
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 18 December 2024
Sec. Aging and Public Health
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1470035
This article is part of the Research Topic Analyses on Health Status and Care Needs among Older Adults View all 40 articles
 Medha N. Munshi1
Medha N. Munshi1 Elizabeth M. Venditti2
Elizabeth M. Venditti2 Ashley H. Tjaden3William C. Knowler4
Ashley H. Tjaden3William C. Knowler4 Edward J. Boyko5
Edward J. Boyko5 Roeland J. W. Middelbeek1
Roeland J. W. Middelbeek1 José A. Luchsinger6Christine G. Lee7Helen P. Hazuda8Marcel E. Salive9Sharon L. Edelstein3
José A. Luchsinger6Christine G. Lee7Helen P. Hazuda8Marcel E. Salive9Sharon L. Edelstein3 Thomas W. Storer10 on behalf of the Diabetes Prevention Program Research Group*
Thomas W. Storer10 on behalf of the Diabetes Prevention Program Research Group*Objectives: Type 2 diabetes (T2D) and prediabetes are associated with poor walking endurance, a marker of physical function. We aimed to examine the long-term effects of metformin or intensive lifestyle intervention in adults at high risk of T2D on their 6-min walk test (6MWT) performance.
Methods: Participants were randomized in the 3-year Diabetes Prevention Program (DPP) to one of the three groups: lifestyle intervention, metformin, or placebo, and were subsequently followed in the DPP Outcomes Study. A 6MWT was conducted 20 years after randomization. Associations between DPP interventions and 6MWT completion (achieving a distance ≥200 m) were assessed using logistic regression. Among the test completers, differences in distance walked (6MWD) were evaluated using multivariable linear regression. Additional variables of interest included concomitant measures of body mass index (BMI) and grip strength along with mean measures of HbA1c and self-reported physical activity (PA).
Results: Data on 1830 participants were analyzed. The interventions were not associated with test completion or the 6MWD among test completers (362, 364, and 360 m in the lifestyle, metformin, and placebo groups, respectively, p = 0.8). Age, education, grip strength, and PA were each significantly associated with the 6MWT completion and the 6MWD after adjustment. Grip strength, PA, and education were positively associated with the 6MWD, while age, BMI, and HbA1c were negatively associated with the 6MWD.
Conclusion: We confirmed that the 6MWT is related to other measures of physical ability such as PA and grip strength in persons at risk for and with T2D, suggesting potential long-term benefits of maintaining a healthy lifestyle. However, we did not observe a sustained effect of the original randomized interventions.
Clinical trial registration: http://www.clinicaltrials.gov/ct/show/NCT00004992, identifier DPP NCT00004992; http://www.clinicaltrials.gov/ct/show/NCT00038727, identifier DPPOS NCT00038727
Both prediabetes and type 2 diabetes mellitus (T2D) are independently associated with reduced physical activity and a higher risk of disability (1–9). Physical fitness, including cardiopulmonary endurance and skeletal muscle strength and power, are important health-related attributes for mitigating disability in older people. Disability in the form of mobility limitation is associated with functional decline (10, 11) and loss of independence among older adults (10, 12). Assessed by walking speed, impaired mobility is well associated with disability in activities of daily living (11, 12), cardiovascular disease, and mortality (13, 14). Mobility, in the context of physical activity, is well-known as a positive determinant of mental health that is associated with psychological (15, 16) and social wellbeing (17, 18).
The 6-min walk test (6MWT) measures how far a person can walk in 6 min under standardized conditions. Since the test is submaximal, it may better indicate an individual’s ability to perform activities of daily living than maximal exercise testing (19). The test is clinically validated to objectively evaluate endurance in older adults (20). The total distance walked in the 6MWT (6MWD) diminishes with greater age, poor overall health status, T2D, a low score on cognitive function tests, and a high C-reactive protein concentration. The 6MWT is also associated with all-cause mortality (21–24). The majority of studies evaluating 6MWT performance are conducted on individuals with heart, lung, or neuromuscular diseases, who are often older adults. Although T2D is a known risk factor for poorer performance on the 6MWT, the effects of diabetes prevention interventions on the 6MWT performance among adults at risk for diabetes are not well-known.
The effect of metformin use on physical functioning has shown mixed results, with benefits shown on some parameters of exercise capacity, including VO2peak, which is associated with 6MWT performance (25–27). An epidemiological study in women with T2D suggested a beneficial effect of insulin sensitizers, particularly metformin, on preventing the loss in gait speed seen with aging (28). It is unclear whether longer-term metformin use affects physical endurance as measured by the 6MWT. Moreover, these previous studies examined individuals with T2D; thus, it is not known how metformin or multicomponent lifestyle interventions aimed at improving eating habits, increasing physical activity, and producing modest weight loss over time, may affect longer-term physical performance in individuals at high risk of T2D.
The Diabetes Prevention Program Outcomes Study (DPPOS) is a long-term follow-up of the Diabetes Prevention Program (DPP). The DPP evaluated the role of metformin and an intensive lifestyle intervention (ILS) in preventing or delaying the onset of T2D in high-risk adults. Data from longer follow-ups in DPPOS showed a sustained impact of interventions administered during the DPP on frailty (29). The goal of this analysis was to determine the effects of treatment with metformin or ILS, compared to placebo, on walking endurance as measured using the 6MWT as part of the long-term follow-up in DPPOS participants. Understanding the effects of metformin therapy and ILS on walk performance may help to prevent frailty and loss of mobility in older adults with or at risk for T2D.
The DPP (July 1996 to July 2001) was a 27-center randomized controlled trial that compared the efficacy of metformin or ILS with placebo to prevent or delay T2D among 3,234 adults aged ≥25 years old who were overweight or obese and had prediabetes at baseline (30–32). ILS participants were offered an individualized 16-lesson curriculum over 24 weeks followed by monthly sessions through the DPP. The curriculum focused on diet, exercise, and behavior change, guiding participants to follow a low-fat, low-calorie diet (<25% kcal from fat) and perform ≥150 min/week of physical activity, with the primary goal to achieve ≥7% weight loss from baseline weight (33). Metformin participants were assigned to take blinded 850 g metformin twice daily; placebo participants were assigned a matching placebo pill twice daily. Both the metformin and placebo groups received written standard lifestyle recommendations and a one-on-one lifestyle session annually. After the DPP ended, the metformin and placebo groups were unmasked, and all participants were offered a modified lifestyle program for 6 months. Subsequently, 2,779 participants consented to participate in the DPP Outcomes Study (DPPOS), and all participants were offered quarterly lifestyle classes. Open-label metformin was continued for those originally randomized to metformin, placebo was discontinued, and ILS was provided as semi-annual group-based classes (34).
The study protocols for DPP/DPPOS are publicly available at https://dppos.bsc.gwu.edu/web/dppos/dpp.
This analysis was limited to those DPP/DPPOS participants who completed a 6MWT eligibility assessment at their DPPOS Year 15 (calendar years 2016–2017) follow-up visit (19–21 years after randomization).
Study coordinators and lead examiners at each DPPOS site completed centralized in-person training and practice in 6MWT administration until proficiency was achieved. One of the authors (TWS) with extensive 6MWT expertise served as the master trainer (35). All training materials were developed from published, standardized guidelines (19). A performance checklist (Supplementary Material) was developed to ensure the ability of 6MWT assessors to proficiently administer the test and to train new examiners at individual study sites.
