 Zhipeng Luo1†
Zhipeng Luo1† Jinfeng Wang
Jinfeng Wang- 1Department of Oncology, The Third People's Hospital of Yibin, Yibin, China
- 2Yibin Vocational and Technical College, Yibin, China
- 3West China Hospital, Sichuan University, Chengdu, China
- 4The Second People's Hospital of Yibin, Yibin, China
- 5Meishan Pharmaceutical College, Meishan, China
Suicide, a global health concern, can be influenced by living arrangements. Hence, the objective of this systematic review was to assess the extent of the association between living alone and suicidal behaviors. We conducted a comprehensive search across eight databases for prospective studies. Hazard ratios (HR) and 95% confidence intervals were pooled using Stata software. Nine large-scale prospective studies with 3,663,205 participants proved eligible. The results of the meta-analysis showed that the pooled prevalence of living alone was 32%. Living alone was associated with suicide attempts and suicide death even after adjusting for all potential confounding factors (AHR = 1.45, 95% CI: 1.13–1.77; AHR = 1.27, 95% CI: 1.06–1.48). Compared to people who live with others, living alone increases the risk of suicide behaviors. Given the anticipated global rise in suicide rates and the growing prevalence of living alone, it is recommended to explore this issue on a broader scale.
Systematic review registration: PROSPERO, identifier: CRD42023464684, https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42023464684.
Introduction
Living alone represents a prevalent global social and psychological concern in contemporary society, constituting a significant element within the realm of negative social indicators. Over the past few decades, the prevalence of living alone has consistent global rise, this trend of living alone is particularly pronounced in developed nations. For instance, in European countries like Norway and Sweden, single-person households now constitute nearly half of all households (1). Between 1940 and 2020, there was a remarkable shift in the United States, with the overall proportion of individuals living alone surging from 7.7 to 27.6% (2). Furthermore, as per data from the 2021 China Statistical Yearbook, the year 2020 saw “one-person households” surpassing 125 million, accounting for more than a quarter of the total number of households (3).
Existing research indicate that there has been a growing interest in exploring the connection between living alone and individual health outcomes. Individuals who live alone are at an elevated risk of experiencing social isolation and loneliness, which can significantly undermine their psychological well-being, ultimately increasing the risk of premature mortality by roughly 30% (4).
Suicide is also a global health challenge, with over 800,000 people dying by suicide annually worldwide (5). In some countries, one in nine young individuals report having engaged in suicidal behaviors (6). Despite five decades of research, there has been limited progress in enhancing the prediction of suicidal behaviors. This underscores the urgent need for more targeted investigations into identifying specific risk factors associated with suicidal behavior (7). According to the interpersonal theory of suicide, individuals who live alone may experience failed belongingness due to unmet interpersonal needs and a lack of social connections, leading to psychological distress that heightens suicide risk (8). An increasing number of studies have noted that suicide risk varies with living arrangements, changes in family structure may contribute to the increase in suicide rates, and living alone may be an important objective risk factor for suicidal behaviors (9–12). A Danish follow-up study showed that living alone was a risk factor for subsequent suicide in men and women whose partners die (13). In addition, studies in Finland (14), the United Kingdom (15), and the Netherlands (16) have consistently reported that living alone is an independent risk factor for suicide.
While research has demonstrated that men are three times more likely to die by suicide than women, the specific nature of the relationship between gender, living alone, and suicidal behaviors remains unclear (17). Moreover, variations in social and cultural environments may influence living habits among individuals who live alone, potentially affecting the development of suicidal thoughts or behaviors (18). Research has shown that older adults individuals living alone who suffer from physical or mental illness are at a higher risk of suicide, particularly in the absence of social support and effective treatment (19, 20). Additionally, major negative life events, such as unemployment or financial difficulties, may serve as triggers for suicide among those living alone. A prospective study, a type of longitudinal research design, follows a cohort of similar individuals who differ in only one research factor over time, allowing researchers to examine the impact of that factor on outcomes such as death or disease progression. A longer follow-up period increases the number of observed outcome events, reveals long-term effects, and enables better control of bias and confounding variables, thereby enhancing the study’s accuracy and reliability.
Current aims
This systematic review aimed to synthesize evidence on the relationship between living alone and suicidal behavior, and to quantify the strength of this association. The specific objectives of the review were to:
i. Identify the prevalence of living alone based on prospective studies;
ii. Determine the extent of the association between living alone and suicidal behaviors based on prospective studies;
iii. Determine whether the relationship between living alone and suicidal behaviors varies with sociodemographic factors, follow-up years, or geographic location.
Methods
The design and write of this review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (21, 22). Additionally, the PROSPERO number is CRD42023464684.
Search strategy
Major English and Chinese databases were systematically searched between January 1, 2000, and September 15, 2023, which include PubMed, Embase, Web of Science, Scopus, ProQuest, PsycINFO, CNKI, and WANFANG database. The search methodology used Boolean operators, combining ‘and’ with two core search terms: firstly, a set comprising ‘living alone’, ‘live alone’, ‘lives alone’, and ‘unaccompanied’ as alternatives; secondly, utilizing the wildcard ‘suicid*’ to capture a broad range of suicide-related concepts. A detailed retrieval strategy is provided in Supplementary material S1. The search was confined to prospective cohort studies published in either English or Chinese. To ensure the thoroughness of our literature search, we manually examined the reference lists of relevant systematic reviews or meta-analyses and also conducted an independent search on Google Scholar.
Eligibility criteria
The inclusion criteria were as follows: (1) Population: individuals aged sixteen years and older, who do not live with others; (2) Exposure: living alone as a predictor of suicidal behaviors; (3) Outcome: reported measure of suicidal behaviors, include suicide attempt and suicide death; (4) Study design: prospective cohort studies.
The exclusion criteria were as follows: (1) Studies in languages other than English or Chinese; (2) Studies with were cross-sectional, case–control, qualitative, expert opinions, reviews, conference abstracts or those lacking available full texts, as well as duplicate studies; (3) Studies that offered incomplete data that could not be analyzed.
