
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Public Health, 07 June 2024
Sec. Public Health Education and Promotion
Volume 12 - 2024 | https://doi.org/10.3389/fpubh.2024.1398869
This article is part of the Research TopicCommunity Oral Health: An Integrative Approach to Population-Based Oral Health EnhancementView all 5 articles
 Abimbola M. Oladayo1,2*
Abimbola M. Oladayo1,2* Folake B. Lawal3,4
Folake B. Lawal3,4 Oyinkansola O. Sofola5
Oyinkansola O. Sofola5 Omolara G. Uti5
Omolara G. Uti5 Afolabi Oyapero6
Afolabi Oyapero6 Adetayo Aborisade7,8
Adetayo Aborisade7,8 Bernal Stewart9
Bernal Stewart9 Carlo Amorin Daep9
Carlo Amorin Daep9 Deon Hines9
Deon Hines9 Jacinto Beard10Aderonke Dedeke3,4
Jacinto Beard10Aderonke Dedeke3,4 Omotayo F. Fagbule3,4
Omotayo F. Fagbule3,4 Adeola T. Williams4,11Obioma C. Uchendu12
Adeola T. Williams4,11Obioma C. Uchendu12 Kudirat Ohiare13
Kudirat Ohiare13 Adetomiwa O. Adedire13
Adetomiwa O. Adedire13 Abdul-Kabir Adegoke Yahya-Imam14Oluwagbenga Ilori Adeniji15Aishatu Baba Mele7,8
Abdul-Kabir Adegoke Yahya-Imam14Oluwagbenga Ilori Adeniji15Aishatu Baba Mele7,8 Amina Sani Baffa8
Amina Sani Baffa8 Ifeoluwa Adetula16
Ifeoluwa Adetula16 Taiwo A. Lawal17Gbemisola Aderemi Oke3,4
Taiwo A. Lawal17Gbemisola Aderemi Oke3,4 Azeez Butali1,2
Azeez Butali1,2Introduction: The primary health care system provides an ideal setting for the integration of oral health into general health care as well as equitable access to oral health care. However, the limited oral health knowledge of primary health care workers necessitates appropriate training before they can participate in health promotion efforts. This pilot training was designed to examine the impact of the Oral Health Education module for Nurses and Community Health Care Workers on their oral health awareness and referral practices.
Methods: This study will utilize a quasi-experimental design (pre-and post with a non-equivalent control group) to assess the impact of a five-day pilot oral health education program on the knowledge and referral practices of Nurses and Community Health Workers in primary health care centers in three states in Nigeria-(Lagos, Oyo, and Kano). The training modules were developed based on the six iterative steps described in the intervention mapping framework – needs assessment, highlighting program objectives and outcomes, selection of theory and mode of intervention, designing program based on theory, designing implementation plans, and developing an evaluation plan. Only the intervention group will participate in the full educational training sessions but both groups will complete the pre-and post-intervention questionnaires.
Discussion: This pilot training combined the standardized training modules from the recently launched “Oral Health Training Course for Community Health Workers in Africa” and a newly developed maternal and child oral health module by our group using an evidence-based approach. To the best of our knowledge, this is the first program to examine the impact of the standardized OpenWHO modules. The success of this training will lay the foundation for developing a sustained channel for providing oral health education at the primary health care level in Nigeria, West Africa, and Africa.
Oral diseases and conditions are the most common non-communicable diseases (NCDs) and are increasingly becoming a global public health concern. Despite being largely preventable, about 50% of the global population (~3.5 billion) have some form of oral disease condition (1, 2). In 2019, about 44% of the population in the World Health Organization (WHO) African Region was affected by oral diseases. This data reflects the highest increase in the prevalence of oral conditions across the world over the past three decades (2). Regarding the burden of oral diseases in Nigeria, the 2019 estimates provided by the WHO reported a prevalence of 35.5% for deciduous caries (aged 1–9 years), 23.9% for decay on permanent teeth (aged ≥5 years), 25.1% for severe periodontal disease (aged ≥15 years); 7.9% for edentulism (aged ≥60 years) and a 1.2% age-standardized incidence rate of lip and oral cancer (2).
Adopting a preventive approach to oral health and integrating oral health into general health care is now a global health priority and is essential to achieving a broader impact on the community and population level and cost-effectiveness, especially in settings with limited healthcare resources (2–5). Access to preventive interventions, early disease detection and management, and more equitable access to comprehensive, high-quality care are just a few possible benefits of oral health-primary care integration (6, 7). However, many Nigerians do not have access to preventive dental care; as such, it remains an unmet health need (3).
In Nigeria, there is persistent difficulty in accessing oral care and inequalities in oral health outcomes as the oral health care system is characterized by limited resources, an overstretched workforce, high out-of-pocket expenses, the predominance of a private dental service model and little or no access for rural communities (8–14). Despite the appearance of progress in oral health-related matters, as evidenced by the introduction of the 2012 National Oral Health Policy (NOHP), which highlighted the role of PHC workers in integrating oral health with general health, efforts made to implement this comprehensively have failed due to limited resources (15). Furthermore, the persistent shortage and current decline in the Nigerian oral health workforce (1 dentist to 40,000 people) highlight the ongoing challenge of inadequate personnel in this country (9) and further bolsters the need to utilize and train midlevel and allied health workers to share and shift the current task burden (2, 8, 16).
