 Wenyu Li
Wenyu Li Zhijie Xu
Zhijie Xu Wenjie Tang3*
Wenjie Tang3*- 1School of Marxism, Capital Normal University, Beijing, China
- 2School of Economics and Management, North China Electric Power University, Beijing, China
- 3Capital Normal University, Beijing, China
Introduction: This study investigates gender-based disparities in self-rated health among older individuals in the Chinese workforce, utilizing data from the China Health and Retirement Longitudinal Study (CHARLS). Understanding these health gaps is crucial for crafting effective health policies and interventions in light of the rapidly aging population.
Materials and methods: Data from the 2020 CHARLS survey, comprising Chinese individuals aged 45 and above, were analyzed, focusing on older adults actively employed. Descriptive statistics and regression analyses examined gender discrepancies in self-rated health, considering diverse sociodemographic, economic, and health-related factors.
Results: Gender disparities in demographics, work environments, and self-rated health were observable among male and female participants. Older males tended to have higher rates of smoking and alcohol consumption, coupled with lower incomes. In contrast, females exhibited healthier behaviors influenced by access to healthcare and lifestyle modifications. For males, economic stability and moderate alcohol use positively influenced self-rated health, while females benefited from healthcare coverage and healthy lifestyle choices. Tailored gender-specific health interventions should prioritize these unique factors to enhance overall well-being.
Discussion: Discussions highlighted the impact of demographic variables, including age, marital status, social security, and employment conditions, on self-rated health. The study emphasized the crucial role of marital relationships in the health outcomes of older adult workers.
Conclusion: This study underscores the pivotal role of gender in self-rated health variations and provides essential insights for targeted interventions. By considering both quantitative and qualitative determinants of well-being, focused health policies can effectively address the health and well-being of aging populations, especially older adult workers.
Introduction
Population aging is a significant global challenge. According to the data from the United Nations, by 2050, one out of every six people in the world will be over 65 years old, which is three times higher than the proportion in 1990 (1). However, productive labour, instead of being a means of subjugating men, should become a means of their emancipation, by offering each individual the opportunity to develop all his faculties, physical and mental, in all directions and exercise them to the full—in which, therefore, productive labour should become a pleasure instead of being a burden (2). Instead of being seen as burdensome or irrelevant individuals, the social value of older adult workforce should be recognized. To achieve this, a thorough investigation of the health status of them is necessary. By addressing their specific health needs and challenges, policymakers can personalize interventions to promote their well-being and maximize their contribution to society, while also enabling the realization of their individual value in old age.
Previous studies (3–5) have not reached a consensus regarding gender differences in self-rated health, and research on the older adult workforce has also indicated the presence of gender discrimination in the labor market. Self-rated health serves as a vital marker, reflecting objective health conditions and correlating with long-term cardiovascular health. Research indicates that self-reporting health status is a critical indicator of cardiovascular health (6) and is closely associated with long-term physical morbidity and mortality (7). Based on data from China, this study aims to reveal gender disparities in self-rated health among the older adult workforce through empirical research. The findings will provide evidence-based interventions to enhance the health and well-being of older adult workforce, promote gender equality, and serve as a reference for policymakers seeking to fully utilize the social value of the older adults.
Literature context
Gender differences in self-rated health have been a topic of extensive research. However, the existing literature has yielded inconsistent findings regarding gender disparities in self-rated health. Some studies suggest no gender differences in self-rated health. Arber et al. (8) found that while older women had higher levels of functional impairment compared to men, there were no gender differences in self-rated health. Conversely, a study on self-rated health during adolescence indicated higher levels of self-rated health among females. Ostberg et al. (9) observed that adolescent girls scored higher on behavioral indicators, displayed greater interest in oral health, and perceived their oral health condition to be better than boys. D’Ambrosio et al. (10) also noted differences in self-regulatory behavioral patterns between males and females. Other research suggests that although women have longer lifespans, their self-rated health tends to be poorer than that of men. Knodel et al. (11) reported that despite higher survival rates among women, their self-rated health tends to be worse than that of men, with more health symptoms and physical functioning issues.
