
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Public Health , 18 December 2024
Sec. Public Health Policy
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1417866
 Josphat Martin Muchangi1*
Josphat Martin Muchangi1* James Mturi2
James Mturi2 Hajra Mukasa3
Hajra Mukasa3 Kioko Kithuki1Sarah Jebet Kosgei1Lennah Muhoja Kanyangi1Rogers Moraro1Samuel Kamau4Maureen Nankanja3
Kioko Kithuki1Sarah Jebet Kosgei1Lennah Muhoja Kanyangi1Rogers Moraro1Samuel Kamau4Maureen Nankanja3Introduction: The government's role in influencing policies related to Coronavirus disease 2019 (COVID-19) vaccine distribution and handwashing practices is essential in controlling the spread of severe acute respiratory syndrome coronavirus 2.
Methods: This study aimed to systematically review published studies to explore the influence of government policies on handwashing and vaccine uptake in Kenya, Uganda and Tanzania to prevent and control COVID-19. A comprehensive search strategy was applied across three databases, and eligibility was determined using strict inclusion and exclusion criteria. We reviewed 9 of 136 research papers following the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines.
Results: The findings revealed that the government has a role in influencing policies related to COVID-19 vaccine distribution and handwashing uptake. Employment of public health campaigns and communication strategies by the government in Uganda increased vaccine acceptance and hand hygiene uptake. Similarly, government efforts to make hand hygiene accessible increased the uptake of handwashing in Tanzania. In Kenya, government efforts to increase access to soap and clean water in informal settlements and markets resulted in increased adherence to handwashing practices. Further, government incentives such as cash increased vaccination rates while vaccination reminders combined with cash incentives increased childhood immunization coverage.
Discussion: Overall, this review indicates that monitoring and enforcing compliance increases vaccine and handwashing uptake across the three countries. The effectiveness of government policies on handwashing and vaccine uptake is influenced by factors such as safety, efficacy and access to information, among others. Therefore, there is a need to address these factors for the successful implementation of these policies.
Systematic review Registration: PROSPERO ID CRD42023396319, https://www.crd.york.ac.uk/prospero/.
The coronavirus disease 2019 (COVID-19) pandemic has led to loss of lives and severely crimpled economies globally (1). At the same time, people have raised social issues including the erosion of public trust in government efforts and expert advice due to misrepresentation and misinformation (2, 3). Whilst the development of COVID-19 vaccines is an extraordinary achievement, successful vaccination of populations and adherence to proper handwashing practices face challenges associated with production, distribution, and acceptance (4). The government's role in influencing policies related to COVID-19 vaccine distribution and handwashing uptake is essential in controlling the spread of the virus and protecting public health (5).
The effective implementation of COVID-19 policies requires public compliance. Of note, public compliance depends on the trust people have in government actions, hence its importance in the success of any government project (6, 7). Government actions include public scrutiny and public participation, equitable distribution of COVID-19 vaccines and handwashing stations (8). Trust in government institutions involved in the distribution of vaccines, monitoring and information reflects people's satisfaction with the government's policy and performance (6)1.
The current infrastructure and supplies are inadequate to warrant a swift vaccination campaign when it comes to the transport and storage of vaccines in most places (9). Several governments have made efforts to ensure the timely delivery of COVID-19 supplies by developing policies and infrastructures for distributing, storing and administering vaccines across their jurisdiction (9). In the United States of America, each state has devised a vaccine tracking system where each state orders doses up to a limit decided at the federal level, making vaccines and other COVID-19 supplies accessible (10–12).
Collaboration between the public and private sectors as well as other international bodies is key in ensuring that the COVID-19 supplies and services are supplied based on risk, resource, and benefit sharing (13, 14). In Zambia, the government has leveraged local and international support to combat the COVID-19 pandemic. The collaboration was seen in the sensitization of Zambian citizens about the pandemic through messages and advertisements distributed through radio, television, and telephone companies (15). In addition, collaboration between academia, government, and the community is crucial in promoting health fairness (16). Further, the government and community collaboration ensures more community members receive vaccinations, raising the total immunization rate.
Effective communication by the government is key for handwashing and COVID-19 uptake to succeed, hence minimizing hesitancy (15). A study to establish why Egyptian medical students were reluctant to receive vaccinations reported that the government should create more awareness about the importance of vaccination to increase vaccination adoption (17). To comprehend vaccine reluctance, investigation of vaccine roll-out in South Africa and Zimbabwe emphasized the importance of the government in disseminating information and knowledge about vaccines to stop false information from stifling vaccination rates (18). Assessment of vaccine reluctance in South Africa from 2020 to 2021 revealed that communication campaigns and other forms of community engagement are key in addressing some of the concerns, hence building people's trust in handwashing practices and vaccine acceptance (19).