Data extraction
Following the removal of duplicates via Endnote 20, we conducted a literature screening in Rayyan, a web application (23). The first and second authors independently assessed the eligibility articles based on the titles and abstracts. Subsequently, full text of the remaining studies will be scrutinized against all inclusion criteria, which required studies to provide information regarding the association between living alone and suicidal behaviors. To guarantee the reliability of the screening process, we mandate that the two authors must achieve an agreement rate of at least 95% during any evaluation stage. In instances where uncertainty arises, we immediately engage a third reviewer for discussion. If, after thorough deliberation, a consensus is still not reached, we escalate the matter to the corresponding author for a definitive resolution. This process ensures that every decision made throughout the evaluation is rigorous and well-founded. To ensure the accuracy and consistency of our data, we have adopted the following methods: Firstly, we clarify the extraction standards and rules prior to data extraction, ensuring a unified understanding among the two reviewers regarding the content to be extracted. Secondly, both reviewers independently extract data from the same segment, and their results are subsequently compared for consistency. Any discrepancies identified are discussed and resolved to reach a consensus. Lastly, we regularly arrange for a review session, where a third reviewer or expert verifies the extracted results. Finally, the following information was extracted independently by two reviewers: study characteristics (author, year of publication, country, cohort designation, follow-up duration); participant characteristics (age, sample size and sample type); outcome characteristics (the prevalence of living alone, the measure, forms and prevalence of suicidal behaviors). Furthermore, effect measures pertaining to the associations between living alone and suicidal behaviors were also be extracted. In cases of missing or unclear data, we initiated correspondence with the researchers, seeking further elaboration on both the methods and/or the results as dictated by the need for accuracy and completeness.
Risk of bias assessment
Two independent reviewers assessed the methodological quality of the included studies, and any discrepancies resolved through consensus. The methodological risk of bias the included prospective studies was evaluated using the Newcastle-Ottawa Quality Assessment Scale (NOS) (24), which assigns scores ranging from 0 to 9 points, with scores of ≥7 points classified as indicative of high quality (25, 26). Meanwhile, we used Egger’s tests to identify publication bias.
Statistical analysis
STATA software (version 17.0) was used for all statistical analyses, and a qualitative synthesis was conducted to summarize the characteristics of the included articles. If two or more adjusted effect size were provided in the same article, we would choose the most comprehensive adjusted effect size for pooling. Subgroup analyses were performed considering gender, continent, sample type and follow-up lengths. All ratios used in the subgroup analysis were adjusted for potentially confounding factors. The Cochrane Q test and I2 statistic were the two most often used indicator of heterogeneity. The model selected (fixed or random-effect) would depend on the magnitude of heterogeneity: A value of 0–25% indicates low heterogeneity and 26–50% indicates moderate heterogeneity, a fixed effects model was chosen; 51–100% indicates substantial heterogeneity, a random effects model was adopted (27, 28). Furthermore, the stability of the results was tested by leave-one-out sensitivity analyses, and a significance level of p < 0.05 (2-tailed) was taken as robustness after removing any observation.
Results
Search results
Figure 1 depicts the process of literature screening and selection using a PRISMA flow chart. Removal of the duplications left 983 records. After screening the title and abstract, 140 articles in the full-text evaluation stage, of which 9 studies were included in qualitative synthesis and meta-analyses.
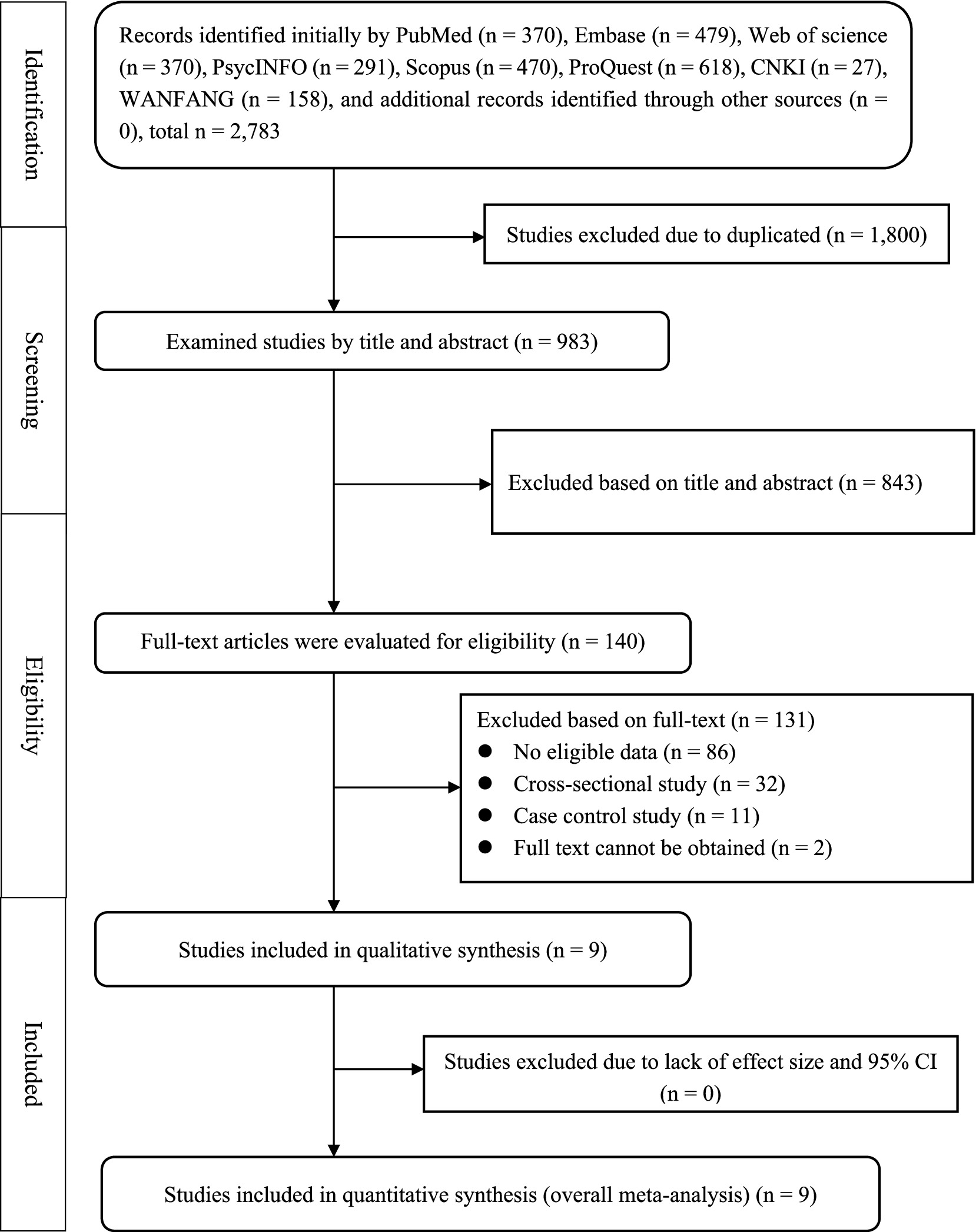
Figure 1. The process of literature search based on the PRISMA statement.