Scholars have demonstrated that gender differences in self-rated health diminish over time. Zajacova et al. (12) found that women generally rated their health lower than men, but this disparity decreased in old age and disappeared after accounting for socioeconomic and health covariates. Other researchers have examined gender differences in self-rated health and other influencing factors among the aging population. Chen et al. (13) investigated the gender differences in the impact of parental bereavement on health outcomes, including self-rated health, among middle-aged and older adults. Sharma et al. (14) delved into the potential mechanisms of age and gender differences in self-rated risk tolerance among the aging population, focusing on cognitive functioning and emphasizing the importance of understanding cognitive function in mitigating low risk tolerance in older adults. Lastly, Qi et al. (15) emphasized the prevalence and risk factors of social frailty in older adult individuals with cardiovascular diseases in China, highlighting an understudied aspect of frailty within this population.
Previous studies in the context of older adult workforce have primarily focused on the economic benefits or have regarded older individuals as a societal burden or recipients of care. Johnson (16) argued that, apart from the interest in the impact of pay-as-you-go pension systems on future tax burdens, economists seem to have generally overlooked the issues of older individuals and population aging. Dhar et al. (17) highlighted that population aging is rapidly becoming a significant socio-economic concern in India, with the rising dependency ratio imposing economic burdens on families. Conrad et al. (18) emphasized that population aging in Japan not only increases the burden on the younger generation but also depletes the resources necessary for driving robust economic growth.
While some studies have mentioned gender differences in the older adult workforce, there is often an emphasis on older women as wives and family members when they become the focus of research. Marenzi et al. (19) analyzed the empirical relationship between female labor market participation and intergenerational family ties using data from the 2000 Bank of Italy’s Survey on Household Income and Wealth (SHIW). Dempse et al. (20) noted that in Australia, retired men tend to assist rather than share the majority of traditional female household chores, with tasks requiring significantly less time and often of lower quality compared to the work of domestic helpers, while not significantly reducing their personal autonomy. Barone et al. (21) investigated whether and how the inflow of female immigrants specializing in household production affects the labor supply of Italian women.
Women are often studied as a specific labor force, namely caregivers. Finch et al. (22) found that care in residential institutions heavily relies on low-wage female labor. Ogawa et al. (23) examined the impact of providing care for older adult parents on the labor force participation of middle-aged women in Japan. The results indicated that regardless of the level of disability among older adult parents, the probability of daughters or daughters-in-law being employed is approximately 75%.
In summary, previous research has not yet reached a consensus on gender differences in self-rated health among the older adult workforce, and these findings have shown variation over time. Older adult workers are often viewed as a societal burden or recipients of care, with older adult women workers typically classified as caregivers, forming a distinct occupational group. Consequently, past studies have exhibited a pessimistic tendency, and older adult female workers also face tendencies of occupational discrimination.
Materials and methods
Source of data
This study utilized data from the China Health and Retirement Longitudinal Study (CHARLS).1 CHARLS is a nationally representative, interdisciplinary public database aimed at understanding the health and well-being of individuals aged 45 and above in China (24). The present study utilized the 2020 wave of the CHARLS national baseline survey, covering 19,351 individuals and over 10,000 households. The selection of the CHARLS baseline survey was motivated by several factors: it provides detailed data on individuals’ socioeconomic status, health conditions, and work situations, which are essential for exploring the health and well-being of China’s older adult labor force. Moreover, this dataset offers an opportunity to investigate the impacts of delayed retirement and gender equality on the health and well-being of the older adult workforce force. Since this study was a secondary analysis of CHARLS data, we did not require a separate ethical approval.
Model
This study utilized Stata 17.0 statistical software to conduct descriptive analysis and provide a detailed report on the differences in demographic characteristics, health conditions, and lifestyles between older adult individuals who are engaged in labor and those who are not. Additionally, chi-square tests are used to analyze the intergroup differences in various variables between these two groups. Logistic regression analysis is conducted to explore the correlations between the older adult workforce and various factors. All significant differences (p < 0.05) are included in the regression model. Results with a p-value less than 0.05 are considered statistically significant.
