of these barriers across studies highlights the heterogeneity of care contexts and the complexity of addressing these challenges.
3.4.3 Training in providing oral health care
Table 4 shows the number and percentage of caregivers who received training in oral health care and the type of training received. In most studies, less than half of the caregivers reported receiving training in oral health care for the older adult (16, 18, 23, 26–28, 39, 42, 43). Unfortunately, not all of these studies evaluated the type of training received. Those that did so concluded that, in most cases, the training was informal or based on personal experience (28, 32, 42, 43, 47, 51). However, in almost all studies that assessed the need for training, participants were interested in implementing training programs (14–16, 18, 23, 27, 32, 35, 40, 42, 46–48). This gap between the need for training and the actual provision of training reflects an important organizational barrier. It highlights the potential for improving nurse education to improve oral health care practice.
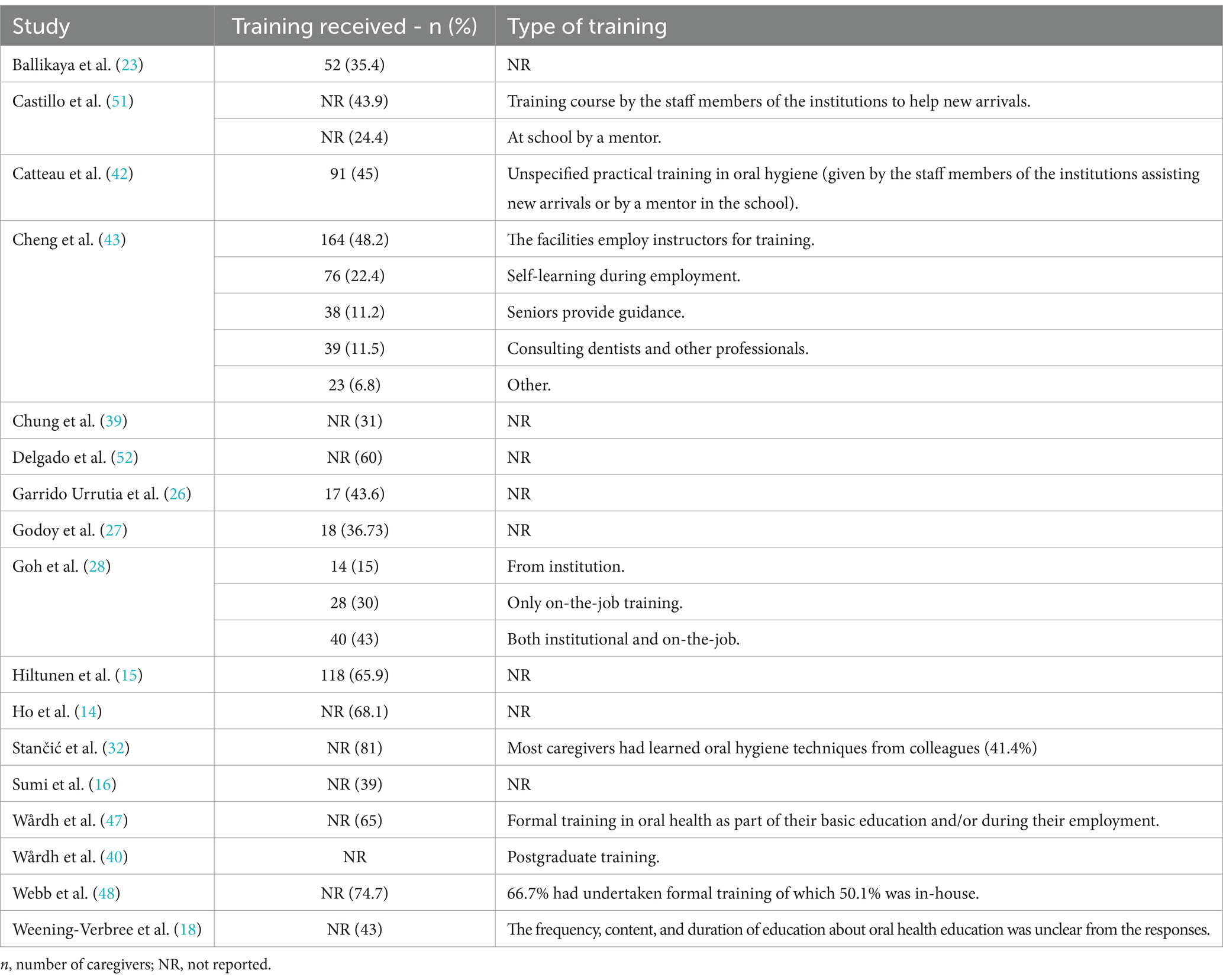
Table 4. Received previous training and type of training received.