Studies characteristics
Table 1 provides an overview of the nine included studies. These studies were all prospective and were published between 2011 and 2021. The majority of them were conducted in European countries, with one study each from Canada (29) and Japan (18). The follow-up duration for these studies ranged from a minimum of 5 years to a maximum of 23 years, with an average duration of 11.2 years. The sample sizes varied considerably, ranging from 12,850 to 2,685,400 individuals, totaling 3,663,205 participants. Notably, except for one study that did not report specific gender counts (29), female participants outnumbered male participants in the remaining studies. In terms of the study populations, four studies focused on individuals diagnosed with various common mental disorders (14, 30–32), while another four investigated samples from the general population (15, 18, 29, 33). Only one study had a sample comprising stroke patients (34). Regarding living arrangements, the proportion of individuals living alone varied significantly, ranging from 4.51 to 55.55%. Data on suicidal behaviors were sourced from database registries or medical records in all the included studies, with suicide death consistently identified as the primary outcome measure. Additionally, three of the studies also simultaneously examined suicide attempts (31, 32, 34). The prevalence of suicide death in these studies ranged from 0.05 to 4.55%, while the prevalence of suicide attempt ranged from 0.45 to 5.8%.
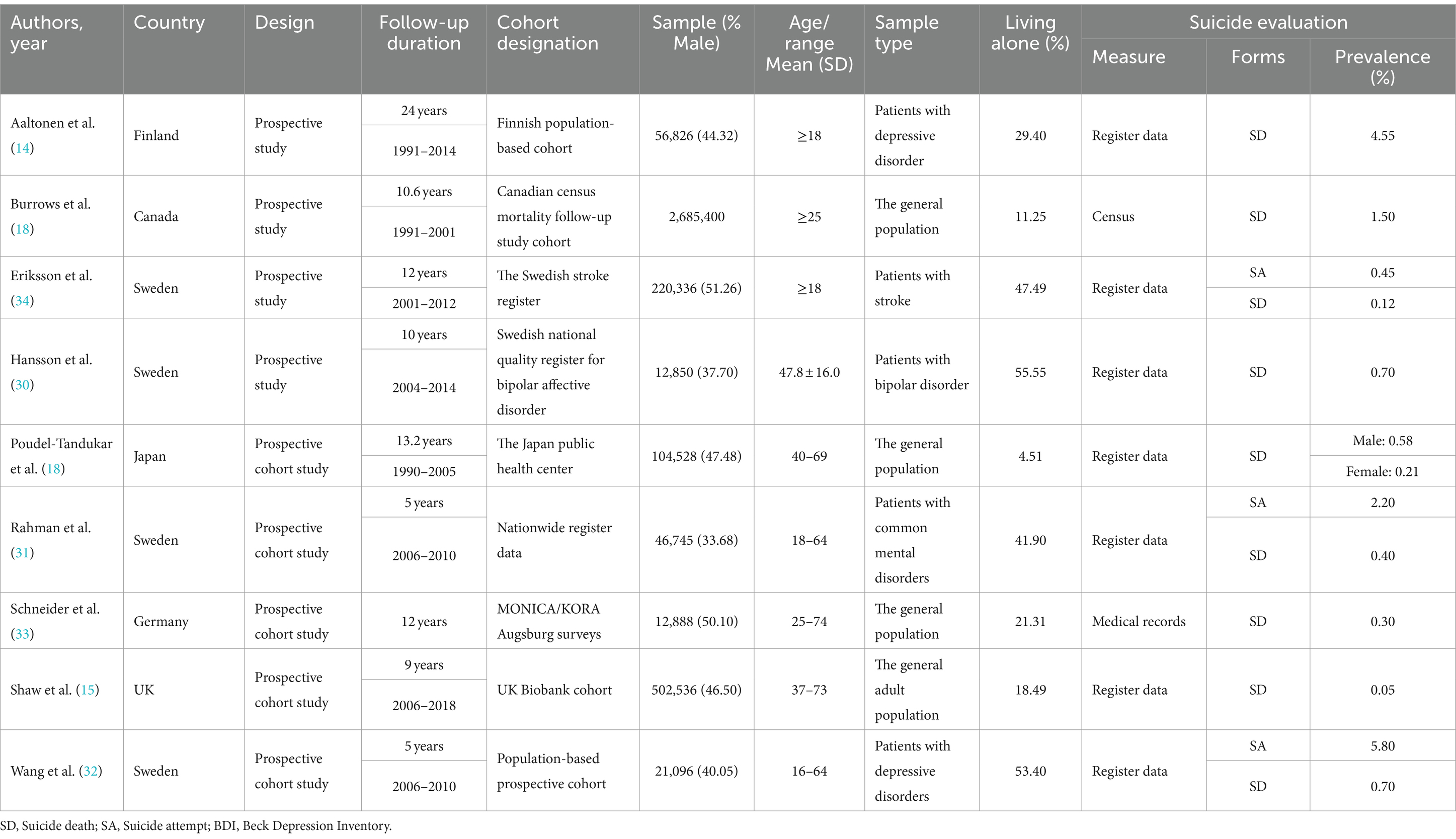
Table 1. Characteristics of included studies.
Assessment quality of studies
The quality of included studies was assessed by the Newcastle Ottawa scale (NOS) for cohort studies. All the studies included in our analysis received quality assessment scores exceeding 7 points, classifying them as high-quality literature. However, four of these articles did not receive scores regarding the representativeness of their included samples due to their focus on specific disease populations (Supplementary Table S1).
Results of meta-analysis
The prevalence of living alone
All included studies provided the proportion of people living alone. The results of the meta-analysis showed that the pooled prevalence of living alone was 32% (95% CI: 19–44%, I2 = 100%) (Table 2 and Supplementary Figure S1).