Dependent variables
The key variable of this study is gender, but specific selection criteria is required for the study population. Firstly, the selection of age range is crucial as there is a lack of clear age definition for the older adult workforce in research. Previous research (25) has suggested research should more broadly include employees aged 60 and above with the acceleration of population aging, so, we selected the older adult population aged 60 and above. Additionally, we determined individuals’ retirement status by using the questionnaire item “Have you already retired?” (FH001), and we utilized the Xworking indicator in the questionnaire to determine whether individuals in the target age group were still engaged in labor activities. Based on the above considerations, the study population is defined as individuals aged 60 and above who are actively participating in labor activities.
In this study, the explanatory variables are analyzed from several aspects, including demographic information, social security, employment status, and individual habits. To provide a clearer representation of the data processing flow, we present a data filtering flowchart (as shown in Figure 1). Demographic information encompasses age, Residence Location, Household registration type, and marital status. Social security includes pension insurance and medical insurance. Employment status includes type of employer, number of days worked per week in the past year, ways of receiving salary, and income level. Lifestyle habits include smoking and drinking habits, duration of sleep, and dietary intake. Detailed variable assignments are given in the Supplementary material S1.
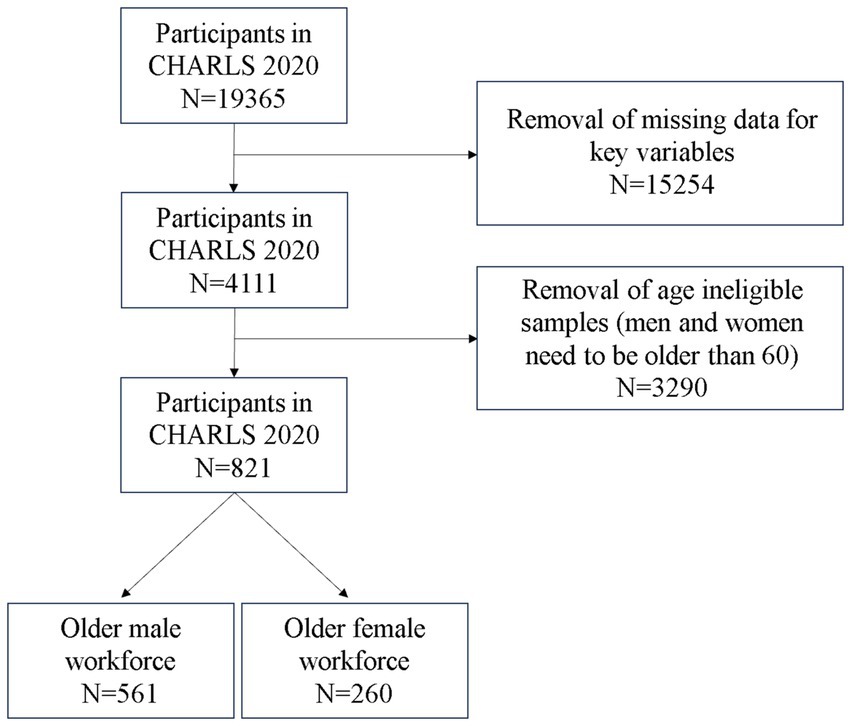
Figure 1. Data filtering flowchart.
Results
Statistical analysis

Analysis of the baseline statistical results
In this section, we conducted a comparative analysis of the demographics and working conditions between male and female respondents. Significant differences were observed: the average age of males was 64.44 years, while females averaged 64.70 years. Married males significantly outweighed females (91.27% vs. 76.92%). Notably, males were more likely to be self-employed or work in companies, and a higher proportion of males occupied managerial positions (14.08% vs. 3.07% for females). Income disparities were also evident, with 52.76% of males in the low-income bracket compared to 75.38% of females. Health habits revealed marked gender differences: 60.07% of males smoked, vastly exceeding the 5% of females who reported smoking. Similarly, alcohol consumption was much higher among males (63.99%) than females (15%). While self-rated health satisfaction was comparable, more females reported dissatisfaction. Males were more likely to work in government, institutions, and companies. They also had higher odds of being married, having pension and medical insurance, and earning more. Additionally, males predominated in smoking and alcohol consumption, and reported higher life and health satisfaction. No significant gender differences were noted in residential location, household registration, wage payment methods, or overall life satisfaction. Furthermore, we also conducted a subgroup analysis, categorizing participants into two groups based on their self-perception of health (good or not), as detailed in Supplementary material S2. These findings not only aid in our understanding of the role of gender in health inequality but also provide crucial insights for developing targeted health intervention measures.