3.4.4 Oral health knowledge, importance given to oral health, and oral health care activities performed
A total of 18 studies (14, 18, 23, 28, 30–37, 40, 42, 46–49, 51) assessed oral health knowledge using different measures. However, the conclusions were consistent with low oral health knowledge. Gaps in oral health knowledge include beliefs that tooth loss is an inevitable part of aging (14, 28) or that caries is a communicable disease, and lack of information about periodontitis (32, 34, 42). In a single study (51), caregivers were highly educated in the theoretical context, but this wasn’t reflected in the oral hygiene of the older adult as observed by the mucosal and plaque index. Although oral health literacy is low, participants recognize the importance of providing oral health care to residents and are aware of the interaction of systemic diseases and medical treatments with oral disease and the well-being of the older adult (14–18, 28, 30, 31, 34, 35, 41, 42, 50).
A total of 22 studies reported oral health activities performed by caregivers (14, 18, 23, 24, 26, 29–37, 40, 41, 43, 46–49, 52). The most common performed oral hygiene activity was tooth brushing (14, 18, 23, 24, 26, 29–37, 40, 41, 43, 46–49, 52) followed by denture cleaning (14, 18, 24, 26, 29–33, 35–37, 41, 43, 46, 48, 49). Other activities such as rinsing the mouth with a mouthwash (24, 26, 32, 35, 43), removing dentures for sleep (26, 41), cleaning the oral mucosa with a gauze in the absence of teeth (26, 29, 30), and flossing (26, 36) were also performed, although with a much lower frequency. While some caregivers confirmed that the necessary materials to provide oral health care were available in the facilities (29, 30, 33, 46), others expressed concern about the lack of resources, such as toothbrushes (18, 25, 32). The heterogeneity of practice across studies and settings further complicates the interpretation of findings, as some studies reported caregivers performing multiple oral health tasks. In contrast, others focused primarily on brushing or denture care.
Access to oral health care by an oral health professional was assessed in 14 of the included studies (14, 15, 17, 18, 24, 30, 31, 35–37, 39, 40, 42). Most staff support the availability of dental chairs or an on-site dentist with portable dental units and regular visits by oral health professionals (31, 35, 37, 39). However, home visits are not followed up and regular check-ups in nursing homes are rare (17, 40). Access to emergency care is a challenge, with reliance on local dentists and delays (36, 48). Only one study mentioned regular oral health campaigns, where a dentist goes to the home care facility to examine the older adult (30). These variations highlight the contextual of care provision and the need for more robust infrastructure and support for carers in many settings.
4 Discussion
4.1 Summary of main findings
This systematic review provides an in-depth analysis of the oral health care challenges that carers of dependent older adults, face. It highlights several key issues: the gap between education and practice, the persistence of barriers to adequate oral health care, and lack of health literacy among carers. The reviewed studies show that although carers recognize the importance of oral health and its link to systemic health, their ability to provide adequate care is often troubled by insufficient formal training, inadequate resources, and organizational challenges. Caregivers were primarily involved in brushing teeth and cleaning dentures but were less likely to perform more complex oral health tasks. Furthermore, despite these challenges, carers demonstrated a strong awareness of the need for oral care in older people, although their knowledge of oral health practices and conditions remained limited.
