 Tesfaye Derbie Begashaw
Tesfaye Derbie Begashaw Fantahun Andualem
Fantahun Andualem- 1Department of Psychiatry, College of Medicine and Health Science, Aksum University, Axum, Ethiopia
- 2Department of Psychiatry, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
Background: Depression is becoming a significant burden and a potential cause of disability worldwide. According to a World Health Organization (WHO) study conducted in both developed and developing countries, the prevalence of depression is 10.4%. There are differences in the prevalence of depression among the population based on a number of variables, including concomitant medical problems, substance abuse, employment environment, and demographics. The purpose of this study was to evaluate the prevalence of depression and its associated risk factors among textile industrial workers.
Methods: A cross-sectional study was conducted on 409 workers from the Almeda Textile Factory in Adwa from May to June 2020. The outcome variable was depression, assessed using the Patient Health Questionnaire-9 (PHQ-9). Variables with p-values of <0.25 in the bivariate analysis were included in the multivariate analysis. An adjusted odds ratio with a 95% confidence interval was computed. Statistical significance was determined at a p-value of <0.05.
Results: The total prevalence of depression at a PHQ-9 cutoff score of 10, PHQ-9(10+), was 24.4%. At a cutoff score of 5, PHQ-9(5+) was 51.1%. In the multivariate analysis, low social support, working rotating day and night shifts, and having a physical injury at the workplace were significantly associated with depression at both PHQ-9(5+) and PHQ-9(10+). In addition, advanced age of 45 years and above and being diagnosed with chronic medical disease were significantly associated with depression at PHQ-9(10+) (p < 0.05).
Conclusion: The prevalence of depression varied based on the PHQ-9 cutoff score, and it is high at both PHQ-9(5+) and PHQ-9(10+). Low social support, working rotating day and night shifts, physical injury at the workplace, advanced age, and chronic medical disease were significantly associated with depression. Our findings suggest that the workers at the Almeda Textile Factory should be screened and managed accordingly.
Introduction
Depression, one of the most prevalent mental illnesses, is characterized by a depressed (sad, empty) or irritated mood, a loss of interest or pleasure, and physical and cognitive abnormalities that have a significant impact on a person’s day-to-day functioning (1–4). Depression is becoming a serious burden and a potential cause of disability worldwide (5–7). According to the World Health Organization (WHO), depression will be the second leading cause of disability-adjusted life years (DALYs) by 2030, following HIV/AIDS (8).
A study carried out by the WHO in both developed and developing countries revealed that the prevalence of depression is 10.4% (3). However, the prevalence of depression varies among the global population by area and by high-, middle-, and low-income countries; in the majority of these countries, the prevalence ranges from 3 to 16.9% (9). The prevalence of depression among the population varies depending on a number of variables, including concomitant medical problems (particularly chronic disorders), substance abuse, employment environment, and demographic factors such as gender, age, domicile, marital status, and educational level (1, 3, 4).
Nowadays, life in factories is undoubtedly rather stressful. The range of materials, techniques, equipment, and components used in the textile industry makes it one of the most valuable and technologically advanced sectors overall (10). The pressure and workload on workers in this industry have increased due to the development of new technologies and increased global competition (11). Research has shown that stress at work, a precursor to depression (3), is commonly experienced by workers in textile factories (12, 13). As depression is more prevalent than other mental illnesses, it is well established that it significantly negatively impacts motivation, productivity, absenteeism, and job retention in the workplace (14).
As previously mentioned, there is a risk factor for depression related to gender because women are twice as likely as men to experience depression (1, 3, 4). The majority of workers in textile factories are women (15–20), but little is known about depression in that industry. According to a study, the prevalence of depression varies by age in the United States, with those aged 18 to 29 experiencing a 3-fold higher prevalence than those aged 60 and older (1). According to several research in Ethiopia, the majority of textile factory workers are under the age of 30 (15, 16). According to research, the majority of garment industry workers in Bangladesh have only completed primary school (17) and are single (18).
Acute or chronic physical disease can have an impact on the social, psychological, or biological aspects of health, potentially leading to depression (3). The study was conducted in Myanmar; among textile industry workers, the prevalence of chronic disease was 18.6% for hypertension, 2.2% for diabetes mellitus (19), and 22.3% for hypertension in India (21). Although using personal protective equipment (PPE) might reduce the risks of physical hazards and accidents that textile factory workers face on the job (16, 17), 41.8% of Ethiopian textile industry workers did not wear PPE (22). As a result, those who experience physical injuries may also exhibit depressive symptoms. In fact, given the nature of the condition, depression may even contribute to physical injuries by diminishing concentration and energy. Alcohol and cigarettes have also been reported to be used by textile plant workers (19), and as previously mentioned, substance users tend to have higher levels of depression.
In Ethiopia, the prevalence of depression varies depending on the research population. For example, it was found to be 17.5% in a community-based study (23), 22.9% among university staff (24), 2.2% among students (25), and 48.9% among outpatients (26). As a result, depression varies across populations. Nevertheless, little research has been conducted on the prevalence of depression and the factors associated with it among textile industry workers in Ethiopia and other countries. Consequently, the purpose of this study was to evaluate the prevalence of depression and its risk factors among textile workers in the Almeda area. In addition, the study aimed to address existing gaps in the literature and provide health policymakers, program planners, and strategists with baseline data for the prevention and intervention of depression.
Methods and materials
Study area and setting
In May and June 2020, a cross-sectional study with an institutional focus was conducted in the Almeda textile industry in Adwa, Tigray, Ethiopia. The factory is located 1,006 km from Addis Ababa, the capital of Ethiopia, in the center of the Tigray region. The factory was built on 550,000 square meters of land and was founded in February 1996 E.C. Its sub-departments include spinning, weaving, woven processing, knit manufacturing, knit dyeing, and garment production, with fully functional mechanical and electrical workshop equipment. With 4,567 employees, the factory has been sustainably producing goods for more than 25 years, providing employment opportunities in the process.
Study population
The study population included employees from the textile factory in Almeda who were working in the study area during that time. Workers at the Almeda textile mill with more than 6 months of work experience were included in the study, while those on annual leave, seriously ill, or diagnosed with a mental health diagnosis were excluded.
Sample size determination
Since no comparable study on depression among Almeda Textile Factory workers has been conducted in our country, the sample size was determined using a single population proportion formula, taking into account the following factors: a standard normal distribution (z = 1.96), a 95% confidence interval (α = 0.05), a prevalence (p = 50%), and a margin of error (d = 0.05). The sample size was 423 when a 10% non-response rate was applied. Using their workplace identification numbers, a computer-generated randomization technique, known as simple random sampling, was used to select study units from among textile industry workers throughout the study.