Twenty of the twenty-four sites that participated in the 6MWT examination used a course length of 20 m; the remaining sites used 10-m courses because of space constraints. Turn-around zones of 2.5 m at each end were provided on all courses. The courses were measured either with a non-distensible tape measure or a measuring wheel; a hand-held stopwatch was used to monitor and record the actual time walked. Clinic staff were instructed to administer the test indoors along a long, flat, straight, enclosed corridor with a hard surface that is seldom traveled. In one clinic with a year-round temperate climate, the 6MWT was administered outdoors.
The 6MWT was first assessed at the DPPOS Year 15 follow-up visit (19–21 years after randomization). Participants rested in a seated position for 5 min before the start of the test. Heart rate and blood pressure were measured along with a brief assessment of contraindications. Participants were not permitted to warm up and only one test was given. Test administrators demonstrated one lap of the walk test and used the same standardized script to instruct participants in the performance of the test (19). Participants were asked to “…walk as far as possible at a speed that you can maintain safely for 6 min.” Lengths were recorded on a score sheet throughout the test. Participants were allowed to use usual walking aids, such as canes or walkers, and stop and rest as necessary, and allowed to discontinue the test at any time. Standardized words of encouragement were given at the end of 1 to 5 min, and again at 5 min 45 s (19). The stopwatch was stopped at approximately 6 min, and a marker was placed at the toe of the foot striking the floor on the command stop. Participants were returned to a seated position for assessment of heart rate, RPE, and signs and symptoms. Participants completed the Borg 0–10 scale for rating of perceived exertion (RPE) after the test (36, 37).
Completed lengths were recorded and multiplied by the course length. Distance walked beyond the last complete length was added to the distance calculated from completed lengths, representing the distance walked in 6 min (6MWD). For participants with stopwatch times that exceeded 6 min, the total distance measured was interpolated to exactly 6 min. Participants with stopwatch times exceeding 7 min were excluded from analyses assessing the 6MWD.
Physical activity data were collected via the Modifiable Activity Questionnaire (MAQ) annually and the median of all available responses [median = 17; range = 4–19 observations per participant] between the DPP baseline and DPPOS Year 12 (3 years prior to the 6MWT) of metabolic equivalent (MET)-hours of leisure activity was used as a measure of habitual activity level (38–40). Diabetes at the concurrent visit was ascertained using ADA criteria as previously described (30, 41). A composite variable for neuropathy signs and symptoms was defined by signs present based on a monofilament test at the concurrent visit or symptoms from Michigan Neuropathy Screening Instrument (MNSI) at the DPPOS Year 13 visit (2 years prior to 6MWT). Participants self-reported recent (within the past 12 months) hospitalizations and falls, as well as ever having a hip replacement. Stroke, CHF (congestive heart failure), MI (myocardial infarction) was adjudicated by review of medical records by reviewers masked to treatment assignment. A composite health issue variable was created to combine recent hospitalization, history of hip replacement, history of stroke, CHF or MI, and recent falls. The FEV1/FVC ratio was collected using a spirometry test at the concurrent visit. Grip strength was assessed with a handheld dynamometer using standardized procedures at the concurrent visit. Total metformin exposure was defined as the number of years taking study or non-study metformin. Cumulative glycemic exposure is defined as the mean HbA1c for all available semi-annual and annual visits between the DPP baseline and the time of 6MWT assessment (median = 24, range = 9–39 visits).
Descriptive statistics were used to examine the characteristics of the study population at baseline and at the time of their DPPOS Year 15 follow-up visit, which occurred 19–21 years after randomization. The baseline characteristics in the analytic cohort were also compared to participants from the original randomized DPP cohort who did not complete the 6MWT. Comparisons between groups were computed using ANOVA for continuous variables and chi-squared tests for categorical variables. Participants with the shortest distance walked (<200 m) were categorized as poor performers (approximately the 10th percentile test completers). Among all participants in the analytic cohort, logistic regression models adjusted for randomization group, age, sex, and ethnicity were used to examine the association of select characteristics at baseline and at follow-up with the ability to complete the 6MWT (completion) with a distance of ≥200 m. Among all participants who completed the test (regardless of distance walked), the mean distance walked (m) was compared by participant characteristics.
General linear regression models were used to examine the differences in total 6MWD by randomization group, diabetes, cumulative glycemic exposure, cumulative metformin exposure, and concurrent BMI. Several possible confounders were identified a priori for the base multivariable linear regression model (Model 1) for the base multivariable linear regression model. Subsequent models included additional covariates identified in a stepwise manner as possible confounders if they were significantly associated with distance walked after adjustment for randomized assignment. Model 2 adds education and health-related variables including smoking, concurrent BMI, height, and waist circumference. Finally, Model 3 adds concurrent grip strength, habitual physical activity, the presence of neuropathy signs/symptoms at the time of assessment, the presence of a health issue, and cumulative glycemic exposure. Effect modification by age, sex, ethnicity, and diabetes was tested.
Of the 3,234 participants randomized in the DPP from 1996 to 1999, 2,130 completed their DPPOS Year 15 annual visit between July 2016 and November 2017 when the 6MWT was conducted. The analytic group assessed for 6MWT eligibility represents 1,830 (86%) of the 2,130 individuals who completed a DPPOS Year 15 visit (Supplementary Figure 1). Of these 1,830 participants, 1,697 (93%) completed the 6MWT. Three participants had stopwatch times that exceeded 7 min and were excluded from subsequent analyses. Thus, 1,830 participants were included in analyses with test completion as the outcome, and 1,694 participants were included in analyses with total distance walked in 6 min as the outcome. Supplementary Table 1 compares the baseline characteristics of participants included in these analyses with those not included among the originally randomized DPP cohort.
Participant characteristics at the DPP baseline and at the DPPOS Year 15 visit are shown in Table 1 for 1,830 participants. Percent and mean values of the majority of variables were similar among the three randomization groups at baseline. The only nominally significant (p < 0.05) difference among the randomization groups was for height, which was highest in the metformin group.