In the present day, Nigerian PHCs rarely or sparingly provide oral health care (15). The direct connection of the PHCs to communities and individuals makes it the ideal platform for reaching the “last mile” population, primarily found in rural and underserved areas (7, 15, 17). PHC staff, including community health workers and nurses, are trusted members of the community. Exposing them to oral health education would provide them with a channel to amplify accurate health information within their communities while improving awareness about the burden of oral diseases. This could help promote health and oral health-seeking behaviors as well as prioritization of interventions for prevention and management. It is thus essential to adequately educate PHC workers before enrolling them on oral health promotion efforts, since research has revealed a lack of exposure to oral health education via their traditional training (18). Furthermore, successes from community-driven oral health promotion practices in Africa have been reported in countries such as Burkina Faso, Kenya, Cameroun, and Gambia (7). However, the absence of a model upon which oral health promotion can be built is a significant barrier to program implementation (18). This is because the application of sound and evidence-based models and theories provide a foundation for program planners to design, implement and evaluate effective health promotion programs (19). One such approach is Intervention Mapping (IM). IM is a planning framework useful for interventions targeted at behavioral change (20). It provides a template for the systematic planning, development, and evaluation of health promotion interventions (21, 22). IM has been characterized by three perspectives; the use of empirical evidence and theories, an ecological approach and stakeholder participation (20, 21), the outcome of which is more effective interventions (22). Despite its use in developing and implementing health interventions across the globe, there is a paucity of information on its use in health promotion planning in Nigeria, particularly in relation to oral health promotion.
The recently launched OpenWHO oral health promotion course for community health workers in Africa provides an opportunity to train PHC workers with standardized training modules, promoting consistency among trainees while serving as a foundation for improvement in the future (23). Moreover, a focus on vulnerable population groups such as infants, young children and pregnant women, who are usually disproportionately affected by gaps in oral health care (24, 25) via increased awareness and training on maternal and child oral health (MCOH) will allow for the provision of culturally appropriate health information for common oral diseases. These oral diseases include debilitating conditions such as orofacial cleft and Noma and training PHC workers will help foster community support and end the stigmatization associated with these conditions. Based on the six iterative steps described in the IM framework, this paper presents the protocol for Project OHE-NCHeW (oral health education module for Nurses and Community Health Care Workers).
The week-long educational intervention was designed using the iterative steps of the IM framework (Figure 1). Step 1 involved conducting a literature review by searching public databases for existing peer-reviewed literature, policy documents and organizational reports to explore the barriers and inequities in accessing quality and comprehensive oral care in developing countries such as Nigeria. Specific focus was placed on the integration of oral health into general health care services. The opinions of key stakeholders consisting of a multidisciplinary team of experts at different levels of the health care system, including dentists and dental public health practitioners, public health practitioners (with vast experience in oral health education, promotion and programming) (26–30), nursing educators, community health educators, industry partners, policymakers, nurses, and community health workers were also sought to answer these questions. Oral health integration, specifically in the PHC system, has been described as an efficient and cost-effective way of promoting population oral health in developing countries (2, 3, 8, 30, 31). The information obtained from the knowledge gaps identified in the literature and stakeholder engagement guided the development of program objectives and outcomes using a logic model in step 2 (Table 1).

Figure 1. Intervention mapping steps adapted from planning health promotion programs (21).
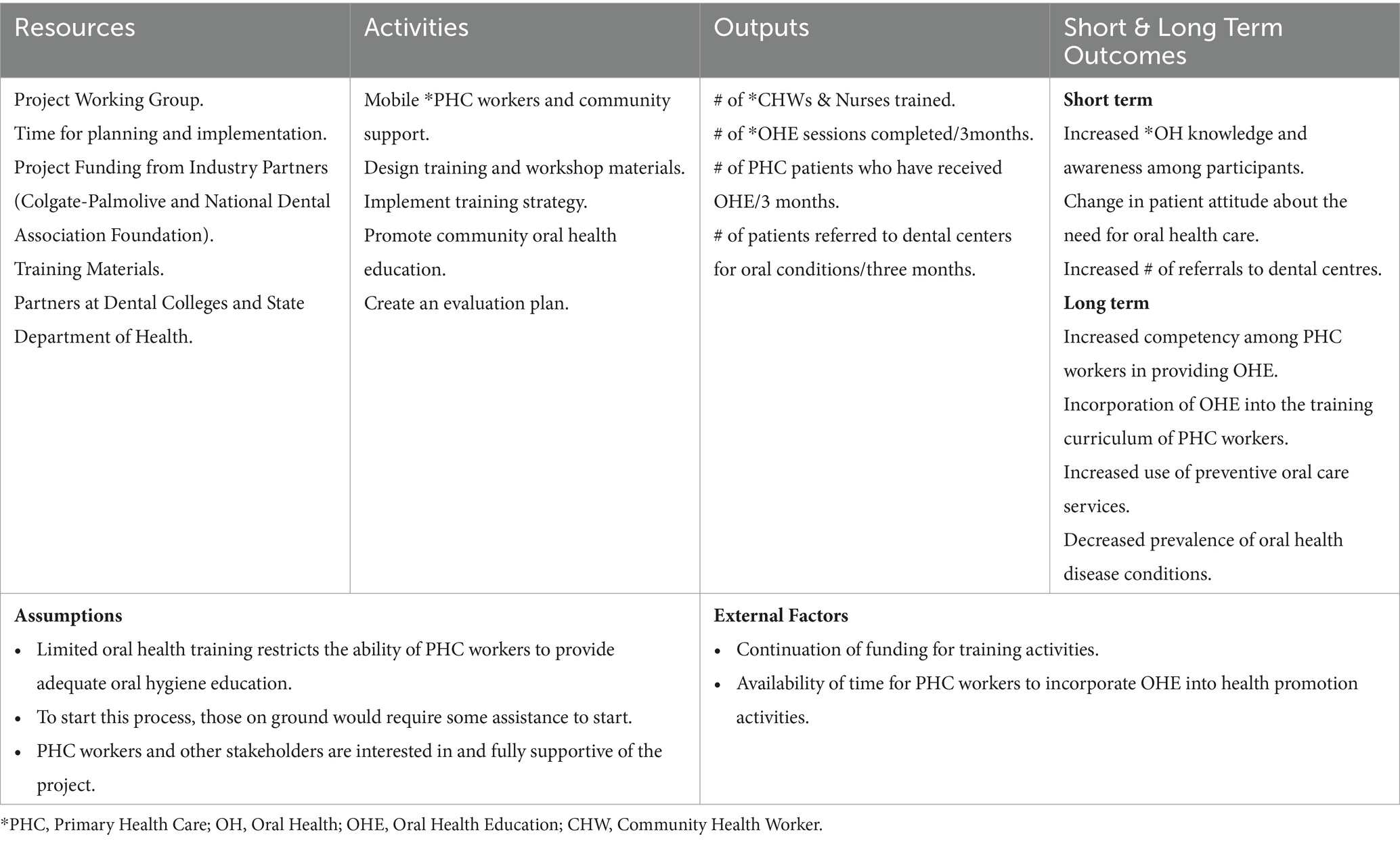
Table 1. Logic Model.