Sampling technique and procedures
During the study period, the workplaces of textile industry workers were used to select the study unit through simple random sampling (using computer-generated randomization). A sample was chosen from five units of Almeda textile manufacturing workers using proportionate allocation, as illustrated in Figure 1.
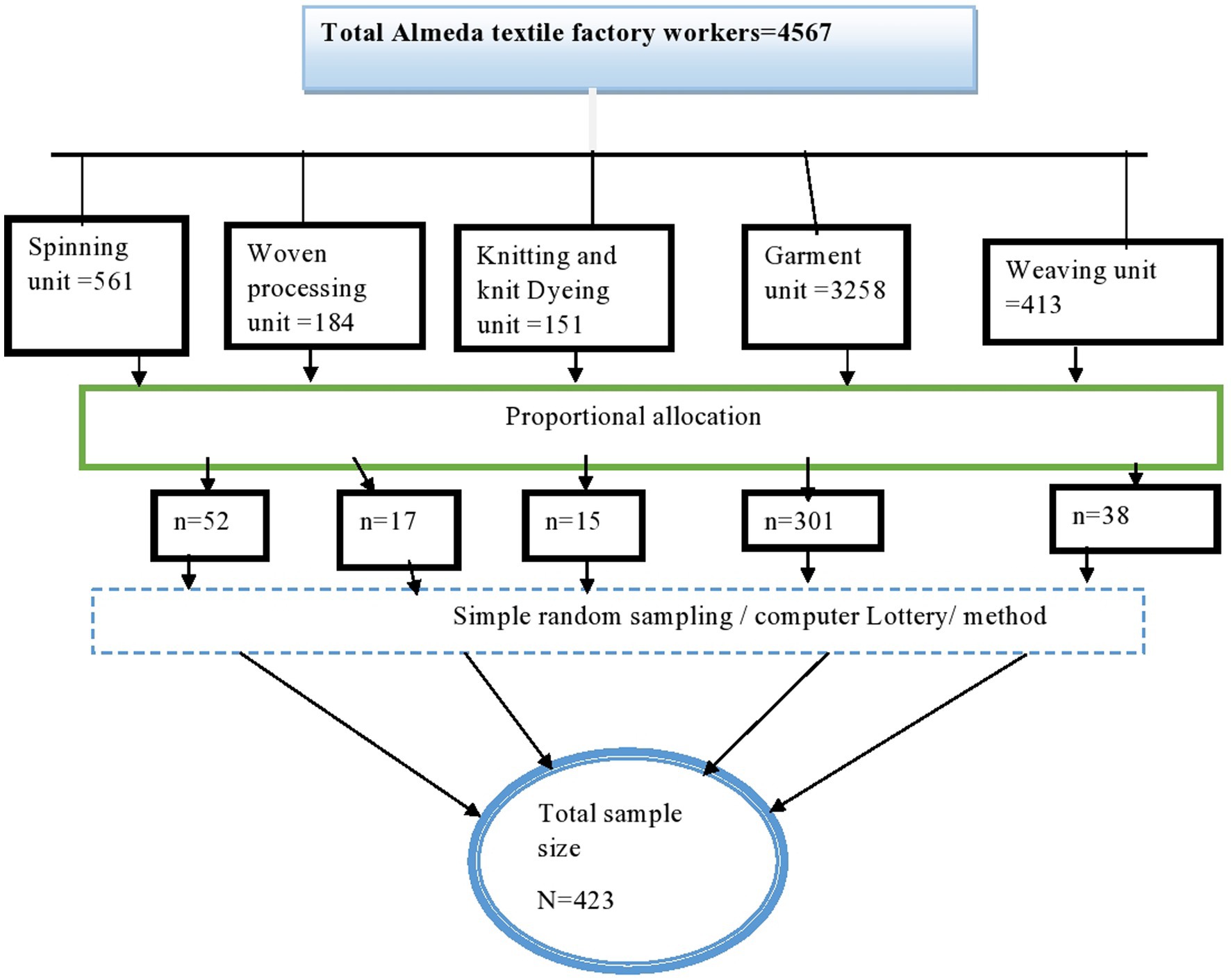
Figure 1. Schematic presentation of proportional allocation to find the required sample among Almeda textile factory workers in Adwa, Tigray, Ethiopia, 2020.
Data collection instruments
The outcome variable, depression, was assessed using the Patient Health Questionnaire-9 (PHQ-9). PHQ-9 cutoff scores of 5 and 10 were used to differentiate the severity grades of depression. The total PHQ-9 score ranges from 0 to 27, with the following cutoff scores: 1–4 indicating “minimal depression,” 5–9 indicating “mild depression,” 10–14 indicating “moderate depression,” 15–19 indicating “moderately severe depression,” and 20–27 indicating “severe depression” (27). In previous studies in Ethiopia, the screening tool was validated at a cutoff point of 10 (27, 28) and at cutoff points of 5 and 10 (29).
Social support was measured using the Oslo Social Support Scale (OSSS-3). The sum score ranges from 3 to 14, with cutoff scores classified as follows: 3–8 indicating poor social support, 9–11 indicating moderate social support, and 12–14 indicating strong social support (30). When categorized into two levels, patients who scored less than 9 were classified as having low social support, and patients who scored 9 or more were classified as having high social support. Work-, clinical-, and substance-related factors were assessed through yes/no answers from the respondents, and socio-demographic background information (age, gender, marital status, occupation, and others) were collected using structured questions.
Data collection procedure
To ensure consistency and tool understandability, data were gathered through self-administered interviews with the Tigrigna version of a pre-tested questionnaire, which was then translated back into English. Four data collectors (psychiatric professionals with a bachelor’s degree) and two supervisors (master’s degree holders in mental health) received training on data collection instruments, ethical consent, sampling techniques, and protocols. At the apparel velocity corporation (AVC), a pre-test was conducted on 5% of the sample size before the actual data collection. The supervisors oversaw the process, and the completed questionnaires were reviewed for consistency and completeness throughout the data collection process.
Data processing and analysis
For statistical analysis, the data were imported into Windows’ EpiData Manager version 4.6 and then exported to Statistics Packages for Social Sciences version 22.0. We generated descriptive statistics using the mean, frequency, and percentage. A collection of independent factors and dependent variables was statistically associated using binary logistic regression. In the multivariate analysis, variables from the bivariate analysis with p-values less than 0.2 were included. To ensure model fit, the Hosmer–Lemeshow test was performed, and an adjusted odds ratio with a 95% confidence interval was calculated. Statistical significance was declared at a p-value of <0.05.