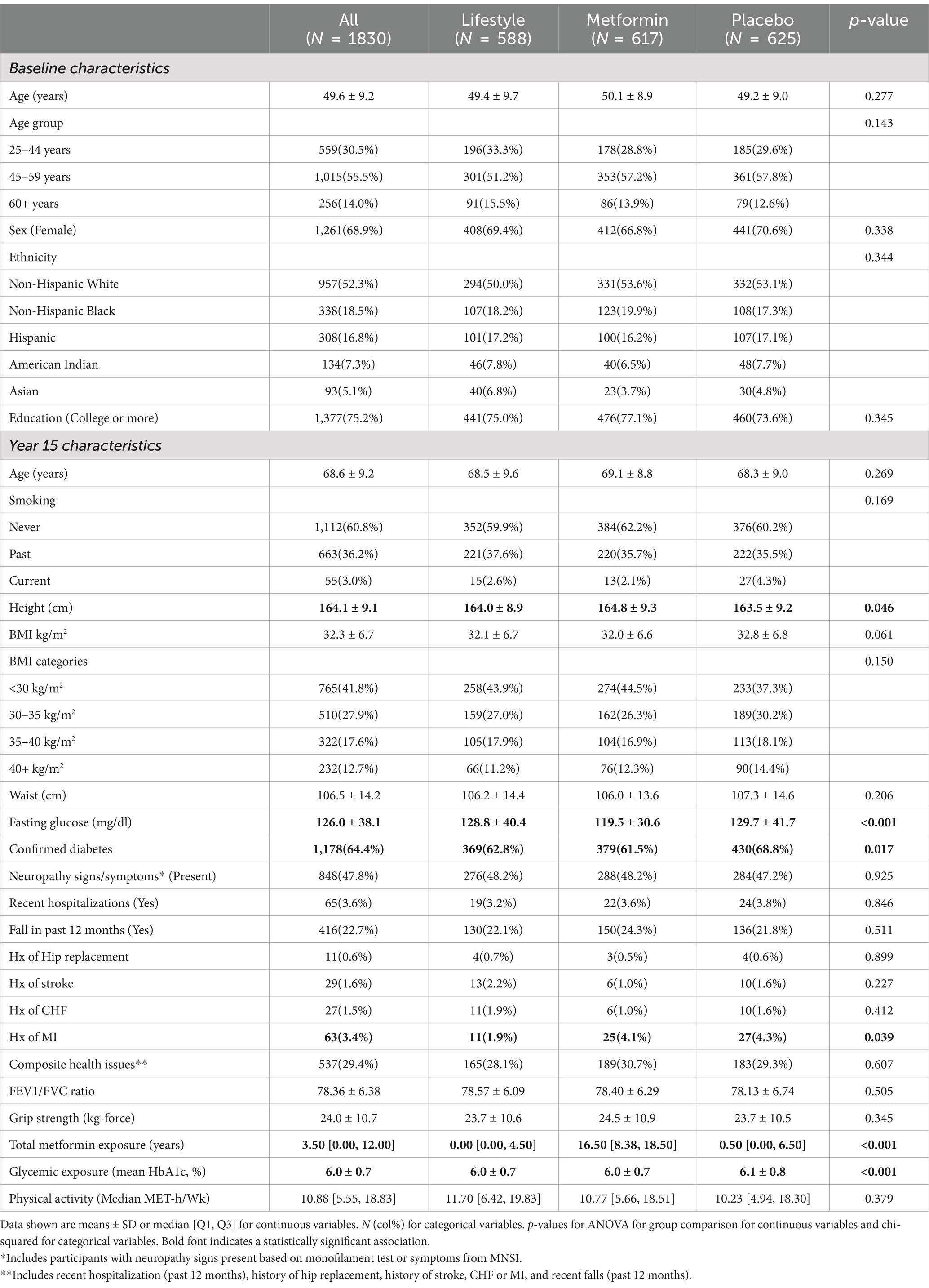
Table 1. Participant characteristics at DPPOS year 15 by treatment assignment group among all participants with a visit (N = 1830).
Because the interventions reduced the incidence of diabetes and its risk factors, diabetes, fasting glucose, and glycemic exposure differed between the randomization groups at the DPPOS Year 15, and were highest, on average, in the placebo group (Tables 1, 2). Diabetes had developed in 62.8% of lifestyle, 61.5% of metformin, and 68.5% of placebo participants. Other behaviors or health conditions potentially related to walking ability were not consistently or statistically significantly different across the DPP randomization groups. As a result of drug assignment in the randomized metformin group and use of metformin in all groups as a treatment for diabetes, the median metformin exposures by the DPPOS Year 15 were 0, 16.5, and 0.5 years in the lifestyle, metformin, and placebo groups, respectively.

Table 2. Variables associated with test completion and distance ≥200 m.
Reasons for the 6MWT ineligibility included dizziness, shortness of breath, chest pain, unstable angina, high or low heart rate or blood pressure, or participant feeling unsafe to attempt the test. Table 2 shows variables associated with participants who completed the test and variables associated with a composite measure of ability to complete the test and walk a distance ≥200 m. A model adjusted for age group, sex, ethnicity, and education, and a model adjusted for all other variables in the table is presented (Table 2). Of the 1,830 participants, 133 did not complete the test (103 ineligible and 30 started but did not complete), and an additional 167 participants completed the test but walked <200 m. The randomization group was not associated with 6MWT completion or the ability to both complete and walk a distance ≥200 m. In contrast, older age, non-Hispanic Black ethnicity, lack of college education, higher BMI category, higher waist circumference, signs and symptoms of neuropathy, and presence of a health issue were each associated with a lower likelihood of test completion in fully-adjusted logistic regression models. These same factors were also associated with a lower likelihood of both completing the 6MWT and walking a distance ≥200 m in fully-adjusted logistic regression models; however, a higher likelihood of this outcome was associated with American Indian ethnicity, greater grip strength, and higher median physical activity.
The primary outcome of this analysis was the distance (m) walked in 6 min (6MWD). Table 3 presents the unadjusted mean distance walked by participant characteristics. There were no differences in distance walked by the randomization group but there were differences in all other variables presented. Neither distance walked nor gait speed was different for participants undergoing testing at sites with 10-m or 20-m courses.
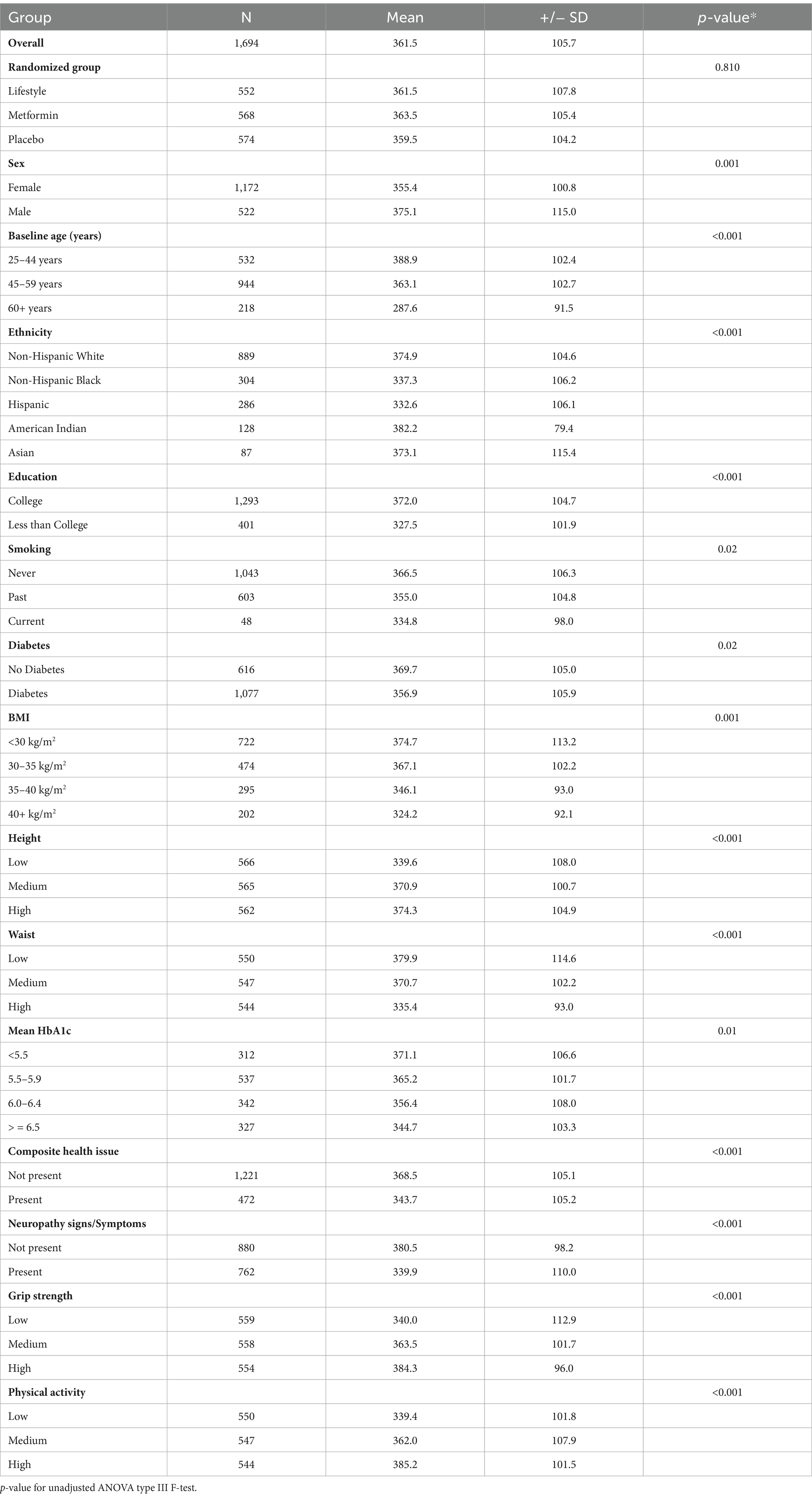
Table 3. Mean distance walked (m) by participant characteristics at DPPOS Year 15 among participants who completed the 6MWT (N = 1,694).
