
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health , 13 November 2024
Sec. Environmental Health and Exposome
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1438748
 Getachew Kabew Mekonnen1*
Getachew Kabew Mekonnen1* Abdurauf Zako2,3
Abdurauf Zako2,3 Fitsum Weldegebreal1,4
Fitsum Weldegebreal1,4 Assefa Desalew5,6
Assefa Desalew5,6 Temam Beshir Raru3
Temam Beshir Raru3 Ukash Umer1
Ukash Umer1 Kedir Urgesa1
Kedir Urgesa1Background: Understanding the level of inadequate water, sanitation, and hygiene (WaSH) services in urban and rural settlements is crucial for prioritizing community interventions and resource allocation. However, there is a lack of evidence regarding discrepancies in WaSH services across rural and urban slum communities in Ethiopia.
Objective: This study aims to assess inequalities in households’ WaSH services and their associated factors among urban slums and rural communities in Eastern Ethiopia from February to April 2024.
Methods: A comparative community-based cross-sectional study design was conducted, with study participants selected through stratified random sampling using proportional-to-size allocation. Data were entered into Epi Data version 3.1 and then exported to STATA version 17 for analysis. Bi-variable and multivariable logistic regression was conducted, and associations were reported as odds ratios (ORs) with 95% confidence intervals (CI), using a p-value less than 0.05 as the significance threshold.
Result: A total of 278 urban and 301 rural households participated in the study, with a response rate of 94%. Key indicators showed that WaSH services were significantly better in urban areas compared to rural households. For example, 98% (95% CI: 96, 99) of urban households had access to an improved water source compared to 76% (95% CI: 71, 80) of rural households. The proportion of households with improved latrines was 44% (95% CI: 38, 50) in urban areas and only 14% (95% CI: 11, 19) in rural areas. Handwashing practices at all five critical times were reported by 52% (95% CI: 46, 58) of urban household heads, compared to 22% (95% CI: 18, 27) of rural households. Additionally, occupation (such as being a farmer, p = 0.000) and water service satisfaction (p = 0.000) were significantly associated with these key WaSH outcomes.
Conclusion: The study revealed that the WaSH services in urban slums are considerably better than in rural households. Socioeconomic factors significantly influence the existing disparities in WaSH services. Stakeholders should focus on providing targeted, strategic support to communities to address the challenges in WaSH service provision.
Access to water, sanitation, and hygiene (WaSH) services is crucial and directly linked to the health of individuals and communities (1). It is also known that inadequate WaSH services have significant economic, environmental, and social impacts (2). In 2020, 74% of the global population used safely managed drinking water services, with 60% in rural areas and 86% in urban areas (3). Similarly, 54% of the global population used safely managed sanitation services, 44% in rural areas, and 62% in urban areas. Furthermore, 71% of the global population had basic handwashing facilities with soap and water at home (3). Despite global efforts, WaSH services are still inadequate in sub-Saharan Africa (SSA) (4). Sustainable Development Goal 6 (SDG6) targets universal and equitable services of safe and affordable drinking water, adequate sanitation and hygiene, and ending open defecation by 2030 (5). Inequalities in WaSH services exist in nearly all nations, affecting urban versus rural areas, the rich versus the poor, and marginalized and vulnerable groups (6). Poor people, in particular, are not only vulnerable but also at high risk of disease. In addition, inadequate WaSH disproportionately impacts women and girls living in urban slums (7).
According to the 2022 JMP WaSH report, urban areas in Ethiopia had 81% coverage for safe water, 65% for improved sanitation, and 83% for basic hygiene services. In contrast, rural areas had significantly lower coverage, with 62% for safe drinking water, 46% for improved sanitation, and 65% for basic hygiene (8). Water supply and sanitation are critical, as they involve hygienically isolating human excreta from human contact and drinking water sources to prevent contamination (9). The World Health Organization (WHO) defines improved sanitation facilities as those that effectively separate human excreta from human contact (10). Unsafe water and inadequate sanitation are major causes of diseases such as diarrhea and hookworm infection, posing serious risks to human health (11). In Ethiopia, only 68.7% of households have access to improved drinking water sources, 27.5% of them have improved toilet facilities, and only approximately 38% have handwashing facilities (12). Moreover, there is considerable variation in access to improved WaSH services across different regions of the country (13).
Multiple studies revealed that households with better economic status and education and urban households are more likely to use basic WaSH facilities (14). While such disparities have received significant attention, there are gaps related to other inequalities, such as gender, ethnicity, displacement, migration, and caste, which have been less measured and monitored (15). Many regions worldwide do not have proper facilities and funding to build or maintain WaSH infrastructure, especially in rural areas (16). However, inadequate WaSH services are more common in slum areas, areas dominated by informal settlements that are characterized by one or more of the five characteristics of overcrowding, poor sanitation, insecure land tenure, lack of access to water supply, poor housing quality and other infrastructure (17, 18). Reducing inequalities in all their forms is one of the key principles of the Sustainable Development Goal (SDG) and the principle of equality and non-discrimination, which applies to all human rights. However, there is a lack of evidence addressing the inequalities in access to WaSH services between the poorest rural society and urban slum communities in the study area. Therefore, this study aimed to evaluate inequalities in access to WaSH services and associated factors in rural and urban slum communities in Eastern Ethiopia.
This study was conducted in the Babile District of the Oromia Regional State and the Amir Nur District of the Harari Regional State. The two districts were randomly selected to represent the rural and urban slum communities. Harari Regional State is one of the regions in Ethiopia, located 526 km away from Addis Ababa to the east. This regional state includes nine districts. Amir Nur district is one of the urban districts with slum settlements in the Harari regional state that includes three urban slums, Kebeles, namely 01, 02, and 07, and it has 24,215 total population. The populations of 01, 02 and 07 Kebeles are 10, 674, 7,713, and 5,828, respectively. The urban Kebele 01 has an urban slum, Ganda Fero village and it includes 1,178 households with 685 vulnerable children under five. The other rural study sites were Bisidimo and Ifadin Kebelles in Babile district, which is located 540 km away from Addis Ababa and 23 km from Harar town in the eastern direction. The number of children aged from 1 to 15 years of age in Bisidimo and Ifadin Kebeles is 3,582, according to the unpublished Babile district administration report, 2023.
A community-based comparative cross-sectional study was conducted from February to April 2024 in the Babile District of Oromia Regional State and the Amir Nur District of Harari Regional State, Eastern Ethiopia.