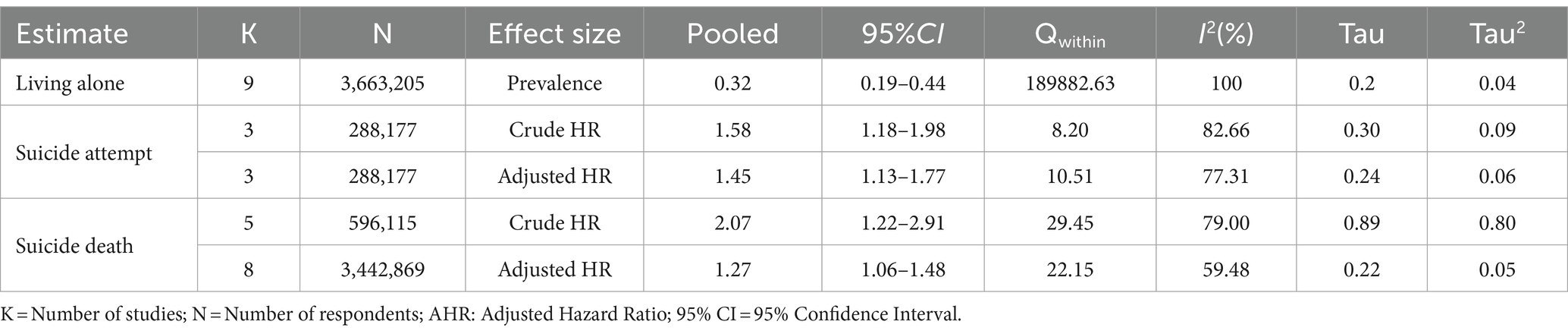
Table 2. Meta-analytic findings on the extent of the association between living alone and suicidal behaviors.
The association between living alone and suicidal behaviors
Table 2 presents the combined crude and adjusted Hazard Ratio (HR) estimates for the relationship between living alone and both suicide attempt and suicide death. This meta-analysis includes data from three studies, involving a total of 288,177 participants (31, 32, 34). The results reveal that, even after adjusting for all potential confounding factors, individuals who live alone exhibit a substantially higher risk of suicide attempt compared to those who do not live alone, the pooled adjusted HR (AHR) is 1.45 (95% CI: 1.13–1.77, I2 = 77.31%). Additionally, eight studies, involving a combined sample of 3,442,869 participants, investigated the association between living alone and suicide death (14, 15, 18, 29–33). Table 2 illustrates these findings, living alone is linked to the subsequent suicide death, with an AHR of 1.27 (95% CI: 1.06–1.48, I2 = 59.48%) (Supplementary Figure S2).
Subgroup analyses of the extent of the relationship between living alone and suicide death
Subgroup analyses were performed to assessment suicide death, considering factors such as gender (Female/Male), continent (Europe/America/Asia), sample type (The general population/Patients with psychiatric problems), and follow-up durations (≤10/>10 years). The consistent findings reveal that males who live alone face a significantly elevated risk of suicide death in comparison to those who do not, with an AHR of 1.26 (95% CI: 1.15–1.37, I2 = 59.56%). Significant difference was observed between females and males (p = 0.02). Furthermore, the study results did not exhibit significant variability across continents, sample types, and follow-up durations. Nonetheless, it’s noteworthy that individuals living alone in Europe exhibit a higher likelihood of suicide compared to those not living alone (AHR = 1.40, 95% CI: 1.01–1.80, I2 = 66.04%). In the general population, living alone was similarly associated with an increased risk of suicide compared to those not living alone (AHR = 1.33, 95% CI: 1.05–1.61, I2 = 47.14%). Furthermore, studies with follow-up periods exceeding 10 years indicated that individuals living alone are more likely to die by suicide than those not living alone (AHR = 1.20, 95% CI: 1.01–1.39, I2 = 51.20%). For further details, please refer to Table 3 and Supplementary Figures S3–S6.
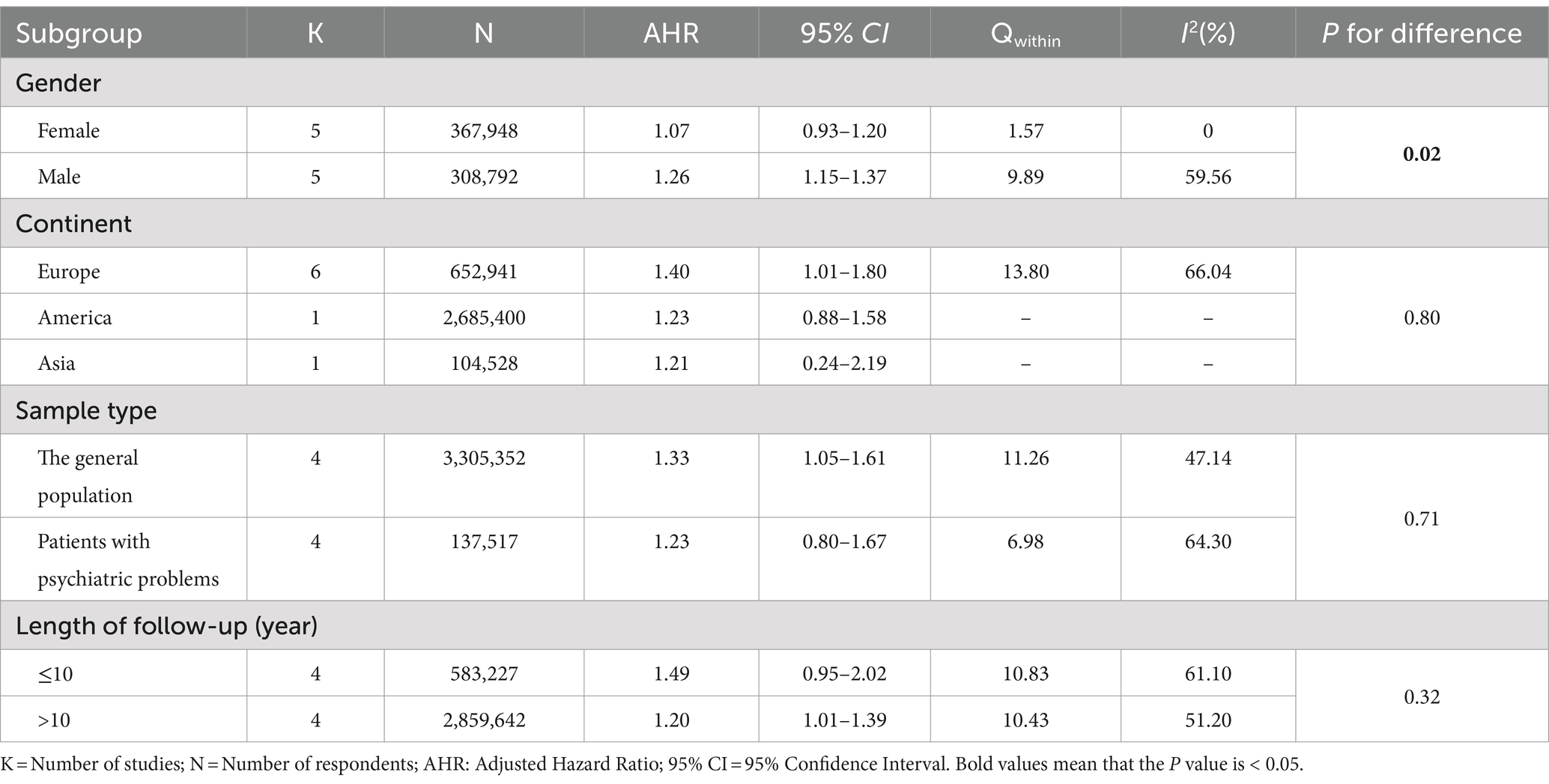
Table 3. Subgroup analysis of the magnitude of the association between living alone and suicide death.