Multivariable models for associations with distance walked among those who completed the test (N = 1,694) are shown in Table 4. In all three models, there was no significant association between the randomization group with 6MWD, with the greatest differences between randomization groups of approximately 4 m (or approximately 1% of the overall mean distance of 361.5 m). No interactions between the randomization groups with sex, ethnicity, and age on walking distance were observed.
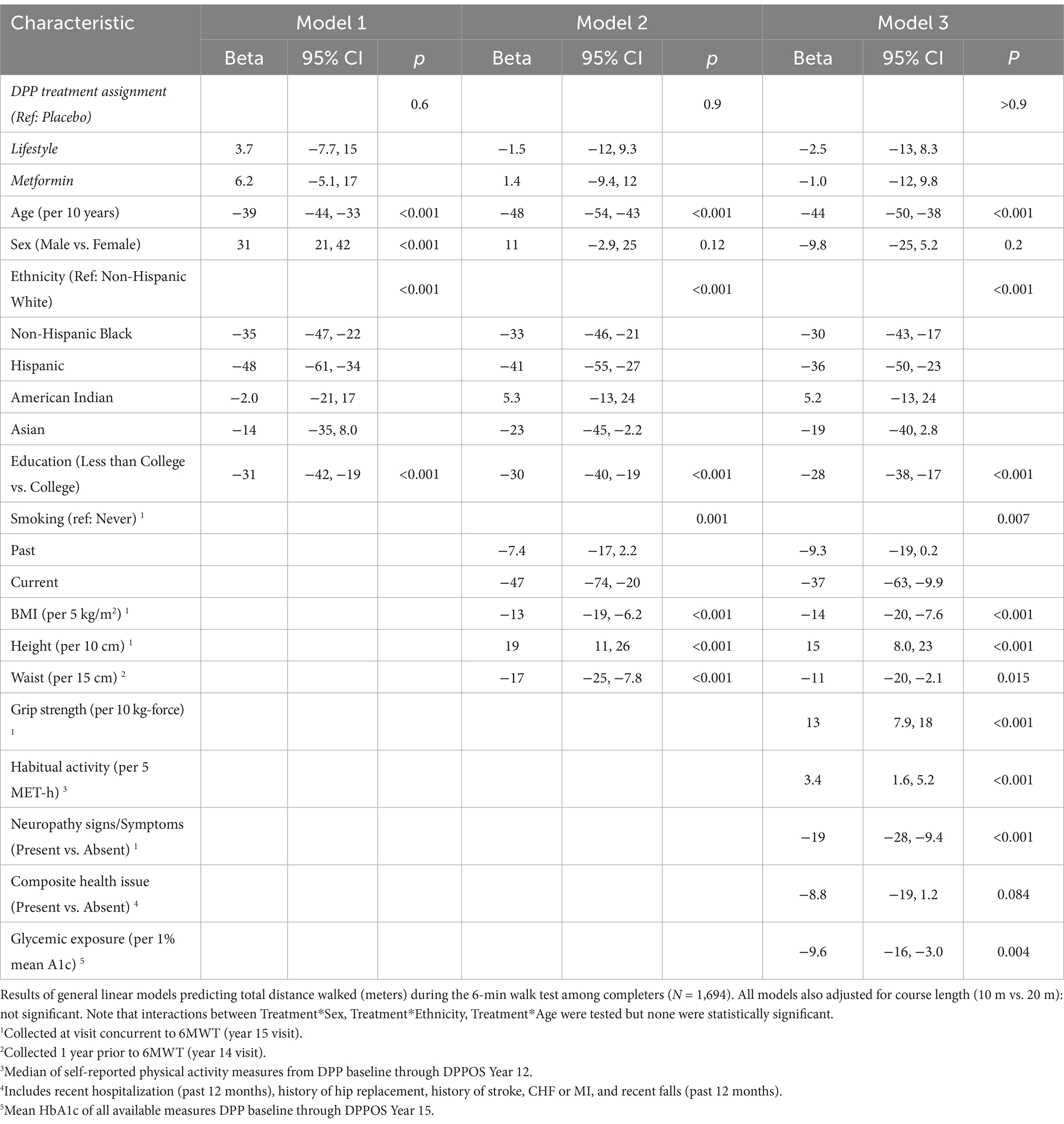
Table 4. Association of randomized treatment assignment and selected covariates with distance walked (m).
Supplementary Tables 2–6 present models evaluating associations of the 6MWD with diabetes, cumulative glycemic exposure, cumulative metformin exposure, BMI, and grip strength. There was no significant effect of concurrent diabetes after adjustment for adiposity, with further attenuation of the effect once adjusted for grip strength and physical activity. Cumulative glycemic exposure was significantly and inversely associated with 6MWD; each 1% increase in mean HbA1c was associated with a 9 m [95% CI -16, −2.5] lower walking distance. Cumulative metformin exposure had no significant association with the 6MWD. Concurrently measured BMI was inversely associated with the 6MWD with a 14 m [95% CI -20, −7.3] lower walking distance per 5 kg/m (2). Concurrently measured grip strength was positively associated with the 6MWD with a 13 m [95% CI 7.9, 18] greater walking distance per 10 kg force. In all models, age and education were inversely related to walking distance.