All households in rural and urban slum kebeles in Babile District of Oromia Regional State and the Amir Nur District of Harari Regional State, respectively, were the source population. The study populations were all randomly selected household heads within the selected rural and urban slum kebeles who were available during the study period. All household heads who were volunteers and lived at least 6 months in the study sites were included in the study.
Households that were closed at the time of the visit and heads who were not volunteers or had not lived in the area for at least the previous 6 months were excluded from the study.
All household heads who were volunteers and lived at least 6 months in the study site were included.
Households that were closed at the time of the visit and heads who are not volunteers and have not lived for at least the previous 6 months were excluded from the study.
The sample size was determined using a household survey formula where the proportion of 11.4 and 25% sanitation coverage in slum and rural areas of Ethiopia, respectively (19), with the assumption of precision or degree of error 0.05, confidence interval 95%, and non-response rate assumed to be 10%. We doubled the sample size considering the stratified analysis based on the type of residences and samples distributed proportionally to the number of rural and urban households in the Babile and Amir Nur districts, respectively. Thus, the rural district = 320 households, the urban district = 296 households, and the total sample size was 616. The target households were included in the study using systematic random sampling techniques.
Households with a handwashing facility with soap and water available on-premises meet the criteria for a basic hygiene service (20). Handwashing with water and soap at five critical times: before eating, after the toilet, after cleaning the child’s bottom, before preparing food, and before feeding the child.
Washing hands with soap and water after toilet visits, after cleansing the child’s defecated buttock, before cooking (preparing food), before eating, and before feeding the child.
Improved sanitation facilities are those designed to hygienically separate excreta from human contact (20). These include wet sanitation technologies, such as flush and pour flush toilets connected to sewers, septic tanks, or pit latrines, and dry sanitation technologies, such as dry pit latrines with slabs and composting toilets.
Improved drinking water sources are those that, by nature of their design and construction, have the potential to deliver safe water that is accessible and available when needed (21). This includes piped water, boreholes or tube wells, protected dug wells, protected springs, rainwater, and packaged or delivered water.
For the practice questions, each correct response was valued as one, while incorrect responses were marked as zero. All the scores were added, and the mean score was calculated. Respondents who had scores below the mean value were categorized as having poor practice, while those who scored above the mean value were categorized as having good practice.
Urban settlements dominated by households of individuals living under the same roof lacking one or more of the following conditions: • Sufficient living area •Access to improved water •Access to improved sanitation •Durability of housing •Security of tenure (22).
The proportion of households that have access to an improved water source, an improved latrine, or those house heads practicing handwashing with water and soap at five critical times.
The project members developed a semi-structured questionnaire and an observation checklist with input from JMP (23). Fluent local language speaker numerators attended a 2-day training on the methods and tools. The data were collected using ODKA, and the tools were pretested on 5% of household heads in the non-selected Kebeles 7 days before the actual data collection to ensure the quality of the data collection tool. A questionnaire-based interview was conducted among heads, primarily mothers of the selected households, because women house heads have better knowledge about the existing WASH services. Spot checks of household WaSH services were held by a supervisor and the research team. The collected data was checked daily for completeness and consistency. Double data entry was done and cross-checked to ensure consistency. The investigators and supervisors coordinated all over the data collection process and took immediate corrective actions accordingly.
Epi Data version 3.1 was used for data entry, and the data were then exported to STATA version 17 for analysis. Descriptive statistics were calculated and presented in tables and figures. Household WaSH services were compared, and a Chi-square test at a 95% significant level was computed to assess differences in access to basic WaSH services between urban slums and rural communities. Bi-variable and multivariable logistic regression analysis was conducted to identify associations between independent variables and outcome variables.
A variance inflation factor (VIF) was used to assess multicollinearity. Variables with a p-value less than 0.25 were included in the bivariate analysis and subsequently used in multivariable analysis to control for all potential confounders. Odds ratios (ORs) were calculated to determine the strength of the association. A p-value of ≤0.05 with a 95% confidence interval (CI) was considered statistically significant.
Ethical approval was obtained from the College of Health and Medical Sciences Institutional Health Research Ethics Review Committee (Ref. No. IHRERC/056/24). Informed, voluntary, written, and signed consent was provided by house heads. The study group (househeads) who participated in the study was informed in the local language (Amharic and Afanoromo) about the study procedure and duration, following which they obtained consent. Data collected from the study group were kept confidential, and households had the right to withdraw from the study at any time. Necessary permissions were obtained from the district health office of Babile in east Hararghe of the Oromia region and the Amir Nur district health office of Harari regional state.
A total of 278 urban and 301 rural households participated in the study, with a response rate of 94%. The mean income in urban slum households was 5,457.527 Ethiopian Birrs (SD: 2,617.87), whereas it was 3,401.015 Ethiopian Birrs (SD: ±1,312.1) in rural households. In this study, monthly income was used as an economic status indicator for households. Although income analysis of households may be inadequate, it is a cost-effective measure, and using a good sample makes it possible to analyze inequalities in a specific area. Households that earn more than the mean monthly income (4,404 Et. Birr) were considered to have a good income. Nearly 93% (532) of the house heads were married, while 70% (408) had no formal education (Table 1).
