
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
COMMUNITY CASE STUDY article
Front. Public Health , 07 February 2025
Sec. Public Health Policy
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1463878
This article is part of the Research Topic Integrating Multidisciplinary Approaches to Mitigate Road Traffic Crashes and Outcomes View all articles
 Katherine Pérez1,2,3*
Katherine Pérez1,2,3* Elena Santamariña-Rubio2Maria José López1,2,3,4
Elena Santamariña-Rubio2Maria José López1,2,3,4 Lucia Artazcoz1,2,3,4Josep Ferrando1Carlos Pastor5
Lucia Artazcoz1,2,3,4Josep Ferrando1Carlos Pastor5 Adnan A. Hyder6
Adnan A. Hyder6 Carme Borrell1,2,3
Carme Borrell1,2,3Road traffic injuries are a significant public health concern, ranking among the leading causes of mortality and disability-adjusted life years lost globally, especially among the young population. Traditionally, road safety has been approached predominantly from a healthcare standpoint, with limited interventions from a comprehensive public health perspective. In Barcelona, the Agència de Salut Pública (Public Health Agency) has been monitoring road traffic injuries and evaluating road safety interventions since the late 1990s. This paper explores how Barcelona has addressed road safety over more than two decades through a public health lens, emphasizing the evaluation of intervention effectiveness, highlighting key success factors, and addressing the challenges encountered. First, we describe the road traffic surveillance system, providing insights into the context of mobility and road safety interventions in the city since the late 1990s. Since then, 10 interventions have been evaluated, encompassing legislation policies (helmet law, motorcycle driving license, and the penalty points system) and infrastructure measures (speed radars, advanced stop lines for motorcycles, safe routes to school, 30 km/h zone, and red-light cameras), as well as a cost–benefit study of speed radars. Next, the paper quantifies the overall impact of road safety interventions by estimating the difference between the observed number of road traffic injuries and the expected number if no interventions had been implemented from January 2008 to December 2023, stratified by gender, injury severity, and mode of transport. Since 2008, injuries were prevented in more than 34,800 individuals, including approximately 1,000 severe injuries. Mode-specific analysis revealed that more than 4,700 pedestrians, 12,300 car users, and 3,200 moped users benefited from injury prevention measures, while the number of injuries among motorcyclists was 5,200 higher than expected. This article discusses key success factors, the pivotal role of public health in road safety, and outlines future challenges, providing valuable insights for cities aiming to adopt a comprehensive public health approach to address road safety concerns.
Road traffic injuries are a well-known public health concern with more than 1.19 million fatalities each year. They are the leading cause of fatalities among 5- to 29-year olds and are the 12th leading cause of death among all age groups, resulting in more than 50 million people being injured or disabled (1). Two-thirds of these fatalities occur in individuals of working age (18–59 years), leading to significant health, social, and economic consequences that reverberate throughout society. More than half of all road traffic deaths occur among vulnerable road users, including pedestrians, cyclists, and motorcyclists (1).
Multiple strategies have been developed since the late 1970s, mainly at the national level. However, less attention has been paid to implementing urban-specific road safety strategies (2). Nonetheless, most of the population lives in cities, both in low-middle and high-income countries. In cities, due to traffic congestion and lower speed limits, the number of fatalities is typically low, but there is a high number of traffic crashes involving many non-severe injuries, frequently affecting vulnerable users such as pedestrians, cyclists, two-wheeled motorists, and other personal mobility vehicles such as scooters (3).
From a health standpoint, road safety has usually been addressed from the perspective of health, treatment at emergency departments, or hospital admissions, especially at sub-national levels (4). There are fewer experiences of public health organizations involved in road safety at small area levels, probably because the actions primarily depend on other sectors such as police or mobility departments.
Barcelona is a Mediterranean city with 1.6 million inhabitants, covering 101.35 km2, and a density of 15,992 people per km2. The city attracts more than 12 million tourists annually. Every working day, there are more than 6.10 million commuting trips in the metropolitan area, of which 72.3% are internal to the city (4.42 million), and the remaining are connections. On weekdays, 74.6% of the trips starting or ending in Barcelona and carried out by city residents are made using sustainable modes of transportation: 46.4% on foot, by bicycle, or personal mobility devices, and 28.2% by public transport. With more than 270,000 two-wheeled motor vehicles registered, the modal share of private vehicles is 25.4%, with motorized two-wheeled vehicles accounting for 7%. Specifically, walking and metro journeys account for a high percentage, together representing 55.5% of the total flow.
In the early 1990s, the Agència de Salut Pública de Barcelona created a road traffic information system, working in close collaboration with the police and the mobility department. This system allowed monitoring of road traffic injuries and the evaluation of road safety interventions to inform policies and decision-makers. Documenting the experiences of road safety in cities for more than two decades is important to help inform the global dialog on road safety. This paper aims to discuss how road safety has been addressed for more than 20 years in Barcelona city by a public health organization, with special emphasis on evaluating the effectiveness of 10 road safety interventions, highlighting key success factors, and addressing the challenges encountered in the process.
The information system initiated in the early 1990s has been enriched by various sources. In addition to local police data, the system incorporates information from other sources such as hospital emergency departments, deaths reported by the Institute of Legal Medicine and Forensic Sciences of Catalonia, the Mortality Register of Barcelona, and regular health surveys conducted in the city (5–7). Since 1997, comparable data have been accessible for monitoring the magnitude and characteristics of individuals injured in traffic collisions. These include details on the type and severity of injuries, sourced from hospital emergency departments and forensic reports. The city’s local police instituted a crash register, encompassing information on the circumstances of collisions, geocoded locations, vehicles, drivers, and injured individuals. This comprehensive effort was formalized through a collaboration agreement signed between the Agència de Salut Pública de Barcelona, the local police, and the mobility department.
Other information sources include: (a) the annual mobility survey (EMEF), which provides information on trips and travel time in the metropolitan area, including Barcelona city; and (b) annual average daily traffic data, which provide traffic volume data from most streets and allow vehicle-km estimates.
These data sources have enabled road traffic injuries to be characterized by gender, age group, type of road user and crossing, and time of the crash. They also allow identification of the nature of injuries, and their severity based on diagnoses [using the Abbreviated Injury Scale (AIS) and Injury Severity Score (ISS)], monitoring of traffic injury trends and calculation of indicators using various exposures, such as the number of inhabitants, vehicles, trips, hours traveling, and vehicle-km. These data sources have also enabled assessment of social inequalities in injury mortality (8). Table 1 shows the main indicators used to monitor road safety annually in Barcelona.