Results from studies using the Nursing Dental Coping Belief Scale (NDCBS) show a significant discrepancy between carers’ beliefs about their competence to provide oral care and the actual practices observed. Experienced carers often reported facing more challenges, possibly due to burnout or a mismatch between training and the demands of caring. The barriers identified across studies can be categorized into resident, organizational, and carer-related factors, each contributing to suboptimal oral health care.
4.2 Implications for practice and research
The included studies showed that oral health care practices for dependent older adults are still inadequate, insufficient, and unsystematic. Although guidelines for appropriate oral health care exist (56, 57), training in oral and prosthetic hygiene has been shown to have a positive impact, and various oral health training programs for care providers working in geriatric settings have been described in the literature (58–62). However, a systematic review of strategies to improve oral health care showed that there is still a need to improve the strategies used to change oral health care behaviors, as providing general information seems to be successful in increasing oral health knowledge but does not necessarily improve oral health (63). In addition, another systematic review (64) showed that oral health education programs may indeed have a positive effect on oral hygiene in the older adult, although some limitations of the included studies were noted.
Therefore, caregivers need structured training programs that improve their knowledge and equip them with the skills and resources to effectively perform daily oral health tasks. Training programs can be more effective if they are tailored to the specific needs of caregivers in different settings and focus on practical training. In addition, such training should be regularly updated to reflect advances in oral health care for older people and integrated into the routine activities of nursing homes and care facilities. Dental professionals must actively participate in training and provide ongoing support, as this significantly improves caregivers’ confidence and competence in delivering oral health care.
In addition, the financial burden of dental care for nursing home residents remains a significant issue. Oral health care is often excluded from public health coverage, leaving residents to pay for treatment. This factor contributes to the neglect of oral health and increases the risk of significant oral disease. We must implement policy changes to integrate dental care into the broader health care framework for older people and provide financial support to reduce out-of-pocket costs for residents.
4.3 Strengths and limitations
This systematic review was conducted according to PRISMA, a rigorous and widely recommended guideline that increases robustness and reduces reporting errors. In addition, an extensive literature search was conducted using a meticulous predefined protocol.
However, there are some limitations that need to be discussed. Most studies used a convenience sample of nursing homes in the study area, so the results may have been different if the other facilities had been included in the studies. In addition, only a few health care professionals from each sample site participated in the surveys. As a result, the small sample size limits the ability to extrapolate the data to the rest of the population and the ability to detect small differences between groups as statistically significant. Another limitation is the reliance on self-reported data, particularly from questionnaires and interviews, which can introduce various forms of bias. Carers may be motivated to give socially desirable answers, overestimating their level of training or the quality of care they provide. Recall bias is also a concern, as caregivers may have difficulty accurately recalling specific events or practices related to oral health care. In addition, the heterogeneity of the studies—ranging from differences in data collection methods (e.g., questionnaires vs. interviews) to differences in study populations (e.g., type of caregiver, setting, geographic location)—makes it difficult to draw firm conclusions about the generalisability of the findings. The lack of standardized measurement tools across studies makes it difficult to compare results, especially for complex constructs such as oral health knowledge and caregiver self-efficacy.
Future studies should focus on data representativeness and method standardization to ensure more homogeneous evidence-based results. The NDCBS is a standardized assessment tool that should be widely used. This information is extremely important for improving the oral health of nursing home residents and, consequently, their well-being and systemic health. It is also important for educating nursing home administrators about the improvements that can be made in oral health care.
4.4 Recommendations for overcoming barriers
The findings of this review support the proposal of several actionable strategies to address the barriers to providing oral health care for older adults:
1. Standardize training programs: Institutions can formalize nursing training, incorporating hands-on sessions that focus on practical aspects of oral health care, especially for non-dental professionals. These programs should be integrated into nurses’ induction processes and continuing education initiatives, ensuring they acquire and maintain up-to-date knowledge and skills.
2. Improve access to resources: Facilities can ensure the availability of adequate oral health supplies, including toothbrushes, denture care products, and other essential materials. Regular efforts are needed to maintain the accessibility and readiness of these resources for staff use.
