 Xiaojuan Deng
Xiaojuan Deng Min Xie
Min Xie Yu Wang
Yu Wang Jia Cai
Jia Cai Min Zou
Min Zou Qiang Wang
Qiang Wang- 1Mental Health Center, West China Hospital, Sichuan University, Chengdu, Sichuan, China
- 2Sichuan Clinical Medical Research Center for Mental Disorders, Chengdu, China
- 3Department of Pharmacy, West China Hospital, Sichuan University, Chengdu, China
Background: This study assesses the impact of adverse childhood experiences (ACEs) on the cognitive function of older adults. Furthermore, it examines the potential underlying mechanism involving education level and the subjective “feeling of loneliness” (FOL).
Methods: Analyzing a population-based cohort sample from the China Health and Retirement Longitudinal Study database, 8,365 subjects aged 45 or older were interviewed in 2018. Ten ACEs indicators were measured using life history questionnaires assessed at 2014. FOL was assessed using a single item from 10-item Center for Epidemiological Studies Depression Scale (CESD-10). Cognitive function was assessed using a structured questionnaire comprising four dimensions: memory, orientation, computation, and visuospatial abilities.
Results: In the fully adjusted model, which accounted for age, gender, marital status, smoke, drink, rural residence, and education levels of both mothers and fathers, the linear regression analysis indicated that ACEs were inversely associated the lower education level (B = −0.058, 95% CI = −0.090, −0.026, p < 0.001), and ACEs were found to be linked to an elevated risk of FOL (B = 0.072, 95% CI = 0.056, 0.089, p < 0.001). In addition, ACEs was not significantly associated with cognitive function (B = −0.047, 95% CI = −0.108, 0.015, p = 0.136), but FOL was significantly associated with cognitive function (B = −0.483, 95% CI = −0.561, −0.404, p < 0.001). Mediation analysis revealed that education level and FOL sequentially and partially mediated the association between ACEs and the total cognitive score, with a proportion mediated of 52.58%.
Limitations: The evaluation of ACEs exposure was based on binary response options. This method limited our ability to explore various dimensions of adversity, such as ages of occurrence, severity, frequency, duration, and the extent of psychological effects at the time. Furthermore, the assessment of loneliness relied on a single item from the CESD-10, introducing a potential source of measurement error.
Conclusion: Our study unveils a substantial association between ACEs and education level, as well as with FOL and cognitive function in the older adults. Moreover, education level and FOL serve as sequential mediating factors in the relationship between ACEs and cognitive function.
1 Introduction
Adverse childhood experiences (ACEs) refer to stressful or traumatic events encountered during childhood, specifically defined as incidents occurring before the age of 18 (1). Over 60% of adults report experiencing at least one adverse childhood experience, and 17% report four or more ACEs. ACEs persistently impact adverse health outcomes throughout an individual’s life, contributing to lower educational attainment, significant causes of adult mortality and influencing various psychosocial outcomes linked to mental illness and poor health, as well as substantial financial costs (2–6).
In China, the escalating aging population has brought about heightened concerns regarding cognitive decline (7). This decline among the older adults can lead to various adverse outcomes, including health complications, reduced social interaction, heightened safety hazards, greater medical complexities, and financial strains (8). Studies have indicated a connection between ACEs and cognitive impairment in adulthood, particularly impacting memory, processing speed, and executive functions, even in later life stages (9–13). Further investigations into the enduring cognitive consequences of specific ACEs could shed light on the specificity and pathways linking individual ACEs to cognitive functions in later life. Some studies have adopted a mediation framework to explore these associations. By examining these potential pathways, invaluable insights could be gained to develop more effective intervention and prevention strategies aimed at mitigating the risks associated with cognitive impairment.
Numerous studies have already found that individuals who have experienced ACEs are more likely to have lower educational attainment (6, 14). This early exposure to ACEs has been linked to a decline in educational achievement, contributing to variations in cognitive skills that manifest in early adulthood and persist into older age, thereby increasing the risk of age-associated cognitive decline and late-life dementia (15). Moreover, recent research has identified specific adverse experiences that may further exacerbate cognitive declines by influencing educational attainment. For instance, one study demonstrated a robust and enduring indirect association between parental substance abuse and poorer cognitive function in later life, mediated through educational level (16). Similarly, Halpin et al. observed that heightened childhood adversity could amplify susceptibility to cognitive impairment by shaping the early educational experiences of older adults (17). Additionally, Burr et al. found that adult loneliness partially mediated the relationship between childhood friendship experiences and cognitive function in later life (18). These findings collectively underscore the intricate relationship between ACEs, educational level, and cognitive function across the lifespan. They highlight the importance of considering the long-term consequences of ACEs on educational outcomes and cognitive health in later life.
Loneliness, characterized as the perception of social isolation or the subjective feeling of being alone (19), represents a significant public health concern that often goes unrecognized or trivialized (20). Considering the escalating number of older adults, it becomes crucial to acknowledge the detrimental effects of loneliness, as revealed in both animal models and longitudinal human investigations (21–23). Substantial studies have found that loneliness was associated with objective social isolation, depression, or poor social skills, cognitive impairment and premature mortality (23–25). Emerging evidence have suggested that those who have been exposed to ACEs are more likely to have the feeling of loneliness (26, 27). For example, individuals who are exposed to ACEs report low self-esteem and problems with emotional regulation, which may lead to encounter challenges in experiencing pleasure, contentment, and happiness. Lin et al. found that ACEs were associated with feeling of loneliness (FOL) trajectory, which play a mediating role between ACEs and problematic internet use in young adults (28). Besides, the mediating role of loneliness have been identified between ACEs and pain, problematic internet abuse and depressive symptoms (28–30). Therefore, one potential explanation for the link between ACEs and cognitive impairment is exposure to adverse events in early life, which can lead to increased feelings of loneliness (FOL) later in life, thus resulting in greater impairment of cognition. However, there remains a scarcity of research delving into the precise mechanisms through which ACEs elevate the risk of cognitive deficits, including factors like educational level and subjective FOL. Exploring these potential pathways could provide valuable insights for the development of more effective intervention and prevention strategies aimed at mitigating the risks associated with cognitive impairment.
There is a lack of studies examining the association between ACEs and the decline of cognitive functioning in later life through a sequential mediating pathway. There could exist a direct relationship between ACEs and cognition. Alternatively, depending on the strength of the mediators, there may be an indirect pathway involving educational level and FOL. Through these indirect pathways, it is possible to elucidate the mechanisms through which ACEs contribute to an elevated risk of cognitive impairment. Drawing from the literature discussed earlier, it can be inferred that the cumulative effect of ACEs may increase the likelihood of lower cognitive function among older individuals. Consequently, we have formulated four hypotheses to guide our investigation:
H1: ACEs are inversely associated with cognitive function among the older adults.
H2: Educational level serves as a mediator in the relationship between ACEs and cognitive function among the older adults.
H3: FOLs acts as a mediator in the relationship between ACEs and cognitive function among the older adults.
H4: Educational level and FOLs sequentially mediate the relationship between ACEs and cognitive function among the older adults.
Figure 1 illustrates the proposed research model for the current study.