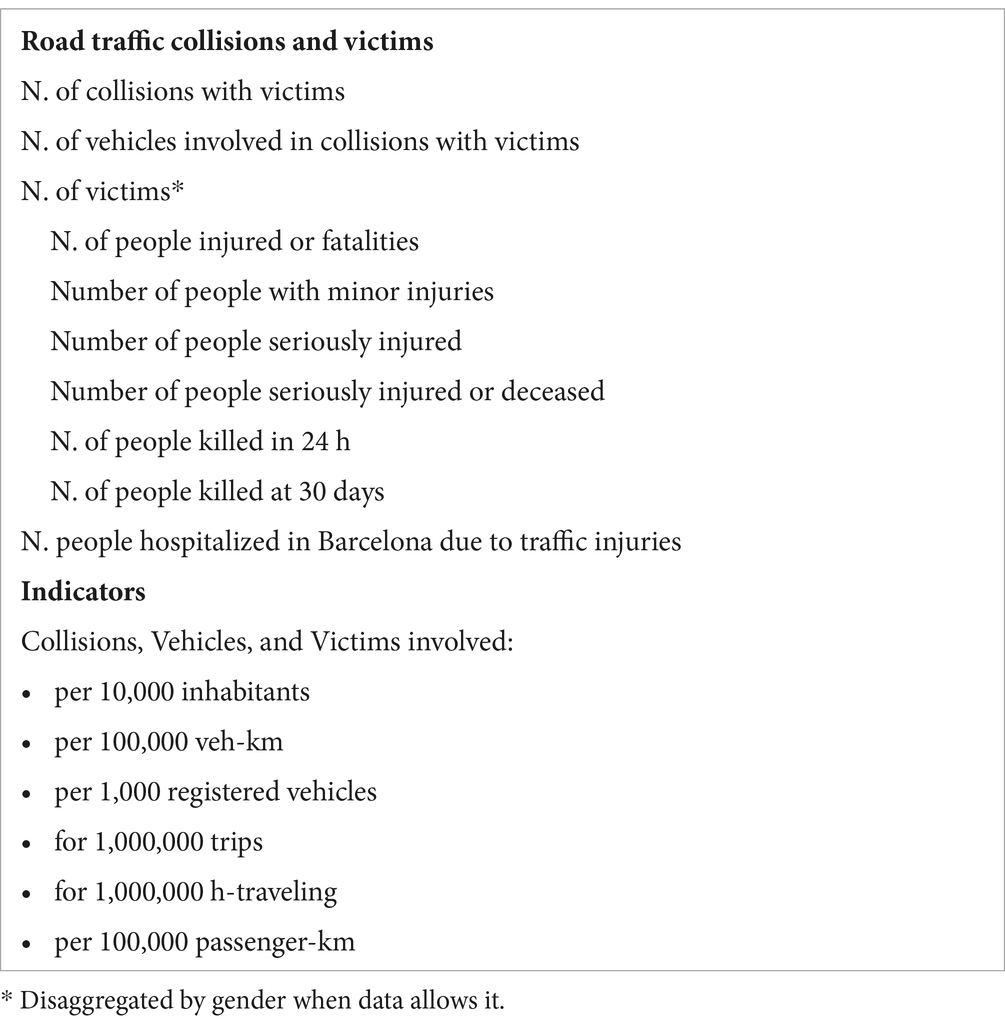
Table 1. Indicators used for monitoring road safety by the city of Barcelona.
The geographical location of collisions, as recorded by police using geocodes, has been essential for understanding their distribution and characteristics, as well as for identifying risk areas based on mobility exposure. This approach has facilitated the selection of specific areas to evaluate road safety interventions. In addition, it has enabled probabilistic record linkage of hospital, forensic, and police data (9), providing a deeper understanding of the nature and severity of injuries according to the circumstances of the crash and type of road user.
Figure 1 shows the trend in road traffic injuries by mode of transport and gender from 2002 to 2023. According to the Accident Register of the Urban Guard of Barcelona, in 2023, there were 7,202 collisions resulting in 8,786 injured or deceased individuals, with 41% being women. Of these, 20 people died (two women and 18 men), and 225 were hospitalized due to serious injuries (78 women and 147 men). Almost half of the injured individuals were motorcyclists (34.5% women and 52.4% men), followed by car occupants (22.5% women, 17.7% men), and pedestrians (15.4% women, 8.4% men). Cyclists accounted for 4.7% of injured women and 6.9% of injured men. In addition, 12.3% of women and 2.8% of men were passengers on busses. Injuries involving personal mobility vehicles, such as scooters, accounted for 6.1% of injured women and 6.9% of injured men, with these figures showing a steady annual increase.
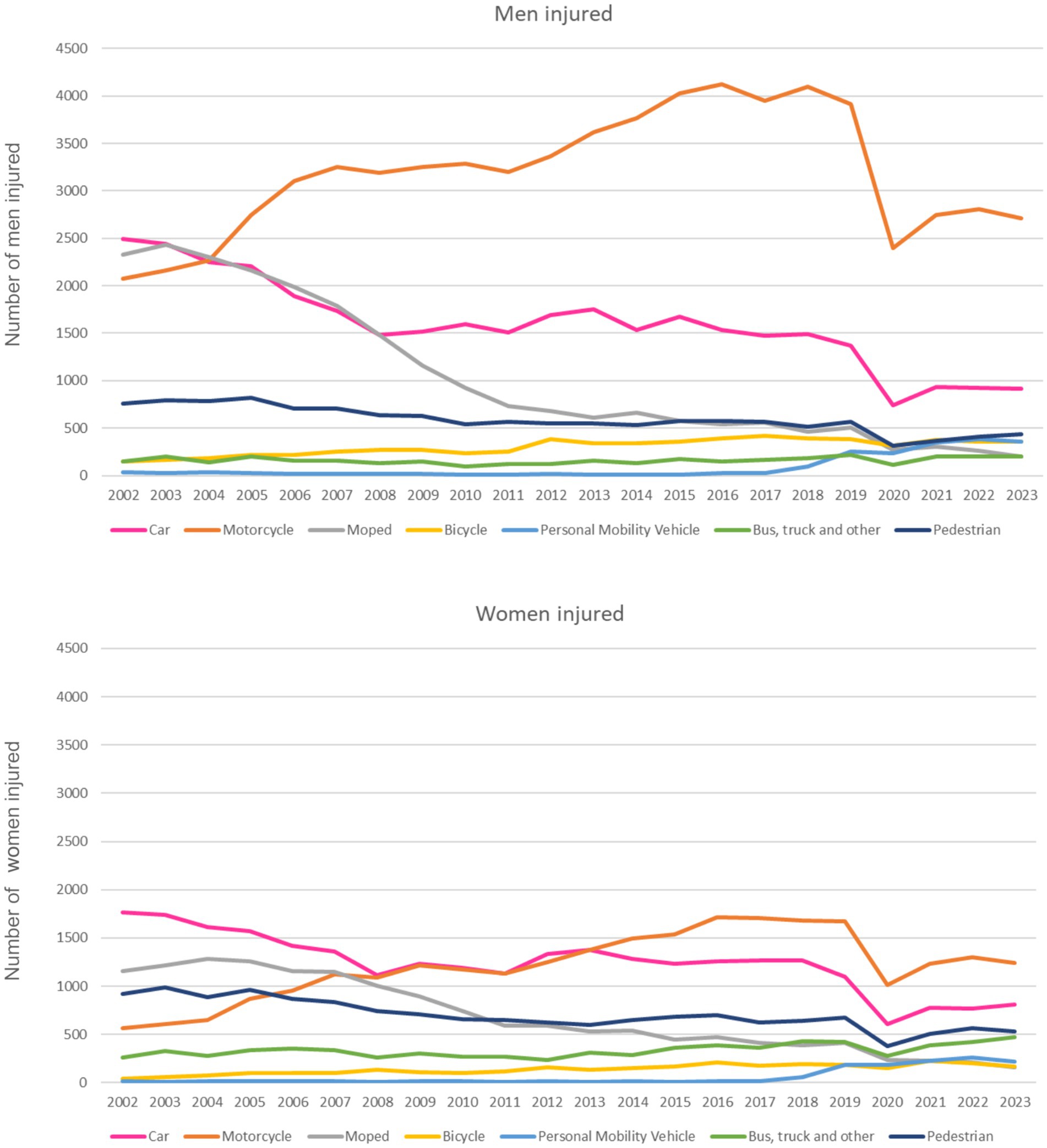
Figure 1. Road traffic injuries by mode of transport in Barcelona and gender. Barcelona 2002–2023.