Multivariate analysis of the self-rated health of the male and female respondents
Figure 2 illustrates the results of a multivariate analysis focusing on gender-specific factors influencing self-rated health. Supplementary material S3 presents a detailed overview of these findings, highlighting the quantitative and qualitative aspects of gender disparities in self-rated health. The comprehensive analysis of our study reveals significant gender-specific factors influencing self-rated health, with both quantitative and qualitative aspects considered. Among males, economic indicators were paramount, particularly income level. Quantitatively, males with moderate-low (OR = 1.6730, 95% CI: 1.0852–2.5794, p = 0.020), moderate (OR = 2.0943, 95% CI: 1.2632–3.4723, p = 0.004), and moderate-high (OR = 4.2916, 95% CI: 2.0767–8.8687, p < 0.001) income levels exhibited significantly higher odds of better self-rated health compared to those with low income levels. Qualitatively, this suggests that economic stability plays a critical role in male self-perceived well-being. Additionally, alcohol consumption among males (OR = 1.9775, 95% CI: 1.3841–2.8251, p < 0.001) was positively associated with self-rated health, indicating a potential beneficial effect of moderate alcohol intake on male well-being.
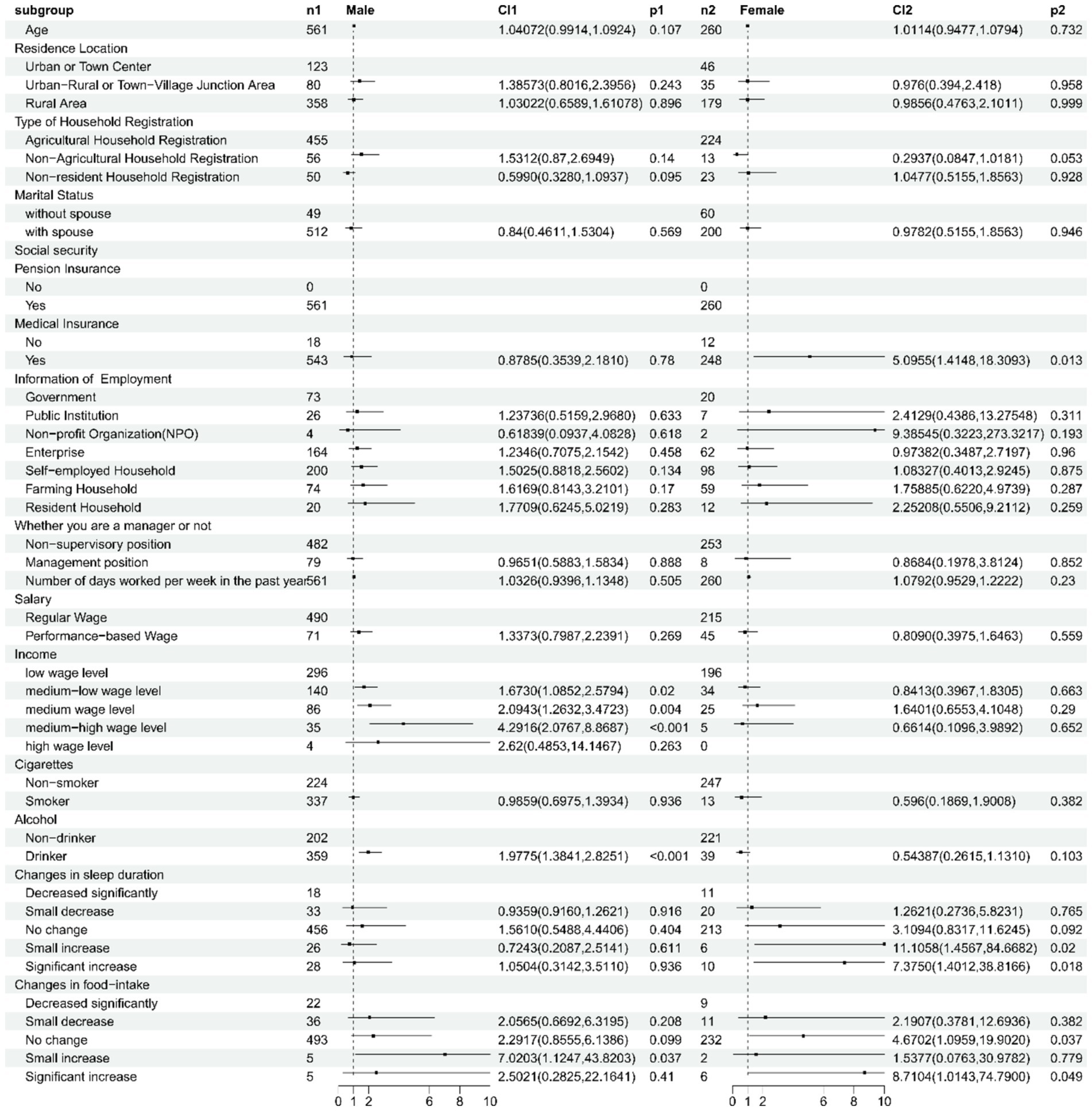
Figure 2. Gender-specific determinants of self-rated health among male and female older adult workers in China.
For females, however, healthcare coverage and lifestyle factors emerged as significant predictors. Quantitatively, females with medical insurance coverage showed significantly better self-rated health (OR = 5.0955, 95% CI: 1.4181–10.0000, p = 0.013), underscoring the importance of accessible healthcare for female well-being. Furthermore, positive changes in sleep duration and food intake among females were associated with improved self-rated health, indicating the beneficial impact of healthy lifestyle practices. Specifically, females reporting no change in sleep duration (OR not reported but positively correlated) and no change in food intake (OR = 2.2917, 95% CI: 0.8555–6.1386, p = 0.099 for trend) had better self-rated health compared to those experiencing significant decreases. Collectively, these findings highlight the need for gender-specific health policies and interventions that target the distinct quantitative factors influencing self-rated health among males and females, while also considering their qualitative implications for overall well-being.