3. Policy changes for financial support: Governments and health systems can extend dental care coverage for older people in long-term care facilities. This may involve incorporating dental services into existing health programs or creating separate funding for dental care for the older adult.
4. Regular monitoring and support: Ongoing support from dental professionals should be integrated into the care routine for older residents, ensuring that carers have access to advice when needed. In addition, regular monitoring of oral health outcomes should be implemented to identify problems early and improve the overall quality of care.
5 Conclusion
This review highlights the multiple barriers to oral health care for dependent older adults, including time constraints, lack of training, inadequate resources, and poor collaboration among caregivers. In particular, caregiver training programs are often informal and experiential, while oral health literacy remains low, creating a critical gap in their ability to provide adequate care. The included studies’ methodological limitations, such as reliance on self-reported data and lack of standardized measures, highlight the need for more robust and standardized research designs.
To address these challenges does not appear to be modifying the subject structured, evidence-based training programs for caregivers. These programs should be comprehensive, combine theoretical knowledge with practical skills, and directly address the barriers identified in this review. In addition, systemic changes are needed to ensure that older adult residents have financial access to dental care, often a significant barrier to optimal care.
Future research should focus on overcoming the limitations of current studies by standardizing data collection methods and using validated instruments, such as the NDCBS, to ensure greater comparability between studies. Longitudinal studies or randomized controlled trials are essential to assess the effectiveness of different educational programs and interventions in improving oral health knowledge and clinical outcomes in older populations.
Researchers must investigate the cost-effectiveness of integrating oral health care into long-term care and develop strategies to incentivize dental professionals to participate in routine care. They should also analyze the benefits of interdisciplinary care models that include nurses and dental professionals and evaluate how policy changes can improve access to dental care for older adults, especially in regions with limited public dental coverage.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
JP-L: Conceptualization, Formal analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. IR: Conceptualization, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. JC: Conceptualization, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. AG: Conceptualization, Investigation, Writing – original draft, Writing – review & editing. JF: Conceptualization, Supervision, Writing – original draft, Writing – review & editing. JG-E: Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Gen AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1504542/full#supplementary-material
References
1. United Nations. World Population Ageing 2020 Highlights: living arrangements of older persons. New York: United Nations (2020).
2. World Health Organization. Global health and aging [Internet]; (2011) Available at: http://www.who.int/ageing/publications/global_health/en/ (accessed December 1, 2023)
3. Petersen, PE, Kandelman, D, Arpin, S, and Ogawa, H. Global oral health of older people--call for public health action. Community Dent Health. (2010) 27:257–67.
4. Bryan, S, Afful, J, Carroll, M, Te-Ching, C, Orlando, D, Fink, S, et al. NHSR 158. National Health and nutrition examination survey 2017–march 2020 pre-pandemic data files [Internet]. National Center for Health Statistics (U.S.); (2021). Available at: https://stacks.cdc.gov/view/cdc/106273 (Accessed March 11, 2024).
5. Raphael, C. Oral health and aging. Am J Public Health. (2017) 107:S44–5. doi: 10.2105/AJPH.2017.303835
6. Chalmers, JM, Carter, KD, and Spencer, AJ. Caries incidence and increments in community-living older adults with and without dementia. Gerodontology. (2002) 19:80–94. doi: 10.1111/j.1741-2358.2002.00080.x
7. Adegbembo, AO, Leake, JL, Main, PA, Lawrence, HL, and Chipman, ML. The effect of dental insurance on the ranking of dental treatment needs in older residents of Durham Region’s homes for the aged. J Can Dent Assoc. (2002) 68:412.