Ethical consideration
The Mekelle University College of Medicine and Health Science (MUCHS) office of the health research ethical review committee accepted the study, which was carried out in accordance with the Declaration of Helsinki. MUCHS provided official letters of support, which Almeda Textile Factory (ATF) received and filed. A study participant was made aware of the protocols and importance of the research. Participants’ signed informed consent was acquired. All information, including the results of the analysis, was kept private and shared exclusively with the relevant authorities. Participants were advised that they had the option to withdraw from the study at any time, and those who were not volunteers were not required to take part in it. No personal identifiers were used on the questionnaire, and confidentiality was guaranteed for all the information submitted.
Results
Prevalence of depression among the socio-demographic characteristics of the study participants
A total of 409 participants responded to the questionnaire, with a response rate of 96.7%. The mean age of participants was 28.49 ± 7.49 years. More than half of the participants were women (63.6%), while 55.5% were single. Regarding ethnicity, all participants identified as Tigrayan. Among the participants aged 45 years and more, more than 16 (69.6%) participants experienced depression at a cutoff score of 5 on the PHQ-9, PHQ-9(5+), compared to those under 45 years, where 10 participants (43.5%) experienced depression at a cutoff score of 10 on the PHQ-9, PHQ-9(10+). The PHQ-9 diagnosis of depression at a cutoff score of 5 was relatively higher among the women (52.7%) than among the men (48.3%). At a cutoff score of 10, the prevalence was higher among women than men. The prevalence of depression, as measured using the PHQ-9 at cutoff scores of 5 and 10 among divorced or widowed participants, was 57.9 and 47.4%, respectively (Table 1).
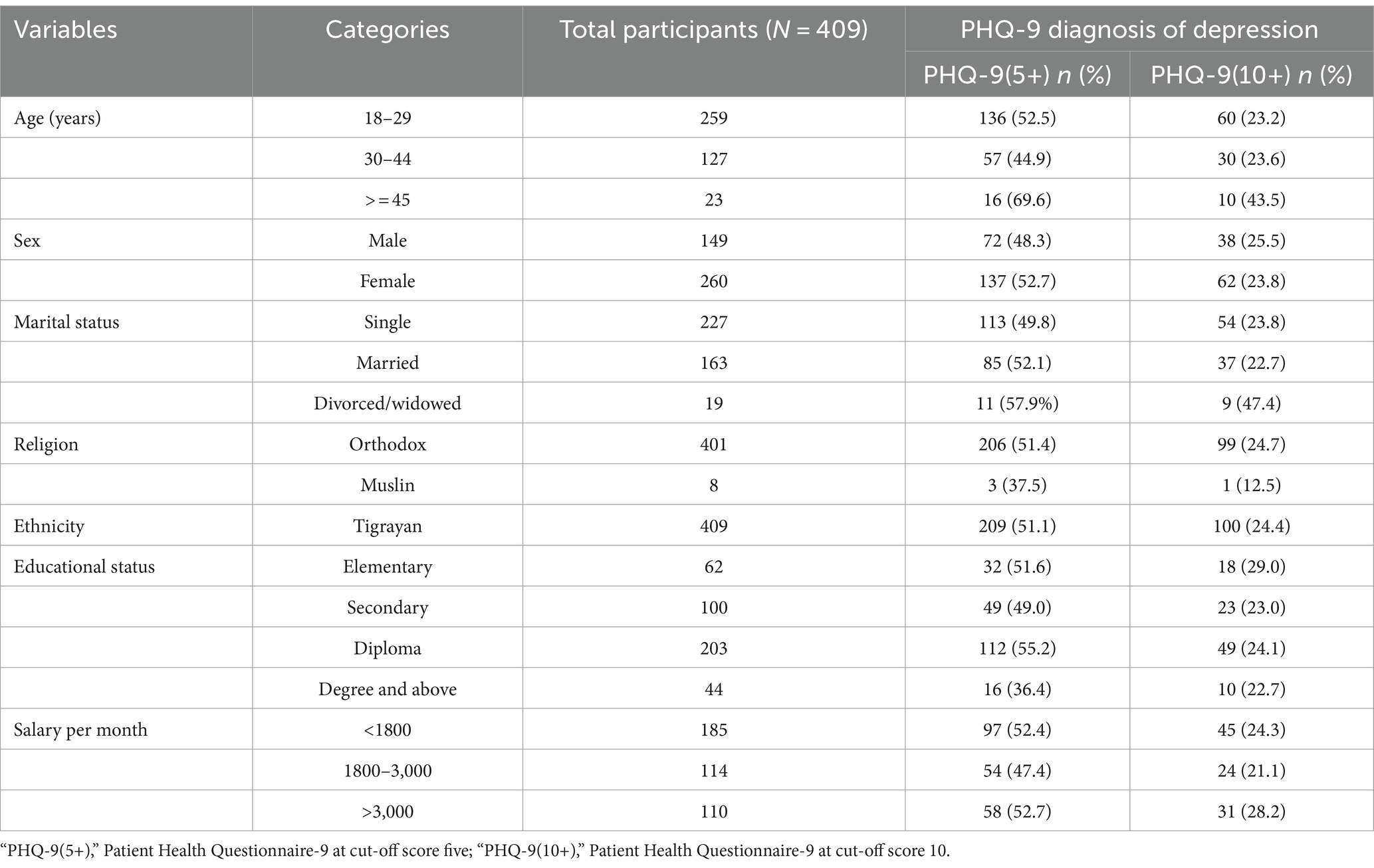
Table 1. The PHQ-9 diagnosis of depression at cut-off score five and ten in socio-demographic characteristics of the study participants (N = 409).
Prevalence of depression in relation to social support, working conditions, and clinical- and substance-related factors among the study participants
Of the total participants, 193(47.2%) had low social support, 93(22.7%) reported a physical injury in the workplace, and 196(47.9%) had consumed alcohol without medical justification in the last 3 months. Among participants with low social support, 58.5% had depression at a cutoff score of 5, while 33.7% had depression at a cutoff score of 10. The PHQ-9 diagnosis of depression at cutoff scores of 5 and 10 among participants who experienced a physical injury at the workplace was 10.5 and 5.3%, respectively. The prevalence of depression at cutoff scores of 5 and 10 was higher among participants with known chronic diseases and those who had used substances (alcohol, cigarettes, or other drugs) in the last 3 months without medical justification (Table 2).