Sensitivity analyses and publication bias
The results of the sensitivity analysis indicated that the estimated prevalence of living alone remained within the 95% confidence interval of the overall combined prevalence, regardless of the exclusion of any individual study. Furthermore, the sensitivity analysis revealed that the prevalence of living alone, upon the exclusion of each study, ranged from 0.28 (95% CI: 0.16–0.41) to 0.35 (95% CI: 0.23–0.47), with all p-values being 0.00 (Supplementary Figure S7). Similarly, after excluding each study, the hazard ratio between living alone and suicide death ranged from 1.21 (95% CI: 1.03–1.38) to 1.33 (95% CI: 1.05–1.61), and all p-values were 0.00 (Supplementary Figure S8). The results of Egger’s publication bias test for both the prevalence of living alone and the adjusted hazard ratio between living alone and suicide death were p = 0.053 and p = 0.177, respectively. Consequently, there was no clear evidence of publication bias (Supplementary Figures S9, S10).
Discussion
Our study constitutes a systematic review of nine large-scale prospective studies conducted worldwide. The primary purpose was to examine whether living alone can predict subsequent suicidal behavior and to determine the strength of this association. This review emphasizes that, as the duration of living alone increases, individuals who live alone are more likely to engage in suicidal behavior compared to those who do not. Additionally, our meta-analysis reveals how factors such as gender, continent, sample type, and follow-up duration influence the extent of the association between living alone and suicide death.
The global prevalence of living alone
A meta-analysis of nine large-scale prospective studies found that the prevalence of living alone was 32% (95% CI: 19–44%, I2 = 100%, p < 0.001), which is similar to previous findings, especially in the middle-aged and older adults population (35, 36). With declining birth rates and an aging global population, social arrangements have undergone significant changes. Many older adults individuals choose to live alone following the death of a spouse, particularly those without children or whose children live far away, leading to a marked increase in single-person households (37, 38). In some European countries, traditional family structures are shifting, with nuclear and single-person households becoming more common, while intergenerational cohabitation has become relatively rare. This cultural shift reflects society’s growing acceptance of independent and autonomous living (39, 40). Furthermore, values that emphasize individualism and self-fulfillment have heightened the demand for independent living, as people increasingly prefer to maintain a self-directed lifestyle. Economic improvements, particularly in developed countries, along with extensive social welfare systems, have fostered economic independence, contributing to a preference for living alone (41–43). Overall, social changes, growing economic independence, shifting cultural values, and other factors have all contributed to the increasing prevalence of living alone in modern society.
Although this study confirmed the prevalence of living alone, the high heterogeneity and narrow confidence intervals revealed by the I2 statistic have affected the credibility of our meta-analysis results. This significant heterogeneity may be attributed to the large sample sizes included in the analysis, which encompass a broad range of populations and span various age and gender distributions. Additionally, the diversity in living arrangements and sociocultural customs across different regions may also contribute to the observed heterogeneity. Given the presence of high heterogeneity, we employed a random effects model in our meta-analysis to better manage and account for the variability between studies, thereby enhancing the robustness and applicability of the analysis results.
Living alone had long-lasting effects on suicidal behaviors
Previous studies have found that living alone increases the risk of suicidal behaviors, however, given the limitation that these analyses were based on cross-sectional studies, we will examine for the first time the relationship between living alone and the risk of suicidal behaviors in the context of longitudinal study data. The findings from this study suggest that, over time, living alone increases the risk of suicide attempts and suicide death by 45 and 27%, respectively. The association remained statistically significant even after controlling for a comprehensive set of covariates to the greatest extent possible, indicating that living alone maintains its independent influence.
The Interpersonal Theory of Suicide, developed by psychologist Thomas Joiner, provides a framework for understanding how living alone contributes to suicidal behavior (44). This theory emphasizes that suicidal thoughts arise from two interrelated but distinct factors: unmet belongingness and the perception of being a burden to others or society. It outlines the progression from ‘experiencing dangerous events’ to ‘developing suicidal thoughts’ and ultimately to ‘engaging in suicidal behavior’ (45). While individuals living alone may enjoy greater freedom and personal space, they are also at risk of experiencing loneliness, a key predictor of suicidal ideation. Prolonged loneliness can lead to a lack of belonging and feelings of hopelessness (46, 47). Additionally, those living alone may avoid social activities due to factors such as social anxiety or poor social skills, resulting in social isolation. This isolation not only exacerbates loneliness but also weakens social support networks, making it harder for individuals to seek help in times of need (48, 49). Furthermore, living alone may facilitate the means and opportunity for engaging in suicidal behavior.
However, there was significant heterogeneity in the association between living alone and suicide mortality. To address this, we conducted subgroup analyses to explore the sources of heterogeneity and discussed in detail the impact of potential confounders on the study results.
Subgroup analysis revealed that men living alone are more likely to die by suicide than women, consistent with previous research findings (50, 51). One valuable and important finding was that gender difference was statistically significant for the relationship between living alone and death by suicide. This disparity may be attributed to differences in social support, help-seeking behaviors, choice of suicide methods, and the impact of health and economic factors. Some studies have indicated the divergent preferences for suicide methods between men and women (52), men are more likely to choose highly lethal methods, such as jumping or hanging, while women are more inclined to use less fatal methods, such as drowning or medication overdose (14). Additionally, men living alone, especially older men, are more prone to undiagnosed or untreated physical and mental health issues, such as depression and alcohol dependence (53, 54), both of which are strongly associated with suicide risk.
