
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Public Health, 09 September 2024
Sec. Infectious Diseases: Epidemiology and Prevention
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1417638
 Yilma Chisha1*
Yilma Chisha1* Tesfaye Feleke1
Tesfaye Feleke1 Eshetu Andarge Zeleke1,2Zeleke Aschalew1
Eshetu Andarge Zeleke1,2Zeleke Aschalew1 Zeleke Girma Abate1
Zeleke Girma Abate1 Yosef Haile1
Yosef Haile1 Mulugeta Dalbo3
Mulugeta Dalbo3 Misganu Endriyas4
Misganu Endriyas4Background: Febrile illnesses are commonly reported as a primary reason for seeking healthcare in sub-Saharan Africa. Timely diagnosis and getting prompt treatment within 24 h of fever onset is crucial to avert the risk of developing severe complications and death. Understanding factors contributing to delayed health seeking is important for public health interventions. Hence, this study aimed to assess individual- and contextual-level factors associated with the delay in seeking prompt treatment for children with fever.
Method: A community-based cross-sectional study was conducted from September 2022 to June 2023 in Gamo zone, southern Ethiopia. Three districts were chosen, and then, from each district, six clusters or kebeles were chosen by simple random sampling. A total of 820 caregivers were randomly selected. A two-level mixed-effects logistic regression model was employed to identify factors associated with the delay in seeking prompt treatment. The associations were measured by an adjusted odds ratio (AOR), and statistical significance was declared at a 5% level of significance.
Result: The prevalence of the delay in seeking prompt care was 47.8%. Factors contributing to the delay were caregivers who were aged 30 years and above [AOR 0.23, 95% confidence interval (CI): 0.10–0.52], caregivers who followed the Protestant religion (AOR 3.67, 95% CI: 2.08–6.48), caregivers unable to read and write (AOR 5.32, 95% CI: 6.80–11.70), merchant caregivers (AOR 6.63, 95% CI: 2.75–15.97), caregivers who were exposed to only one media source (AOR 9.3, 95% CI: 8.43–15.60), caregivers with the experience of child death (AOR 0.05, 95% CI: 0.01–0.22), and caregivers seeking permission from their partners to access healthcare (AOR 12.64, 95% CI: 6.98–22.89).
Conclusion and recommendations: There was a high level of delay in seeking healthcare. Targeted community education through mass media, healthcare facilities, and community-level awareness campaigns should be strengthened to improve early treatment seeking and lessen the consequences of delayed treatment seeking.
Fever is a non-specific response to various infectious and non-infectious triggers. It is indeed a significant public health concern and a prevalent clinical symptom in children under 5 years of age who visit healthcare facilities (1, 2). Febrile illnesses are commonly reported as a primary reason for seeking healthcare in sub-Saharan Africa (SSA) (3, 4), and a substantial majority (over 80%) of pediatric consultations in resource-limited countries are attributed to febrile illnesses (5, 6).
In SSA, fever cases are often treated using a combination of modern and traditional medicines in community settings (7, 8). Fever can be associated with various childhood illnesses, including bacterial infections, parasitic infections, and upper or lower respiratory tract viral infections (9, 10). However, in areas where malaria is prevalent, fever is strongly indicative of a potential malaria infection and plays a significant role in influencing decisions regarding malaria treatment (11, 12). In health facilities across SSA, ~30–40% of all fever cases are attributed to malaria, with significant seasonal variations between rainy and dry seasons (13). Malaria is a major public health concern in Ethiopia, with ~75% of the country's landmass considered at risk of malaria (areas below 2,000 m altitude) and 68% of the population residing in malaria risk areas (14–17).
The World Health Organization (WHO) recommends confirming the presence of plasmodium species through testing before starting anti-malaria treatment (18). In addition, it is now evident that febrile children under the age of five should be investigated for other potential causes of fever as there are significant proportions of patients with fever caused by infections other than malaria (9, 19). It is important for caregivers of children to seek medical care within 24 h of the onset of fever to ensure timely diagnosis and appropriate management (9). If a child is not diagnosed early and does not receive prompt treatment, the child is at risk of developing severe complications and potential fatalities associated with malaria (20). Malaria is a significant global health issue, particularly in Africa. In 2015, it caused 429,000 estimated deaths worldwide, with over 75% of those deaths occurring in children under 5 years of age. Tragically, it is estimated that malaria claims the life of one child every 2 min (21, 22). In Africa alone, there are 300–500 million estimated cases of malaria each year, resulting in ~1 million malaria-related deaths.
More than 90% of these deaths occur in children under 5 years of age (23). In Ethiopia, malaria is the leading communicable disease, accounting for ~30% of the overall disability-adjusted life years lost (24). Annually, there are over five million new cases of malaria in Ethiopia (25, 26), making it the leading cause of outpatient visits, health facility admissions, and inpatient deaths for children under 5 years of age (27, 28). In 2016, an estimated US$ 2.7 billion was invested globally in malaria control and elimination efforts, with ~74% of the funding allocated to the WHO African Region. Despite these investments, malaria continues to be a significant burden for African countries (29). Studies have shown that many deaths related to febrile illnesses, including malaria, occur at home without patients receiving appropriate medical care, and when care is sought, it is often delayed (30–33). Prompt and effective treatment involves administering recommended medicines within 24 h of fever onset after confirming the root cause of the fever. Timely access to effective treatment, particularly with first-line artemisinin combination therapies (ACTs), is crucial in preventing the progression of the disease to the severe stage and reducing mortality, especially among children under 5 years of age. However, the proportion of febrile patients receiving prompt and effective treatment across SSA remains low (34–37).
It is true that populations in Ethiopia, including the population in Gamo zone, have been facing various diseases, both communicable and non-communicable. Among the communicable diseases, acute febrile illnesses, such as malaria, are of particular concern and have a significant impact on public health. In response to this, the Federal Ministry of Health (FMOH) has developed a national strategic plan for malaria prevention and control (38). This plan focuses on early diagnosis and prompt treatment, selective vector control, the use of insecticide-treated nets (ITNs) for mosquitoes, and environmental management. Despite these efforts, challenges still persist in effectively addressing the issue. Early diagnosis and prompt treatment are crucial in saving lives from acute febrile illnesses, including malaria. However, there is limited information on healthcare-seeking behavior among households of febrile children in Ethiopia, particularly in Gamo zone. This study aimed to fill the knowledge gap by examining individual- and contextual-level factors that influence prompt healthcare-seeking behavior of caregivers of febrile children under 5 years of age. By understanding these factors, we can improve strategies to encourage timely seeking of healthcare for febrile illnesses in Ethiopia.
A community-based cross-sectional survey was conducted in Gamo zone from September 2022 to June 2023. Gamo zone is in southern Ethiopia. Arbaminch town, the capital of Gamo zone, is situated ~505 km southwest of Addis Ababa, the capital of Ethiopia, and 134 km from Wolaita Soddo, the administrative and political center of South Ethiopia state. Administratively, the zone is subdivided into woredas (districts) and towns, which are again subdivided into kebeles. A kebele is the smallest administrative structure with an estimated population of 5,000. According to the 2007 census, the total population of Gamo zone was projected to be 1,341,901. The zone has one general hospital, five primary hospitals, 33 private clinics, and 56 public health centers according to the information gathered from officials of the health department. Malaria consistently ranks among the top 10 diseases for adults and the top five diseases for children every year, as reported by health officials.
The source population consisted of all caregivers living in Gamo zone who had children under the age of five diagnosed with fever before 1 month of the survey. The study population included households with children under the age of five who had fever within 1 month before the survey and met the inclusion criteria. These households were randomly selected from the selected kebele. Caregivers with children under the age of five who had fever within 1 month before the survey and who had been residing in Gamo zone for at least 6 months were included in the study. However, caregivers who were mentally handicapped or critically ill and unable to respond to the interview were excluded from the study.
The minimum sample size for this cross-sectional study was calculated using the one population proportion formula. The following assumptions were considered:
• The proportion of the delay in seeking prompt treatment among caregivers was 49.4% (39).
• The level of significance (α) was set at 5%.
• The standard normal curve or Z at a 95% confidence interval (CI; two-tailed) was 1.96.
• The margin of error (E) was 5%.
• The estimated power of the study was 80%.
• The formula used to calculate the sample size was
• To account for a 10% non-response rate, 38 caregivers were added to the sample size, resulting in a total of 422 caregivers. Finally, after multiplying the sample size by 2 (Design Effect), the total sample size required for the study was 844 caregivers.
The sampling procedure for this study involved selecting three out of 14 administrative districts through a simple random sampling method. From each of the three selected districts, six kebeles (clusters) were chosen again through the simple random sampling method, resulting in a total of 18 clusters for the study. Lists of households with children under the age of five who experienced fever within 1 month preceding the survey were obtained from each selected cluster and inputted into Microsoft Excel on Windows 10. Using this program, a random selection process was conducted to choose a total of 820. If there were two children under the age of five with fever in the household, the younger child was included (Figure 1).