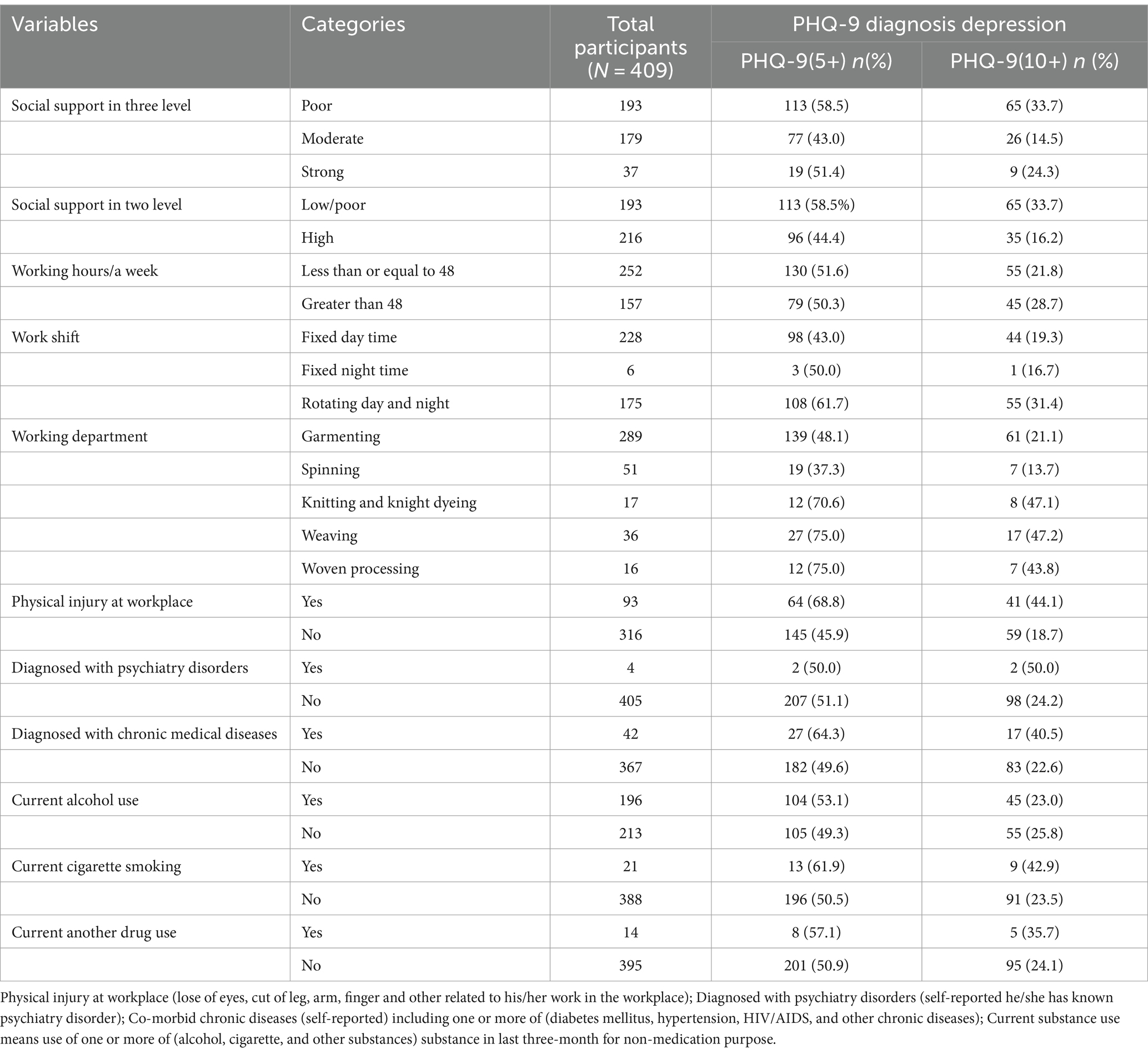
Table 2. The PHQ-9 diagnosis of depression at cut off score five and ten in level of social support, working condition, clinical and substance related factors among study participants (N = 409).
Prevalence of depressive symptoms among study participants
More than half (64.1%) of the participants reported having little interest or pleasure in doing things over the last 2 weeks, indicating that they were at least bothered by this on several days, more than half of the days, or nearly every day. Seventy-one (17.4%) of the participants had suicidal thoughts on at least one of the following frequencies in the last 2 weeks: several days, more than half of the days, or nearly every day. Among the participants, 63.6% reported that their day-to-day activities were slightly to extremely challenging related to the problems (Table 3).
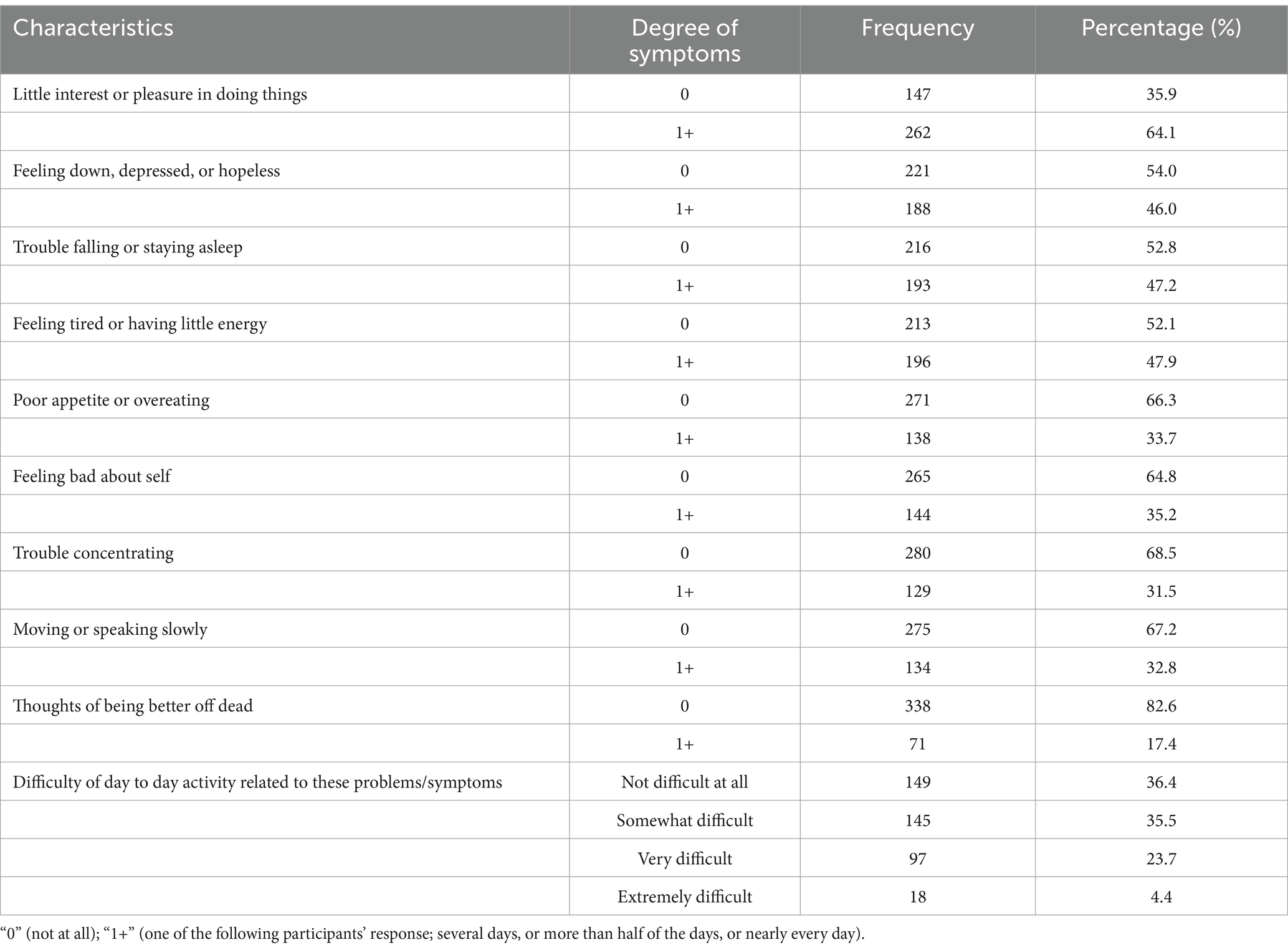
Table 3. Prevalence of PHQ-9 depressive symptoms.