Government incentives such as cash rewards, free meals, or reduced transportation costs can encourage people to get vaccinated. An increase in government spending in a program to increase the number of free vaccines available to citizens who willingly underwent mass vaccination has been previously shown to enhance vaccine uptake in nations with low and intermediate incomes (20). Local and federal governments in the United States of America offered financial incentives, including gift cards, a lottery with a million-dollar top prize, and savings bonds to entice people to get immunized (21). Another study indicated that financial incentives had raised vaccination rates among Swedish people (22). Government policies play a key role in shaping vaccine policy and availability, as well as in implementing programs and influencing vaccine acceptance in society.
However, literature supporting this notion remains scarce in sub-Saharan Africa, where the uptake of COVID-19 vaccine and handwashing remains low. For instance, in Tanzania, a community based survey found only 18% of respondents had received COVID-19 vaccine (38) while a longitudinal study across 10 sub-Saharan African countries observed a significant decline in handwashing prevalence between July and November 2020 (39). Therefore, this study aims to investigate the role of government policies in promoting key public health behaviors, specifically the uptake of COVID-19 vaccines and handwashing practices, as part of the broader effort to control the spread of COVID-19 in sub-Saharan Africa. The focus of this research is on how governments can enhance prevention through public health campaigns, ensure compliance with health guidelines, and guarantee the availability of essential materials and tools such as soap and vaccine doses. By analyzing the impact of these policies, the study seeks to identify effective strategies for increasing both vaccination rates and adherence to hand hygiene practices, which are critical in preventing the transmission of COVID-19.
This review was undertaken in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and the Centre for Reviews and Dissemination (CRD) guidelines (23, 24). The protocol was registered at the International Prospective Register of Systematic Reviews (PROSPERO) database with approval ID CRD42023396319.
A systematic search of the literature was conducted using PubMed and ScienceDirect as the primary databases. We also used Google Scholar as a supplementary tool to identify additional relevant studies that the primary databases may not have captured. A search strategy was formulated based on the PECOS framework by combining all possible combinations (Supplementary Tables 1, 2). The following search terms and their synonyms using Boolean operators were used to perform the search strategy: handwashing, vaccine, COVID-19, prevention, policy, Kenya, Uganda, and Tanzania.
Our review considered all published studies focusing on the influence of government policies on COVID-19 vaccination and handwashing conducted in Kenya, Uganda, and Tanzania. There was no restriction on the publication date or language.
We excluded studies that did not address the influence of government policies on handwashing and vaccine uptake in Kenya, Uganda, and Tanzania to prevent and control COVID-19. In addition, literature reviews and preprints were ineligible for inclusion in this systematic review.
We selected studies in two stages after the initial removal of duplicates. First, titles and abstracts of the retrieved articles were screened for relevance by two independent reviewers, JM and KK. The full texts of potentially relevant studies were further assessed for data extraction. We used Mendeley for reference management of the potentially relevant articles. Disagreements were resolved through discussion with a third reviewer, RM. We ensured internal consistency by conducting training for reviewers to ensure they understand the criteria and process.
JM and KK assessed the potential for bias in the eligible articles based on the Quality Assessment Tool for Observational Cohort and Cross-sectional studies (https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools) (25). This checklist encompasses 14 crucial criteria regarded as fundamental for ensuring the quality of reporting in cohort and cross-sectional studies. These recommendations focus on various aspects, including the article's objectives, the study population, exposure measures and potential confounders, among others.
JM and KK extracted data from the selected studies using a standardized data extraction form, and any disagreements were resolved by consensus. The data extracted included the name of the first author(s) and year of publication, study title, country of study, study objective(s), study design, outcome definition, and main findings on how government policies have influenced COVID-19 vaccine and handwashing uptake as an intervention.
We used narrative synthesis to summarize the main results of the eligible studies. A table was used to show the study characteristics and indicate how government policies influence handwashing and vaccine uptake in Kenya, Uganda, and Tanzania to prevent and control COVID-19.
We identified 136 research papers from our database searches, as summarized by Figure 1. After removing duplicates, 78 papers underwent abstract and title screening, which resulted in the exclusion of 51 studies. The remaining 27 studies underwent full-text screening, 18 of which were excluded due to irrelevant study outcomes. This systematic review includes 9 articles focusing on the influence of government policies on vaccine uptake and handwashing to prevent and control COVID-19.