In step 3, we identified an evidence-based approach most likely to influence change using the Lay Health Worker Model/Promotora de Salud (32), a public health model of workforce development targeted at health professionals such as community health workers, in this context, who lack formal oral health training but are members of the communities that they work in (33, 34). This model is often utilized to improve and support access to care in settings with workforce shortages (35). Although this is not commonly used in this population, the promising outcomes reported as it concerns oral health-related knowledge and behaviors in minority populations (36–39) and the need for a more competent allied health workforce capable of providing culturally appropriate oral health care in Nigeria makes it applicable to this study. By exploring parallel processes through collaborative partnerships and considering cultural nuances in the curation of training materials to maximize relevance and acceptability, we anticipate an impactful and lasting program outcome. This led to the fourth step, where program components, like training modules, assessment questions, activity sheet and the logbook for evaluation, were designed following extensive deliberation with all stakeholders. For the fifth and sixth steps, we established how, when, and where the training will be implemented and developed an evaluation plan to assess the effectiveness of the program. In this case, the impact of OHE-NCHeW will be immediately evaluated post-intervention and after 3 months in the training and intervention group.
This study aims to report the experience of adapting, developing, facilitating, and evaluating a five-day pilot of the modules for Project OHE-NCHeW in three states in Nigeria. This training seeks to examine the impact of the standardized OpenWHO oral health promotion modules and an additional Maternal and Child Oral Health (MCOH) module on participants’ oral health knowledge and referral practices as they relate to oral health. This pilot is intended to serve as a foundation for promoting oral health knowledge among primary care workers in the country. Our long-term objective with this systems-level intervention is to increase the capacity of PHC workers (Nurses and Community Health Workers) to provide oral health promotion via oral health education and engage patients attending PHCs to promote primary prevention methods for oral health in a bid to reduce risk for oral diseases.
Does the introduction of oral health education modules by designated trainers improve the oral health knowledge, attitude, and referral practices regarding oral conditions in PHC Nurses and CHWs?
No measurable difference will be observed in the post-intervention knowledge scores and referral practices as it relates to oral health between participants with access to the 5-day training workshop vs. the control group.
An observable difference will be present in post-intervention knowledge scores and referral practices as it relates to oral health between participants with access to the training workshop vs. the control group.
We will utilize a quasi-experimental design (QED) (pre-and post-with a nonequivalent control group) to assess the impact of a five-day pilot oral health education program on the knowledge level and referral practices of Nurses and Community Health Workers in PHCs in three States in Nigeria - (Lagos, Oyo and Kano). A three-month post-training evaluation will follow this. A pre-training evaluation will be conducted prior to the commencement of training, and a post-evaluation will be conducted immediately and 3 months after training. Furthermore, we have included a qualitative assessment via unstructured interviews with the program trainers to explore their experience delivering the training modules and interacting with participants. We will also conduct a focus group discussion (FGD) with the participants in the intervention group to have an in-depth understanding of their opinions, training impact and points of improvement at the 3-month post-training evaluation. Quasi-experiments are often conducted to assess the effectiveness of a treatment, such as educational intervention in field settings where random assignment is not feasible (40–42). This method remains a quick and convenient approach to evaluating a target group to which an intervention has been applied (43).
For the feasibility of pilot studies, research has shown that a sample size consisting of 30 participants in a group is sufficient (44, 45). Based on this evidence, we plan to recruit a minimum of 10 and a maximum of 20 nurses and community health workers in each group per study site. Overall, the estimated sample size for the quantitative component of this pilot study across the three study sites is 120 (60 participants in the intervention group and 60 participants in the control group). The data obtained from this pilot program will be used to estimate a suitable sample size for our major study in the future (46). For the qualitative assessment, unstructured interviews will be conducted with the trainers. A full-group focus group discussion [>7 participants per group as defined by Cortini et al. (47)] will be conducted at each study site. For this study, we intend to engage 8–10 participants per site.
For each study site, 40 participants (20 interventions and 20 controls) will be selected from a minimum of 4 PHCs. Participant selection will be by cluster sampling in each study site. In order to prevent cross-contamination among the participants, those in the intervention and control groups will be selected from different centers. Eligible participants will be 18 years and older, who speak and respond to questions in English, are employed full-time as a Nurse or CHW at the selected PHCs, have had no previous exposure to oral health training, and be willing to participate in the study. Participants with previous exposure to oral health training and those who cannot commit to the entire duration of the training will be excluded from the study.