The Barcelona City Council launched its first Municipal Road Safety Plan in 2000–2003, demonstrating its commitment to designing policies to reduce traffic injuries and enhance mobility and road safety in the city. At the same time, the Barcelona City Council formalized a Mobility Pact to encourage civil society to participate in promoting mobility and road safety in the city. Since its inception, the Mobility Pact has facilitated initiatives and consensus on actions to improve mobility and urban road safety. Currently, nearly 100 associations, companies, bodies, and public entities related to mobility are involved in this pact.
The second Municipal Road Safety Plan, covering 2004–2007, integrated the Urban Mobility Plan for the first time. Its main objectives included: a European commitment to reducing fatalities by 50% between 2000 and 2010; decreasing the number of road traffic injuries in the city by 45% between 2003 and 2010; proposing a social agreement to achieve zero fatal crashes in Barcelona and joining 30 European cities in this commitment. Barcelona signed the European Road Safety Charter in 2004.
The main actions included addressing the behavior of users through education and enforcement; enhancing vehicle safety; improving infrastructure and traffic management; increasing safety in the professional transport of goods and passengers; improving assistance and first aid to injured individuals; and ensuring more accurate collection, analysis, and dissemination of data on crashes.
Interventions were implemented in the city to achieve these goals, in line with the first Decade of Action on Road Safety 2011–2020, proclaimed by the UN General Assembly. These interventions included measures to reduce car use, such as raising parking costs and implementing traffic calming measures. Specific actions involved establishing 30 km/h zones, installing red-light cameras, creating bicycle lanes, and enhancing pedestrian protection with barriers, wider pavements, and safe routes to school. Figure 2 shows a timeline of major policies implemented in the city or brought about by national legislation (described later in this article) and evaluated.
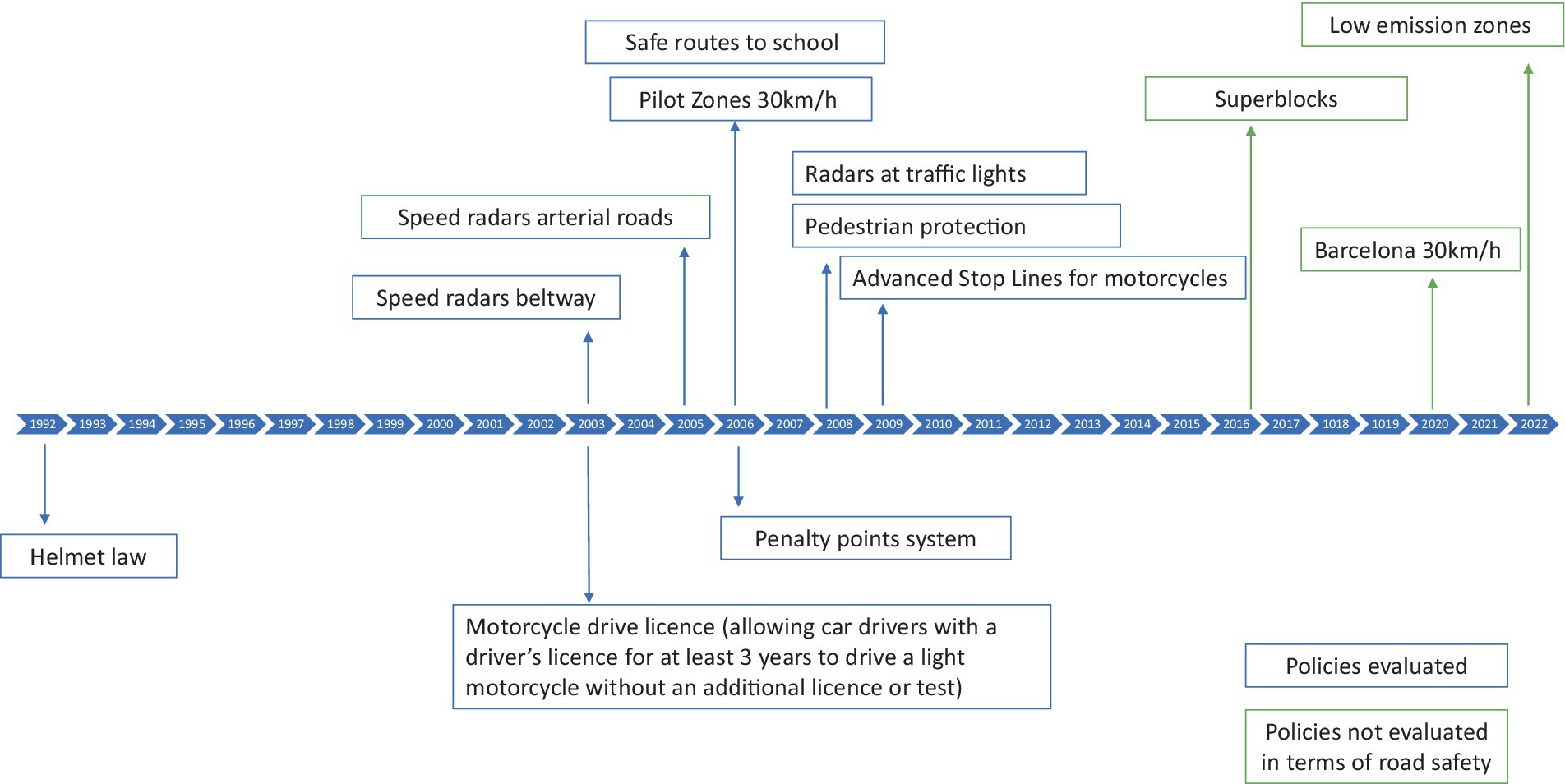
Figure 2. Timeline of Barcelona road safety interventions and evaluations (in blue).
Since then, additional road safety plans were developed, covering the periods 2013–2018 and 2018–2023, and linked to the city’s mobility plans. The most recent mobility plan for 2019–2024 is based on five main areas: safety, sustainability, health, equity, and smart mobility. This plan includes 62 lines of action and over 300 specific measures (10). Notably, it incorporates health as a new area of focus with 5 objectives.