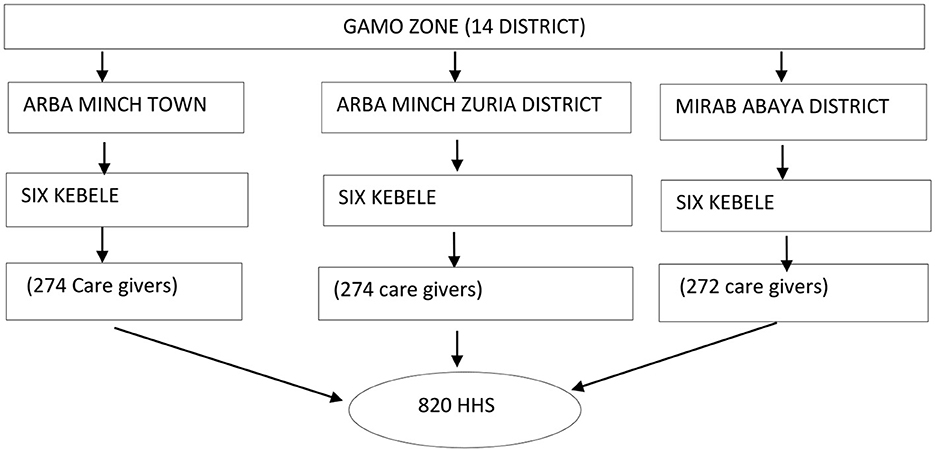
Figure 1. Schematic representation of the sampling procedure in Gamo zone, 2022/23.
The questionnaire used in the study was developed based on relevant literature from different parts of Ethiopia and Africa (46, 51, 52, 55) and adapted to the local context. It was translated from English to Amharic and then back to English by experts to ensure consistency. Nine diploma nurse data collectors and five degree-holding nurse supervisors were trained for 2 days by the investigators to ensure accurate data collection. They were trained on the purpose of the study, how to interview study subjects, and how to supervise the data collection process. A census was conducted, and we identified 1,356 households with children under the age of five who had experienced fever within 1 month before the survey. From this figure, 820 caregivers were randomly selected for the interview. Face-to-face interviews were conducted with the selected caregivers using interviewer-administered data collection techniques through a hand-held digital device using the Kobo collect toolbox data collection platform. In cases where the household members were not present during the initial data collection, a repeat visit was made. For households with multiple children under the age of five, the younger child was purposefully selected for data collection. In the case of households with twins, one child was selected using a lottery method. The data collection process spanned 15 consecutive days, and the data collection format included information on child-, household-, and community-level characteristics.
Multi-level modeling refers to a modeling approach that is carried out for more than one level. This means that the data are organized in a hierarchical order, with units nested within each other.
The clustering of units into a hierarchical order is referred to as nesting.
The fixed part of a model, represented by Xβ, represents the average relationship between the predictor variable (X) and the outcome variable (Y). It is a component of the model that remains constant across all levels.
It refers to a situation where the caregiver takes children under the age of five to the healthcare facility after 24 h of fever onset.
It refers to timely and appropriate treatment with recommended medicines within 24 h after the onset of fever.
In the context of multi-level modeling, individual-level factors refer to factors related to the child, household, and caregiver. These factors are specific to each individual within the hierarchical structure.
These factors refer to community-related factors that may influence behavior or outcomes. They operate at a higher level than individual-level factors and can impact multiple individuals within the community.
In this context, behavior refers to the response of an individual or group to an action, environment, or stimulus. It can encompass a wide range of actions or reactions exhibited by individuals or groups in different situations.
The dependent variable for this research was the delay in healthcare seeking for febrile children under the age of 5 years. It was coded as “0” for non-delay and “1” for delay, with delay referring to seeking treatment after 24 h of fever onset.
To analyze factors influencing this delay, two sets of independent variables were considered due to the nested nature of the study. These sets included child- and household-level variables (individual-level variables) and contextual-level variables (community-level variables).
The child-level variables included the age of the child in completed months, sex of the child, birth order of the child, and history of child death in the household.
The household-level variables included the socio-demographic and other characteristics of caregivers, such as age and sex of the household leader, educational status, marital status, type of marriage, relationship of the caregiver with the child, occupation, monthly income, possession of health insurance, caregviers' media exposure and media asset availability at home, source of health information for the households, caregiver's perception of the capability of protecting his/her family from malaria, knowledge, perception, and practice toward malaria, religion, distance of the household to the nearest health facility, number of household members, number of children under the age of five at home, decision maker in the household for obtaining healthcare, and so on.
The community-level variables included in this study were composed of place of residence and average score community-level educational status. Since the lower-level factors were nested on the higher-level factors (community), the framework was circular in shape (Figure 2).
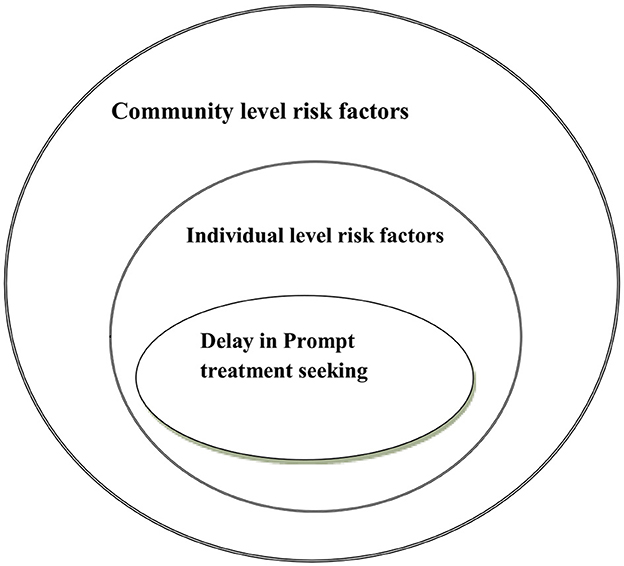
Figure 2. Conceptual framework of the individual- and contextual-level determinants of the delay in seeking prompt treatment for febrile children under the age of five, 2022.
The data collection for this study was conducted through a face-to-face interviewer-administered technique using a hand-held digital device and the Kobo collect toolbox data collection platform. Subsequently, the data were transferred to StataMP version 17 for data management and analysis purposes. Data cleaning procedures were performed to ensure the quality of the data. Furthermore, a test of normality, specifically the Shapiro–Wilk test, was conducted to identify and manage extreme values if they were present in the dataset. Coding, categorizing, labeling, and aggregating were also carried out as part of the data management process.
Several measures were taken to ensure data quality. Data cleaning was performed to assess completeness, consistency, and extreme values. In addition, a 2-day training session was provided to both the data collectors and supervisors to ensure their understanding of the data collection process. A pre-test was conducted on 5% of caregivers (households) outside of the study clusters to validate the data collection tools (Eligo Wozeka). Based on the results of the pre-test, necessary corrections were made, and the questionnaire was further modified to improve its effectiveness. These steps were taken to enhance the accuracy and reliability of the collected data.
Two-level (individual and community) data modeling was performed. Direct modeling of the clustered data was performed without sample weighting. This was possible because an equal number of samples were taken from each cluster. For continuous variables that followed a normal distribution, the mean (±SD) was used, while for continuous variables that did not follow a normal distribution, the median [interquartile range (IQR)] was used. Categorical predictors were presented as frequency and percentage.
In traditional or ordinary regression models, study subjects are assumed to be independent in relation to the outcome being studied. However, when data are structured in hierarchies, such as clusters, units within the same group are often not independent. The units within the same cluster tend to be more similar to each other in terms of the outcome of interest compared to the units from different clusters. This violation of the assumption of independence can lead to the underestimation of standard errors and an increased type I error rate (false-positive results). To address this issue, multi-level modeling was employed.
Multi-level modeling allows for simultaneous consideration of factors at both individual and community levels, providing a more robust understanding of the factors associated with the outcome variable. By accounting for the hierarchical structure of data, multi-level modeling helps mitigate the effects of violating the assumption of independence and improves the accuracy of results. The intra-community correlation (ICC) was calculated to measure the community effect and account for the clustered data nature, within-community and between-community variations. The ICC helps in determining the extent of similarity or correlation within each community. By considering the ICC, we could appropriately choose the method for determining the factors associated with prompt healthcare seeking among caregivers with children under the age of five. The ICC was approximated as follows:
where σu2 denotes community-level variance, and σe2 denotes individual-level variance that is fixed for log distribution to π2/3 or the value of 3.29. In this study, the value of the ICC being above zero indicates that the multi-level logistic regression model is considered better for predicting the outcome of interest compared to the traditional or standard binary logistic regression analysis model. A two-level mixed-effect logistic regression model was fitted to estimate the effects of explanatory variables and community-level random effects on the delay in treatment-seeking behavior. The first level represents the individual level, while the second level represents the community level. The model aimed to estimate both the independent (fixed) effects of the explanatory variables and the community-level random effects on the log probability of the delay in prompt treatment seeking. The specific formulation of the two-level multi-level model used to model the log probability of the delay in prompt treatment seeking is provided in the study, outlining the variables and their respective effects within the model. The log of the probability of the delay in prompt treatment seeking was modeled using the two-level multi-level model as follows:
In the given context, i and j represent level 1 (individual) and level 2 (community or cluster) units, respectively. The variables X and Z refer to the individual- and community-level variables, respectively. The probability of the delay in treatment seeking by the ith caregiver in the jth community is represented by πij. The β's are fixed coefficients, indicating that for every one unit increase in X or Z (a set of predictor variables), there is a corresponding effect on the probability of the caregiver delaying prompt treatment seeking. The intercept, β0, represents the effect on the probability of the caregiver delaying treatment in the absence of any influence from predictors. The random effect Uj represents the effect of the community level or cluster level on the decision of the caregiver regarding treatment seeking. Statistical analysis was conducted to examine the relationship between the delay in treatment seeking and various predictors. The analysis involved building models, including a null model as a baseline for comparison. A median odds ratio (MOR) was calculated in the null model to measure the median value of the odds ratio to depict variations in the delay in treatment seeking between the randomly chosen households from the clusters that had high rates of delay and the households from the clusters that had low rates of delay. The proportional change in variance (PCV) was used to estimate the portion of the outcome variable explained by different models.