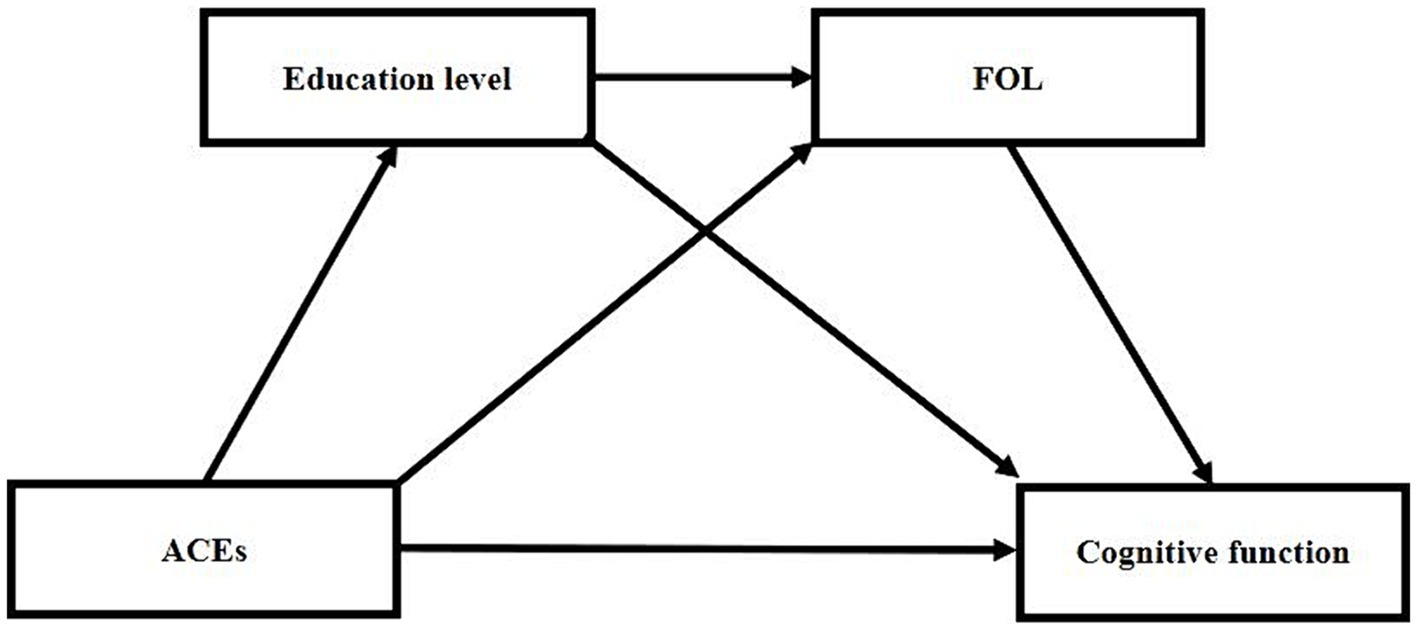
Figure 1. Hypothesized model of ACEs, education level, FOLs and cognitive function. ACEs, adverse childhood experiences; FOL, feeling of lonely.
Therefore, leveraging the unique longitudinal cohort of the China Health and Retirement Longitudinal Study (CHRLS), the current aimed to (1) examine the association between ACEs and education level, FOL and cognitive function in older adults; (2) investigate the connection between FOL and cognitive function; and (3) determine if education level and FOL sequentially mediated the association between ACEs and cognitive function.
2 Materials and methods
2.1 Study design and participants
This study utilized data from fourth wave (2018) and Life History Survey Questionnaire data (2014) obtained from a nationally representative longitudinal survey (CHARLS), which conducted by the China Center for Economic Research at Peking University. Eligible participants, aged 45 and above, were enrolled using a multistage probability sampling method, with follow-up interviews conducted every 2 years. The datasets are accessible for download on the CHARLS homepage at http://charls.pku.edu.cn/en. Approval for the CHARLS survey project was granted by the Biomedical Ethics Committee of Peking University, and all participants were required to provide informed consent through signing.
2.2 Data collection instruments
2.2.1 Demographic information
The general information included age, gender, education level, married status, smoke, drink, rural residence and education levels of both mothers and fathers (Table 1; Supplementary Table S1). The married status is a binary variable representing either “married” or “not in marriage.” Smoking and drinking are binary variables that signify the presence or absence of a history of smoking and alcohol consumption. Rural residence is also a binary variable indicating whether individuals live in urban or rural areas. The education level includes: no formal education illiterate (1), did not finish primary school but cap (2), sishu (a type of educational institution in China that focuses on the early education and development of young children) (3), elementary school (4), middle school (5), high school (6), vocational school (7), two/three-year college/associate degree (8), four-year college/bachelor’s degree (9), and post-graduated (master/PhD) (10). And the marry status includes: married, partnered, separated, divorced, widowed, and never married. In our study, we utilized rural residence, and the educational levels of both mothers and fathers as covariates. These factors have been previously linked to cognitive function and were included to account for their potential influence on our findings.
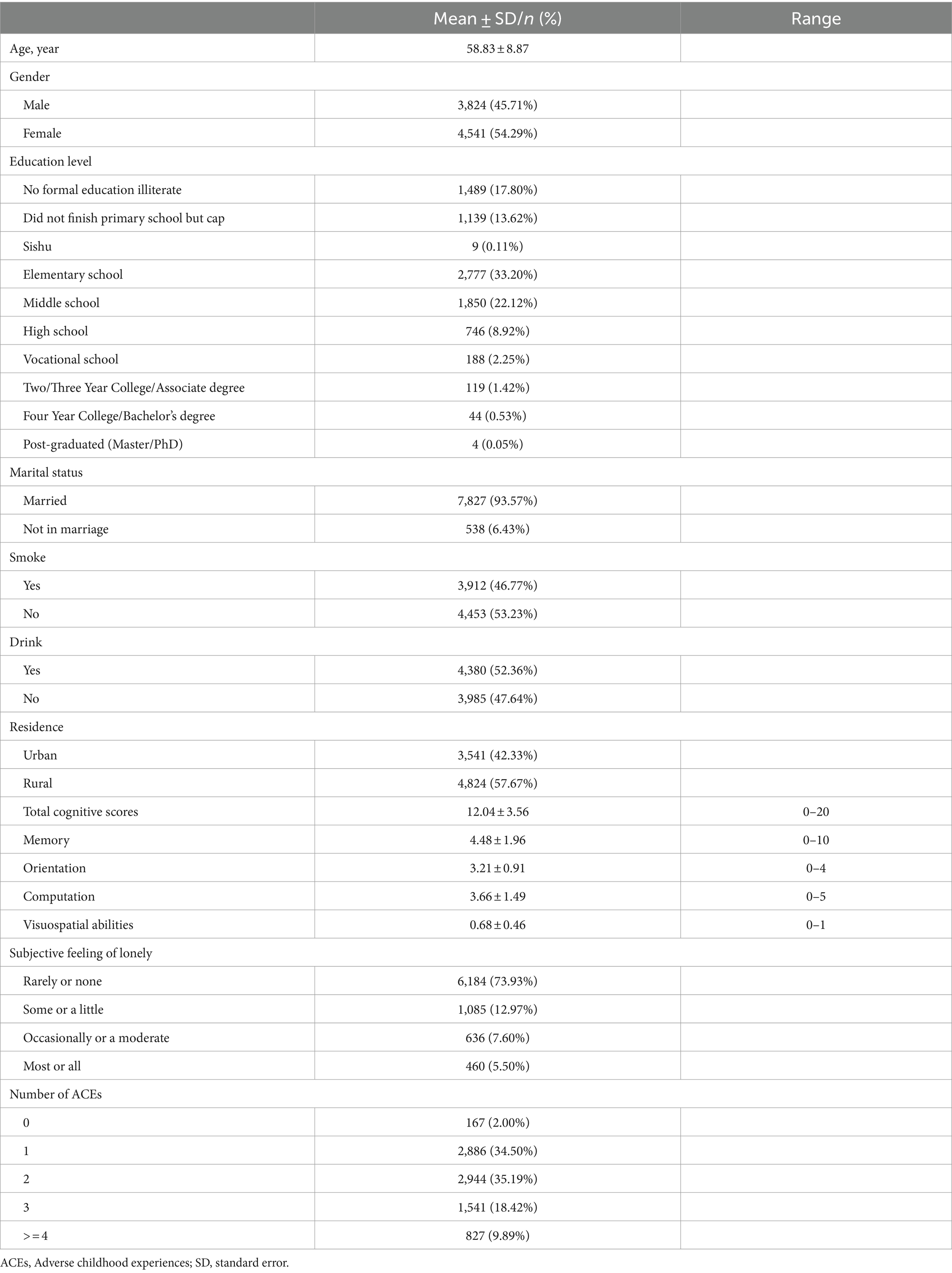
Table 1. The demographic characteristics of participants assessed at 2018 (n = 8,365).