Discussion
This study presents an empirical analysis of self-rated health among the older adult labor force in China, revealing significant gender differences in multiple dimensions. Univariate analysis provides rich background information for understanding these disparities, while multivariate regression analysis further elucidates the specific impacts of various factors on self-rated health for men and women. A detailed discussion of these findings follows.
Impact of demographic characteristics
There appears to be a positive correlation between age and self-rated health, although it is not statistically significant (p = 0.1070). This may suggest that as people age, their perception of health is influenced by various complex factors, including chronic diseases, physical functioning, and changes in social roles (26). Furthermore, marital status significantly affects self-rated health for both men and women, with married men tending to assess their health as good compared to unmarried men, while the opposite is true for unmarried women. This could be attributed to the social support, emotional solace, and coping abilities that marriage brings. Previous research (27) has also found that marriage indirectly influences health outcomes through emotions and lifestyle habits. Therefore, for the older adult labor force, a good marital relationship is crucial for health.
Social security and self-rated health
This study found that nearly all participants have access to pension and medical insurance, which to some extent safeguards their basic living and health needs. However, it is worth noting that although the coverage of medical insurance is high, its positive impact on women’s self-rated health is more significant (OR = 5.0955, p = 0.013). This may be related to higher healthcare needs and expectations among women, and it could also reflect the greater responsibility women have in caring for family health within the context of gender role division. Research has shown (28) that older adult women in China have lower coverage under the basic medical insurance for urban employees, based on the labor market situation. Overall, women exhibit a more proactive demand for health beliefs and attention to medical insurance, preventive care, and regular check-ups compared to men (29).