Throughout the implementation of road safety policies in Barcelona, we assessed the effectiveness of several legislative and infrastructure interventions in terms of their impact on the number of collisions and injuries (Figure 2). The legislative policies evaluated include a helmet law (11), the penalty points system, and a motorcycle driver’s license (12). The infrastructure interventions assessed included speed radars (13, 14), 30 km/h speed limit zones, safe routes to school (15), advanced stop lines for motorcycles (16), and red-light cameras. We also estimated the cost–benefit ratio of speed radars (17). Table 2 summarizes the objectives, study designs, and main results of these evaluations conducted by the Agència de Salut Pública in Barcelona.
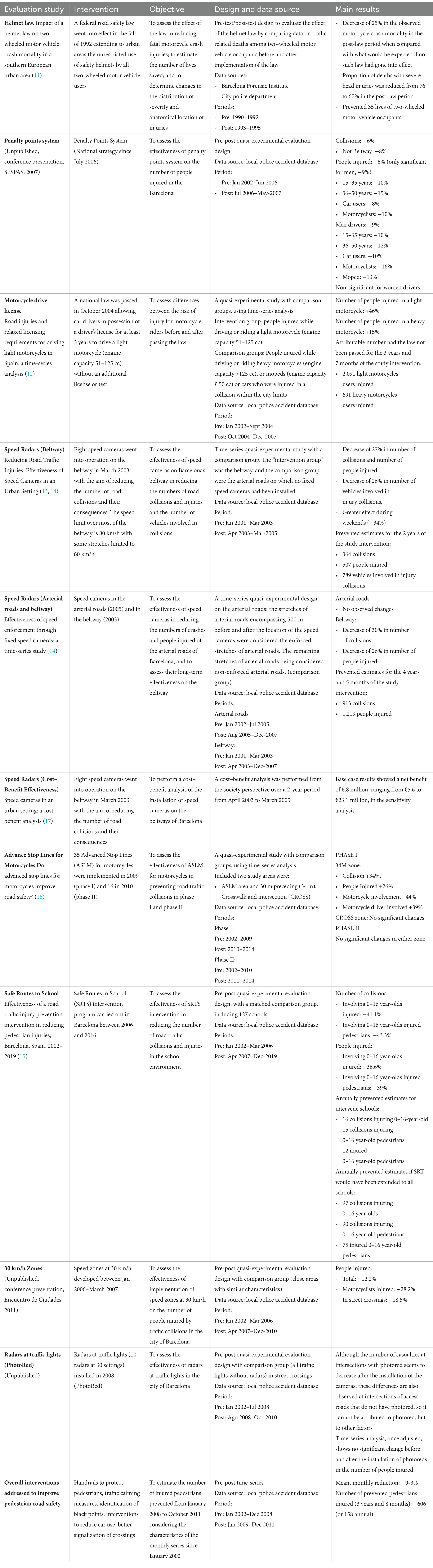
Table 2. Road safety interventions implemented and evaluated in Barcelona.
A national road safety law, enacted in 1992, mandated the use of safety helmets for all two-wheeled motor vehicle users in urban areas. Barcelona was the first Spanish city to strictly enforce the law, rigorously stopping two-wheeled motor users, imposing fines, and immobilizing vehicles until their drivers used a helmet. The evaluation showed a 25% decrease in motorcycle mortality 3 years after implementing the law compared with expected mortality without the law. The proportion of fatalities with severe head injuries decreased from 76 to 67%, and the law prevented an estimated 35 deaths among two-wheeled motor vehicle occupants (11).
Spain introduced the penalty points system as a national strategy in July 2006. After 11 months, injury-producing collisions were reduced by 6% in Barcelona city, with a reduction of 8% on the beltway. Injuries decreased by 6% overall and by 9% among men (more detail in Table 2). Age and gender analyzes revealed no significant effect among individuals older than 50 years, women, or collisions occurring outside the beltway. Despite the short follow-up, these results were consistent with an evaluation in Rome and the Lazio Region (18).
A national law passed in October 2004 allowed car drivers in possession of a driver’s license for at least 3 years to ride light motorcycles (engine capacity 51–125 cc) without an additional license or test. An evaluation revealed that the law significantly increased traffic and injuries. The number of injuries in light motorcyclists increased by 46%, and those in heavy motorcyclists by 15%. In the 3-years and 7 months after the passing of the law, nearly 3,000 more riders were injured than before the implementation of the law (12).
Speed cameras led to a significant 27% reduction in injury-producing collisions after 2 years of follow-up, which was maintained at 30% after 4.5 years, preventing 1,219 injuries (13, 14). A net benefit of €6.8 million was estimated (17). However, no effect was observed on arterial roads (14).
The initial phases of implementing 30 km/h speed zones resulted in a 12.2% reduction in injuries, an 18.5% reduction at street crossings, and a 28.2% reduction in injuries to motorcyclists. This evaluation supported the expansion of 30 km/h speed zones to the entire city in 2020, except for the beltway and arterial roads, where speed limits are between 60 and 80 km/h.
This intervention led to a significant 36.6% reduction in injuries among 0- to 16-year-olds and a 39.9% reduction among child and youth pedestrians. The intervention prevented an estimated 15 collisions injuring 0 to 16-year-olds, and 12 injuries to 0 to 16 year-old pedestrians annually (15).
However, not all interventions resulted in significant traffic injury reductions:
To facilitate mobility, a pioneering intervention was designed with no prior experience in other cities: implementing advanced stop lines for motorcycles (ASLM) without a specific lane to approach red lights, similar to bicycle lanes. The evaluation of the first phase showed a 34% increase in collisions, a 26% increase in injuries, a 44% increase in motorcycle involvement, and a 39% increase in motorcycle drivers involved in collisions in the space preceding the advanced stop line. Nonetheless, there were no significant changes in the space after the red lights at the crossing, which could have posed a risk for pedestrian collisions. The evaluation of the second phase of ASLM, implemented in a large arterial road, revealed no significant changes (16).
The evaluation of the effectiveness of installing 10 red-light radars in Barcelona in 2008, after 27 months of follow-up, showed no impact on the number of injured people, the number of drivers involved, or the number of injury-producing collisions. These results supported the decision not to extend red-light radars to the rest of the city.
In this section, we discuss the overall impact of the interventions discussed above on road traffic injuries from January 2008, when most interventions had been implemented, until December 2023. The analysis was conducted by gender, injury severity, and mode of transport. We conducted a pre-post evaluation using a temporal series based on the Police Register of traffic crashes from the local police of Barcelona. The outcome variable was the number of injured individuals, analyzed using generalized linear models with a robust Poisson distribution. We adjusted for possible confounders, such as linear trend, seasonal patterns, and regression to the mean, using sine and cosine functions. The effects of the financial crisis since 2010 and the pandemic since March 2020 were also included. No adjustment was made for mobility exposure, as the interventions aimed to modify mobility itself. The aim was to assess magnitude trends rather than the risk of injury. For more detailed methods, see the Supplementary material.