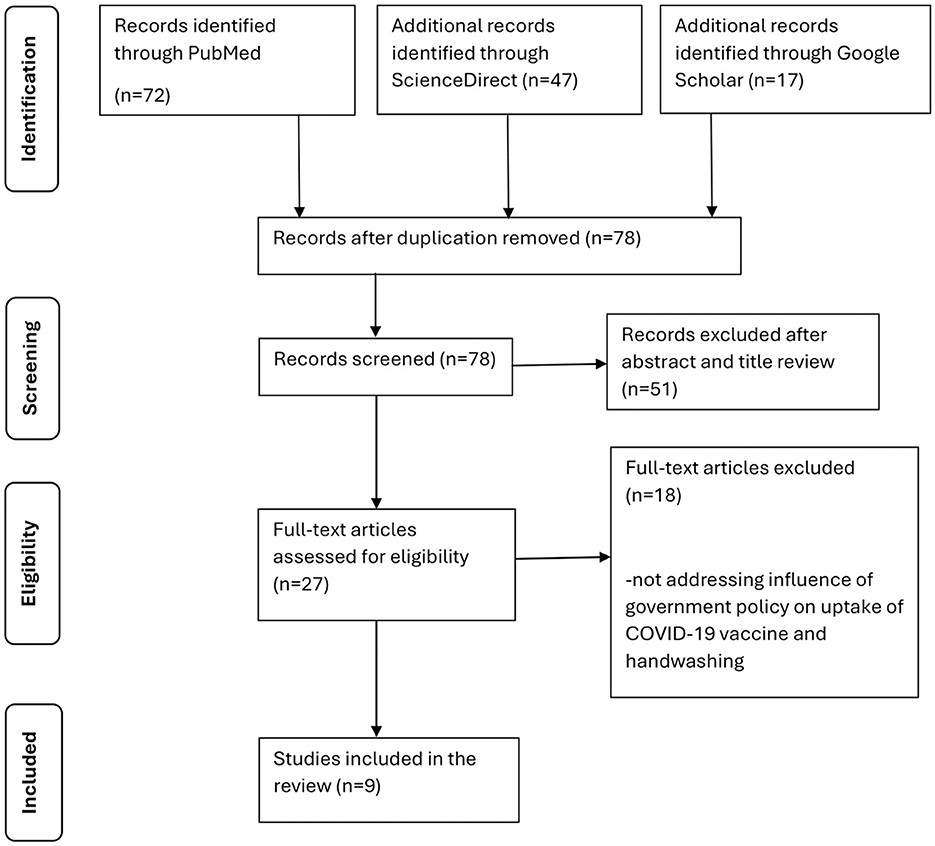
Figure 1. PRISMA chart depicting the study selection process.
The main characteristics of the studies included in this systematic review are presented in Table 1. Three of the eligible studies focused on Kenya, with Tanzania and Uganda having two and four studies, respectively. Publication years ranged from 2021 to 2022. The study designs consisted of cross-sectional studies, multi-sited historically informed ethnographic fieldwork, and qualitative interviews. The study participants ranged from pregnant and lactating women to health workers, policymakers, and institutions such as supermarkets. Similarly, the eligible studies' sample sizes ranged from 33 to 2,245.
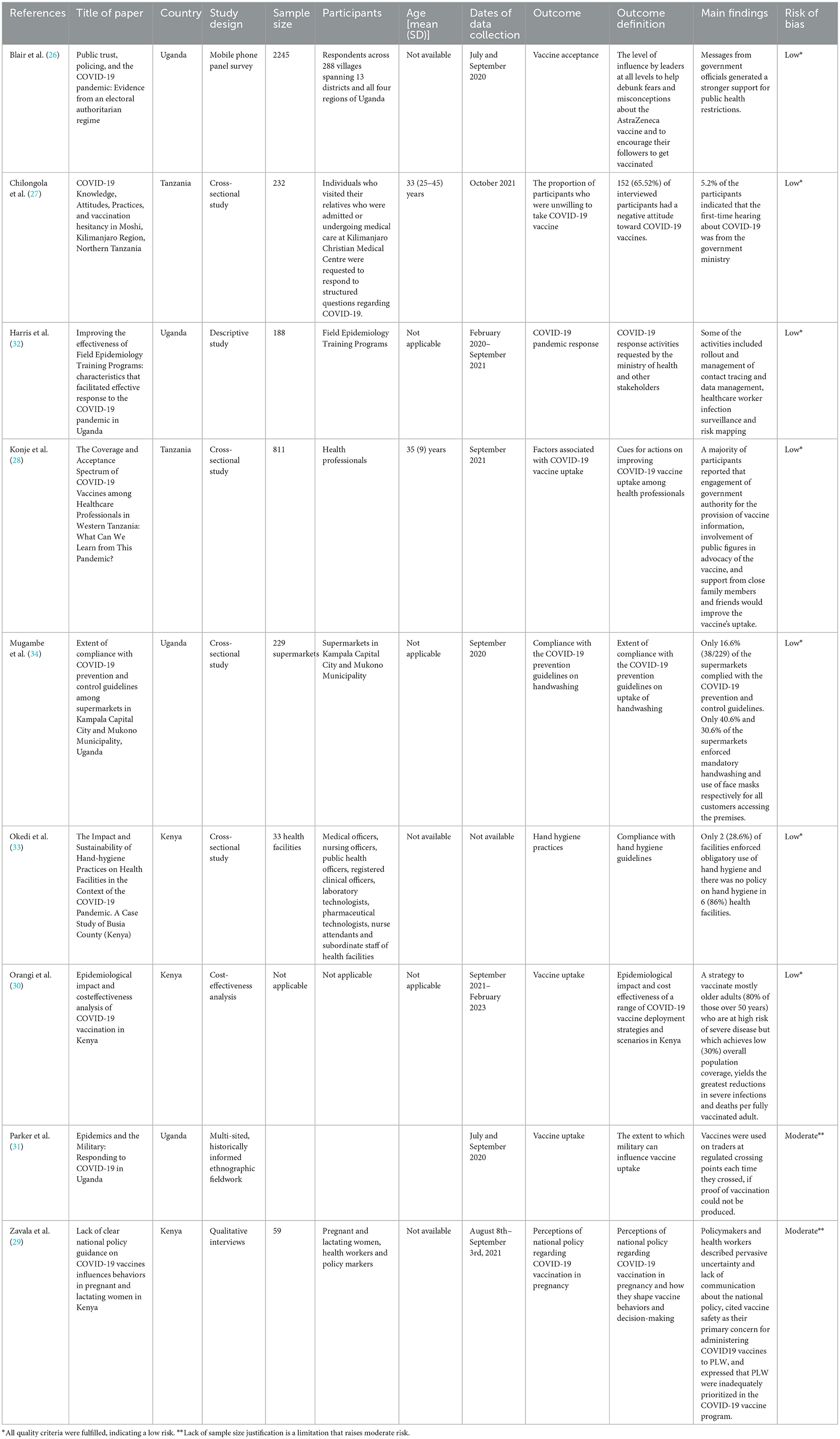
Table 1. The characteristics of the eligible studies.