The prevalence of depression among the study participants
In this study, the prevalence of depression varied according to the PHQ-9 cutoff score. At a PHQ-9 cutoff score of 10, 24.4% of the participants had potential depression, with a 95% CI of 20–29%. In contrast, at a PHQ-9 cutoff score of 5, the lowest and optimal cutoff point, the prevalence of depression was 51.1%, with a 95% CI of 46–56% (Table 4).
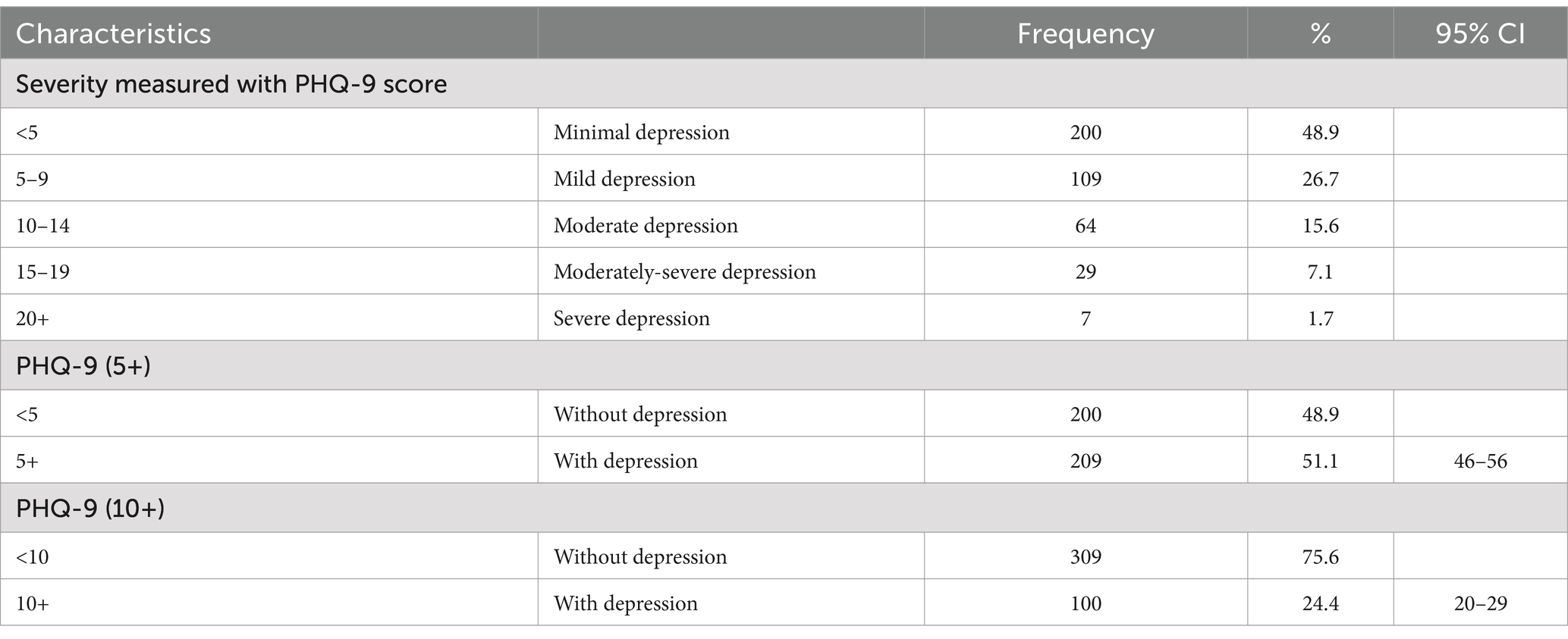
Table 4. Prevalence of PHQ-9 diagnosis depression in different cut off score in the study participants.
Factors associated with depression
After testing all variables for their association with depression at cutoff scores of 5 (PHQ-9(5+)) and 10 (PHQ-9(10+)) in the bivariate analysis, age, social support, work shift, physical injury at the workplace, and diagnosed chronic disease had a p-value of less than 0.2. In addition, educational status had a p-value of less than 0.2 at PHQ-9(5+), and current cigarette smoking status also had a p-value of less than 0.2 at PHQ-9(10+). These factors were included in the multivariate analysis as candidates for multivariable logistic regression at a significance level of p < 0.05.
In the multivariate analysis, low social support, working rotating day and night shifts, and having a physical injury at the workplace were significantly associated with depression at both PHQ-9(5+) and PHQ-9(10+). In addition, an advanced age of 45 years or above and a diagnosis of chronic disease were significantly associated with depression at the cutoff score of PHQ-9(10+) (p < 0.05). The remaining factors were not significantly associated with depression (p < 0.05), as shown in Tables 5, 6, respectively.