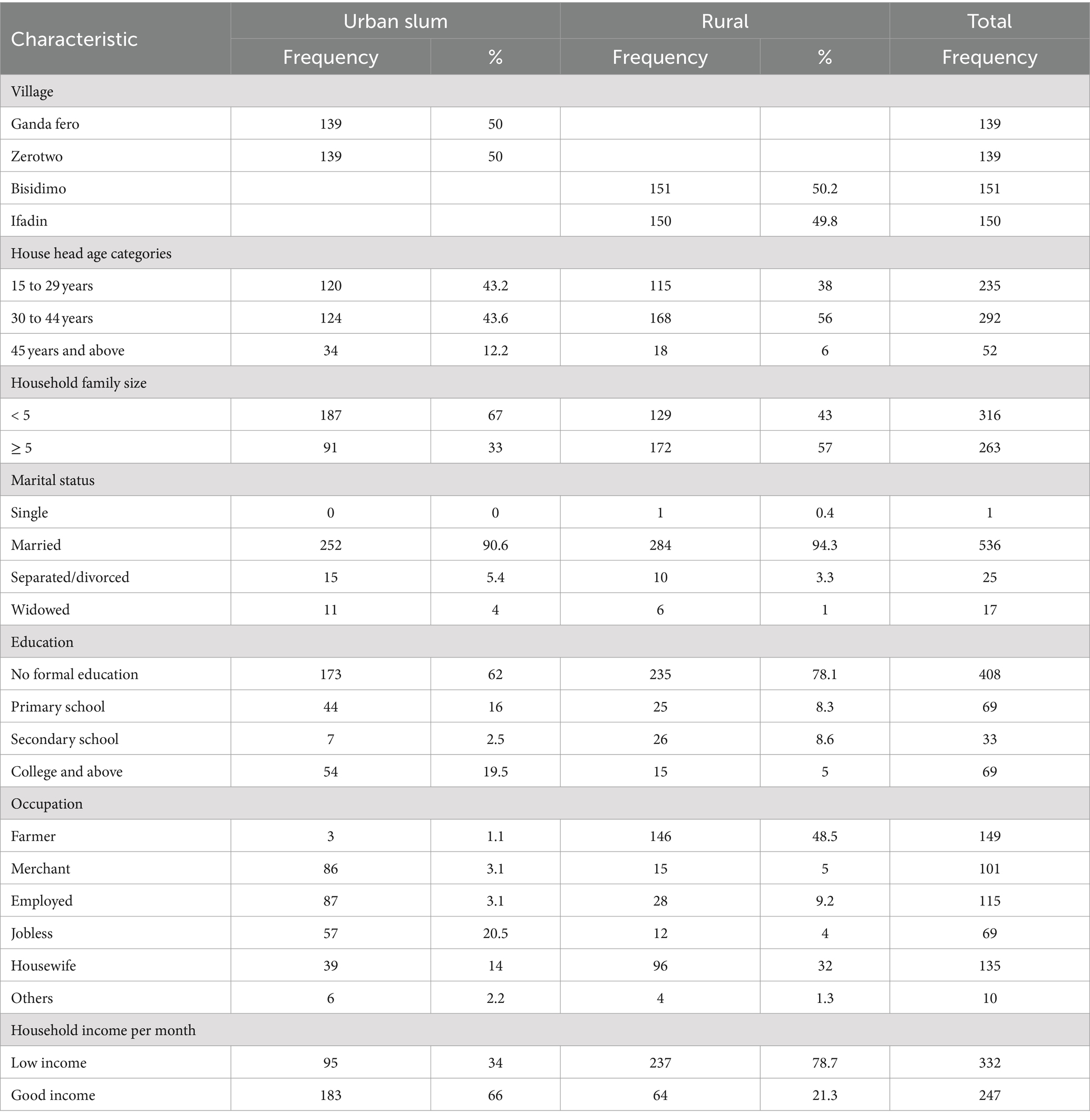
Table 1. Sociodemographic characteristics of households participated in WaSH inequalities assessment in Eastern Ethiopia, 2024 (n = 579).
The chi-square test showed that there are significant WaSH service inequalities in urban slums and rural households. More than 98% (95% CI: 96, 99) of the urban slum communities utilized improved water sources, while improved water source coverage was approximately 76% (95% CI: 71, 80) in rural households. The mean volume of water utilized per day per capita was 11.5 L. The mean distance of the household from the water source was 34.625 (SD: 112.6898) and 729.0317 (SD: 2458.032) in urban and rural areas, respectively. Water shortages were observed in 20% of urban and 48.7% of rural households within the previous month prior to the study. Approximately 8.3% of the urban households were satisfied with their water services, in contrast with 55% of the rural households (Figure 1). Nearly equal proportions, 90% of the urban and rural communities, did not get a standard minimum 20 L per day per capita water volume for drinking and domestic hygiene purposes. However, there was a greater trend of water service interruptions in rural areas than in urban areas.
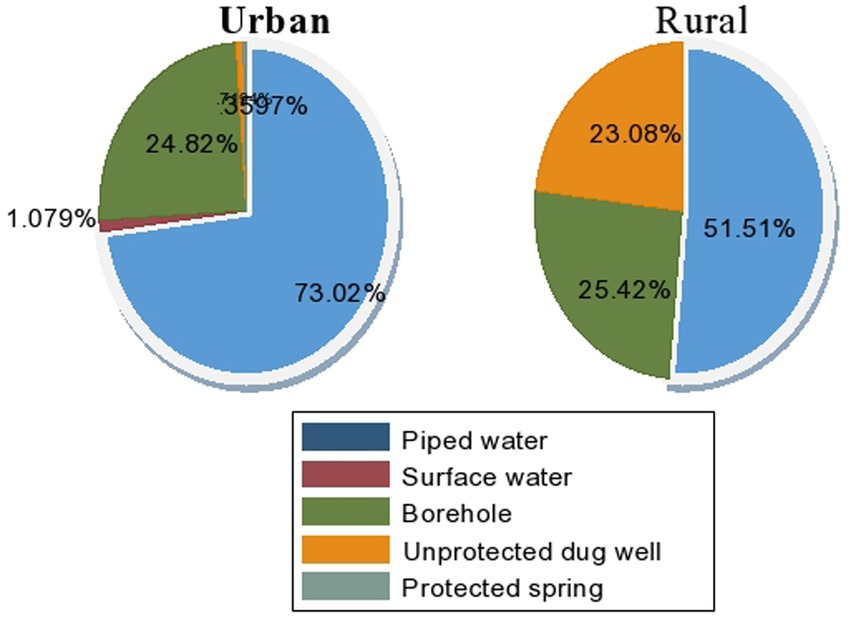
Figure 1. Type of drinking water sources in Amir Nur and Babile districts in Eastern Ethiopia, 2024 (n = 579).
Approximately 81% of the urban slums and 76.6% of the rural households had some kind of toilet. Improved latrine was 44% (95% CI: 38, 50) in urban households and 14% (95% CI: 11, 19) in rural households. Furthermore, only 5.7 and 2% of urban and rural households had handwashing setups near their toilets, respectively. In contrast, the proportion of handwashing practices at all five critical times among urban house heads was 52% (95% CI: 46, 58), and it was 22% (95% CI: 18, 27) (Table 2). This is because the majority of the people in Eastern Ethiopia are Muslims and tend to frequently practice handwashing for religious reasons. However, they are mainly using portable small water containers instead of installing handwashing setups attached to the toilet. Similarly, the current study found that the most common handwashing practice was observed before eating food in both urban slums (71%) and rural (64%) communities (Figure 2).