According to the Quality Assessment Tool for Observational Cohort and Cross-sectional Studies checklist, all the studies met the recommendations for conducting observational studies (Supplementary Table 3). This finding indicates high overall methodological quality and low risk of bias in these studies.
The following results are organized into key themes that emerged during data extraction and synthesis. These themes represent the various ways in which government policies have influenced COVID-19 vaccine uptake and handwashing practices. The themes include public health campaigns and communication strategies, accessibility of vaccines and hand hygiene supplies, vaccine certification, collaborations with community leaders, and monitoring and enforcement of compliance. These categories emerged organically from the analysis of the studies, allowing us to systematically assess the diverse impact of government interventions on these preventive behaviors.
Four studies in the systematic literature review have revealed that the government's efforts to promote public health campaigns and communication strategies to educate the public about COVID-19 have led to vaccine acceptance and handwashing uptake. A Ugandan study reported that messages from government officials generated a stronger support for public health restrictions (26). Governments can influence the control and prevention of COVID-19 by making citizens aware of the disease. Chilongola et al. reported that 5.2% of the participants first heard about COVID-19 from the government ministry after assessing COVID-19 knowledge (27). The engagement of government authorities in the provision of vaccine information was also reported as a potential factor in improving COVID-19 vaccine uptake (28). Conversely, a study involving pregnant and lactating women (PLW) showed uncertainty and lack of communication about the national policy, with healthcare workers citing vaccine safety as their primary concern for administering COVID-19 vaccines to this population (29). As such, there was a perception by the PLW of the restrictive policy as an indicator of a safety risk, resulting in vaccine hesitancy and potentially exacerbated inequities in vaccine access (29).
Increased accessibility of vaccines and hand hygiene supplies by the government can increase uptake of COVID-19 vaccine and handwashing practices. For instance, a cost-effectiveness analysis conducted in Kenya showed that vaccine deployment strategies targeting those at risk of disease and other vulnerable groups rather than the whole population could increase vaccine uptake (30). One important strategy is to ensure that there is an appropriate supply of the vaccine in all locations and that it is distributed fairly to all populations, regardless of their socioeconomic situation or geography.
A study to examine the extent to which the military can influence vaccine uptake in Uganda revealed soldiers stationed on the ground exerted authority by making people without vaccine cards be vaccinated (31). As such, government policies requiring vaccination for specific activities; and verifying vaccination status through proof-of-vaccine programs can increase vaccination rates. Putting such a policy into practice at the local or national level and in particular professions, like healthcare, education, or travel, would be crucial in raising vaccination rates.
Harris et al. highlighted government policies that allow collaborations with community leaders in awareness creation about COVID-19 could build trust. Strong leadership and collaborations, as witnessed in Uganda, are critical in building trust and influencing handwashing and COVID-19 vaccine uptake (32).
Two studies involving 33 health facilities and 229 supermarkets indicated that monitoring and enforcement of vaccine-related policies is key in raising the uptake of handwashing and vaccines (33, 34). The findings revealed that only one hospital had a national policy on hand hygiene. The majority of the respondents indicated that enabling factors for implementing hand hygiene include a clear commitment of national and county governments to providing clear policy frameworks and guidelines that support hand hygiene initiatives (33). Similarly, an assessment of compliance levels among supermarkets in Kampala and Mukono Municipality indicated that the supermarkets complied with the COVID-19 prevention and control guidelines, including the establishment of handwashing stations, with more than half of the supermarkets having someone or a team in charge of enforcing compliance to COVID-19 measures (34).