2.2.2 Adverse childhood experiences
The ACEs included ten types of adverse experiences occurred during childhood, including emotional neglect, physical abuse, domestic violence, unsafe neighborhood, and bullying, parental separation or divorce, parental death, household substance abuse, household mental illness, and incarcerated household member (31). The ACEs were quantified as cumulative scores, ranging from 0 to 10, and subsequently classified into four groups: 0 and 1, 2, 3, and 4 or more.
2.2.3 Loneliness symptom
A solitary item from the 10-item Center for Epidemiological Studies Depression Scale (CESD-10) was employed to evaluate loneliness symptoms throughout investigation conducted in 2018. Respondents were instructed to assess the frequency of feeling lonely during the past week, assigning scores within the range of 0 to 3. The survey utilizes a 4-point Likert scale: 0 indicating very rarely or not at all (< 1 day), 1 representing not too much (1–2 days), 2 signifying occasionally or about half the time (3–4 days), and 3 denoting most of the time (5–7 days).
2.2.4 Cognition
This research, conducted using data from the fourth wave assessment of cognitive function, focused on four dimensions: episodic memory, orientation, computation, and visuospatial abilities. Episodic memory was assessed through immediate and delayed word recall, with participants recalling as many words as possible after hearing 10 Chinese nouns, both immediately and 4–10 min later. The episodic memory score was determined as the average of immediate and delayed word recalls, ranging from 0 to 10. Orientation and computation were measured using the 10 items in the Telephone Interview for Cognitive Status (TICS-10), rated on a scale of 0 to 10. Orientation involved inquiries about the date (month, day, year), day of the week, and season. Computation was evaluated by subtracting 7 from 100 five times consecutively, resulting in scores ranging from 0 to 5. Visuospatial abilities were evaluated through graphic rendering, where respondents were presented with a painting and asked to draw a similar figure. The scoring range for drawing is from 0 to 1, with successful drawings earning 1 point and unsuccessful attempts receiving 0 points. The cognitive score, comprising TICS-10, word recall, and graph drawing, ranged from 0 to 21, with higher scores indicating better cognitive function.
2.3 Statistical analysis
Linear regression analyses were conducted to investigate the relationships between ACEs and outcomes of education level and FOL. In Model 1, ACEs were included; in Model 2, covariates such as age, gender, smoke, drink, marital status, rural living or education level were added to Model 1; in Model 3, education level of mother and father were added to Model 2. Furthermore, linear regression analyses were carried out to explore the association between ACEs and cognitive function. In Model 1, ACEs were included; in Model 2, FOL was added into Model 1; in Model 3, covariates such as age, gender, smoke, drink, marital status, rural living or education level were added to Model 3; in Model 4, education level of mother and father were added to Model 3. Spearman correlation analysis was conducted to examine the relationship between ACEs, education level, FOL, and total cognitive score, with Bonferroni correction applied for multiple comparisons. Finally, a serial mediation analysis was used to examine the sequential mediated effects of education level and FOL on the relationship between ACEs and cognitive function (i.e., ACEs (X), education level (M1), FOL trajectories (M2) and total cognitive score (Y)). The significant level of estimates was set as two-tailed p < 0.05. Serial mediation analysis was conducted by MPLUS (version 8.3) and other statistical analyses were conducted using Stata (version 17.1).
3 Results
3.1 Participant characteristics
The demographic, ACEs, loneliness scores and cognition of the 8,365 selected subjects are described in Table 1. The 8,365 participants included 3,824 (45.71%) male and 4,541 (54.29%) female, with mean age of 58.83 ± 8.87. 93.57% of participants are married, while 6.43% are not in a marital relationship. There are 3,912 (46.77%), 4,380 (52.36%) and 4,824 (57.67%) participants reported smoke, drink and living in rural, respectively. The education levels of the subjects are also detailed in Table 1, and the education levels of their mothers and fathers are detailed in Supplementary Table S1. The total cognitive score, memory, orientation, computation and drawing scores assessed at wave 4 were 12.04 ± 3.56 (range: 0–20), 4.48 ± 1.96 (range: 0–10), 3.21 ± 0.91 (range: 0–4), 3.66 ± 1.49 (range: 0–5) and 0.68 ± 0.46 (range: 0–1), respectively. There are 6,184 (73.93%), 1,085 (12.97%), 636 (7.60%) and 460 (5.50%) subjects reported very rarely or not at all (< 1 day), not too much (1–2 days), occasionally or about half the time (3–4 days), and most of the time of FOL, respectively. And there are 167 (2.00%), 2,886 (34.50%), 2,944 (35.19%), 1,541 (18.42%) and 827 (9.89%) reported 0, 1, 2, 3, 4 or above adverse experiences.
3.2 Association between ACEs and education level
The linear regression analysis showed that ACEs were associated with lower education level (B = −0.078, 95% CI = −0.113, −0.042, p < 0.001) in Model 1 (Table 2), without adjusting for covariates. In Model 2, after adjusting for age, gender, marital status, smoke, drink, and rural residency, ACEs remained significantly associated with education level (B = −0.066, 95% CI = −0.098, −0.033, p < 0.001). In Model 3, after further adjustment for the education levels of both the mothers and fathers, ACEs remained significantly associated with education level (B = −0.058, 95% CI = −0.090, −0.026, p < 0.001).