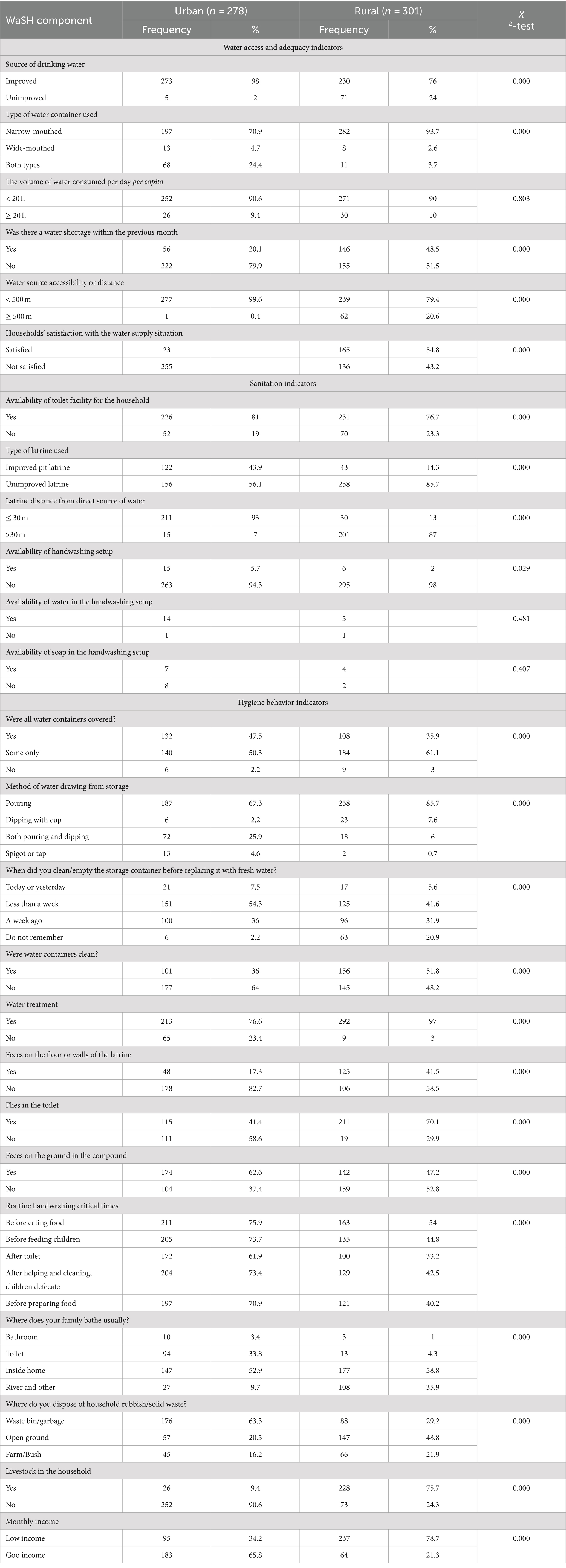
Table 2. WaSH service inequalities among rural and urban slum communities in Babile District of Oromia Regional State and Amir Nur District of Harari Regional State, Eastern Ethiopia, 2024 (n = 579).
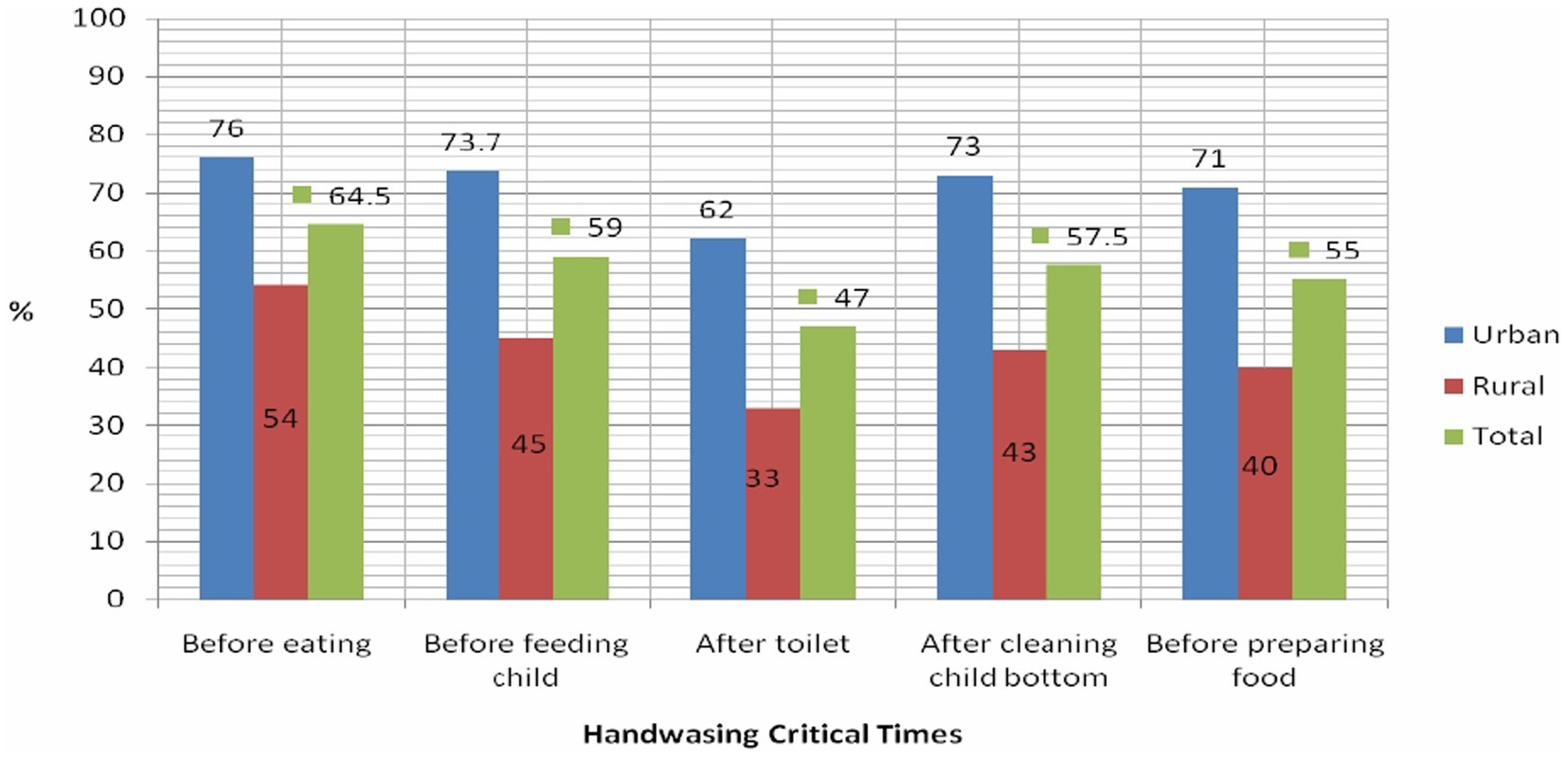
Figure 2. Hand washing practices of household heads at critical time in Amir Nur and Bisidimo districts in Eastern Ethiopia, 2024 (n = 579).