A stepwise backward elimination model-building procedure was employed, and information criteria [Akaike information criterion (AIC) and Bayesian information criterion (BIC)] were used for the model comparison and selection of the final parsimonious model. Interactions and cofounders were tested using the changes in the regression coefficients, with a cutoff point of 15–20% beta change (40). Multi-collinearity was assessed using the variance inflation factor (VIF) with a cutoff point of a mean VIF > 10 (41). The value of the mean VIF was 8.4. Based on the above, it was determined that there was no potential collinearity between covariates that violated our estimation. The classification of the data in the final model was evaluated using the receiver observed characteristics (ROC) curve, and ~92.4% of the data were correctly classified. The associations between the delay in treatment-seeking behavior and predictors were summarized using an adjusted odds ratio (AOR) and corresponding 95% confidence interval. Statistical significance was determined using the Wald chi-square test with a p-value threshold of 0.05.
The study obtained ethical approval from the institutional research ethical review board of Arba Minch University. In addition, a letter of permission was obtained from the Gamo zone health department, selected districts, and kebeles. Before data collection, the participants were informed about the overall aim of the survey, and written informed consent was obtained from the head of the household or the children's caregivers. The participants were assigned identification numbers to ensure confidentiality. In cases febrile children were identified during the data collection, they were referred to the nearest health facility to receive appropriate healthcare.
Out of the initial 844 households with children under the age of five with fever that were expected to be included, 820 households were actually included in the study, resulting in a response rate of 97.2%. From the 820 caregivers, 409 (49.9%) sought care early, 374 (45.6%) delayed seeking care, and 37 (4.5%) did not seek care at all. Approximately two-thirds, 532 (67.9%), of the households had a male head. The majority of the caregivers 655 (83.7%) fell within the age group of 30 years and below. More than three-fourths, 607 (77.5%), of the study participants resided in rural areas. Out of the total study participants, 643 (82.1%) reported having only one child under the age of five at home (Table 1).
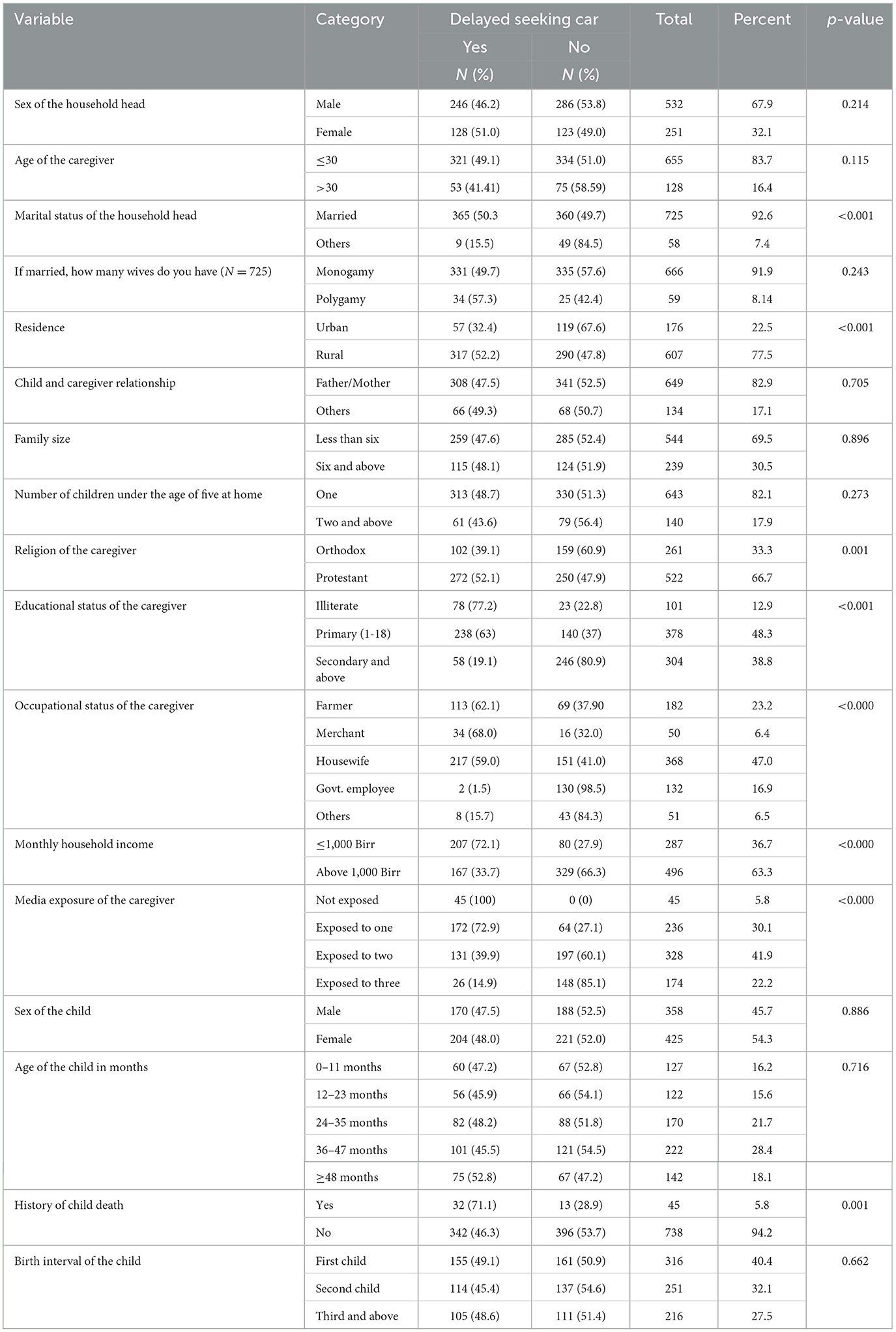
Table 1. Socio-demographic characteristics of the caregivers who delayed seeking care for febrile children in Gamo zone, Ethiopia 2022 (N = 783).
According to the information provided, nearly half, 378 (48.3%), of the caregivers had an educational level of grades 1–8. In addition, ~101 (12.9%) of the caregivers reported that they had no education or literacy skills. In terms of occupation, nearly half, 368 (47.0%), of the caregivers identified themselves as housewives, followed by farmers. Furthermore, ~132 (16.9%) of the caregivers stated that they were government employees. Only 51 (6.5%) of the caregivers were engaged in other occupational identities, such as student, daily laborer, Bajaj driver, or fisherman. Regarding the monthly household income, 496 (63.3%) reported earning more than 1,000 birr per month (Table 1).
In addition, 328 (41.9%) caregivers mentioned having exposure to two media sources, namely television and radio, along with owning a mobile phone. On the other hand, only 45 (5.8%) caregivers reported not being exposed to any media sources. Regarding characteristics of the children, more than half, 425 (54.3%), were female. Approximately 222 (28.4%) children fell within the age category of 36–47 months. The median age of the children was 32.5 months, with an interquartile range (IQR) of 26 months (Table 1).
According to the information provided, all study participants in the study area were aware of the disease malaria. The primary source of information about malaria for the participants was healthcaregivers (Figure 3).
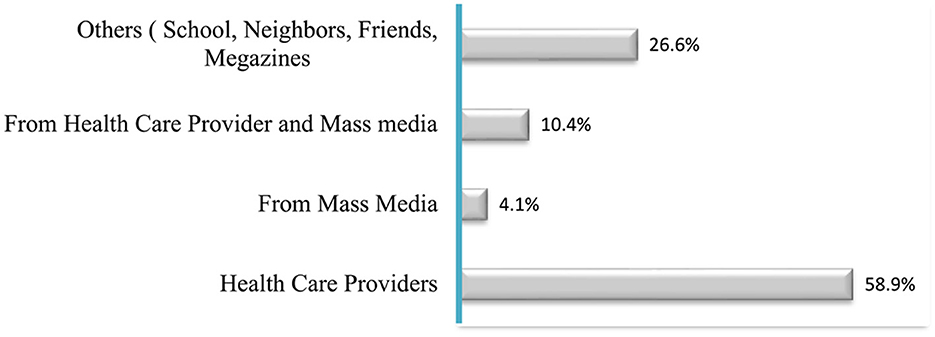
Figure 3. Percentage of the information sources for malaria and its prevention methods among the study participants, Gamo zone, 2022 (N = 820).
Based on the data provided, it was revealed that the majority (40%) of the respondents identified March to May as the peak season for the burden of malaria (Figure 4).