The permission to conduct the study was sought, and relevant approvals were obtained from the Permanent Secretary (PS) of the State Primary Boards, Permanent Secretaries of State Health Districts, Director of Nursing Services and the Director of Community Services. Nurses who are in the dental and maxillofacial unit and/or nurses who have assisted with Smile Train education and surgeries were excluded. The nominal rolls of nurses and community health workers in the State Health Districts served as the sampling frame, and five nurses and five community health workers who met the selection criteria were selected from each district by simple random sampling (balloting). To avoid contamination, participants from Health districts who were from more distant locations were selected for the control group, while the participants from locations closer to the training center were selected for the intervention group. Following the IRB approval from the Ethics Committee of the participating centers, each recruited participant signed a written consent before active recruitment into the study.
The intervention and control groups will consist of participants selected by a non-random process but with comparable characteristics. Across the three study sites, a total of 60 PHC workers (20 Nurses and CHWs at each site) will be assigned to the intervention group, and a corresponding number of participants will constitute the control group. Participants in the control group will receive a one-off conventional oral health education session consisting of a lecture on oral health, tooth brushing, and diet and oral hygiene demonstration using dental models. The intervention group will be exposed to the week-long pilot training on oral health education delivered by designated trainers (see Table 2). They will also participate in group activities such as oral exams and activity sheets. Each module is expected to last for approximately 4 h. Participants in the intervention group (those who will be trained) will be compared to the control group at each study site. Before the training begins, each participant will be administered a pre-intervention questionnaire to evaluate their oral health knowledge at baseline. The assessment will be repeated immediately after training and after 3 months. These evaluations not only serve as a means of monitoring training impact but also allow participants to observe how they improve throughout the training.
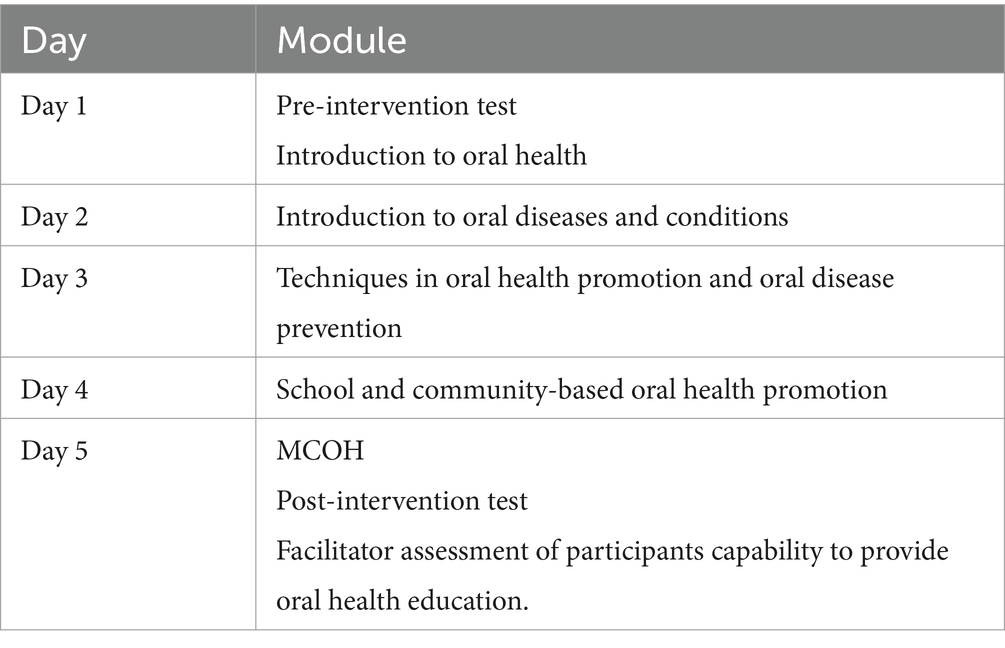
Table 2. Program and module delivery for the five-day training.
The training modules will include the adaptation of existing training resources - Oral Health Training Course for Community Health Workers in Africa developed by the World Health Organization (WHO),1 Oral Health in Comprehensive Cleft Care Educational resources for non-oral health professionals developed by the World Dental Federation (48), and a maternal and child oral health (MCOH) module co-developed by our group consisting of subject matter experts in the field of dental education, dental public health and public health with particular emphasis on stigmatizing conditions such as orofacial clefts and Noma. Participants will be exposed to 4 modules from the OpenWHO course and an additional MCOH module (Table 2). These modules will cover an introduction to oral health, an introduction to oral diseases and conditions, techniques in oral health promotion and oral disease prevention, school and community-based oral health promotion and the MCOH module developed by our group. The OpenWHO course also has a special module that designated trainers will be required to study before the commencement of the training. For this pilot, a member of the research team (an Indigenous local) fluent in the local language at each study site (Hausa and Yoruba) will be designated to provide summaries and interpretation for complex terms. Each group of the participants will also have a designated group lead who will be fluent in both the Indigenous language and in English to also summarize each daily’s training module and direct the associated training activities of the participants. To corroborate dissemination of the training modules, participants will be picked randomly from each group to further explain each module’s concepts to ascertain profound understanding of interpreted complex terms and salient aspects of the training module.
The assessment of the study outcome will be performed using a quantitative and a qualitative approach. Quantitative assessment will be conducted using questionnaires administered by the designated trainers, and the data will be fed into the Qualtrics software for data management. Before the training commences, all participants will take the pre-intervention test that measures their initial knowledge of oral health. The questions will be co-developed by Dental Public Health (DPH) consultants and educators on the research team based on available evidence and will be assessed for face and content validity before deployment. The questionnaire will also be pre-tested among participants who would not be involved in the study. The control group will be immediately provided with the post-intervention evaluation after the one-day lecture. After the training, participants in the training group will be assessed using the post-test. The pre and post-test scores will be compared for participants in the treatment and control groups. Participant’s capability to screen and detect oral diseases will be assessed post-intervention using picture tests.