The impact of working conditions on self-rated health
Regarding working conditions, this study found that the proportion of men working in non-rural areas such as government and corporate sectors is higher than that of women, while women have a higher proportion of employment in rural and remote areas. This difference is particularly significant among men (p = 0.045) and may be attributed to factors such as the nature of work, work intensity, and income levels in different industries. Furthermore, the proportion of men holding managerial positions is significantly higher than that of women (p = 0.001), which could be related to the manifestation of gender inequality in the occupational domain. The impact of income levels on self-rated health is particularly significant for men, as men with middle to high-income levels are more inclined to assess their health as good. This may reflect the importance of economic stability in men’s perception of their own health. Research has found (30) that in relatively unequal societies, people generally perceive their health to be worse. Additionally, a study (31) has also found that income inequality significantly exacerbates subjective health disparities among older adult individuals in China, especially those with low incomes. Therefore, targeted efforts should be made to improve the health and well-being of the older adult population.
Lifestyle habits and self-rated health
Lifestyle habits have a significant impact on the self-rated health of both men and women. Specifically, consumption of cigarettes and alcohol is more prevalent among men (p < 0.001), and moderate alcohol consumption is positively correlated with men’s self-rated health (OR = 1.9775, p < 0.001). It should be noted that it may reflect the potential benefits of moderate alcohol intake or the consumption of alcoholic beverages on health (32). In contrast, women demonstrate a greater sensitivity to changes in sleep and dietary patterns. Specifically, the stability of sleep duration and dietary structure shows a significant positive correlation with women’s self-rated health. This finding highlights the critical role of healthy lifestyle habits in women’s health maintenance. Maintaining good sleep quality and a balanced dietary structure are of undeniable importance in promoting overall health among women. Therefore, encouraging women to pay attention to and improve their sleep and dietary habits would contribute to enhancing their quality of life and effectively preventing the occurrence of various health issues.
Gender-specific factors and self-rated health
An important finding of this study is the crucial role of gender-specific factors in self-rated health assessment. Economic factors and employment status have a more pronounced impact on men’s self-rated health, while social security and lifestyle habits have a more pivotal influence on women’s self-rated health. This finding emphasizes the importance of developing gender-specific health policies and interventions. For men, strengthening economic support and career development opportunities can enhance their perception of self-rated health. For women, enhancing the social security system and promoting the adoption of healthy lifestyle habits may be beneficial.
Limitations
Despite uncovering the significant role of gender-specific factors in self-rated health assessment, there are several limitations to this study. Firstly, the data used in this study are cross-sectional, which prevents establishing causal relationships. Future research can employ longitudinal designs to further explore the dynamic relationships among these factors. Secondly, this study did not consider other potential confounding factors such as genetics and psychological health status. Future research could control for these confounding factors to improve the accuracy of the results. Thirdly, the study sample primarily consists of a specific region or population, which may introduce certain regional and cultural differences. Future research can expand the sample size to enhance the generalizability of the findings. The fourth limitation of this study is the lack of direct comparison with international data on older workforce health, which could provide valuable insights into how the findings and implications of this research in China align or diverge with experiences in other countries. Lastly, the study’s reliance on single-year data limits its capacity to track longitudinal trends critical for comprehending temporal shifts in health outcomes. Additionally, the use of t-tests to evaluate gender disparities may fail to account for biases adequately. Future research should employ advanced statistical methods to establish causal relationships and mitigate omitted variable bias.