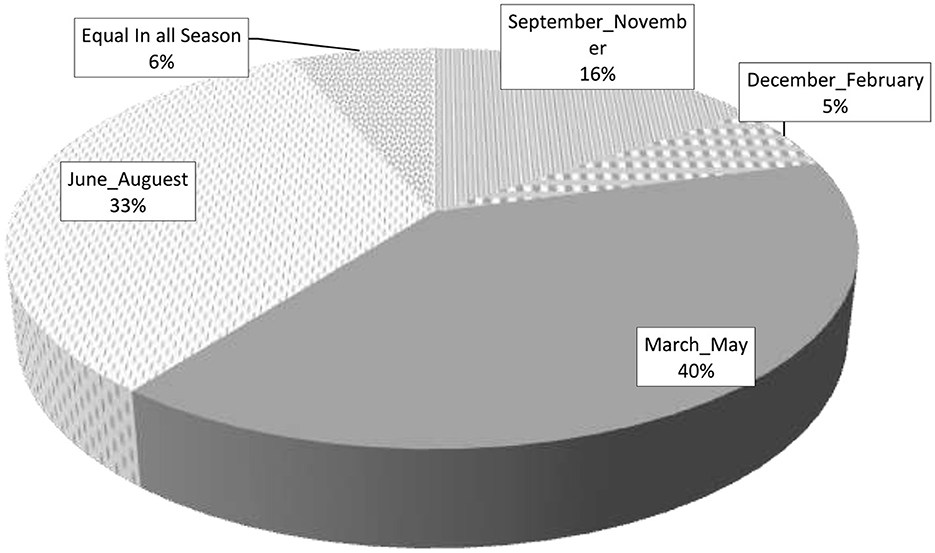
Figure 4. Percentage of the malaria peak season reported by the study participants, Gamo zone, 2022 (N = 820).
It was evident that a significant portion of the respondents had knowledge about malaria and its prevention. The majority (77.6%) of the respondents recognized malaria as a public health problem in the study area. In addition, a high percentage of the respondents (80.6%) were aware of the use of modern medications for malaria, with a majority (84.6%) correctly identifying Coartem as the drug of choice. Furthermore, a large proportion of the participants (75.9%) were knowledgeable about the signs and symptoms of malaria and identified pregnant women and children under the age of five as the most at-risk population groups (73.8%). Moreover, a substantial number of the respondents (84.4%) were able to clearly report at least one of the major preventive methods for malaria. Nearly two-thirds of the participants (66.4%) knew about the major complications of untreated malaria, and only 58.5% of the participants correctly identified mosquito bites as the cause of malaria (Table 2). Based on the dichotomized scoring of the participants' knowledge out of 10 items, the mean score was calculated to be 6.95 ± 1.97. Out of the total participants, 424 (54.1%) scored at or above the mean, which was operationally defined as having good knowledge about malaria and its prevention. On the other hand, 359 (45.9%) of the participants scored below the mean, and they were categorized as having poor knowledge about this area (Table 2).
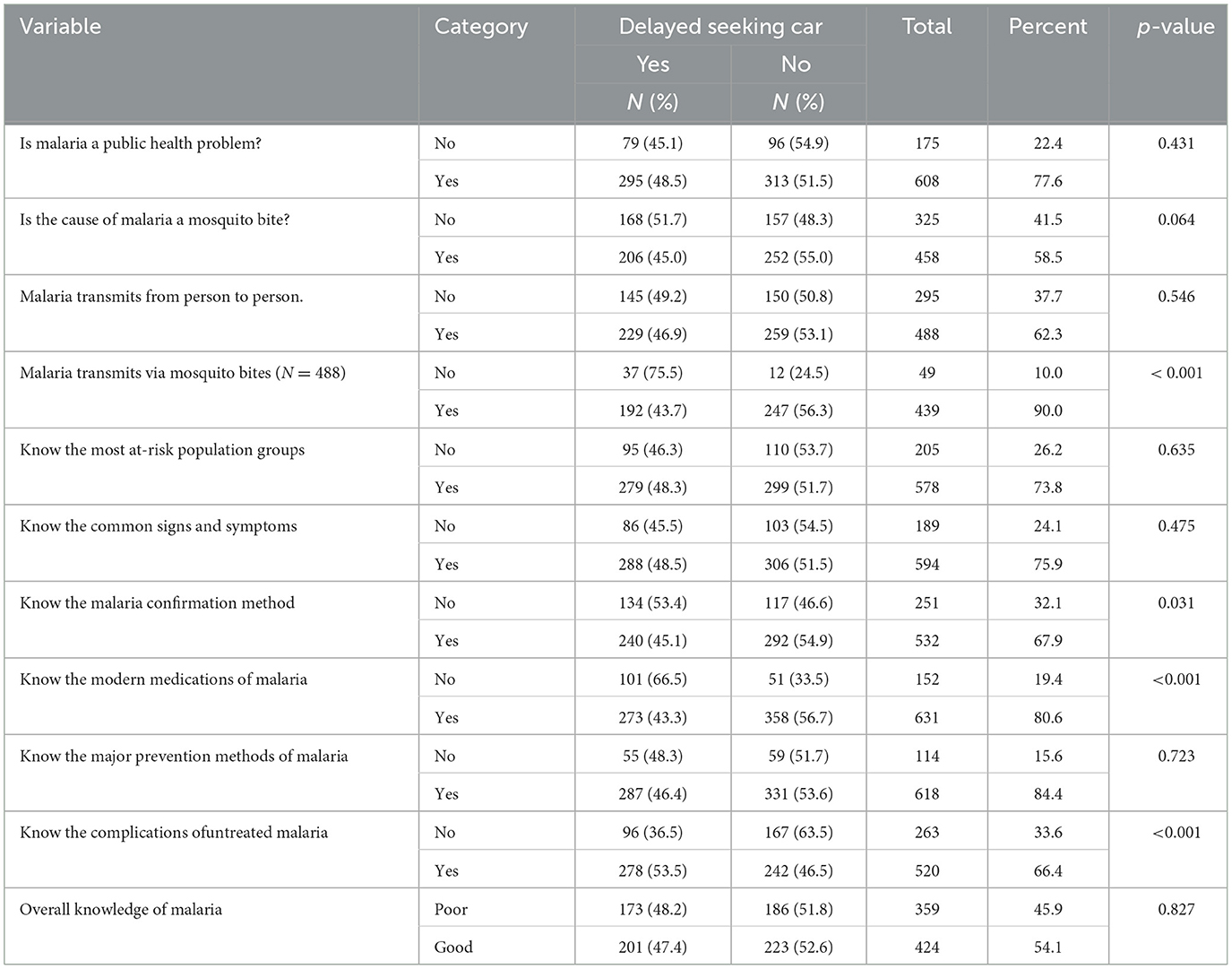
Table 2. Knowledge of the caregivers about malaria and its prevention methods and the delay in seeking care among the study participants in Gamo zone, South Ethiopia, 2022 (N = 783).
Out of 820 study participants, 783 (95.5%) took their febrile children to a healthcare facility and 37 (4.5%) gave homemade treatment. Among those who took their children to a healthcare facility, it was found that 374 (47.8%), 95% CI (44.3%, 51.3%), of the respondents in the study area experienced delay in seeking early treatment for their febrile children within 24 h. The majority of those who reported delay (56.7%) mentioned waiting for permission from their partner as a reason for the delay. In terms of healthcare costs, for more than half of the respondents, 424 (51.71%), the costs were covered by household pocket purchases, while for 396 respondents (48.29%), the healthcare costs were covered by the community-based health insurance (CBHI) scheme (Table 3).
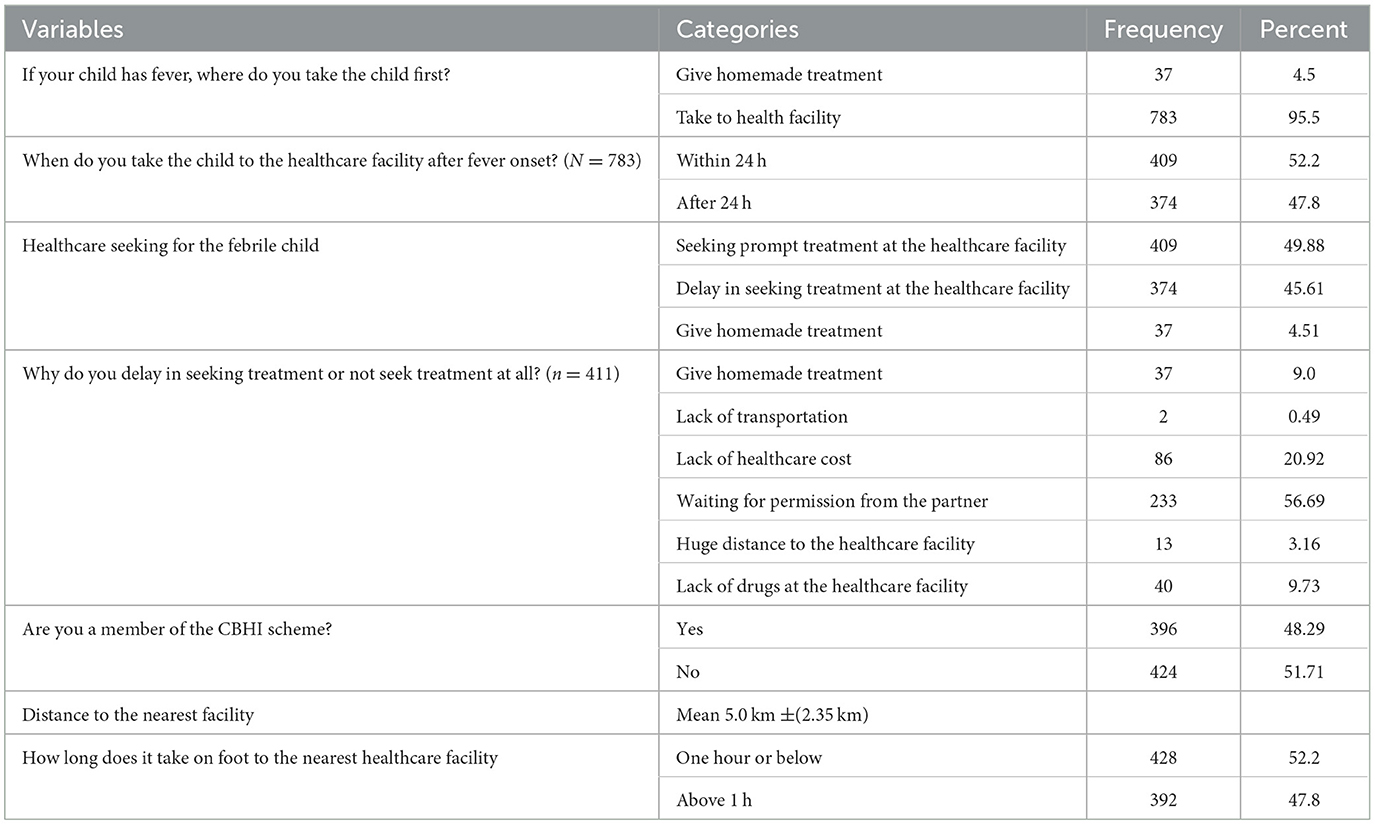
Table 3. Healthcare seeking and other characteristics of the study participants, Gamo zone, 2022.