Another subgroup analysis was related to geographic location. The majority of the included studies were from Europe, with only one study each from America and Asia. Therefore, caution is advised when interpreting the association between living alone and suicide mortality across different regions. Individuals living alone in Europe face a higher risk of suicide compared to those in America and Asia. This disparity may be attributed to a combination of sociocultural factors, including social isolation caused by individualistic culture, limited family support, the hidden of mental health issues, and reduced participation in social activities, particularly among older adults (55, 56). Many European countries are facing significant challenges related to population aging (57). As life expectancy increases, more and more older adults people choose to live alone or have to live alone. These older adults people often face problems such as widowhood, deteriorating physical health, and loss of social roles, which are recognized risk factors for suicide. In some European countries, suicide is historically or culturally viewed as a personal choice, and societal attitudes toward suicidal behavior are relatively tolerant (58). Similarly, in the Americas, many people who live alone place a high value on individualism and free will, which can influence their perspectives on suicide (59, 60). In some cases, suicide might be viewed as the ultimate expression of control over one’s own destiny. While this is not a mainstream belief, it reflects the cultural emphasis on personal freedom and autonomy. In Asia, particularly in Japanese culture, suicidal behavior is sometimes given a special meaning, especially under the influence of the “Bushido” spirit (61). This cultural concept may make it easier for some people to choose suicide as a solution when faced with difficulties or despair. Although modern society broadly promotes suicide prevention, this cultural legacy may subconsciously influence societal attitudes toward suicide, potentially resulting in inadequate prevention efforts or delayed social interventions.
Our subgroup results showed a puzzling finding that the association between living alone and suicide death was significant in the general population but not in those with psychiatric problems. This may be due to living alone has a stronger independent effect on suicide risk in the absence of other significant risk factors, whereas among people with mental problems, mental illness itself is the main driver of suicide risk. Therefore, the effect of living alone on suicide risk in these populations may be less prominent than the effect of mental illness. In other words, the presence of mental illness masks the effect of living alone. In the general population, living alone may be seen as a sign of isolation and helplessness, and psychological crises are not easily discovered by the outside world, increasing the risk of suicide. However, people with mental problems are usually considered a high-risk group, so society and family members may be more likely to be alert and intervene.
The results showed that variations in the length of follow-up did not exert a significant impact on the risk of suicide death among individuals living alone. The impact of follow-up time on suicidal behavior among individuals living alone may be obscured or weakened by various factors, including the individual’s living conditions, the effectiveness of intervention measures, and the methods of data collection and analysis. It’s crucial to emphasize that prolonged living alone does not necessarily lead to suicidal behaviors, and many individuals effectively manage the challenges associated with living alone while maintaining positive mental health (36).
Strengths and limitations
In this study, we conducted a meta-analysis to assess the extent of the relationship between living alone and suicidal behaviors, aiming to draw a powerful conclusion. This meta-analysis providing comprehensive insights into the impact of living alone on the risk of suicidal behaviors. The study’s strengths include the following aspects: (1) We carried out a comprehensive search across eight major databases and included nine large-scale prospective studies, involving a cumulative total of 3,663,205 participants. The large population size enhances the generalizability of our findings; (2) All data included in the meta-analysis were sourced from database registries or medical records, enhancing the credibility of the study’s findings; (3) We conducted a range of subgroup analyses to identify potential sources of heterogeneity, and the pooled the crude and adjusted effect sizes separately, minimizing the probability of bias.
This study has some limitations. First, there is heterogeneity across cohort designs, such as sample size, duration of follow-up, etc., and the possibility of confounding by other unmeasured factors cannot be ruled out, so the interpretation and generalizability of the results will be limited. Secondly, lack of evidence to explore other subgroup effects that may be of interest, and considerable clinical heterogeneity in some subgroup analyses. For example, age and income should be considered as important factors affecting suicidal behaviors. However, subgroup analyses were not conducted due to inadequate original data. This might conceal some valuable information that affects the association between living alone and suicidal behavior. Furthermore, apart from considering the crude effect size, we chose to focus exclusively on the fully adjusted effect sizes for pooling, which may appear to overlook a substantial amount of information. Finally, the analysis was based on the dichotomous status of living alone or not, without discussion of the quality, commitment, or types of relationships people may be in, which may limit the generalizability of the findings.
Conclusion
This study founded that compared to people who live with others, living alone increases the risk of suicide behaviors. The subgroup analysis revealed that gender, continent, sample type, and follow-up years were potential sources of heterogeneity, indicating that further research should focus on these factors. Additionally, future studies should thoroughly investigate the impact of age, economic status, and sociocultural factors on suicidal behavior among individuals living alone. Given that both living alone and suicide are significant social and psychological issues, future studies need to reveal the relationship between living alone and suicide in detail from the perspective of mixed-methods.
Public health departments should develop targeted policies and plans to improve social welfare systems. These should include enhancing the social support networks for individuals living alone to reduce loneliness and social isolation, strengthening education and publicity on suicide prevention to raise public awareness of the suicide risks of people living alone, and providing easily accessible psychological counseling and support services to assist individuals living alone in managing emotional distress and crises.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
ZL: Conceptualization, Methodology, Writing – original draft, Writing – review & editing, Software. JW: Writing – original draft, Conceptualization, Investigation, Methodology. XC: Data curation, Investigation, Software, Methodology, Writing – original draft. DC: Methodology, Software, Visualization, Writing – review & editing. YZ: Conceptualization, Software, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We gratefully acknowledge all authors who participated in the studies included in the meta-analysis, and the authors who provided the original data for their help in this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1444820/full#supplementary-material
References
1. Esteban, O. The rise of living alone: how one-person households are becoming increasingly common around the world. Oxford: Our World in Data (2019).
2. Anderson, L. Share of one-person households more than tripled from 1940 to (2020). Maryland: United Sates Census Bureau (2023).
3. Cheung, AKL, and Yeung, WJJ. Socioeconomic development and young adults’ propensity of living in one-person households. Demogr Res. (2021) 44:277–306. doi: 10.4054/DemRes.2021.44.11
4. Zhao, Y, Guyatt, G, Gao, Y, Hao, Q, Abdullah, R, Basmaji, J, et al. Living alone and all-cause mortality in community-dwelling adults: a systematic review and meta-analysis. EClinicalMedicine. (2022) 54:101677. doi: 10.1016/j.eclinm.2022.101677
5. World Health Organization. World health statistics 2017: monitoring health for the SDGs. sustainable development goals. Geneva: World Health Organization (2017).