The distance walked in 6 min is a functional measure of mobility and walking endurance that decreases during the aging process, particularly in individuals with T2D. Both metformin and lifestyle interventions slow the progression of prediabetes to T2D, which may in turn impact walking endurance. In this study of DPPOS participants who were at risk of developing T2D, greater age and BMI negatively impacted walking endurance while physical activity and grip strength, a measure of muscle function, were positively associated with walking endurance. However, in this large cohort of participants followed longitudinally over 2 decades, there was no difference in walking endurance, as measured by the 6MWT, among those randomized to metformin, lifestyle, or placebo. Additionally, there was no association between cumulative metformin exposure and walking endurance as determined by the 6MWT.
We observed negative associations between 6MWT walking distance and age, BMI, health issues, and duration of diabetes, in line with previous studies (42). The Look AHEAD study assessed exercise capacity by a symptom-limited graded exercise treadmill test to voluntary exhaustion, in a large cohort of overweight/obese individuals with type 2 diabetes (43). The authors observed greater impairment of aerobic exercise capacity associated with greater levels of general and central obesity and a further reduction in fitness with increasing age and a longer duration of diabetes. In a study evaluating a healthy, younger cohort between 18 and 50 years of age, the 6MWD was not associated with age (44). However, in healthy older adults, older age has a negative association with distance walking during the 6MWT (21).
We also found an association between higher mean HbA1c and lower 6MWD suggesting that cumulative glycemic exposure negatively influences walking endurance. A study by Senefeld et al. did not find a difference in the 6MWD between T2D (HbA1c ≥7.0%) and controls; however, sample sizes were small (45, 46). The difference between these observations may lie in the study design and different glycemic exposures over time. Our study expands on this research and suggests that one possible effect of long-term hyperglycemia on 6MWT performance may be mediated via sustained hyperglycemia directly affecting skeletal muscle function and exercise adaptation (47). Finally, as with past research (48), we observed a positive association between walk distance and education, a marker of socioeconomic status.
In individuals with established T2D, lifestyle interventions that emphasize moderate-intensity physical activities have improved walking endurance. In the Look AHEAD study of adults with overweight/obesity and T2D, an intensive lifestyle intervention that included increasing physical activity had benefits in mobility, including an improvement in a 400-m walk test (49). Thus, while previous studies have shown a benefit of intensive lifestyle intervention on walking endurance in individuals with T2D during the active intervention period, treatment assignment did not show sustained benefits for walking endurance in DPP participants at risk for T2D during the DPPOS follow-up period, approximately 20 years after randomization.
The 6MWT is considered a useful and valid test of functional exercise capacity and endurance clinically in healthy aging populations (21, 50) and in those with chronic disease (51–54). Distance walking in 6 min may also represent an individual’s ability to perform certain activities of daily living since both require only a submaximal effort (19, 55, 56). In a previous analysis of DPPOS participants, those randomized to the lifestyle arm compared to the metformin or placebo arms had 37% lower odds of frailty (29). The components of the frailty assessment included walking speed (15-foot walk test), grip strength, physical activity, exhaustion, and unexplained weight loss (57). However, none of these individual frailty characteristics were different across the DPPOS randomization groups. Walking endurance, as measured by the 6MWT is not part of the frailty assessment (57). In the current analysis, we found that the 6MWD was associated with grip strength and habitual physical activity but we did not observe differences in walking distances by randomization group. Thus, while walking endurance and frailty are related (58), one possibility for our null findings may be that the effects of a lifestyle intervention wane over time when not maintained. The 6MWT assessment took place approximately 15 years after the end of the intensive lifestyle intervention phase of the DPP and only semi-annual lifestyle classes were provided for this group during DPPOS. However, the strong association between grip strength, physical activity, and 6MWT completion, as well as the 6MWD, suggests that maintaining an active lifestyle and maintaining muscle function after the end of the intervention may affect walking endurance in a population at risk for T2D. These findings are consistent with another small study evaluating an older cohort with T2D, where the 6MWD was positively associated with physical regular activity (48).
The strengths of our study include a long follow-up of a large, well-phenotyped, cohort of adults overweight and obese, all with a high risk of developing T2D at baseline, and continued assessment of glycemia semi-annually. Other strengths include a significant representation of Black, Hispanic, Native American, and Asian individuals, a high participation rate of those enrolled in DPPOS and still active (80%), and a comprehensive set of variables to examine the long-term effects of DPP interventions on walking endurance, and standardized procedures administered at diverse clinical sites in the United States.
There are a number of limitations to this analysis. The 6MWT was conducted approximately 15 years after the more active intervention period, and we cannot exclude the possibility that there may have been differences in the 6MWD among the groups had the test been performed earlier. Additionally, the 6MWT was not performed at randomization and was conducted only in a subset of the original DPP cohort (Supplementary Table 1). While we did not observe differences in attrition by treatment group, there is likely the presence of survivorship bias, where healthier individuals remain in the cohort. Furthermore, the conduct of the 6MWT was subject to variation by clinic, including differences in test environment and course length. Stop-watch time was recorded and exceeded 6 min for a subset of participants. Additional limitations include the potentially biased self-reports of leisure physical activity and the crossover in metformin use among the participants in the lifestyle and placebo cohorts who have been diagnosed with T2D. Metformin is a first-line treatment for type 2 diabetes; thus there is an increasing risk to the randomized analyses over time. However, total metformin exposure remained much higher in participants originally randomized to metformin. Similarly, the intensity of the lifestyle intervention was not sustained after the initial 3.2 years, and all participants were offered quarterly lifestyle classes during the DPPOS; however, participation in lifestyle classes was low across the intervention groups: approximately 80% of participants attended fewer than a quarter of the sessions offered, leading to reduced differences in weight between the groups. These features of the study may have reduced the relative effects of our interventions on 6MWT. Finally, while the 6MWT is a valid test of mobility and physical function, alternative measures such as the sit-to-stand, timed-up-and-go, or stair-climbing tests were not included in this analysis.
Although we did not observe a sustained effect of the originally randomized interventions on the 6MWT, we confirmed that the 6MWT is related to other measures of physical ability such as habitual physical activity and muscle strength (grip strength) in persons at risk for and with T2D. Our study also demonstrated that long-term metformin exposure does not negatively impact walking distance. While the randomized lifestyle treatment assignment was not associated with walking test distance, greater self-reported habitual physical activity, grip strength, and lower BMI were all associated with greater walking distances, suggesting potential long-term benefits of maintaining a healthy lifestyle. Given the importance of the 6MWT as a functional health measure reported in the literature, we anticipate that as DPPOS continues, it may predict future outcomes such as mortality and cognitive impairment.
In accordance with the NIH Public Access Policy, we continue to provide all manuscripts to PubMed Central including this manuscript. DPP/DPPOS has provided the protocols and lifestyle and medication intervention manuals to the public through its public website (https://www.dppos.org). The DPPOS abides by the NIDDK data sharing policy and implementation guidance as required by the NIH/NIDDK (https://www.niddkrepository.org/studies/dppos/).
Complete list of investigators in the Supplementary Appendix.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found at: https://www.niddkrepository.org/studies/dppos/.