Our study shows that the government has an essential role in influencing policies related to COVID-19 vaccine distribution and handwashing uptake to control its spread. The government's employment of public health campaigns and communication strategies to educate the public about the safety of COVID-19 vaccines and hand hygiene practices has led to increased uptake. These findings are consistent with previous research where awareness creation by the government about vaccines was shown to improve vaccine acceptance (17). Similar findings emphasized the government's role in creating awareness to reduce vaccine hesitancy (18, 19). Campaigns and community engagement activities can increase people's confidence in the safety and efficacy of COVID-19 vaccines by addressing the associated concerns and the importance of hand hygiene.
Government involvement in increasing vaccine availability and hand hygiene supplies can increase the COVID-19 vaccine and handwashing uptake. The results are consistent with the literature, which notes that vaccine uptake could be improved by increasing government budgets (20). Additionally, this finding is parallel with global experiences beyond the COVID-19 pandemic. For instance, in Australia, the introduction of funded influenza vaccine programs for children under 5 years old led to a significant increase in vaccine uptake, with a 2.7- to 4.2-fold rise observed. Importantly, this initiative also had spillover effects, enhancing vaccine coverage among older children and adults (40). Such initiatives are aimed at increasing the availability of free vaccines among citizens who voluntarily undergo vaccination in large numbers. As such, policymakers can invest in minimizing the scarcity of vaccines, boosting vaccine intention and vaccination rates among populations.
A critical factor in understanding the outcomes of government interventions is the level of exposure to these policies and the resources available to support them. In countries with higher levels of public health funding and infrastructure, strict containment measures accompanied by effective communication and resource distribution have led to improved handwashing adherence and vaccine uptake. For instance, studies from high-income countries like Australia and Sweden demonstrate that well-resourced government programs yield positive outcomes in both hand hygiene and vaccination rates (22, 40).
However, in low- and middle-income countries (LMICs), where strict policies were not always accompanied by adequate resources, adherence to these behaviors was lower, often due to limited access to necessary supplies or a lack of public trust (42). In some cases, stricter containment measures, without sufficient support, or communication, resulted in public frustration and lower adherence.
Moreover, findings from a study conducted in 14 countries suggested that strict government policies during the COVID-19 pandemic may have inadvertently undermined individual self-regulatory processes, reducing handwashing adherence. More lenient policies, on the other hand, may have prompted greater self-regulatory efforts, as individuals faced higher-risk situations and were motivated to adopt protective behaviors (44). Additionally, government incentives such as cash rewards can encourage people to get vaccinated, thus increasing vaccination rates. This outcome is in concordance with previous research which highlighted that financial incentives and other nudges amplified vaccination rates in the United States of America (21). In a different setting, an assessment of monetary incentives in relation to vaccination rates among Swedish individuals revealed that the use of incentives increased vaccination rates by about four points (22). Monetary compensation to individuals who accept vaccination and adhere to proper handwashing practices can help in controlling the spread of COVID-19.
Previous research has also explored how proof of vaccination in accessing government services increases vaccination concurs with the current research findings (35). The study findings revealed that school-entry mandates increased COVID-19 vaccination rates among children. Other studies have shown that the announcement of vaccination mandates can increase vaccination rates by over 60% (36).
Government policies that allow partnering with community leaders and organizations can build trust and engage with hard-to-reach communities, thus increasing vaccination rates. For instance, collaborations between governments and the community can be used to address vaccine hesitancy (37). Other studies have revealed that faith-based wellness programs rooted in African American communities are trusted to provide accurate information. Therefore, the academic-government-community collaboration is essential in ensuring health equity (16).
Recent studies have provided valuable insights into the effectiveness of government interventions in promoting these crucial public health measures. For instance, Matkovic et al. demonstrated that simple, brief, and easily conveyable messages could positively impact behavioral intentions around handwashing during the early stages of a health crisis across the United States during the COVID-19 pandemic (41). Their findings emphasize the importance of clear, consistent messaging from authorities in promoting proper hand hygiene. Additionally, a systematic review of handwashing interventions in low- and middle-income countries highlighted the importance of multi-level interventions and the combination of training, policy, and funding strategies in implementing effective hand hygiene programs (42). Regarding vaccine uptake, studies have examined the impact of various government policies, revealing that state-level mandates and incentives significantly increase vaccination rates (36, 43). This aligns with our findings on the effectiveness of government incentives and mandates in boosting vaccine acceptance.
The study's findings also imply that the government seeking to increase vaccination rates must collaborate with community-based organizations to increase awareness of vaccines and vaccination centers.
This systematic review has some strengths: first, we used a comprehensive search strategy to identify eligible research papers, and our protocol was registered on the PROSPERO database. We did not limit our search based on publication date or language of publication, thereby increasing the number of studies identified. Despite these advantages, it's important to acknowledge our study's limitations. The heterogeneity of the included studies and potential publication bias may affect the generalizability of our findings. We employed a rigorous methodology to mitigate these issues, including a comprehensive search strategy and independent screening by multiple reviewers. However, future research should consider conducting primary studies with standardized measures to further validate the effectiveness of government policies on handwashing and vaccine uptake. Moreover, we only focused on Kenya, Uganda, and Tanzania; hence, the results may not be generalizable to other areas due to differing political, environmental, economic, and social characteristics. Additionally, we recognize the need to explore the long-term sustainability of government interventions and their ethical implications, particularly concerning mandates and incentives. These aspects call for further investigation to ensure the development of effective and ethically sound public health policies.