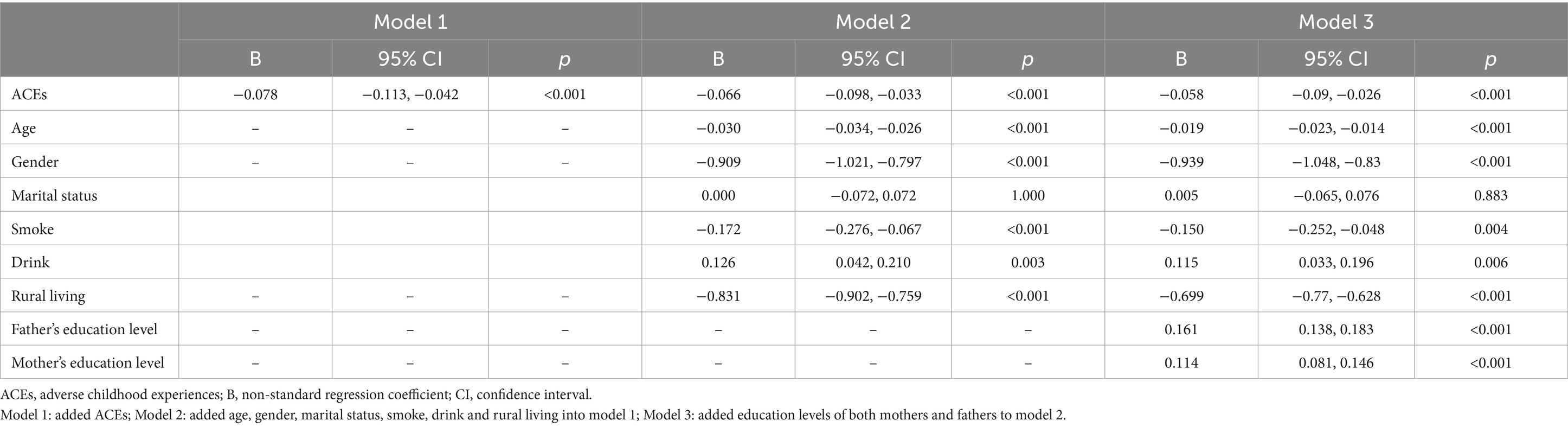
Table 2. Association between ACEs and education level.
3.3 Association between ACEs and FOL
The linear regression analysis revealed that ACEs were linked to an increased risk of FOL (B = 0.074, 95% CI = 0.057, 0.091, p < 0.001) in Model 1 (Table 3), prior to adjusting for any covariates. In Model 2, even after accounting for factors such as age, gender, education level, marital status, smoke, drink and rural residency, the association between ACEs and an elevated risk of FOL remained significant (B = 0.072, 95% CI = 0.056, 0.089, p < 0.001). Further adjustments in Model 3, which included the educational levels of both parents, still showed a significant association between ACEs and an increased risk of FOL (B = 0.072, 95% CI = 0.056, 0.089, p < 0.001).
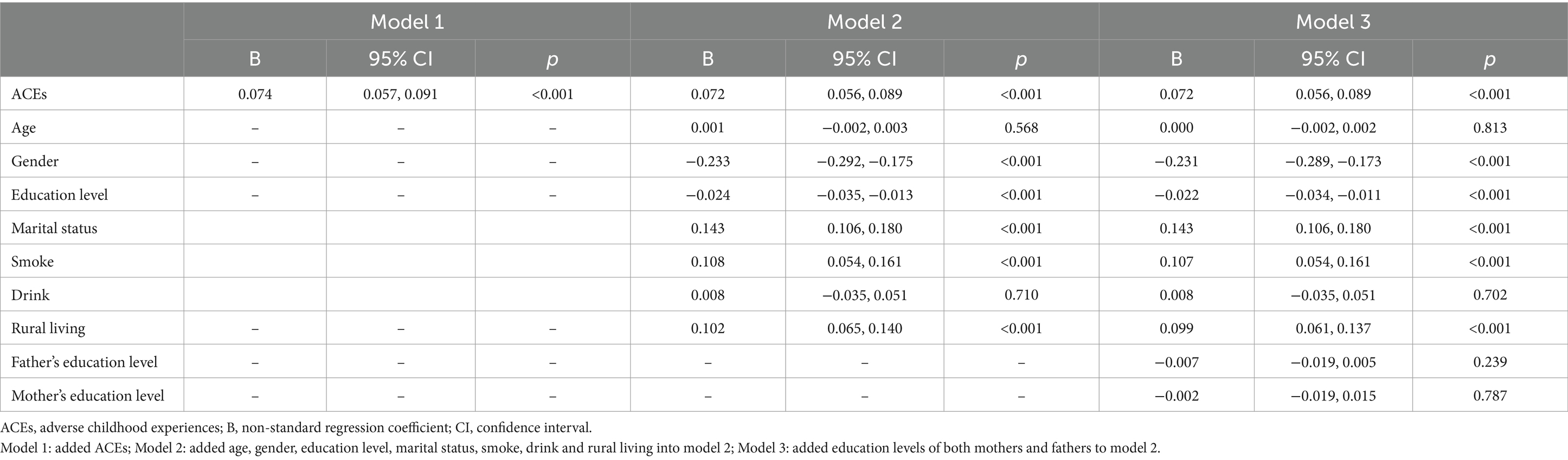
Table 3. Association between ACEs and FOL.
3.4 Association between ACEs, FOL, and cognition
The linear regression analysis revealed a significant association between ACEs and poor cognitive function (B = −0.082, 95% CI = −0.148, −0.015, p = 0.016). However, in Model 2, after incorporating FOL into Model 1, ACEs lost their significant association with cognition (B = −0.038, 95% CI = −0.104, 0.028, p = 0.258), while FOL displayed a significant inverse association with cognition (B = −0.589, 95% CI = −0.673, −0.505, p < 0.001). Advancing to Model 3, which integrated covariates such as age, gender, education level, marital status, smoke, drink, and rural residency into Model 2, ACEs were not associated with cognition (B = −0.050, 95% CI = −0.111, 0.012, p = 0.122), while FOL retained its significant association with cognition (B = −0.485, 95% CI = −0.564, −0.407, p < 0.001). Transitioning to Model 4, with the additional inclusion of the education levels of both mother and father into Model 3, FOL maintained a significant association with poor cognitive function (B = −0.483, 95% CI = −0.561, −0.404, p < 0.001). However, ACEs no longer exhibited an association with cognitive function (B = −0.047, 95% CI = −0.108, 0.015, p = 0.136, refer to Table 4).
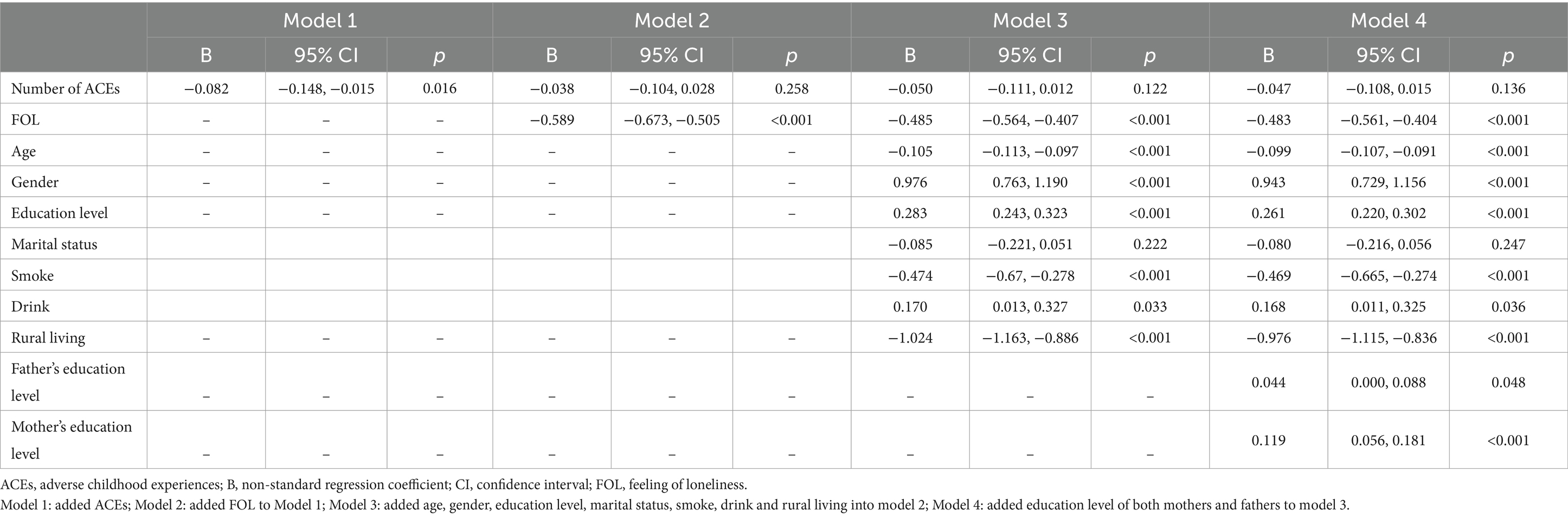
Table 4. Association between ACEs, FOL, and cognition.