In this study, we used Key JAMP WaSH service indicators—availability of an improved water source, availability of an improved latrine, and handwashing practices at five critical times—to assess the major factors associated with existing WaSH services in urban slums and rural households (21, 24). Accordingly, variables such as residence, age of respondents, educational status, occupation, monthly income, family size, and satisfaction with the water situation showed statistically significant associations with the three key WaSH indicators. All variables with a p-value less than or equal to 0.25 were considered for multivariable analysis. In multivariable analysis, variables such as residence, age of respondents, educational status, occupation, family size, and satisfaction with the water situation remained statistically significant at a p-value of less than 0.05 (Table 3).
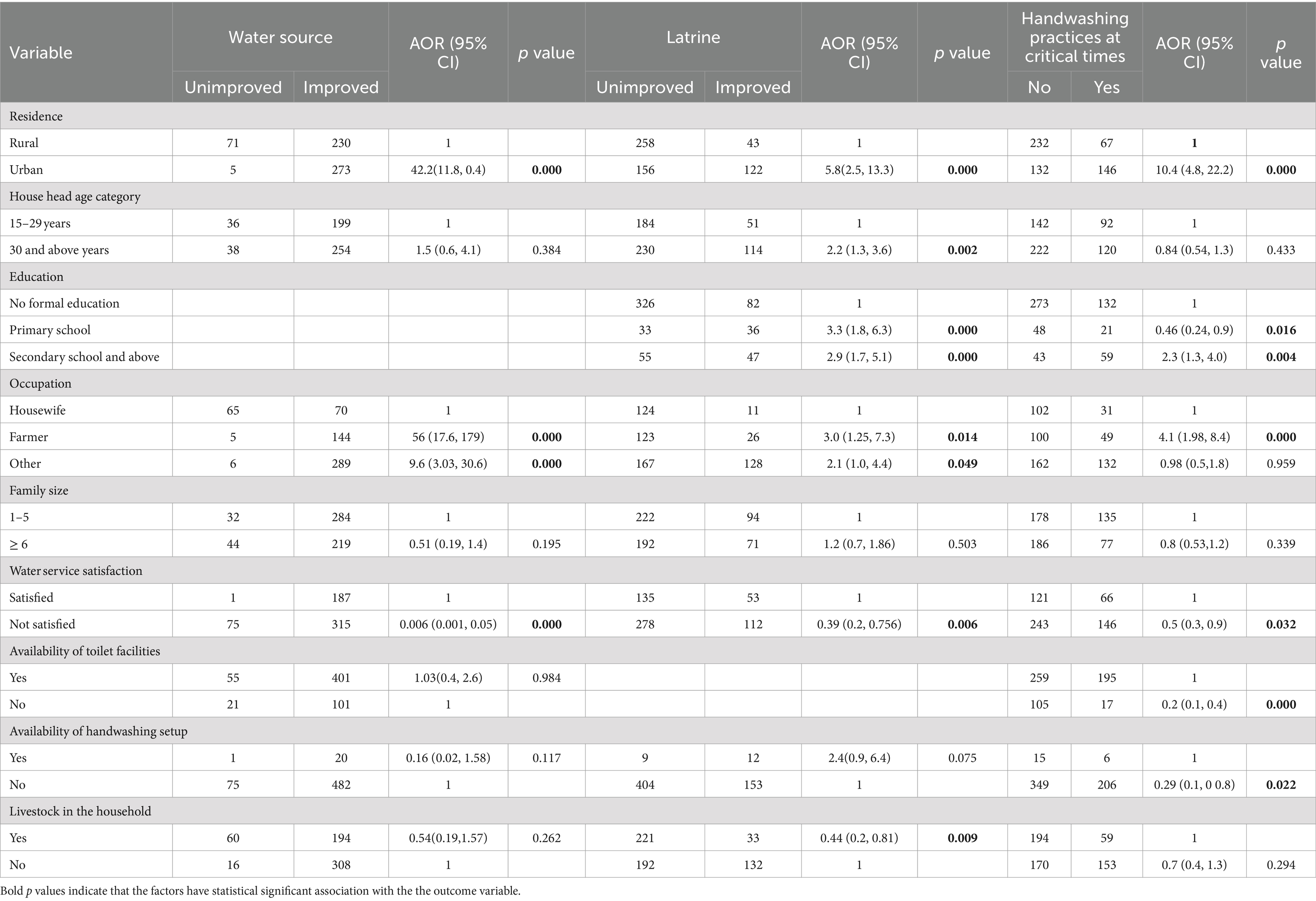
Table 3. Associated factors of WaSH services.
Generally, WaSH services are significantly higher in urban than rural households. This included access to an improved water source (AOR; 42.2, 95% CI; 11.8, 150.4), improved latrine facilities (AOR; 5.8, 95% CI; 2.5, 13.3), and handwashing practices at five critical times (AOR; 10.4, 95% CI; 4.8, 22.2). Types of occupation such as farmers (p = 0.000) and other jobs (p = 0.000) were significantly associated with existing improved water services compared to housewives. Furthermore, household satisfaction with water services (p = 0.000) was strongly associated with the availability of improved water sources (Table 3).
In terms of improved latrine availability, significant associations were found with the household head’s age (30 years and above, p = 0.002) and education levels—primary (p = 0.000) and secondary and above (p = 0.000). Additionally, occupations such as farmers (p = 0.014), other jobs (p = 0.049), household satisfaction with the existing water service (p = 0.006), and the availability of livestock in the household (p = 0.009) were significantly associated with the type of latrine used by the households.
In this current study, handwashing practices were assessed by categorizing participants who washed their hands at all five critical times—after using the toilet, before eating, before food preparation, after handling babies’ excreta, and before feeding a child—as having good handwashing practices. Participants who failed to wash their hands at any of these critical times were categorized as having poor handwashing practices. Significant associations were found with primary school education (p = 0.016), secondary school education (p = 0.004), occupation as farmers (p = 0.000), satisfaction with current water services (p = 0.032), availability of toilet facilities (p = 0.000), and availability of handwashing facilities (p = 0.022), all of which were linked to better handwashing practices at the five critical times.