Bivariable multi-level logistic regression analysis was conducted to select candidate variables for multivariable multi-level logistic regression analysis. The variables that met the preset criteria with a p-value of 0.25 and below were sex of the household head, age of the caregiver, marital status, type of marriage, residence, religion, educational status, average score community education, occupational status, monthly income, media exposure, history of child death, distance to the nearest health facility, and need for permission from the partner to obtain healthcare. These were identified as the candidate variables for the multivariable multi-level model (Table 4).
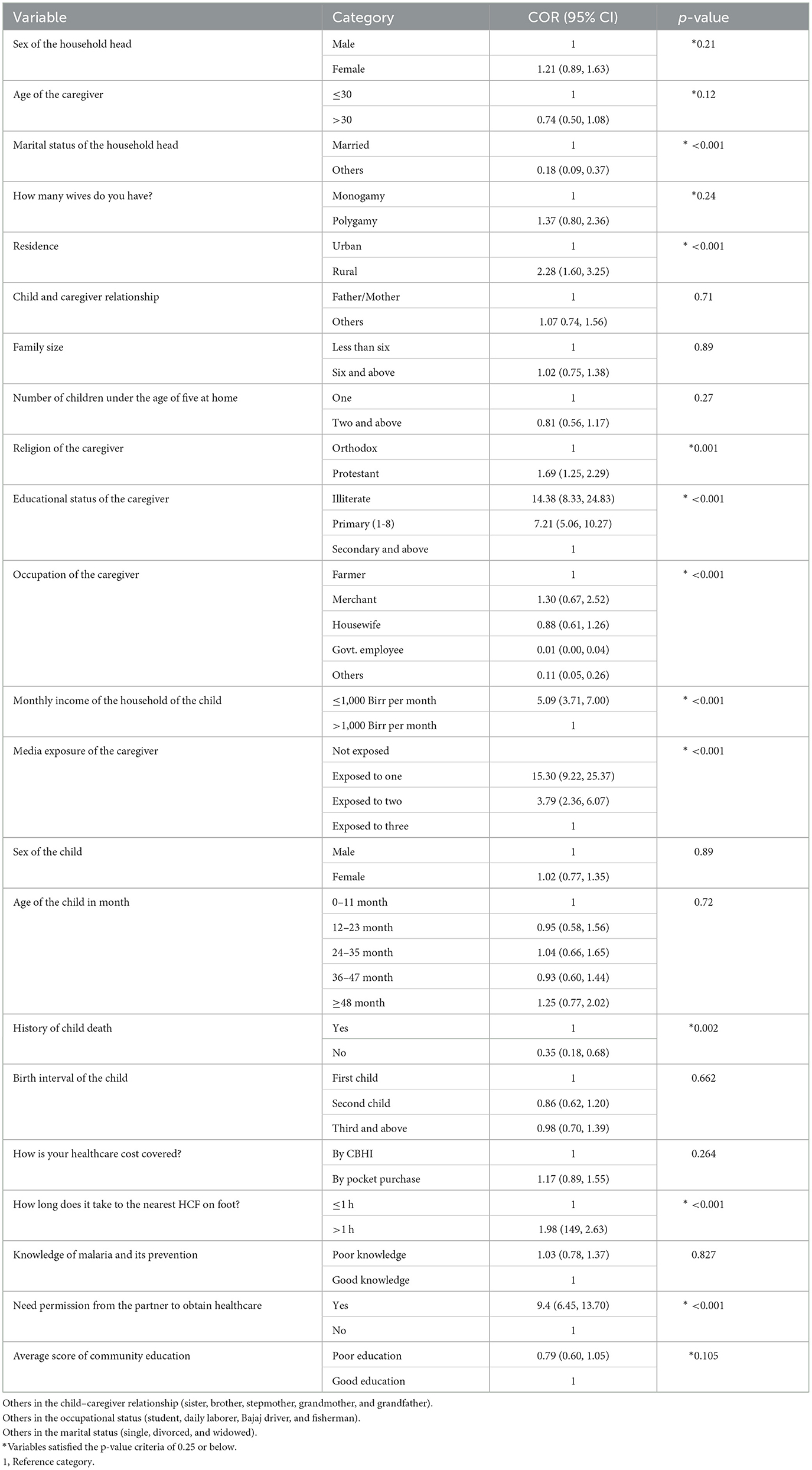
Table 4. Bivariable multi-level logistic regression analysis results, Gamo zone, 2022.
The intraclass correlation coefficient (ICC) in the null model was found to be 6%, indicating that 6% of the variability in the delay in prompt treatment seeking for febrile children under the age of five was attributed to differences between the clusters or unobserved factors at the community level. The Akaike information criterion (AIC) in model 4 was the smallest, which was 551.27, making it the best-fitted model for the data. Therefore, all the interpretations and reports were based on model 4. Furthermore, the median odds ratio (MOR) in the null model was >1, suggesting variations in the delay in prompt treatment seeking between the study clusters in the zone. When we randomly selected two caregivers from the clusters with a high rate and low rate of delay, the caregivers from the cluster with a high rate of delay were 52% more likely to access treatment after 24 h for febrile children compared to their counterparts (MOD = 1.52). The high level of variance in the delay in seeking prompt treatment for febrile children was contributed by caregiver-related factors (variance 22.7, MOR 1.58). In addition, the proportional change in variance (PCV) value in the fourth model indicated that almost 39.6% of the variability in the delay in prompt treatment seeking was explained or determined by both individual-level and community-level predictors. This highlights the importance of considering both individual- and community-level factors in understanding and addressing delays in seeking prompt treatment (Table 5).
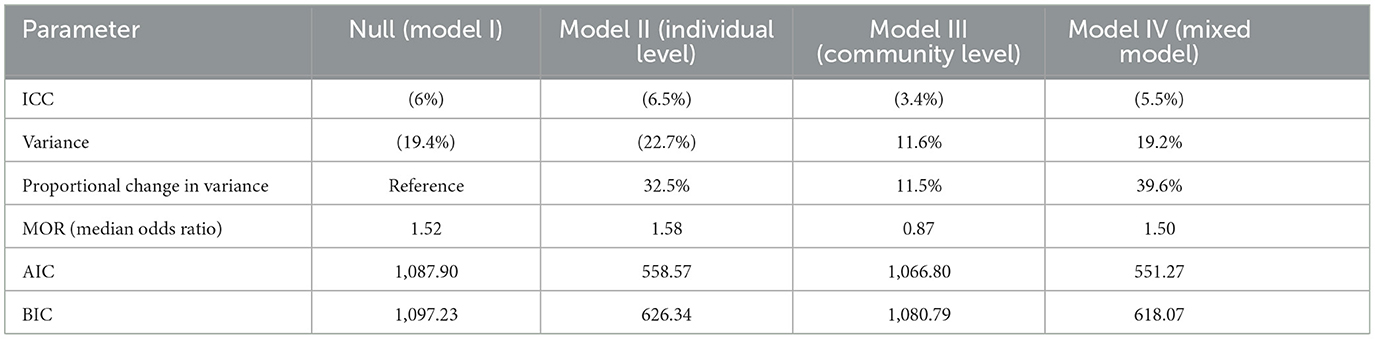
Table 5. Model summary of all models used in the analysis.
Out of 14 variables that met the preset p-value criteria of 0.25 to be considered candidate variables for the multivariable multi-level logistic regression analysis, half of them (50%) were identified as predictors of the delay in seeking prompt treatment in the multivariable analysis. These predictors included the following: age of the caregiver, educational status of the caregiver, occupation of the caregiver, religious preference of the caregiver, media exposure status of the caregiver, history of child death at the home, and need for permission to access healthcare services from the partner. These variables were found to have a significant impact on the delay in seeking prompt treatment. This information can help in understanding the factors influencing delays in accessing healthcare services and can guide interventions to improve timely treatment seeking (Table 6).