After 3 months, a follow-up evaluation will be conducted. The number of logged referrals from the PHCs to the dental centers for oral health conditions will also be assessed for 3 months post-training based on the information logged by these providers (see Logic Model-Table 1). In addition, 5% of patients who were referred to dental centers as entered in the logbooks will be contacted via phone calls to verify their final visit to the dental centers.
The qualitative assessment to assess the impact of the training, points of improvement and the practicability of incorporation of oral health promotion activities into maternal and child health visits will be conducted with select participants in the intervention group at the 3-month evaluation using Deliberative Focus group discussions. This approach to evaluation serves to enhance program feedback through participants’ experiences and opinions. Refresher training will be conducted accordingly in month three if necessary. Data collection will be from February to May 2024.
Quantitative data analysis will be conducted using SPSS version 28. Univariate analysis presenting the frequencies and percentages for categorical variables and the means and standard deviation (SD) for the continuous variables will be performed. For the bivariate analysis, t-tests and ANOVA or their nonparametric analogs (based on normality) will be conducted for within and between group associations with a p-value set at <0.05. For the qualitative data analysis, audio recordings obtained during data collection will be transcribed verbatim by the research team and will be analyzed by content analysis. Data will be analyzed using Nvivo12. Responses will be coded into themes and sub-themes, ensuring data saturation when no new information is discovered in data analysis. Comparison, mapping, and verification of conclusions will be conducted and arranged according to the study objectives. Prominent quotes from the participants will be selected and cited within the report.
Pilot studies are essential for improving the quality and efficiency of the major study (49). Thus, the success of this pilot program could help set the foundation for sustained oral health education training for primary health care workers, invariably creating a pool of qualified peer trainers for PHC workers, PHC patients, their families, and the general population. Studies have shown how misinformation, myths and cultural beliefs among individuals and community stakeholders negatively impact oral health attitudes and care-seeking behaviors in developing countries (50–54). Promoting approaches where qualified care professionals provide adequate and accurate oral health information may thus influence positive oral health practices, leading to improved oral health and overall health. The scope of the current project will encompass most of the essential components of primary oral care recommended by the WHO by leveraging the strategic positioning of the PHC system and its link with individuals, communities, and the health care system. These recommendations include “age-friendly primary health care for oral health, maternal and child oral health care, health communication/oral health education, disease prevention methods, early detection, pain control - emergency care for oral health, continuity of oral healthcare, supportive referral systems and priority to those people most in need” (7). The strength of the QED approach lies in its simplicity regarding data collection, ease of implementation and associated low cost (55). However, there are some limitations to this study design. Due to non-randomization of study participants, other factors related to the outcome of interest beyond the control of the researchers could potentially influence study results (56). Secondly, it is impossible to determine causality because quasi-experimental research is not an actual experiment; thus, only associations between interventions and outcomes can be made (43). Furthermore, because the treatment and control groups are nonequivalent (group assignment is by non-random selection), selection bias may exist. The presence of a nonequivalent no-treatment control in this study reduces issues such as threats to internal validity (i.e., observing the same participants over time). This is due to the assumption that the presence of similarity between the treatment and the control groups at baseline reduces the likelihood of having significant confounder differences between both groups (55, 57, 58).
In this study, we will ensure that a consistent approach is taken to select participants within and across study sites, administer evaluation surveys and follow-up (59). Additionally, we will conduct a pre-intervention assessment (allowing for the baseline comparison of the treatment and control group), an immediate post-intervention assessment, and 3 months following the training to allow for consideration of learning or attitude decay (43). Before use, the pre and post-tests will be validated for accuracy in measuring the outcomes of interest in the study. Also, tests will be scored consistently by a non-biased grader blinded to the participants and not part of the team that designed or conducted the oral health training (43). Regarding the establishment of causality, given that the intervention- (oral health education) comes before the assessment of the outcome, associations identified in QEDs meet an essential causality requirement (60).
The OpenWHO online course on oral health for CHWs in WHO African Region is the first of its kind, with several modules aimed at building participant’s capacity “on oral health promotion, oral disease prevention, and control to meet some of the unmet demand for oral health services and strengthen the oral health system through a cross-cutting approach” (61). To the best of our knowledge, no study has been done to document the experiences of trainees and participants engaging in this course. Additionally, this training includes an extra module which will provide culturally appropriate information for maternal and child oral health in this population. Lessons learnt could be useful to strengthen adoption and implementation practices in Nigeria and across the WHO African Region.
The studies involving humans have been approved by the Institutional Review Boards at the University of Iowa (IRB-01/202312517); the University of Ibadan/University College Hospital, Ibadan (UI/EC/23/0724); the University of Lagos/Lagos University Teaching Hospital, Lagos (ADM/DSCST/HREC/APP/6454) and Bayero University Kano/Aminu Kano Teaching Hospital, Kano (NHREC/28/01/2020/AKTH/EC/3739), Nigeria. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in the pilot study. Written informed consent to participate in the main study will be obtained from participants.