The studies involving humans were approved by the Pennington Biomedical Research Center Pennington Biomedical Research Center, IRB University of Chicago University of Chicago, IRB Jefferson Medical College Thomas Jefferson University, IRB University of Miami University of Miami, IRB University of Texas Health Science Center at San Antonio UT Health, IRB University of Colorado Colorado Multiple Institutional Review Board Joslin Diabetes Center Committee On Human Studies Joslin Diabetes Center University of Washington University of Washington, IRB/Veterans Affairs, IRB University of Tennessee University Of Tennessee Health Science, IRB Northwestern University Northwestern University, IRB Massachusetts General Hospital Massachusetts General Hospital/Partners Human Research Committee University of California, San Diego UCSD Human Research Protections Program Columbia University (formerly St. Luke’s-Roosevelt Hospital Center) St. Luke’s-Roosevelt Hospital Center IRB/Human Research Protection Office CUMC, IRB Indiana University Indiana University Medstar Research Institute Georgetown - Medstar, IRB System University of California, Los Angeles UCLA Medical IRB1 Washington University School of Medicine Washington University Institutional Review Board Johns Hopkins School of Medicine Johns Hopkins Medicine, IRB1 The University of New Mexico UNM HSC Human Research Review Committee Albert Einstein College of Medicine Albert Einstein College of Medicine University of Pittsburgh University of Pittsburgh, IRB University of Hawaii University of Hawaii Human Studies Program SW Indian Center – Salt River/Phoenix National Institutes of Health Intramural Institutional Review Board SW Indian Center - Zuni National Institutes of Health Intramural Institutional Review Board SW Indian Center - Gila River National Institutes of Health Intramural Institutional Review Board SW Indian Center - Shiprock National Institutes of Health Intramural Institutional Review Board University of Southern California USC Office for the Protection of Research Subjects. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
MM: Supervision, Writing – original draft, Writing – review & editing, Conceptualization. EV: Writing – original draft, Writing – review & editing, Conceptualization. AT: Formal analysis, Writing – original draft, Writing – review & editing, Data curation, Investigation. WK: Writing – original draft, Writing – review & editing. EB: Writing – review & editing. RM: Writing – review & editing. JL: Writing – review & editing. CL: Writing – review & editing, Conceptualization. HH: Writing – review & editing. MS: Writing – review & editing. SE: Writing – review & editing, Data curation, Formal analysis, Investigation, Writing – original draft. TS: Writing – original draft, Writing – review & editing, Conceptualization, Methodology. DR: Writing – original draft, Writing – review & editing, Supervision.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. Research reported in this publication was supported by the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) of the National Institutes of Health (NIH) under award numbers U01 DK048489, U01 DK048339, U01 DK048377, U01 DK048349, U01 DK048381, U01 DK048468, U01 DK048434, U01 DK048485, U01 DK048375, U01 DK048514, U01 DK048437, U01 DK048413, U01 DK048411, U01 DK048406, U01 DK048380, U01 DK048397, U01 DK048412, U01 DK048404, U01 DK048387, U01 DK048407, U01 DK048443, and U01 DK048400, by providing funding during DPP and DPPOS to the clinical centers and the Coordinating Center for the design and conduct of the study, and collection, management, analysis, and interpretation of the data. Funding was also provided by the National Institute of Child Health and Human Development, the National Institute on Aging, the National Eye Institute, the National Heart Lung and Blood Institute, the National Cancer Institute, the Office of Research on Women’s Health, the National Institute on Minority Health and Health Disparities, the Centers for Disease Control and Prevention, and the American Diabetes Association. The Southwestern American Indian Centers were supported directly by the NIDDK, including its Intramural Research Program, and the Indian Health Service. The General Clinical Research Center Program, National Center for Research Resources, and the Department of Veterans Affairs supported data collection at many of the clinical centers. Merck KGaA provided medication for DPPOS. DPP/DPPOS have also received donated materials, equipment, or medicines for concomitant conditions from Bristol-Myers Squibb, Parke-Davis, and LifeScan Inc., Health O Meter, Hoechst Marion Roussel, Inc., Merck-Medco Managed Care, Inc., Merck and Co., Nike Sports Marketing, Slim Fast Foods Co., and Quaker Oats Co. McKesson BioServices Corp., Matthews Media Group, Inc., and the Henry M. Jackson Foundation provided support services under subcontract with the Coordinating Center.
The DPP Research Group gratefully acknowledges the commitment and dedication of the participants of the DPP and DPPOS.
MM has been a consultant to Sanofi. JL has been a consultant to Merck KGaA and receives metformin drug and placebo from EV Serono, a subsidiary of Merck KGaA, for a clinical trial (NCT04098666). CL was an employee in the Division of Diabetes, Endocrinology, and Metabolic Diseases at the National Institute of Diabetes and Digestive and Kidney Diseases at the NIH at the time this research was conducted and is now an employee of Amgen. RM receives research support from Novo Nordisk. RM was an employee at Joslin Diabetes Center at the time this research was conducted and is now also an employee of Novo Nordisk.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The sponsor of this study was represented on the Steering Committee and played a part in study design, how the study was done, and publication. All authors in the writing group had access to all data. The opinions expressed are those of the study group and do not necessarily reflect the views of the funding agencies. A complete list of Centers, investigators, and staff can be found in the Supplementary Material.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1470035/full#supplementary-material
1. Gregg, EW, Beckles, GL, Williamson, DF, Leveille, SG, Langlois, JA, Engelgau, MM, et al. Diabetes and physical disability among older U.S. adults. Diabetes Care. (2000) 23:1272–7. doi: 10.2337/diacare.23.9.1272
2. Ferrucci, L, Penninx, BW, Leveille, SG, et al. Characteristics of nondisabled older persons who perform poorly in objective tests of lower extremity function. J Am Geriatr Soc. (2000) 48:1102–10. doi: 10.1111/j.1532-5415.2000.tb04787.x
3. Bardenheier, BH, Lin, J, Zhuo, X, Ali, MK, Thompson, TJ, Cheng, YJ, et al. Disability-free life-years lost among adults aged >/=50 years with and without diabetes. Diabetes Care. (2016) 39:1222–9. doi: 10.2337/dc15-1095
4. de Rekeneire, N, and Volpato, S. Physical function and disability in older adults with diabetes. Clin Geriatr Med. (2015) 31:51–65, viii. doi: 10.1016/j.cger.2014.08.018
5. Dhamoon, MS, Moon, YP, Paik, MC, Sacco, RL, and Elkind, MSV. Diabetes predicts long-term disability in an elderly urban cohort: the northern Manhattan study. Ann Epidemiol. (2014) 24:362–368.e1. doi: 10.1016/j.annepidem.2013.12.013
6. Palmer, RF, Espino, DV, Dergance, JM, Becho, J, and Markides, K. The role of physical activity and diabetes status as a moderator: functional disability among older mexican americans. Age Ageing. (2012) 41:752–8. doi: 10.1093/ageing/afs106
7. Wray, LA, Ofstedal, MB, Langa, KM, and Blaum, CS. The effect of diabetes on disability in middle-aged and older adults. J Gerontol A Biol Sci Med Sci. (2005) 60:1206–11. doi: 10.1093/gerona/60.9.1206
8. Shang, Y, Fratiglioni, L, Vetrano, DL, Dove, A, Welmer, A, and Xu, W. Not only diabetes but also prediabetes leads to functional decline and disability in older adults. Diabetes Care. (2021) 44:690–8. doi: 10.2337/dc20-2232
9. Gregg, EW, and Menke, A. Diabetes and disability. In: Cowie CC, Casagrande SS, Menke A, Cissell MA, Eberhardt MS, Meigs JB, Gregg EW, Knowler WC, Barrett-Connor E, Becker DJ, Brancati FL, Boyko EJ, Herman WH, Howard BV, Narayan KMV, Rewers M, Fradkin JE, editors. Diabetes in America. 3rd ed. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases (US). (2018).