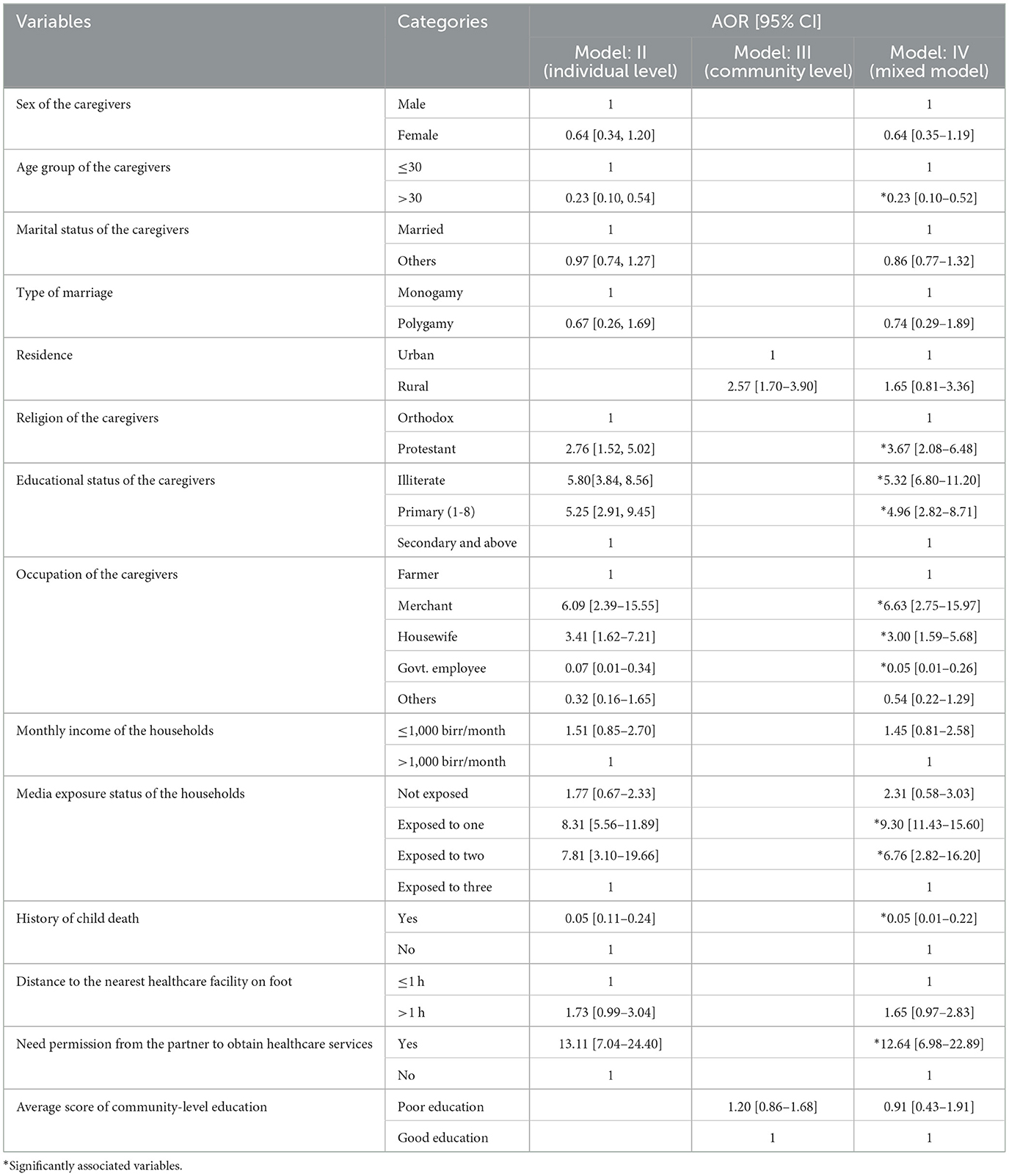
Table 6. Multivariable multi-level logistic regression analysis of the factors associated with the delay in seeking prompt treatment among the caregivers with febrile children, Gamo zone, 2022.
According to the multivariable multi-level analysis, caregivers aged 30 years and above were 77% (AOR 95% CI: 0.23 [0.10–0.52]) less likely to delay in seeking prompt treatment for febrile children compared to the age of the caregiver being 30 years or younger. In addition, the caregivers who followed the Protestant religion were found to be 3.67 (AOR 95% CI: 3.67 [2.08–6.48]) times more likely to delay in seeking prompt treatment for febrile children compared to the caregivers who followed the Orthodox religion. The educational status of the caregivers was found to be statistically and significantly associated with the delay in seeking prompt treatment for febrile children. Specifically, the caregivers who were unable to read and write or illiterate were 5.32 (AOR 95% CI: 5.32 [6.80–11.70]) times more likely to delay in seeking prompt treatment compared to the caregivers who had a high school education or above. Similarly, the caregivers who had completed primary-level education (Grades 1–8) were 4.96 (AOR 95% CI: 4.96 [2.82–8.71]) were almost five times more likely to delay in seeking prompt treatment compared to the caregivers with a high school education or above. The occupation of the caregivers was found to have a significant impact on the delay in seeking prompt treatment for febrile children.
Merchant caregivers were 6.63 (AOR: 95% CI: 6.63 [2.75–15.97]) times more likely to delay in seeking treatment within 24 h compared to farmer caregivers. Similarly, the caregivers who were housewives were three times (AOR 95% CI: 3.00 [1.59–5.68]) more likely to delay in seeking prompt treatment compared to the caregivers who were farmers. On the other hand, government employees exhibited better prompt treatment-seeking behavior compared to farmers. The odds of the delay in seeking treatment within 24 h for febrile children were 95% less likely (AOR 95% CI: 0.05 [0.01–0.26]) for the caregivers who were government employees compared to the caregivers who were farmers. The number of media sources to which the caregivers were exposed was found to impact the delay in seeking prompt treatment for febrile children. The caregivers who were exposed to only one media source were 9.3 times (AOR 95% CI: 9.3 [8.43–15.60]) more likely to delay seeking treatment within 24 h compared to the caregivers who were exposed to three or more media sources. Similarly, the caregivers who were exposed to two media sources were 6.76 times (AOR 95% CI: 6.76 [2.82–16.20]) more likely to delay in seeking prompt treatment within 24 h compared to the caregivers who were exposed to three or more media sources. The caregivers who had previously experienced a child death were found to be 95% (AOR 95% CI: 0.05 [0.01–0.22]) less likely to delay in seeking prompt treatment compared to the caregivers with no history of previous child death. Seeking permission from the partner before accessing healthcare services for a child with fever was found to be significantly associated with the delay in seeking treatment within 24 h. The caregivers who required permission from their partners were found to be over 10 times more likely to experience delay in seeking prompt treatment for a child with fever compared to their counterparts (AOR 95% CI: 12.64 [6.98–22.89]; Table 6).
The current study highlighted that 47.8% (95% CI: 44.3–51.3%) of the caregivers delayed seeking early treatment for febrile children, indicating that only 52.2% sought prompt treatment within 24 h. This finding aligns with a similar multicounty study in SSA, where Kenya reported 50.6% prompt treatment and 49.4% delay (42). However, the percentage was lower than that of other countries, such as Angola, 57.8%; Benin, 77.8%; Ghana, 55.2%; Liberia, 61.3%; Malawi, 73.3%; Mozambique, 74.4%; Rwanda, 70.8%; Senegal, 73.0%; Tanzania, 68.9%; Uganda, 65.4%; Zambia, 53.4%; and Zanzibar, 87.2% (42–46). The variation in the results could be attributed to the zonal focus of the current study compared to the broader national scope of the previous studies. In addition, social desirability bias might have influenced responses, leading to potential over-reporting of prompt treatment-seeking behavior. This information underscores the importance of addressing delays in seeking healthcare for febrile children to improve overall health outcomes.
The study indicated that the caregivers aged over 30 years were 77% less likely to delay seeking prompt treatment for febrile children compared to the caregivers aged 30 years or younger. This finding is consistent with the findings of previous studies (47, 48), which suggested that older caregivers are more inclined to seek appropriate healthcare for their children. This might be due to older caregivers often having more experience in providing adequate care and knowing when to seek treatment for sick children. In addition, individuals over 30 years could be financially more stable, which reduces the likelihood of delaying treatment due to economic constraints. However, other studies conducted in the Rwimi town of Uganda (49) and the Mandura district in southwest Ethiopia (46) revealed that caregivers aged 30 years or younger were significantly more likely to seek early treatment within 24 h compared to caregivers over the age of 30 years. This difference could be attributed to younger caregivers potentially having fewer household responsibilities and more time and energy to seek treatment for their children, including being able to walk long distances if needed. The roles and responsibilities at home increase when the age of the caregiver increases. Further research through prospective cohort studies could help identify the real-life determinants behind these inconsistencies.