Conclusion
In conclusion, the study reveals significant gender disparities among China’s older adult labor force in terms of occupation, marital status, insurance, income, health behaviors, and subjective well-being. Males are more likely to work in government, public institutions, and companies, indicating a gender imbalance in job distribution. The proportion of males with spouses is significantly higher, suggesting differences in marital status between genders. Males exhibit higher proportions of having pension insurance and medical insurance compared to females. Income disparities are observed, with higher proportions of males in low, medium, and medium-high income. Males also demonstrate higher rates of consuming cigarettes and alcohol. Moreover, males report higher levels of self-rated health compared to females. The findings highlight the need for targeted interventions to address these disparities and improve public health outcomes. For males, improving income levels and regulating and educating about consuming alcohol may enhance their self-rated health level. For females, promoting healthcare insurance coverage and encouraging healthy sleep duration and dietary habits may contribute to improving their self-rated health status.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
WL: Conceptualization, Writing – original draft, Writing – review & editing. ZX: Writing – original draft, Writing – review & editing. WT: Conceptualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1450045/full#supplementary-material
Footnotes
References
1. GBD 2021 Fertility and Forecasting Collaborators. Global fertility in 204 countries and territories, 1950-2021, with forecasts to 2100: a comprehensive demographic analysis for the global burden of disease study 2021. Lancet. (2024) 403:2057–99. doi: 10.1016/S0140-6736(24)00550-6
2. Marx, K, and Engels, F: Marx & Engels collected works Vol 25: Engels: dialectics of nature. London: Lawrence & Wishart (1987) p. 280.
3. Gil-Lacruz, M, Gil-Lacruz, AI, and Navarro-López, J. Aguilar-Palacio I: gender gap in self-rated health: a cohort perspective in eastern European countries. Healthcare (Basel). (2022) 10:365. doi: 10.3390/healthcare10020365
4. Vafaei, A, Yu, J, and Phillips, SP. The intersectional impact of sex and social factors on subjective health: analysis of the Canadian longitudinal study on aging (CLSA). BMC Geriatr. (2021) 21:473. doi: 10.1186/s12877-021-02412-6
5. Pan, Y, Pikhart, H, Bobak, M, and Pikhartova, J. Labour-market characteristics and self-rated health: evidence from the China health and retirement longitudinal study. Int J Environ Res Public Health. (2023) 20:4748. doi: 10.3390/ijerph20064748
6. Barger, SD, Cribbet, MR, and Muldoon, MF. Participant-reported health status predicts cardiovascular and all-cause mortality independent of established and nontraditional biomarkers: evidence from a representative US sample. J Am Heart Assoc. (2016) 5:3741. doi: 10.1161/JAHA.116.003741
7. Amstadter, AB, Begle, AM, Cisler, JM, Hernandez, MA, Muzzy, W, and Acierno, R. Prevalence and correlates of poor self-rated health in the United States: the national elder mistreatment study. Am J Geriatr Psychiatry. (2010) 18:615–23. doi: 10.1097/JGP.0b013e3181ca7ef2
8. Arber, S, and Cooper, H. Gender differences in health in later life: the new paradox? Soc Sci Med. (1999) 48:61–76. doi: 10.1016/S0277-9536(98)00289-5
9. Ostberg, AL, Halling, A, and Lindblad, U. Gender differences in knowledge, attitude, behavior and perceived oral health among adolescents. Acta Odontol Scand. (1999) 57:231–6. doi: 10.1080/000163599428832
10. D’Ambrosio, LA, Donorfio, LK, Coughlin, JF, Mohyde, M, and Meyer, J. Gender differences in self-regulation patterns and attitudes toward driving among older adults. J Women Aging. (2008) 20:265–82. doi: 10.1080/08952840801984758
11. Knodel, J, and Zimmer, Z. Gender and Well-being of Older Persons in Cambodia. In: Devasahayam T., editor. Gender and Ageing: Southeast Asian Perspectives. Singapore: ISEAS Publishing (2014). p. 68–98. doi: 10.1355/9789814517980-006
12. Zajacova, A, Huzurbazar, S, and Todd, M. Gender and the structure of self-rated health across the adult life span. Soc Sci Med. (2017) 187:58–66. doi: 10.1016/j.socscimed.2017.06.019
13. Chen, Z, Ying, J, Ingles, J, Zhang, D, Rajbhandari-Thapa, J, Wang, R, et al. Gender differential impact of bereavement on health outcomes: evidence from the China health and retirement longitudinal study, 2011-2015. BMC Psychiatry. (2020) 20:514. doi: 10.1186/s12888-020-02916-2
14. Sharma, M, and Chatterjee, S. Cognitive functioning: an underlying mechanism of age and gender differences in self-assessed risk tolerance among an aging population. Sustainability. (2021) 13:42361. doi: 10.3390/su13042361
15. Qi, X, Jia, N, Hu, J, Meng, LB, Zeng, P, Liu, J, et al. Analysis of the status of social frailty in Chinese older adults with cardiovascular and cerebrovascular diseases: a national cross-sectional study. Front Public Health. (2023) 11:1022208. doi: 10.3389/fpubh.2023.1022208
16. Johnson, P: The structured dependency of the elderly: a critical note. CEPR Discussion Papers, CEPR Discussion Papers (1987).