10. Stuck, AE, Bérod, AC, Stuck, AE, Alessi, CA, Aronow, HU, Santos-Eggimann, B, et al. Effectiveness of preventive in-home geriatric assessment in well functioning, community-dwelling older people: secondary analysis of a randomized trial. J Am Geriatr Soc. (1999) 47:389–95. doi: 10.1111/j.1532-5415.1999.tb07228.x
11. Guralnik, JM, Ferrucci, L, Simonsick, EM, Salive, ME, and Wallace, RB. Lower-extremity function in persons over the age of 70 years as a predictor of subsequent disability. N Engl J Med. (1995) 332:556–62. doi: 10.1056/NEJM199503023320902
12. Gitlin, LN, Winter, L, Dennis, MP, Corcoran, M, Schinfeld, S, and Hauck, WW. A randomized trial of a multicomponent home intervention to reduce functional difficulties in older adults. J Am Geriatr Soc. (2006) 54:809–16. doi: 10.1111/j.1532-5415.2006.00703.x
13. Newman, AB, Simonsick, EM, Naydeck, BL, Boudreau, RM, Kritchevsky, SB, Nevitt, MC, et al. Association of long-distance corridor walk performance with mortality, cardiovascular disease, mobility limitation, and disability. JAMA. (2006) 295:2018–26. doi: 10.1001/jama.295.17.2018
14. Studenski, S, Perera, S, Patel, K, Rosano, C, Faulkner, K, Inzitari, M, et al. Gait speed and survival in older adults. JAMA. (2011) 305:50–8. doi: 10.1001/jama.2010.1923
15. Lin, H, Zhu, Y, Liu, Q, and Li, S. The mediating effect of resilience between physical activity and mental health: a meta-analytic structural equation modeling approach. Front Public Health. (2024) 12:1434624. doi: 10.3389/fpubh.2024.1434624
16. Nordbakke, SST. Well-being and mobility: a theoretical framework and literature review focusing on older people. Mobilities. (2013) 9:104–29. doi: 10.1080/17450101.2013.784542
17. Moeyersons, M, De Vliegher, K, Huyghe, B, De Groof, S, Milisen, K, and de Casterle, BD. 'Living in a shrinking world'-the experience of loneliness among community-dwelling older people with reduced mobility: a qualitative grounded theory approach. BMC Geriatr. (2022) 22:285. doi: 10.1186/s12877-022-02998-5
18. Mellor, KSE, and Edelmann, RJ. Mobility, social support, loneliness and well-being amongst two groups of older adults. Personal Individ Differ. (1988) 9:1–5. doi: 10.1016/0191-8869(88)90024-4
19. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. (2002) 166:111–7. doi: 10.1164/ajrccm.166.1.at1102
20. Harada, ND, Chiu, V, and Stewart, AL. Mobility-related function in older adults: assessment with a 6-minute walk test. Arch Phys Med Rehabil. (1999) 80:837–41. doi: 10.1016/s0003-9993(99)90236-8
21. Bautmans, I, Lambert, M, and Mets, T. The six-minute walk test in community dwelling elderly: influence of health status. BMC Geriatr. (2004) 4:6. doi: 10.1186/1471-2318-4-6
22. Yazdanyar, A, Aziz, MM, Enright, PL, Edmundowicz, D, Boudreau, R, Sutton-Tyrell, K, et al. Association between 6-minute walk test and all-cause mortality, coronary heart disease-specific mortality, and incident coronary heart disease. J Aging Health. (2014) 26:583–99. doi: 10.1177/0898264314525665
23. Enright, PL, McBurnie, MA, Bittner, V, Tracy, RP, McNamara, R, Arnold, A, et al. The 6-min walk test: a quick measure of functional status in elderly adults. Chest. (2003) 123:387–98. doi: 10.1378/chest.123.2.387
24. Melzer, D, Lan, T, and Guralnik, JM. The predictive validity for mortality of the index of mobility-related limitation--results from the EPESE study. Age Ageing. (2003) 32:619–25. doi: 10.1093/ageing/afg107
25. das, S, Behera, SK, Srinivasan, A, Xavier, AS, Selvarajan, S, Kamalanathan, S, et al. Effect of metformin on exercise capacity: a meta-analysis. Diabetes Res Clin Pract. (2018) 144:270–8. doi: 10.1016/j.diabres.2018.08.022
26. Metz, L, Thivel, D, Peirrera, B, Richard, R, Julian, V, and Duclos, M. A new equation based on the 6-min walking test to predict VO(2peak) in women with obesity. Disabil Rehabil. (2018) 40:1702–7. doi: 10.1080/09638288.2017.1304582
27. Coen, PM, Jubrias, SA, Distefano, G, Amati, F, Mackey, DC, Glynn, NW, et al. Skeletal muscle mitochondrial energetics are associated with maximal aerobic capacity and walking speed in older adults. J Gerontol A Biol Sci Med Sci. (2013) 68:447–55. doi: 10.1093/gerona/gls196
28. Lee, CG, Schwartz, AV, Yaffe, K, Hillier, TA, LeBlanc, ES, Cawthon, PM, et al. Changes in physical performance in older women according to presence and treatment of diabetes mellitus. J Am Geriatr Soc. (2013) 61:1872–8. doi: 10.1111/jgs.12502
29. Hazuda, HP, Pan, Q, Florez, H, Luchsinger, JA, Crandall, JP, Venditti, EM, et al. Association of intensive lifestyle and metformin interventions with frailty in the diabetes prevention program outcomes study. J Gerontol A Biol Sci Med Sci. (2021) 76:929–36. doi: 10.1093/gerona/glaa295
30. Diabetes prevention program research group. The diabetes prevention program. Design and methods for a clinical trial in the prevention of type 2 diabetes. Diabetes Care. (1999) 22:623–34. doi: 10.2337/diacare.22.4.623
31. Diabetes prevention program research group. The diabetes prevention program: baseline characteristics of the randomized cohort. The diabetes prevention program research group. Diabetes Care. (2000) 23:1619–29. doi: 10.2337/diacare.23.11.1619
32. Knowler, WC, Barrett-Connor, E, Fowler, SE, Hamman, RF, Lachin, JM, Walker, EA, et al. Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. (2002) 346:393–403. doi: 10.1056/NEJMoa012512
33. Diabetes prevention program (DPP) research group. The diabetes prevention program (DPP): description of lifestyle intervention. Diabetes Care. (2002) 25:2165–71. doi: 10.2337/diacare.25.12.2165
34. Diabetes Prevention Program Research GroupKnowler, WC, Fowler, SE, Hamman, RF, Christophi, CA, Hoffman, HJ, et al. 10-year follow-up of diabetes incidence and weight loss in the diabetes prevention program outcomes study. Lancet. (2009) 374:1677–86. doi: 10.1016/S0140-6736(09)61457-4
35. Snyder, PJ, Bhasin, S, Cunningham, GR, Matsumoto, AM, Stephens-Shields, AJ, Cauley, JA, et al. Effects of testosterone treatment in older men. N Engl J Med. (2016) 374:611–24. doi: 10.1056/NEJMoa1506119
36. Borg, GA. Psychophysical bases of perceived exertion. Med Sci Sports Exerc. (1982) 14:377–81. doi: 10.1249/00005768-198205000-00012