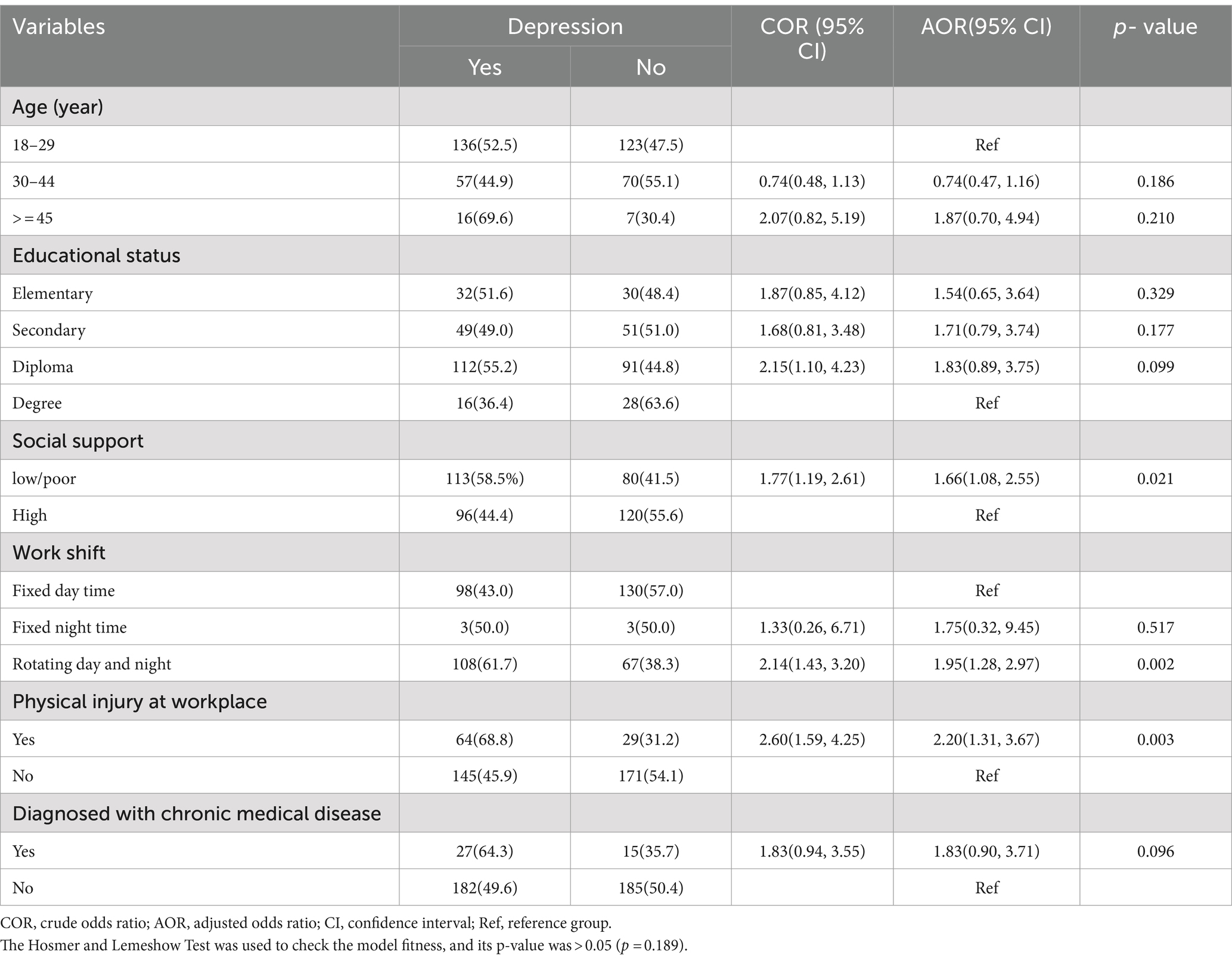
Table 5. Factors associated with depression at cut-off score five PHQ-(5+).
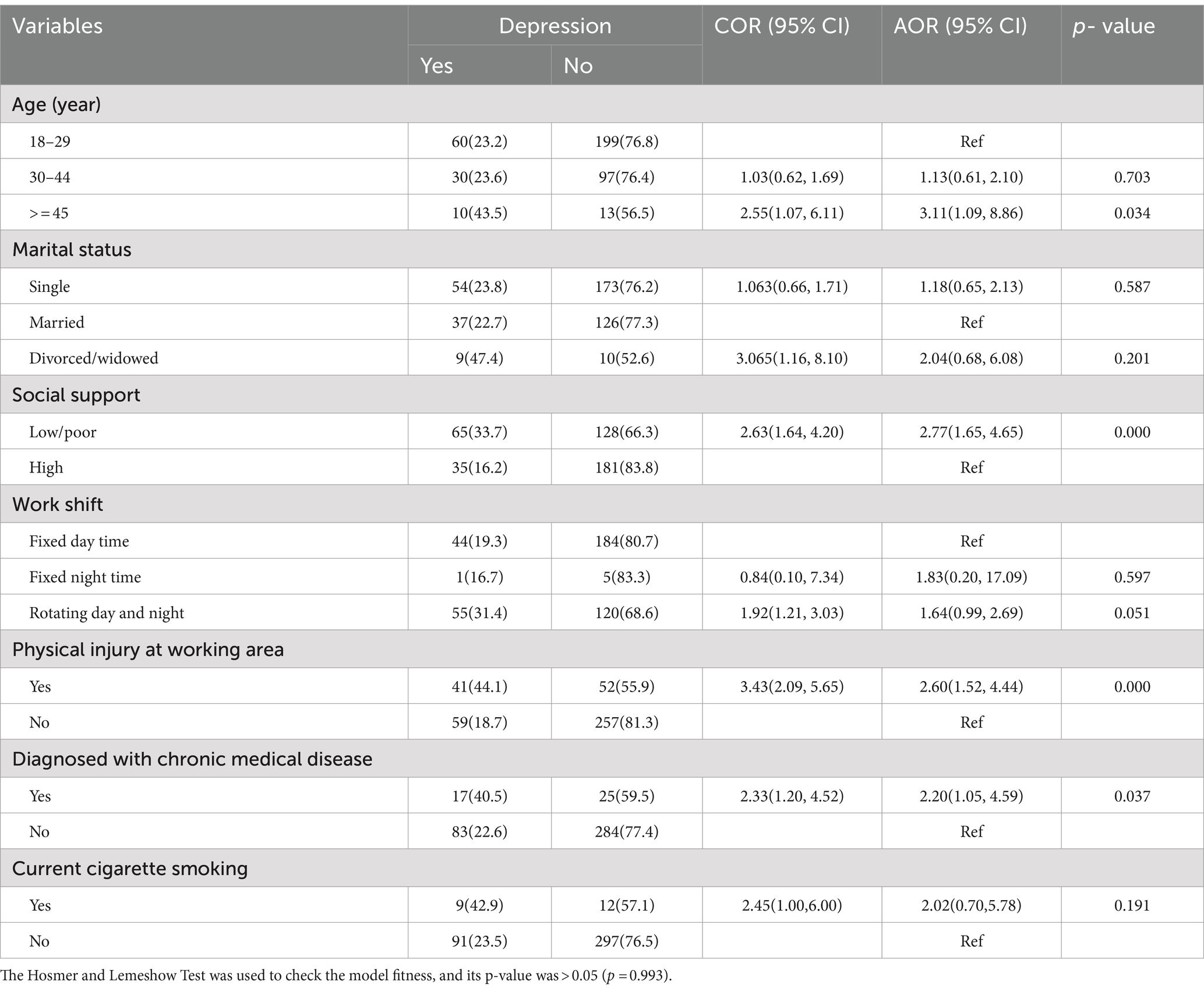
Table 6. factors associated with depression at cut-off score 10 PHQ-(10+).