In conclusion, government policies that promote access to accurate information about hand hygiene through health campaigns and the provision of water and soap have been shown to be effective in increasing handwashing practices among the general public. The requirement to verify vaccination status, provision of cash incentives, and government partnership with community leaders and organizations help build trust and improve vaccine uptake rates. Therefore, policymakers should not only formulate but also implement government policies that employ the identified strategies to significantly enhance the uptake of preventive measures and contribute to controlling and preventing COVID-19 in Kenya, Uganda, Tanzania, and similar regions. While the COVID-19 pandemic is no longer classified as an emergency, these strategies could be crucial in the event of a resurgence of COVID-19 or the emergence of a new virus with similar transmission characteristics. Policymakers can apply these lessons to future public health challenges to improve preparedness and response to pandemics.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
JMM: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. JM: Methodology, Validation, Visualization, Writing – review & editing. HM: Data curation, Methodology, Writing – review & editing. KK: Data curation, Methodology, Writing – review & editing. SJK: Data curation, Methodology, Writing – review & editing. LK: Data curation, Methodology, Writing – review & editing. RM: Data curation, Methodology, Writing – review & editing. SK: Data curation, Methodology, Writing – review & editing. MN: Data curation, Methodology, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was funded by the Foreign, Commonwealth & Development Office (FCDO). The funding body did not have any role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1417866/full#supplementary-material
COVID-19, Coronavirus disease-19; PRISMA-P, Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols; CRD, Centre for Reviews and Dissemination guidelines; PROSPERO, International Prospective Register of Systematic Reviews; LMICs, Low Middle-Income Countries; FCDO, Foreign, Commonwealth & Development Office; PECOS, population, exposure, comparator, outcome and study.
1. Adekola J, Fischbacher-Smith D, Okey-Adibe T, Audu J. Strategies to build trust and COVID-19 vaccine confidence and engagement among minority groups in Scotland. Int J Disaster Risk Sci. (2022) 13:890–902. doi: 10.1007/s13753-022-00458-7
2. Walsh MJ, Baker SA, Wade M. Evaluating the elevation of authoritative health content online during the COVID-19 pandemic. Online Inf Rev. (2023) 47:782–800. doi: 10.1108/OIR-12-2021-0655
3. Leng Y, Zhai Y, Sun S, Wu Y, Selzer J, Strover S, et al. Misinformation during the COVID-19 outbreak in China: cultural, social and political entanglements. IEEE Trans Big Data. (2021) 7:69–80. doi: 10.1109/TBDATA.2021.3055758
4. Mohamed K, Rzymski P, Islam MS, Makuku R, Mushtaq A, Khan A, et al. COVID-19 vaccinations: the unknowns, challenges, and hopes. J Med Virol. (2022) 94:1336–49. doi: 10.1002/jmv.27487
5. Talic S, Shah S, Wild H, Gasevic D, Maharaj A, Ademi Z, et al. Effectiveness of public health measures in reducing the incidence of covid-19, SARS-CoV-2 transmission, and covid-19 mortality: systematic review and meta-analysis. BMJ. (2021) 375:e068302. doi: 10.1136/bmj-2021-068302
6. Saechang O, Yu J, Li Y. Public trust and policy compliance during the COVID-19 pandemic: the role of professional trust. In: Healthcare. MDPI (2021). p. 151. doi: 10.3390/healthcare9020151
7. Schmelz K. Enforcement may crowd out voluntary support for COVID-19 policies, especially where trust in government is weak and in a liberal society. Proc Natl Acad Sci. (2021) 118:e2016385118. doi: 10.1073/pnas.2016385118
8. Solís Arce JS, Warren SS, Meriggi NF, Scacco A, McMurry N, Voors M, et al. COVID-19 vaccine acceptance and hesitancy in low-and middle-income countries. Nat Med. (2021) 27:1385–94. doi: 10.1038/s41591-021-01454-y
9. Williams BA, Jones CH, Welch V, True JM. Outlook of pandemic preparedness in a post-COVID-19 world. NPJ Vaccines. (2023) 8:178. doi: 10.1038/s41541-023-00773-0