Figures 3, 4 show the monthly distribution of observed (red line) and expected (dashed green line, with gray confidence intervals) numbers of people injured in road traffic collisions from 2002 to 2023, categorized by severity, gender, and mode of transport, assuming no interventions had been implemented. Except for motorcyclists, the number of expected injuries consistently exceeded the number of observed injuries. The total number of injuries decreased until 2011, then rose steadily until April 2020, when they fell sharply due to the COVID-19 lockdown. Severe injuries and fatalities decreased until 2010 and then stabilized, with an annual mean of 211 severe injuries and 23 fatalities.
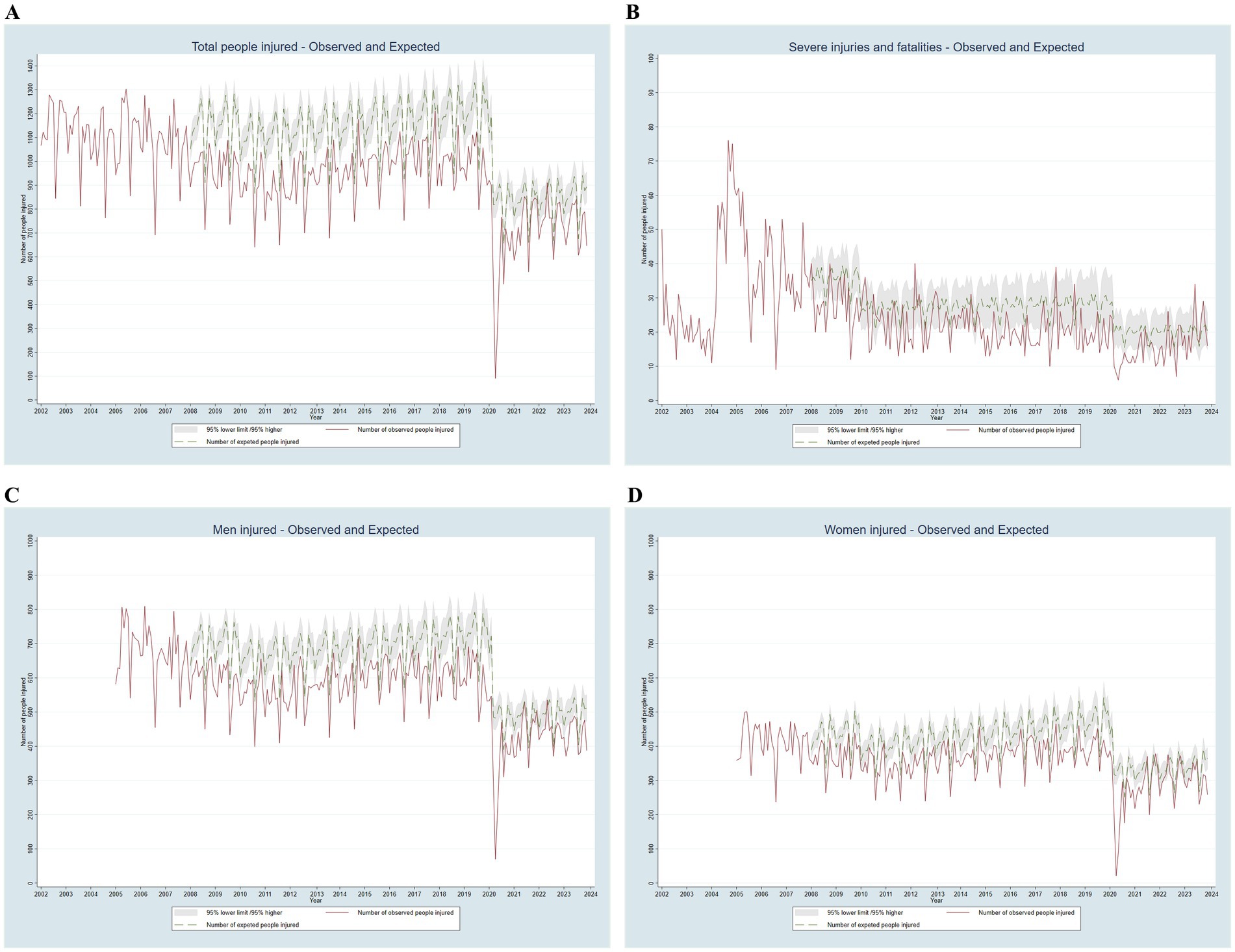
Figure 3. Observed and expected monthly number of people injured in road traffic collisions in Barcelona by severity and gender, adjusted for the financial crisis and COVID-19, 2002–2023.
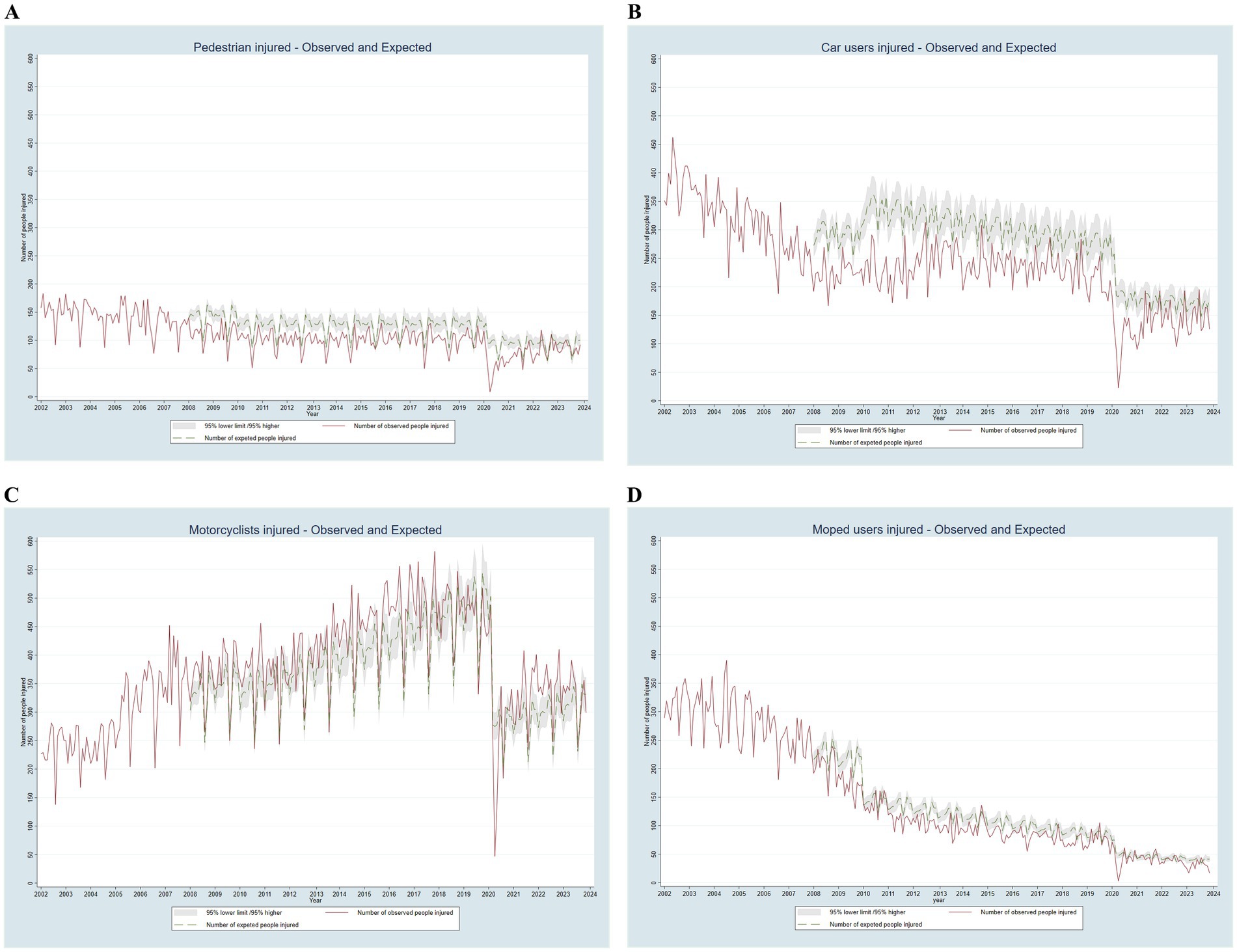
Figure 4. Observed and expected monthly number of people injured in road traffic collisions in Barcelona by mode of transport, adjusted for the financial crisis and COVID-19, 2002–2023.