Relevant actors in the WaSH domain now acknowledge that various social and economic inequalities mediate access to WaSH services (14, 15, 25, 26). The current study assessed these inequalities and found that virtually all indicators demonstrated significantly higher levels of WaSH services in urban slums compared to rural households. The proportion of households with good monthly income was also significantly higher in urban slums than in rural settings (p = 0.000). Rural populations typically have lower incomes than their urban counterparts in developing countries, a gap that can be attributed to disparities in education, job experience, and occupational categories (27).
It is well established that a household’s wealth index and monthly income significantly influence access to WaSH services (28), with wealthier households being more likely to have access to improved WaSH services compared to the poorest households (29, 30). This rural–urban inequality presents a significant challenge for authorities, who are encouraged to pursue spatially optimized policy reforms rather than implementing uniform nationwide measures.
The current study found that coverage of improved water sources was 98% (95% CI; 95.7–99.2%) in urban slums and 76% (95% CI; 71.2–80.6%) in rural communities. The availability of improved water sources was significantly higher in urban slums than in rural communities (AOR; 42.2, 95% CI; 11.8–150.4). While approximately 90% of households in both communities accessed less than 20 L of water per capita per day, water shortages were more prevalent in rural households than in urban slums. These findings, though varying in degree, align with the WHO SDGs five-year report (23).
Access to improved water sources was strongly associated with occupations, such as farming (AOR; 56, 95% CI; 17.6, 179) and other jobs (AOR; 9.6, 95% CI, 3.03, 30.6) when compared to housewives. This finding indicates a lower level of WaSH service awareness among housewives in the study areas. Additionally, households whose heads were dissatisfied with the available water services were approximately 100% less likely to have access to an improved water source compared to those who were satisfied. Household satisfaction with existing water services has been shown to have a positive and significant impact on ‘the improvement of WaSH services and the willingness to pay for those services (31).
Regarding sanitation, households in urban slums were six times more likely to have improved latrines compared to rural households, a finding consistent with other studies (23, 32). This result is in agreement with other similar studies and highlights the ongoing challenge of WaSH service inequalities in developing countries (33, 34). Our study showed that household heads aged 30 years and above were twice as likely to use improved latrines compared to those under 30 years. This finding is consistent with other similar studies and could indicate that the majority of individuals in this age group are economically active and better able to afford improved sanitation facilities (35).
Additionally, household heads with primary education (AOR; 3.3; 95% CI: 1.8, 6.3) and secondary or higher education (AOR; 2.9, 95% CI; 1.7, 5.1) were more likely to use improved latrines compared to those without formal education. This result mirrors findings from other studies, which suggest that educated household heads are more likely to adopt improved latrine practices than those without education (35, 36). Education plays a critical role in enabling individuals to make informed health decisions and to wisely allocate resources toward building and using improved latrine facilities (37).
Similarly, individuals working as farmers or in other occupations were at least three and two times more likely, respectively, to have improved latrines compared to housewives. This finding contrasts with other studies, possibly due to sociocultural differences between study areas. Additionally, households where the head was dissatisfied with the existing water service were 61% less likely to have improved latrines than those who were satisfied. Furthermore, households with livestock were 56% less likely to use improved latrines compared to those without livestock. In developing countries, farmers with lower levels of education are more likely to own livestock and less likely to build improved latrines, often resorting to open defecation (38).
In our study, good handwashing practices were defined as washing hands with water and soap at five critical times: before eating food, before preparing food, before feeding children, after using the toilet, and after helping or cleaning children. The results showed that good handwashing practices were 10 times more common in urban slums than in rural households (AOR; 10, 95% CI: 4.8, 22.2). This finding is consistent with other studies from Ethiopia (32). Households led by individuals with secondary and higher education demonstrated 2.3 times better handwashing practices than those led by individuals with no formal education, which aligns with findings from similar studies (39). These results are supported by other research (40, 41), likely because educated household heads tend to have greater awareness of the benefits of good hand hygiene practices.
Additionally, education fosters long-term changes in healthy behaviors and effectively promotes hygiene and sanitation (42). However, participants with only primary education were 54% less likely to wash their hands at critical times. This could be attributed to younger pupils in primary schools typically having incomplete information and a higher risk of poor personal hygiene (43). Surprisingly, farmers were four times more likely to practice good handwashing practices compared to housewives, possibly because housewives may perceive that their hands are clean as they usually stay home.
Household heads who were dissatisfied with the existing water service were 50% less likely to practice good handwashing at critical times, likely due to the necessity of household resources and adequate water services to maintain such practices (44). Households without toilet facilities were 80% less likely to have good hygiene practices compared to those with toilet facilities, as sanitation infrastructure promotes better hygiene practices among adults (45). Additionally, households lacking handwashing setups were 71% less likely to practice handwashing at critical times than those with available setups. This finding aligns with other studies (46), which suggest that the availability of handwashing setups significantly increases the likelihood of proper handwashing (41). To address these disparities, it is crucial to explicitly focus on reducing inequalities and targeting the poorest and most marginalized populations, as well as underdeveloped areas, in hygiene and sanitation efforts.
This community-based study provided valuable insights into WaSH inequalities between urban and rural communities. However, certain key elements, such as the wealth index, were not assessed due to resource and time constraints.
By examining the differences in access to basic WaSH between urban slums and rural areas access using selected household-level indicators, this study confirmed that WaSH services are significantly higher in urban slums than in rural communities. The study also identified several socioeconomic factors, such as sex, age, education of household heads, type of occupation, and monthly income, as affecting access to improved WaSH services. National and local governments should prioritize addressing these disparities responsibly, ensuring efficient resource allocation with a focus on equal opportunity and shared growth. Despite the differences, the limited availability of WaSH services in both urban and rural communities requires urgent attention. Collaborative efforts are required to maximize these services at the highest possible level. Therefore, stakeholders should focus on key socioeconomic and behavioral factors to help communities achieve the 2030 global WaSH goals and mitigate the significant health issues related to inadequate WaSH services.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical approval was obtained from the College of Health and Medical sciences Institutional Health Research Ethics Review Committee (Ref. No. IHRERC/056/24). Informed, voluntary, written and signed consent was provided by house heads. The study group (house head) who participated in the study was informed in the local language (Amharic and Afanoromo) about the study procedure and duration following which consent was obtained from them. Data collected from the study group were kept confidential and households had the right to withdraw from the study at any time. Necessary permissions were obtained from the district health office of Babile health office of east Hararghe of Oromia region and Amir Nur district health office of Harari regional state.