10. Schmidt H, Weintraub R, Williams MA, Buttenheim A, Sadecki E, Wu H, et al. Equitable allocation of COVID-19 vaccines: an analysis of the initial allocation plans of CDC's jurisdictions with implications for disparate impact monitoring. Georgetown Law Faculty Publications and Other Works. (2020). doi: 10.2139/ssrn.3740041
11. Tewarson H, Greene K, Fraser MR. State strategies for addressing barriers during the early US COVID-19 vaccination campaign. Am J Public Health. (2021) 111:1073–7. doi: 10.2105/AJPH.2021.306241
12. Hajibabai L, Hajbabaie A, Swann J, Vergano D. Using COVID-19 data on vaccine shipments and wastage to inform modeling and decision-making. Transp Sci. (2022) 56:1135–47. doi: 10.1287/trsc.2022.1134
13. Baxter D, Casady CB. Proactive and strategic healthcare public-private partnerships (PPPs) in the coronavirus (COVID-19) epoch. Sustainability. (2020) 12:5097. doi: 10.3390/su12125097
14. Casady CB, Baxter D. Procuring healthcare public-private partnerships (PPPs) through unsolicited proposals during the COVID-19 pandemic. J Public Procure. (2022) 22:6–16. doi: 10.1108/JOPP-07-2020-0061
15. Mudenda S, Chileshe M, Mukosha M, Hikaambo CN, Banda M, Kampamba M, et al. Zambia's response to the COVID-19 pandemic: exploring lessons, challenges and implications for future policies and strategies. Pharmacol Pharm. (2022) 13:11–33. doi: 10.4236/pp.2022.131002
16. Irvin R, Venkataramani M, Galiatsatos P, Hitchcock JD, Hemphill N, Dearey M, et al. A path forward: COVID-19 vaccine equity community education and outreach initiative. Heal Secur. (2023) 21:85–94. doi: 10.1089/hs.2022.0096
17. Saied SM, Saied EM, Kabbash IA, Abdo SAE-F. Vaccine hesitancy: Beliefs and barriers associated with COVID-19 vaccination among Egyptian medical students. J Med Virol. (2021) 93:4280–91. doi: 10.1002/jmv.26910
18. Dzinamarira T, Nachipo B, Phiri B, Musuka G. COVID-19 vaccine roll-out in South Africa and Zimbabwe: urgent need to address community preparedness, fears and hesitancy. Vaccines. (2021) 9:250. doi: 10.3390/vaccines9030250
19. Cooper S, Van Rooyen H, Wiysonge CS. COVID-19 vaccine hesitancy in South Africa: a complex social phenomenon. South African Med J. (2021) 111:702–3. doi: 10.7196/SAMJ.2021.v111i8.15800
20. Tagoe ET, Sheikh N, Morton A, Nonvignon J, Sarker AR, Williams L, et al. COVID-19 vaccination in lower-middle income countries: national stakeholder views on challenges, barriers, and potential solutions. Front Public Heal. (2021) 9:709127. doi: 10.3389/fpubh.2021.709127
21. Jacobson M, Chang TY, Shah M, Pramanik R, Shah SB. Can financial incentives and other nudges increase COVID-19 vaccinations among the vaccine hesitant? A randomized trial. Vaccine. (2022) 40:6235–42. doi: 10.1016/j.vaccine.2022.08.060
22. Campos-Mercade P, Meier AN, Schneider FH, Meier S, Pope D, Wengström E. Monetary incentives increase COVID-19 vaccinations. Science. (2021) 374:879–82. doi: 10.1126/science.abm0475
23. Moher D, Liberati A, Tetzlaff J, Altman DG, Group TP. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
24. Akers J, Aguiar-Ibáñez R, Baba-Akbari A. Systematic reviews : CRD's guidance for undertaking reviews in health care. York: CRD, University of York. (2009).
25. National Heart and Blood Institute L. Quality assessment tool for observational cohort and cross-sectional studies. Natl Institutes Heal. (2021).
26. Blair RA, Curtice T, Dow D, Grossman G. Social Science & Medicine Public trust, policing, and the COVID-19 pandemic : evidence from an electoral authoritarian regime. Soc Sci Med. (2022) 305:115045. doi: 10.1016/j.socscimed.2022.115045
27. Chilongola JO, Rwegoshola KM, Balingumu OH, Semvua HS, Kwigizile ET. COVID-19 Knowledge, Attitudes, Practices, and vaccination hesitancy in Moshi, Kilimanjaro Region, Northern Tanzania. Tanzan J Health Res. (2022) 23:1–12. doi: 10.21203/rs.3.rs-1327017/v1
28. Konje ET, Basinda N, Kapesa A, Mugassa S, Nyawale HA, Mirambo MM, et al. The coverage and acceptance spectrum of COVID-19 vaccines among healthcare professionals in western Tanzania: what can we learn from this pandemic? Vaccines. (2022) 10:1429. doi: 10.3390/vaccines10091429
29. Zavala E, Fesshaye B, Lee C, Mutwiwa S, Munyao P, Njogu R, et al. Lack of clear national policy guidance on COVID-19 vaccines influences behaviors in pregnant and lactating women in Kenya. Hum Vaccin Immunother. (2022) 18:2127561. doi: 10.1080/21645515.2022.2127561