8. Matthews, DC, Clovis, JB, Brillant, MGS, Filiaggi, MJ, McNally, ME, Kotzer, RD, et al. Oral health status of long-term care residents-a vulnerable population. J Can Dent Assoc. (2012) 78:c3
9. Porter, J, Ntouva, A, Read, A, Murdoch, M, Ola, D, and Tsakos, G. The impact of oral health on the quality of life of nursing home residents. Health Qual Life Outcomes. (2015) 13:102. doi: 10.1186/s12955-015-0300-y
10. Haumschild, MS, and Haumschild, RJ. The importance of oral health in long-term care. J Am Med Dir Assoc. (2009) 10:667–71. doi: 10.1016/j.jamda.2009.01.002
11. Emami, E, De Souza, RF, Kabawat, M, and Feine, JS. The impact of edentulism on oral and general health. Int J Dent. (2013) 2013:1–7. doi: 10.1155/2013/498305
12. Azarpazhooh, A, and Tenenbaum, HC. Separating fact from fiction: use of high-level evidence from research syntheses to identify diseases and disorders associated with periodontal disease. J Can Dent Assoc. (2012) 78:c25
13. Zhang, H, and Sun, H. Knowledge, attitude and self-efficacy of elderly caregivers in Chinese nursing homes: a cross-sectional study in Liaoning Province. BMJ Open. (2019) 9:e029869. doi: 10.1136/bmjopen-2019-029869
14. Ho, SY, Walsh, LJ, Pradhan, A, Yang, J, Chan, PY, and Lopez Silva, CP. Interprofessional collaboration utilizing oral health therapists in nursing homes: perceptions of oral health therapists and nursing home staff in Singapore. Spec Care Dentist. (2023) 43:795–805. doi: 10.1111/scd.12765
15. Hiltunen, K, Fogelholm, N, Saarela, RKT, and Mäntylä, P. Survey of health care personnel’s attitudes toward oral hygiene in long-term care facilities in Finland. Spec Care Dentist. (2019) 39:557–63. doi: 10.1111/scd.12424
16. Sumi, Y, Nakamura, Y, Nagaosa, S, Michiwaki, Y, and Nagaya, M. Attitudes to oral care among caregivers in Japanese nursing homes. Gerodontology. (2001) 18:2–6. doi: 10.1111/j.1741-2358.2001.00002.x
17. Paley, GA, Slack-Smith, LM, and O’Grady, MJ. Aged care staff perspectives on oral care for residents: Western Australia. Gerodontology. (2004) 21:146–54. doi: 10.1111/j.1741-2358.2004.00020.x
18. Weening-Verbree, LF, Schuller, AA, Cheung, SL, Zuidema, SU, Van Der Schans, CP, and JSM, H. Barriers and facilitators of oral health care experienced by nursing home staff. Geriatr Nur (Lond). (2021) 42:799–805. doi: 10.1016/j.gerinurse.2021.04.012
19. Ferguson, CA, Thomson, WM, Smith, MB, Kerse, N, Peri, K, and Gribben, B. Medication taking in a national sample of dependent older people. Res Soc Adm Pharm. (2020) 16:299–307. doi: 10.1016/j.sapharm.2019.05.010
20. Wong, FMF, Ng, YTY, and Leung, WK. Oral health and its associated factors among older institutionalized residents—a systematic review. Int J Environ Res Public Health. (2019) 16:4132. doi: 10.3390/ijerph16214132
21. Wells, G, Shea, B, O’Connell, D, Peterson, J, Welch, V, Losos, M, et al. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses [Internet]. (2021) Available at: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (Accessed March 11, 2024)
22. Landis, JR, and Koch, GG. The measurement of observer agreement for categorical data. Biometrics. (1977) 33:159–74. doi: 10.2307/2529310
23. Ballikaya, E, Ergin, E, Turgut, MD, Güçiz Doğan, B, and Uzamış Tekçiçek, M. Oral health related knowledge, practices and opinions of caregivers at the biggest care home for people with disability in Turkey. Meandros Med Dent J. (2021) 22:94–101. doi: 10.4274/meandros.galenos.2021.15870