GM: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AZ: Conceptualization, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. FW: Conceptualization, Data curation, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – review & editing. AD: Conceptualization, Data curation, Investigation, Supervision, Validation, Visualization, Writing – review & editing. TR: Conceptualization, Data curation, Formal analysis, Methodology, Software, Validation, Visualization, Writing – review & editing. UU: Conceptualization, Data curation, Investigation, Project administration, Supervision, Validation, Visualization, Writing – review & editing. KU: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We would like to thank Haramaya University for supporting us in conducting this research. We also extend our gratitude to the local government officials, data collectors, and study participants for their genuine assistance in the research process. Finally, our deepest thanks go to the research team members, whose dedication and unwavering efforts made this research possible.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Agbadi, P, Darkwah, E, and Kenney, PL. A multilevel analysis of Regressors of access to improved drinking water and sanitation facilities in Ghana. J Environ Public Health. (2019) 2019:1–11. doi: 10.1155/2019/3983869
2. Roche, R, Bain, R, and Cumming, O. A long way to go – estimates of combined water, sanitation and hygiene coverage for 25 sub-Saharan African countries. PLoS One. (2017) 12:e0171783. doi: 10.1371/journal.pone.0171783
3. JMP , "WHO | UNICEF JMP progress on household drinking water, sanitation and hygiene 2000-2020." (2022) Available at: https://washdata.org/sites/default/files/2022-01/jmp-2021-wash-households-highlights.pdf (accessed March 30, 2024).
4. Iqbal, A. , "See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/323614212. Ovarian leiomyoma associated with serous cystadenoma-a case report of an uncommon entity ovarian leiomyoma associated with serous cystadenoma-a case report of an uncommon entity" (2023).
5. UN , "The sustainable development goals report: Special edition" (2023) Available at: https://unstats.un.org/sdgs/report/2023/The-Sustainable-Development-Goals-Report-2023.pdf (accessed March 30, 2024).
6. Ohwo, O, and Vivian Odubo, T. Comparative analysis of WASH services between the rich and poor in sub-Saharan Africa. Int J Nat Resour Ecol Manag. (2021) 6:147–55. doi: 10.11648/j.ijnrem.20210603.16
7. Sahiledengle, B, Alemseged, F, and Belachew, T. Sanitation practice and associated factors among slum dwellers residing in urban slums of Addis Ababa, Ethiopia: A community based cross-sectional study. J Public Health Epidemiol. (2018) 10:370–9. doi: 10.5897/JPHE2018.1064
8. JMP , "WHO/UNICEF joint monitoring programme for water supply, sanitation and hygiene special focus on gender launch version: gender pullout progress on household drinking water, sanitation and hygiene 2000-2022" (2022) Available at: https://www.unicef.org/wca/media/9161/file/jmp-2023-wash-households-gender-pullout-launch.pdf (accessed September 2024).
9. Cha, S, Jin, Y, Elhag, MS, Kim, Y, and Ismail, HAHA. Unequal geographic distribution of water and sanitation at the household and school level in Sudan. PLoS One. (2021) 16:e0258418. doi: 10.1371/journal.pone.0258418
10. World Health Organization . WHO water, sanitation and hygiene strategy 2018–2025. Geneva: World Health Organization (2018).
11. Patel, SK, Pradhan, MR, and Patel, S. Water, sanitation, and hygiene (wash) conditions and their association with selected diseases in urban India. J Popul Soc Stud. (2020) 28:103–15. doi: 10.25133/JPSSv28n2.007
12. Desye, B, Berhanu, L, Ebrahim, AM, Natnael, T, Wagaye, B, Gufue, ZH, et al. Access to basic water, sanitation, and hygiene (WaSH) facilities and associated factors in Ethiopia: evidence from demographics and health surveys. J Water Sanit Hyg Dev. (2023) 13:39–49. doi: 10.2166/washdev.2022.226
13. Azage, M, Motbainor, A, and Nigatu, DJH. Exploring geographical variations and inequalities in access to improved water and sanitation in Ethiopia: mapping and spatial analysis. Heliyon. (2020) 6:e03828. doi: 10.1016/j.heliyon.2020.e03828
14. Rahut, DB, Singh, A, and Sonobe, T. WaSH facilities prevalence and determinants: evidence from 42 developing countries. Front Environ Sci. (2022) 10:1013657. doi: 10.3389/fenvs.2022.1013657
15. Stewart, F, et al. "Horizontal inequalities: a neglected dimension of development," Wider Perspectives on Global Development, (2005) 101–135.
16. Wallgreen, OB . Inadequate WaSH infrastructure among rural populations in the Pacific Islands. Ballard Brief. (2022) 2022:1. Available at: https://scholarsarchive.byu.edu/ballardbrief/vol2022/iss2/1
17. UN-Habitat: United Nations Human Settlements Programme , "Global report on human settlements," (2009).
18. Alice, A, Behera, D, Behera, MR, Patra, SK, and Mishra, J. Assessment of sanitation and drinking water facilities among slum households in Bhubaneswar, Odisha – a cross-sectional study. JFMPC. (2023) 12:484–92. doi: 10.4103/jfmpc.jfmpc_1544_22
19. Beyene, A, Hailu, T, Faris, K, and Kloos, H. Current state and trends of access to sanitation in Ethiopia and the need to revise indicators to monitor progress in the Post-2015 era. BMC Int Health Hum Rights. (2015) 15:451–8. doi: 10.1186/s12889-015-1804-4
20. WHO UNICEF , "The WHO/UNICEF Joint monitoring Programme estimates on WaSH." (2020) Available at: http://washdata.org (accessed September 2024).
21. Rakotomanana, H, Komakech, JJ, Walters, CN, and Stoecker, BJ. The WHO and UNICEF Joint monitoring Programme (JMP) indicators for water supply, sanitation and hygiene and their association with linear growth in children 6 to 23 months in East Africa. Environ Res Public Health. (2020) 17:6262. doi: 10.3390/ijerph17176262
22. World Health Organization , "Why urban health matters," Geneva: World Health Organization (2010).
23. World Health Organization and UNNICEF . Progress on household drinking water, sanitation and hygiene 2000–2020: Five years into the SDGs. Geneva: World Health Organization (2021).
24. Flores Baquero, O., Giné Garriga, R., Pérez Foguet, A., and De Palencia, A. Jiménez Fdez, "Post-2015 WaSH targets and indicators: a review from a human rights perspective," (2013).