3.5 Spearman relationship analysis of variables of interests
The Spearman relationship analysis revealed inversely correlations between ACEs and educational level (r = −0.048, p < 0.001) as well as cognitive function (r = −0.026, p = 0.016). ACEs exhibited a positive relationship with FOL (r = 0.076, p < 0.001). Educational level demonstrated an inversely correlation with FOL (r = −0.038, p < 0.001) and a positive association with cognitive function (r = 0.200, p < 0.001). FOL was inversely associated with cognitive function (r = −0.126, p < 0.001). The association between ACEs and cognitive function was failed to undergo Bonferroni correction (r = −0.026, p = 0.098). The correlation analysis of other variables of interest has undergone multiple corrections, with all p-values remaining below 0.01 after Bonferroni correction (Table 5).

Table 5. Spearman relationship between number of ACEs, education level, FOL, and cognition.
3.6 Chain mediation analysis
Figure 2 illustrates the sequential mediating roles of educational level and FOL between ACEs and cognitive function. In the initial model, we tested the association between ACEs and educational level. The results (R2 = 0.206, F = 26.826, p < 0.001) revealed a positive relationship, indicating that ACEs were inversely correlated with educational level (B = −0.058, 95% CI = −0.086, −0.031, p < 0.001). Subsequently, the model examined whether ACEs and educational level were directly linked to the FOL. The outcomes (R2 = 0.031, F = 7.786, p < 0.001) demonstrated a positive correlation between ACEs and FOL (B = 0.072, 95% CI = 0.057, 0.087, p < 0.001), while educational level exhibited a negative association with FOL (B = −0.022, 95% CI = −0.032, −0.013, p < 0.001). Finally, we explored the relationship among ACEs, education level, FOL, and cognitive function. The results (R2 = 0.166, F = 22.734, p < 0.001) indicated a direct and positive association between educational level and cognitive function (B = 0.261, 95% CI = 0.226, 0.296, p < 0.001). FOL was inversely related to cognitive function (B = −0.483, 95% CI = −0.551, −0.416, p < 0.001). However, the association between ACEs and cognitive function was not significant (B = −0.047, 95% CI = −0.096, 0.005, p = 0.136) (see Supplementary Table S2). We employed the bootstrap method with 5,000 iterations to conduct the mediating effect test. The mediating effect of educational level and the sequential mediating effects of FOL were considered significant if the 95% confidence interval did not include 0. The total indirect effect of ACEs (B = −0.051, 95% CI = −0.062, −0.039, p < 0.001) on cognitive function in the older adults was dissected into three pathways: (1) ACEs → Education level → Cognitive function (B = −0.015, 95% CI = −0.023, −0.008, p = 0.001); (2) ACEs → FOL → Cognitive function (B = −0.035, 95% CI = −0.044, −0.026, p < 0.001); and (3) ACEs → Education level → FOL → Cognitive function (B = −0.001, 95% CI = −0.001, 0.000, p = 0.012) (Supplementary Table S3). The effect of ACEs on cognitive function in the older population was partially serial mediated by educational level and FOL (Proportion mediated: 52.58%, see Supplementary Table S3). All models were adjusted age, gender, marital status, smoke, drink, rural living and education levels of both mothers and fathers.
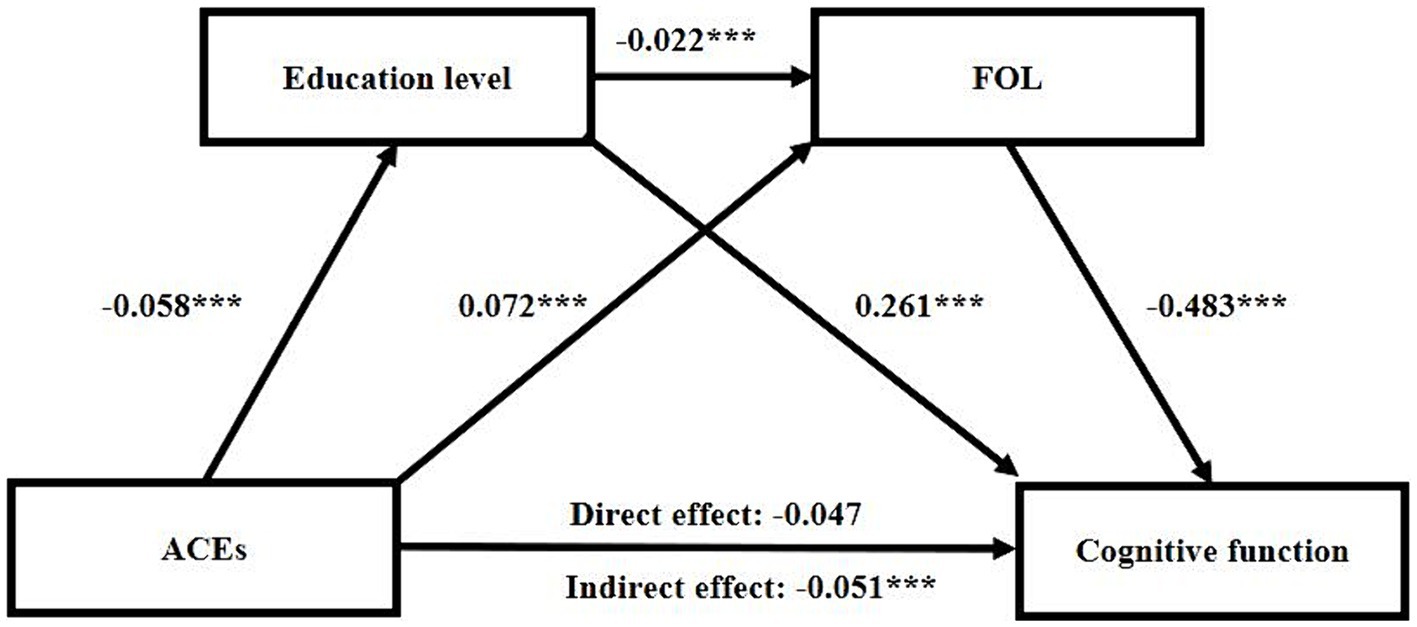
Figure 2. Chain mediation analysis between ACEs and cognition. The models utilize the ACEs path, as indicated in the 2014 Life History Survey Questionnaire assessments, as the independent variable. The sequential mediators are education level and FOL, while the dependent variable is the total cognition score assessed at wave 4. The mediation model is adjusted for age, gender, rural living and education level of mothers and fathers. ACEs, adverse childhood experiences; FOL, feeling of lonely. *p < 0.05; **p < 0.01; ***p < 0.001.