30. Orangi S, Ojal J, Brand SP, Orlendo C, Kairu A, Aziza R, et al. Epidemiological impact and cost-effectiveness analysis of COVID-19 vaccination in Kenya. BMJ Glob Heal. (2022) 7:e009430. doi: 10.1136/bmjgh-2022-009430
31. Parker M, Baluku M, Ozunga BE, Okello B, Kermundu P, Akello G, et al. Social science & medicine epidemics and the military : responding to COVID-19 in Uganda. Soc Sci Med. (2022) 314:115482. doi: 10.1016/j.socscimed.2022.115482
32. Harris JR, Kadobera D, Kwesiga B, Kabwama SN, Bulage L, Kyobe HB, et al. Improving the effectiveness of Field Epidemiology Training Programs: characteristics that facilitated effective response to the COVID-19 pandemic in Uganda. BMC Health Serv Res. (2022) 22:1532. doi: 10.1186/s12913-022-08781-x
33. Okedi W, Wakoli C, Emojong I. The impact and sustainability of hand-hygiene practices on health facilities in the context of the COVID-19 pandemic: a case study of Busia County (Kenya). Int J Med Public Heal. (2022) 12:116–30. doi: 10.5530/ijmedph.2022.3.23
34. Mugambe RK, Id TS, Kisaka S, Id STW, Isunju JB, Nalugya A, et al. Extent of compliance with COVID-19 prevention and control guidelines among supermarkets in Kampala Capital City and Mukono Municipality, Uganda. PLoS ONE. (2021) 16:e0258840. doi: 10.1371/journal.pone.0258840
35. Mello MM, Opel DJ, Benjamin RM, Callaghan T, DiResta R, Elharake JA, et al. Effectiveness of vaccination mandates in improving uptake of COVID-19 vaccines in the USA. Lancet. (2022) 400:535–8. doi: 10.1016/S0140-6736(22)00875-3
36. Karaivanov A, Kim D, Lu SE, Shigeoka H. COVID-19 vaccination mandates and vaccine uptake. Nat Hum Behav. (2022) 6:1615–24. doi: 10.1038/s41562-022-01363-1
37. Majee W, Anakwe A, Onyeaka K, Harvey IS. The past is so present: understanding COVID-19 vaccine hesitancy among african american adults using qualitative data. J Racial Ethn Heal Dispar. (2023) 10:462–74. doi: 10.1007/s40615-022-01236-3
38. Msuya SE, Manongi RN, Jonas N, Mtei M, Amour C, Mgongo MB, et al. COVID-19 vaccine uptake and associated factors in sub-Saharan Africa: evidence from a community-based survey in Tanzania. Vaccines. (2023) 11:465. doi: 10.3390/vaccines11020465
39. Olapeju B, Hendrickson ZM, Rosen JG, Shattuck D, Storey JD, Krenn S, et al. Trends in handwashing behaviours for COVID-19 prevention: longitudinal evidence from online surveys in 10 sub-Saharan African countries. PLOS Glob Public Health. (2021) 1:e0000049. doi: 10.1371/journal.pgph.0000049
40. Howard ZL, Dalton CB, Carlson S, Baldwin Z, Durrheim DN. Impact of funding on influenza vaccine uptake in Australian children. Public Health Res Pract. (2021) 31:3112104. doi: 10.17061/phrp3112104
41. Matkovic J, Clemens KS, Faasse K, Geers AL. Handwashing message type predicts behavioral intentions in the United States at the beginning of the global COVID-19 pandemic. Front Public Health. (2021) 9:583491. doi: 10.3389/fpubh.2021.583491
42. Mbakaya BC, Lee PH, Lee RL. Hand Hygiene intervention strategies to reduce diarrhoea and respiratory infections among schoolchildren in developing countries: a systematic review. Int J Environ Res Public Health. (2017) 14:371. doi: 10.3390/ijerph14040371
43. Khazanov GK, Stewart R, Pieri MF, Huang C, Robertson CT, Schaefer KA, et al. The effectiveness of financial incentives for COVID-19 vaccination: a systematic review. Prev Med. (2023) 172:107538. doi: 10.1016/j.ypmed.2023.107538
Keywords: handwashing, COVID-19 vaccine, uptake, policy, government, Kenya, Uganda, Tanzania
Citation: Muchangi JM, Mturi J, Mukasa H, Kithuki K, Kosgei SJ, Kanyangi LM, Moraro R, Kamau S and Nankanja M (2024) Influence of government policies on handwashing and vaccine uptake in Kenya, Uganda, and Tanzania to prevent and control COVID-19: a systematic review. Front. Public Health 12:1417866. doi: 10.3389/fpubh.2024.1417866
Received: 15 April 2024; Accepted: 20 November 2024;
Published: 18 December 2024.
Edited by:
Bolanle Olapeju, Uniformed Services University of the Health Sciences, United StatesReviewed by:
Marco Tagliabue, Oslo Metropolitan University, NorwayCopyright © 2024 Muchangi, Mturi, Mukasa, Kithuki, Kosgei, Kanyangi, Moraro, Kamau and Nankanja. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Josphat Martin Muchangi, TWFydGluLk11Y2hhbmdpQGFtcmVmLm9yZw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.