This research indicated that the caregivers who were Protestant followers were 3.67 times more likely to delay seeking prompt treatment for febrile children compared to those of the Orthodox faith. This aligns with a similar study in Kigali, Rwanda (50), which suggested that gospel believer caregivers might first turn to special prayers offered by the ministers of God before seeking medical care. If the child's illness or fever does not improve after these prayers, they would then seek medical treatment at healthcare facilities. These cultural and religious practices may influence the timing of seeking medical help. The educational status of the caregivers played a statistically significant role in the prompt treatment seeking for febrile children. Those who were illiterate or had completed only primary education were more likely to delay seeking care compared to those with a high school education and above. This finding is consistent with studies from Rwanda (49), Tanzania (51), and Shashogo District, Hadiya zone (52). This may be because caregivers with secondary-level education are more likely to seek treatment early within 24 h, possibly due to increased awareness and knowledge, which leads to timely recognition of symptoms and complications of malaria. Education can indeed empower caregivers to act promptly in seeking care for febrile children (53, 54). The likelihood of the delay in seeking prompt treatment for febrile children was significantly lower among the caregivers who were government employees compared to the caregivers with other occupations. It aligns with a study conducted in Gambella town (55). This better prompt treatment-seeking behavior of the government employees may be attributed to the fact that government employees generally have higher educational levels and better access to mass media, and some may even have backgrounds in healthcare. These factors likely contribute to their ability to recognize and respond promptly to signs of illness in children.
The study findings suggested that the caregivers who were exposed to multiple (three and above) media sources were more likely to seek prompt treatment within 24 h compared to the caregivers who were exposed to only one or two media sources. This result is congruent with a study finding in Tanzania (51). Caregivers exposed to more than one type of mass media source have higher odds of seeking appropriate care when they have febrile children. This could be attributed to the messages on malaria prevention and management delivered through mass media, emphasizing the importance of using insecticide-treated nets, getting tested for malaria before taking antimalarial, and understanding that not all fevers are malaria-related. Mass media have been shown to have a similar positive impact on healthcare facility deliveries and contraceptive use (56).
It is interesting to note that the caregivers with a history of child death at home were significantly less likely to delay seeking prompt treatment compared to the caregivers with no history of child death at home. This finding is consistent with similar studies conducted in Shashogo District, Hadiya zone (52), Gambella Town (55), and Jimma zone (31). It suggests that past experiences of child death may influence caregivers' decision to seek treatment more promptly in the future. This insight could potentially help improve healthcare practices for children in need of timely medical attention.
It is important for caregivers to have the autonomy to seek prompt treatment for their child's health needs, especially in urgent situations, such as when a child has fever. When caregivers need permission from their partners to access healthcare services, it can lead to delay in seeking treatment within the 24-h window. This delay can have serious consequences on the child's health. Caregivers should be empowered to make timely decisions regarding their child's health without unnecessary barriers.
The study's usage of multi-level modeling analysis to identify determinants of delay in seeking timely treatment for febrile children is commendable. However, it is important to acknowledge the potential biases that may have influenced the results, such as recall bias and social desirability bias. As a policy and public health implication, this study recommends implementing cost-effective technology-based health education and behavior change communication interventions at the community level. Policymakers, officials, and professionals can work together to reduce the prevalence of delay in seeking healthcare and improve health outcomes for children by leveraging cost-effective technologies and targeted communication strategies.
Almost half of the caregivers delayed seeking medical care for febrile children in the study area. The caregivers who were aged 30 years or younger, caregivers who followed the Protestant religion, caregivers who had lower educational status, caregivers who were merchants or housewives, caregivers who had lower media exposure, caregivers who had no history of child death, and caregivers who needed permission from their partner to access healthcare were more likely to delay seeking healthcare. Targeted intervention should be implemented for caregivers with these identified risk factors to address the delayed care-seeking behavior. Health education and awareness campaigns through mass media, healthcare facilities, and community initiatives can help emphasize the importance of seeking early treatment and the consequences of delaying care for sick children and family members.
The original contributions presented in the study are included in the article/Supplementary material. Further inquiries can be directed to the corresponding author.
The studies involving humans were approved by the institutional ethical review board of Arba Minch University. In addition, a letter of permission was obtained from Gamo zone health department, selected districts, and kebeles. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was obtained from each study participant.
YC: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. TF: Data curation, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. EZ: Data curation, Investigation, Methodology, Supervision, Validation, Writing – review & editing. ZA: Data curation, Investigation, Methodology, Supervision, Validation, Writing – review & editing. ZGA: Formal analysis, Investigation, Software, Supervision, Validation, Writing – review & editing. YH: Investigation, Project administration, Supervision, Validation, Writing – review & editing. MD: Investigation, Project administration, Supervision, Validation, Writing – review & editing. ME: Formal analysis, Investigation, Supervision, Validation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was funded by Arba Minch University, College of Medicine and Health Sciences, Research Co-ordination Office. Funder had no role in this research work.
First, we would like to express our honest gratitude to the Arba Minch University College of Medicine and Health Sciences for providing the fund to conduct this study. Next, we would like to thank the Gamo zone health department, Arba Minch town and Zuria District health offices, data collectors and supervisors, and all other individuals who directly or indirectly contributed to the success and realization of this study. Finally, we would like to thank the study participants for their voluntary participation.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1417638/full#supplementary-material
ACTs, Artimesin combination therapies; FMOH, Federal Ministry of Health; ITNs, Insecticide-treated nets; NGOs, Non-governmental organizations; MOR, Median odds ratio; PCV, Proportional change in variance; ROC, Receiver observed characteristics; SNNPR, Southern Nations Nationalities and Peoples Region; SSA, Sub-Saharan Africa; WHO, World Health Organization.
1. Nnedu NO, Rimel B, Terry C, Jalloh-Vos H, Baryon B, Bausch GD. Syndromic diagnosis of malaria in rural Sierra Leone and proposed additions to the national integrated management of childhood illness guidelines for fever. Am J Trop Med Hyg. (2010) 82:525–8. doi: 10.4269/ajtmh.2010.09-0188
2. Richardson M, Lakhanpaul M. Assessment and initial management of feverish illness in children younger than 5 years: summary of NICE guidance. Br Med J. (2007) 334:1163–4. doi: 10.1136/bmj.39218.495255.AE
3. Manock SR, Jacobsen KH, de Bravo NB, Russell KL, Negrete M, Olson JG, et al. Etiology of acute undifferentiated febrile illness in the Amazon basin of Ecuador. Am J Trop Med Hyg. (2009) 81:146e51. doi: 10.4269/ajtmh.2009.81.146
4. World Health Organization. WHO Informal Consultation on Fever Management in Peripheral Health Care Settings: a Global Review of Evidence and Practice. Geneva: World Health Organization (2013). Available at: https://www.who.int/publications/i/item/9789241506489
5. Prasad N, Sharples KJ, Murdoch DR, Crump JA. Community prevalence of fever and relationship with malaria among infants and children in low-resource areas. Am J Trop Med Hyg. (2015) 93:178–80. doi: 10.4269/ajtmh.14-0646
6. Feikin DR, Scott JA, Gessner BD. Use of vaccines as probes to define disease burden. Lancet. (2014) 383:1762–70. doi: 10.1016/S0140-6736(13)61682-7
7. Biritwum RB, Welbeck J, Barnish G. Incidence and management of malaria in two communities of different socio-economic level, in Accra, Ghana. Ann Trop Med Parasitol. (2000) 94:771–8. doi: 10.1080/00034983.2000.11813601
8. Nonvignon J, Chinbuah MA, Gyapong M, Abbey M, Awini E, Gyapong JO, et al. Is home management of fevers a cost-effective way of reducing under-five mortality in Africa? The case of a rural Ghanaian District. Trop Med Int Health. (2012) 17:951–7. doi: 10.1111/j.1365-3156.2012.03018.x
9. D'Acremont V, Kilowoko M, Kyungu E, Philipina S, Sangu W, Kahama-Maro J, et al. Beyond malaria–causes of fever in outpatient Tanzanian children. N Engl J Med. (2014) 370:809–17. doi: 10.1056/NEJMoa1214482
10. Poyer S, Musuva A, Njoki N, Okara R, Cutherell A, Sievers D, et al. Fever case management at private health facilities and private pharmacies on the Kenyan coast: analysis of data from two rounds of client exit interviews and mystery client visits. Malar J. (2018) 17:112. doi: 10.1186/s12936-018-2267-8
11. Okiro EA, Snow RW. The relationship between reported fever and Plasmodium falciparum infection in African children. Malar J. (2010) 9:99. doi: 10.1186/1475-2875-9-99
12. Tarimo DS. Accuracy of fever and fraction of fevers attributable to malaria among under-fives under reduced malaria infection prevalence in district. Malar Chemother Control Elimin. (2014) 3:1–6. doi: 10.4172/2090-2778.1000121
13. Federal Democratic Republic of Ethiopia. National Malaria Guideline of 2012. Addis Ababa: FMOH (2012). Available at: https://www.medbox.org/pdf/5e148832db60a2044c2d2c93 (accessed July 1, 2019).
14. Federal Ministry of Health. National Strategic Plan For Malaria Prevention Control And Elimination In Ethiopia 2011–2015. Addis Ababa: Federal Ministry of Health [Ethiopia] (2010).
15. Woyessa A, Deressa W, Ali A, Lindtjørn B. Ownership and use of long-lasting insecticidal nets for malaria prevention in Butajira area, south-central Ethiopia: complex samples data analysis. BMC Public Health. (2014) 14:99. doi: 10.1186/1471-2458-14-99
16. Ethiopian Health Nutrition Research Institute. Ethiopia National Malaria Indicator Survey 2011. Addis Ababa: Ethiopian Health Nutrition Research Institute (2012).