4 Discussion
Building upon a large cohort study, this research delved into exploring the connection between ACEs and cognition. Additionally, it examined the extent to which education level and the FOL sequentially mediate this association. There are several noteworthy findings to highlight. First, ACEs were linked to diminished educational level, heightened FOL, and lower cognitive function. Furthermore, potential indirect pathways were identified involving the education and FOL between ACEs and cognitive function. In summary, our findings contribute to the existing literature by presenting new evidence supporting the role of educational level and FOL as mediators in the relationship between ACEs and cognition.
Consistent with previous research, our finding showed that ACEs were inversely related with education level. Giovanelli et al. discovered that individuals who experienced one or more conventional or expanded ACEs during early childhood were associated with fewer years of education, a diminished likelihood of achieving a bachelor’s degree or higher, and a decreased likelihood of obtaining an associate’s degree or higher. And they proposed that youths at higher risk can benefit most from early intervention for reducing ACE-related disparities (14). Numerous studies suggest that ACEs have significant impacts on individuals’ health and development, including affecting learning ability in school (32, 33), having a negative impact on children’s cognitive development (34), limiting educational resources and opportunities, and influencing individuals’ emotional regulation and coping strategies (35, 36). These effects collectively make it challenging for individuals to effectively deal with academic and life pressures. The cumulative impact of ACEs can create barriers to educational success and overall well-being.
Additionally, our examination also revealed that ACEs were positively associated with subjective FOL. Lin et al. found that individuals exposed to ACEs were at a higher risk of experiencing an increasing trajectory of FOL, with a dose–response relationship existing between the two (28). In the context of subjective experiences of social feelings, one review has highlighted the involvement of neurotransmitters, neurohormonal modulators, and specific brain regions in the mechanisms underlying loneliness (37). Furthermore, Brent and Silverstein et al. further proposed a link between early stress or adversity and the influence on oxytocin release and signaling (38). Oxytocin, known for its impact on interpersonal processes, affiliation, and feelings of love and trust, establishes a logical connection. This early influence may become deeply embedded in the life course, exerting enduring and long-term effects (39).
Emerging evidence showed that the long-lasting effect has been recognized that ACEs have a detrimental impact cognitive function in adults (31, 40). Prior researches investigated the association between ACEs and objective cognition (41, 42), which imply that adverse experiences in early life contribute to inferior cognitive outcomes as individuals age. One study, utilizing data from the English Longitudinal Study of Aging, demonstrated a subtle association between ACEs and memory decline over a ten-year period, spanning from middle to older age (42). Another study, which concentrated on older adults in rural South Africa, discovered a correlation between environmental ACEs, such as cohabiting with someone experiencing psychopathology (substance abuse or mental health challenges), and lower memory scores (43). There may be several potential mechanisms underlying the association between ACEs and cognitive impairment. Exposure to early-life adversity has crucial impact on brain development (44, 45). Specially, in animal models, there is direct evidence illustrating that stress during early life stages triggers structural, functional, and epigenetic alterations in brain regions linked to cognition. Notably, this includes a decrease in hippocampal volume, which has been associated with cognitive impairments, particularly memory deficits (46). These findings suggest that ACEs, education level and FOL should be taken into account as potential factors in measures of cognitive reserve, with the potential to reduce cognitive reserve.
The correlation between ACEs and cognition is mediated by both educational level and FOL. More precisely, individuals who experienced adverse events in their early lives were inclined to have a lower level of education, subsequently experiencing a heightened sense of FOL. This, in turn, elevated their likelihood of experiencing cognitive impairment. In general, both animal models and human studies have profoundly enriched our understanding of the neurodevelopmental mechanisms underlying the association between ACEs and the neural and behavioral phenotypes that result from a complex interplay between environmental, genetic, and epigenetic factors (47). Evidence indicated that early life adversity can impact life course development, including brain development, consequently leading to diminished cognitive, academic and behavioral performance and lower education attainment (6, 48). Moreover, individuals with lower levels of education in Latvia tend to experience higher levels of loneliness (49). This heightened loneliness is subsequently associated with lower scores in composite cognitive score, memory (immediate and delayed recall), verbal fluency, and backward digit span (50). Research findings highlight various measures of social isolation in long-term care settings and illuminate the contextual components that are correlated with a decrease in loneliness among older adults (51, 52). These measures may help to alleviate the cognition decline in older adults.
Our research possesses several limitations that should be acknowledged. Firstly, we did not thoroughly elucidate the relationship between the various components of ACEs and cognition. Secondly, the measures of ACEs exposure in our study utilized binary response options, which limited the exploration of adversity dimensions such as frequency, severity, duration, ages when it occurred, and the degree of psychological effects at the time. Employing more detailed and precise measures of ACEs may be essential to obtain accurate estimates of the relationships between ACEs and memory decline. Thirdly, the assessment of loneliness relied on a single item from ICSD-10. Future studies could enhance accuracy by utilizing structural questionnaires to evaluate the intricacies of FOL. For future research, to enhance the generalizability of findings and mitigate recall bias, incorporating diverse racial and cohort populations could be beneficial.
5 Conclusion
ACEs emerge as reliable predictors for educational level, the FOL, and cognitive function. Notably, chain mediation analyses revealed a novel underlying mechanism in the relationship between ACEs and cognitive function among the older population. ACEs serve as effective predictors for cognition by influencing educational level and the FOL. These findings are instrumental in early identification of individuals at risk for poor cognitive impairment, enabling interventions to exert the maximum impact on preventing or delaying cognitive and functional decline. Interventions aimed at optimizing cognitive health in the older adults and preventing future cognitive deficits should carefully consider the potential roles of ACEs, educational level, and the FOL within the relevant population.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material. All data from CHARLS were accessible to the public through the website (http://charls.pku.edu.cn/).
Ethics statement
This study was based on publicly available datasets. Ethical review and approval was not required for the study, in accordance with the local legislation and institutional requirements. The datasets are accessible for download on the CHARLS homepage at http://charls.pku.edu.cn/en. Approval for the CHARLS survey project was granted by the Biomedical Ethics Committee of Peking University, and all participants were required to provide informed consent through signing.
Author contributions
XD: Writing – review & editing, Writing – original draft, Validation, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. MX: Writing – review & editing, Writing – original draft, Visualization, Validation, Resources, Project administration, Methodology, Investigation, Funding acquisition, Formal analysis, Data curation, Conceptualization. YW: Writing – original draft, Resources, Methodology, Investigation, Funding acquisition, Conceptualization. JC: Writing – original draft, Software, Methodology, Investigation, Funding acquisition, Data curation, Conceptualization. MZ: Writing – review & editing, Visualization, Validation, Supervision, Project administration, Methodology, Conceptualization. QW: Writing – review & editing, Validation, Supervision, Project administration, Methodology, Funding acquisition, Conceptualization.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the National Natural Science Foundation of China (grant number: 82171499), Post Doctor Research Project, West China Hospital, Sichuan University (JC, 2021HXBH027 and 2023HXBH084), and Natural Science Foundation of Sichuan Province (JC, Grant no. 2023NSFSC0126).