6. Wetherall, K, Cleare, S, Eschle, S, Ferguson, E, O'Connor, DB, O'Carroll, RE, et al. From ideation to action: differentiating between those who think about suicide and those who attempt suicide in a national study of young adults. J Affect Disord. (2018) 241:475–83. doi: 10.1016/j.jad.2018.07.074
7. Franklin, JC, Ribeiro, JD, Fox, KR, Bentley, KH, Kleiman, EM, Huang, X, et al. Risk factors for suicidal thoughts and behaviors: a meta-analysis of 50 years of research. Psychol Bull. (2017) 143:187–232. doi: 10.1037/bul0000084
9. Cerel, J, Brown, M, Maple, M, Singleton, M, Van De Venne, J, Moore, M, et al. How many people are exposed to suicide? Suicide Life Threat Behav. (2019) 49:529–34. doi: 10.1111/sltb.12450
10. McClelland, H, Evans, JJ, Nowland, R, Ferguson, E, and O'Connor, RC. Loneliness as a predictor of suicidal ideation and behaviour: a systematic review and meta-analysis of prospective studies. J Affect Disord. (2020) 274:880–96. doi: 10.1016/j.jad.2020.05.004
11. World Health Organization. Preventing suicide: A global imperative. Geneva: World Health Organization (2014).
12. Shaw, RJP. Living alone and suicide risk: a complex problem requiring a whole population approach. Am J Public Health. (2022) 112:1699–701. doi: 10.2105/AJPH.2022.307138
13. Agerbo, E. Midlife suicide risk, partner's psychiatric illness, spouse and child bereavement by suicide or other modes of death: a gender specific study. J Epidemiol Community Health. (2005) 59:407–12. doi: 10.1136/jech.2004.024950
14. Aaltonen, KI, Isometsä, E, Sund, R, and Pirkola, S. Risk factors for suicide in depression in Finland: first-hospitalized patients followed up to 24 years. Acta Psychiatr Scand. (2019) 139:154–63. doi: 10.1111/acps.12990
15. Shaw, RJ, Cullen, B, Graham, N, Lyall, DM, Mackay, D, Okolie, C, et al. Living alone, loneliness and lack of emotional support as predictors of suicide and self-harm: a nine-year follow up of the UK biobank cohort. J Affect Disord. (2021) 279:316–23. doi: 10.1016/j.jad.2020.10.026
16. Marquet, RL, Bartelds, AI, Kerkhof, AJ, Schellevis, FG, and van der Zee, J. The epidemiology of suicide and attempted suicide in Dutch general practice 1983-2003. BMC Fam Pract. (2005) 6:45. doi: 10.1186/1471-2296-6-45
17. Office for National Statistics Office for National Statistics-suicide in the UK: 2018 registrations. (2019). Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/suicidesintheunitedkingdom/2018registrations (Accessed September 25, 2023).
18. Poudel-Tandukar, K, Nanri, A, Mizoue, T, Matsushita, Y, Takahashi, Y, Noda, M, et al. Differences in suicide risk according to living arrangements in Japanese men and women--the Japan public health center-based (JPHC) prospective study. J Affect Disord. (2011) 131:113–9. doi: 10.1016/j.jad.2010.11.027
19. Abell, JG, and Steptoe, A. Why is living alone in older age related to increased mortality risk? A longitudinal cohort study. Age Ageing. (2021) 50:2019–24. doi: 10.1093/ageing/afab155
20. Renwick, KA, Sanmartin, C, Dasgupta, K, Berrang-Ford, L, and Ross, N. The influence of low social support and living alone on premature mortality among aging Canadians. Can J Public Health. (2020) 111:594–605. doi: 10.17269/s41997-020-00310-9
21. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. (2021) 10:89. doi: 10.1186/s13643-021-01626-4
22. Stroup, DF, Berlin, JA, Morton, SC, Olkin, I, Williamson, GD, Rennie, D, et al. Meta-analysis of observational studies in epidemiology: a proposal for reporting. JAMA. (2000) 283:2008–12. doi: 10.1001/jama.283.15.2008
23. Ouzzani, M, Hammady, H, Fedorowicz, Z, and Elmagarmid, A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. (2016) 5:1–10. doi: 10.1186/s13643-016-0384-4
24. Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. (2010) 25:603–605. doi: 10.1007/s10654-010-9491-z
25. Lo, CKL, Mertz, D, and Loeb, M. Newcastle-Ottawa scale: comparing reviewers’ to authors’ assessments. BMC Med Res Methodol. (2014) 14:1–5. doi: 10.1186/1471-2288-14-45
26. Wells, GA, Shea, B, and O’Connell, D. The Newcastle-Ottawa scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. (2014) Availabe at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (Accessed September 8, 2024).
27. Higgins, J, and Green, S. Cochrane handbook for systematic reviews of interventions The Cochrane Collaboration. John Wiley & Sons, Ltd., Publication. (2011).
28. Higgins, JP, Thompson, SG, Deeks, JJ, and Altman, DG. Measuring inconsistency in meta-analyses. BMJ. (2003) 327:557–60. doi: 10.1136/bmj.327.7414.557
29. Burrows, S, Auger, N, Gamache, P, St-Laurent, D, and Hamel, D. Influence of social and material individual and area deprivation on suicide mortality among 2.7 million Canadians: a prospective study. BMC Public Health. (2011) 11:1–11. doi: 10.1186/1471-2458-11-577
30. Hansson, C, Joas, E, Palsson, E, Hawton, K, Runeson, B, and Landén, M. Risk factors for suicide in bipolar disorder: a cohort study of 12 850 patients. Acta Psychiatr Scand. (2018) 138:456–63. doi: 10.1111/acps.12946
31. Rahman, S, Alexanderson, K, Jokinen, J, and Mittendorfer-Rutz, E. Risk factors for suicidal behaviour in individuals on disability pension due to common mental disorders—a nationwide register-based prospective cohort study in Sweden. PLoS One. (2014) 9:e98497. doi: 10.1371/journal.pone.0098497
32. Wang, M, Alexanderson, K, Runeson, B, and Mittendorfer-Rutz, E. Sick-leave measures, socio-demographic factors and health care as risk indicators for suicidal behavior in patients with depressive disorders—a nationwide prospective cohort study in Sweden. J Affect Disord. (2015) 173:201–10. doi: 10.1016/j.jad.2014.10.069
33. Schneider, B, Lukaschek, K, Baumert, J, Meisinger, C, Erazo, N, and Ladwig, KH. Living alone, obesity, and smoking increase risk for suicide independently of depressive mood findings from the population-based MONICA/KORA Augsburg cohort study. J Affect Disord. (2014) 154:416–21. doi: 10.1016/j.jad.2013.10.007
34. Eriksson, M, Glader, EL, Norrving, B, and Asplund, K. Post-stroke suicide attempts and completed suicides: a socioeconomic and nationwide perspective. Neurology. (2015) 84:1732–8. doi: 10.1212/WNL.0000000000001514
35. Raymo, JM. Living alone in Japan: relationships with happiness and health. Demogr Res. (2015) 32:1267–98. doi: 10.4054/DemRes.2015.32.46
36. Tamminen, N, Kettunen, T, Martelin, T, Reinikainen, J, and Solin, P. Living alone and positive mental health: a systematic review. Syst Rev. (2019) 8:134. doi: 10.1186/s13643-019-1057-x
37. Eurostat. Statistics explained. Household composition statistics. (2020) Available at: http://ec.europa.eu/eurostat/statisticsexplained/index.php/Household_composition_statistics (Accessed October 20, 2023).