AOl: Conceptualization, Funding acquisition, Methodology, Resources, Writing – original draft, Writing – review & editing. FL: Conceptualization, Writing – review & editing, Resources, Methodology. OS: Conceptualization, Writing – review & editing, Resources, Methodology. OUt: Conceptualization, Writing – review & editing, Resources, Methodology, Visualization. AOy: Conceptualization, Writing – review & editing, Methodology, Resources. AAb: Conceptualization, Methodology, Writing – review & editing, Resources. BS: Writing – review & editing, Resources. CD: Writing – review & editing, Resources. DH: Writing – review & editing, Resources. JB: Writing – review & editing. AD: Writing – review & editing. OF: Writing – review & editing. AW: Writing – review & editing. OUc: Writing – review & editing. KO: Writing – review & editing. AAd: Writing – review & editing. Y-IA: Writing – review & editing. IO: Writing – review & editing. AM: Writing – review & editing. ABa: Writing – review & editing. IA: Writing – review & editing. TL: Writing – review & editing. GO: Writing – review & editing. ABu: Methodology, Resources, Supervision, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This pilot training was supported jointly by Colgate-Palmolive and the National Dental Association Foundation (PI, AMO and the National Institute of Dental and Craniofacial Research T90 Training Grant under grant [NIH DE023520]. The funder Colgate-Palmolive was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
We would like to express our sincere gratitude to the World Health Organization (WHO) for providing the training framework and course materials through the Oral Health Training Course for Community Health Workers in Africa on OpenWHO, Bayero University Kano, University of Ibadan, University of Lagos and the State Primary Health Care Boards for endorsing and supporting this vital project, and to the Nurses and Community Health Workers who agreed to participate in this study.
BS, CD and DH were employed by Colgate-Palmolive Company.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author, AB, declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Jain, N, Dutt, U, Radenkov, I, and Jain, S. WHO's global oral health status report 2022: actions, discussion and implementation. Oral Dis. (2023) 30:73–9. doi: 10.1111/odi.14516
2. WHO. Global oral health status report: towards universal health coverage for oral health by 2030. Regional summary of the African Region. Geneva: World Health Organization, (2023).
3. Braimoh, M, Ogunbodede, E, and Adeniyi, A. Integration of Oral health into primary health care system: views of primary health Care Workers in Lagos State, Nigeria. J Public Health Afr. (2014) 5:328. doi: 10.4081/jphia.2014.328
4. Nakre, PD, and Harikiran, AG. Effectiveness of oral health education programs: a systematic review. J Int Soc Prev Community Dent. (2013) 3:103–15. doi: 10.4103/2231-0762.127810
6. Greiner, AC, and Glicken, AD. What primary care innovation teaches us about Oral health integration. AMA J Ethics. (2022) 24:E64–72. doi: 10.1001/amajethics.2022.64
7. Petersen, PE. Strengthening of oral health systems: oral health through primary health care. Med Princ Pract. (2014) 23:3–9. doi: 10.1159/000356937
8. Amedari, MI, Ogunbodede, EO, Uti, OG, Aborisade, AO, and Amedari, IK. Strengthening the Oral health system in Nigeria: a health systems building block approach. Niger Postgrad Med J. (2022) 29:173–82. doi: 10.4103/npmj.npmj_127_22
9. Uguru, N, Onwujekwe, O, Ogu, UU, and Uguru, C. Access to Oral health care: a focus on dental caries treatment provision in Enugu Nigeria. BMC Oral Health. (2020) 20:1–13. doi: 10.1186/s12903-020-01135-1
10. Uguru, N, Onwujekwe, O, Uguru, CC, and Ogu, UU. Achieving universal health coverage in Nigeria: the dilemma of accessing dental care in Enugu state, Nigeria, a mixed methods study. Heliyon. (2021) 7:e05977. doi: 10.1016/j.heliyon.2021.e05977
11. Isiekwe, IG, Umeizudike, KA, Daramola, OO, Akeredolu, MO, and Leo-Olagbaye, AA. The COVID-19 pandemic and dental residency training in Nigeria. Eur J Dent Educ. (2021) 25:753–61. doi: 10.1111/eje.12654
12. Sede, M, Enone, L, and Makanjuola, J. COVID-19 pandemic: the implication for the practice of restorative dentistry in Nigeria. Niger Dent J. (2020) 28:5–17. doi: 10.61172/ndj.v28i1.84
13. Isiekwe, IG, Adeyemi, TE, Aikins, EA, and Umeh, OD. Perceived impact of the COVID-19 pandemic on orthodontic practice by orthodontists and orthodontic residents in Nigeria. J World Fed Orthod. (2020) 9:123–8. doi: 10.1016/j.ejwf.2020.07.001
14. Aladelusi TOAtiba, FA, Gbadebo, SO, Adeyemo, YI, Olusanya, AA, and Akadiri, OA. COVID-19 outbreak and dental health care provision in Nigeria: a national survey. BMC Oral Health. (2021) 21:1–11. doi: 10.1186/s12903-021-01860-1
15. Amedari, MI. Primary oral health care in Nigeria; four decades after the Alma Ata declaration. PAMJ-One Health. (2020) 2:23. doi: 10.11604/pamj-oh.2020.2.13.24357
16. Aderinokun, G. Review of a community oral health programme in Nigeria after ten years. Afr J Biomed Res. (2000) 3:123–8.
17. Shiroya, V, Shawa, N, Matanje, B, Haloka, J, Safary, E, Nkhweliwa, C, et al. Reorienting primary health care services for non-communicable diseases: a comparative preparedness assessment of two healthcare networks in Malawi and Zambia. Int J Environ Res Public Health. (2021) 18:5044. doi: 10.3390/ijerph18095044
18. Ogunbodede, EO, Rudolph, MJ, Tsotsi, NM, Lewis, HA, and Iloya, JI. An Oral health promotion module for the primary health care nursing course in Acornhoek, South Africa. Public Health Nurs. (1999) 16:351–8. doi: 10.1046/j.1525-1446.1999.00351.x
19. Simpson, V. Models and theories to support health behavior intervention and program planning. Health Human Sci. (2015) 2:45–7.