24. De Mello, ALSF, and Padilha, DMP. Oral health care in private and small long-term care facilities: a qualitative study. Gerodontology. (2009) 26:53–7. doi: 10.1111/j.1741-2358.2008.00238.x
25. Frenkel, HF. Behind the screens: care staff observations on delivery of oral health care in nursing homes. Gerodontology. (1999) 16:75–80. doi: 10.1111/j.1741-2358.1999.00075.x
26. Garrido Urrutia, C, Romo Ormazábal, F, Espinoza Santander, I, and Medics Salvo, D. Oral health practices and beliefs among caregivers of the dependent elderly. Gerodontology [Internet]. (2012) 29:e742–7. doi: 10.1111/j.1741-2358.2011.00553.x
27. Godoy, J, Rosales, E, and Garrido-Urrutia, C. Creencias relacionadas al cuidado de la salud oral en cuidadores de adultos mayores institucionalizados de la ciudad de Antofagasta, Chile 2019. Odontoestomatología [Internet]. (2021); p. 38. Available at: https://odon.edu.uy/ojs/index.php/ode/article/view/366
28. Goh, CE, Guay, MP, Lim, MY, Lim, SM, Loke, SY, Toh, HE, et al. Correlates of attitudes and perceived behavioural control towards oral care provision among trained and untrained nursing home caregivers in Singapore. J Clin Nurs. (2016) 25:1624–33. doi: 10.1111/jocn.13162
29. Junges, R, Portella, FF, Hugo, FN, Padilha, DMP, and Samuel, SMW. Caregivers’ attitudes regarding oral health in a long-term care institution in Brazil. Gerodontology. (2014) 31:178–83. doi: 10.1111/ger.12019
30. Reis, SCGB, Marcelo, VC, Da Silva, ET, and Leles, CR. Oral health of institutionalised elderly: a qualitative study of health caregivers’ perceptions in Brazil: caregivers’ perception of elderly oral health. Gerodontology. (2011) 28:69–75. doi: 10.1111/j.1741-2358.2010.00366.x
31. Rovida, TAS, Peruchini, LFD, Moimaz, SAS, and Garbin, SAS. The meaning of general and oral health on the elderly caregiver’s view. Odontol Clín-Cient. (2013) 12:43–6.
32. Stančić, I, Petrovic, M, Popovac, A, Vasovic, M, and Despotovic, N. Caregivers’ attitudes, knowledge and practices of oral care at nursing homes in Serbia. Vojnosanit Pregl. (2016) 73:668–73. doi: 10.2298/VSP141001065S
33. Unfer, B, Braun, KO, De Oliveira Ferreira, AC, Ruat, GR, and Batista, AK. Challenges and barriers to quality oral care as perceived by caregivers in long-stay institutions in Brazil. Gerodontology [Internet]. (2012) 29:e324–e330. doi: 10.1111/j.1741-2358.2011.00475.x
34. Vieira, JC, Massoni, ACLT, de Morais Freitas, CHS, Marinho, FB, and da Costa, CHM. A look at the elderly caregivers of the geriatric institutions of joão Pessoa, paraíba: profile and oral health care for the elderly. Rev Baiana Saúde Pública. (2011) 35:604–18.
35. Villarosa, AR, Clark, S, Villarosa, AC, Patterson Norrie, T, Macdonald, S, Anlezark, J, et al. Promoting oral health care among people living in residential aged care facilities: perceptions of care staff. Gerodontology. (2018) 35:177–84. doi: 10.1111/ger.12336
36. Webb, BC, Whittle, T, and Schwarz, E. Provision of dental care in aged care facilities NSW Australia- part 2 as perceived by the carers (care providers). Gerodontology. (2015) 32:254–9. doi: 10.1111/ger.12103
37. Wilk, A, LaSpina, L, Boyd, LD, and Vineyard, J. Perceived Oral health literacy, behaviors, and oral health care among caregivers to the homebound population. Home Health Care Manag Pract. (2021) 33:280–7. doi: 10.1177/10848223211008435
38. Palmers, E, Janssens, L, Phlypo, I, Vanhaecht, K, De Almeida, MJ, De Visschere, L, et al. Perceptions on Oral care needs, barriers, and practices among managers and staff in long-term care settings for older people in Flanders, Belgium: a cross-sectional survey. Innov Aging. (2022) 6:igac046. doi: 10.1093/geroni/igac046