Discussion
The overall magnitude of depression varied depending on the PHQ-9 cutoff score. The prevalence of depression at a PHQ-9 cutoff score of 5 was more than 2-fold that of depression at a cutoff score of 10. This finding is consistent with a previous study conducted in Ethiopia (29) and higher than that of an earlier study conducted among healthcare professionals in Ethiopia (31). Furthermore, our search revealed that there were few studies on the prevalence of depression at a PHQ-9 cutoff score of 5 in the same study population. Therefore, we focused our discussion on the PHQ-9 cutoff score of 10. The prevalence of depression at a PHQ-9 cutoff score of 10 was 24.4%, which aligns with studies conducted in Ethiopia (24, 32) and Bangladesh (33). However, this finding was lower than that of previous studies conducted in Ethiopia among university students (25) and in Vietnam (34), while it was higher than that of studies conducted in Ethiopia (35), Saudi Arabia (36), and Vietnam (37). The differences might be related to the study participant, study area and setting, and assessment tool used.
This study revealed the risk factors of depression at PHQ-9 cutoff scores of 5 (PHQ-9(5+)) and 10 (PHQ-9(10+)), which were analyzed during a multivariable logistic regression analysis. In the multivariate analysis, low social support, working rotating day and night shifts, and physical injury at the workplace were significantly associated with depression at both PHQ-9(5+) and PHQ-9(10+). In addition, an advanced age of 45 years and above and a diagnosis of chronic disease were significantly associated with depression at the cutoff score of PHQ-9(10+) (p < 0.05). The remaining factors were not significantly associated with depression (p < 0.05).
When social support was categorized into two—low and high—low social support was significantly associated with depression, which is consistent with earlier studies conducted in Vietnam (36). However, this finding is not supported by another study conducted in Ethiopia (31). Working in rotating day and night shifts was significantly associated with depression compared to working during the day. Shift work disrupts the circadian clock and affects sleep, which can lead to depression (3). Physical injury at the workplace was significantly associated with depression as compared to the absence of physical injury. Physical injury affected 42.7% of textile factory workers in Ethiopia (16). Loss of an eye, amputation of a leg or arm, and loss of a finger all have psychological and social impacts that may lead to depression (3).
In this study, regarding age, advanced age (45 years and above) was significantly associated with depression at PHQ-9(10+). Advanced age is a risk factor for depression (3), although this finding is not supported by other studies (24, 31, 34, 36). Self-reported known chronic disease was significantly associated with depression at PHQ-9(10+) when compared to no known diagnosis of chronic disease. Chronic disease is directly (biological: HIV/AIDS) or indirectly (psychological and social) a risk factor for depression (3); however, this finding is not supported by a previous study conducted in Ethiopia (A. Belete & Anbesaw, 2022; Yeshaw et al., 2017).
Limitations
There might have been limitations in establishing a causal relationship between the risk factors and depression due to the cross-sectional study design. In addition, the sample size calculation method used in this study might not support conclusions drawn from an analytical method.
Conclusion
The prevalence of depression varies according to the PHQ-9 cutoff score. The prevalence of depression at a PHQ-9 cutoff score of 5 was more than 2-fold compared to that of depression at a cutoff score of 10, indicating a high prevalence at both cutoff scores. Low social support, working rotating day and night shifts, physical injury at the workplace, belonging to the advanced age group of 45 years and above, and having a chronic disease were all significantly associated with depression. This study may provide valuable information to concerned stakeholders for the early screening and management of depression among textile factory workers.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/supplementary material.
Ethics statement
The study was conducted as per the Declaration of Helsinki and approved by the Mekelle University Ethical Review Board. Ethical clearance was obtained from the institutional review board of the Mekelle University, college of medicine and health science ethical review committee with CHS/4066115/12 ethical approval number. An informed written consent was obtained from each participant after giving a clear explanation about the purpose of the research. Study participants were assured their response will be kept confidential and no personal identifiers were used.
Author contributions
FA: Formal analysis, Methodology, Software, Writing – original draft, Writing – review & editing. TB: Conceptualization, Data curation, Investigation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We would like to thank the administrators of the Almeda Textile Factory for allowing us to collect the data. We also thank the data collectors and participants for their time.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. First, MB. DSM-5 handbook of differential diagnosis. Washington, DC: American Psychiatric Association Publishing (2013).
2. Marcus, M, Yasamy, MT, Van Ommeren, MV, Chisholm, D, and Saxena, S. Depression: a global public health concern. (2012).
3. Sadock, BJ. Kaplan and Sadock’s synopsis of psychiatry: Behavioral sciences/clinical psychiatry. Philadelphia, PA: Wolters Kluwer Health (2007).
4. Townsend, MC, and Morgan, KI. Psychiatric mental health nursing: Concepts of care in evidence-based practice. Philadelphia, PA: FA Davis (2017).
5. Chisholm, D, Sanderson, K, Ayuso-Mateos, JL, and Saxena, S. Reducing the global burden of depression: population-level analysis of intervention cost-effectiveness in 14 world regions. Br J Psychiatry. (2004) 184:393–403. doi: 10.1192/bjp.184.5.393
6. Murray, CJ, Vos, T, Lozano, R, Naghavi, M, Flaxman, AD, Michaud, C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the global burden of disease study 2010. Lancet. (2012) 380:2197–223. doi: 10.1016/S0140-6736(12)61689-4
7. Ustün, T. The global burden of mental disorders. Am J Public Health. (1999) 89:1315–8. doi: 10.2105/AJPH.89.9.1315
8. Mathers, CD, and Loncar, D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. (2006) 3:e442. doi: 10.1371/journal.pmed.0030442
9. Reddy, MS. Depression–the global crisis. Indian J Psychol Med, (2012), 34, 201–203. doi: 10.4103/0253-7176.106011
10. Hasanbeigi, A, and Price, L. A review of energy use and energy efficiency technologies for the textile industry. Renew Sust Energ Rev. (2012) 16:3648–65. doi: 10.1016/j.rser.2012.03.029