Acknowledgments
The authors express gratitude to the CHARLS team for their dedicated efforts and generous sharing of survey data.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpubh.2024.1409966/full#supplementary-material
References
1. Felitti, VJ, Anda, RF, Nordenberg, D, Williamson, DF, Spitz, AM, Edwards, V, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The adverse childhood experiences (ACE) study. Am J Prev Med. (1998) 14:245–58. doi: 10.1016/s0749-3797(98)00017-8
2. Bellis, MA, Hughes, K, Ford, K, Ramos Rodriguez, G, Sethi, D, and Passmore, J. Life course health consequences and associated annual costs of adverse childhood experiences across Europe and North America: a systematic review and meta-analysis. Lancet Public Health. (2019) 4:e517–28. doi: 10.1016/s2468-2667(19)30145-8
3. Bhutta, ZA, Bhavnani, S, Betancourt, TS, Tomlinson, M, and Patel, V. Adverse childhood experiences and lifelong health. Nat Med. (2023) 29:1639–48. doi: 10.1038/s41591-023-02426-0
4. Lin, L, Wang, HH, Lu, C, Chen, W, and Guo, VY. Adverse childhood experiences and subsequent chronic diseases among middle-aged or older adults in China and associations with demographic and socioeconomic characteristics. JAMA Netw Open. (2021) 4:e2130143. doi: 10.1001/jamanetworkopen.2021.30143
5. Petruccelli, K, Davis, J, and Berman, T. Adverse childhood experiences and associated health outcomes: a systematic review and meta-analysis. Child Abuse Negl. (2019) 97:104127. doi: 10.1016/j.chiabu.2019.104127
6. Houtepen, LC, Heron, J, Suderman, MJ, Fraser, A, Chittleborough, CR, and Howe, LD. Associations of adverse childhood experiences with educational attainment and adolescent health and the role of family and socioeconomic factors: a prospective cohort study in the UK. PLoS Med. (2020) 17:e1003031. doi: 10.1371/journal.pmed.1003031
7. Jia, J, Wei, C, Chen, S, Li, F, Tang, Y, Qin, W, et al. The cost of Alzheimer's disease in China and re-estimation of costs worldwide. Alzheimers Dement. (2018) 14:483–91. doi: 10.1016/j.jalz.2017.12.006
8. Panza, F, Lozupone, M, Solfrizzi, V, Sardone, R, Dibello, V, Di Lena, L, et al. Different cognitive frailty models and health- and cognitive-related outcomes in older age: from epidemiology to prevention. J Alzheimers Dis. (2018) 62:993–1012. doi: 10.3233/jad-170963
9. Gould, F, Clarke, J, Heim, C, Harvey, PD, Majer, M, and Nemeroff, CB. The effects of child abuse and neglect on cognitive functioning in adulthood. J Psychiatr Res. (2012) 46:500–6. doi: 10.1016/j.jpsychires.2012.01.005
10. Majer, M, Nater, UM, Lin, JM, Capuron, L, and Reeves, WC. Association of childhood trauma with cognitive function in healthy adults: a pilot study. BMC Neurol. (2010) 10:61. doi: 10.1186/1471-2377-10-61
11. Petkus, AJ, Lenze, EJ, Butters, MA, Twamley, EW, and Wetherell, JL. Childhood trauma is associated with poorer cognitive performance in older adults. J Clin Psychiatry. (2018) 79:16m11021. doi: 10.4088/JCP.16m11021
12. Ritchie, K, Jaussent, I, Stewart, R, Dupuy, AM, Courtet, P, Malafosse, A, et al. Adverse childhood environment and late-life cognitive functioning. Int J Geriatr Psychiatry. (2011) 26:503–10. doi: 10.1002/gps.2553
13. Wang, L, Yang, L, Yu, L, Song, M, Zhao, X, Gao, Y, et al. Childhood physical neglect promotes development of mild cognitive impairment in old age – a case-control study. Psychiatry Res. (2016) 242:13–8. doi: 10.1016/j.psychres.2016.04.090
14. Giovanelli, A, Mondi, CF, Reynolds, AJ, and Ou, SR. Evaluation of midlife educational attainment among attendees of a comprehensive early childhood education program in the context of early adverse childhood experiences. JAMA Netw Open. (2023) 6:e2319372. doi: 10.1001/jamanetworkopen.2023.19372
15. Lövdén, M, Fratiglioni, L, Glymour, MM, Lindenberger, U, and Tucker-Drob, EM. Education and cognitive functioning across the life span. Psychol Sci Public Interest. (2020) 21:6–41. doi: 10.1177/1529100620920576
16. Kraal, AZ, Zaheed, AB, Krasnova, A, Vadari, H, Byrd, DR, and Zahodne, LB. Time-lagged associations between two adverse childhood experiences and later-life cognitive function through educational attainment and stroke. Journal of the international neuropsychological society. JINS. (2023) 30:107–16. doi: 10.1017/s135561772300036x
17. Halpin, AB, MacAulay, RK, Boeve, AR, D'Errico, LM, and Michaud, S. Are adverse childhood experiences associated with worse cognitive function in older adults? J Int Neuropsychol Soc. (2022) 28:1029–38. doi: 10.1017/s1355617721001272
18. Burr, JA, Han, SH, and Peng, C. Childhood friendship experiences and cognitive functioning in later life: the mediating roles of adult social disconnectedness and adult loneliness. The Gerontologist. (2020) 60:1456–65. doi: 10.1093/geront/gnaa055
19. National Academies of Sciences, Division of Behavioral, Social Sciences, Medicine Division, Board on Behavioral, Sensory Sciences, Board on Health Sciences Policy, Committee on the Health, Medical Dimensions of Social Isolation, and Loneliness in Older Adults . Social isolation and loneliness in older adults: opportunities for the health care system. Washington (DC): National Academies Press (US). Copyright 2020 by the National Academy of Sciences. All rights reserved.; (2020). eng.