The gender distribution followed a similar trend but with a lower magnitude for women (male/female ratio of 1.4 in more recent years). The trend for pedestrians remained highly stable. Car user injuries decreased until 2008, followed by a slight increase and then a stable pattern. Motorcyclists showed a continuous increase after 2005, following changes in light motorcycle driving license (12). In contrast, moped user injuries showed a continuous reduction.
According to the statistical model, since 2008 injury-producing road traffic collisions have been prevented in more than 34,800 individuals, including approximately 1,000 with severe injuries. By mode of transportation, injuries have been prevented in more than 4,700 pedestrians, 12,300 car users, and 3,200 moped users. However, there has been an excess of 5,200 injuries among motorcyclists (Table 3).

Table 3. Road traffic injuries observed, relative risk pre-post 2008, and prevented cases.
This study highlights the imperative of analyzing traffic injuries through an intersectoral approach, particularly from a public health perspective, given their significant scale. Evaluating the health impact of interventions is essential, as it enables the informed shaping of policies that extend beyond the health sector and profoundly affect the wider population. The article presents compelling evidence of the effectiveness of road safety interventions within urban settings, recognizing the distinct characteristics of space, roads, and transportation modes compared to interurban areas, which is a context with limited existing evidence.
Moreover, this study emphasizes the ongoing need to assess the health impact of policies under varying circumstances. Even interventions with established effectiveness may not consistently yield positive outcomes. As exemplified in this study, the influence of speed cameras on the beltway differed from their impact on arterial roads and intersections (e.g., red-light radars), illustrating the nuanced effects of interventions in diverse urban settings. This evaluation approach is essential for refining strategies and tailoring interventions to optimize their effectiveness in specific urban environments.
Nearly all the evaluations discussed in this paper were published in peer-reviewed journals, providing robust evidence of the effectiveness of these interventions. These findings align with other published experiences and suggest that similar strategies could be successfully implemented in other cities. However, the transferability of these interventions requires careful consideration of local contexts, as factors such as population characteristics, commuting patterns, and urban infrastructure can significantly influence outcomes (19). Therefore, while these interventions offer a valuable framework for road safety improvements, new implementations should always be evaluated to ensure they achieve the desired impact in different settings.
The estimated prevented injuries due to road safety policies in Barcelona over more than two decades is substantial, particularly severe injuries. Although being a rough estimation it aims to quantify effect of road safety policies to support further implementation. Some of the reduction since 2008 can also be attributed to the financial crisis, which appears to have affected car users more than motorcyclists. In addition to the financial crisis, policies to reduce car use, such as increased parking costs and traffic calming measures, may have led more people to switch from cars to motorcycles. Furthermore, some moped users might have transitioned to motorcycle use after he change in driver license law (12).
As conditions evolve over time, it is challenging to isolate and assess the effectiveness of each individual intervention over an extended period. Despite this limitation, the use of generalized linear models with a robust Poisson distribution provides a robust statistical framework for analyzing injury trends. This approach accounts for key confounders such as linear trends, seasonality, the financial crisis, and the COVID-19 pandemic, enhancing the reliability of the findings. Additionally, the analysis spans a broad period (2002–2023) and examines trends by severity, gender, and mode of transport, offering a comprehensive and nuanced understanding of road safety outcomes. However, as the study relies on observational data, it cannot establish direct causality, and unaccounted-for confounding factors may still influence the results. Several factors were important for success. Firstly, an essential factor was the recognition by public health professionals of road safety as a critical issue in health outcomes monitoring. Secondly, the early establishment of a comprehensive information system that integrated data from health and police sources proved instrumental in characterizing incidents, prioritizing road safety measures, and facilitating evaluation. Thirdly, effective collaboration and coordination among public health, police, and mobility professionals were achieved through a formalized agreement. Intersectoral collaboration for road safety in Barcelona involved regular coordination through joint committees, data sharing, and integrated action plans of mobility and road safety. The public health agency provided insights on injury trends, determinants, evaluation, monitoring and follow-up of action plans. In police role, there was enforced traffic laws and analysis of incident reports, and the mobility department focused on infrastructure improvements, and developing plans. Together, they allocate resources, engage the community for input (Mobility Pact) projects to test and refine strategies, such advanced zones for motorcycle. Continuous communication and monitoring ensure alignment, enabling to collectively reduce traffic-related injuries and fatalities while improving urban mobility.
Finally, civic engagement—evident in participation in the Mobility Pact, and more recently, the advocacy efforts of civil society groups—highlighted concerns about health impacts, particularly in road safety and air quality, thereby advancing road safety policies.
Several challenges mainly focused in developing a surveillance system and evaluating interventions merit attention. First, despite being well-documented for decades, significant gender-based inequalities in mobility patterns (20), modes of transportation, and consequently, the nature, frequency, and severity of injuries (21, 22), must be acknowledged. It is imperative to consistently incorporate a gender perspective into surveillance systems, data analysis, and the design and evaluation of interventions (23).
Second, another methodologically significant challenge in assessing road safety concerns the calculation of rates, which requires a denominator representing exposure to mobility (21, 22). While the resident population serves as a common denominator for numerous health issues, including country-wide analyzes of road safety, this approach is less practical at the city level due to the dynamic nature of population movement. To address this issue, precise denominators are essential, enabling risk analysis at smaller geographic levels and the inclusion of factors such as age groups, gender, mode of transport, and type of collision. This is important when implementing policies to reduce car usage, especially in a globalized society where, beyond daily commutes, individuals engage in extensive travel for tourism. Cities therefore experience substantial fluctuations in daily travel patterns, emphasizing the need for exposure denominators that reflect population movement.