11. Kohli, N, and Mehta, M. Occupational stress among textile industry worker. IOSR J Hum Soc Sci. 27:1–7.
12. Anandi, BS, Rajaram, D, Aravind, B, Sukumar, GM, and Radhika, K. Work-related stress assessment among a garment factory employee in Bangalore suburban locality. Int J Community Med Public Health. (2017) 4:3870–6. doi: 10.18203/2394-6040.ijcmph20174266
13. Belete, H, Ergetie, T, Ali, T, Birhanu, S, and Belete, T. Work-related stress and associated factors among textile factory employees in Northwest Ethiopia: a cross-sectional study. Psychol Res Behav Manag. (2020) 13:1071–8. doi: 10.2147/PRBM.S282061
14. Burton, WN, Schultz, AB, Chen, CY, and Edington, DW. The association of worker productivity and mental health: a review of the literature. Int J Workplace Health Manag. (2008) 1:78–94. doi: 10.1108/17538350810893883
15. Angaw, Y, Kumie, A, Tefera, Y, Wakuma, S, Nega, A, Hidru, HD, et al. Temporary hearing loss and associated factors among Ayka Addis textile factory workers in Oromia region, Ethiopia: a cross-sectional study. Risk Manag. Healthcare Policy. (2021) 14:719–28. doi: 10.2147/RMHP.S269609
16. Damtie, D, and Siraj, A. The prevalence of occupational injuries and associated risk factors among workers in Bahir Dar textile share company, Amhara region, Northwest Ethiopia. J Environ Public Health. (2020) 2020, 1:1–9. doi: 10.1155/2020/2875297
17. Gupta, RD, Nag, S, Datta, D, Roy, S, Das, S, and Aziz, SMY. Occupational health hazards among workers in garment factories in Bangladesh: a cross-sectional study. Occup Health. (2015) 5:90–8.
19. Zaw, AK, Myat, AM, Thandar, M, Htun, YM, Aung, TH, Tun, KM, et al. Assessment of noise exposure and hearing loss among workers in textile mill (Thamine), Myanmar: a cross-sectional study. Saf Health Work. (2020) 11:199–206. doi: 10.1016/j.shaw.2020.04.002
20. Zele, YT, Kumie, A, Deressa, W, Bråtveit, M, and Moen, BE. Registered health problems and demographic profile of integrated textile factory workers in Ethiopia: a cross-sectional study. BMC Public Health. (2021) 21:1–15. doi: 10.1186/s12889-021-11556-4
21. Ismail, IM, and Binub, K. Prevalence of hypertension and its associated factors among cotton textile workers of Kannur, Kerala. Menoufia Med J. (2016) 29:991. doi: 10.4103/1110-2098.202520
22. Zegeorgous, KG, Gebru, HT, Demssie, AF, Mekonnen, TH, Aregawi, BG, and Woldegebriel, MK. Utilization of personal protective equipment and associated factors among Kombolcha textile factory workers, Kombolcha, Ethiopia: a cross-sectional study. J Public Health. (2020) 7:11. doi: 10.5348/100025P16KZ2020RA
23. Molla, GL, Sebhat, HM, Hussen, ZN, Mekonen, AB, Mersha, WF, and Yimer, TM. Depression among Ethiopian adults: cross-sectional study. Psychiatry J. (2016) 2016:1–5. doi: 10.1155/2016/1468120
24. Yeshaw, Y, and Mossie, A. Depression, anxiety, stress, and their associated factors among Jimma University staff, Jimma, Southwest Ethiopia, 2016: a cross-sectional study. Neuropsychiatr Dis Treat. (2017) 13:2803–12. doi: 10.2147/NDT.S150444
25. Birhanu, A, and Hassein, K. Prevalence and factors associated to depression among ambo university students, Ambo West Ethiopia. J Health Med Nurs. (2016) 25:26–34.
26. Ebrahim, M, Tamiru, D, Hawulte, B, and Misgana, T. Prevalence and associated factors of depression among diabetic outpatients attending diabetic clinic at public hospitals in eastern Ethiopia: a cross-sectional study. SAGE Open Med. (2021) 9:244. doi: 10.1177/20503121211066244
27. Kroenke, K, Spitzer, RL, and Williams, JBJ. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
28. Gelaye, B, Williams, MA, Lemma, S, Deyessa, N, Bahretibeb, Y, Shibre, T, et al. Validity of the patient health questionnaire-9 for depression screening and diagnosis in East Africa. Psychiatry Res. (2013) 210:653–61. doi: 10.1016/j.psychres.2013.07.015
29. Fekadu, A, Medhin, G, Selamu, M, Giorgis, TW, Lund, C, Alem, A, et al. Recognition of depression by primary care clinicians in rural Ethiopia (2017) 18:1–9. doi: 10.1186/s12875-017-0628-y,
30. Kocalevent, R-D, Berg, L, Beutel, ME, Hinz, A, Zenger, M, Härter, M, et al. Social support in the general population: standardization of the Oslo social support scale (OSSS-3). BMC Psychol. (2018) 6:1–8. doi: 10.1186/s40359-018-0249-9
31. Belete, A, and Anbesaw, TJB. Prevalence and associated factors depressive symptoms among healthcare professionals at Dessie comprehensive specialized hospital, Ethiopia. BMC Psychiatry. (2022) 22:446. doi: 10.1186/s12888-022-04102-y
32. Bifftu, BB, Takele, WW, Guracho, YD, and Yehualashet, FA. Depression and its help seeking behaviors: a systematic review and meta-analysis of community survey in Ethiopia. Depress Res Treat. (2018) 2018:1–11. doi: 10.1155/2018/1592596
33. Fitch, TJ, Moran, J, Villanueva, G, Sagiraju, HKR, Quadir, MM, and Alamgir, H. Prevalence and risk factors of depression among garment workers in Bangladesh. Int J Soc Psychiatry. (2017) 63:244–54. doi: 10.1177/0020764017695576’
34. Do, HN, Nguyen, AT, Nguyen, HQT, Bui, TP, Nguyen, QV, Tran, NTT, et al. Depressive symptoms, suicidal ideation, and mental health service use of industrial workers: evidence from Vietnam. Int J Environ Res Public Health. (2020) 17:2929. doi: 10.3390/ijerph17082929
35. Hailemariam, S, Tessema, F, Asefa, M, Tadesse, H, and Tenkolu, GJI. The prevalence of depression and associated factors in Ethiopia: findings from the National Health Survey. Int J Ment Health Syst. (2012) 6, 6:23, 23–11. doi: 10.1186/1752-4458-6-23
36. AlFahhad, N. Prevalence and factors associated with depression among health care workers in National Guard Hospital in Riyadh, KSA. Int J Med Develop Ctries. (2018) 2:92–6. doi: 10.24911/IJMDC.51-1526306040
Keywords: depressive symptoms, depression, associated factors, textile factory workers, textile factory, Ethiopia
Citation: Begashaw TD and Andualem F (2024) Depression and its associated factors among textile factory workers at the Almeda textile factory, North Ethiopia. Front. Public Health. 12:1393581. doi: 10.3389/fpubh.2024.1393581
Edited by:
Xiao Zhang, Peking University Sixth Hospital, ChinaReviewed by:
Kampanat Wangsan, Chiang Mai University, ThailandGebeyaw Kassie, Lecturer, Injibara, Ethiopia
Copyright © 2024 Begashaw and Andualem. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fantahun Andualem, ZmFudGFhbmR1MjdAZ21haWwuY29t