20. Kok, G, Peters, LWH, and Ruiter, RAC. Planning theory-and evidence-based behavior change interventions: a conceptual review of the intervention mapping protocol. Psicologia: Reflexão e Crítica. (2017) 30:19. doi: 10.1186/s41155-017-0072-x
21. Eldredge, LKB, Markham, CM, Ruiter, RA, Fernández, ME, Kok, G, and Parcel, GS. Planning health promotion programs: an intervention mapping approach. San Franciso: John Wiley & Sons (2016).
22. Fernandez, ME, Ruiter, RAC, Markham, CM, and Kok, G. Intervention mapping: theory-and evidence-based health promotion program planning: perspective and examples. Front Public Health. (2019) 7:209. doi: 10.3389/fpubh.2019.00209
23. Mĺkva, M, Prajová, V, Yakimovich, B, Korshunov, A, and Tyurin, I. Standardization – one of the tools of continuous improvement. Procedia Eng. (2016) 149:329–32. doi: 10.1016/j.proeng.2016.06.674
24. Barbieri, W, Peres, SV, Pereira, CB, Peres Neto, J, Sousa, MLR, and Cortellazzi, KL. Sociodemographic factors associated with pregnant women's level of knowledge about oral health. Einstein. (2018) 16:eAO4079. doi: 10.1590/s1679-45082018ao4079
25. NIH. Oral health in America: Advances and challenges. Oral health in America: Advances and challenges. Bethesda (MD): National Institute of Dental and Craniofacial Research(US) (2021).
26. Lawal, FB, and Taiwo, JO. An audit of school oral health education program in a developing country. J Int Soc Prev Community Dent. (2014) 4:S49–55. doi: 10.4103/2231-0762.144600
27. Lawal, FB, and Taiwo, JO. Making a case for formal school-based oral health promotion: oral health knowledge, attitude and practices of pupils in Ibadan, Nigeria. Int Q Community Health Educ. (2018) 38:99–105. doi: 10.1177/0272684X17749574
28. Uti, O, and Sofola, O. Impact of an educational intervention on smoking counseling practice among Nigerian dentists and dental students. Niger J Clin Pract. (2015) 18:75–9. doi: 10.4103/1119-3077.146983
29. Adekunle, AA, Uti, OG, and Sofola, OO. Correlates of illness behaviour related to orofacial infections of odontogenic origin among adults in a semi urban community in Nigeria. Ghana Med J. (2019) 53:294–8. doi: 10.4314/gmj.v53i4.7
30. Adeniyi, AA, Ajieroh, V, Sofola, OO, Asiyanbi, O, and Oyapero, A. A pilot test of an oral health education module for community health workers in Ikeja LGA, Lagos state. African J Oral Health. (2017) 7:8–16. doi: 10.4314/ajoh.v7i1.162231
31. FMOH. National oral health policy. Federal Ministry of Health. Nigeria: Policy Document. (2012).
32. Logan, RI, and Castañeda, H. Addressing health disparities in the rural United States: advocacy as caregiving among community health workers and Promotores de Salud. Int J Environ Res Public Health. (2020) 17:9223. doi: 10.3390/ijerph17249223
33. Chakawa, A. Bridging the gap: a pilot study of a lay health worker model to decrease child mental health stigma and promote parents’ professional help-seeking for black/African American children. Psychol Serv. (2023) 20:64–77. doi: 10.1037/ser0000620
34. Barnett, ML, Klein, CC, Gonzalez, JC, Luis Sanchez, BE, Green Rosas, Y, and Corcoran, F. How do lay health workers engage caregivers? A qualitative study to enhance equity in evidence-based parenting programs. Evid-Based Pract Child Adolesc Mental Health. (2023) 8:221–35. doi: 10.1080/23794925.2021.1993111
35. Barnett, ML, Lau, AS, and Miranda, J. Lay health worker involvement in evidence-based treatment delivery: a conceptual model to address disparities in care. Annu Rev Clin Psychol. (2018) 14:185–208. doi: 10.1146/annurev-clinpsy-050817-084825
36. Hoeft, KS, Rios, SM, Pantoja Guzman, E, and Barker, JC. Using community participation to assess acceptability of “contra caries”, a theory-based, promotora-led oral health education program for rural Latino parents: a mixed methods study. BMC Oral Health. (2015) 15:1–11. doi: 10.1186/s12903-015-0089-4
37. Huang, SJ, Galárraga, O, Smith, KA, Fuimaono, S, and McGarvey, ST. Cost-effectiveness analysis of a cluster-randomized, culturally tailored, community health worker home-visiting diabetes intervention versus standard care in American Samoa. Hum Resour Health. (2019) 17:1–9. doi: 10.1186/s12960-019-0356-6
38. Hyde, S, and Hawkins, K. The cost-effectiveness of close-to-community health Programmes: what do we know and where are the gaps. Economic evaluation of community based practitioners in low-and middle-income countries: A literature review, country case studies and a generalized cost-effectiveness model. Switzerland: World Health Organization (2017).
39. Javanparast, S, Windle, A, Freeman, T, and Baum, F. Community health worker programs to improve healthcare access and equity: are they only relevant to low-and middle-income countries? Int J Health Policy Manag. (2018) 7:943–54. doi: 10.15171/ijhpm.2018.53
40. Price, P, Jhangiani, R, and Chiang, I. Research methods in psychology (2nd canadian edition). The Saylor Foundation, BCCAMPUS, VICTORIA, BC. (2015) 4.
41. Hallberg, K, and Eno, J. Quasi-Experimental Designs In: JD Wright, editor. International encyclopedia of the Social & Behavioral Sciences. 2nd ed. Oxford: Elsevier (2015). 742–6.
42. Linda, H. Quasi-Experiment In: K Kempf-Leonard, editor. Encyclopedia of social measurement. New York: Elsevier (2005). 255–61.