Third, there is a pressing need to make progress in the interoperability of diverse data sources, likely linked through some form of common identifier. This would enable the severity and type of injuries to be studied, drawing from health sources, in conjunction with the circumstances of collisions, as reported by police sources. Harnessing the strengths of each source would provide a more comprehensive understanding of the impact of road incidents.
Fourth, it is essential to integrate the perspective of socioeconomic inequalities into road safety analysis (24). To achieve this, individual information on social class, educational level, place of residence, and the location of collisions is required. However, such information is often lacking in existing data sources due to data protection concerns. Moreover, collisions frequently occur outside individuals’ residential area due to their mobility (22). Addressing these challenges is vital for a comprehensive understanding of the impact of socioeconomic inequalities on road traffic injuries. It is highly recommended that this individual data becomes available for public health officers and researchers.
Fifth, while health records effectively document diagnoses and procedures—primarily due to their link with economic outcomes—details such as the external cause of the injury (e.g., frontal collision, pedestrian hit), mode of transport (e.g., bicycle, motorcycle), and position in the vehicle (e.g., driver, passenger) are often inadequately recorded. Although the ICD-10-CM provides a framework for detailed encoding, the absence of specific reporting or the use of non-specific codes poses a significant challenge. Comprehensive data on these factors is crucial for studying the nature and severity of injuries related to the vehicle involved and the circumstances of the collision, which would facilitate the design of preventive measures.
Sixth, intersectoral collaboration can be hampered by various political agendas. Road safety, framed within the “health in all policies” approach, requires a collaborative strategy that highlights the co-benefits for health, extending beyond the health sector to encompass multiple sectors. However, engaging these sectors has often proven challenging. In certain instances, policymakers have supported measures detrimental to health, often relying on overly narrow economic arguments that prioritize short-term gains for specific sectors over long-term societal benefits. Furthermore, some policymakers may misunderstand “Health in All Policies” as an expectation that health decision-makers resolve issues beyond their domain. Perceptions can be shifted by introducing the concept of “Health For All Policies” and emphasizing co-benefits, offering win-win solutions for all sectors (25). In Barcelona, for instance, health arguments have been effective in advocating for policies facing resistance, such as car restrictions within the city. Recognizing and integrating cross-sectoral action is imperative for advancing toward Sustainable Development Goals. Finally, evaluating all road safety policies and interventions, as with any health-related issue, is imperative. Determining their impact on health and health inequalities is crucial, as their effectiveness may vary among different territories and population groups. It is important to emphasize that the reported and evaluated interventions are the result of long-term planning and the gradual evolution of mobility in the city. These interventions were not all planned simultaneously but developed over time in response to emerging needs. Furthermore, the evaluations focused on interventions for which sufficient data were available, including adequate sample sizes, geographic distribution, follow-up data, and, when possible, comparable areas for controlling confounders. At the same time, they show the evolution of mobility policies in the city that gives priority to pedestrians, active mobility and reduces car use. The commitment to evaluation upholds the principles of transparency and accountability. Assessing the effectiveness of road safety interventions requires planning assessments alongside interventions, including comparison groups, and collecting exposure and outcome measures both before and after implementation. Additionally, it is vital to document interventions thoroughly, including details about the location and dates of implementation.
To strengthen the evidence base for policy-making, it is necessary conducting a more comprehensive cost–benefit analysis of road safety interventions in the future. Such an analysis would provide valuable insights into the economic and societal impacts of these measures, helping to identify the most cost-effective strategies for reducing road traffic injuries. By considering both direct costs, such as implementation and maintenance, and indirect benefits, including health outcomes and productivity gains, policymakers can make more informed decisions about allocating resources to maximize public health and safety outcomes.
In conclusion, the surveillance and evaluation of road safety interventions at the city level are pivotal for optimizing resources, tailoring strategies to local conditions, and continuously enhancing urban safety. This comprehensive 25-year assessment of road safety interventions in Barcelona reveals the complexity of implementing and appraising diverse strategies. The findings reveal a spectrum of effectiveness among interventions, with some demonstrating remarkable success and others falling short. This holistic evaluation approach, encompassing legislation, infrastructure, and economic considerations, provides indispensable insights for ongoing improvements and future road safety initiatives. These findings offer valuable insights to other cities but it needs to be approached with careful adaptation and additional evaluation.
A public health perspective serves as a guiding principle, ensuring a thorough understanding of the impacts of interventions on individuals, communities, and populations. Aligned with preventive and equity-focused principles, this approach contributes to the formulation of evidence-based strategies that promote and safeguard health and well-being. The estimation of prevented road traffic injuries in Barcelona serves as a testament to the effectiveness of the interventions implemented at the local level, providing a robust foundation for continual policy evaluation and refinement. These findings significantly contribute to the broader field of road safety and public health, offering invaluable insights for evidence-based strategies in injury prevention and advocacy for sustainable transportation modes at the city level.
The raw data supporting the conclusions of this article will be made available by the authors, upon reasonable request. Requests to access these datasets should be directed to KP, Y3BlcmV6QGFzcGIuY2F0.
KP: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Visualization, Writing – original draft, Writing – review & editing. ES-R: Conceptualization, Methodology, Validation, Writing – original draft, Writing – review & editing. ML: Validation, Writing – original draft, Writing – review & editing. LA: Validation, Writing – original draft, Writing – review & editing. JF: Writing – original draft, Writing – review & editing. CP: Writing – original draft, Writing – review & editing. AH: Writing – original draft, Writing – review & editing. CB: Conceptualization, Methodology, Validation, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. With the support of the Department of Research and Universities of the Generalitat de Catalunya (AGAUR), N. 2021 SGR 01462.
During the preparation of this work, we used ChatGPT-3 to improve readability and language. After using this tool, a professional translator reviewed the article, and all authors reviewed and edited the content as needed and took full responsibility for the content of the publication.
KP, ES-R, CB, and AH have been involved in road safety for over 20 years. KP, ES-R, JF, and CB are authors of many of the interventions included. KP, ML, LA, and CB are currently staff of the Agència de Salut Pública de Barcelona, and ES-R and JF are former staff. CP is currently responsible of the Unit of Road Traffic Accidents of Guardia Urbana de Barcelona. AH has received funds from NIH, World Bank, UN/WHO and has worked with these organizations on road safety for over 25 years.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1463878/full#supplementary-material
1. World Health Organization . Global status report on road safety 2023. Geneva. (2023). Available at: https://iris.who.int/bitstream/handle/10665/375016/9789240086517-eng.pdf?sequence=1 (Accessed December 15, 2023).