39. Chung, J, Dent, M, Mojon, P, Budtz-Jørgensen, E, and Odont,. Dental care of elderly in nursing homes: perceptions of managers, nurses, and physicians. Spec Care Dentist. (2000) 20:12–7. doi: 10.1111/j.1754-4505.2000.tb00004.x
40. Wårdh, I, Hallberg, LRM, Berggren, U, Andersson, L, and Sörensen, S. Oral health care-a low priority in nursing: in-depth interviews with nursing staff. Scand J Caring Sci. (2000) 14:137–42. doi: 10.1111/j.1471-6712.2000.tb00574.x
41. Chebib, N, Waldburger, TC, Boire, S, Prendki, V, Maniewicz, S, Philippe, M, et al. Oral care knowledge, attitude and practice: caregivers’ survey and observation. Gerodontology. (2021) 38:95–103. doi: 10.1111/ger.12502
42. Catteau, C, Piaton, S, Nicolas, E, Hennequin, M, and Lassauzay, C. Assessment of the oral health knowledge of health care providers in geriatric nursing homes: additional training needs required. Gerodontology. (2016) 33:11–9. doi: 10.1111/ger.12094
43. Cheng, YM, Ping, CC, Ho, CS, Lan, SJ, and Hsieh, YP. Home-care aides’ self-perception of oral health care provision competency for community-dwelling older people. Int Dent J. (2019) 69:158–64. doi: 10.1111/idj.12417
44. Forsell, M, Sjögren, P, Kullberg, E, Johansson, O, Wedel, P, Herbst, B, et al. Attitudes and perceptions towards oral hygiene tasks among geriatric nursing home staff: attitudes towards oral hygiene tasks. Int J Dent Hyg. (2011) 9:199–203. doi: 10.1111/j.1601-5037.2010.00477.x
45. Kohli, R, Nelson, S, Ulrich, S, Finch, T, Hall, K, and Schwarz, E. Dental care practices and oral health training for professional caregivers in long-term care facilities: an interdisciplinary approach to address oral health disparities. Geriatr Nur (Lond). (2017) 38:296–301. doi: 10.1016/j.gerinurse.2016.11.008
46. Sigurdardottir, AS, Geirsdottir, OG, Ramel, A, and Arnadottir, IB. Cross-sectional study of oral health care service, oral health beliefs and oral health care education of caregivers in nursing homes. Geriatr Nur (Lond). (2022) 43:138–45. doi: 10.1016/j.gerinurse.2021.11.010
47. Wårdh, I, Jonsson, M, and Wikström, M. Attitudes to and knowledge about oral health care among nursing home personnel – an area in need of improvement. Gerodontology [Internet]. (2012) 29:e787–92. doi: 10.1111/j.1741-2358.2011.00562.x
48. Webb, BC, Whittle, T, and Schwarz, E. Provision of dental care in aged care facilities, NSW, Australia – part 1 as perceived by the directors of nursing (care providers). Gerodontology. (2013) 30:226–31. doi: 10.1111/j.1741-2358.2012.00670.x
49. Willumsen, T, Karlsen, L, Næss, R, and Bjørntvedt, S. Are the barriers to good oral hygiene in nursing homes within the nurses or the patients? Gerodontology [Internet]. (2012) 29:e748–e755. doi: 10.1111/j.1741-2358.2011.00554.x
50. Edman, K, and Wårdh, I. Oral health care beliefs among care personnel working with older people – follow-up of oral care education provided by dental hygienists. Int J Dent Hyg. (2022) 20:241–8. doi: 10.1111/idh.12588
51. Castillo, LO, Braz, MA, Seehaber, KA, Botega, DM, Frasca, LCF, and Rivaldo, EG. Influência da qualificação de cuidadores na saúde bucal de idosos dependentes de Santa Maria/RS, Brasil (2018), p. 24.
52. Delgado, AM, Prihoda, T, Nguyen, C, Hicks, B, Smiley, L, and Taverna, M. Professional caregivers’ Oral care practices and beliefs for elderly clients aging in place. J Dent Hyg. (2016) 90:244–8.