38. Jamieson, L, and Simpson, R. Living alone: Globalization, identity and belonging. Cham: Springer (2013).
39. Snell, KDM. The rise of living alone and loneliness in history. Soc Hist. (2017) 42:2–28. doi: 10.1080/03071022.2017.1256093
40. Wall, R. Leaving home and living alone: an historical perspective. Popul Stud. (1989) 43:369–89. doi: 10.1080/0032472031000144196
41. Burlina, C, and Rodríguez-Pose, A. Alone and lonely. The economic cost of solitude for regions in europe. EPA. (2023) 55:2067–87. doi: 10.1177/0308518X231169286
42. Mudrazija, S, Angel, J, Cipin, I, and Smolic, S. Living alone in the United States and Europe: the impact of public support on the independence of older adults. Res Aging. (2018) 42:150–62. doi: 10.1177/0164027520907332
43. Reher, D, and Requena, M. Living alone in later life: a global perspective. Popul Dev Rev. (2018) 44:427–54. doi: 10.1111/padr.12149
44. Van Orden, KA, Witte, TK, Cukrowicz, KC, Braithwaite, SR, Selby, EA, and Joiner, TE. The interpersonal theory of suicide. Psychol Rev. (2010) 117:575–600. doi: 10.1037/a0018697
45. Chu, C, Buchman-Schmitt, JM, Stanley, IH, Hom, MA, Tucker, RP, Hagan, CR, et al. The interpersonal theory of suicide: a systematic review and meta-analysis of a decade of cross-national research. Psychol Bull. (2017) 143:1313–45. doi: 10.1037/bul0000123
46. Huang, M, Liu, K, Liang, C, Wang, Y, and Guo, Z. The relationship between living alone or not and depressive symptoms in older adults: a parallel mediation effect of sleep quality and anxiety. BMC Geriatr. (2023) 23:506. doi: 10.1186/s12877-023-04161-0
47. Wu, D, Liu, F, and Huang, S. Assessment of the relationship between living alone and the risk of depression based on longitudinal studies: a systematic review and meta-analysis. Front Psych. (2022) 13:954857. doi: 10.3389/fpsyt.2022.954857
48. Niu, L, Jia, C, Ma, Z, Wang, G, Sun, B, Zhang, D, et al. Loneliness, hopelessness and suicide in later life: a case–control psychological autopsy study in rural China. Epidemiol Psychiatr Sci. (2020) 29:e119. doi: 10.1017/S2045796020000335
49. Park, JE, Kim, BS, Bae, JN, Kim, KW, Song, SJ, and Cho, MJ. Depressive symptomatology among the living-alone elderly: hopelessness and boredom. J Korean Geriatr Psychiatry. (2012) 16:97–103.
50. Grande, E, Vichi, M, Alicandro, G, Marchetti, S, Frova, L, and Pompili, M. Suicide mortality among the elderly population in Italy: a nationwide cohort study on gender differences in sociodemographic risk factors, method of suicide, and associated comorbidity. Int J Geriatr Psychiatry. (2022) 37:5726. doi: 10.1002/gps.5726
51. Kim, J, Lee, YS, and Lee, J. Living arrangements and suicidal ideation among the Korean older adults. Aging Ment Health. (2016) 20:1305–13. doi: 10.1080/13607863.2015.1078280
52. Pirkola, S, Isometsä, E, and Lönnqvist, J. Do means matter?: differences in characteristics of Finnish suicide completers using different methods. J Nerv Ment Dis. (2003) 191:745–50. doi: 10.1097/01.nmd.0000095127.16296.c1
53. Gillies, CL, Rowlands, AV, Razieh, C, Nafilyan, V, Chudasama, Y, Islam, N, et al. Association between household size and COVID-19: a UK biobank observational study. J R Soc Med. (2022) 115:138–44. doi: 10.1177/01410768211073923
54. Girgus, JS, Yang, K, and Ferri, CV. The gender difference in depression: are elderly women at greater risk for depression than elderly men? Geriatrics. (2017) 2:35. doi: 10.3390/geriatrics2040035
55. Burholt, V. Culture, social isolation and loneliness in later life In: A Hajek, SG Riedel-Heller, and HH König, editors. Loneliness and Social Isolation in Old Age. London: Routledge (2023)
56. Swader, CS. Loneliness in Europe: personal and societal individualism-collectivism and their connection to social isolation. Soc Forces. (2019) 97:1307–36. doi: 10.1093/sf/soy088
57. Luchetti, M, Terracciano, A, Aschwanden, D, Lee, JH, Stephan, Y, and Sutin, AR. Loneliness is associated with risk of cognitive impairment in the survey of health, ageing and retirement in Europe. Int J Geriatr Psychiatry. (2020) 35:794–801. doi: 10.1002/gps.5304
58. Stack, S. Contributing factors to suicide: political, social, cultural and economic. Prev Med. (2021) 152:106498. doi: 10.1016/j.ypmed.2021.106498
59. Eskin, M, Tran, US, Carta, MG, Poyrazli, S, Flood, C, Mechri, A, et al. Is individualism suicidogenic? Findings from a multinational study of young adults from 12 countries. Front Psych. (2020) 11:259. doi: 10.3389/fpsyt.2020.00259
60. Lenzi, M, Colucci, E, and Minas, H. Suicide, culture, and society from a cross-national perspective. Cross-Cult Res. (2012) 46:50–71. doi: 10.1177/1069397111424036
Keywords: living alone, suicide behaviors, prospective studies, systematic review, meta-analysis
Citation: Luo Z, Wang J, Chen X, Cheng D and Zhou Y (2024) Assessment of the relationship between living alone and suicidal behaviors based on prospective studies: a systematic review and meta-analysis. Front. Public Health. 12:1444820. doi: 10.3389/fpubh.2024.1444820
Edited by:
Yuka Kotozaki, Iwate Medical University, JapanCopyright © 2024 Luo, Wang, Chen, Cheng and Zhou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jinfeng Wang, MTQ2NDk3Njg0MUBxcS5jb20=
†These authors have contributed equally to this work and share first authorship