25. Dickin, S, and Gabrielsson, S. Inequalities in water, sanitation and hygiene: challenges and opportunities for measurement and monitoring. J Water Secur. (2023) 20:100143. doi: 10.1016/j.wasec.2023.100143
27. Ananian, S., and Dellaferrera, G., Employment and wage disparities between rural and urban areas (no. 107). ILO Working Paper (2024). doi: 10.54394/LNZT9066
28. Adank, M, Butterworth, J, Godfrey, S, and Abera, M. Looking beyond headline indicators: water and sanitation services in small towns in Ethiopia. J Water Sanit Hyg Dev. (2016) 6:435–46. doi: 10.2166/washdev.2016.034
29. Adams, EA, Boateng, GO, and Amoyaw, JA. Socioeconomic and demographic predictors of potable water and sanitation access in Ghana. Soc Indic Res. (2016) 126:673–87. doi: 10.1007/s11205-015-0912-y
30. Bamou Tankoua, L . Determinants of access, use and sustainability of improved water sources by households in Cameroon In book: Sustainable development in Africa. (2021) (pp. 427–44).
31. Egziabher, KG, and Adnew, B. Valuing water supply service improvements in Addis Ababa. Ethiop J Econ. (2009) 16:39–84. doi: 10.4314/eje.v16i2.46187
32. Sesay, BP, Hakizimana, JL, Elduma, AH, and Gebru, GN. Assessment of water, sanitation and hygiene practices among households, 2019 – Sierra Leone: a community-based cluster survey. Environ Health Insights. (2022) 16:11786302221125042. doi: 10.1177/11786302221125042
33. Chaudhuri, S, and Roy, M. Rural-urban spatial inequality in water and sanitation facilities in India: a cross-sectional study from household to national level. Appl Geogr. (2017) 85:27–38. doi: 10.1016/j.apgeog.2017.05.003
34. Tesfaw, A, Tiruneh, M, Mamuye, M, Walle, Z, Teshager, W, Teshome, F, et al. Magnitude and determinants of improved household latrine utilization in Ethiopia: multilevel analysis of the mini Ethiopian demographic health survey (EDHS) 2019. PLoS One. (2023) 18:e0289427. doi: 10.1371/journal.pone.0289427
35. Akpakli, DE, Manyeh, AK, Akpakli, JK, Kukula, V, and Gyapong, M. Determinants of access to improved sanitation facilities in rural districts of southern Ghana: evidence from Dodowa health and demographic surveillance site. BMC Res Notes. (2018) 11:1–7. doi: 10.1186/s13104-018-3572-6
36. Mulenga, JN, Bwalya, BB, and Kaliba-Chishimba, K. Determinants and inequalities in access to improved water sources and sanitation among the Zambian households. Int J Dev Sustain. (2017) 6:746–62.
37. Leshargie, CT, Alebel, A, Negesse, A, Mengistu, G, Wondemagegn, AT, Mulugeta, H, et al. Household latrine utilization and its association with educational status of household heads in Ethiopia: a systematic review and meta-analysis. BMC Int Health Hum Rights. (2018) 18:901–12. doi: 10.1186/s12889-018-5798-6
38. Davis, KE, Ekboir, J, and Spielman, DJ. Strengthening agricultural education and training in sub-Saharan Africa from an innovation systems perspective: a case study of Mozambique. J Agric Educ Ext. (2008) 14:35–51. doi: 10.1080/13892240701820371
39. Assefa, Y, Atnafu, N, and Abebe, K. Hand washing practices at critical times and their associated factors among mothers in Ethiopia: a systematic review and meta-analysis. J Sci Inclusive Dev. (2024) 6:42–69. doi: 10.20372/jsid/2024-270
40. Gizaw, Z, Demissie, NG, Gebrehiwot, M, Destaw, B, and Nigusie, A. Hand hygiene practice and associated factors among rural communities in Northwest Ethiopia. Sci Rep. (2023) 13:4287. doi: 10.1038/s41598-023-30925-0
41. Wolde, M, Abate, M, Mandefro, G, Beru, E, Kassahun, A, and Tesema, GA. Determinants of handwashing practice and its associated factors among mothers of under-5 children in Kolladiba town, Northwest Ethiopia: cross-sectional study. BMJ Open. (2022) 12:e058960. doi: 10.1136/bmjopen-2021-058960
42. World Health Organization . State of the World’s hand hygiene: A global call to action to make hand hygiene a priority in policy and practice. Geneva: World Health Organization (2021).
43. Kouakou, JS, Tiadé, ML, Barro, PK, Kouamé, J, Bediakon, MG, Desquith, AA, et al. Factors influencing personal hygiene among primary schoolchildren in western Côte d'Ivoire. J Water Sanit Hyg Dev. (2021) 11:687–92. doi: 10.2166/washdev.2021.265
44. Ekanem, AM, and Johnson, OE. Hand washing practices at critical times among mothers in selected health facilities in Akwa Ibom state. Ibom Med J. (2015) 8:1–10. doi: 10.61386/imj.v8i1.122
45. Agaro, A, Hareru, HE, Muche, T, Sisay W/tsadik, D, Ashuro, Z, Negassa, B, et al. Predictors of hand-washing practices at critical times among mothers of under-5 years old children in rural setting of Gedeo zone, southern Ethiopia. Environ Health Insights. (2022) 16:11786302221120784. doi: 10.1177/11786302221120784
46. Abebe, A, Debela, BG, Zenebe, GA, Hareru, HE, and Ashuro, ZJH. Mothers' hand washing practices and associated factors among model and non-model households in the rural community of Bibugn district, north West Ethiopia: the context of the Ethiopian health extension package. Vaccine reports. (2023) 9:e17503. doi: 10.1016/j.heliyon.2023.e17503
Keywords: Eastern Ethiopia, hygiene, inequality, rural, sanitation, urban slum, water services
Citation: Mekonnen GK, Zako A, Weldegebreal F, Desalew A, Raru TB, Umer U and Urgesa K (2024) Water, sanitation, and hygiene service inequalities and their associated factors among urban slums and rural communities in Eastern Ethiopia. Front. Public Health. 12:1438748. doi: 10.3389/fpubh.2024.1438748
Edited by:
Nur A. Hasan, EzBiome Inc., United StatesReviewed by:
Priscila Neves Silva, Oswaldo Cruz Foundation (Fiocruz), BrazilCopyright © 2024 Mekonnen, Zako, Weldegebreal, Desalew, Raru, Umer and Urgesa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Getachew Kabew Mekonnen, Z2VjaG1pY3JvQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.