20. Cacioppo, JT, and Cacioppo, S. The growing problem of loneliness. Lancet. (2018) 391:426. doi: 10.1016/s0140-6736(18)30142-9
21. Cacioppo, S, Capitanio, JP, and Cacioppo, JT. Toward a neurology of loneliness. Psychol Bull. (2014) 140:1464–504. doi: 10.1037/a0037618
22. Phillips, DM, Finkel, D, Petkus, AJ, Muñoz, E, Pahlen, S, Johnson, W, et al. Longitudinal analyses indicate bidirectional associations between loneliness and health. Aging Ment Health. (2023) 27:1217–25. doi: 10.1080/13607863.2022.2087210
23. Stokes, JE, Prasad, A, Barooah, A, and Stam, EJ. Longitudinal dyadic associations between loneliness and cognition among older couples in the United States. J Gerontol B Psychol Sci Soc Sci. (2023) 78:1204–14. doi: 10.1093/geronb/gbad050
24. Kanbay, M, Tanriover, C, Copur, S, Peltek, IB, Mutlu, A, Mallamaci, F, et al. Social isolation and loneliness: undervalued risk factors for disease states and mortality. Eur J Clin Investig. (2023) 53:e14032. doi: 10.1111/eci.14032
25. Elovainio, M, Hakulinen, C, Pulkki-Råback, L, Virtanen, M, Josefsson, K, Jokela, M, et al. Contribution of risk factors to excess mortality in isolated and lonely individuals: an analysis of data from the UK biobank cohort study. Lancet Public Health. (2017) 2:e260–6. doi: 10.1016/s2468-2667(17)30075-0
26. Lin, WH, and Chiao, C. Adverse childhood experience and young adult's problematic internet use: the role of hostility and loneliness. Child Abuse Negl. (2024) 149:106624. doi: 10.1016/j.chiabu.2023.106624
27. Nicolaisen, M, and Thorsen, K. Loneliness among men and women--a five-year follow-up study. Aging Ment Health. (2014) 18:194–206. doi: 10.1080/13607863.2013.821457
28. Lin, WH, and Chiao, C. Relationship between adverse childhood experiences and problematic internet use among young adults: the role of the feeling of loneliness trajectory. J Behav Addict. (2022) 11:1080–91. doi: 10.1556/2006.2022.00074
29. Stout, ME, Tsotsoros, CE, and Hawkins, MAW. Does loneliness mediate the relationship between adverse childhood experiences (ACEs) and pain catastrophizing among women? J Child Adolesc Trauma. (2022) 15:1137–43. doi: 10.1007/s40653-022-00442-9
30. Fan, L, Chen, Y, Zhu, M, Mao, Z, and Li, N. Correlation between childhood trauma experience and depressive symptoms among young adults: the potential mediating role of loneliness. Child Abuse Negl. (2023) 144:106358. doi: 10.1016/j.chiabu.2023.106358
31. Lin, L, Cao, B, Chen, W, Li, J, Zhang, Y, and Guo, VY. Association of Adverse Childhood Experiences and Social Isolation with Later-Life Cognitive Function among Adults in China. JAMA Netw Open. (2022) 5:e2241714. doi: 10.1001/jamanetworkopen.2022.41714
32. Jackson, DB, Testa, A, and Vaughn, MG. Adverse childhood experiences and school readiness among preschool-aged children. J Pediatr. (2021) 230:191–197.e5. doi: 10.1016/j.jpeds.2020.11.023
33. Zarei, K, Xu, G, Zimmerman, B, Giannotti, M, and Strathearn, L. Adverse childhood experiences predict common neurodevelopmental and behavioral health conditions among U.S. Children. Children (Basel, Switzerland). (2021) 8:761. doi: 10.3390/children8090761
34. Hawkins, MAW, Layman, HM, Ganson, KT, Tabler, J, Ciciolla, L, Tsotsoros, CE, et al. Adverse childhood events and cognitive function among young adults: prospective results from the national longitudinal study of adolescent to adult health. Child Abuse Negl. (2021) 115:105008. doi: 10.1016/j.chiabu.2021.105008
35. Thurston, H, Bell, JF, and Induni, M. Community-level adverse experiences and emotional regulation in children and adolescents. J Pediatr Nurs. (2018) 42:25–33. doi: 10.1016/j.pedn.2018.06.008
36. Sheffler, JL, Piazza, JR, Quinn, JM, Sachs-Ericsson, NJ, and Stanley, IH. Adverse childhood experiences and coping strategies: identifying pathways to resiliency in adulthood. Anxiety Stress Coping. (2019) 32:594–609. doi: 10.1080/10615806.2019.1638699
37. Eslinger, PJ, Anders, S, Ballarini, T, Boutros, S, Krach, S, Mayer, AV, et al. The neuroscience of social feelings: mechanisms of adaptive social functioning. Neurosci Biobehav Rev. (2021) 128:592–620. doi: 10.1016/j.neubiorev.2021.05.028
38. Brent, DA, and Silverstein, M. Shedding light on the long shadow of childhood adversity. JAMA. (2013) 309:1777–8. doi: 10.1001/jama.2013.4220
39. Danese, A, and Baldwin, JR. Hidden wounds? Inflammatory links between childhood trauma and psychopathology. Annu Rev Psychol. (2017) 68:517–44. doi: 10.1146/annurev-psych-010416-044208
40. Zhang, T, Kan, L, Jin, C, and Shi, W. Adverse childhood experiences and their impacts on subsequent depression and cognitive impairment in Chinese adults: a nationwide multi-center study. J Affect Disord. (2023) 323:884–92. doi: 10.1016/j.jad.2022.12.058
41. Gold, AL, Meza, E, Ackley, SF, Mungas, DM, Whitmer, RA, Mayeda, ER, et al. Are adverse childhood experiences associated with late-life cognitive performance across racial/ethnic groups: results from the Kaiser healthy aging and diverse life experiences study baseline. BMJ Open. (2021) 11:e042125. doi: 10.1136/bmjopen-2020-042125
42. O'Shea, BQ, Demakakos, P, Cadar, D, and Kobayashi, LC. Adverse childhood experiences and rate of memory decline from mid to later life: evidence from the English longitudinal study of ageing. Am J Epidemiol. (2021) 190:1294–305. doi: 10.1093/aje/kwab019
43. Kobayashi, LC, Farrell, MT, Payne, CF, Mall, S, Montana, L, Wagner, RG, et al. Adverse childhood experiences and domain-specific cognitive function in a population-based study of older adults in rural South Africa. Psychol Aging. (2020) 35:818–30. doi: 10.1037/pag0000552
44. Holz, NE, Berhe, O, Sacu, S, Schwarz, E, Tesarz, J, Heim, CM, et al. Early social adversity, altered brain functional connectivity, and mental health. Biol Psychiatry. (2023) 93:430–41. doi: 10.1016/j.biopsych.2022.10.019
45. McLaughlin, KA, Weissman, D, and Bitrán, D. Childhood adversity and neural development: a systematic review. Annu Rev Dev Psychol. (2019) 1:277–312. doi: 10.1146/annurev-devpsych-121318-084950
46. Lupien, SJ, McEwen, BS, Gunnar, MR, and Heim, C. Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat Rev Neurosci. (2009) 10:434–45. doi: 10.1038/nrn2639
47. Gee, DG . Early adversity and development: parsing heterogeneity and identifying pathways of risk and resilience. Am J Psychiatry. (2021) 178:998–1013. doi: 10.1176/appi.ajp.2021.21090944
48. Black, MM, Walker, SP, Fernald, LCH, Andersen, CT, DiGirolamo, AM, Lu, C, et al. Early childhood development coming of age: science through the life course. Lancet. (2017) 389:77–90. doi: 10.1016/s0140-6736(16)31389-7
49. Reine, I, Miķelsone, M, Guðmundsson, H, Ivanovs, A, Tomsone, S, and Guðmundsson, HS. Loneliness, social isolation and ageing: a methodological approach to compare Latvian and Icelandic older populations in the course of COVID-19 pandemic. Res Sq. (2023) rs.3.rs:2870118. doi: 10.21203/rs.3.rs-2870118/v1
50. Lara, E, Caballero, FF, Rico-Uribe, LA, Olaya, B, Haro, JM, Ayuso-Mateos, JL, et al. Are loneliness and social isolation associated with cognitive decline? Int J Geriatr Psychiatry. (2019) 34:1613–22. doi: 10.1002/gps.5174
51. Masi, CM, Chen, HY, Hawkley, LC, and Cacioppo, JT. A meta-analysis of interventions to reduce loneliness. Pers Soc Psychol Rev. (2011) 15:219–66. doi: 10.1177/1088868310377394
Keywords: adverse childhood experiences, education attainment, loneliness, cognitive function, older adult, Chinese
Citation: Deng X, Xie M, Wang Y, Cai J, Zou M and Wang Q (2024) Adverse childhood experiences and cognitive function in later life: the sequential mediating roles of education level and adult loneliness. Front. Public Health. 12:1409966. doi: 10.3389/fpubh.2024.1409966
Edited by:
Shen Liu, Anhui Agricultural University, ChinaReviewed by:
Carlo Lazzari, International Center for Healthcare and Medical Education, United KingdomPatrícia Maidana Miguel, McGill University, Canada
Copyright © 2024 Deng, Xie, Wang, Cai, Zou and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Min Zou, em91bWluMDgxOEBzY3UuZWR1LmNu
†These authors have contributed equally to this work and share first authorship