43. Stratton, SJ. Quasi-experimental design (pre-test and post-test studies) in prehospital and disaster research. Prehosp Disaster Med. (2019) 34:573–4. doi: 10.1017/S1049023X19005053
44. Whitehead, AL, Julious, SA, Cooper, CL, and Campbell, MJ. Estimating the sample size for a pilot randomised trial to minimise the overall trial sample size for the external pilot and main trial for a continuous outcome variable. Stat Methods Med Res. (2016) 25:1057–73. doi: 10.1177/0962280215588241
45. Teresi, JA, Yu, X, Stewart, AL, and Hays, RD. Guidelines for designing and evaluating feasibility pilot studies. Med Care. (2022) 60:95–103. doi: 10.1097/MLR.0000000000001664
46. Thabane, L, and Lancaster, G. A guide to the reporting of protocols of pilot and feasibility trials. Pilot Feasibility Stud. (2019) 5:37. doi: 10.1186/s40814-019-0423-8
47. Cortini, M, Galanti, T, and Fantinelli, S. Focus group discussion: how many participants in a group? Encyclopaideia. (2019) 23:29–43.
48. Barnett, ML, Lau, AS, and Miranda, J. Orenuga oral health in comprehensive cleft care educational resources for non-oral health professionals. World Dental Federation.(2021).
49. In, J. Introduction of a pilot study. Korean J Anesthesiol. (2017) 70:601–5. doi: 10.4097/kjae.2017.70.6.601
50. Mwangosi, IEAT, and Nyandindi, U. Oral health related knowledge, behaviours, attitude and self-assessed status of primary school teachers in Tanzania. Int Dent J. (2002) 52:130–6. doi: 10.1111/j.1875-595X.2002.tb00617.x
51. Omo, J, and Enabulele, J. Self-reported prevalence of missing teeth and unmet prosthetic treatment needs among a population of Nigerian undergraduate students. Kanem J Med Sci. (2020) 17:1–9. doi: 10.31173/bomj.bomj_179_17
52. Nicol, P, Al-Hanbali, A, King, N, Slack-Smith, L, and Cherian, S. Informing a culturally appropriate approach to oral health and dental care for pre-school refugee children: a community participatory study. BMC Oral Health. (2014) 14:69. doi: 10.1186/1472-6831-14-69
53. Bankole, OO, Lawal, FB, and Ibiyemi, O. Development of a tool for dispelling myths associated with natal/neonatal teeth: "ADUNNI" a health education video in a native NIGERIAN language. Ann Ib Postgrad Med. (2017) 15:137–41.
54. Heglund, SP. Dental myths: a deterrent to dental care seeking behaviors in developing countries. Med Case Rep Rev. (2018) 1:2–5. doi: 10.15761/MCRR.1000115
55. Handley, MA, Lyles, CR, McCulloch, C, and Cattamanchi, A. Selecting and improving quasi-experimental designs in effectiveness and implementation research. Annu Rev Public Health. (2018) 39:5–25. doi: 10.1146/annurev-publhealth-040617-014128
56. Privitera, GJ, and Delzell, L.“Quasi-experimental and single-case experimental designs” in Research methods for education. eds. G. J. Privitera and L. Ahlgrim-Delzell SAGE Publications, (2018):333–370.
57. Krass, I. Quasi experimental designs in pharmacist intervention research. Int J Clin Pharm. (2016) 38:647–54. doi: 10.1007/s11096-016-0256-y
58. Weinhardt, LS, Galvao, LW, Yan, AF, Stevens, P, Mwenyekonde, TN, Ngui, E, et al. Mixed-method quasi-experimental study of outcomes of a large-scale multilevel economic and food security intervention on HIV vulnerability in rural Malawi. AIDS Behav. (2017) 21:712–23. doi: 10.1007/s10461-016-1455-1
59. Cousins, K, Connor, JL, and Kypri, K. Effects of the campus watch intervention on alcohol consumption and related harm in a university population. Drug Alcohol Depend. (2014) 143:120–6. doi: 10.1016/j.drugalcdep.2014.07.015
60. Harris, AD, McGregor, JC, Perencevich, EN, Furuno, JP, Zhu, J, Peterson, DE, et al. The use and interpretation of quasi-experimental studies in medical informatics. J Am Med Inform Assoc. (2006) 13:16–23. doi: 10.1197/jamia.M1749
61. Open WHO. Oral health training course for community health Workers in Africa [Internet]. (2023). Available at: https://openwho.org/courses/oral-health-community-AFRO
Keywords: primary health care (PHC), oral health education, oral health, nurses, community health workers, pilot study
Citation: Oladayo AM, Lawal FB, Sofola OO, Uti OG, Oyapero A, Aborisade A, Stewart B, Daep CA, Hines D, Beard J, Dedeke A, Fagbule OF, Williams AT, Uchendu OC, Ohiare K, Adedire AO, Yahya-Imam A-KA, Adeniji OI, Mele AB, Baffa AS, Adetula I, Lawal TA, Oke GA and Butali A (2024) Study protocol for a pilot quasi-experimental study on oral health education for nurses and community health workers in Nigeria. Front. Public Health. 12:1398869. doi: 10.3389/fpubh.2024.1398869
Edited by:
Nélio Veiga, Portuguese Catholic University, PortugalReviewed by:
Pedro Campos Lopes, Catholic University of Portugal, PortugalCopyright © 2024 Oladayo, Lawal, Sofola, Uti, Oyapero, Aborisade, Stewart, Daep, Hines, Beard, Dedeke, Fagbule, Williams, Uchendu, Ohiare, Adedire, Yahya-Imam, Adeniji, Mele, Baffa, Adetula, Lawal, Oke and Butali. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abimbola M. Oladayo, Ymltb2xhZGF5b0BnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.