17. President's Malaria Initiative. President's Malaria Initiative-Ethiopia Malaria Operational Plan FY 2014. Addis Ababa: President's Malaria Initiative (2014).
19. Smithson P, Florey L, Salgado SR, Hershey CL, Masanja H, Bhattarai A, et al. Impact of malaria control on mortality and anemia among Tanzanian children less than five years of age, 1999–2010. PLoS ONE. (2015) 10:e0141112. doi: 10.1371/journal.pone.0141112
20. Metta E, Haisma H, Kessy F, Hutter I, Bailey A. We have become doctors for ourselves: motives for malaria self-care among adults in southeastern Tanzania. Malaria J. (2014) 13:249. doi: 10.1186/1475-2875-13-249
22. World Health Organization. World Malaria Report 2016. Geneva: World Health Organization (2016). Available at: https://www.who.int/publications/i/item/9789241511711
23. Maslove DM, Mnyusiwalla A, Mills EJ, McGowan J, Attaran A, Wilson K. Barriers to the effective treatment and prevention of malaria in Africa: a systematic review of qualitative studies. BMC Int Health Hum Rights. (2009) 9:26. doi: 10.1186/1472-698X-9-26
24. President's Malaria Initiative. Ethiopia Malaria Operational Plan. Addis Ababa: President's Malaria Initiative (2013).
25. Ministry of Health, Ethiopia. Entomological Profile of Malaria in Ethiopia; African Network on Vector Resistance. WHO/Regional office for Africa. Addis Ababa: Ministry of Health, Ethiopia (2007).
26. Ministry of Health, Ethiopia. Health and Health Related Indicators 2003/04. Planning and Programming Department. Addis Ababa: Ministry of Health, Ethiopia (2004).
27. Derebew A, Alemseged F, Birhanu Z, Sena L, Tegegn A, Zeynudin A, et al. Effect of training on the use of Long Lasting Insecticide Nets on the burden of malaria among vulnerable groups, South West Ethiopia. Malaria J. (2010) 9:121. doi: 10.1186/1475-2875-9-121
28. Federal Democratic Republic of Ethiopia, Ministry of Health. National Malaria Guidelines. Addis Ababa: Federal Democratic Republic of Ethiopia, Ministry of Health (2012).
30. Stefanie G, Lenore M, Brigit O, Marcel T. Appropriating “Malaria”: local responses to malaria treatment and prevention in Abidjan, Côte d'Ivoire. Med Anthropol. (2011) 30:488664. doi: 10.1080/01459740.2010.488664
31. Alemayehu G, Kebede D, Amare D. Determinants of delay in malaria treatment-seeking behaviour for under-five children in south-west Ethiopia: a case control study. Malar J. (2010) 9:320. doi: 10.1186/1475-2875-9-320
32. Sonkong K, Chaiklieng S, Neave P, Suggaravetsiri P. Factors affecting delay in seeking treatment among malaria patients along Thailand-Myanmar border in Tak province, Thailand. Malar J. (2015) 14:3. doi: 10.1186/1475-2875-14-3
33. Chukwuocha UM, Okpanma AC, Nwakwuo GC, Dozie IN. Determinants of delay in seeking malaria treatment for children under-five years in parts of South Eastern Nigeria. J Commun Health. (2014) 39:1171–8. doi: 10.1007/s10900-014-9872-4
35. Roll Back Malaria. Framework for Monitoring Progress and Evaluating Outcomes and Impact. Geneva: World Health Organization (2000).
36. Baird J. Effectiveness of anti-malarial drugs. N Engl J Med. (2005) 352:1565–77. doi: 10.1056/NEJMra043207
37. Baume CA. Guide to Research on Care-Seeking for Childhood Malaria. Arlington, VA: SARA, BASICS II (2002).
38. Ministry of Health. National Malaria Strategic Plan (2014–2020). Addis Ababa: Federal Democratic Republic of Ethiopia Ministry of Health (2014).
39. Noor AM, Kirui1 VC, Brooker SJ, Snow RW. Delay to seek care for under five children with fever. BMC Public Health. (2009) 9:369. doi: 10.1186/1471-2458-9-369
40. Bursac Z, Heath Gauss Z, Keith Williams D, Hosmer D. A purposeful selection of variables macro for logistic regression. Stat Data Anal. (2007) 3:17. doi: 10.1186/1751-0473-3-17
41. Dormann CF, Elith J, Bacher S, Buchmann C, Carl G, Carre G, et al. Collinearity: a review of methods to deal with it and a simulation study evaluating their performance. Nordic Soc. Oikos Ecogr. (2012) 36:27–46. doi: 10.1111/j.1600-0587.2012.07348.x
42. Shah JA, Emina JBO, Ye Y. Timeliness of Malaria Treatment in Children Under Five Years of Age in Sub Saharan Africa: A Multicountry Analysis of National Household Survey Data. Maryland: MEASURE Evaluation (2014).
43. Kassile T, Lokina R, Mujinja P, Mmbando BP. Determinants of delay in care seeking among children under five with fever in Dodoma region, central Tanzania: a cross-sectional study. BMC Malar J. (2014) 13:348. doi: 10.1186/1475-2875-13-348
44. Abrham A. Preventing malaria among under five children in Damot Gale District, Wolayta Zone, Ethiopia: the role of parents knowledge and treatment seeking. Prim Health Care. (2017) 7:284. doi: 10.4172/2167-1079.1000284
45. Birhanu Z, Abebe L, Sudhakar M, Dissanayake G, Yihdego YY, et al. Malaria related perceptions, care seeking after onset of fever and anti-malarial drug use in malaria endemic settings of southwest Ethiopia. PLoS ONE. (2016) 11:160234. doi: 10.1371/journal.pone.0160234
46. Mitiku I, Assefa A. Caregivers' perception of malaria and treatment-seeking behaviour for under five children in Mandura District, West Ethiopia: a cross-sectional study. BMC Malar J. (2017) 16:144. doi: 10.1186/s12936-017-1798-8
47. Muriithi M. The determinants of health-seeking behavior in a Nairobi slum, Kenya. Eur Sci J. (2013) 9:151–64.
48. Kirzinger WK, Cohen RA, Gindi RM. Health care access and utilization among young adults aged 19–25: Early release of estimates from the National Health Interview Survey, January–September 2011. National Center for Health Statistics (2012). Available at: http://www.cdc.gov/nchs/nhis/releases.htm
49. Gerald M. Assessing factors influencing health seeking behavior for malaria treatment in children under five years in Rwimi Town Council Kabarole District. Int J Sch Cog Psychol. (2015) 2:151. doi: 10.4172/2469-9837.1000151
50. Umuhoza C, Karambizi AC, Tuyisenge L, Cartledge P. Caregiver delay in seeking healthcare during the acute phase of pediatric illness, Kigali, Rwanda. Pan Afri Med J. (2018) 30:2–10. doi: 10.11604/pamj.2018.30.160.15286
51. Adinan J, Damian DJ, Mosha NR, Mboya IB, Mamseri R, Msuya SE. Individual and contextual factors associated with appropriate healthcare seeking behavior among febrile children in Tanzania. PLoS ONE 12:e0175446. doi: 10.1371/journal.pone.0175446
52. Turuse EA, Gelaye KA, Beyen TK. Determinants of delay in malaria prompt diagnosis and timely treatment among under-five children in Shashogo District, Hadiya Zone, Southern Ethiopia, 2013. Health. (2014) 6:950–9. doi: 10.4236/health.2014.610120
53. Adeneye A, Jegede A, Mafe M, Nwokocha E. Community perceptions and home management of malaria in selected rural communities of Ogun state, Nigeria. Int J Malar Res Rev. (2013) 1:22–34.
54. Burton DC, Flannery B, Onyango B, Larson C, Alaii J, et al. Healthcare-seeking behaviour for common infectious disease-related illnesses in rural Kenya: a community-based house-to-house survey. J Health Popul Nutr. (2011) 29:61–70. doi: 10.3329/jhpn.v29i1.7567
55. Shumerga AT, Hebo HJ, Gebrehiwot TT, Gebre MN. Determinants of delay in seeking malaria treatment for under-five children at Gambella Town, Southwest Ethiopia: a case-control study. Hindawi J Trop Med. (2020) 200:2–8. doi: 10.1155/2020/2310971
Keywords: delay treatment seeking, Gamo zone, Ethiopia, under five children, multi-level, prompt treatment seeking, fever
Citation: Chisha Y, Feleke T, Zeleke EA, Aschalew Z, Abate ZG, Haile Y, Dalbo M and Endriyas M (2024) Predictors of delayed health seeking for febrile children: multi-level analysis of cross-sectional study data from southern Ethiopia. Front. Public Health 12:1417638. doi: 10.3389/fpubh.2024.1417638
Received: 15 April 2024; Accepted: 12 August 2024;
Published: 09 September 2024.
Edited by:
Peter Bai James, Southern Cross University, AustraliaReviewed by:
Zvifadzo Matsena Zingoni, University of California, Los Angeles, United StatesCopyright © 2024 Chisha, Feleke, Zeleke, Aschalew, Abate, Haile, Dalbo and Endriyas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yilma Chisha, Y3lpbG1hMTk5N0BnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.