2. Hyder, AA, Hoe, C, Hijar, M, and Peden, M. The political and social contexts of global road safety: challenges for the next decade. Lancet. (2022) 400:127–36. doi: 10.1016/S0140-6736(22)00917-5
3. Garcia-Altés, A, and Pérez, K. The economic cost of road traffic crashes in an urban setting. Inj Prev. (2007) 13:65–8. doi: 10.1136/ip.2006.012732
4. Razzak, JA, Bhatti, J, Wright, K, Nyirenda, M, Tahir, MR, and Hyder, AA. Improvement in trauma care for road traffic injuries: an assessment of the effect on mortality in low-income and middle-income countries. Lancet. (2022) 400:329–36. doi: 10.1016/S0140-6736(22)00887-X
5. Xavier, Bartoll, and Catherine, Pérez. Col·lisions de trànsit i persones lesionades a Barcelona, 2020. Barcelona. (2021). Available at: https://www.aspb.cat/wp-content/uploads/2022/02/ASPB-colisions-transit-2020.pdf (Accessed January 26, 2024).
6. Mònica, Cortés, and Catherine, Pérez. Persones mortes a Barcelona per lesions per col·lisions de trànsit 2020. Barcelona. (2021). Available at: https://www.aspb.cat/wp-content/uploads/2020/08/ASPB-persones-mortes-barcelona-lesions-collisio-transit-2020.pdfç (Accessed January 26, 2024).
7. Novoa, A, Sánchez, C, and Catherine, P.. Personas lesionadas por tráfico atendidas en los servicios de urgencias en Barcelona, 2020. (2022). Available at: https://www.aspb.cat/es/documents/personas-lesionades-transito-urgencias-barcelona/ (Accessed January 15, 2024).
8. Gotsens, M, Marí-Dell’Olmo, M, Pérez, K, Palència, L, and Borrell, C. Trends in socio-economic inequalities in injury mortality among men in small areas of 26 Spanish cities, 1996-2007. Accid Anal Prev. (2013) 51:120–8. doi: 10.1016/j.aap.2012.10.020
9. Cirera, E, Plasència, A, Ferrando, J, and Arribas, P. Probabilistic linkage of police and emergency department sources of information on motor-vehicle injury cases: a proposal for improvement In: 43rd annual proceedings Association for the Advancement of automotive medicine (1999). 17–28.
10. de Barcelona, Ajuntament . Pla de Mobilitat Urbana 2024. Ens movem cap al futur de manera més sostenible, segura, saludable, equitativa i eficient. Pla Estratègic (2022). 1–228. Available at: https://bcnroc.ajuntament.barcelona.cat/jspui/bitstream/11703/128157/1/Pla%20de%20Mobilitat%20Urbana_bcn_2024.pdf (Accessed November 17, 2023).
11. Ferrando, J, Plasència, A, Orós, M, Borrell, C, and Kraus, JF. Impact of a helmet law on two wheel motor vehicle crash mortality in a southern European urban area. Inj Prev. (2000) 6:184–8. doi: 10.1136/ip.6.3.184
12. Pérez, K, Marí-Dell’Olmo, M, Borrell, C, Nebot, M, Villalbí, JR, Santamariña, E, et al. Road injuries and relaxed licensing requirements for driving light motorcycles in Spain: a time-series analysis. Bull World Health Organ. (2009) 87:497–504. doi: 10.2471/BLT.08.051847
13. Pérez, K, Marí-Dell’Olmo, M, Tobias, A, and Borrell, C. Reducing road traffic injuries: effectiveness of speed cameras in an urban setting. Am J Public Health. (2007) 97:1632–7. doi: 10.2105/AJPH.2006.093195
14. Novoa, AM, Pérez, K, Santamariña-Rubio, E, Marí-Dell’Olmo, M, and Tobías, A. Effectiveness of speed enforcement through fixed speed cameras: a time series study. Inj Prev. (2010) 16:12–6. doi: 10.1136/ip.2008.021485
15. Pérez, K, Santamariña-Rubio, E, Ferrando, J, López, MJ, and Badiella, L. Effectiveness of a road traffic injury prevention intervention in reducing pedestrian injuries, Barcelona, Spain, 2002-2019. Am J Public Health. (2023) 113:495–9. doi: 10.2105/AJPH.2022.307216
16. Pérez, K, and Santamariña-Rubio, E. Do advanced stop lines for motorcycles improve road safety? J Transp Health. (2019) 15:100657. doi: 10.1016/j.jth.2019.100657
17. Mendivil, J, García-Altés, A, Pérez, K, Marí-Dell’Olmo, M, and Tobías, A. Speed cameras in an urban setting: a costebenefit analysis. Inj Prev. (2012) 18:75–80. doi: 10.1136/ip.2010.030882
18. Farchi, S, Chini, F, Rossi, PG, Camilloni, L, Borgia, P, and Guasticchi, G. Evaluation of the health effects of the new driving penalty point system in the Lazio region, Italy, 2001-4. Inj Prev. (2007) 13:60–4. doi: 10.1136/ip.2006.012260
19. Craig, P, Dieppe, P, Macintyre, S, Mitchie, S, Nazareth, I, and Petticrew, M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. (2008) 337:979–83. doi: 10.1136/bmj.a1655
20. Olabarria, M, Pérez, K, Santamariña-Rubio, E, and Novoa, AM. Daily mobility patterns of an urban population and their relationship to overweight and obesity. Transp Policy (Oxf). (2014) 32:165–71. doi: 10.1016/j.tranpol.2014.01.012
21. Santamariña-Rubio, E, Pérez, K, Olabarria, M, and Novoa, AM. Gender differences in road traffic injury rate using time travelled as a measure of exposure. Accid Anal Prev. (2014) 65:1–7. doi: 10.1016/j.aap.2013.11.015
22. Santamariña-Rubio, E, Pérez, K, Olabarria, M, and Novoa, AM. Measures of exposure to road traffic injury risk. Inj Prev. (2013) 19:436–9. doi: 10.1136/injuryprev-2012-040686
23. Heise, L, Greene, ME, Opper, N, Stavropoulou, M, Harper, C, Nascimento, M, et al. Gender inequality and restrictive gender norms: framing the challenges to health. Lancet. (2019) 393:2440–54. doi: 10.1016/S0140-6736(19)30652-X
24. Gotsens, Miquel M. Desigualdades socioeconómicas en la mortalidad por lesiones en áreas pequeñas de zonas urbanas. Barcelona: Universitat Pompeu Fabra. (2012). 1–188.
Keywords: road safety, road traffic injuries, policy evaluation, evaluation, injury surveillance, public health, information system, health impact assessment
Citation: Pérez K, Santamariña-Rubio E, López MJ, Artazcoz L, Ferrando J, Pastor C, Hyder AA and Borrell C (2025) 25 years of providing evidence on road safety interventions at the city level. Front. Public Health. 12:1463878. doi: 10.3389/fpubh.2024.1463878
Edited by:
Maximilian Pangratius de Courten, Victoria University, AustraliaReviewed by:
Pengpeng Ye, Chinese Center for Disease Control and Prevention, ChinaCopyright © 2025 Pérez, Santamariña-Rubio, López, Artazcoz, Ferrando, Pastor, Hyder and Borrell. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Katherine Pérez, Y3BlcmV6QGFzcGIuY2F0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.