53. Hardy, DL, Darby, ML, Leinbach, RM, and Welliver, MR. Self-report of oral health services provided by nurses’ aides in nursing homes. Dent Hyg. (1995) 69:75–82.
54. Wolfe, GR, Stewart, JE, and Hartz, GW. Relationship of dental coping beliefs and oral hygiene. Community Dent Oral Epidemiol. (1991) 19:112–5. doi: 10.1111/j.1600-0528.1991.tb00123.x
55. Wårdh, I, and Sörensen, S. Development of an index to measure oral health care priority among nursing staff. Gerodontology. (2005) 22:84–90. doi: 10.1111/j.1741-2358.2005.00063.x
56. Ministry of Health (Singapore). MOH nursing clinical practice guidelines 1/2004. Nursing Management of Oral Hygiene [Internet]; (2004). Available at: https://www.moh.gov.sg/docs/librariesprovider4/guidelines/nursing_management_of_oral_hygiene.pdf (Accessed March 11, 2024).
57. Fiske, J, Griffiths, J, Jamieson, R, and Manger, D. Guidelines for Oral health Care for Long-stay Patients and Residents. Gerodontology. (2000) 17:55–64. doi: 10.1111/j.1741-2358.2000.00055.x
58. Mynors-Wallis, J, and Davis, DM. An assessment of the oral health knowledge and recall after a dental talk amongst nurses working with elderly patients: a pilot study*. Gerodontology. (2004) 21:201–4. doi: 10.1111/j.1741-2358.2004.00036.x
59. Kullberg, E, Forsell, M, Wedel, P, Sjögren, P, Johansson, O, Herbst, B, et al. Dental hygiene education for nursing staff. Geriatr Nur (Lond). (2009) 30:329–33. doi: 10.1016/j.gerinurse.2009.06.009
60. Peltola, P, Vehkalahti, MM, and Simoila, R. Effects of 11-month interventions on oral cleanliness among the long-term hospitalised elderly. Gerodontology. (2007) 24:14–21. doi: 10.1111/j.1741-2358.2007.00147.x
61. Frenkel, H, Harvey, I, and Newcombe, RG. Improving oral health in institutionalised elderly people by educating caregivers: a randomised controlled trial. Community Dent Oral Epidemiol. (2001) 29:289–97. doi: 10.1034/j.1600-0528.2001.290408.x
62. Nicol, R, Petrina Sweeney, M, McHugh, S, and Bagg, J. Effectiveness of health care worker training on the oral health of elderly residents of nursing homes. Community Dent Oral Epidemiol. (2005) 33:115–24. doi: 10.1111/j.1600-0528.2004.00212.x
63. Weening-Verbree, L, Huisman-de Waal, G, Van Dusseldorp, L, Van Achterberg, T, and Schoonhoven, L. Oral health care in older people in long term care facilities: a systematic review of implementation strategies. Int J Nurs Stud. (2013) 50:569–82. doi: 10.1016/j.ijnurstu.2012.12.004
Keywords: institutionalized older adult, nursing home, nurse, caregiver, health care, oral health
Citation: Pombo-Lopes J, Rodrigues I, Costa J, Gomes AC, Fonseca J and Grillo-Evangelista J (2025) Health professionals’ perceptions, barriers and knowledge towards oral health care of dependent people in nursing homes: a systematic review. Front. Public Health. 12:1504542. doi: 10.3389/fpubh.2024.1504542
Edited by:
Wei-Chen Lee, University of Texas Medical Branch at Galveston, United StatesReviewed by:
Soraya León, University of Talca, ChileAna Paula Macedo, University of Minho, Portugal
Copyright © 2025 Pombo-Lopes, Rodrigues, Costa, Gomes, Fonseca and Grillo-Evangelista. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joana Pombo-Lopes, am1sb3Blc0BlZ2FzbW9uaXouZWR1LnB0
†Present Address: Joana Pombo-Lopes Aging Lab, Egas Moniz School of Health & Science, Egas Moniz Center for Interdisciplinary Research (CiiEM), Almada, Portugal