17. Dhar, A. Workforce participation among the elderly in India: struggling for economic security. Indian J Labour Econ. (2014) 57:221–45.
18. Conrad, H, Heindorf, V, and Waldenberger, F. Human resource management in ageing societies: Perspectives from. Japan and Germany: Springer (2008).
19. Marenzi, A, and Pagani, L. The impact of elderly parents on labour market participation of Italian women. Rivista di Politica Economica. (2005) 95:155–90.
20. Dempsey, K. Gender exploitation and the domestic division of labour among the elderly: an Australian case study. Austr J Ageing. (1989) 8:3–10. doi: 10.1111/j.1741-6612.1989.tb00763.x
21. Barone, G, and Mocetti, S. With a little help from abroad: the effect of low-skilled immigration on the female labour supply. Labour Econ. (2011) 18:664–75. doi: 10.1016/j.labeco.2011.01.010
22. Finch, J, and Groves, D. By women for women: caring for the frail elderly. Women’s studies international forum. (1982). 5:427–438. doi: 10.1016/0277-5395(82)90005-X
23. Ogawa, N, Retherford, RD, and Saito, Y. Care of the elderly and women’s labour force participation in. Japan: Springer (2010).
24. Zhao, Y, Hu, Y, Smith, JP, Strauss, J, and Yang, G. Cohort profile: the China health and retirement longitudinal study (CHARLS). Int J Epidemiol. (2014) 43:61–8. doi: 10.1093/ije/dys203
25. Nagarajan, NR, Wada, M, Fang, ML, and Sixsmith, A. Defining organizational contributions to sustaining an ageing workforce: a bibliometric review. Eur J Ageing. (2019) 16:337–61. doi: 10.1007/s10433-019-00499-w
26. Kim, J, and Kim, H. Demographic and environmental factors associated with mental health: a cross-sectional study. Int J Environ Res Public Health. (2017) 14:431. doi: 10.3390/ijerph14040431
27. Kiecolt-Glaser, JK, and Newton, TL. Marriage and health: his and hers. Psychol Bull. (2001) 127:472–503. doi: 10.1037/0033-2909.127.4.472
28. Zhou, M, Zhao, S, and Zhao, Z. Gender differences in health insurance coverage in China. Int J Equity Health. (2021) 20:52. doi: 10.1186/s12939-021-01383-9
29. Ray-Mazumder, S. Role of gender, insurance status and culture in attitudes and health behavior in a US Chinese student population. Ethn Health. (2001) 6:197–209. doi: 10.1080/13557850120078125
30. Pickett, KE, and Wilkinson, RG. Income inequality and health: a causal review. Soc Sci Med. (2015) 128:316–26. doi: 10.1016/j.socscimed.2014.12.031
31. Yu, Q, and Wu, J. Impact of income inequalities on subjective perception of older adult health: an analysis of healthy life expectancy in China from 1997 to 2006. Geriatr Gerontol Int. (2024) 24:109–15. doi: 10.1111/ggi.14768
Keywords: self-rated health, gender differences, older adult workforce, economic factors, lifestyle habits
Citation: Li W, Xu Z and Tang W (2024) Gender differences in self-rated health among older adults in the Chinese workforce. Front. Public Health. 12:1450045. doi: 10.3389/fpubh.2024.1450045
Edited by:
Susana Rubio-Valdehita, Complutense University of Madrid, SpainReviewed by:
Wei Chen, Renmin University of China, ChinaFrancisco Palencia-Sánchez, Pontifical Javeriana University, Colombia
Copyright © 2024 Li, Xu and Tang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wenjie Tang, Y2FuZHljaGluYXRvd25AMTI2LmNvbQ==