37. Borg, G. Borg's perceived exertion and pain scales, vol. viii. Champaign, IL, US: Human Kinetics (1998). 104 p.
38. Kriska, AM, Sandler, RB, Cauley, JA, LaPorte, RE, Hom, DL, and Pambianco, G. The assessment of historical physical activity and its relation to adult bone parameters. Am J Epidemiol. (1988) 127:1053–63. doi: 10.1093/oxfordjournals.aje.a114881
39. Pereira, MA, FitzerGerald, SJ, Gregg, EW, Joswiak, ML, Ryan, WJ, Suminski, RR, et al. A collection of physical activity questionnaires for health-related research. Med Sci Sports Exerc. (1997) 29:5–9.
40. Kriska, AM, Rockette-Wagner, B, Edelstein, SL, Bray, GA, Delahanty, LM, Hoskin, MA, et al. The impact of physical activity on the prevention of type 2 diabetes: evidence and lessons learned from the diabetes prevention program, a long-standing clinical trial incorporating subjective and objective activity measures. Diabetes Care. (2021) 44:43–9. doi: 10.2337/dc20-1129
41. American Diabetes Association. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2019. Diabetes Care. (2019) 42:S13–28. doi: 10.2337/dc19-S002
42. Maniscalco, M, Zedda, A, Giardiello, C, Faraone, S, Cerbone, M, Cristiano, S, et al. Effect of bariatric surgery on the six-minute walk test in severe uncomplicated obesity. Obes Surg. (2006) 16:836–41. doi: 10.1381/096089206777822331
43. Ribisl, PM, Lang, W, Jaramillo, SA, Jakicic, JM, Stewart, KJ, Bahnson, J, et al. Exercise capacity and cardiovascular/metabolic characteristics of overweight and obese individuals with type 2 diabetes: the look AHEAD clinical trial. Diabetes Care. (2007) 30:2679–84. doi: 10.2337/dc06-2487
44. Halliday, SJ, Wang, L, Yu, C, Vickers, BP, Newman, JH, Fremont, RD, et al. Six-minute walk distance in healthy young adults. Respir Med. (2020) 165:105933. doi: 10.1016/j.rmed.2020.105933
45. Senefeld, JW, D'Astice, SE, Harmer, AR, and Hunter, SK. Increased cardiovascular response to a 6-minute walk test in people with type 2 diabetes. Diabetes Spectr. (2020) 33:104–10. doi: 10.2337/ds19-0002
46. Janssen, SM, and Connelly, DM. The effects of exercise interventions on physical function tests and glycemic control in adults with type 2 diabetes: a systematic review. J Bodyw Mov Ther. (2021) 28:283–93. doi: 10.1016/j.jbmt.2021.07.022
47. MacDonald, TL, Pattamaprapanont, P, Pathak, P, Fernandez, N, Freitas, EC, Hafida, S, et al. Hyperglycaemia is associated with impaired muscle signalling and aerobic adaptation to exercise. Nat Metab. (2020) 2:902–17. doi: 10.1038/s42255-020-0240-7
48. Fritschi, C, Bronas, UG, Park, CG, Collins, EG, and Quinn, L. Early declines in physical function among aging adults with type 2 diabetes. J Diabetes Complicat. (2017) 31:347–52. doi: 10.1016/j.jdiacomp.2016.06.022
49. Houston, DK, Leng, X, Bray, GA, Hergenroeder, AL, Hill, JO, Jakicic, JM, et al. A long-term intensive lifestyle intervention and physical function: the look AHEAD movement and memory study. Obesity (Silver Spring). (2015) 23:77–84. doi: 10.1002/oby.20944
50. Troosters, T, Gosselink, R, and Decramer, M. Six minute walking distance in healthy elderly subjects. Eur Respir J. (1999) 14:270–4. doi: 10.1034/j.1399-3003.1999.14b06.x
51. Regan, E, Middleton, A, Stewart, JC, Wilcox, S, Pearson, JL, and Fritz, S. The six-minute walk test as a fall risk screening tool in community programs for persons with stroke: a cross-sectional analysis. Top Stroke Rehabil. (2020) 27:118–26. doi: 10.1080/10749357.2019.1667657
52. Giannitsi, S, Bougiakli, M, Bechlioulis, A, Kotsia, A, Michalis, LK, and Naka, KK. 6-minute walking test: a useful tool in the management of heart failure patients. Ther Adv Cardiovasc Dis. (2019) 13:1753944719870084. doi: 10.1177/1753944719870084
53. Lee, MC. Validity of the 6-minute walk test and step test for evaluation of cardio respiratory fitness in patients with type 2 diabetes mellitus. J Exerc Nutrition Biochem. (2018) 22:49–55. doi: 10.20463/jenb.2018.0008
54. Celli, B, Tetzlaff, K, Criner, G, Polkey, MI, Sciurba, F, Casaburi, R, et al. The 6-minute-walk distance test as a chronic obstructive pulmonary disease stratification tool. Insights from the COPD biomarker qualification consortium. Am J Respir Crit Care Med. (2016) 194:1483–93. doi: 10.1164/rccm.201508-1653OC
55. Leone, M, Duverge, S, Kalinova, E, Bui, HT, and Comtois, AS. Comparison of bioenergetics of walking during a multistage incremental shuttle walk test and a 6-min walk test in active older adults. Aging Clin Exp Res. (2017) 29:239–46. doi: 10.1007/s40520-016-0555-0
56. Unver, B, Kahraman, T, Kalkan, S, Yuksel, E, and Karatosun, V. Reliability of the six-minute walk test after total hip arthroplasty. Hip Int. (2013) 23:541–5. doi: 10.5301/hipint.5000073
57. Fried, LP, Tangen, CM, Walston, J, Newman, AB, Hirsch, C, Gottdiener, J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. (2001) 56:M146–57. doi: 10.1093/gerona/56.3.m146
Keywords: diabetes, walking endurance, aging, six-minute walk test, lifestyle
Citation: Munshi MN, Venditti EM, Tjaden AH, Knowler WC, Boyko EJ, Middelbeek RJW, Luchsinger JA, Lee CG, Hazuda HP, Salive ME, Edelstein SL and Storer TW (2024) Long-term impact of Diabetes Prevention Program interventions on walking endurance. Front. Public Health. 12:1470035. doi: 10.3389/fpubh.2024.1470035
Edited by:
Jian Sun, Nanjing Agricultural University, ChinaReviewed by:
Anu Grover, Mangrove Creations LLP, IndiaCopyright © 2024 Munshi, Venditti, Tjaden, Knowler, Boyko, Middelbeek, Luchsinger, Lee, Hazuda, Salive, Edelstein and Storer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: The Diabetes Prevention Program Research Group, ZHBwbWFpbEBic2MuZ3d1LmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.